Anatomy and Physiology
16
1 R. Sutcliffe & O. Tucker Liver segmental anatomy 2 Hepatic artery anatomy 6 Liver resection planes 7 Liver physiology 8 Gallbladder anatomy 10 Biliary anatomy 13 Pancreatic anatomy 14 Pancreatic physiology 15 Anatomy and physiology Chapter 1 01-Sutcliffe-Chap01.indd 1 01-Sutcliffe-Chap01 indd 1 8/5/09 12:49:22 PM 8/5/09 12:49:22 PM
-
Upload
matt-lao-dionela -
Category
Documents
-
view
33 -
download
2
description
Know the Anatomy and Physiology
Transcript of Anatomy and Physiology
1
R. Sutcliffe & O. Tucker
Liver segmental anatomy 2
Hepatic artery anatomy 6
Liver resection planes 7
Liver physiology 8
Gallbladder anatomy 10
Biliary anatomy 13
Pancreatic anatomy 14
Pancreatic physiology 15
Anatomy and physiology
Chapter 1
01-Sutcliffe-Chap01.indd 101-Sutcliffe-Chap01 indd 1 8/5/09 12:49:22 PM8/5/09 12:49:22 PM

2 CHAPTER 1 Anatomy and physiology
Liver segmental anatomy
The liver is the largest solid organ (weight 1.2–1.6kg), and lies in the
right upper quadrant of the abdomen below the right hemidiaphragm.
Peritoneal attachments: falciform ligament, coronary ligament, and
left and right triangular ligaments (see Fig. 1.3).
The Glissonian capsule is a fi brous covering over the liver, except the
bare area, where the liver is in direct contact with the diaphragm.
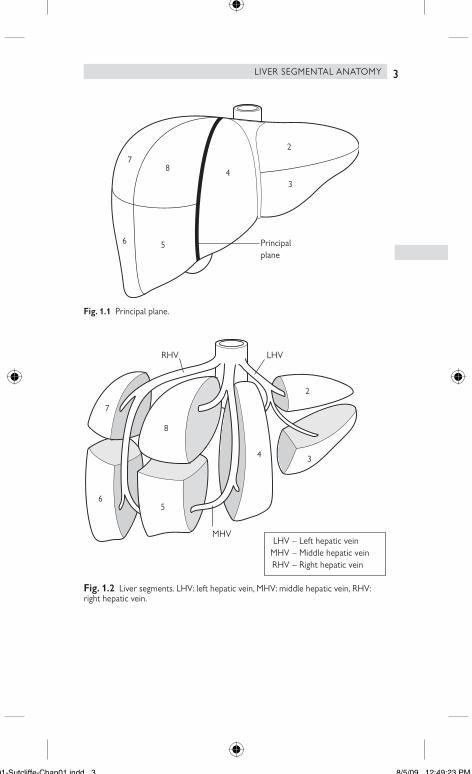
Liver segments
Anatomical divisions are based on vascular and biliary anatomy not
surface markings (see Figs 1.1 and 1.2).
The arterial supply to the liver is via the common hepatic artery
(branch of coeliac axis), which usually runs to the left of the common
bile duct, before dividing into left and right branches. There is consider-
able anatomical variation of the hepatic arteries (Hepatic artery
anatomy b p. 6).
The mid-plane of the liver separates the right lobe (supplied by
right hepatic artery and right portal vein) from the left lobe (supplied
by left hepatic artery and left portal vein). The principal plane
(see Fig. 1.1) intersects the gallbladder fossa anteriorly and the
inferior vena cava fossa posteriorly.
The left and right hepatic ducts (fi rst-order ducts) drain bile into the
common hepatic duct from each lobe.
Second-order ducts and arteries divide each lobe into two sections.
right lobe => anterior and posterior sections;
left lobe => medial and lateral sections.
The left intersectional plane corresponds to the umbilical fi ssure
and the attachment of the falciform ligament to the liver. The right
intersectional plane does not have a surface marking.
Third-order divisions of the liver are also known as Couinaud’s
segments.
right anterior section => segments 5 and 8
right posterior section => segments 6 and 7;
left lateral section => segments 2 and 3;
left medial section => segment 4.
