Anatomy of Nerves and Muscles of CS
6
SPINE Volume 28, Number 13, pp 1379–1384 ©2003, Lippincott Williams & Wilkins, Inc. Surgical Anatomy of the Nerves and Muscles in the Posterior Cervical Spine A Guide for Avoiding Inadvertent Nerve Injuries During the Posterior Approach Junwei Zhang, MD,* Nobuyuki Tsuzuki, MD,* Shigeru Hirabayashi, MD,* Kunio Saiki, MD,* and Kazumasa Fujita† Study Design. An anatomic study investigated the cer- vical dorsal rami and major cervical paravertebral muscles. Objective. To provide a detailed description of the cervical dorsal rami and important paravertebral muscles as a way of avoiding inadvertent injuries during the pos- terior approach. Summary of Background Data. No detailed anatomic studies of the nerves and the muscles in the posterior neck useful for the posterior approach have been re- ported previously. Methods. Running courses of the cervical dorsal rami of spinal nerves and the morphology of cervical major paravertebral muscles were studied using 14 cadavers. In four posterior approaches of cervical laminoplasty, sub- cutaneous facial exits of cutaneous nerves and the run- ning course of the right C3 medial branches around facet joint were exposed for observation of living anatomy. Results. Every medial branch from the dorsal rami of the C3–C8 spinal nerves passed through an anatomic tun- nel dorsolateral to the facet joint. The base of the tunnel was a bony gutter between neighboring facet joint cap- sules, and the roof was the tendon of the semispinalis capitis. In this tunnel, the medial branch had a little laxity in moving, and was assumed to be the most susceptible to iatrogenic injury during the operation. The semispina- lis cervicis was composed with long muscle bundles. Each of these had only one or two innervating nerves from the dorsal rami of cervical spinal nerves. Cutaneous branches from the dorsal rami were found adjacent to every spinous process below the C2 spinous process in cadaveric studies. However, only two or three larger cu- taneous nerves were discernible below the C5 or C6 spi- nous process in surgical approaches. Conclusions. With the posterior approach to the cervi- cal spine, a precise knowledge of the cervical dorsal rami anatomy and the innervating patterns of the paraverte- bral muscles is necessary for avoidance of inadvertent injuries to the nerves. [Key words: cervical dorsal rami, medial branch, paravertebral muscle, posterior approach] Spine 2003;28:1379 –1384 Cervical axial symptoms after the posterior approach, such as pain and stiffness of the neck and shoulder, were widely noticed recently, and their causes were assumed to be the destroyed facet joints (FJs), atrophy of the para- vertebral muscles, anterior tilt of the cervical spine re- sulting from a loss of static, and functional posterior stabilizing forces. 1,2 However, because of the complexity of the neck pain, 3–5 the precise mechanism remains un- clear. Approximately 40% of the 114 patients in this study who had undergone cervical laminoplasty in the past 2 years reported the aforementioned symptoms, and tenderness often was found on the dorsolateral aspect of FJs, where the medial branches (MBs) 6–11 are located. Injection of anesthetics at the tender points helped to relieve the pain for most of these patients. The authors assumed from their experience that MBs may be injured during the operation, causing the axial pain later. Their purpose for this study was to give pre- cise information on the surgical anatomy of the cervical dorsal rami and paravertebral muscles, to investigate the likely iatrogenic nerve injury, and identify the method for avoiding it during the posterior approach to the cer- vical spine. Materials and Methods Cadaveric Investigation. This study used 14 adult Japanese embalmed cadavers (10 females and 4 males) with no history of cervical spinal disease. The mean age was 65 years (range, 18 – 81 years). After harvesting of the head and neck en bloc, dissections were performed as follows. The soft tissue sur- rounding the C3–C8 cervical ventral rami (VR) was dissected until the origins of the dorsal rami (DR) were clearly exposed. Then the C3–C8 DRs were traced from their origins: from the dividing point of a spinal nerve into a VR and a DR (point O) to the dividing point of DR into a lateral branch (LB) and MB (point B). The MBs then were traced carefully to the distal portions where they gave branches to the innervated muscles and finally to cutaneous branches. The numbers of innervating nerves and locations, including the site of entry into the mus- cles, were