ANATOMY & PHYSIOLOGY 1 (101-805 - AB) Unit 7...
23
ANATOMY & PHYSIOLOGY 1 (101-805 - AB) PAUL ANDERSON 2011 Unit 7 THE MUSCULAR SYSTEM KEY CONCEPTS 1. The muscular system consists of all the skeletal muscle organs of the body together with their connections to bones (e.g. tendons). 2. The major homeostatic functions of the muscular system are to convert chemical energy to mechanical energy and heat for the following: • to power movement (reflex and voluntary behaviour, breathing movements and facial expression): • for posture and balance: posture means proper position or alignment of body parts: maintaining an upright posture means positioning of body parts in opposition to gravity and is normally a function of “anti - gravity muscles” (extensors) which put the center of gravity over the base of the body so that the body is stable. In walking, the center of gravity shifts first over one foot then over the other: • for heat production; muscles are the major sources of body heat, for body temperature control: • stabilization of joints by constant muscle tone (especially for knee and shoulder joints): • control of entrances and exits of digestive and urinary tracts (sphincter muscles).
Transcript of ANATOMY & PHYSIOLOGY 1 (101-805 - AB) Unit 7...

ANATOMY & PHYSIOLOGY 1 (101-805 - AB) PAUL ANDERSON 2011 Unit 7 THE MUSCULAR SYSTEM KEY CONCEPTS 1. The muscular system consists of all the skeletal muscle organs of the body together with their
connections to bones (e.g. tendons). 2. The major homeostatic functions of the muscular system are to convert chemical energy to
mechanical energy and heat for the following:
• to power movement (reflex and voluntary behaviour, breathing movements and facial expression):
• for posture and balance: posture means proper position or alignment of body parts:
maintaining an upright posture means positioning of body parts in opposition to gravity and is normally a function of “anti - gravity muscles” (extensors) which put the center of gravity over the base of the body so that the body is stable. In walking, the center of gravity shifts first over one foot then over the other:
• for heat production; muscles are the major sources of body heat, for body temperature control:
• stabilization of joints by constant muscle tone (especially for knee and shoulder joints): • control of entrances and exits of digestive and urinary tracts (sphincter muscles).

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 2 3. The two major tissues in the muscular system are skeletal (striated or voluntary) muscle and
various collagenous dense connective tissues (e.g. tendons). These are organised into muscle organs e.g. biceps brachii muscle.
4. Skeletal muscle tissue, like other muscle tissues, is specialised for the following properties:
• ability to generate an impulse when stimulated (excitability or irritability) • ability to conduct the impulse to all parts of the cell (conductivity) • ability to generate a force for movement (contractility) • ability to stretch (extensibility) • ability to return to original length after contracting or stretching (elasticity).
5. Muscle organs are composed of various connective tissue sheaths which are of non - contractile, elastic, collagenous tissues. These sheaths have the following functions:
• conduct nerve fibers, blood and lymph vessels to muscle cells • bind the cells together • transmit the contractile force of the muscle cells to bones • give shape to muscle organs • contribute to muscle’s extensibility and elasticity. These sheaths are as follows: • The epimysium covers the surface of a muscle and shapes the muscle. • The perimysium covers the fasciculi (fascicles) which are bundles of microscopic
muscle fibers and also contains stretch receptors. • The thin endomysium surrounds each muscle fiber or cell.
6. The muscle tendon is continuous with all of the other sheaths and binds most muscles to the
periosteum of a bone to which it transmits the force of muscle contraction. 7. Skeletal (striated or voluntary) muscle tissue differs from both smooth and cardiac muscle as
follows:
• its cells are multinucleated, very long (stretching the length of a muscle organ), with obvious cross striations
• its force of contraction is usually transmitted to bone and produces visible movements
• its contraction requires a nerve impulse so skeletal muscle is not autorhythmic • it is controlled by the somatic branch of the peripheral nervous system and so is
under voluntary control • its speed of contraction (<0.1sec.) is faster • it is subject to muscle fatigue

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 3
STRUCTURE OF A SKELETAL MUSCLE