The caudate lobe is distinct from the left and right lobes, and is also
referred to as segment 1. It lies between the porta hepatis and the
inferior vena cava. It receives a blood supply from both left and right
hepatic arteries, and bile drains into both left and right hepatic ducts.
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
01-Sutcliffe-Chap01.indd 201-Sutcliffe-Chap01 indd 2 8/5/09 12:49:23 PM8/5/09 12:49:23 PM
3
7
6
8
5
4
2
3
Principalplane
Fig. 1.1 Principal plane.
Fig. 1.2 Liver segments. LHV: left hepatic vein, MHV: middle hepatic vein, RHV:
right hepatic vein.
– Left hepatic vein– Middle hepatic vein– Right hepatic vein
LHVMHVRHV
7
65
4 3
2
8
RHV LHV
MHV
LIVER SEGMENTAL ANATOMY
01-Sutcliffe-Chap01.indd 301-Sutcliffe-Chap01 indd 3 8/5/09 12:49:23 PM8/5/09 12:49:23 PM
4 CHAPTER 1 Anatomy and physiology
The portal vein drains blood from the gastrointestinal tract
(from lower oesophagus to rectum), pancreas, and spleen. It is formed
by the union of the splenic and superior mesenteric veins posterior to
the neck of the pancreas. The inferior mesenteric vein invariably drains
into the splenic vein.
The right portal vein supplies the right lobe and its branches
correspond to those of the right hepatic artery.
The left portal vein is initially horizontal and changes direction at the
ligamentum venosum to become vertical (umbilical portion, in the
umbilical fi ssure). The vertical portion is a remnant of the umbilical
vein, and gives branches to segment 4 (to its right), and segments 2
and 3 (to its left).
The hepatic veins drain blood from the liver into the inferior vena
cava, and lie between sections or lobes:
left hepatic vein – between s2 and s3 then left intersectional plane;
middle hepatic vein – mid-plane (between s4 and s5/8);
right hepatic vein – right intersectional plane (between s5/8
and s6/7).
10% of patients have a large inferior right hepatic vein in addition to a
superior right hepatic vein.
The caudate lobe drains blood directly into the IVC, via several small
veins.
See Fig. 1.3.
•
•
•
•
•
•
•
•
•
01-Sutcliffe-Chap01.indd 401-Sutcliffe-Chap01 indd 4 8/5/09 12:49:23 PM8/5/09 12:49:23 PM
5
G
G
FL
LTL
IVC
R
L
PH
BA
UC
LC
RTL
Posterior view
Anterior view
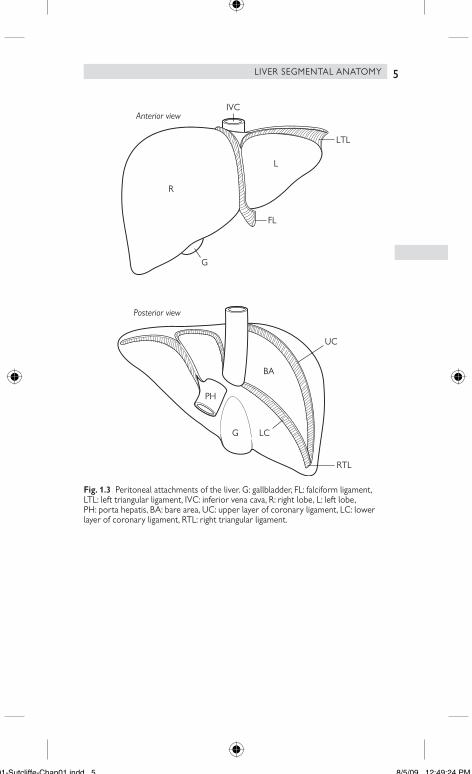
Fig. 1.3 Peritoneal attachments of the liver. G: gallbladder, FL: falciform ligament,
LTL: left triangular ligament, IVC: inferior vena cava, R: right lobe, L: left lobe,
PH: porta hepatis, BA: bare area, UC: upper layer of coronary ligament, LC: lower
layer of coronary ligament, RTL: right triangular ligament.