carefully studied (Figure 1). In contrast to other re- searchers, 12,13 after removal of the dorsal cervical muscles su- perficial to the splenius capitis (SpCa) and splenius cevicis (SpCe), the current authors disconnected only one side of the attachment of the deeply lying muscles while tracing the nerves, namely, to remove the rostral part of the SpCa and the SpCe to detach the semispinalis capitis (SSCa) from the occipital bone and the semispinalis cervicis (SSCe) from the ligamentum nu- chae. Special attention was paid to the three-dimensional run- ning course of the MBs, particularly their positional relations to the paravertebral muscles and the FJ capsules. The running courses of C1 and C2 DR were excluded from the investigation because with the usual posterior approaches (i.e., laminectomy From the *Department of Orthopedic Surgery, Saitama Medical Cen- ter, Saitama Medical School, and the †Department of Anatomy, Saitama Medical School, Saitama, Japan. Acknowledgment date: June 5, 2002. First revision date: October 14, 2002. Second revision date:. Acceptance date: November 26, 2002. Address correspondence and reprint requests to Junwei Zhang, MD, De- partment of Orthopedic Surgery, Saitama Medical Center, Saitama Med- ical School, Saitama, 350-8550, Japan; E-mail: [email protected] 1379
description
Journal Article
Transcript of Anatomy of Nerves and Muscles of CS

SPINE Volume 28, Number 13, pp 1379–1384©2003, Lippincott Williams & Wilkins, Inc.
Surgical Anatomy of the Nerves and Muscles in thePosterior Cervical SpineA Guide for Avoiding Inadvertent Nerve Injuries During thePosterior Approach
Junwei Zhang, MD,* Nobuyuki Tsuzuki, MD,* Shigeru Hirabayashi, MD,*Kunio Saiki, MD,* and Kazumasa Fujita†
Study Design. An anatomic study investigated the cer-vical dorsal rami and major cervical paravertebralmuscles.
Objective. To provide a detailed description of thecervical dorsal rami and important paravertebral musclesas a way of avoiding inadvertent injuries during the pos-terior approach.
Summary of Background Data. No detailed anatomicstudies of the nerves and the muscles in the posteriorneck useful for the posterior approach have been re-ported previously.
Methods. Running courses of the cervical dorsal ramiof spinal nerves and the morphology of cervical majorparavertebral muscles were studied using 14 cadavers. Infour posterior approaches of cervical laminoplasty, sub-cutaneous facial exits of cutaneous nerves and the run-ning course of the right C3 medial branches around facetjoint were exposed for observation of living anatomy.
Results. Every medial branch from the dorsal rami ofthe C3–C8 spinal nerves passed through an anatomic tun-nel dorsolateral to the facet joint. The base of the tunnelwas a bony gutter between neighboring facet joint cap-sules, and the roof was the tendon of the semispinaliscapitis. In this tunnel, the medial branch had a little laxityin moving, and was assumed to be the most susceptibleto iatrogenic injury during the operation. The semispina-lis cervicis was composed with long muscle bundles.Each of these had only one or two innervating nervesfrom the dorsal rami of cervical spinal nerves. Cutaneousbranches from the dorsal rami were found adjacent toevery spinous process below the C2 spinous process incadaveric studies. However, only two or three larger cu-taneous nerves were discernible below the C5 or C6 spi-nous process in surgical approaches.
Conclusions. With the posterior approach to the cervi-cal spine, a precise knowledge of the cervical dorsal ramianatomy and the innervating patterns of the paraverte-bral muscles is necessary for avoidance of inadvertentinjuries to the nerves. [Key words: cervical dorsal rami,medial branch, paravertebral muscle, posterior approach]Spine 2003;28:1379–1384
Cervical axial symptoms after the posterior approach,such as pain and stiffness of the neck and shoulder, werewidely noticed recently, and their causes were assumed
to be the destroyed facet joints (FJs), atrophy of the para-vertebral muscles, anterior tilt of the cervical spine re-sulting from a loss of static, and functional posteriorstabilizing forces.1,2 However, because of the complexityof the neck pain,3–5 the precise mechanism remains un-clear. Approximately 40% of the 114 patients in thisstudy who had undergone cervical laminoplasty in thepast 2 years reported the aforementioned symptoms, andtenderness often was found on the dorsolateral aspect ofFJs, where the medial branches (MBs)6–11 are located.Injection of anesthetics at the tender points helped torelieve the pain for most of these patients.