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 4
Anatomy of a Muscle Organ
Martini & Bartholomew fig 7-1
Microscopic Anatomy of a Skeletal Muscle Fiber
Martini & Bartholomew fig 7- 2a

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 5 8. The structure of a skeletal muscle cell (as revealed by the light and electron microscope and
biochemical studies) is as follows:
• The muscle fiber is tightly packed with parallel cylindrical units called myofibrils. • The myofibril has the same striated (or striped) appearance as the muscle fiber with
alternating light (I) bands and dark (A) bands (lIght-dArk). • The striations are caused by cylindrical proteins in each myofibril called myofilaments;
these interact to cause muscle contraction. • The light (I) bands consist of thin myofilaments containing the protein actin. • In the center of the I band is a line called the Z line (or Z disk) containing another protein
connecting the thin actin myofilaments together. • The dark (A) bands consist of thick myofilaments containing the protein myosin together
with overlapping thin (actin) myofilaments. • In the center of the A band is a lighter zone called the H zone; this represents the region
containing only thick myosin myofilaments (no actin myofilaments). • In the center of the H zone is another line (the M line) containing proteins that bind the
myosin myofilaments together. • The region of a myofibril between successive Z lines is called a sarcomere and is
considered the functional unit of a muscle cell.

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 6
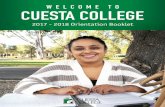
Structure of a Sarcomere
Martini & Bartholomew fig 7-2b
Sliding Filament Theory of Muscle Contraction
Martini & Bartholomew fig 7-3
Martini & Bartholomew fig 7-2e

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 7
• The cell membrane of the muscle cell (called the sarcolemma) has invaginations that form tubules (called T tubules) running around each myofibril at the junction between A and I bands.
• The cytoplasm of a muscle cell (called the sarcoplasm) has an extensive smooth endoplasmic reticulum (called the sarcoplasmic reticulum or SR) which stores Ca+2 in its lateral sacs (terminal cisternae).
• Each T tubule passes between two adjacent lateral sacs of the SR forming a combination called a triad.
• When an impulse carried by the T tubules reaches the triad it causes release of Ca+2 from the lateral sacs of the SR. This triggers muscle contraction.
Contraction of a Muscle Cell
9. The sliding filament theory of muscle contraction states that when a muscle contracts the
myofilaments do not shorten but instead slide past each other; the thin actin filaments are pulled towards the H zone by the thick myosin filaments which therefore approach the Z line.
10. The sliding filament theory is borne out by the following observed changes when a muscle
contracts: • the H zone gets smaller and disappears, as the actin filaments on each side approach each
other • the I band gets smaller and disappears as the thick filaments approach the Z line • the A bands get closer together but do not change their length since this is equal in length
to the thick myosin filaments • the sarcomere gets shorter since adjacent Z lines are pulled together

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 8 RELAXED SARCOMERE
CONTRACTED SARCOMERE
11. Muscle cell contraction is triggered by the release of Ca+2 from the SR into the ICF. In the
resting muscle cell Ca+2 is actively transported into the SR, the function of which is to store Ca+2 until needed. Therefore there is a low ICF [Ca+2] in the resting cell, insufficient to trigger contraction.
12. The thick filaments contain many myosin molecules each of which has a two globular heads
all oriented towards the Z line. Therefore on either side of the H zone the myosin molecules are oriented in opposite directions. In the presence of Ca+2 the myosin heads bind to the adjacent actin molecule of the thin filament forming cross bridges and pull these towards the center of the sarcomere (the H zone). This happens during muscle contraction.

