
Anatomy of cornea & corneal tranparency dr.ysr
51
ANATOMY OF CORNEA AND CORNEAL TRANSPARENCY By: Dr. Yajuvendra Singh Rathore
-
Upload
dryajuvendra-rathore -
Category
Documents
-
view
76 -
download
0
Transcript of Anatomy of cornea & corneal tranparency dr.ysr
ANATOMY OF CORNEA AND CORNEAL TRANSPARENCY
By: Dr. Yajuvendra Singh Rathore

INTRODUCTION• Cornea is a
transparent, avascular, watchglass like structure
• It forms anterior 1/6th of the outer fibrous coat of eyeball.

DIMENSIONS
• Anterior surface of the cornea is elliptical
• Horizontal diameter – 11.75mm
• Vertical diameter-11mm• Posterior surface is
spherical with average diameter 11.5 mm.

• The radius of curvature of cornea – Anterior radius 7.8mm– Posterior radius
6.5mm• Thickness of cornea– Center 0.52mm– Periphery 0.67mm
• Central corneal thickness has direct influence in IOP measurement.

• The central 5 mm of the cornea forms the most powerful refracting surface of the eye.
• The net refractive power of the cornea is +43D which is 3/4th of the total refractive power of eye.
• The refractive index of cornea is 1.37

Layers Thickness (in µm)
Composition
Epithelium 50 Stratified Squamous Epithelium
Bowman's Membrane 8-14 Compact layer of collagen fibres
Stroma 500(0.5mm)
Orderly arrangement of collagen lamellae with keratocytes
Descemet's Membrane 10-12 Consists of collagen & glycoprotein
Endothelium 5 single layer of simple squamous epithelium
Cornea is composed of Five Layers.

Layers of Epithelium
Description Mitoticactivity
Basal Cell Single layer of columnar cells found adjacent to basal layer
+
Wing Cell 2-3 layers of polyhedral cells -
Surface Cell 3 layers of flattened epithelial cells with microvilli in contact with the tear film.
-
It takes normally 7 days for replacement entire corneal epithelium
LAYERS OF EPITHELIUM


• The surface corneal epithelial cells has numerous microvilli and microplicae and these cells secrete glycocalyx which helps in adhesion and stability of the tear film.
• The Basal cells are firmly joined laterally to other basal cell & anteriorly to the wing cell by desmosomes & maculae occludent and with the basal lamina with the help of hemidesmosomes and other filaments.
• Corneal epithelium sheds at regular interval & replaced by growth from its basal cell

BOWMAN’S LAYER/ANTERIOR LIMITING MEMBRANE
• It is an acellular tough membrane like zone situated in between corneal epithelium and stroma.
• It is 8-14 µm thick • composed of condensed collagen fibers. • These collagen fibers are continuous with that of
anterior stroma.• Because of the compact arrangement of collagen
fibers, it is comparatively resistant to trauma. However, once destroyed it cannot be regenerated.

STROMA/SUBSTANSIA PROPRIA• The stroma or substantia propria, which occupies about
90% of the total corneal thickness• Composed of collagen fibrils, keratocytes and
extracellular ground substances• Lamellae are arranged in many layers (200-250)• Each layer is parallel to each other & with corneal surface
and become continuous with scleral plane• Lamellae run from limbus to limbus• Parallel arrangement of lamellae in the cornea allow an
easy intralamellar dissection during superficial keratectomy & lamellar keratoplasty
• The peculiar arrangement of lamellae has also been implicated in the corneal transparency

• Cells are embedded in hydrated matrix of proteoglcans
• Amongst the cellular components, keratocytes, wandering macrophages, histiocytes & few lymphocytes (corneal fibroblasts) are the major cell type of the stroma.
• They occupy 2-4% of the stromal volume.
• They synthesize collagen and proteoglycan and thus maintain the stroma.


DESCEMET’S MEMBRANE/POSTERIOR LIMITING MEMBRANE
• It is strong homogenous layer which binds the stroma posterioly
• Represents the basement membrane of the endothelium from which it is produced
• Elasticity is one of its physical characteristic• It is made up of glycoprotein & collagen fibrils with no
elastic fibers • Thickness varies with age, at birth is 3 µm , young
adults is 10-12 µm• It is resistant to chemical agents, trauma and infection
• Even if whole stroma is sloughed off, Descemet’s membrane can maintain the intergrity of the eyeball for long

• In case of Descemet’s Membrane detachment or tear, the membrane curls towards the stroma (inwards) because of the elastic property of Descemet’s membrane.
• In periphery, it appears to end at the anterior limit of the trabecular meshwork as schwalbe’s line(ring)
• It can regenerate

ENDOTHELIUM• Corneal endothelium is a simple squamous
epithelium. • Endothelial cells are hexagonal which forms
continuous mosaic pattern, best seen in specular microscopy.
• Cell density – Birth-6000cells/mm2
– Young adults-22500-3000cells/mm2
• The endothelial cells are interconnected with each other with various junctional complexes like zonula occludans, macula occludans and macula adherens.
• These cells possess ion transport system which is known as endothelial pump. These endothelial pumps regulate the water content of corneal stroma.