The authors assumed from their experience that MBsmay be injured during the operation, causing the axialpain later. Their purpose for this study was to give pre-cise information on the surgical anatomy of the cervicaldorsal rami and paravertebral muscles, to investigate thelikely iatrogenic nerve injury, and identify the methodfor avoiding it during the posterior approach to the cer-vical spine.
Materials and Methods
Cadaveric Investigation. This study used 14 adult Japaneseembalmed cadavers (10 females and 4 males) with no history ofcervical spinal disease. The mean age was 65 years (range,18–81 years). After harvesting of the head and neck en bloc,dissections were performed as follows. The soft tissue sur-rounding the C3–C8 cervical ventral rami (VR) was dissecteduntil the origins of the dorsal rami (DR) were clearly exposed.Then the C3–C8 DRs were traced from their origins: from thedividing point of a spinal nerve into a VR and a DR (point O)to the dividing point of DR into a lateral branch (LB) and MB(point B). The MBs then were traced carefully to the distalportions where they gave branches to the innervated musclesand finally to cutaneous branches. The numbers of innervatingnerves and locations, including the site of entry into the mus-cles, were carefully studied (Figure 1). In contrast to other re-searchers,12,13 after removal of the dorsal cervical muscles su-perficial to the splenius capitis (SpCa) and splenius cevicis(SpCe), the current authors disconnected only one side of theattachment of the deeply lying muscles while tracing the nerves,namely, to remove the rostral part of the SpCa and the SpCe todetach the semispinalis capitis (SSCa) from the occipital boneand the semispinalis cervicis (SSCe) from the ligamentum nu-chae. Special attention was paid to the three-dimensional run-ning course of the MBs, particularly their positional relationsto the paravertebral muscles and the FJ capsules. The runningcourses of C1 and C2 DR were excluded from the investigationbecause with the usual posterior approaches (i.e., laminectomy
From the *Department of Orthopedic Surgery, Saitama Medical Cen-ter, Saitama Medical School, and the †Department of Anatomy,Saitama Medical School, Saitama, Japan.Acknowledgment date: June 5, 2002. First revision date: October 14,2002. Second revision date:. Acceptance date: November 26, 2002.Address correspondence and reprint requests to Junwei Zhang, MD, De-partment of Orthopedic Surgery, Saitama Medical Center, Saitama Med-ical School, Saitama, 350-8550, Japan; E-mail: [email protected]
1379

or laminoplasty), they are rarely encountered, and the detailedanatomic descriptions already mentioned by Bogduk12 seemedto provide a sufficient knowledge for avoiding iatrogenic inju-ries to these courses when their territories are entered.
Clinical Investigation. With four posterior approaches forcervical laminoplasty, the positions of subcutaneous facial exitsof the cutaneous nerves and the right C3 MBs were exposed forinvestigation of the difference between living and cadavericconditions.
Results
Cadaveric Investigation
Running Courses of the C3, C4, and C5 Dorsal Rami. (Figures2– 4). The third to fifth cervical DRs had a common run-ning course as follows. Each DR branched from its be-longing spinal nerve just outside the intervertebral fora-men. At the anterior aspect of the FJ, the DR curveddorsolaterally along the superior articular pillar throughthe space between the adjacent upper and the lowertransverse processes. In this course, just before the baseof the transverse process, the DR branched into the MBor MBs and the LB. The LB crossed the transverse pro-cess and reached dorsocaudally to the anterior surface ofthe longissimus capitis (LgCa) or the SpCa, whereas theMBs curved dorsally and crossed the transverse processbetween its root and the FJ capsule. At the lateral aspectof the FJ, MBs, located at the lower margin of the FJcapsule, continued to run dorsomedially in a gutterformed between neighboring FJ capsules, passed throughunder the tendon of the SSCa (Figure 2), and reached thelateral edge of the multifidus (M) (point P) (Figure 4).
