Anatomy of Cholelithiasis
20
PRESENTATION ON CHOLELITHIASIS
-
Upload
healthabove60 -
Category
Healthcare
-
view
198 -
download
4
Transcript of Anatomy of Cholelithiasis

PRESENTATION ONCHOLELITHIASIS
DEFINITION
Cholelithiasis (calculi or gallstones) usually form in the gallbladder from the solid constituents of bile and vary greatly in size, shape and composition.
INCIDENCE•Uncommon in children and young adults
• Increasingly prevalent after age 40.
•The incidence increases thereafter to such an extent that it has been estimated that by the age of 75, one of every three people will have gall stones
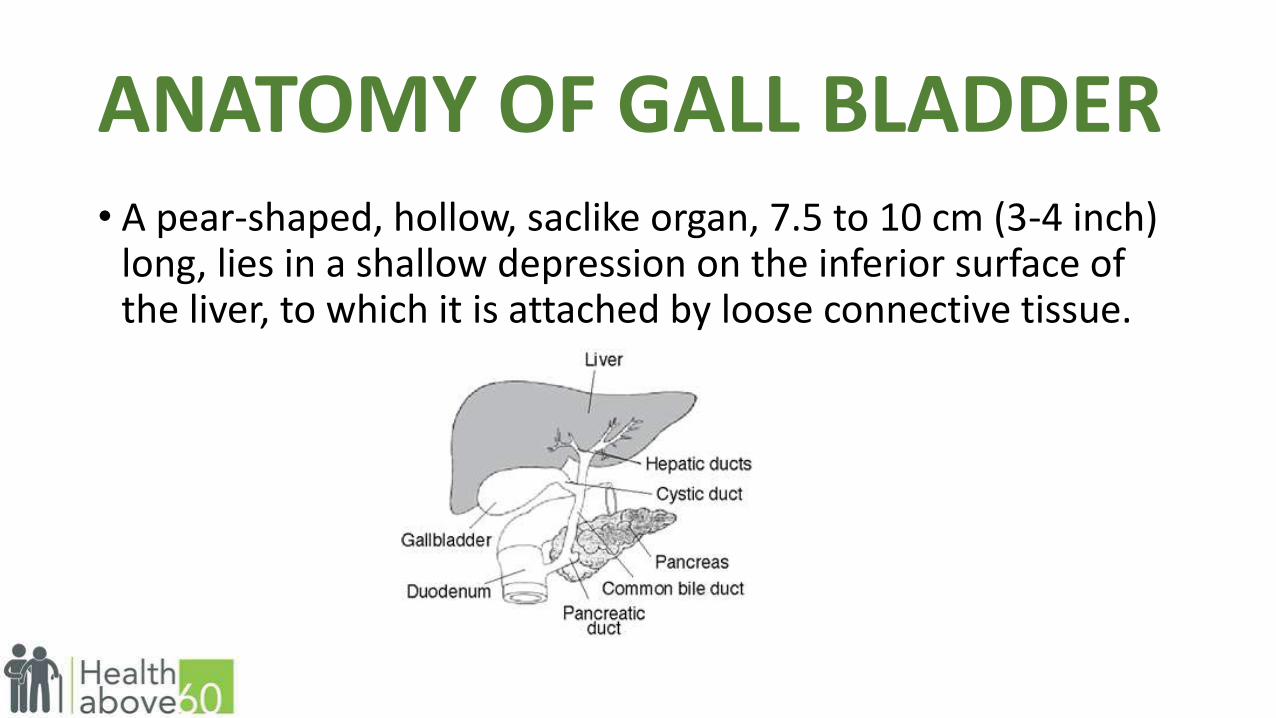
ANATOMY OF GALL BLADDER• A pear-shaped, hollow, saclike organ, 7.5 to 10 cm (3-4 inch)
long, lies in a shallow depression on the inferior surface of the liver, to which it is attached by loose connective tissue.
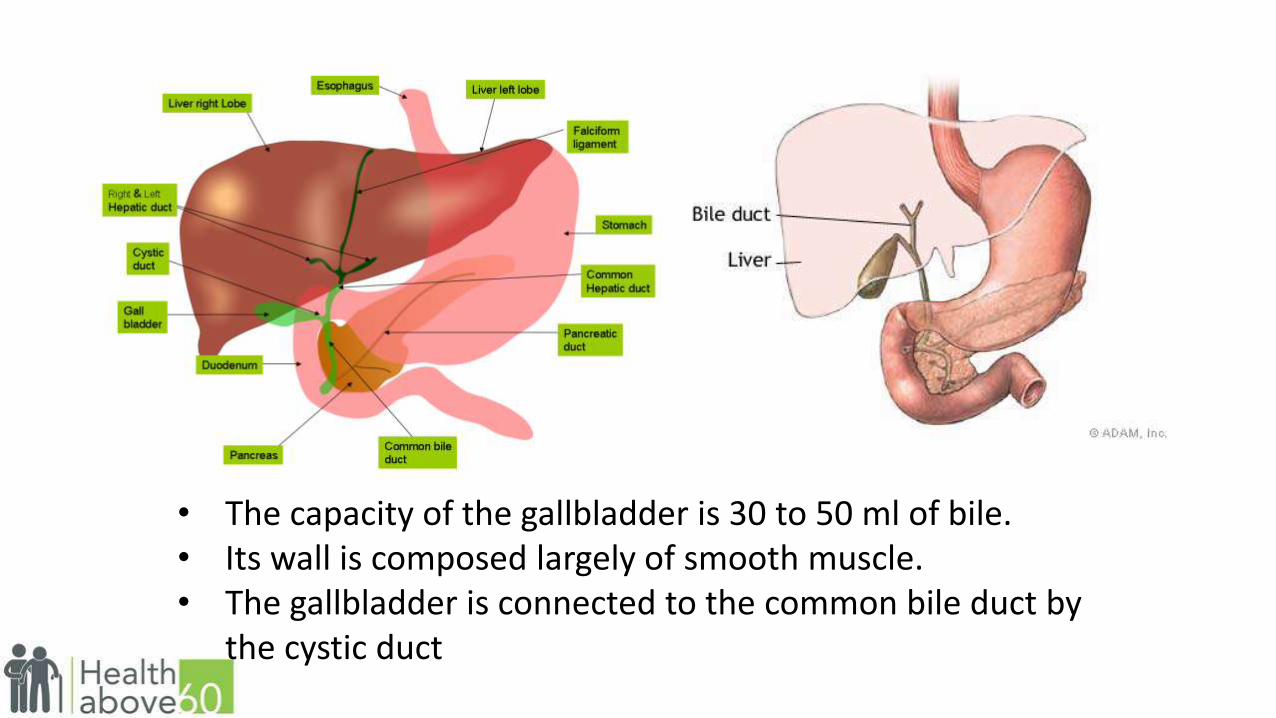
• The capacity of the gallbladder is 30 to 50 ml of bile. • Its wall is composed largely of smooth muscle.• The gallbladder is connected to the common bile duct by
the cystic duct