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 9 13. ROLES OF ATP ATP powers muscle contraction. To do this ATP has three roles to play.
energy from ATP hydrolysis activates myosin molecules so they can pull on actin molecules causing muscle contraction. Therefore myosin heads must have an enzyme (ATPase) to split ATP and release its energy activating the myosin heads.
• When the energy from ATP hydrolysis is spent, a new ATP molecule binds to myosin.
Binding of ATP to myosin causes the detachment of myosin from actin allowing a new contraction cycle to begin.
• Energy from ATP hydrolysis is used to pump Ca+2 into the SR after contraction. 14. CONTRACTION SEQUENCE The sequence by which myosin pulls on actin causing muscle
shortening is as follows. In a single muscle contraction each myosin head must go through this sequence many times.
• ATP binds to myosin and is hydrolysed to ADP and Pi. This activates the myosin head
so that it extends along the actin molecule towards the Z line. • If Ca+2 is present the activated myosin head binds to actin and flexes, pulling actin
towards the center of the sarcomere (i.e. towards the center of the H zone). • This releases ADP and Pi from myosin which allows another ATP to bind to myosin. • The binding of ATP to the myosin head causes it to detach from actin. • ATP hydrolysis reactivates the myosin head. If Ca+2 is reabsorbed into the SR the
contraction cycle ends here. • If Ca+2 is not reabsorbed into the SR the sequence repeats from step 2 above.
15. RIGOR MORTIS Since binding of ATP to myosin causes it to detach from actin, in the complete absence of ATP
(following death), Ca+2 cannot be actively transported into the SR and myosin molecules are unable to detach from actin. Therefore the muscle remains stiffly contracted, a condition called rigor mortis.
16. RESTING MUSCLE: ROLE OF TROPONIN, TROPOMYOSIN & Ca+2 In the resting muscle binding of activated myosin is normally prevented by two additional
proteins (troponin and tropomyosin) which are attached to actin and protect its binding site. Release of Ca+2 from the sacs of the SR causes a shape change in troponin which then pulls tropomyosin away from the actin binding site and allows myosin to bind and muscle contraction to occur.
17. EXCITATION – CONTRACTION COUPLING Ca+2 release from the sacs of the SR is triggered by an action potential (impulse) which arrives
at the triad from the sarcolemma via the T tubules. The triggering of muscle contraction by an action potential is called excitation – contraction coupling.

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 10
Arrival of a Motor Impulse at Neuromuscular Junction
Martini & Bartholomew fig 7-4
Steps in Muscle Contraction Cycle
Martini & Bartholomew fig 7-5

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 11
18. Excitation – Contraction Coupling occurs as follows:
• A nerve impulse arrives at the axon terminals of a motor neuron to a skeletal muscle: the junction of the two cells is called a neuromuscular junction.
• The axon terminal ends in a swelling which fits into a depression in the sarcolemma called the motor end plate.
• The impulse causes release of acetylcholine (Ach) by exocytosis. • Ach activates membrane receptors in the motor end plate which triggers an impulse in the
sarcolemma of the muscle cell. • The impulse spreads over the surface of the muscle cell and enters the T tubules where it is
conducted to the triad causing the lateral sacs of the SR to release Ca+2 . • Ca+2 binds to troponin which changes shape pulling tropomyosin away from actin; the site on
actin where myosin can bind is now exposed. • The ATP activated myosin heads now bind to actin and pull actin towards the H zone. • In the absence of an impulse the SR removes Ca+2 from the ICF by active transport, troponin
and tropomyosin once more block actin’s binding site, myosin cannot bind and the muscle relaxes.

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 12
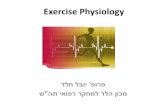
Motor impulse to muscle cell
Ca+2 released from SR
Active sites exposed on actin
Activated myosin heads bind to sctive sites on actin forming "crossbridges"
Myosin heads flex and pull actin towards the center of the H zone
impulse conducted to triad
troponin/tropomyosin block removed
ADP + Pi released ATP binds to myosin heads
Myosin detaches from actin
ATP hydrolysed
Myosin heads activated
CONTRACTION CYCLE
No impulse to muscle
Ca+2 pumped back into SR
Active sites blocked
Muscle relaxes
MUSCLE
RELAXATION
Contraction Cycle of a Muscle Cell
active

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 13 Summary of Muscle Contraction
Martini & Bartholomew Table 7-1