The bony gutter and the covering tendon constituted atunnel situated just dorsolaterally to the FJ, in which theMB had a little laxity in moving (Figure 2, inlet). At C3,C4, and C5, there usually were two MBs, a superficialone and a deep one, which arose separately or as a singlecommon stem from the DR (Figure 2). Distally to pointP, the MBs took their individual running courses: At C3,they ran dorsomedially between the multifidus and theSSCa, and the running course of the superficial one isknown as the third occipital nerve. The deep one, whichis the same as those of C4–C5, entered the multifidus andramified in the muscle. However, at C4–C5, the superfi-cial branches remained superficial to the multifidus, pass-ing through the vascular connective tissue dorsal to themultifidus. Then they either ran dorsally between the SSCaand the semispinalis cervicis (SSCe) or entered the SSCeand finished in cutaneous branches. In 8 of 14 cases, at
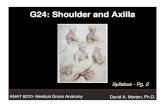
Figure 1. Axial view of cervical spine showing the running courseof the dorsal rami and the running course designation. For detail,see the text. SSCa, semispinalis capitis; SSCe, semispinalis cervi-cis; M, multifidus; LgCa, longissimus capitis; LgCe, longissimus cer-vicis; DRG, dorsal root ganglion; VR, ventral ramus; DR, dorsal ramus;LB, lateral branch; FJ-B, facet joint branch; O, origin of the DR;B, branching point of DR into LB and medial branch; P, point at whichthe medial branch reaches the lateral edge of the multifidus.
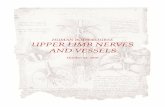
Figure 2. Lateral view of the cervical spine showing medialbranches (MBs), lateral branches (LBs) of the cervical dorsal ramiand their relation to semispinalis capitis (SSCa). The diameter of thepin used to fix C4 ventral ramus (VR) is 1 mm. The superficial musclesand rostral part of the splenius capitis (SpCa) and splenius cervicis(SpCe) were removed. *MBs; #LBs; FJC, facet joint capsule.
Figure 3. Lateral view of the cervical spine showing medialbranches (MBs) and their relation to the semispinalis capitis(SSCa) and facet joint capsules (FJCs). Inlet scheme shows therelation of MBs to the SSCa and FJCs. For detail, see the text. Thescale is marked by every 1 mm. ABV, accompanying blood vessel;VR, ventral ramus; LB, lateral branch.
1380 Spine • Volume 28 • Number 13 • 2003

C5 a branch secondary to SSCe via its dorsal surfacewere found arising from the superficial branch.
Running Courses of the C6, C7, and C8 Dorsal Rami. The sixthto eighth DRs showed running courses different fromthose of the C3–C5 DRs in that the DRs branched fromthe spinal nerves more distally outside the foramen andthen divided into an LB and an MB, both of which randorsorostrally under the anterior surface of the trans-verse process (Figure 2). After crossing the transverseprocess, the LB ran dorsally to reach the longissimuscervicis (LgCe) or the SpCe, whereas the MB, as only onebranch, continued to curve along the root of transverseprocess. Then the MB changed its direction dorsally andcaudomedially to the lower margin of the upper FJ cap-sule. Partially covered by the tendon of the SSCa, the,MB reached the lateral edge of the multifidus (point P),namely, the dorsolateral part of the FJ capsule (Figures 3and 4). Distally to point P, the MB ran medially betweenthe multifidus and the SSCe, finally ramifying in the in-nervating muscles, and its terminal branch innervatedthe interspinales.
Articular Branches to the Facet Joint Capsules. In six ca-davers, articular branches were examined from C3 MBto C8 MB bilaterally, with the aid of a dissecting micro-scope (magnification, �10). Only a rostral branch wasfound at 26 of the 72 MBs, directed to the dorsolateralaspect of the upper FJ capsule (Figure 5).
Blood Vessels Around the Medial Branches. At each level ofC3 to C8, one or two small blood vessels always accom-panied the MBs throughout their running coursesaround the FJs.
Positions of Medial Branches Relative to Paravertebral Mus-cles. After the paravertebral muscles had been detachedfrom C1 to T1 laminae, they were retracted laterally andthe portions of MB around point P of all the MBs wereexposed (Figure 6).
Measurements. At C3–C8, the mean lengths of the DRtrunks (i.e., the lengths from point O to point B) were,respectively, 5, 3, 3, 5, 7, and 10 mm, and the meanlengths of the MB portion from point B to point P were,respectively, 14, 17, 17, 16, 14, and 12 mm.
