ANATOMICAL VARIATIONS OF TENTORIAL VENOUS SINUS IN …
88
ANATOMICAL VARIATIONS OF TENTORIAL VENOUS SINUS IN 100 CASES OF AUTOPSY DISSERTATION SUBMITTED FOR MASTER OF CHIRURGIE – BRANCH II NEUROSURGERY – 3 YEARS THE TAMILNADU DR.M.G.R MEDICAL UNIVERSITY CHENNAI TAMILNADU AUGUST 2010
Transcript of ANATOMICAL VARIATIONS OF TENTORIAL VENOUS SINUS IN …

ANATOMICAL VARIATIONS OF
TENTORIAL VENOUS SINUS IN 100
CASES OF AUTOPSY
DISSERTATION SUBMITTED FOR
MASTER OF CHIRURGIE – BRANCH II
NEUROSURGERY – 3 YEARS
THE TAMILNADU DR.M.G.R MEDICAL UNIVERSITY
CHENNAI
TAMILNADU
AUGUST 2010

ANATOMICAL VARIATIONS OF TENTORIAL VENOUS SINUS IN 100 CASES OF AUTOPSY
DISSERTATION
Submitted to THE TAMILNADU DR. M.G.R. MEDICAL
UNIVERSITY
in partial fulfillment of the requirement for the award of
degree
MASTER OF CHIRURGIE - BRANCH II
NEUROSURGERY - 3 YEARS
August 2010
MADURAI MEDICAL COLLEGE Madurai
THE TAMILNADU DR.M.G.R MEDICAL
UNIVERSITY
CHENNAI
CERTIFICATE
This is to certify that this dissertation titled
“ANATOMICAL VARIATIONS OF TENTORIAL VENOUS
SINUS IN 100 CASES OF AUTOPSY” is an original bonafide
work conducted by Dr.L.SANKAR at Madurai Medical College,
Madurai under my guidance and supervision.
The DEAN,
Madurai Medical College,
Madurai.
Prof.Dr.N.ASOKKUMAR, M.Ch.,
Professor and Head of Department,
Department of Neurosurgery,
Madurai Medical College,
Madurai.
DECLARATION
I solemnly declare that this dissertation “ANATOMICAL
VARIATIONS OF TENTORIAL VENOUS SINUS IN 100
CASES OF AUTOPSY” was prepared by me under the
guidance and supervision of Professor & HOD, Department of
Neurosurgery, Madurai Medical College and Government
Rajaji Hospital, Madurai between 2007 and 2010.
This is submitted to The Tamil Nadu Dr. M.G.R. Medical
University, Chennai, in partial fulfillment of the requirement
for the award of MASTER OF CHIRURGIE, NEUROSURGERY,
degree Examination to be held in AUGUST 2010.
Place: Madurai.
Date :
Dr. L.SANKAR
ACKNOWLEDGEMENT
I thank with gratitude, The DEAN, Madurai medical
college, Madurai for permitting me to utilize the clinical
materials of this hospital.
I am gratefully indebted to Prof.Dr.N.Asokkumar, M.Ch.,
Head of Department, Department of Neurosurgery for the
valuable guidance, advice and inspiration rendered in this
study.
I acknowledge the guidance and support given by
Prof.Dr.N.Muthu Kumar, M.Ch., to complete the study
successfully.
I wish to express my sincere thanks to
Prof.Dr.S.Manoharan, M.Ch., and Prof.Dr.D.Kailairajan,
M.Ch., for their guidance and help during this study.
I am thankful to all assistant professors of my
department and Professor of Forensic Medicine,
Dr.G. Natarajan M.D. for their encouragement and guidance
to complete the study.

Finally I would like to extent my heart felt appreciation to
my parents and wife who assisted me in every way in
preparing this study.
CONTENTS
PARTICULARS PAGE NO.
1. INTRODUCTION 1
2. AIM OF STUDY 2
3. MATERIALS AND METHODS 3
4. REVIEW OF LITERATURE 5
5. RESULTS 32
6. DISCUSSION 44
7. CONCLUSION 55
8. BIBLIOGRAPHY
8. PROFORMA
9. MASTER CHART

1
INTRODUCTION
The presence of venous sinuses within the tentorium cerebelli is
not mentioned in standard textbooks of neuroanatomy1. Gibbs and
Gibbs2, in their study on the torcular and lateral sinuses, seem to have
been the first to describe tentorial sinuses. Since then it was subsequently
studied by many anatomist, neurosurgeon and radiologist.
Certain neurosurgical procedures such as transoccipital
transtentorial, infratentorial supracerebellar, and subtemporal
transtentorial approaches require sectioning of the tentorium. The
presence of venous sinuses within the tentorium makes these procedures
difficult. Knowledge of their anatomy is important to decide the direction
of incision and appropriate method of hemostasis to reduce venous
congestion and bleeding.

2
AIM OF STUDY
The aim of study is
1. To determine the incidence of venous sinuses within the tentorium
cerebelli.
2. To identify the location, configuration and size of the sinuses
within the tentorium.
3. To know the pattern of drainage of these sinuses.
3
MATERIALS AND METHODS
This anatomical study of tentorial venous sinus is a cadaveric study.
Cases excluded from the study are
1. Head injury
2. Intracranial pathology
3. Accidental distortion during dissection
In this study, 100 human cadaveric brains of both male and female
that underwent autopsy with in 12-48 hrs after death were studied. Skull
cap was opened in circular manner. The frontal lobes were lifted after
opening the duramater and the anterior falx was cut. The brain stem was
cut axially just above the level of tentorial insisura.
The cerebral hemispheres were removed and the tentorium was
inspected macroscopically for the presence of venous sinuses. The size,
configuration, location, and pattern of venous drainage were noted.
Subsequently, the brain stem and cerebellum were removed through the
tentorial incisura, and the tentorium was inspected again. This was
performed to avoid confusing the veins on the surface of the cerebellum
with venous sinuses, which was possible especially when the tentorium

4
was thin. In addition, the tentorial sinus was opened, and a probe was
passed inside to confirm its presence.
An imaginary line drawn horizontally at the junction of the
superior petrosal sinus and transverse sinus was used to divide the
tentorium arbitrarily into anterior and posterior portions. And again the
tentorium was arbitrarily divide into medial one-third, middle one-third,
lateral one-third on relation to the transverse sinus.

5
REVIEW OF LITERATURE
Anatomy of the Tentorium cerebelli
The tentorium is a membrane which covers the cerebellum3. It
separates the cerebrum from the cerebellum. The term tentorium was first
coined by Winslow. He called it as la tente4. Tent means something
covers rather than supports.
The tentorium is attached to temporal, occipital, and sphenoid
bones. All of the tentorial margins, except the free edges bordering the
incisura, are rigidly attached to the cranium5. The anterior border is
attached to the petrous ridge. The lateral and posterior borders are
attached to the inner surface of the occipital and temporal bones along the
internal occipital protuberance and to the edges of the groove for the
transverse sinus5.
The anterior end of each free edge is attached to the petrous apex
and the anterior and posterior clinoid processes.
6
The attachment to the petrous apex and the clinoid processes forms
three dural folds: the anterior and posterior petroclinoid folds and the
interclinoid fold. Between these folds the oculomotor trigone is located,
through which the oculomotor and trochlear nerves enter the sinus. The
posterior petroclinoid fold extends from the petrous apex to the posterior
clinoid process5.
The anterior petroclinoid fold extends from the petrous apex to the
anterior clinoid process; The interclinoid fold covers the ligament
extending from the anterior to the posterior clinoid process. The
oculomotor nerve penetrates the dura in the central part of this triangle,
the oculomotor triangle, and the trochlear nerve enters the dura at the
posterolateral edge of this triangle.
The petro sphenoid ligament passes between the leaves of the
posterior petroclinoid fold from the petrous apex to the lateral border of
the dorsum sellae, just below the posterior clinoid process6. The abducens
nerve passes below the petro sphenoid ligament to enter the cavernous
sinus.
7
From the anterior part of the free edge, the dura mater slopes
steeply downward to form the lateral wall of the cavernous sinus and to
cover the middle cranial fossa. The attachment of the anterior end of the
free edge to the petrous apex may be situated as much as 10 mm lateral
and 8 mm below the level of the clinoid processes7.
The low position of the free edge may facilitate descending
tentorial herniations. The falx cerebri fuses into the dorsal surface of the
tentorium in the midline behind the apex. The straight sinus is enclosed in
the falcotentorial junction. It begins at the tentorial apex, where it receives
the vein of Galen and of the inferior sagittal sinus, and terminates in the
torcular sinus.
Embryology of Tentorial venous sinus
Based on literatures tentorial venous sinuses may be formed by any
one of the ways described below.
By the end of the first month of gestation, when the embryo is
approximately 5 to 8 mm in length, the neural tube is surrounded by a
primitive capillary plexus throughout its length. The rostral portion of the
neural tube from which the brain arises is drained by three dural plexuses,

8
as follows: 1) the anterior plexus, which drains the forebrain
(telencephalon and diencephalon); 2) the middle plexus, which drains the
pons and the cerebellum (metencephalon); and 3) the posterior plexus,
which drains the medulla (myelencephalon).
These plexuses drain over the dorsal aspect of the neural tube and
enter the dorsal aspect of the primary head sinus. By the 14-mm stage, the
tentorial sinus (to be differentiated from the postnatal structure of the
same name), located at the caudoventral portion of the cerebral
hemispheres, terminates in the stem of the anterior dural sinus.
During the 24-mm stage, the tentorial sinus gains prominence as the
stem of the anterior dural plexus dwindles and/or disappears. It serves as
the major drainage for the largest vessels of the cerebrum, including the
middle cerebral veins, as well as the diencephalon and corpus striatum
before the formation of the basal cerebral vein.
The tentorial sinus as described here, however, may have a
protracted existence developmentally and may endure permanently 7. The
relationship between the tentorial sinus of adults and that of the human
9
embryo is not firmly established8. However, as suggested by Lasjaunias
and Raybaud9, the tentorial sinus described above probably represents one
of the several possible modes of persistence of the embryonic
arrangement.
During the 24-mm stage, are grouped together as the tentorial
plexus. This plexus occupies the wedge of the mesenchyme (the primitive
tentorium cerebelli) located between the enlarging cerebrum and
cerebellum. As the cerebral hemispheres expand and overgrow the
developing diencephalic and mesencephalic areas, the tentorial plexus is
gradually reduced. Ultimately, it is represented by the torcular or
confluens of sinuses7. The venous sinuses in the tentorium may represent
the persistent remnants of the primitive tentorial venous plexus.
Okudera et al.10 reported that until the age of 4 1/2 fetal months,
the transverse sinus has a relatively even caliber. At this stage, it begins to
enlarge from its lateral border on each side.
This enlargement or ballooning rapidly progresses medially and
reaches the torcular sinus approximately 1 to 1 1/2 months later. This

10
ballooning is most conspicuous by the 5th fetal month and may further
extend into the posterior portion of the superior sagittal sinus and superior
petrosal sinuses. At the age of 7 fetal months, enlargement of the sinus
practically ceases.
Rapid increase and decrease in the inner diameter of the
transverse sinuses frequently results in irregular inner diameters and
irregular margins of the transverse sinus. Pouches of the dural sinus may
be formed and may extend from the transverse sinus into the convexity
dura or the tentorial dura. These pouches may receive cortical veins from
the convexity or from the undersurface of the temporo-occipital lobes.
Because most of the tentorial venous sinuses encountered in this
study were observed to drain into the torcular herophili, transverse sinus,
and the junction of the transverse sinus and superior petrosal sinus, it is
possible that they may represent outpouching of the transverse sinus10.
Okudera et al. provided an explanation for this occurrence.
Beginning at 4 1/2 to 5 fetal months, the superficial cortical veins of the
expanding cerebral hemispheres rapidly increase in size and drain into the
11
transverse sinus on each side. This corresponds to the period of ballooning
of the transverse sinuses and to the rapid increase in the total blood
draining into the transverse sinuses. On the other hand, the junctional area
of the sigmoid sinus and jugular vein is poorly developed; their inner
diameters range from 1 to 2 mm until the age of 7 fetal months.
The narrow internal lumina of the sigmoid sinuses and the
internal jugular veins, particularly at their junctions (which Okudera et al.
named as the jugular sinuses), results in physiological intraluminal venous
hypertension, secondary ballooning of the transverse sinuses, and
enlargement and some formation of multiple emissary veins for better
extracranial drainage (formation of physiological collateral channels).
The formation of dural outpouches was considered by Okudera
et al.10 as another outcome of ballooning and the later decrease in the
diameter of the transverse sinuses. These dural outpouches may involve
the convexity dura or the tentorium cerebelli.
Therefore, they thought that, in some cases, a cortical vein or veins
indirectly join the transverse sinus through a small tentorial sinus. During
the present study, we noticed several cadavers with outpouching of the

12
transverse sinus into the convexity dura. Most of these outpouchings of
the transverse sinus were located in the medial one-third close to the
torcular sinus. However, there was no apparent relationship between the
outpouching of the transverse sinus and the presence, location, size, or
configuration of the tentorial venous sinuses.
Anatomy of Tentorial venous sinus
Gibbs and Gibbs, in their study on the torcular and lateral sinuses,
seem to have been the first to describe tentorial sinuses. They observed
two sinuses in the tentorium which received blood from the superior
cerebellar veins and emptied into the transverse sinus near the straight
sinus. After their report, the tentorial sinuses were noted in studies of the
dural sinuses near the torcular sinus.
Each half of the tentorium has two constant but rarely
symmetrical venous channels, the medial and lateral tentorial sinuses11.
The medial tentorial sinuses are formed by the convergence of veins from
the superior surface of the cerebellum, and the lateral tentorial sinuses are
formed by the convergence of veins from the basal and lateral surfaces of
the temporal and occipital lobes.

