Anatomy & Incisions General Surgery. Incisions A variety of incisions are used The type chosen is...
24
Anatomy & Incisions General Surgery
-
Upload
ashlee-hines -
Category
Documents
-
view
266 -
download
4
Transcript of Anatomy & Incisions General Surgery. Incisions A variety of incisions are used The type chosen is...
Anatomy & Incisions
General Surgery
IncisionsA variety of incisions are usedThe type chosen is dependent on a number
of factorsAccess desiredProcedureSurgeonExtensibility (can we make it bigger?)Wound security

Layer by layer…Abdominal wall layers:
SkinSubcutaneousFasciaMusclesPreperitoneal fatPeritoneum
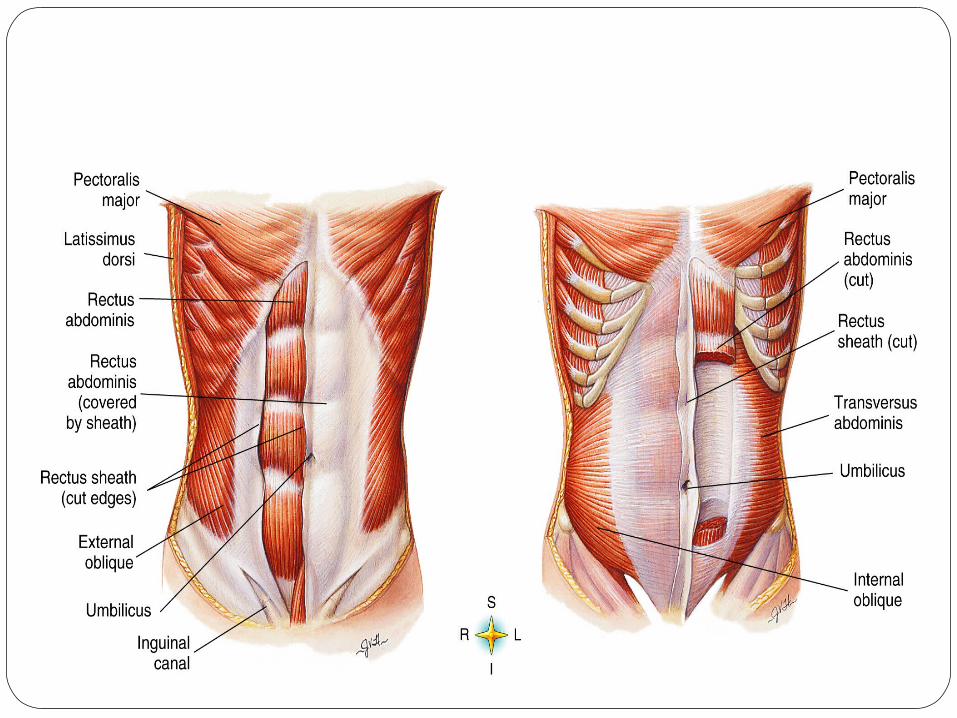

Anterolateral Abdominal Wall
The abdominal wall consists of skin, layers of fascia (connective tissue), muscles and parietal peritoneum1. It is subdivided into the anterior wall, right and left lateral walls and posterior wall for descriptive purposes2. Since the boundary between the anterior and lateral walls is indefinite and some structures (e.g. muscles and cutaneous nerves) are present in both, the combined term anterolateral abdominal wall is often used2.
1. Pectoralis major 5. Linea alba
2. Tendinous intersection of the rectus abdominis
6. Rectus abdominis muscle
3. Scarpa's fascia 7. Umbilicus
4. External oblique muscle 8. Rectus sheath (anterior layer)
After we removed the skin of the anterolateral abdominal wall, the vertical muscles, superficial flat muscles and the fascia could be clearly seen. The vertical muscle, pyramidalis muscle is missing in approximately 20% of people1,2 and it was not present in our cadaver. If present, it arises from the anterior surface of the pubis and inserts into the linea alba (a tendinous band extending down the

Tissue Layers of the Abdominal Wall
(Redrawn from Ethicon: Wound closure manual, Somerville, NJ, 2002, Ethicon, Inc.)