Arrangement and Innervation of the Semispinalis Capitis, theSemispinalis Cervicis, and the Multifidus by the MedialBranches. The SSCa is a broad muscle covering the dor-solateral aspect of the cervical spine superficial to theSSCe. The SSCa originates from the articular processesof the C4, C5, and C6 vertebrae, and from the tips of the
Figure 4. Running course of medial branches (MBs) and theirrelation to the semispinalis cervicis (SSCe), multifidus (M), andfacet joint capsules (FJCs) after removal of the semispinalis ca-pitis. The scale is marked by every 1 mm. VR, ventral ramus; LB,lateral branch.
Figure 5. A closed view of the articular branch from the C6 medialbranch (MB) to the C5–C6 facet joint capsule. The scale is markedby every 1 mm. VR, ventral ramus; FJ-B, facet joint branch.
Figure 6. Appearance of the trunks of the C3–C8 medial branches(MBs) by lateral traction of paravertebral muscles (PVM) aftercomplete release of them from spinous processes and laminae.The scale is marked by every 1 mm. FJ, facet joint; SP, spinousprocess.
1381Anatomy of the Posterior Neck • Zhang et al

transverse processes of C7 and the first six or seven tho-racic vertebrae and inserts into the occiput, as mentionedin the literature.14 The innervating pattern was found tobe as follows. One LB from the C2 DR and one LB fromthe C3 DR, directed dorsomedially, lay on the dorsalsurface of the SSCa. In eight cases, they formed a loop.The two LBs sent secondary branches to the SSCa. Fur-thermore, two or three secondary branches from thegreat occipital nerve (MB of C2 and two or three second-ary branches from the third occipital nerve [the superfi-cial MB of C3]) contributed to the innervation of theSSCa. These nerves reached the lateral edge of the SSCarunning parallel to the laminae of their exits. They thenran caudomedially on the ventral surface of the SSCa,communicating with each other, and finally forming along, descending innervating nerve. A branch from C4(MB to the SSCa), described by Bogduk, was not verifiedin the current study.
The SSCe is a composite muscle consisting of five longmuscle bundles that originate at the thoracic transverseprocesses of the first six thoracic vertebrae and insert intothe cervical spinous processes from C2 to C5.14 At eachlevel of the C4–C8 intervertebral foramen, a secondarybranch from the deep MB enters the SSCe bundle via itsventral surface at the middle level of lamina (Figure 7).However, at C5 in 8 of 14 cadavers, a branch from thesuperficial MB was found to enter the SSCe via its dorsalsurface. The multifidus was the deepest postvertebralmuscle lying on the dorsal surfaces of laminae. At cervi-cal and cervicothoracic levels, the multifidus originatedfrom lower articular process below C4 (including C4),ran mediorostrally, and inserted into the spinous pro-cesses from C2 below.14 Muscle bundles from one originseparated to insert multiple spinous processes, from justabove vertebra to two or three further proximal verte-bra. Therefore, every spinous process below C3 had mul-tifidus with multiple origins. Each of the C3–C8 MBssent innervating nerves to multifidus via its dorsal sur-face at each midlamina level. The multifidus inserting thesame spinous process received innervation from the sameMB, with a segmental number one more than that of thespinous process, even if the origins of multifidus weredifferent.
Cutaneous Nerves. Cutaneous branches from the DRwere found adjacent to every spinous process bilaterallybelow C2 in cadaveric studies. Except for a greater oc-cipital nerve at C2 and a third occipital nerve, the cuta-neous nerves at each spinous process below C3 weresmall, with diameters less than 2 mm in the current cases.
Clinical InvestigationIn four cervical operations using posterior approaches,large cutaneous nerves were discernible below the C5 orC6 spinous process level (Figure 8a). The right C3 MBwas exposed at the lateral margin of the C2–C3 FJ (Fig-ure 8b), and found to be located slightly more distallythan in the cadaveric specimens, probably because of thedistal traction of the paravertebral muscles after proxi-
mal detachment. The lateral retraction of the paraverte-bral muscles stretched the C3 MB.
