anatomy stomach - University of Babylon
23
UNIVERSITY OF BABYLON HAMMURABI MEDICAL COLLEGE GASTROINTESTINAL TRACT S4-PHASE 1 2018-2019 Session 5 _ Lect.2 Anatomy of Stomach Dr. Suhad Kahdum Ali F.I.B.M.S. (Surg.), M.B.Ch.B. [email protected]om
Transcript of anatomy stomach - University of Babylon

UNIVERSITY OF BABYLONHAMMURABI MEDICAL
COLLEGE
GASTROINTESTINAL TRACTS4-PHASE 12018-2019
Session 5 _ Lect.2 Anatomy of StomachDr. Suhad Kahdum AliF.I.B.M.S. (Surg.), [email protected]

Objectives´ describe the gross structure, parts and curvatures of the stomach´ describe the structure and function of the oesophageal/gastric sphincter and the
pyloric sphincter´ describe the macro and microscopic structure of the gastric mucosa´ describe and identify the following structures:
v attachments of the lesser and greater omentumvcurvatures of the stomach and its regions (fundus, body, pyloric antrum& pylorus)vcoeliac trunk and its main branches (left gastric, splenic and common hepatic)vblood supply (arteries&veins) of stomach the enterance of the lesser sac (epiploic
foramen)

Oesophagus
´fibromuscular tube that extends from the pharynx to the stomach and is roughly 25cm in length.
´three main strictures (cervical, thoracic, and oesophageal) ´the oesophageal constrictor is produced as the oesophagus passes
through the diaphragm at the oesophageal hiatus (T10).
´The anterior and posterior vagal trunks join the oesophageal plexus that surround the oesophagus, and then follow the oesophagus through the diaphragm into the abdomen.

Clinical Considerations
Hiatus hernia is a protrusion of part of the stomach into the mediastinum through the oesophageal hiatus of the diaphragm. The hernias occur due to weakening in the diaphragm muscle causing the widening of the oesophageal hiatus, meaning that parts of the stomach can move upwards.
This can be either the fundus alone, whereby there is usually no regurgitation due to the correct positioning of the cardia, or the cardia and parts of the
fundus, whereby some regurgitation is possible.

General Anatomy of Stomach
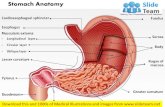
´ J-shaped organThe stomach has 5 parts and a greater and lesser curvature:
Cardia, Fundus,Body,Antrum,Pylorus.
´Lies in the epigastric (E),umbilical (U) & Left hypochondrium (LH) ´ Size & position depends on body
shape, degree of distension &posture.

Gastric Mucosa – Endoscopy
Gastric Cardia
Gastric body
Gastric Fundus
Gastric Antrum
Pylorus

Oesophageal/gastric sphincter and the pyloric sphincter
Sphincters exist at the entry and exit parts of the stomach. Inferior Oesophageal Sphincter
The oesophagogastric junction lies to the left of the T11 vertebra on the horizontal plane that passes through the tip of the xiphoid process. Z-Line : a line where the mucosa changes from oesophageal to gastric.
Immediately superior to the Z-line, the diaphragmatic musculatureforming the oesophageal hiatus functions as a physiological sphincter that contracts and relaxes. This, coupled with the cardiac notch prevents the reflux of stomach contents.

Reflux of Gastric Contents into the oesophagus is common
If it is frequent and/or clearance of reflux material is deficient,
“heartburn” and/or inflammation with ulceration may result.
Chronic reflux may result in metaplastic changes in the mucosa (Barrett’s oesophagus).

Pyloric Sphincter
At the pyloric end of the stomach, the circular muscle coat is thickened to produce the pyloric sphincter. This controls the discharge of the stomach contents through the pyloric orifice into the duodenum.