LIVER SEGMENTAL ANATOMY
01-Sutcliffe-Chap01.indd 501-Sutcliffe-Chap01 indd 5 8/5/09 12:49:24 PM8/5/09 12:49:24 PM
6 CHAPTER 1 Anatomy and physiology
Hepatic artery anatomy
An accessory artery indicates that the proper hepatic artery
(left, right, or common) is also present.
A replaced artery indicates that the proper artery is absent.
An accessory or replaced left hepatic artery arises from the left
gastric artery and runs in the lesser omentum.
An accessory or replaced right hepatic artery arises from the
superior mesenteric artery, and passes behind the common bile duct
to run along its right posterolateral border into the liver.
•
•
•
•
01-Sutcliffe-Chap01.indd 601-Sutcliffe-Chap01 indd 6 8/5/09 12:49:24 PM8/5/09 12:49:24 PM
7
Liver resection planes
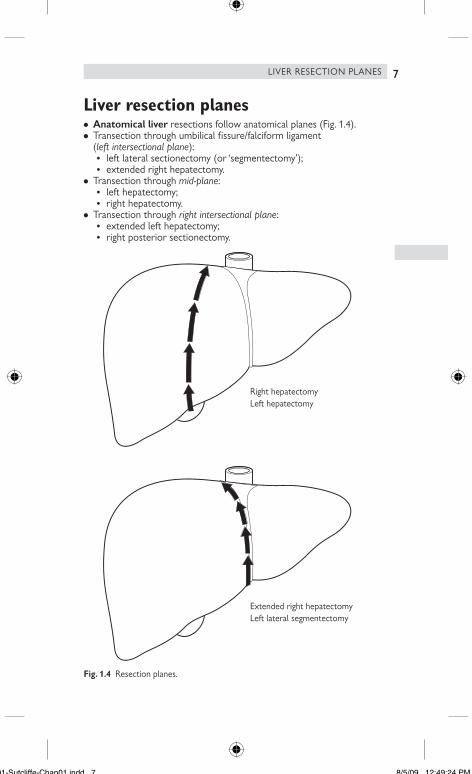
Anatomical liver resections follow anatomical planes (Fig. 1.4).
Transection through umbilical fi ssure/falciform ligament
(left intersectional plane):
left lateral sectionectomy (or ‘segmentectomy’);
extended right hepatectomy.
Transection through mid-plane:
left hepatectomy;
right hepatectomy.
Transection through right intersectional plane:
extended left hepatectomy;
right posterior sectionectomy.
Fig. 1.4 Resection planes.
Extended right hepatectomyLeft lateral segmentectomy
Right hepatectomyLeft hepatectomy
•
•
•
•
•
•
•
•
•
•
LIVER RESECTION PLANES
01-Sutcliffe-Chap01.indd 701-Sutcliffe-Chap01 indd 7 8/5/09 12:49:24 PM8/5/09 12:49:24 PM

8 CHAPTER 1 Anatomy and physiology
Liver physiology
The liver parenchyma is arranged into lobules, which contain several
acini. An acinus is arranged around terminal branches of the hepatic
artery and portal vein.
Hepatocytes receive their blood supply via the hepatic sinusoids, which
are fenestrated capillaries lined by endothelial cells. Sinusoids are lined
by Kupffer cells (part of reticulo-endothelial system), hepatic stellate
cells, and liver-associated lymphocytes.
Bile canaliculi drain bile from hepatocytes into a network of cholangi-
oles and larger ducts, before entering the common hepatic duct
Liver function
The liver has substantial reserve capacity, which allows signifi cant damage
(e.g. cirrhosis) to occur before symptoms develop. A signifi cant volume
of liver (up to 60%) can be resected safely, without patients developing
liver failure, provided that the future liver remnant is of good quality and
an adequate volume (see Complications after liver resection, Early, Small-
for-size syndrome b p. 190).
Metabolism:
carbohydrates (gluconeogenesis, glycogenesis, glycogenolysis);
protein;
lipids;
bilirubin;
hormones;
haemoglobin;
drugs;
lactate.
Synthesis:
albumin;
clotting factors (fi brinogen, prothrombin, V, VII, IX, XI, protein C,
protein S, antithrombin);
cholesterol;
triglycerides;
bile;
lipoproteins;
caeruloplasmin;
transferrin;
complement;
glycoproteins.