Discussion
In the comparison of the current anatomic findings withthose of Bogduk, it is natural that the running courses ofC3–C8 DRs and MBs were common. However, the C4MB innervating the SSCa and the caudal articular branchto the FJ, first described in Bogduk’s4,12,15–17 reports,could not be found. The basic difference in the investiga-tions was that the current study tried to find clinicalsignificances of the anatomic arrangements of structuresalong the running courses of MBs from the surgical pointof view, whereas Bogduk’s purpose was to investigatethe anatomic basis to explain the neck pain. The majorcontributions of the current study were that its figures
Figure 7. Innervation of the semispinalis cervicis (SSCe) by medialbranches (MBs) from a posterior view. T1–T4, T2–T4, T3–T5, T3–T6, T6 –T8, T7–T9 indicate the muscle bundles arising from thetransverse process of the Th1– 4, Th2– 4, Th3–5, Th3– 6, Th6 – 8 andTh7–9, respectively. SP, spinous process; C4F, lower articularfacet of C4.
1382 Spine • Volume 28 • Number 13 • 2003

provided the dimensional running course of the cervicaldorsal rami, made clear the innervation patterns of theimportant neck stabilizer (SSCe), and highlighted therisky procedures that could injure MBs in the posteriorapproach to the cervical spine.
Despite their long running distances, the motorbranches of SSCa and SSCe innervations had rostral en-try points and originated from only two levels of thecervical dorsal rami. The innervation pattern of theSSCa, by the branches from the C2 and C3 MB, resem-bled that of the trapezius in that long descending nervesinnervated the whole muscle.18 It has been stressed thatduring laminoplastic procedures, preservation of the C2SSCe is important for the postoperative stability of theneck. However, attention has not been focused on howto preserve the muscle innervation. Only two nerves, theC4 MB and the C5 MB, innervated the long C2 SSCewhose muscle belly extended from the T1–T4 transverseprocesses to the C2 spinous process (Figure 6). Any in-juries of the two nerves makes the preservation of themuscle belly meaningless. In this study, the multifiduswas confirmed as a myotomal muscle in terms of ana-tomic characteristics, as muscle bundles of one cervicalmultifidus from one origin inserted generally into two or
three different spinous processes of the immediate upperlevel. The rule of innervation was that the multifidi in-serting the same spinous process got the same nerve sup-ply from the MB immediately below the inserted spinousprocess, although the origins of multifidi were different,and the same pattern was noted also in the lumbar mul-tifidus.16,19–23 The clinical significance of this particularinnervation rule in the electromyographic study is thatalthough the multifidus was myotomal, electromyo-graphic potentials of multifidi on the surface of one lam-ina could contain potentials of two or three different rootorigins.
In the surgical procedures of stripping and retractingparavertebral muscles from spines and laminae with theposterior approach, four procedures carry a possible riskfor iatrogenic injuries of MBs including a 1) middorsalskin incision that could injure a major cutaneous nerve,2) an intermuscular development that could injure inter-muscular branches of MBs, 3) an approach to the lateralarea of the FJ that could injure the trunk portions ofMBs, and 4) lateral retraction of PVMs after their com-plete release from the spine and laminae that could causeoverstretching of MBs. The following discussion de-scribes each of these risks in greater detail.
1. Cutaneous nerves may be cut inadvertently nearthe spine in a bleeding operative field, even if they haddiscernible diameters of approximately 2 mm (Figure7a) during a middorsal skin incision. The nerves thatshould be spared are the greater occipital nerve, thethird occipital nerve, and the large cutaneousbranches, which usually are present below the C5 orC6 spinous process level.2. Medial branches run among paravertebral muscles(Figure 1). Innervating nerves of the SSCa, SSCe, andmultifidus run among these muscles and send second-ary branches to them. Therefore, an intermuscularrelease of PVMs should not be performed to avoid aniatrogenic injury of nerves.3. In an approach to the lateral area of the FJ, trunksof MBs appear directly in an operative field after acomplete release of PVM from spines and laminae, asshown in Figures 6 and 8b. Therefore, inadvertent useof a knife or electrical cautery may injure MBs. Asmentioned earlier, MBs in this area accompany bloodvessels, and electrical cautery by a power of 50 W for2 seconds was required for satisfactory bleeding con-trol, which could destroy the nerve sheath of MBs atthe same time. Monopolar cautery produced a wideelectrical current with high risks of involving a neigh-boring nerve by the excessive temperature. Therefore,the use of bipolar cautery with short duration wasrecommended22–24.4. Every MB had little laxity in moving in an ana-tomic tunnel just dorsolateral to the FJ (Figure 2, in-let). Therefore, a high degree of lateral retraction ofPVMs after a complete their release from the spineand laminae could overstretch MBs between the ana-
Figure 8. a, Operative photo showing the cutaneous branches ofmedial branches at C5 and C6 after middorsal skin incision. SSCa,semispinalis capitis; SP, spinous process. b, Operative photoshowing the right C3 medial branches (MB) located laterally to theC2–C3 facet joint (FJ).