PHYSIOLOGY OF GALLBLADDER
• It act as a storage depot for bile
• Between meals, when the sphincter of Oddi is closed, bile produced by the hepatocytes enters the gallbladder
• During storage, a large portion of the water in bile is absorbed through the walls of the gallbladder, so that gallbladder bile is 5-10 times more concentrated than that originally secreted by the liver.
• When food enters the duodenum, the gallbladder contracts and the sphincter of Oddi relaxes, allowing the bile to enter the intestine.
• This response is mediated by secretion of the hormone cholecystokinin-pancreozymin (CCK-PZ) from the intestinal wall
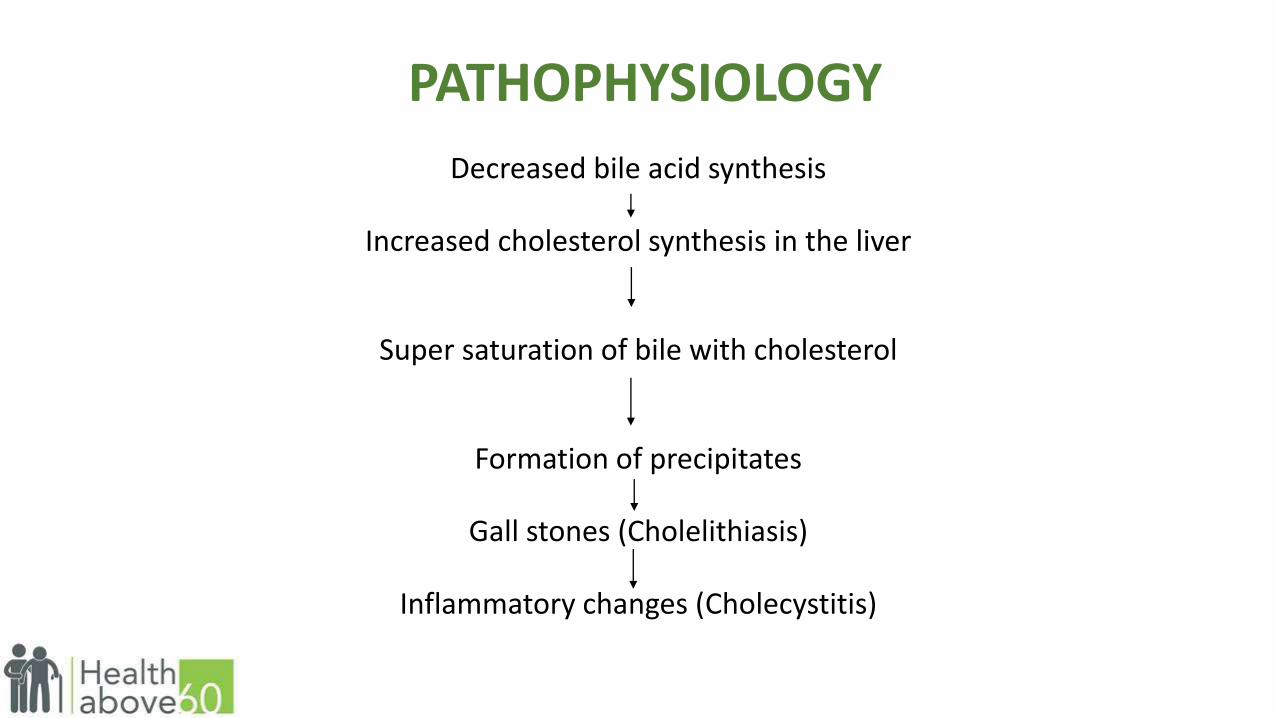
PATHOPHYSIOLOGY
Decreased bile acid synthesis
Increased cholesterol synthesis in the liver
Super saturation of bile with cholesterol
Formation of precipitates
Gall stones (Cholelithiasis)
Inflammatory changes (Cholecystitis)
TYPES OF GALLSTONES
• Cholesterol stones
• Pigment stones
• Mixed stones - the most common type. They are comprised of cholesterol and salts.
• Cholesterol stones are usually yellow-green and are made primarily of hardened cholesterol.
• Pigment stones are small, dark stones made of bilirubin. The exact cause is not known. They tend to develop in people who have cirrhosis, biliary tract infections, and hereditary blood disorders such as sickle cell anaemia in which too much bilirubin is formed.
RISK FACTORS
• Age over 40 years
• Multiparous women
• Obesity
• Users of oral contraceptives
• Hormonal therapy
• Diabetic persons
• Patients with gastro-intestinal diseases
CLINICAL MANIFESTATION• Epigastric distress
• Feeling of Fullness
• Abdominal distention
• Vague pain in the right upper quadrant of the abdomen
• Distress may follow a meal high in fried or fatty foods
• Pain and biliary colic
• Fever
• Palpable abdominal mass
• Biliary colic with excruciating upper right abdominal pain that radiates to the back or right abdominal pain and radiates to the back or right shoulder, associated with nausea and vomiting and is noticeable several hours after a heavy meal
• Constant pain, restless in all position
• Jaundice
• Obstruction of the flow of bile into the duodenum results in
• Yellow colour skin and mucous membrane