13
The lateral tentorial sinuses arise within the lateral part of the
tentorium and course laterally to drain into the terminal portion of the
transverse sinus. The medial tentorial sinuses course medially to empty
into the straight sinus or the junction of the straight and transverse
sinuses.
Variations of the tentorial sinus in cerebellar tentoria of 13
cadavers were examined under a surgical microscope by Matsushima
et al12 and classified the tentorial sinuses into four groups: Group I, in
which the sinus receives venous blood from the cerebral hemisphere;
Group II, in which the sinus drains the cerebellum; Group III, in which
the sinus originates in the tentorium itself: and Group IV, in which the
sinus originates from a vein bridging to the tentorial free edge. The
tentorial sinuses of Groups I and II were frequently located in the
posterior portion of the tentorium.
The sinuses of Group I were short and most frequently present in
the lateral portion of the tentorium. The tentorial sinuses of Group II,
which were usually large and drained into the dural sinuses near the

14
torcular, were separated into five subtypes according to the draining veins
and direction of termination.
The tentorial sinuses of Groups III and IV were located near the
tentorial free edge or the straight sinus.
Group I: Tentorial sinuses draining the cerebral hemisphere
Several cerebral veins usually converged at the superior surface
of the cerebellar tentorium to form bridging veins. They were frequently
present in the posterolateral part of the tentorium or near the transverse
sinus. Most formed a short tentorial sinus draining into the large dural
sinus, and the rest drained into the sinus through a converging stem vein.
The locations of the sinuses and the converging stem veins were
classified into the medial, middle, and lateral third of the tentorium.
62.2% were situated in the lateral portion of the tentorium. These veins
drained the basal surface of the temporal and occipital lobes, including the
vein of Labb6 from the lateral surface of the temporal lobe.

15
Group II: Tentorial sinus draining the cerebellum
Bridging veins from the cerebellar tentorial surface to the tentorium
often formed a tentorial sinus, which eventually drained into the torcular
or the dural sinus nearby. On the lateral tentorial cerebellar surface, the
inferior and superior hemispheric veins joined and formed bridging veins
to drain into the tentorial sinus. Near the midline, some of the veins
converging in the posterior cerebellar incisura drained into a short
tentorial sinus after forming a bridging vein . Because the tentorial
sinuses of Group II were frequently present as a large sinus, they were
separated into five subtypes according to their draining veins and the
direction of termination .
In Type 1, the sinus courses transversely to drain into the straight
sinus. In Type 2a, the sinus drains the medial cerebellar hemisphere and
courses posteromedially to drain into the torcular sinus. In Type 2b, the
sinus draining the vermis is short and in a manner similar to the Type 2a
sinus. In Type 3, the sinus draining most of the cerebellar hemisphere
courses directly posteriorly to the middle one-third of the transverse sinus.
In Type 4, the sinus drains the lateral tentorial cerebellar surface then runs
posterolaterally to drain into the junction of the superior petrosal and
16
transverse sinuses. All of the Group II tentorial sinuses were present in the
posterior half of the cerebellar tentorium.
The bridging veins draining into the tentorial sinus of Group II
were of two kinds: the vermian bridging vein on the vermis in the midline
and the hemispheric bridging vein located on the lateral cerebellar
surface. Most of the former veins were the terminal portions of the
inferior vermian vein. Hemispheric bridging veins, formed by the joining
of the inferior and superior hemispheric veins, were found in 80% of 20
sides.
These hemispheric bridging veins were less frequently located in the
lateral one-third of the hemisphere than in the middle and medial one-
thirds.
Group III: Tentorial sinus arising in the tentorium
The tentorial sinuses originating in the tentorium were present
near the tentorial free edge or the straight sinus These were small sinuses
with no bridging veins, and drained in two different directions. One type
17
was a tentorial sinus originating from the posterior part of the tentorial
incisura and running anteriorly along the tentorial edge to drain into the
superior petrosal sinus. The other originated near the incisura and ran
posteriorly along the straight sinus to drain into the posterior portion of
the straight sinus or the torcular sinus.
Group IV: Tentorial sinus formed by a bridging vein to the tentorial
free edge
A rarer type of tentorial sinus was described in two cases. In one,
the basal vein of Rosenthal terminated as a bridging vein to the tentorial
free edge, forming a tentorial sinus. The sinus ran posteriorly from the
tentorial edge to the torcular, almost parallel to the straight sinus. In the
other case, the peduncular vein running on the midbrain became a
bridging vein to the tentorial edge forming a short tentorial sinus which
coursed laterally to drain into the superior petrosal sinus.
18
Surgical significance of Tentorial venous sinus The tentorium cerebelli is frequently sectioned to access deep
seated lesions13,14,15. During these procedures, the venous sinuses within
the tentorium might have to be occluded and divided. In most instances,
this occlusion has no adverse consequences because of the inherent
tendency of the venous system to contain collateral pathways.
However, when the main venous channels have been occluded
by disease processes, these sinuses within the tentorium may act as
important collateral channels for venous outflow and, in such
circumstances, occlusion and division of these sinuses may have adverse
consequences.
This has been amply illustrated by a number of case reports.
Browder et al.16 and Kaplan were the first to realize and hypothesize the
importance of the venous channels within the tentorium as potential
collateral pathways when the straight sinus was occluded.

19
In the occipital transtentorial operative approach, the occipital pole
can usually be retracted from the straight sinus and the junction of the falx
and the tentorium without sacrificing any veins to the superior sagittal or
transverse sinuses.
The superior sagittal sinus is commonly devoid of bridging veins
in the area just in front of the torcular herophili, but bridging veins are
encountered if the exposure is directed further forward along the superior
sagittal sinus in the posterior parietal area. The posterior calcarine vein,
which empties into the veins on the lateral surface and into the superior
sagittal sinus 4 to 9 cm proximal to the torcular herophili, is infrequently
encountered in the occipital transtentorial approaches.
However, the anterior calcarine (internal occipital) vein, which
crosses at a much deeper level, frequently blocks access to the
quadrigeminal cistern as it passes from the anterior end of the calcarine
fissure to the great vein, thus making its obliteration unavoidable in
reaching some tumor in the pineal region. Sacrificing the anterior
calcarine vein may cause a homonymous hemianopsia. No bridging veins
pass directly from the occipital lobe to the straight sinus.

20
The medial and lateral tentorial sinuses may be encountered in the
operative approaches in which the tentorium is divided. The medial
tentorial sinus would be encountered in incising the tentorium from
anterior to posterior adjacent to the straight sinus, as might be conducted
in an occipital transtentorial or infratentorial supracerebellar approach.
The lateral tentorial sinus would be encountered in the lateral part of an
incision in the tentorium extending from the free edge toward the
transverse sinus in the area just behind the petrous ridge, as would be
conducted in a subtemporal approach to the front of the brainstem.
The veins that arise on the brainstem and cerebellum and drain into
the superior petrosal sinus are also encountered in sectioning the
anteromedial edge of the tentorium through a subtemporal craniectomy to
expose the trigeminal nerve. The temporobasal bridging veins, which
have relatively strong adhesions to the dura mater of the middle fossa and
the superior surface of the tentorium, could be injured proximal to their
termination during elevation of the temporal lobe in the course of a
subtemporal operative approach to the basal cisterns.
21
Yamamota 17described the advantages of occipital transtentorial
approach over other approaches to pineal region
1. Wide operative field
2. No veins crossing from occipital lobe into superior sagittal sinus
3. Easy visualization of deep venous structure
4. Largely extra-axial above the tentorium
5. Good visualization of ipsilateral dorsal and lateral extension
Ziyal et al reported the combined supra/infratentorial-transsinus
approach is preferred for the resection of certain large pineal region
tumors. During the procedure, the transverse sinus and tentorium were
sectioned after review of preoperative angiographic studies, after taking
intraoperative measurements of the venous pressure in the nondominant
transverse sinus before and after clipping and while monitoring the
somatosensory evoked potentials.
Nagashima et al.18 reported a case of hemangiopericytoma
involving the torcular herophili and the straight sinus. The tumor was
totally resected, with a radial artery graft interposed between the straight

22
sinus and transverse sinus. However, during surgery, they noted swelling
of the occipital lobe even in the presence of a functioning bypass graft.
This swelling eventually necessitated occipital lobectomy.
They suggested that in the presence of occlusion of the torcular
herophili and the straight sinus, the venous channels in the tentorium
might have been the collateral channels and the wide resection of the
tentorium might have caused the brain swelling.
Nakagawa et al.19 reported a case of papillary meningiomas arising
from the confluens of the sinuses, with extension into the sagittal, straight,
and both transverse sinuses. They noted that, in such cases, the normal
hemodynamic state is maintained by collateral circulation through venous
channels in the tentorium and that care needs to be taken not to sacrifice
this collateral circulation.
Odake20 reported two falcotentorial meningiomas with occlusion of
the straight sinus and emphasized the importance of preserving the
collateral venous pathways in the tentorium.

23
Commenting on Odake's article, Morgan also reiterated the
importance of preserving the collateral venous pathways when the major
venous sinuses were occluded21. The importance of these collateral
venous channels in falcotentorial and peritorcular meningiomas has also
been adequately highlighted by several other authors, including Asari
et al.22, Harsh and Wilson , Rostomily et al.23, and Tanaka et al.24.
Piatt repored that simultaneous compromise of the galenic and
tentorial bridging veins and interruption of collateral pathways between
these systems and the petrosal bridging veins, as in the combined
infratentorial supracerebellar / cerebellomedullary fissure approach, may
cause cerebellar venous insufficiency with venous congestion and
possible venous infarction.
Importance of Tentorial sinuses in vascular lesions
The tentorial venous sinuses may have a significant role in certain
vascular diseases of the brain. Girard et al.25 and Lasjaunias et al. noted
that when the vein of Galen was absent, there emerged two distinct
pathways of drainage of the deep venous system, one of which consisted
of the thalamostriate veins draining into the tentorial sinus.
24
While studying the role of dural anomalies in the pathogenesis of
vein of Galen malformations, Lasjaunias et al.26 noted that, in the absence
of a straight sinus, a tentorial sinus often bridges the vein of Galen to the
torcular herophili. This is especially important because of the recent
reports of a high incidence of straight sinus agenesis in vein of Galen
aneurysms and in deep seated cerebral AVMs27.
Raybaud et al.28 reported that in certain patients with vein of Galen
aneurysms, the lateral and sigmoid sinuses were not visualized, and the
blood drained through the tentorial and petrosal sinuses into the cavernous
sinus. Some extrasinusoidal dural AVMs are thought to develop from the
remnants of the tentorial sinuses.
Duckwiler29, Houser et al.30 and Lasjaunias et al. have reported
that the dural AVMs located in the tentorium may drain via the venous
channels in the tentorium.
Zhou et al. reported five cases of tentorial arterio venous fistulas
and classified the tentorial arterio venous fistulas into three types;tentorial
marginal, tentorial medial and tentorial lateral. He considered the tentorial
dural arteriovenous fistulas are aggressive vascular lesions causing SAH

25
and progressive neurologic deficits and need prompt diagnosis and
definite treatment.
The findings of Vidyasagar31 have demonstrated that, in many
AVMs of the brain, there are many venous channels that do not resemble
known anatomic channels. He postulated that these channels are persistent
embryonic veins that do not undergo atresia during development because
of the persistence of flow through them. He reported that in AVMs in the
region of the sylvian fissure, one of the abnormal venous drainage
channels represents the persistent primitive tentorial sinus.
Ruaz et al reported a case of bilateral collateral tentorial venous
sinus drainage of the basal vein (of Rosenthal). The observation was made
on a corrosion cast of the cerebral venous system obtained from a fresh
cadaver. Radiographic correlation was obtained by performing standard
X-ray imaging of the corrosion cast.
During development, the tentorial sinus receives blood from the
developing diencephalon, telencephalon, and mesencephalon. However,
this drainage is later taken over by the basal vein. In AVMs, there may be

26
persistence of these primitive pial veins that may drain into tentorial
sinuses.
Terbrugge and Lasjaunias reported the radiological and anatomic
features of a tentorial venous sinus that they encountered incidentally
during a four-vessel angiogram. This sinus drained the telencephalic and
diencephalic tributaries of the basal vein and eventually emptied into the
straight sinus and the confluence of the sinuses.
They also mentioned that they had encountered eight such cases
in their experience, six cases in angiograms that disclosed nothing
abnormal and two cases in association with cerebral arteriovenous
malformations (AVMs). They noted that these sinuses can have different
posterior openings, i.e., into the straight sinus, the confluens, or the
transverse sinus. The anterior and diencephalic afferents to the basal vein
constitute the usual veins draining into the sinus; however, an
infratemporal vein may also join the sinus.
Kaplan et al.32, in their study of venous channels within the
intracranial dural partitions, noted that, in many instances, natural blood

27
injections were sufficient to demonstrate the course, size, and connections
of the venous channels, particularly in the tentorium cerebelli and falx
cerebri.
They also noted that because three-fourths of the circumference of
the tentorium contained venous channels, venous pathways within the
tentorium cerebelli may be frequently observed connecting the major
sinuses in this region, in patients of all age groups.
They also described a cavernous network of veins within the
dorsal aspect of the tentorium cerebelli in infants that anastomosed with
the larger channels in the tentorium and was maximal near the caudal
straight sinus and adjacent tentorium; during early to midchildhood, these
small vessels apparently dwindle, whereas larger venous channels within
the tentorium persist.
In addition, the tentorial sinuses may serve as important venous
channels that communicate the posterior dural sinuses with the cavernous
sinus. The straight sinus communicates with the cavernous sinus by the
tentorial sinus(straight sinus > tentorial sinus > petrosal sinus > cavernous
sinus).
28
The transverse and sigmoid sinuses may receive direct drainage
from the superficial sylvian vein by way of the tentorial sinus; thus, they
may communicate with the cavernous sinus33. The basal vein may also
drain into the tentorial sinus34.
Tentorial sinuses in congenital malformation
The deep venous system is abnormal in certain congenital
malformations of the brain. Yokota et al.35 and Osaka et al.35 reported that
in holoprosencephaly, diencephalic cysts, and midline porencephalies, the
galenic system is deficient. In such cases, the basal ganglia are drained by
peculiar veins that course laterally and drain into the transverse sinus
through the tentorial sinus35,36.
They considered these to be diencephalic veins that retained their
embryological pattern of drainage (early in development, before the
development of the basal vein, the diencephalic veins drain into the
tentorial sinus). Yokota et al.and Osaka et al. also reported that this type
of deficiency of the deep venous system is absent in other congenital
midline anomalies, such as agenesis of the corpus callosum, and thus
serves to differentiate between the two35,36.