1383Anatomy of the Posterior Neck • Zhang et al

tomic tunnel and entry points into PVM (Figure 5).This traction force on MBs could be reduced if themuscles connecting the PVM to laminae (i.e., multifi-dus muscles) were not completely released. Injuries ofmuscle fibers or intramuscular nerves by excessivetraction of PVMs has been reported in cases of a pos-terior approach to the lumbar spine.25–32 Nagayamaet al33 showed that an overstretch of lumbar spinalroot causes the atrophy of PVM experimentally. Al-though the atrophy of PVM by a direct overstretch ofinnervating nerves had not been reported clinically,this possibility should be investigated in the case ofsurgery manipulating the PVM.
Characteristics of the MB’s running course around FJimplied that excess movements of the FJ in addition tothe degenerative articular bony protrusions could exertdamaging forces to the MB in the anatomic tunnel dor-solateral to FJ, causing chronic neck pain, as in a whip-lash injury.34–36 However, evidence of the nerve distur-bance, namely, impairment of nerve conduction velocity,is impossible to obtain. Therefore, it remains conjecture.
Key Points
● The running course of the cervical dorsal rami(C3–C8), especially the relation of the medialbranches to the facet joints and deep paravertebralmuscles, is presented.● The most important posterior stabilizer, thesemispinalis cervicis, showed a typical anatomicfinding, namely, a long-running course with a fewrostral innervating nerves from the cervical dorsalrami.● The portion of the medial branches along thedorsolateral part of the facet joints was susceptibleto operative procedures, so care must be taken toavoid iatrogenic injury to these nerves.
References
1. Hosono N, Yonenobu K, Ono K. Neck and shoulder pain after laminoplasty.Spine 1996;21:1969–73.
2. Tsuzuki N, Abe R, Saiki K, et al. Extradural tethering effect as one mecha-nism of radiculopathy complicating posterior decompression of the cervicalspinal cord. Spine 1996;21:203–11.
3. Bogduk N, Marsland A. The cervical zygapophysial joints as a source of neckpain. Spine 1988;13:610–7.
4. Bransley L, Bogduk N. Medial branch blocks are specific for the diagnosis ofcervical zygapophysial joint pain. Reg Anesth 1993;18:343–50.
5. Fukui S, Ohseto K, Shiotani M, et al. Referred pain distribution of thecervical zygapophysial joints and cervical dorsal rami. Pain 1996;68:79–83.
6. Hayashi K. Clinical anatomy of the cervical spine with relation to the cervicalspondylosis (in Japanese). In: Itami Y, Nishio A, eds. Orthop Mook 6. To-kyo: Kanehara Shuppan, 1979:1–12.
7. Johnston HM. The cutaneous branches of the posterior primary divisions ofthe spinal nerves, and their distribution in the skin. Ana Physiol 1908;43:89–92.
8. Kasai T, Chiba S, Suzuki T, et al. Cutaneous branches from the dorsal rami
of the cervical nerves, with emphasis on their positional relations to thesemispinalis cervicis. Okajimas Folia Anat Jpn 1989;66:153–60.
9. Pearson AA, Sauter RW, Bass JJ. Cutaneous branches of the dorsal (primary)rami of the cervical nerves. Am J Anat 1963;112:169–80.
10. Pearson AA, Sauter RW, Buckley TF. Further observations on the cutaneousbranches of the dorsal rami of the spinal nerves. Am J Anat 1966;118:891–903.
11. Standring SM, Berry MM, Bannister LH. The spinal nerves. In: Williams PL,ed. Gray’s Anatomy. New York: Churchill Livingstone, 1995:1261–3.
12. Bogduk N. The clinical anatomy of the cervical dorsal rami. Spine 1982;7:319–30.
13. Eraheim NA, Haman ST, Rongming Xu, et al. The anatomic location of thedorsal ramus of the cervical nerve and its relation to the superior articularprocess of the lateral mass. Spine 1998;23:1968–71.