Storage
glycogen;
vitamin B12;
iron;
copper.
Foetal erythropoiesis.
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
01-Sutcliffe-Chap01.indd 801-Sutcliffe-Chap01 indd 8 8/5/09 12:49:24 PM8/5/09 12:49:24 PM
9LIVER PHYSIOLOGY
01-Sutcliffe-Chap01.indd 901-Sutcliffe-Chap01 indd 9 8/5/09 12:49:25 PM8/5/09 12:49:25 PM

10 CHAPTER 1 Anatomy and physiology
Gallbladder anatomy
The gallbladder is a hollow organ that concentrates and stores bile.
It lies in the gallbladder fossa on the inferior aspect of the right lobe.
It has a rounded fundus, a body, and an infundibulum. Gallstones may
become impacted in Hartmann’s pouch.
The presence of fat in the duodenum stimulates the release of
cholecystokinin (CCK), which causes contraction of the gallbladder and
secretion of bile through the cystic duct, common bile duct, and into
the duodenum.
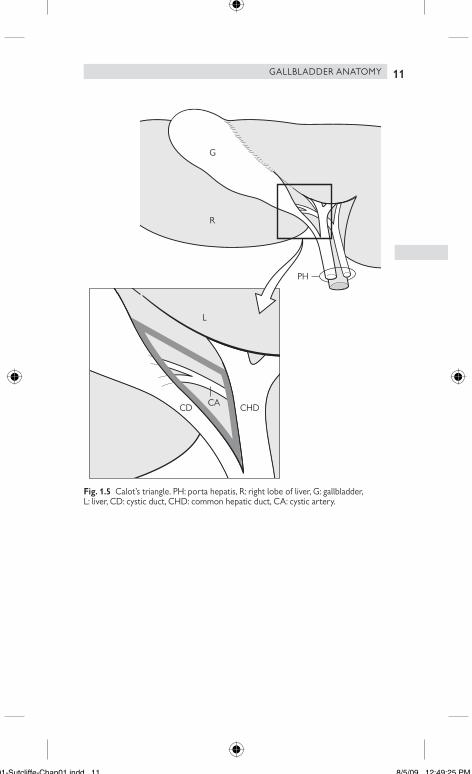
Calot’s triangle is bordered by the gallbladder, the common hepatic
duct and the liver (Fig. 1.5). The peritoneal covering of the gallbladder
extends onto the anterior and posterior aspects of Calot’s triangle and
onto the portal structures. The arterial supply of the gallbladder is via
the cystic artery, which usually arises from the right hepatic artery and
lies within Calot’s triangle. Occasionally, the cystic artery has anterior
and posterior branches before entering the gallbladder.
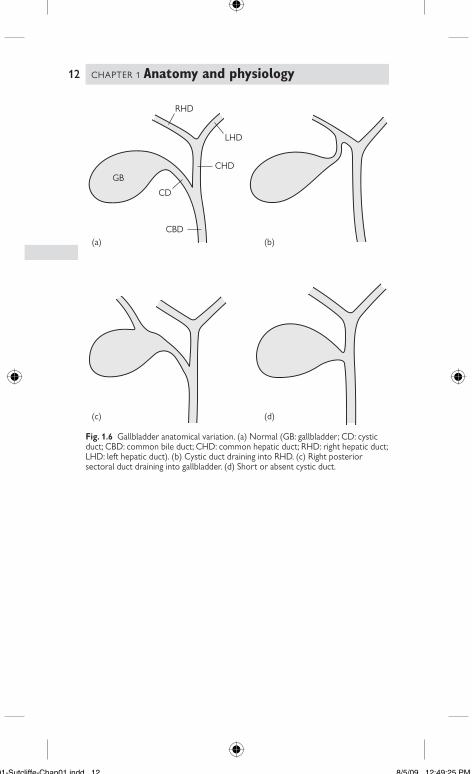
The cystic duct joins the common hepatic duct to form the common
bile duct, usually about 5cm above the duodenum. Rarely, an accessory
cystic duct (duct of Luschka) drains bile intrahepatically through the
gallbladder fossa, and is susceptible to injury during cholecystectomy
(Fig. 1.6).