29
Radiological demonstration of Tentorial sinuses
Several angiographic studies described the presence of venous
sinuses in the tentorium37. However, when compared with the high
incidence of venous sinuses in the tentorium as described in anatomic
studies, the number of radiological studies that describe the presence of
these sinuses is disproportionately low.
This apparent discrepancy may be attributable to several reasons
1) the lack of awareness of the presence of these venous sinuses
2) because dural venous sinuses fill from many sources, the venous
sinuses (in venous phase images obtained from any single arterial
injection) may not be opacified because of inflow of unopacified
blood from other vascular territories.
However, recent advances in magnetic resonance venography and
computed tomographic venography may allow a more reliable way of
studying the dural venous sinuses than conventional angiography.
Mattle et al.38 reported that venous sinuses are better visualized on
magnetic resonance venograms. Advances in magnetic resonance

30
venography might allow accurate demonstration of venous sinuses within
the tentorium.
Other noninvasive techniques such as contrast-enhanced
transcranial color-coded real-time sonography may be useful to evaluate
these dural venous sinuses.
Suzuki et al in his study of three-dimensional computed
tomography angiography of the galenic system for the occipital
transtentorial approach,mentioned about various types of tentorial venous
sinus.
Miabi et al.39 studied the lateral tentorial sinus with routine contrast
enhanced MR images in 55 adult patients and reported that it was detected
in 104 of 110 lobes. The lateral tentorial sinus in each lobe was classified
as type I (candelabra) in 30 (28.8%), type II (independent veins) in 22
(21.1%), and type III (venous lakes) in 37 (35.5%); in 15 (14.4%) of the
lobes, the lateral tentorial sinus was indeterminate. Lateral tentorial sinus
branches were inconsistently detected, with the exception of the vein of
Labbé. Five of eight branches were seen in approximately half of the
cases.

31
The vein of Labbé was identified in 94 (85.4%) lobes. Among
these, 53 (56.4%) were draining into the lateral tentorial sinus and 22
(23.4%) into the transverse sinus; in 19 (20.2%) cases, the terminal
portion was not visualized. The right transverse sinus was dominant in 19
(34.5%) patients and the left in 18 (32.7%); codomination was present in
18 (32.7%) cases. At least one arachnoid granulation was seen in the
transverse sinus in 27 (49.1%) patients.
Mapping the temporal venous anatomy is crucial for surgeons
considering lateral skull base explorations. During such operations,
surgeons often manipulate the lateral tentorial sinus and its branches while
lifting up the temporal lobe to achieve adequate exposure and working
space. Surgeons make the best effort to preserve the bridging veins to
avoid a venous infarct. They considered that conventional contrast-
enhanced MR imaging can be used as a tool to evaluate the temporal
venous anatomy.

32
RESULTS
Variations of tentorial venous sinus in cadaver cerebellar tentoria
were examined in 100 autopsy. Venous sinuses were present in tentorium
in 91(91%) cadavers and absent in 9 cadavers. There were 145 tentorial
venous sinuses in 91 cadavers. Of these sinuses, 81 (55.9%) occurred on
left side, 64 (44.1%) occurred on right side.
An imaginary line drawn horizontally at the junction of the superior
petrosal sinus and transverse sinus was used to divide the tentorium
arbitrarily into anterior and posterior portions. And again the tentorium
was arbitrarily divide into medial one-third, middle one-third, lateral one-
third on corresponding to the transverse sinus.
Only one tentorial venous sinus was encountered in the anterior
portion of tentorium cerebelli. The sinuses were bilateral in 33 cadavers
and more than 2 sinuses encountered in 16 cadavers.
The tentorial sinuses were classified into four groups, depending on
their location, size, configuration, and pattern of drainage.

33
Group1: venous sinuses in medial one-third of tentorium cerebelli
Type a: sinuses draining into straight sinus
Type b: sinuses draining into torcular sinus
Type c: sinuses draining into medial one-third of transverse sinus
Group2: venous sinuses in middle one-third of tentorium cerebelli
Group3: venous sinuses in lateral one-third of tentorium cerebelli
Group 4: venous ring pattern
Group1: Venous sinuses in medial one-third of tentorium cerebelli
Group 1 sinuses constituted 47.6% (69 sinuses) of the total
tentorial venous sinuses in this study. Among these sinuses 53.6% (37
sinuses) were on the left side of the tentorium cerebelli and 46.4% (32
sinuses) were on the right side of the tentorium cerebelli. The tentorial
sinuses of Group 1 were frequently present as a large sinus with
occasional branching when compare with other groups.
According to their draining veins they were separated into three
subtypes. In Type a, the sinus courses transversely to drain into the
straight sinus. In Type b, the sinus courses posteromedially to drain into
34
the torcular sinus. In Type c, the sinus drains into the medial one-third of
transverse sinus.
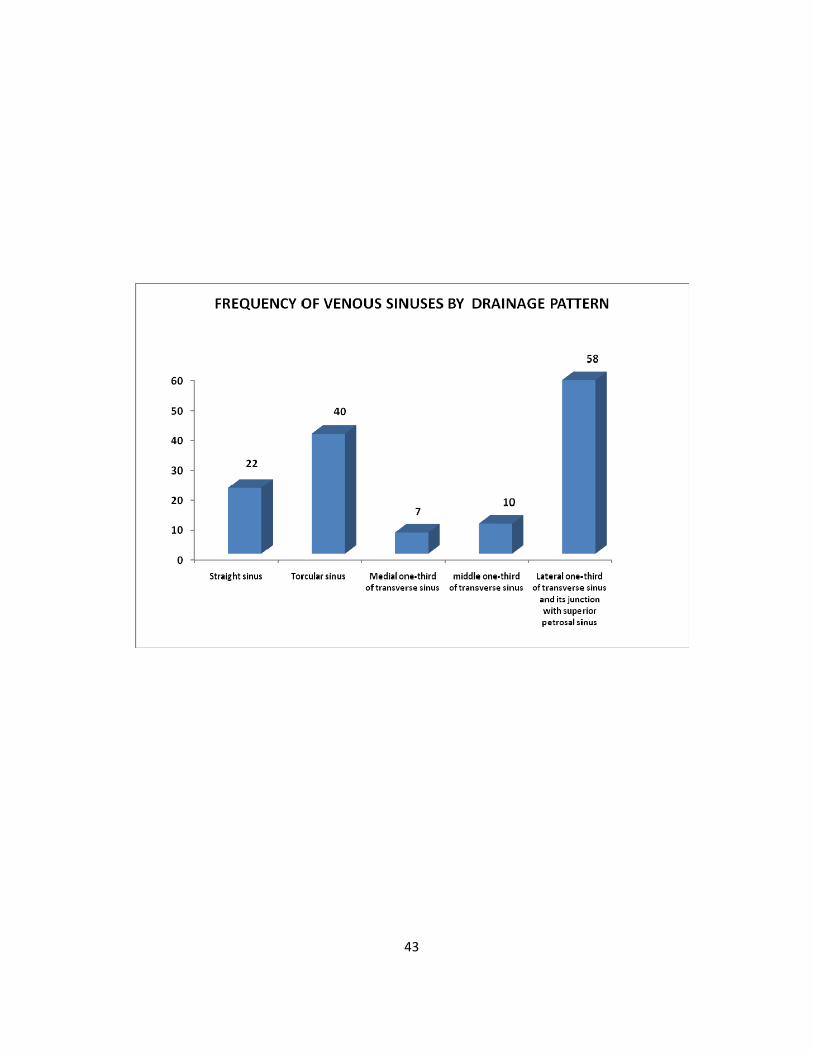
In this study, 22 (32%) sinuses were type a, 40 (58%) sinuses
were type b, 7 (10%) sinuses were type c, among the Group 1 sinuses. Of
these 69 sinuses, 6 sinuses which were longer in size occupying a small
portion of medial part of middle one-third of tentorium cerebelli along
with its course in entire medial one-third of tentorium cerebelli.
Most often Group1 sinuses were drained by the terminal portions
of the cerebellar hemispheric or vermian veins.
Group2: Venous sinuses in middle one-third of tentorium cerebelli
Group 2 sinuses constituted 6.9%(10 sinuses) of the total. Among
these sinuses, two sinuses were on the right side and eight sinuses were on
the left side . All of these sinuses were smaller in size. No branching
pattern was observed in Group 2 sinuses. All of these sinuses were
observed to drain into the middle one-third of the transverse sinus.
Group3: Venous sinuses in lateral one-third of tentorium cerebelli
Group3 sinuses constituted 40% (58 sinuses) of the 145 sinuses in
35
this study. Among these sinuses 55.2% (32 sinuses) were on the left side
and 44.8% (26 sinuses) were on the right side. The tentorial sinuses of
Group 3 were drained into lateral one-third of transverse sinus or to the
junction of the transverse sinus and superior petrosal sinus.
When compare with Group 1 sinuses these sinuses were smaller
and occasionally showing branching pattern like that of the above
mentioned one. Most often these siuses were drained by the the terminal
portions of the cerebral hemispheric veins, frequently by vein of labbe.
Group 4: Venous ring pattern
In six cadavers, there was a large tentorial venous sinus
connecting the torcular sinus to the lateral one-third of transverse sinus or
to the junction of transverse sinus and superior petrosal sinus, thereby
forming a "venous ring". These venous ring was occupying the entire
posterior portion of tentorium cerebelli. This venous ring was bilateral in
two cadavers and unilateral in four cadavers. Among these 8 sinuses(5.5%
of total sinuses), four sinuses(50%) were on the right side of the tentorium
cerebelli and four sinuses(50%) were on the left side of the tentorium
cerebelli.
36
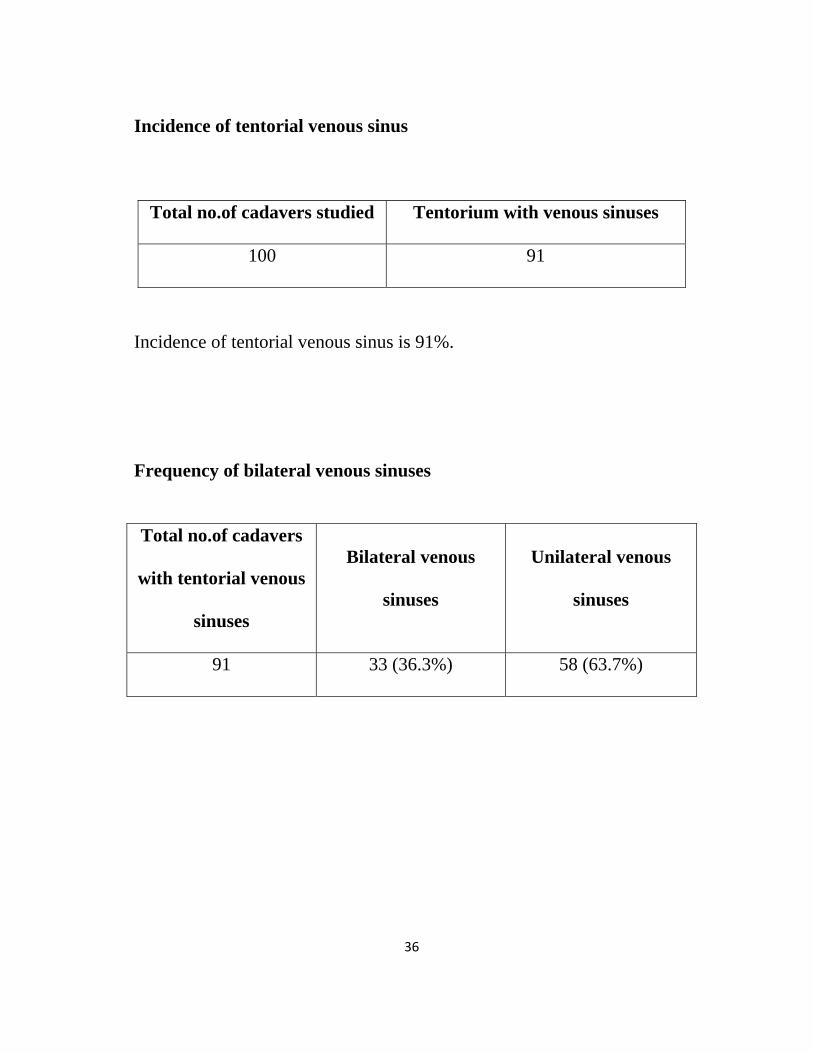
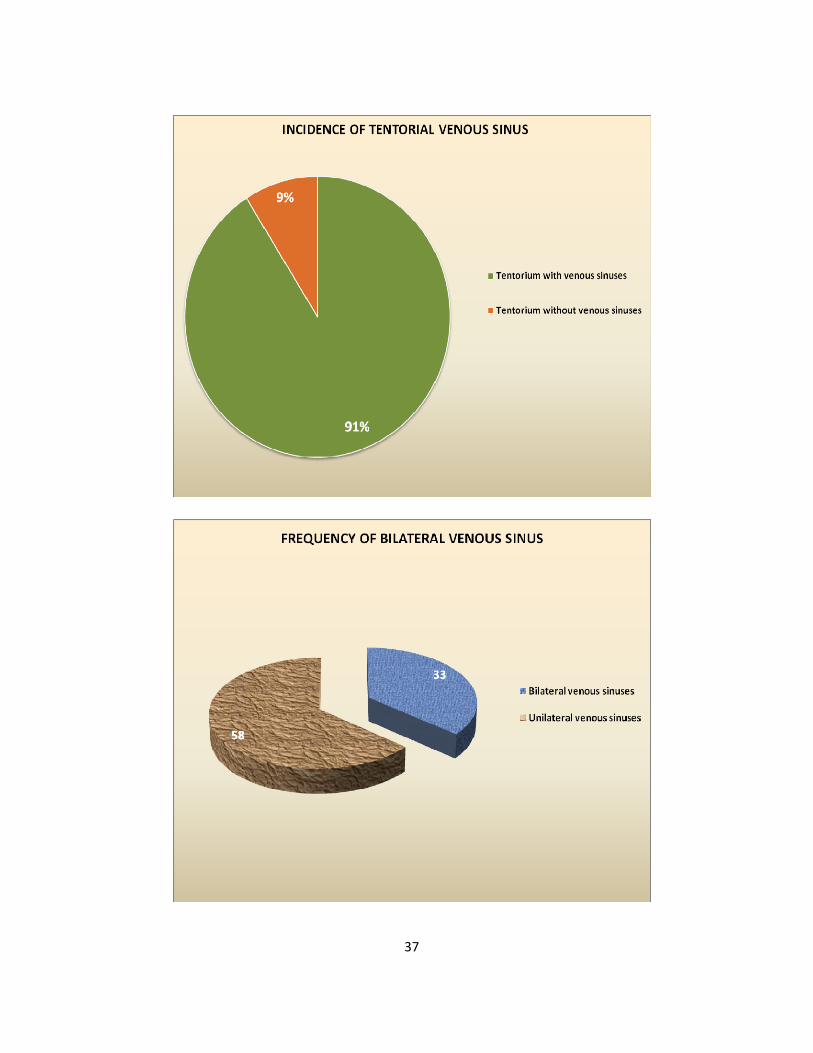
Incidence of tentorial venous sinus
Total no.of cadavers studied Tentorium with venous sinuses
100 91
Incidence of tentorial venous sinus is 91%.
Frequency of bilateral venous sinuses
Total no.of cadavers
with tentorial venous
sinuses
Bilateral venous
sinuses
Unilateral venous
sinuses
91 33 (36.3%) 58 (63.7%)
37
38
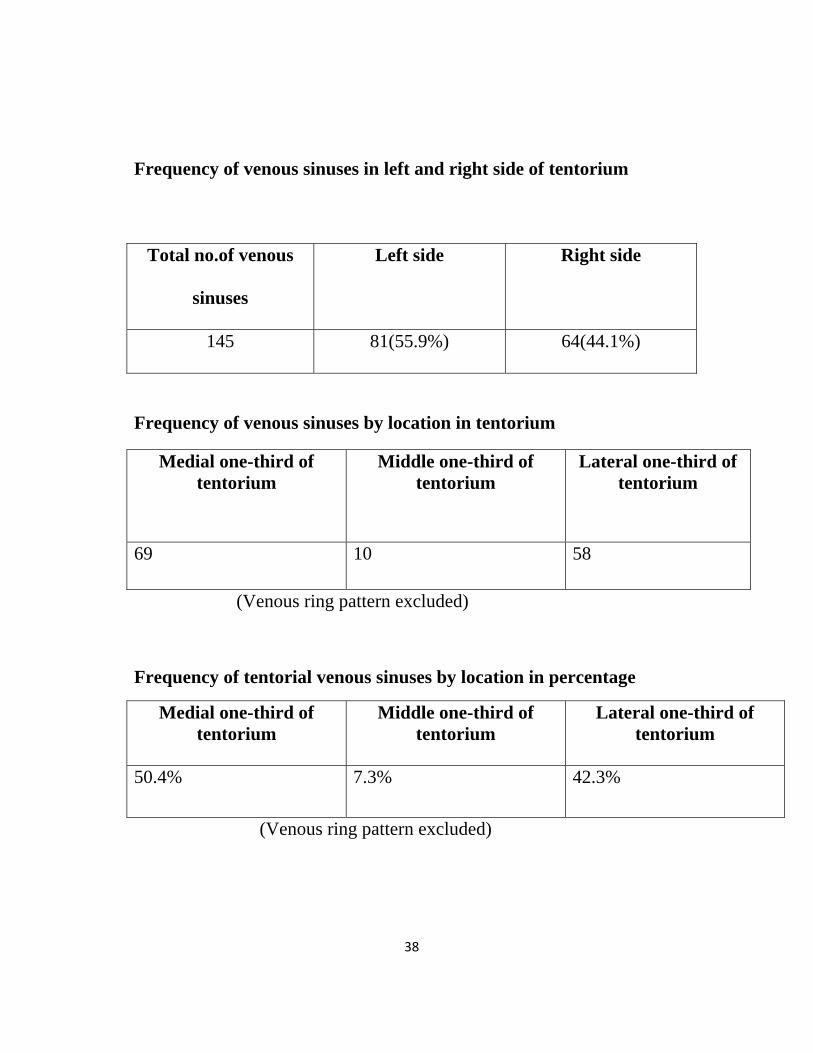
Frequency of venous sinuses in left and right side of tentorium
Total no.of venous
sinuses
Left side Right side
145 81(55.9%) 64(44.1%)
Frequency of venous sinuses by location in tentorium
Medial one-third of tentorium
Middle one-third of tentorium
Lateral one-third of tentorium
69 10 58
(Venous ring pattern excluded)
Frequency of tentorial venous sinuses by location in percentage
Medial one-third of tentorium
Middle one-third of tentorium
Lateral one-third of tentorium
50.4% 7.3% 42.3%
(Venous ring pattern excluded)