Macro and Microscopic structure of the gastric Rugae: it is longitudinal folds of gastric mucosa.
Gastric canal: forms temporarily between the gastric folds along lesser curvature to allow saliva and other fluids to pass along to the pylorus.
The Gastric mucosa has 3 histologically zones: ´ Cardia Neck cells - Mucus´Fundus and Body
Neck cells – MucusParietal – AcidChief – Pepsinogen
´Pyloric Neck cells – MucusG-Cells – Gastrin

Peptic ulcersUlcer :- is an erosion or loss of continuity.
commonly occur in the antrum and along the lesser curvature of the stomachPerforation of ulcers leads to the spillage of
gastric contents into the peritoneal cavity, which may affect abdominal structures such as the pancreas and associated blood vessels lying in close proximityto the stomach.

Gastric Ulcers
gastric ulcer → pain on eatingduodenal ulcer →pain when they are hungry
Anatomical relationships determine Posterior wall ulcers penetrate the regionsof the gastroduodenal artery and thus bleed.
Anterior wall ulcers penetrate the peritoneumand thus perforate into the peritoneal cavity.

Greater Omentumfour-layered peritoneal fold that hands down like an apron from the Greater
Curve of the Stomach.
After descending it folds back and attaches to the anterior surface of the Transverse Colon and its mesentery.
Lesser Omentumdouble-layered peritoneal fold that
connects the Lesser Curvature of the Stomach and the Proximal part ofthe Duodenum to the Liver.It also connects the stomach to the portal triad.

Epiploic ForamenThe greater and lesser sacs communicate through the omental foramen (epiploic foramen),
an opening situated posterior to the free edge of the less omentum .
The omental foramen can located by running a finger along the gall bladder to free the edge of the lesser omentum, and usually admits 2 fingers.

Stomach – Arterial Blood Supplyarises from the celiac trunk and its branches.
Lesser Curvature´ Coeliac Trunk à Left Gastric
´ Coeliac Trunk à Common Hepatic àRight Gastric
Greater Curvature´ Coeliac Trunk à Splenic àLeft Gastro-Omental (epiploic)
´ Coeliac Trunk àCommon Hepatic àGastroduodenal àRight Gastro-Omental
Fundus and Body´ Coeliac Trunk à Splenic à Posterior Gastric / Small Gastric
CoeliacTrunkoriginates from the Abdominal Aorta,
Left Gastric, Splenic and Common Hepatic Arteries.


Stomach – Venous DrainageLeft Gastric Vein & Right Gastric Vein
Follows the course of the LT & RT Gastric ArteryDrains → Hepatic Portal Vein
Short Gastric VeinFollows the course of the Short Gastric ArteryDrains → Splenic Vein & Joins SMV to form Hepatic Portal Vein
Left Gastro-Omental VeinFollows the course of the Left Gastro-Omental Artery
Drains → Splenic Vein & Joins SMV to form Hepatic Portal VeinRight Gastro-Omental Vein
Follows the course of the Right Gastro-Omental ArteryDrains → Superior Mesenteric Vein & Joins Splenic Vein to
form Hepatic Portal Vein


Nerve supply of stomach
Sympathetic nerve supply from T6 to T9 segments via
Greater Splanchnic Nerveto the Celiac plexus

Stomach Nerve Supply – Vagus Nerves
´ The left & right vagus nerves enter the abdomenthrough the oesophageal hiatus (T10 vertebral level)• The anterior vagus supplies the anterior surfacethe stomach and gives off a hepatic branch of( liver, gall bladder & the pylorus)´ The posterior vagus gives off a celiac branch
(which passes to the celiac plexus) & a posteriorbranch to the posterior surface of the stomach

Inflammation of the stomach (Gastritis)
may be:´ Acute
´Caused by NSAIDS / Alcohol´Exfoliation of the surface epithelial cells and decreased secretion
of protective mucus´ Chronic
´Infection with the bacteria Helicobacter Pylori´Inflammatory changes in the mucosa result in atrophy and
epithelial metaplasia (may develop into carcinoma)

Posterior gastric canceror ulcer mayerode the pancreas –leading to back pain
Ulceration intoSplenic artery
may result inseverehaemorrhage
pancrease
Stomach post. wall
Normal air