• Endothelial cells cannot divide or replicate. With ageing, the cell density of the endothelium decreases which is compensated by an increase in cell size (Polymegathism) or shape (Pleomorphism).
• As these endothelial cells are involved in corneal hydration they help in maintenance of corneal transparency

New Layer Discovered-DUA’S LAYER
• In a paper published in 2013, the existence of Dua's layer was suggested by Harminder Singh Dua et al.

Implications of findings of Dua’s layer
• The layer may help surgeons improve outcomes for patients undergoing corneal grafts and transplants. During surgery, tiny air bubbles are injected into the corneal stroma in what is known as the "big bubble technique". Sometimes the bubble bursts, damaging the patient's eye. If the air bubble is injected under Dua's layer instead of above it, the layer's strength could reduce the risk of tearing

BLOOD SUPPLY• In normal condition, cornea does not
contain any blood vessel. • Anterior ciliary artery, a branch of
ophthalmic artery forms a vascular arcade in the limbal region invades its periphery for about 1mm
• helps in corneal metabolism and wound repair by providing nourishment.
• Absence of blood vessel in cornea is one of the contributing factors for its transparency.
NERVE SUPPLY
• Cornea is primarily innervated through the ophthalmic branch of the trigeminal nerve.
• The nasociliary nerve provides sensory innervation to the cornea.
• The Long ciliary nerves after arising from nasociliary nerve enter the eyeball around the optic nerve along with short ciliary nerve & run forward in suprachoroidal space.
• A short distance from the limbus , these nerve pierce into sclera to leave the eyeball

• Divide dichotomously & connect with each other & conjunctival nerves to form a pericorneal plexus of nerve.
• About 60-80 myelinated trunks from the pericorneal plexus enter into the cornea at various levels– Sclera– Episclera– Conjunctiva
• After having gone for 1-2mm in the stroma the corneal nerves loose their myelin sheath, branch dichotomously & form stromal plexus
• Some nerves end in mid stroma. Most pass anteriorly & form subepithelial plexus
• The fibers from here penetrate the pores in bowman’s membrane ,lose their schwann’s sheath, divide into filaments under basal layer of epithelium which extend between the cells of all layers of epithelium, & form intra epithelial plexus
• Thus nerve end in epithelium as fine beaded filaments.

PHYSIOLOGY OF CORNEA PHYSIOLOGICAL
• To act as powerful refracting lens.
• To protect the intraocular contents.
• Cornea plays imp. role in absorption of topically applied drugs.
• Wound healing after anterior segment Sx or trauma.
BIOCHEMICAL • Biochemical composition• Metabolism of cornea• Corneal transparency• Drug permeability• Corneal wound healing

BIOCHEMICAL COMPOSITION
EPITHILUM• Water: 70%• Proteins: 5 times > stroma & 2 times >
endothelium and Descemets membrane.• Lipids: phospholipids & cholesterol are
components wich constitue 5.4% of the dry wt of epithelium.• Enzymes: Necessary for krebs, glycolysis are
present in high no.s• Achetylcholine & cholinestrase play a role in
cation transport• Electrolytes: HIGH K+ and LOW Na+ and Cl-

STROMA• Water :75-80%• Collagen : Predominant type I. Type V, XII, XIV
collagen also found • In boiling water or acids collagen is converted to
gelatin(acids burns are less serious than alkali burns).• Soluble proteins: albumin,
immunoglobulins(G,A&M), glycoproteins • Proteoglcans: -keratin sulphate,chondrotin.
Glycosamino glycans is present in interfibrillar space and accounts for stromal swelling pressure(N=60mmhg) plays imp role in transparency and hydration.
• Enzymes: glycolsis & krebs cycle enzymes in stromal keratocytes
• Matrix metalloprotinase help in remodelling after injury
• Electrolytes: Na+ is high & K+ is low

BIOCHEMICAL COMPOSITION
DESCEMET’S MEMBRANE:oCollagen : 75%oGlycoproteinsoThe collagen of this layer is
insoluble and extremely resistant to chemical and enzymatic action.