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 14
Contraction and Relaxation of Muscle Organs
19. MUSCLE CONTRACTION is the process of generating a force in a muscle organ. The net force produced by a muscle organ is called muscle tension.
20. MUSCLE RELAXATION is loss of force in a muscle and so is the opposite of muscle
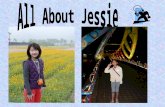
contraction. Types of Muscle Contraction 21. ISOTONIC CONTRACTION occurs whenever a muscle changes its length while
contracting. Part of the energy of contraction performs mechanical work (= resistance x distance moved). Any movement involves isotonic contraction.
22. There are two types of isotonic contraction, concentric and eccentric.
• CONCENTRIC CONTRACTION occurs whenever a muscle shortens while contracting isotonically. Here the tension generated by the muscle exceeds the load (resistance, or force opposing the muscle).
• Sometimes a muscle lengthens while contracting isotonically (e.g. the quadriceps femoris
while sitting down, or the biceps brachii while lowering a weight in the hand). Here the load exceeds the tension. This is referred to as ECCENTRIC CONTRACTION (or paradoxical action) and the muscle performs negative work.
23. ISOMETRIC CONTRACTION occurs when the tension exerted by a muscle does not exceed
the load (resistance) opposing the muscle and the muscle organ does not change its length. Here all the energy escapes as heat and no mechanical work is done.
Examples: standing still (extensors of leg), pushing against a closed door (extensors of arm), holding a weight in a stationary position.
24. All movements involve isotonic and isometric phases and normal functioning of the skeleto-
muscular system depends on a combination of isotonic and isometric contractions.
• In walking and running isometric contractions keep the legs stiff when the feet touch the ground.
• All movements begin with a brief isometric phase when the tension is increasing but is still
less than the load.
Isotonic Concentric Movement Muscle Contraction Eccentric
Isometric No Movement

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 15
Graded Responses of Muscle Organs
25. A single impulse to a muscle produces a single brief all- or -none contraction and relaxation response called a muscle twitch. However, muscle responses are normally smooth and vary in intensity according to needs. Such GRADED RESPONSES of muscles depend on temporal and spatial summation of individual contractions (twitches).
26. TEMPORAL (OR WAVE) SUMMATION occurs when motor impulses arrive in such rapid
succession (i.e. at a high frequency) that each contraction adds onto the previous one and eventually a fusion of twitches occurs, forming a smooth sustained stronger contraction, called tetanus.
Temporal summation is caused by • increased availability of Ca+2 (each impulse releases more Ca+2 • sustained stretching of non- contractile tissues (“series elastic elements”) such as tendons in
the muscle (i.e. these are not allowed to recoil as in a twitch). 27. SPATIAL SUMMATION refers to the RECRUITMENT of increasing numbers of motor
units in a muscle.
• A motor unit consists of all the muscle cells controlled by a single motor neuron. A motor unit is the smallest unit of contraction for a muscle, i.e. represents the minimum response of a muscle. Each muscle cell contracts as part of a motor unit. Both muscle cells and motor units obey the all – or – none law.
• Spatial summation (by multiple motor unit summation or recruitment) is therefore
largely responsible for increasing the force of contraction of the muscle. • Recruitment occurs when the brain activates more axons in each motor nerve to a muscle.
28. The innervation ratio is the ratio between the number of axons in a motor nerve to a muscle
and the number of muscle cells in the muscle. It is used to calculate the average motor unit size for a muscle.
29. Muscles controlling precision movements requiring many fine gradations of movement have
small motor units, e.g. flexors of the fingers, 1 axon: 10 muscle fibers: extrinsic eye muscles, 1: 3.
30. Muscles controlling gross movements requiring little variation have large motor units, e.g.
extensors of the thighs 1: 150.

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 16
Spatial Summation (Recruitment) of Motor Units
Martini & Bartholomew fig 7-8

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 17
Muscle Tone and The Stretch Reflex 31. MUSCLE TONE is the continual partial contraction of a resting muscle and is maintained by
the stretch reflex. Tone is most important for "anti gravity" muscles. 32. The STRETCH REFLEX is initiated by stretching of a muscle: in response the same muscle
shortens. Thus stretching of extensor muscles of the trunk and legs ("anti - gravity" muscles) by gravity causes a reflex contraction of the same muscles which therefore stiffen and oppose gravity.
The nerve pathway mediating the reflex involves muscle receptors called muscle spindles, a
sensory nerve fiber, a motor nerve fiber and a synapse in the spinal cord.
33. Muscle tone is important for muscle health, rapidity of response, for stabilizing joints and
for posture. Muscle tone is present during waking hours and is dependent on the stretch reflex and on descending motor pathways from the brain. Tone is reduced during sleep and in flaccid paralysis.
Muscle Paralysis 34. Paralysis means loss of voluntary control over muscles. 35. Spastic paralysis is characterised by hypertonia (spasticity) and exaggerated reflexes.
Spasticity is caused by the stretch reflex which is overactive. The usual cause is a stroke (cerebrovascular accident) which damages upper motor neurons.
36. Flaccid paralysis is characterised by hypotonia (flaccidity) and the absence of reflexes. This is
caused by muscle denervation , i.e. damage to lower motor neurons (e. g. with poliomyelitis). 37. Flaccid paralysis causes muscle atrophy or shrinking of the muscle caused by shrinking of
cells and/or reduction in cell number.