Venous drainage of the gallbladder occurs via multiple small veins that
enter the portal vein, either through the gallbladder fossa or Calot’s
triangle
•
•
•
•
•
01-Sutcliffe-Chap01.indd 1001-Sutcliffe-Chap01 indd 10 8/5/09 12:49:25 PM8/5/09 12:49:25 PM
11
L
CHDCD CA
PH
G
R
Fig. 1.5 Calot’s triangle. PH: porta hepatis, R: right lobe of liver, G: gallbladder,
L: liver, CD: cystic duct, CHD: common hepatic duct, CA: cystic artery.
GALLBLADDER ANATOMY
01-Sutcliffe-Chap01.indd 1101-Sutcliffe-Chap01 indd 11 8/5/09 12:49:25 PM8/5/09 12:49:25 PM
12 CHAPTER 1 Anatomy and physiology
(a) (b)
(c) (d)
RHD
LHD
CHD
CD
CBD
GB
Fig. 1.6 Gallbladder anatomical variation. (a) Normal (GB: gallbladder; CD: cystic
duct; CBD: common bile duct; CHD: common hepatic duct; RHD: right hepatic duct;
LHD: left hepatic duct). (b) Cystic duct draining into RHD. (c) Right posterior
sectoral duct draining into gallbladder. (d) Short or absent cystic duct.
01-Sutcliffe-Chap01.indd 1201-Sutcliffe-Chap01 indd 12 8/5/09 12:49:25 PM8/5/09 12:49:25 PM
13
Biliary anatomy
The left and right hepatic ducts unite at the base of segment 4,
anterior to the portal vein bifurcation. The common hepatic duct
passes inferiorly in the right edge of the hepatoduodenal ligament,
to the right of the common hepatic artery, and joins the cystic duct
to become the common bile duct.
The common bile duct (diameter 3–7mm) passes behind the fi rst part
of the duodenum, enters the head of the pancreas, and terminates at
the ampulla of Vater.
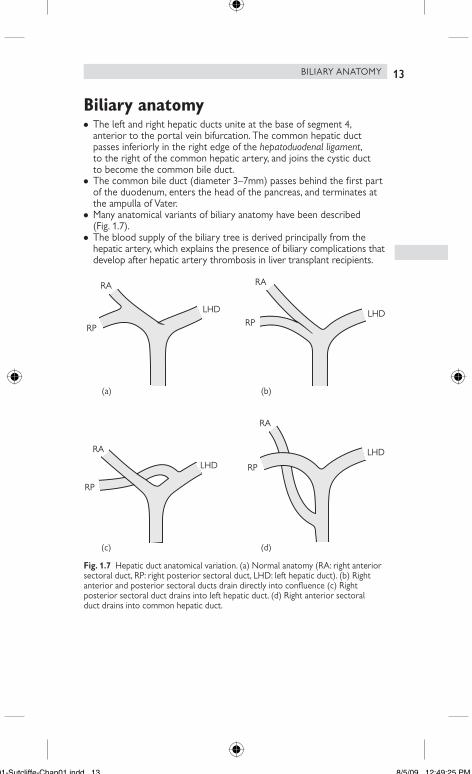
Many anatomical variants of biliary anatomy have been described
(Fig. 1.7).
The blood supply of the biliary tree is derived principally from the
hepatic artery, which explains the presence of biliary complications that
develop after hepatic artery thrombosis in liver transplant recipients.
Fig. 1.7 Hepatic duct anatomical variation. (a) Normal anatomy (RA: right anterior
sectoral duct, RP: right posterior sectoral duct, LHD: left hepatic duct). (b) Right
anterior and posterior sectoral ducts drain directly into confl uence (c) Right
posterior sectoral duct drains into left hepatic duct. (d) Right anterior sectoral
duct drains into common hepatic duct.