39

40
Frequency of each group of venous sinuses
Classification Left side Right side total
Group 1 37 32 69
Group 2 08 02 10
Group 3 32 26 58
Group 4 04 04 08
Total 81 64 145
Frequency of each group of tentorial venous sinuses by percentage
Classification No. of venous sinuses Percentage
Group 1 69 47.6%
Group 2 10 6.9%
Group 3 58 40%
Group 4 08 5.5%

41

42
Frequency of venous sinuses by drainage pattern
Draining sinuses Total no.of tentorial sinuses
Straight sinus 22
Torcular sinus 40
Medial one-third of transverse sinus 07
middle one-third of transverse sinus 10
Lateral one-third of transverse sinus and its junction with superior petrosal sinus
58
(Venous ring pattern excluded)
Frequency of venous sinuses by drainage pattern in percentage
Draining sinuses Percentage
Straight sinus 16.1%
Torcular sinus 29.2%
Medial one-third of transverse sinus 5.1%
middle one-third of transverse sinus 7.3%
Lateral one-third of transverse sinus and its junction with superior petrosal sinus
42.3%
(Venous ring pattern excluded)
43

44
DISCUSSION
Traditionally, anatomists, pathologists, and clinicians have devoted
their attention to the major intracranial venous sinuses. Following in their
footsteps, neurosurgeons have become knowledgeable regarding the size,
course, and tributaries of the major venous sinuses. Knowledge of the
variations of the dural venous sinuses is important to distinguish normal
variations from pathological processes .
However, until recently, venous sinuses in the tentorium cerebelli
received scant attention in the text book of neuroanatomy, neurosurgery
and even in the literature.
Gibbs and Gibbs, in their study on the torcular and lateral sinuses,
seem to have been the first to describe tentorial sinuses. They observed
two sinuses in the tentorium which received blood from the superior
cerebellar veins and emptied into the transverse sinus near the straight
sinus. After their report, the tentorial sinuses were noted in studies of the
dural sinuses near the torcular.
45
Browder et al. studied the presence of venous channels in the
tentorium by injecting a vinylite-acetone mixture and then producing
corrosion casts. They observed that venous channels are extremely
common in the tentorium.
They also noted that, in most instances, the least vascular part of
the tentorium is its middle portion. They suggested that in addition to
phlebographic studies, the presence and the course of these venous
channels could be established intraoperatively by jugular compression.
In his study of the anatomic variations of the venous sinuses in the
region of the torcular herophili, Bisaria40 noted the presence of venous
sinuses within the tentorium cerebelli.
Saxena et al.41 reported that in 10% of healthy patients, the straight
sinus communicates with the lateral sinus by means of tentorial veins.

46
Oka et al.42 reported that each half of the tentorium had two
consistent, but frequently asymmetrical, sinuses, the medial and lateral
tentorial sinuses. The medial sinuses received the superficial veins of the
cerebellum and drained into the junction of the straight and transverse
sinuses, and the lateral tentorial sinuses received the veins of the lateral
surface of the temporal and occipital lobes and drained into the transverse
sinuses.
Variations of the tentorial sinus in cerebellar tentoria of 13
cadavers were examined under a surgical microscope by Matsushima et al
and classified the tentorial sinuses into four groups: Group I, in which the
sinus receives venous blood from the cerebral hemisphere; Group II, in
which the sinus drains the cerebellum; Group III, in which the sinus
originates in the tentorium itself: and Group IV, in which the sinus
originates from a vein bridging to the tentorial free edge. The tentorial
sinuses of Groups I and II were frequently located in the posterior portion
of the tentorium.
The sinuses of Group I were short and most frequently present in
the lateral portion of the tentorium. The tentorial sinuses of Group II,
47
which were usually large and drained into the dural sinuses near the
torcular, were separated into five subtypes according to the draining veins
and direction of termination.
The tentorial sinuses of Groups III and IV were located near the
tentorial free edge or the straight sinus.
In their study, venous sinuses were present in all of the 13 tentoria
studied; Group II sinuses were the most frequent, with Group I being the
next most frequent. Group I sinuses were predominantly located in lateral
one-third of tentorium cerebelli, but the Group II sinuses were less
frequently located in the lateral one-third of the tentorium cerebelli than in
the middle and medial one-thirds.
Koperna et al.43 studied the termination of Labbé's vein and observed
that in 73% of the cases, Labbé's vein reaches the transverse sinus through
a tentorial sinus. Information about the termination of the inferior
anastomotic vein of Labbé is of crucial importance in the subtemporal
neurosurgical approach and its modifications. By dissecting the vein of

48
Labbé out of its dural bed and shifting its fixation point, microsurgical
access is facilitated considerably.
Duval et al. studied 23 cadavers using a retrograde veinous
injection of a mixture of Rhodopas and lead tetroxide and observed that
the tentorial sinus was present in more than half of the cases and
considered this sinus as a true sinus, principally draining the superior and
inferior hemispheric veins of the cerebellum. He also noted the tentorial
sinus traversed the posterior portion of the tentorium cerebelli and opened
into the lateral or straight sinus.
Muthukumar et al.1 studied cerebellar tentoria in 80 cadavers and
reported that the tentorium cerebelli was revealed to contain sinuses in
86% of the cadavers. He classified the sinuses into the following three
types:
Type I sinuses constituted 25% of the total and were most often
located in the medial one-third of the tentorium. They were larger than the
other types, frequently occurring with a branching "stag-horn"

49
configuration and a tendency to drain into the straight sinus, the torcular
herophili, and the medial one-third of the transverse sinus.
Type II sinuses constituted 25% of the total and were most often
located in the lateral one-third of the tentorium. They were smaller than
the other types, and tended to drain into the duction of the transverse sinus
and superior petrosal sinus and into the lateral one-third of the transverse
sinus.
Type III sinuses constituted 50% of the total and were located in
the medial one-third of the tentorium. Their size ranged from small to
medium. Unlike Type I sinuses, no branching pattern was observed.
These sinuses tended to drain into the straight sinus, the torcular herophili,
and the medial one-third of the transverse sinus.
He considered, the medial one-third of the tentorium was the most
vascular part. No venous sinus was observed in the anterior part of the
tentorium in his study. He observed the venous ring pattern in three
cadavers.
Jin et al44 in his study of the normal variation of tentorial sinuses
draining into the straight sinus in 50 cadavers reported that tentorial