METABOLISM OF CORNEA
• Cornea requires energy for maintenance of transparency & dehydration.
• Most actively metabolising layers are epithelium & endothelium.
• Nutrients: Oxygen, glucose and aminoacids
METABOLIC PATHWAY– Glycolysis– Hexose monophosphate shunt

CORNEAL TRANSPARENCY
ANATOMICAL FACTORS• Optically smooth tear film.• Role of corneal epithelium• Arrangement of stromal fibers• Corneal avascularity.• Absence of myelin sheath around corneal nerves.
PHYSIOLOGICAL FACTOR• Corneal dehydration

TEAR FILM
• Forms a homogeneous layer over ant surface of cornea.
• Acts as a lubricant.• Fills up the small surface irregularity on the cornea• Condition associated with abnormalities of tear is
associated with loss of corneal transparency.
CORNEAL EPITHELIUM• Homogeneous refractive
medium.• Basal cell are firmly joined
laterally to other basal cells & anteriorly to the wing cells by desmosomes & maculae occludents.
• Tight intercellular junction accounts for epithelial transparency as well as its resistance to flow of water, electrolytes & glucose i.e barrier function.
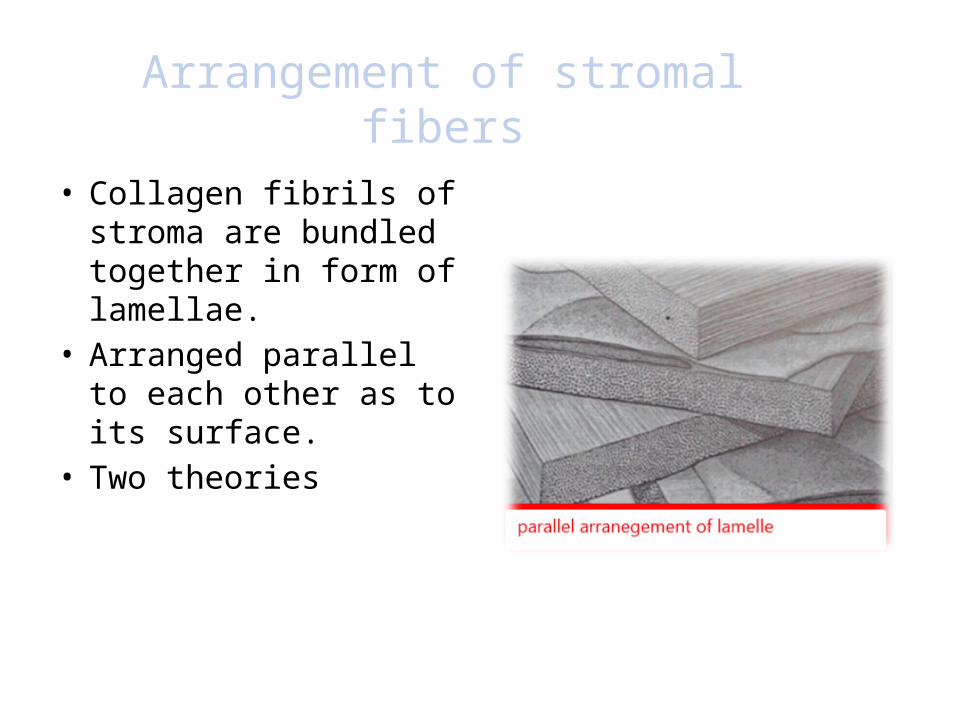
Arrangement of stromal fibers• Collagen fibrils of
stroma are bundled together in form of lamellae.
• Arranged parallel to each other as to its surface.
• Two theories – Maurice theory– Goldman et al theory

MAURICE THEORY• Uniform collagen
fibrils are arranged in a regular lattice
• Scattered light is destroyed by destructive interferance
• Interfibrillar distance is < wavelength of light (4000A-7000A)

MAURICE THEORY
GOLDMAN ET AL THEORY• Diffraction theory.• Lattice arrangement is not
required• Fibrils will not interfere
transmission of light unless they are larger than 1/3rd of the wave length of incident light.
• Refractive elements with the dimensions < 2000A do not scatter light.

CORNEAL AVASCULARITY• Cornea is asvascular except for small loops
which invade the periphery for about 1mm • Some conditions of cornea is associated with
vascularization • The purpose of this is to bring defense
mechanisms into play against the noxious agent
• It facilitates nutrition, transport of antibiotics & drugs
• Progressive vascularization is harmful as it interferes with corneal transparency

THEORY• Chemical theory:– Role of Vaso-inhibiting factor: (Meyer &
Chafre )• Presence of sulfate ester of hyaluronic acid in the stroma
glycosaminoglycan acts as VIF
– Role of Vaso-stimulatory factor: (Campbell & Michaelson)• Experimental corneal burns, release of VSF at the of
lesion which diffuses through the stroma to limbus & stimulates new vessel growth from limbal plexus.
• VSF is thought be low molecular weight amine• Corneal hypoxia also induces neovascularization by
activation of VSF

Contd.• Mechanical theory: (Cogan)– Blood vessels cannot invade normal cornea
because of its compact structural nature & that of loosening of compactness of corneal tissue due to edema was mandatory for neovascularization
Combined theory: ( Maurice et al)
• Role of both VIF & compactness of cornea
Role of leucocytes
• Leucocytes perform an essential role in stimulating vascularization

Absence of myelin sheath around corneal nerves.
• Corneal nerves loose their myelin sheath at 1-2mm away from the limbus.