RA
RP
LHD LHD
RA
RP
RA
RP
LHD
RA
RP
LHD
(a) (b)
(c) (d)
•
•
•
•
BILIARY ANATOMY
01-Sutcliffe-Chap01.indd 1301-Sutcliffe-Chap01 indd 13 8/5/09 12:49:25 PM8/5/09 12:49:25 PM
14 CHAPTER 1 Anatomy and physiology
Pancreatic anatomy
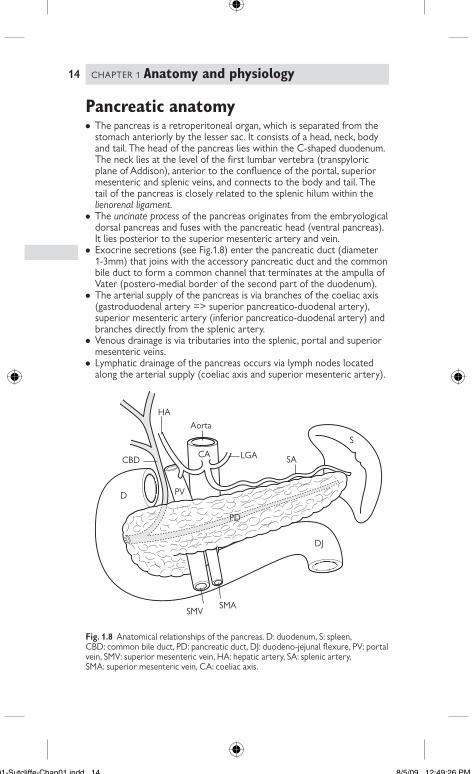
The pancreas is a retroperitoneal organ, which is separated from the
stomach anteriorly by the lesser sac. It consists of a head, neck, body
and tail. The head of the pancreas lies within the C-shaped duodenum.
The neck lies at the level of the fi rst lumbar vertebra (transpyloric
plane of Addison), anterior to the confl uence of the portal, superior
mesenteric and splenic veins, and connects to the body and tail. The
tail of the pancreas is closely related to the splenic hilum within the
lienorenal ligament.
The uncinate process of the pancreas originates from the embryological
dorsal pancreas and fuses with the pancreatic head (ventral pancreas).
It lies posterior to the superior mesenteric artery and vein.
Exocrine secretions (see Fig.1.8) enter the pancreatic duct (diameter
1-3mm) that joins with the accessory pancreatic duct and the common
bile duct to form a common channel that terminates at the ampulla of
Vater (postero-medial border of the second part of the duodenum).
The arterial supply of the pancreas is via branches of the coeliac axis
(gastroduodenal artery => superior pancreatico-duodenal artery),
superior mesenteric artery (inferior pancreatico-duodenal artery) and
branches directly from the splenic artery.
Venous drainage is via tributaries into the splenic, portal and superior
mesenteric veins.
Lymphatic drainage of the pancreas occurs via lymph nodes located
along the arterial supply (coeliac axis and superior mesenteric artery).
Fig. 1.8 Anatomical relationships of the pancreas. D: duodenum, S: spleen,
CBD: common bile duct, PD: pancreatic duct, DJ: duodeno-jejunal fl exure, PV: portal
vein, SMV: superior mesenteric vein, HA: hepatic artery, SA: splenic artery,
SMA: superior mesenteric vein, CA: coeliac axis.
LGACBD
D
PD
HA
Aorta
CA
DJ
S
SA
SMASMV
PV
•
•
•
•
•
•
01-Sutcliffe-Chap01.indd 1401-Sutcliffe-Chap01 indd 14 8/5/09 12:49:26 PM8/5/09 12:49:26 PM

15
Pancreatic physiology
Exocrine: acinar cells secrete bicarbonate (regulated by secretin) and
inactive pro-enzymes (regulated by CCK), which are activated in the
duodenum (e.g. trypsin, amylase, lipase, chymotrypsin). Bicarbonate
neutralizes gastric acid, and enzymes digest dietary proteins, lipids, and
carbohydrate to allow absorption. Lipid absorption is facilitated by bile
acids (secreted in bile).
Endocrine: Islets of Langerhans consist of alpha, beta, delta, and
PP cells, which secrete glucagon, insulin, somatostatin, and pancreatic
polypeptide, respectively.
•
•
PANCREATIC PHYSIOLOGY
01-Sutcliffe-Chap01.indd 1501-Sutcliffe-Chap01 indd 15 8/5/09 12:49:26 PM8/5/09 12:49:26 PM
01-Sutcliffe-Chap01.indd 1601-Sutcliffe-Chap01 indd 16 8/5/09 12:49:26 PM8/5/09 12:49:26 PM