50
venous sinuses present in 29(58%) cadavers and absent in 21(42%)
cadavers.
He divided the draining site of the tentorial sinuses at the straight
sinus into 3 zones : Zone 1, anterior one third of the straight sinus, into
which 15 out of 63 tentorial sinuses were found to be drained, zone 2
which is the most prevalent site, middle one third of the straight sinus
draining 27 out of 63 tentorial sinuses and zone 3, posterior one third of
the straight sinus draining 21 out of 63 tentorial sinuses.
In this present study, tentorial venous sinus was present in 91 (91%)
cadavers and absent in 9 cadavers. It is bilateral in 33 cadavers and more
than two sinuses were present in 16 cadavers. The incidence of tentorial
venous sinus is more when compare with the studies of Muthukumar et al
(86%) Duval et al and Jin et al (58%) and less with the studies of
Matsushima et al (100%).
Comparison of Incidence of Tentorial venous Sinus
Present study Muthukumar et al Jin et al Matsushima et al
91% 86% 58% 100%

51

52
The incidence of tentorial venous sinuses in left side (55.9%) is
more than the right side(44.1%).
In this study, 50.4% of tentorial venous sinuses are located in
medial one-third of tentorium cerebelli, 7.3% in middle one-third of
tentorium cerebelli,42.3% in lateral one-third of tentorium cerebelli. But
in the study of Muthukumar 69.3% of tentorial venous sinuses are located
in medial one-third of tentorium cerebelli, 8.6% in middle one-third of
tentorium cerebelli, 22.1% in lateral one-third of tentorium.
Comparison of Venous sinuses by location
Studies
Medial
one –third of
tentorium
Middle
one-third of
tentorium
Lateral
one-third of
tentorium
Present study 50.4% 7.3% 42.3%
Muthukumar et al 69.3% 8.6% 22.1%

53

54
Miabi et al in his study of lateral tentorial sinus with routine
contrast enhanced MR images in 55 adult patients, reported that it was
detected in 104 of 110 lobes.
The incidence of tentorial venous sinuses located in lateral one-
third of tentorium cerebelli in this study is almost twice that of
Muthukumar et al study.
In this study, the middle one-third of tentorium cerebelli is found to
be least vascular.
55
CONCLUSION
1. The incidence of tentorial venous sinus in this cadaveric study is
91%.
2. Depending on their location,size,configuration, and pattern of
drainage, the tentorial venous sinuses are classified into four groups
3. Group1: venous sinuses in medial one-third of tentorium
cerebelli
Type a: sinuses draining into straight sinus
Type b: sinuses draining into torcular sinus
Type c: sinuses draining into medial one-third of transverse
sinus
Group2: venous sinuses in middle one-third of tentorium
cerebelli
Group3: venous sinuses in lateral one-third of tentorium
cerebelli
Group 4: venous ring pattern
4. 50.4% of tentorial venous sinuses are located in medial one-third of
tentorium cerebelli, 7.3% in middle one-third of tentorium

56
cerebelli, 42.3% in lateral one-third of tentorium cerebelli. (venous
ring pattern is excluded)
5. Middle one-third of tentorium cerebelli is the least vascular portion.
6. These findings will be useful for procedures that require sectioning
of the tentorium.
7. These sinuses serve as important collateral channels when the
straight sinus or torcular herophili is occluded by pathological
processes.
8. They also play an important role in several vascular and congenital
malformations of the brain.

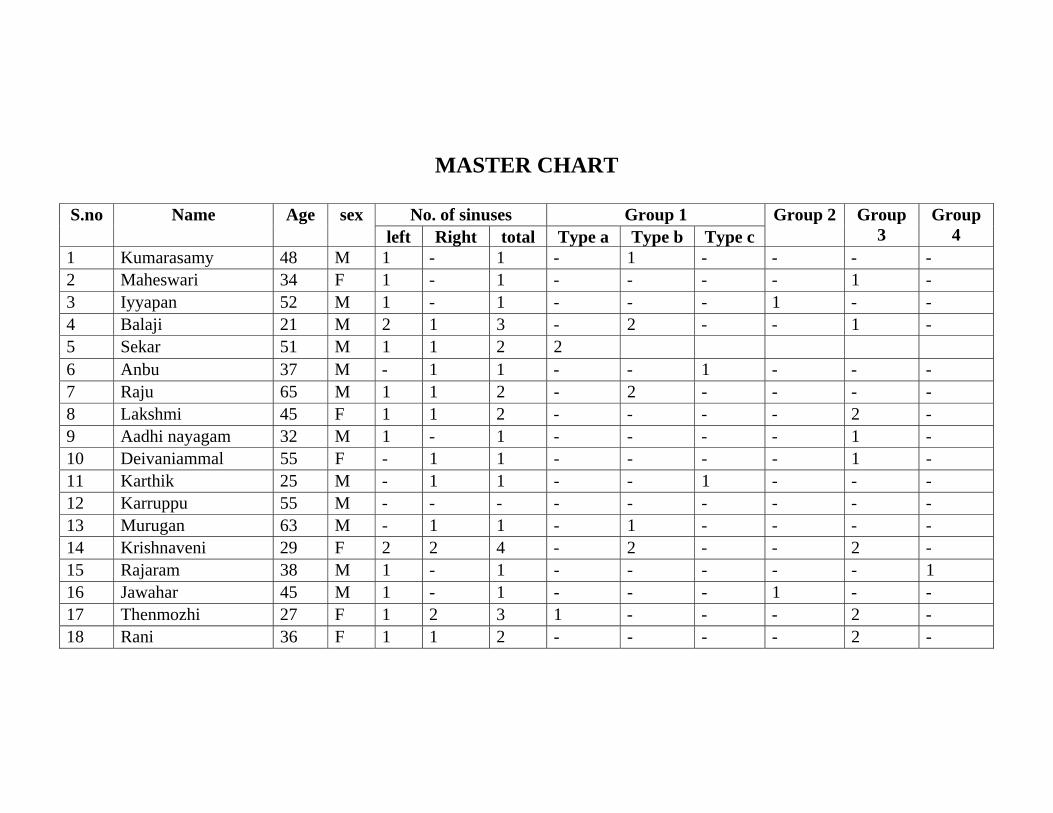
MASTER CHART
S.no Name Age sex No. of sinuses Group 1 Group 2 Group 3
Group 4 left Right total Type a Type b Type c
1 Kumarasamy 48 M 1 - 1 - 1 - - - - 2 Maheswari 34 F 1 - 1 - - - - 1 - 3 Iyyapan 52 M 1 - 1 - - - 1 - - 4 Balaji 21 M 2 1 3 - 2 - - 1 - 5 Sekar 51 M 1 1 2 2 6 Anbu 37 M - 1 1 - - 1 - - - 7 Raju 65 M 1 1 2 - 2 - - - - 8 Lakshmi 45 F 1 1 2 - - - - 2 - 9 Aadhi nayagam 32 M 1 - 1 - - - - 1 - 10 Deivaniammal 55 F - 1 1 - - - - 1 - 11 Karthik 25 M - 1 1 - - 1 - - - 12 Karruppu 55 M - - - - - - - - - 13 Murugan 63 M - 1 1 - 1 - - - - 14 Krishnaveni 29 F 2 2 4 - 2 - - 2 - 15 Rajaram 38 M 1 - 1 - - - - - 1 16 Jawahar 45 M 1 - 1 - - - 1 - - 17 Thenmozhi 27 F 1 2 3 1 - - - 2 - 18 Rani 36 F 1 1 2 - - - - 2 -

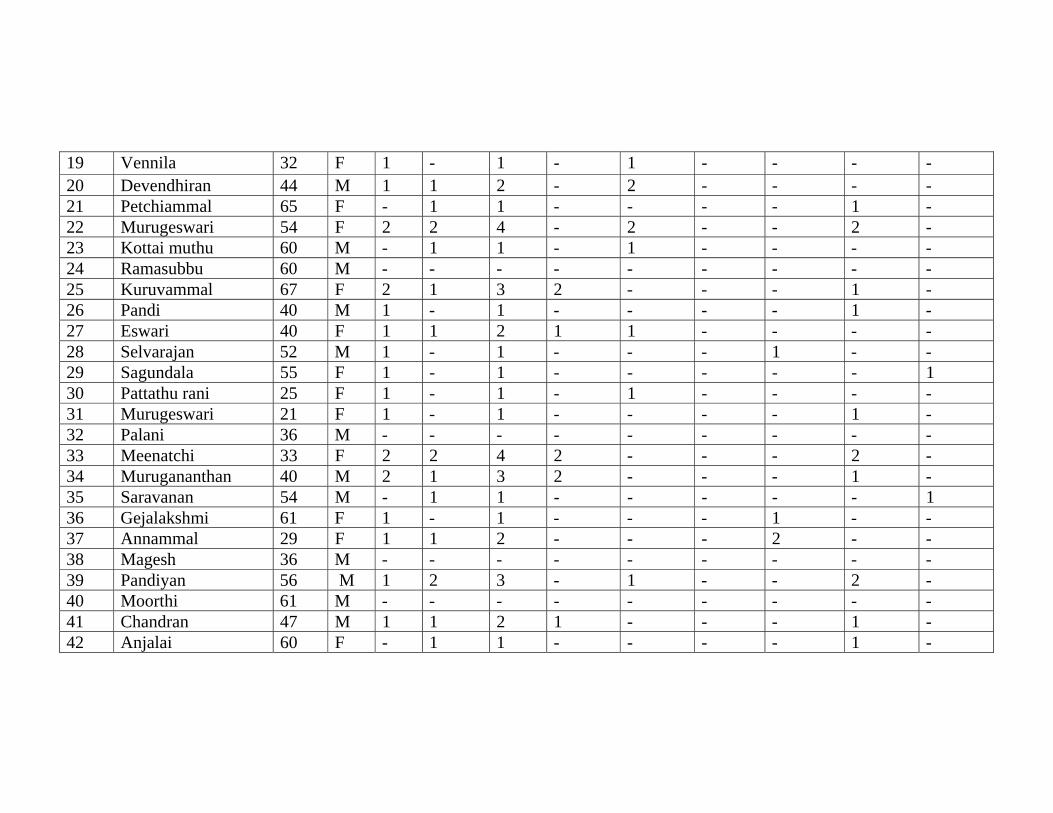
19 Vennila 32 F 1 - 1 - 1 - - - - 20 Devendhiran 44 M 1 1 2 - 2 - - - - 21 Petchiammal 65 F - 1 1 - - - - 1 - 22 Murugeswari 54 F 2 2 4 - 2 - - 2 - 23 Kottai muthu 60 M - 1 1 - 1 - - - - 24 Ramasubbu 60 M - - - - - - - - - 25 Kuruvammal 67 F 2 1 3 2 - - - 1 -26 Pandi 40 M 1 - 1 - - - - 1 - 27 Eswari 40 F 1 1 2 1 1 - - - - 28 Selvarajan 52 M 1 - 1 - - - 1 - -29 Sagundala 55 F 1 - 1 - - - - - 1 30 Pattathu rani 25 F 1 - 1 - 1 - - - - 31 Murugeswari 21 F 1 - 1 - - - - 1 - 32 Palani 36 M - - - - - - - - - 33 Meenatchi 33 F 2 2 4 2 - - - 2 - 34 Murugananthan 40 M 2 1 3 2 - - - 1 - 35 Saravanan 54 M - 1 1 - - - - - 1 36 Gejalakshmi 61 F 1 - 1 - - - 1 - -37 Annammal 29 F 1 1 2 - - - 2 - - 38 Magesh 36 M - - - - - - - - - 39 Pandiyan 56 M 1 2 3 - 1 - - 2 -40 Moorthi 61 M - - - - - - - - - 41 Chandran 47 M 1 1 2 1 - - - 1 - 42 Anjalai 60 F - 1 1 - - - - 1 -