14. Salmons S. Muscles and fasciae of the trunk. In: Williams PL, ed. Gray’sAnatomy. New York: Churchill Livingstone, 1995:809–12.
15. Bogduk N. Cervical zygapophysial joint pain and percutaneous neurotomy:an update to the Quebec task force report on whiplash-associated disorders.In: Gunzburg R, Szpalski M, eds. Whiplash Injury: Current Concepts inPrevention, Diagnosis, and Treatment of the Cervical Whiplash Syndrome.Philadelphia: Lippincott-Raven, 1998:211–9.
16. Kalimo H, Rantanen J, Viljanen T, et al. Lumbar muscles: structure andfunction. Ann Med 1989;21:353–9.
17. Suseki K, Takahashi Y, Takahashi K. Innervation of the lumbar facet joints,origins, and functions. Spine 1997;22:477–85.
18. Ando M. Anatomy of the accessory nerve and the innervation of the trape-zius (in Japanese). J Jpn Soc Surg Hand 1992;9:288–91.
19. Bogduk N. The innervation of the lumbar spine. Spine 1983;8:286–93.20. Bogduk N, Wilson AS, Tynan W. The human lumbar dorsal rami. J Anat
1982;134:383–97.21. Kaplan M, Dreyfuss P, Halbrook B, et al. The ability of lumbar medial
branch blocks to anesthetize the zygapophysial joint: a physiologic chal-lenge. Spine 1998;23:1847–52.
22. Hnatuk LA, Li KT, Carvalho AJ, et al. The effect of bipolar electrocautery onperipheral nerves. Plast Reconstr Surg 1998;101:1867–74.
23. Veck S. An introduction to the principles and safety of electrosurgery. Br JHosp Med 1996;55:27–30.
24. Zohar Y, Sadov R, Strauss M, et al. Ultrastructural study of peripheral nerveinjury induced by monopolar and bipolar diathermy. Ann Otol Rhinol La-ryngol 1996;105:673–7.
25. Blom S, Lemperg R. Electromyographic analysis of the lumbar musculaturein patients operated on for lumbar rhizopathy. J Neurosurg 1967;26:25–30.
26. Jonson EW, Burkhart JA, Earl WC. Electromyography in postlaminectomypatients. Arch Phys Med Rehabil l972;53:407–9.
27. Kawaguchi Y, Matsui H, Tsuji H. Back muscle injury after posterior lumbarspine surgery: Part 1. Histologic and histochemical analyses in rats. Spine1994;19:2590–7.
28. Kawaguchi Y, Matsui H, Tsuji H. Back muscle injury after posterior lumbarspine surgery: Part 2. Histologic and histochemical analyses in humans.Spine 1994;19:2598–602.
29. Macnab I, Cuthbert H, Godfrey CM. The incidence of denervation of thesacrospinalis muscles following spinal surgery. Spine 1997;2:294–8.
30. Mck EW. Electromyographic observations in the postoperative patient.J Neurosurg 1951;8:466–72.
31. Soeda S, Satou N, Minamioka S, et al. Regeneration of back muscles injuredby posterior approach to the lumbar spine: damage to the dorsal rami oflumbar spinal nerves as a potent cause of deficient regeneration (in Japanese).J Jpn Spine Res Soc 1997;10:643–50.
32. Weddel G, Feinstein B, Pattle RE. The electrical activity of voluntary musclein man under normal and pathological conditions. Brain 1944;67:178–257.
33. Nagayama R, Nakamura H, Yamano Y, et al. An experimental study ofthe effects of nerve root retraction on the posterior ramus. Spine 2000;25:418–24.
34. Cusick JF, Pintar FA, Yoganandan N. Whiplash syndrome: kinetic factorsinfluencing pain patterns. Spine 2001;26:1252–8.
35. Kaneoka K, Ono K, Inami S, et al. Motion analysis of the cervical vertebraeduring whiplash loading. Spine 1999;24:763–70.
36. Tsuzuki N, Zhang JW, Hirabayashi S, et al. Distribution of posteromedialbranches of the cervical spinal nerves in the vicinity of facet joint, includingarticular branches to the facet joint: can these nerves be damaged by whip-lash loading to cause neck pain? (in Japanese). J East Jpn Orthop Traumatol2001;13:48–54.
1384 Spine • Volume 28 • Number 13 • 2003