Organs by Quadrants

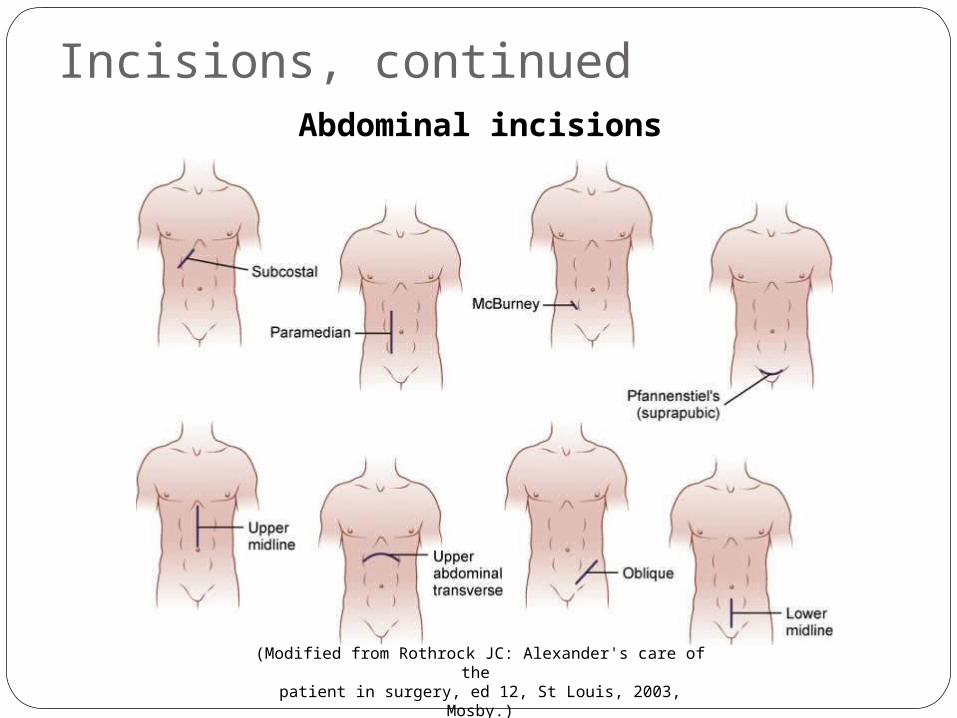
Incisions, continuedAbdominal incisions
(Modified from Rothrock JC: Alexander's care of the patient in surgery, ed 12, St Louis, 2003, Mosby.)
The good, the bad and the scar tissueEach incision type has advantages and
disadvantagesAdequacy of exposureClosure timeDisruption of blood and nerve suppliesMuscle damageWound herniaEffect pulmonary function
Other FactorsOther things may influence choice
Patient conditionNeed for speedPrevious surgeryMinimize bleeding and traumaPostop discomfortRoom to roam
And yet more pain…CosmeticsChanges in the blood supplies to the
anterior wallLimit choices for future surgeries and
reconstruction

Vertical Midline IncisionSimple to performGood exposure to all of the abdominal
cavityCan be extended from the sternal notch to
the symphysis pubis

ParamedianVertical incision that is placed 2” off of the
midlineSame indications as the vertical with the
exception of traumaLonger to create and closeBleed more readilyProne to herniation

Oblique IncisionsAllow access to specific structuresStrong However,
Splits musclesBleedingNerve damage

Muscle-Splitting IncisionsSurgical options for muscle
(Redrawn from Ethicon: Wound closure manual, Somerville, NJ, 2002, Ethicon, Inc.)

McBurneyUsed most commonly for open
appendectomyQuick and easy to closeFirm closurePoor exposure

Oblique Inguinal From the pubic tubercle to the iliac crest
above the inguinal creaseUsed for Inguinal Herniorraphy repairMay also be used for urologic, transplant or
vascular procedures in this region

SubcostalUsually made on the right side (kocher) Used for open gall bladder proceduresLeft sub costal used for spleenectomyStrong but painfulLimited exposureGood cosmetic closure

Transverse IncisionsUsed to expose either the upper or lower
regions of the abdomenSame issues as the oblique incision
PfannenstielUsed for pelvic surgeryApproximately ½” above the symphysis
pubisMost commonly used for OB/GYNExcellent exposureCosmetic
MidabdominalUsed for retroperitoneal approachesColectomy or colostomy
ThoracoabdominalUsed for proximal stomach, distal
esophagus, and anterior spinePatient is in a lateral positionBegins at midpoint between xiphoid and
umbilicus and extends to midscapular line into the chest