43 Papa 58 F 1 - 1 - - 1 - - - 44 Rajagopal 53 M 1 1 2 1 1 - - - - 45 Palanivel 46 M 2 1 3 - 2 - - 1 - 46 Gurusamy 66 M 1 - 1 - - - - 1 - 47 Ibrahim 30 M 1 - 1 - 1 - - - - 48 Kumaresan 59 M 1 1 2 1 - - - 1 -49 Latha 36 F - 1 1 - - - - 1 - 50 Kuppammal 65 F 1 - 1 - 1 - - - - 51 Vellayan 68 M 2 2 4 - 2 - - 2 - 52 Raman 68 M 2 1 3 - 1 - - 2 - 53 Ganesan 42 M - - - - - - - - - 54 Uma 38 F 1 1 2 - 1 - - 1 - 55 Loganayaki 65 F - 1 1 - - - - 1 - 56 Babu 41 M 1 - 1 - - - - 1 - 57 Sagayam 48 M 1 1 2 - - - 2 - - 58 Rajalakshmi 30 F 1 - 1 1 - - - - - 59 Indirani 47 F 1 - 1 - - - 1 - -60 Akilandam 60 F 1 - 1 - - 1 - - - 61 Perumol 65 M 1 2 3 2 - - - 1 - 62 Suseela 22 F - 1 1 - 1 - - - - 63 Balakrishnan 70 M 1 - 1 - - - - 1 - 64 Chinnasamy 46 M 1 1 2 - 2 - - - - 65 Mumthajbanu 45 F - 1 1 - 1 - - - - 66 Kalidoss 52 M 2 2 4 2 - - - 2 -
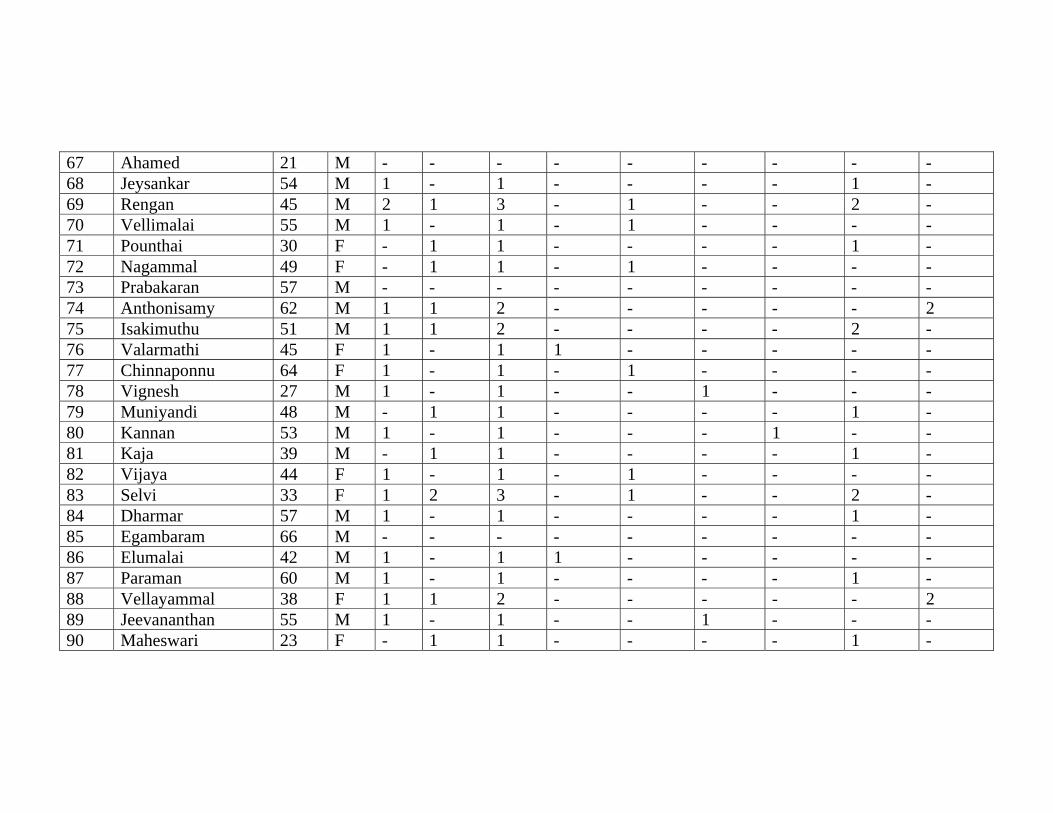
67 Ahamed 21 M - - - - - - - - - 68 Jeysankar 54 M 1 - 1 - - - - 1 - 69 Rengan 45 M 2 1 3 - 1 - - 2 - 70 Vellimalai 55 M 1 - 1 - 1 - - - - 71 Pounthai 30 F - 1 1 - - - - 1 - 72 Nagammal 49 F - 1 1 - 1 - - - -73 Prabakaran 57 M - - - - - - - - - 74 Anthonisamy 62 M 1 1 2 - - - - - 2 75 Isakimuthu 51 M 1 1 2 - - - - 2 - 76 Valarmathi 45 F 1 - 1 1 - - - - - 77 Chinnaponnu 64 F 1 - 1 - 1 - - - - 78 Vignesh 27 M 1 - 1 - - 1 - - - 79 Muniyandi 48 M - 1 1 - - - - 1 - 80 Kannan 53 M 1 - 1 - - - 1 - - 81 Kaja 39 M - 1 1 - - - - 1 - 82 Vijaya 44 F 1 - 1 - 1 - - - - 83 Selvi 33 F 1 2 3 - 1 - - 2 -84 Dharmar 57 M 1 - 1 - - - - 1 - 85 Egambaram 66 M - - - - - - - - - 86 Elumalai 42 M 1 - 1 1 - - - - - 87 Paraman 60 M 1 - 1 - - - - 1 - 88 Vellayammal 38 F 1 1 2 - - - - - 2 89 Jeevananthan 55 M 1 - 1 - - 1 - - - 90 Maheswari 23 F - 1 1 - - - - 1 -
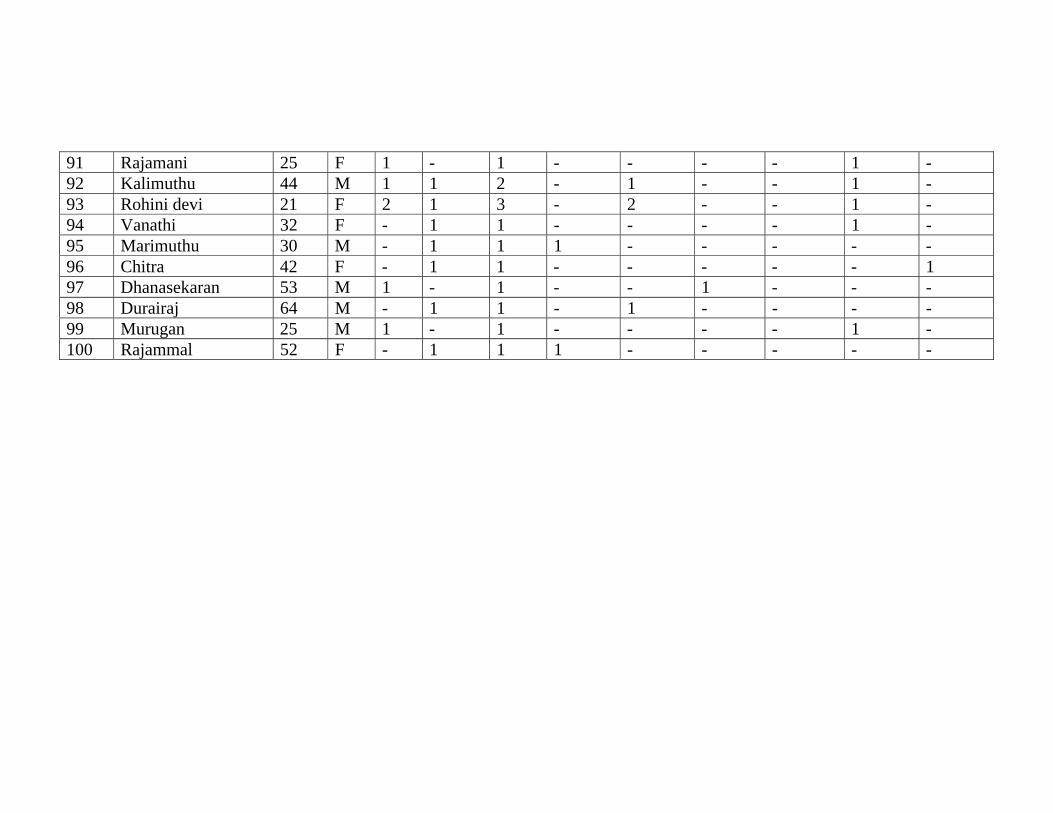
91 Rajamani 25 F 1 - 1 - - - - 1 - 92 Kalimuthu 44 M 1 1 2 - 1 - - 1 - 93 Rohini devi 21 F 2 1 3 - 2 - - 1 - 94 Vanathi 32 F - 1 1 - - - - 1 - 95 Marimuthu 30 M - 1 1 1 - - - - - 96 Chitra 42 F - 1 1 - - - - - 197 Dhanasekaran 53 M 1 - 1 - - 1 - - - 98 Durairaj 64 M - 1 1 - 1 - - - - 99 Murugan 25 M 1 - 1 - - - - 1 - 100 Rajammal 52 F - 1 1 1 - - - - -
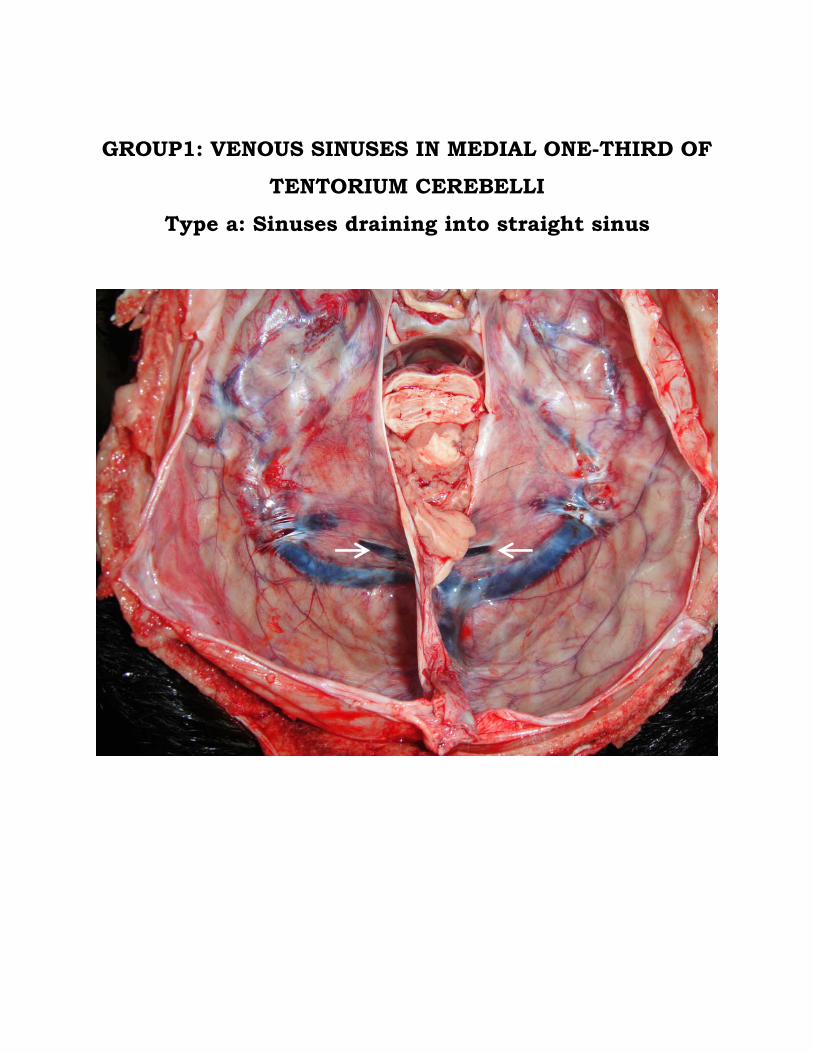
GROUP1: VENOUS SINUSES IN MEDIAL ONE-THIRD OF TENTORIUM CEREBELLI
Type a: Sinuses draining into straight sinus

GROUP1: VENOUS SINUSES IN MEDIAL ONE-THIRD OF
TENTORIUM CEREBELLI Type b: Sinuses draining into torcular sinus
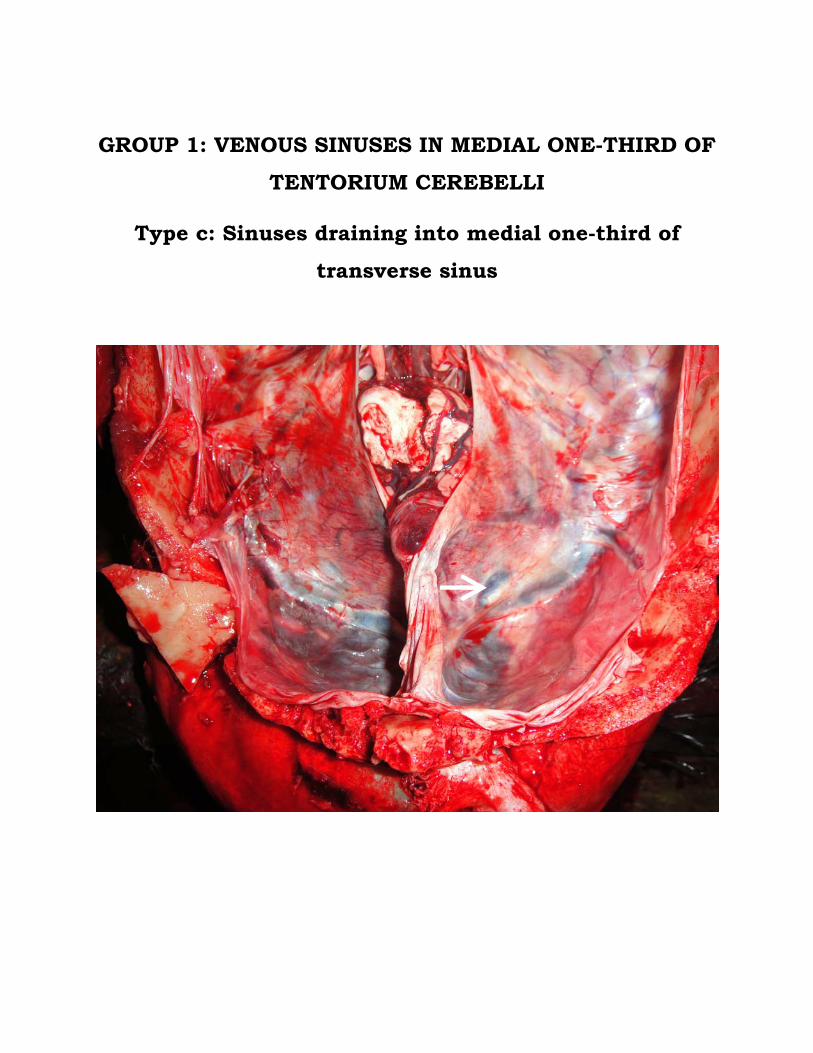
GROUP 1: VENOUS SINUSES IN MEDIAL ONE-THIRD OF
TENTORIUM CEREBELLI
Type c: Sinuses draining into medial one-third of transverse sinus