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 18 38. Types of Muscle Atrophy. There are two types of muscle atrophy depending on the cause:
• atrophy of denervation is caused by the cutting of the neve supply (innervation) to the muscle i.e. denervation (e.g.. in poliomyelitis); unless the muscle is renervated (or electrically stimulated) within four months the atrophy is irreversible.
• atrophy of disuse occurs when a muscle is not used for an extended period (e.g. limb in a cast,
bedridden person; since the muscle is not stretched muscle tone is reduced (hypotonia). This type of atrophy is reversible if the muscle is reused.
39. Muscle hypertrophy refers to the increase in size of the muscle by an increase in the size of
individual cells (more myofibrils) without increase in cell number. This is caused by increased use of muscles with or without the use of anabolic steroids.
Roles of Muscles in Movements 40. During any movement muscles may function as:
• Prime Movers (or agonists) which directly cause a movement by their contraction e.g.. biceps brachii is a prime mover for flexion of the elbow.
• Antagonists which oppose a given movement when they contract e.g. the triceps brachii is
an antagonist for flexion of the elbow. • Synergists which are muscles which also contract during a movement but do not directly
cause the movement but help the prime mover to work efficiently. Fixators are synergists which steady the movement by stabilising (or “fixing”) a joint e.g. the pectoralis major and deltoid muscles steady the humerus bone during flexion of the elbow and so are fixators.
41. Muscles in the body are grouped into antagonistic pairs. The two members of the antagonistic
pair are prime movers for opposing movements and occur on opposite sides of the limb or trunk (e.g.. biceps brachii and triceps brachii are on opposite sides of the upper arm).
42. During any movement the antagonist must relax while the prime mover contracts. 43. Relaxation of the antagonist during a movement involves inhibiting the motor nerve fibers
going to the muscle, thus preventing the stretch reflex (which would otherwise cause contraction of the antagonist).

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 19 44. The reflex inhibition of motor fibers to an antagonist during a movement with the
simultaneous excitation of motor fibers to the prime mover is called reciprocal inhibition. examples:
• the withdrawal reflex involves reflex inhibition of nerve fibers to ipsilateral (same side) limb extensors.
• in the crossed - extensor reflex flexion of one limb is accompanied by reflex inhibition of flexors of the opposite (contralateral) limb so that this limb can extend and support the body’s weight.
Reciprocal Inhibition.