CLINICAL MANIFESTATION Contd…..
• Marked itching of the skin
• Changes in urine and stool colour
• A very dark colored urine
• Grayish, like putty, and usually described as “clay-colored” stool.
• Vitamin deficiency
• Obstruction of bile flow also interferes with absorption of the fat-soluble vitamins A,D,E, and K
• If gallstone continues to obstruct the duct
• Abscess
• Necrosis
• Perforation
• Generalized peritonitis

DIAGNOSTIC EVALUATION
• Abdominal X-ray
• USG
• Radionuclide imaging or cholecintography
• Cholecystography
• Endoscopic retrograde cholangiopancreatography (ERCP)
• Percutaneous transhepatic cholangiography (PTC)
MEDICAL MANAGEMENT
• Ursodeoxycholic acid (UDCA)
• Chenodeoxycholic acid (chenodiol or CDCA)
The mechanism of action is the inhibition of liver synthesis and secretion of cholesterol, thereby desaturating bile. Existing stones can be decreased in size, small stones dissolved and new stones prevented from forming (6-12 months therapy)

NONSURGICAL REMOVAL
•Dissolving gallstones – MTBE – Methyl tertiary butyl ether
•A catheter and instrument with basket
•Extracorporeal shock-wave lithotripsy (ESWL)
• Intracorporeal lithotripsy

SURGICAL MANAGEMENT
•Cholecystectomy
•Minicholecystectomy
•Laparoscopic cholecystectomy
•Percutaneous cholecystostomy

CHOLECYSTECTOMY

CHOLEDOCHOSTOMY
SUPPORTIVE OR DIETARY MANAGEMENT• Low fat liquids
• Powdered supplements high in protein and carbohydrates
• Cooked fruits
• Rice or tapioca
• Lean meats
• Smashed potatoes
• Non gas forming vegetables
The following to be avoided
• Eggs
• Cream
• Pork
• Fried foods, cheese and rich dressings
• Gas forming vegetables
• Alcohol
NURSING MANAGEMENT
•Relieving pain• Improving respiratory status •Promoting skin care and biliary drainage• Improving nutritional status•Patient education and home care considerations•Monitoring and managing potential complications

THANK YOU