GROUP 2: VENOUS SINUSES IN MIDDLE ONE-THIRD OF
TENTORIUM CEREBELLI
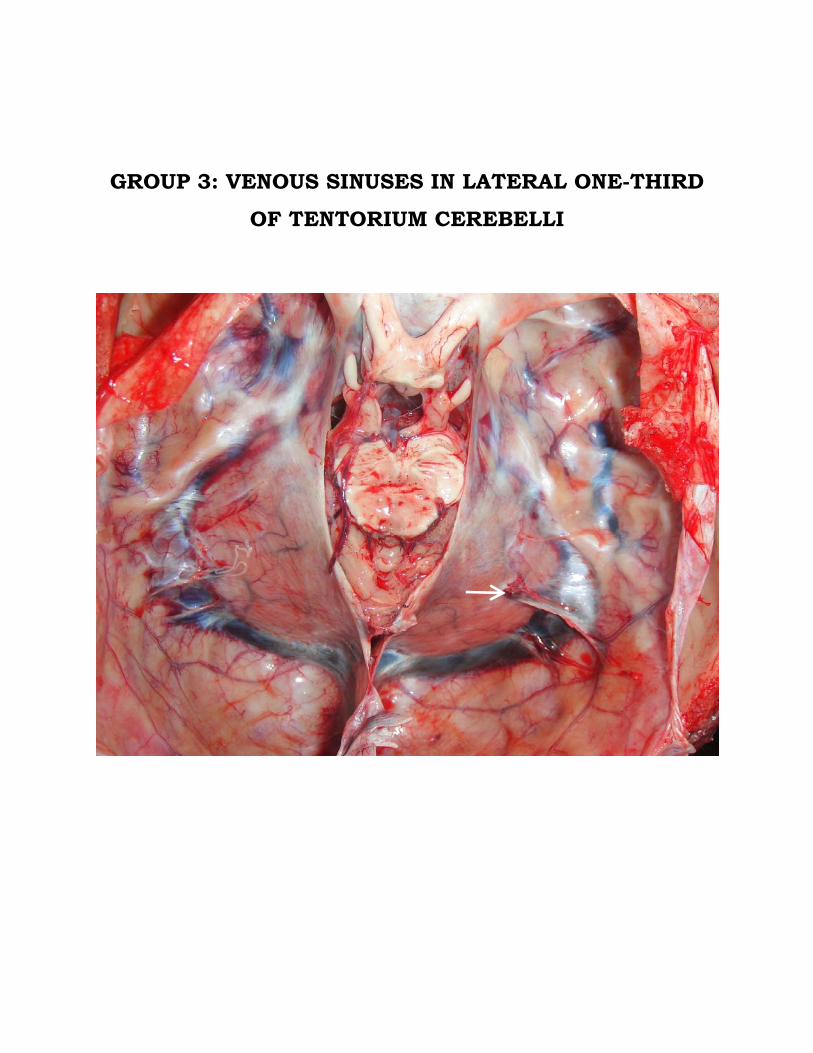
GROUP 3: VENOUS SINUSES IN LATERAL ONE-THIRD
OF TENTORIUM CEREBELLI
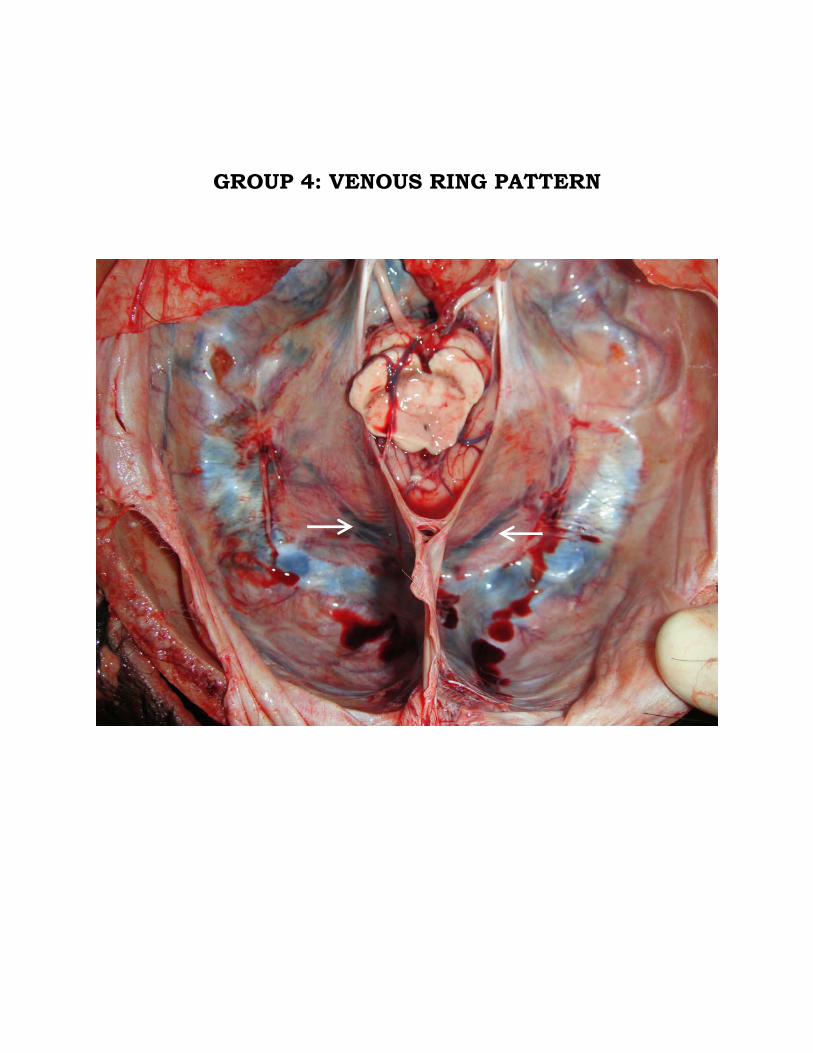
GROUP 4: VENOUS RING PATTERN
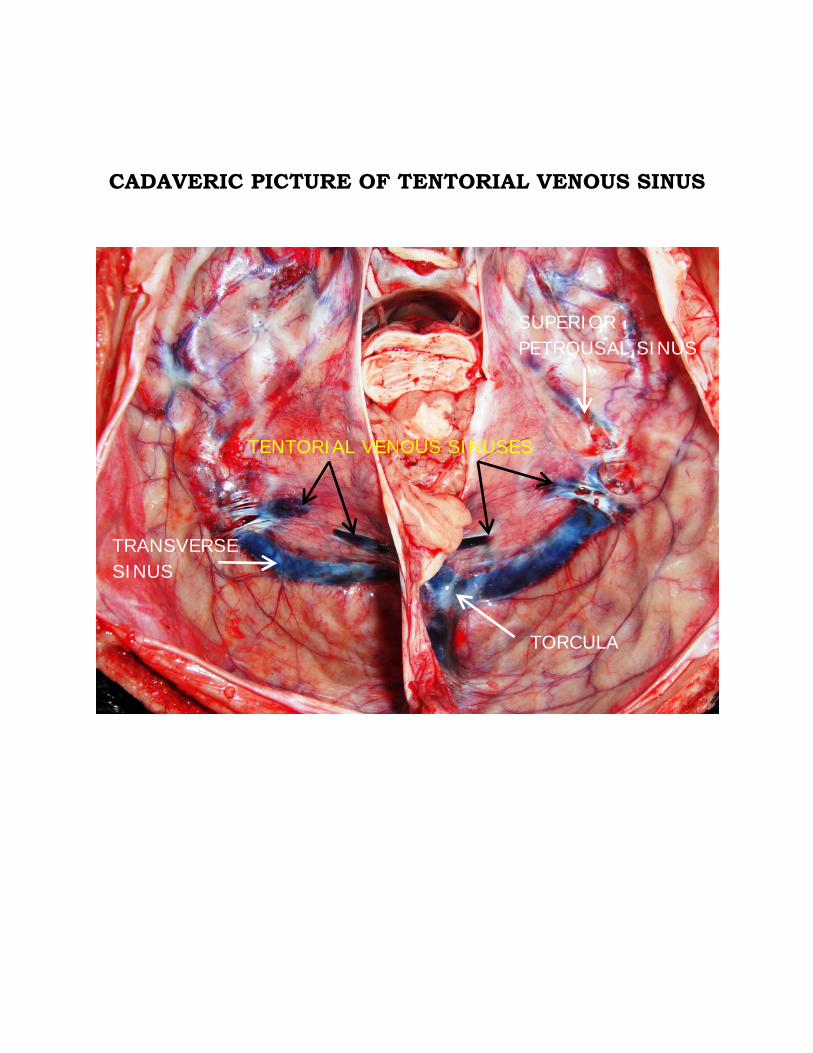
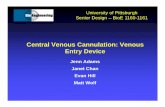
CADAVERIC PICTURE OF TENTORIAL VENOUS SINUS
TORCULA
TRANSVERSE SINUS
SUPERIOR PETROUSAL SINUS
TENTORIAL VENOUS SINUSES
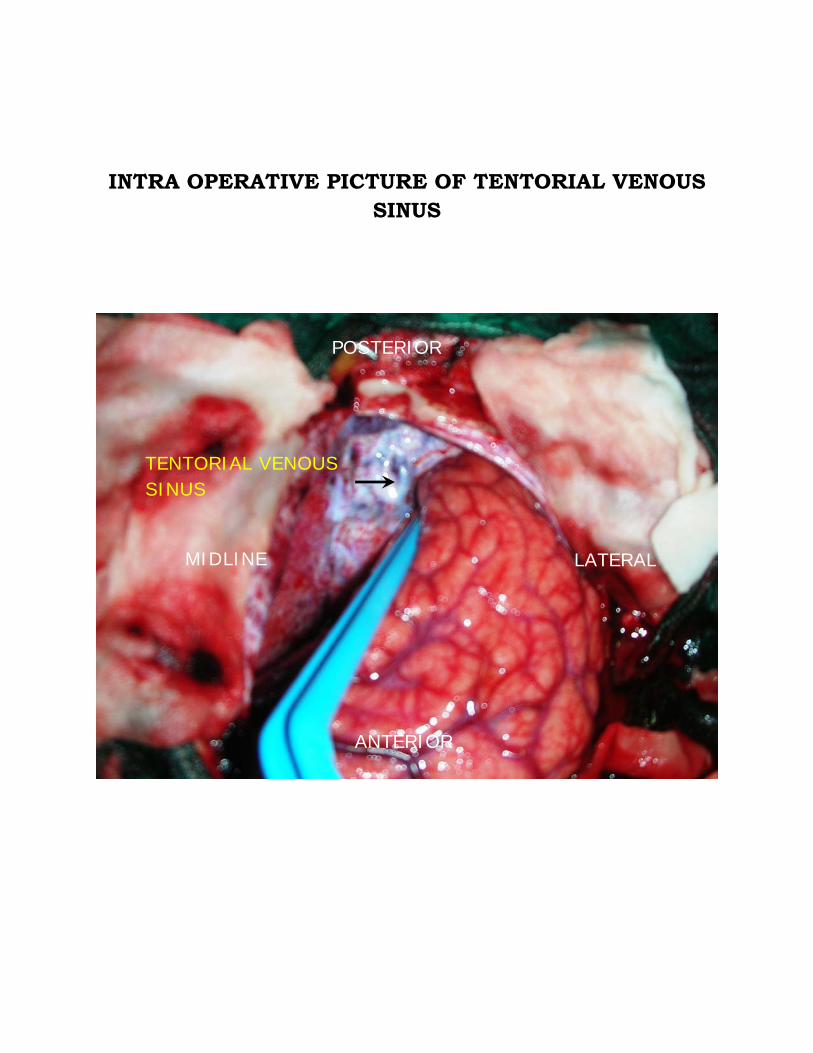
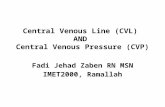
INTRA OPERATIVE PICTURE OF TENTORIAL VENOUS SINUS
POSTERIOR
MIDLINE LATERAL
ANTERIOR
TENTORIAL VENOUS SINUS
MASTER CHART
S.no Name Age sex No. of sinuses Group 1 Group 2 Group 3
Group 4 left Right total Type a Type b Type c
1 Kumarasamy 48 M 1 - 1 - 1 - - - - 2 Maheswari 34 F 1 - 1 - - - - 1 - 3 Iyyapan 52 M 1 - 1 - - - 1 - - 4 Balaji 21 M 2 1 3 - 2 - - 1 - 5 Sekar 51 M 1 1 2 2 6 Anbu 37 M - 1 1 - - 1 - - - 7 Raju 65 M 1 1 2 - 2 - - - - 8 Lakshmi 45 F 1 1 2 - - - - 2 - 9 Aadhi nayagam 32 M 1 - 1 - - - - 1 - 10 Deivaniammal 55 F - 1 1 - - - - 1 - 11 Karthik 25 M - 1 1 - - 1 - - - 12 Karruppu 55 M - - - - - - - - - 13 Murugan 63 M - 1 1 - 1 - - - - 14 Krishnaveni 29 F 2 2 4 - 2 - - 2 - 15 Rajaram 38 M 1 - 1 - - - - - 1 16 Jawahar 45 M 1 - 1 - - - 1 - - 17 Thenmozhi 27 F 1 2 3 1 - - - 2 - 18 Rani 36 F 1 1 2 - - - - 2 -
19 Vennila 32 F 1 - 1 - 1 - - - - 20 Devendhiran 44 M 1 1 2 - 2 - - - - 21 Petchiammal 65 F - 1 1 - - - - 1 - 22 Murugeswari 54 F 2 2 4 - 2 - - 2 - 23 Kottai muthu 60 M - 1 1 - 1 - - - - 24 Ramasubbu 60 M - - - - - - - - - 25 Kuruvammal 67 F 2 1 3 2 - - - 1 -26 Pandi 40 M 1 - 1 - - - - 1 - 27 Eswari 40 F 1 1 2 1 1 - - - - 28 Selvarajan 52 M 1 - 1 - - - 1 - -29 Sagundala 55 F 1 - 1 - - - - - 1 30 Pattathu rani 25 F 1 - 1 - 1 - - - - 31 Murugeswari 21 F 1 - 1 - - - - 1 - 32 Palani 36 M - - - - - - - - - 33 Meenatchi 33 F 2 2 4 2 - - - 2 - 34 Murugananthan 40 M 2 1 3 2 - - - 1 - 35 Saravanan 54 M - 1 1 - - - - - 1 36 Gejalakshmi 61 F 1 - 1 - - - 1 - -37 Annammal 29 F 1 1 2 - - - 2 - - 38 Magesh 36 M - - - - - - - - - 39 Pandiyan 56 M 1 2 3 - 1 - - 2 -40 Moorthi 61 M - - - - - - - - - 41 Chandran 47 M 1 1 2 1 - - - 1 - 42 Anjalai 60 F - 1 1 - - - - 1 -