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 20 Muscles as Components of Levers
45. The skeleto - muscular system is a system of levers (devices for performing work). In any movement:
• one end of the prime mover muscle is attached to a relatively immobile tissue (usually a
bone); this is called the muscle’s origin • the other end of the muscle is attached to a moveable tissue (bone); this is called the
muscle’s insertion • the insertion point of the muscle is the power point (P) of the lever • the fulcrum (F) of the lever is the moveable joint at which movement occurs • the resistance (R) is the weight of the part being moved.
46. There are three types of levers. The action of the biceps brachii in flexing the elbow represents
type III (R-P-F), the common lever type in the body. 47. If the PF/RF ratio of a lever is < 1 the lever works at a mechanical disadvantage, i.e. the power
used must be much greater than the load. Many levers in the body sacrifice mechanical advantage (i.e. power) for increased speed and range of movement by having a smaller PF/RF ratio. For the biceps brachii PF/RF may equal 1/6 or 0.17, a mechanical disadvantage. However, the speed of hand movement is increased by an equivalent factor of 6 giving increased mobility of the hand. If the biceps moves 1cm in 1 sec the hand moves 6cm.
Strength and Mobility of Muscles 48. The STRENGTH (POWER) of a muscle depends on three factors:
a. The NUMBER OF FASCICULI (bundles of fibers). The greater the number of fasciculi the stronger the muscle. This is achieved by having the muscle fibers pulling at an angle to the tendon. By increasing the tendon - muscle fiber angle more fasciculi can be packed into the same muscle diameter which increases power but reduces mobility.
Examples:
• Unipennate muscles (e.g.. flexor pollicus longus) have fibers pulling the tendon on one side only.
• Bipennate muscle (with more fasciculi) have fibers on two sides of the tendon (e.g.. rectus femoris).
The following muscles have fibers pulling on several sides of the tendon and so are the strongest muscles. • Multipennate muscles (e.g. deltoid), convergent muscles (e.g.. pectoralis major) and • Circumpennate muscles (e.g. tibialis anterior)
b. The INSERTION POINT of the muscle tendon on the bone. The further the insertion point is
from the fulcrum of the lever the greater is the mechanical advantage and so the greater the muscle’s power.

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 21 c. The DEGREE OF ACTIVITY OF THE MUSCLE. If a muscle is used forcefully (especially
isometrically) on a regular (daily) basis there will be an increase in muscle cell diameter, number of contractile units and strength of connective tissue components. The muscle will therefore show hypertrophy and increased strength.
49. The MOBILITY (degree of movement) and SPEED of a muscle depends on two factors:
a. The TENDON - FIBER ANGLE. The smaller the tendon - fiber angle the greater the mobility and speed. Maximum mobility and speed occurs when the tendon - fiber angle is zero (i.e. they are parallel) where the muscle fibers are pulling the tendon in the direction of the movement. This also means that fewer fasciculi are possible so the muscle power is relatively weak e.g.. rectus abdominis, sartorius, sternohyoid, superior rectus, gracilis muscles.
b. The INSERTION POINT of the muscle tendon on the bone. The closer the insertion point
is to the fulcrum of the lever the greater is the muscle’s mobility. This is because a small degree of movement near the fulcrum causes a large degree of moment of the other end of the bone. At the same time since mechanical advantage is reduced muscle power is weakened.

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 22 Energy for Muscle Contraction
50. Muscle contraction depends directly on energy from ATP hydrolysis. ATP is replenished in
exercising muscle cells from two sources, from hydrolysis of creatine phosphate and from cell respiration of glucose and other organic molecules.
51. Creatine phosphate (CP) is a second high energy molecule in muscle cells. During rest CP is
formed from ATP and during exercise as ATP is being depleted, CP is the most direct and so is the first source for regenerating ATP.
rest creatine +ATP CP + ADP exercise 52. During intense exercise blood supply cannot keep up with oxygen demands of muscles and
muscles respire anaerobically. Anaerobic respiration (anaerobic glycolysis) oxidises glucose incompletely to lactic acid and forms only 2 ATP per glucose.
53. Anaerobically muscles therefore fatigue easily due to a shortage of ATP and buildup of
lactic acid (which lowers the pH of muscle cells). 54. During moderate exercise ATP is replenished by aerobic respiration of glucose or fatty acids.
Glucose is first obtained from glycogen reserves and then from the blood sugar. Aerobic respiration of glucose forms 36 – 38 ATP per glucose molecule and completely oxidises glucose to CO2 and H2O. Muscle fatigue occurs more slowly since more ATP is available and lactic acid is not formed.
55. After anaerobic exercise an “oxygen debt” must be paid to reoxidise the lactic acid to CO2 and
H2O and to replenish ATP and CP reserves from aerobic respiration. 56. Muscle cells which specialize for aerobic respiration are called oxidative fibers; they have
many mitochondria and contain much myoglobin for O2 storage so are called red fibers. 57. Muscle cells which specialize for anaerobic respiration (anaerobic glycolysis) are called
glycolytic fibers; they have few mitochondria and little myoglobin so are called white fibers.

Human Anatomy & Physiology 1 (805) Unit 6 Muscular System Key Concepts Page 23