PHYSIOLOGICAL FACTORS• Cornea maintains itself in a state of
relative dehydration• Water content of normal cornea is around
80%, which is highest water content of any connective tissue in the body.

PHYSIOLOGICAL FACTORS• Factors which draw water in cornea
Imbibition Pressure
• Factors which prevent the flow of water in the cornea
Barrier Mechanism Of Epithelium
• Factors which pump out water from the cornea
Endothelial Metabolic Pump
IMBIBITION PRESSURE • Factors which draw water in cornea• Stromal swelling pressure• Pressure is 60mm of Hg which is exerted by
glycoaminoglycans(GAGs)of corneal stroma which acts like sponge
• The electrostatic repulsion of anionic charges on the GAGs molecule expands the tissue ,sucking in the fluid with equal but negative pressure called IMBIBITION PRESSURE
• Imbibition pressure=Stromal pressure in vitro• IP is reduced equivalent to IOP in vivo i.e IP =IOP-
SP• SP generates a level of inter-fibillar tension• SP may reciprocally activate chloride channels.

BARRIER MECHANISM
• Factors which prevents the flow of water• Both epithelium & endothelium function
as barrier to excessive flow of water • Diffusion of electrolytes into the stroma
due its semi-permeable nature• Corneal epithelium offers twice the
resistance to flow of water than endothelium
• Perfect semi-permeable membrane for small solutes such as NaCl+ & urea when they are used to produce hypertonicity of the solution bathing the cornea.

Endothelial Active Pump
• Factors which draw water out of cornea• Solutes diffuse across the layer ,water is
extracted osmotically• Barrier function of endothelium is calcium
dependent• Corneal transparency is decreased & corneal
thickness is increased when endothelium is damaged and to lesser extent when the epithelium is damaged

Endothelial Barrier Mechanism• Na+/K+ATPase Pump System
– Enzyme Na+/K+ACTIVATED ATPase mediates the extrusion of Na+ from tissue
– Oubain, a specific ATPase inhibitor, when applied topically to eye blocks endothelial fluid transport & results in corneal over hydration
• Bicarbonate Dependent ATPase– Depletion of bicarbonate from incubation/perfusion induces swelling
• Carbonic Anhydrase Enzyme– Implicated in regulation of fluid transport , – Carbonic anhydrase inhibitor decreases flow of fluid from stroma to
aqueous humour• Na+/H+ Pump• Passive ion movement also occur,K+, Cl-& HCO3- ions diffuse into the
aqueous humour,• In contralateral direction, Na+, Cl- & HCO3 passively diffuse from the
aqueous to cornea.

• Role of Evaporation of Tears– Evaporation of precorneal tear film results in
increased osmolarity– Hypertonicity of the tear film draw water from the
cornea, loss of fluid is replaced by aqueous
• Role of Intraocular Pressure (IOP)– Edema may occur
o When IOP exceeds stromal pressureo In normal IOP when Stromal Pressure is
decreased

Drug Permeability Across Cornea
• Lipid & water solubility of drug• Molecular size, weight & concentration of drug• Ionic form of the drug• Ph of the solution• Tonicity of solution• Surface active agents• Pro-drug form

• LIPID & WATER SOLUBILITY
– A drug should be amphipathic i.e both lipid & water soluble to readily penetrate across cornea
MOLECULAR SIZE , WEIGHT, & CONCENTRATION
– Molecular weight < 100 can pass easily & those with >500 cannot pass easily
– The rate of penetration through cornea of drug such as pilocarpine, homatropine, atropine, steroids depend upon their concentration in the solution.

• Ionic Form of The Drug– The drug intended for topical use in eye must
have capacity to exist in both ionized & non–ionized form for better penetration through the cornea since only non-ionized drugs can penetrate through epithelium & ionized drugs can pass through stroma
• Ph of the Solution– Varies from 4-10 without affecting the
permeability of the epithelium, but solution outside this range increases the permeability

Tonicity Of The Solution• Hypotonicity of solution (those below 0.9% of sodium
chloride)increases the permeability of epithelium
Surface Active Agents • Agents that reduce surface tension ,increase corneal wetting
& therefore present more drug for absorption e.g. bezalkonium chloride used as perservative also acts as wetting agent & thus increases the drug asorption
Pro-drug Form• are lipophilic & after absorption through epithelium are
converted into proper drug which can easily pass through stroma e.g. dipiverfin is pro-drug which is converted into epinephrine after its absorption into the eye

THANK YOU


