43 Papa 58 F 1 - 1 - - 1 - - - 44 Rajagopal 53 M 1 1 2 1 1 - - - - 45 Palanivel 46 M 2 1 3 - 2 - - 1 - 46 Gurusamy 66 M 1 - 1 - - - - 1 - 47 Ibrahim 30 M 1 - 1 - 1 - - - - 48 Kumaresan 59 M 1 1 2 1 - - - 1 -49 Latha 36 F - 1 1 - - - - 1 - 50 Kuppammal 65 F 1 - 1 - 1 - - - - 51 Vellayan 68 M 2 2 4 - 2 - - 2 - 52 Raman 68 M 2 1 3 - 1 - - 2 - 53 Ganesan 42 M - - - - - - - - - 54 Uma 38 F 1 1 2 - 1 - - 1 - 55 Loganayaki 65 F - 1 1 - - - - 1 - 56 Babu 41 M 1 - 1 - - - - 1 - 57 Sagayam 48 M 1 1 2 - - - 2 - - 58 Rajalakshmi 30 F 1 - 1 1 - - - - - 59 Indirani 47 F 1 - 1 - - - 1 - -60 Akilandam 60 F 1 - 1 - - 1 - - - 61 Perumol 65 M 1 2 3 2 - - - 1 - 62 Suseela 22 F - 1 1 - 1 - - - - 63 Balakrishnan 70 M 1 - 1 - - - - 1 - 64 Chinnasamy 46 M 1 1 2 - 2 - - - - 65 Mumthajbanu 45 F - 1 1 - 1 - - - - 66 Kalidoss 52 M 2 2 4 2 - - - 2 -

67 Ahamed 21 M - - - - - - - - - 68 Jeysankar 54 M 1 - 1 - - - - 1 - 69 Rengan 45 M 2 1 3 - 1 - - 2 - 70 Vellimalai 55 M 1 - 1 - 1 - - - - 71 Pounthai 30 F - 1 1 - - - - 1 - 72 Nagammal 49 F - 1 1 - 1 - - - -73 Prabakaran 57 M - - - - - - - - - 74 Anthonisamy 62 M 1 1 2 - - - - - 2 75 Isakimuthu 51 M 1 1 2 - - - - 2 - 76 Valarmathi 45 F 1 - 1 1 - - - - - 77 Chinnaponnu 64 F 1 - 1 - 1 - - - - 78 Vignesh 27 M 1 - 1 - - 1 - - - 79 Muniyandi 48 M - 1 1 - - - - 1 - 80 Kannan 53 M 1 - 1 - - - 1 - - 81 Kaja 39 M - 1 1 - - - - 1 - 82 Vijaya 44 F 1 - 1 - 1 - - - - 83 Selvi 33 F 1 2 3 - 1 - - 2 -84 Dharmar 57 M 1 - 1 - - - - 1 - 85 Egambaram 66 M - - - - - - - - - 86 Elumalai 42 M 1 - 1 1 - - - - - 87 Paraman 60 M 1 - 1 - - - - 1 - 88 Vellayammal 38 F 1 1 2 - - - - - 2 89 Jeevananthan 55 M 1 - 1 - - 1 - - - 90 Maheswari 23 F - 1 1 - - - - 1 -

91 Rajamani 25 F 1 - 1 - - - - 1 - 92 Kalimuthu 44 M 1 1 2 - 1 - - 1 - 93 Rohini devi 21 F 2 1 3 - 2 - - 1 - 94 Vanathi 32 F - 1 1 - - - - 1 - 95 Marimuthu 30 M - 1 1 1 - - - - - 96 Chitra 42 F - 1 1 - - - - - 197 Dhanasekaran 53 M 1 - 1 - - 1 - - - 98 Durairaj 64 M - 1 1 - 1 - - - - 99 Murugan 25 M 1 - 1 - - - - 1 - 100 Rajammal 52 F - 1 1 1 - - - - -

BIBLIOGRAPHY
1. Muthukumar N, Palaniappan P. Tentorial Venous Sinuses: An
Anatomic Study.Neurosurgery. 1998 Feb;42(2):363-71 .
2. Gibbs EL, Gibbs FA: The cross section areas of the vessels that
form the torcular and the manner in which flow is distributed to the
right and to the left lateral sinus. Anat Rec 59:419-426, 1934.
3. Bull JW: Tentorium cerebelli. Proc R Soc Med 62:1301–1310,
1969.
4. Winslow J B (1732) Expositicn Anatomique de la Structure du
Corps Humain. Paris
5. Rhoton AL Jr. Tentorial incisura. Neurosurgery. 2000 Sep; 47(3
Suppl):S131-53.
6. Ono M, Ono M, Rhoton AL Jr, Barry M. Microsurgical anatomy of
the region of the tentorial incisura. J Neurosurg. 1984
Feb;60(2):365-99.
7. Plaut hf. Size of the tentorial incisura related to cerebral herniation.
Acta Radiol Diagn (Stockh). 1963 May;1:916-28.
8. Padget DH: The cranial venous system in man in reference to
development, adult configuration, and relation to arteries. Am J
Anat 98:307-355, 1956.
9. Lasjaunias P, Raybaud C: Intracranial venous system, in Lasjaunias
P, Bernstein A (eds): Surgical Neuroangiography. New York,
Springer-Verlag, 1993, vol 3, pp 223-245.
10. Okudera T, Huang YP, Ohta T, Yokota A, Nakamura Y, Maehara
F, Utsunomiya H, Uemura K, Fukasawa H: Development of
posterior fossa dural sinuses, emissary veins, and jugular bulb:
Morphological and radiologic study. AJNR Am J Neuroradiol
15:1871-1883, 1994.
11. Rhoton AL Jr:Cerebral veins. Neurosurgery 51[Suppl 1]: 159–205,
2002.
12. Matsushima T, Suzuki SO, Fukui M, Rhoton AL Jr, Oliveira ED,
Ono M: Microsurgical anatomy of the tentorial sinuses. J
Neurosurg 71:923-928, 1989.
13. Al-Mefty O, Fox JL, Smith RR: Petrosal approach for petroclival
meningiomas. Neurosurgery 22:51-57, 1988.
14. Hakuba A, Nishimura S, Inoue Y: Transpetrosal-transtentorial
approach and its application in the therapy of retrochiasmatic
craniopharyngiomas. Surg Neurol 24:405-415, 1985.
15. Kawase T, Shiobara R, Toya S: Anterior transpetrosal-transtentorial
approach for sphenopetroclival meningiomas: Surgical methods
and results in 10 patients. Neurosurgery 28:868-876, 1991.
16. Browder J, Kaplan HA, Krieger AJ: Venous lakes in the
suboccipital dura mater and falx cerebelli of infants: Surgical
significance.Surg Neurol 4:53-55, 1975.
17. Yamamoto I, Pineal region tumor: surgical anatomy and approach.
Journal of Neuro-Oncology 54: 263–275, 2001.
18. Nagashima H, Kobayashi S, Takemae T, Tanaka Y: Total resection
of torcular herophili hemangiopericytoma with radial artery graft:
Case report. Neurosurgery 36:1024-1027, 1995.
19. Nakagawa H, Nakajima S, Murasawa A, Niiyama K, Ishiguro S:
Papillary meningioma arising from the confluens sinuum with
multidirectional extension through venous sinuses. Surg Neurol
32:219-224,1989.
20. Odake G: Meningioma of the falcotentorial region: Report of two
cases and literature review of occlusion of the galenic
system.Neurosurgery 30:788-794, 1992.
21. Morgan MK: Meningioma of the falcotentorial region: Report of
two cases and literature review of occlusion of the galenic system.
Neurosurgery 30:794, 1992 (comment).
22. Asari S, Maeshiro T, Tomita S, Kawauchi M, Yabuno N, Kinugasa
K, Ohmoto T: Meningiomas arising from the falcotentorial
junction: Clinical features, neuroimaging studies, and surgical
treatment. J Neurosurg 82:726-738, 1995.
23. Rostomily RC, Eskridge JM, Winn HR: Tentorial meningiomas.
Neurosurg Clin N Am 5:331-348,1994.
24. Tanaka Y, Sugita K, Kobayashi S, Hongo K: Straight sinus
meningioma. Surg Neurol 24:550-554,1985.
25. Girard N, Lasjaunias P, Taylor W: Reversible tonsillar prolapse in
vein of Galen aneurismal malformations: Report of eight cases and
pathophysiological hypothesis. Childs Nerv Syst 10:141-47,1994.
26. Lasjaunias P, Ter Brugge K, Lopez Ibor L, Chiu M, Flodmark O,
Chuang S, Goasguen J: The role of dural anomalies in Vein of

Galen aneurysms: Report of six cases and review of the
literature.AJNR Am J Neuroradiol 8:185-192, 1987.
27. Minakawa T, Tanaka R, Koike T, Takeuchi S, Abe H: Cerebral
arteriovenous malformations associated with straight sinus
anomaly.Neurosurgery 31:19-24, 1992.
28. Raybaud CA, Strother CM, Hald JK: Aneurysms of the vein of
Galen: Embryonic considerations and anatomical features relating
to the pathogenesis of the malformation. Neuroradiology 31:109-
128,1989.
29. Duckwiler G: Dural arteriovenous fistula. Neuroimaging Clin N
Am 2:291-302, 1992.
30. Houser WO, Baker HL, Rhoton AL Jr, Okazaki H: Intracranial
dural arteriovenous malformations. Radiology 105:55-64, 1972.
31. Vidyasagar C: Persistent embryonic veins in arteriovenous
malformations of the brain. Acta Neurochir (Wien) 40:103-116,
1978.
32. Kaplan HA, Browder J, Kreiger AJ: Venous channels within the
intracranial dural partitions. Radiology 115:641-645, 1975.

33. Raybaud CA, Strother CM, Hald JK: Aneurysms of the vein of
Galen: Embryonic considerations and anatomical features relating
to the pathogenesis of the malformation. Neuroradiology 31:109-
128,1989.
34. Cure JK, Van Tassel P, Smith MT: Normal and variant anatomy of
the dural venous sinuses. Semin Ultrasound CT MR 15:499-519,
1994.
35. Yokota A, Oota T, Matsukado Y, Okudera T: Structures and
development of the venous system in congenital malformations of
the brain. Neuroradiology 16:26-30, 1978.
36. Osaka K, Sato S, Yamasaki S, Fujita K, Matsumoto S, Kodama S:
Dysgenesis of the deep venous system as a diagnostic criterion for
holoprosencephaly. Neuroradiology 13:231-238, 1977.
37. Huang YP, Okudera T, Ohtal T, Robbins A: The torcular, the
straight, sagittal, lateral, occipital and tentorial sinuses: The
variations and clinical significance, in Kapp JP, Schmideck HH
(eds):The Cerebral Venous System and Its Disorders. Orlando,
Grune & Stratton, 1984, pp 109-167.
38. Mattel HP, Wentz KU, Edelman RR, Wallner B, Fenn JP, Barnes P,
Atkinson DJ, Kleefield J, Hoogewoud HM: Cerebral venography
with MR. Radiology 178:453-458, 1991
39. Miabi Z: Delineation of lateral tentorial sinus with contrast-
enhanced MR imaging and its surgical implications. AJNR Am J
Neuroradiol. 25(7):1181-8, 2004.
40. Bisaria KK: Anatomic variations of the venous sinuses in the
region of the torcular herophili. J Neurosurg 62:90-95, 1985.
41. Saxena RC, Beg MAQ, Das AC: Double straight sinus: Report of
six cases. J Neurosurg 39:540-542,1973.
42. Oka K, Rhoton AL Jr, Barry M, Rodriguez R: Microsurgical
anatomy of the superficial veins of the cerebrum.Neurosurgery
17:711-748, 1985.
43. Koperna TH, Tschabitscher M, Knosp E: The termination of the
vein of Labbe and its microsurgical significance. Acta Neurochir
(Wien) 118:172-175, 1992.
44. Jin DK, Yoon SH, Choi JU, Lee HY, Chung IH:
The Normal Variation of Tentorial Sinuses Draining into the
Straight Sinus. J Korean Neurosurg Soc. 1994 Jun;23(6): 681-684.