Anatomic and Microbiologic Challenges to Achieving Success ... · Anatomic and Microbiologic...
6
Anatomic and Microbiologic Challenges to Achieving Success with Endodontic Treatment: A Case Report Domenico Ricucci, MD, DDS,* and José F. Siqueira Jr, DDS, MSc, PhD † Abstract This article describes a case of persistent apical peri- odontitis that required several nonsurgical and surgical approaches for resolution. A 28-year-old woman pre- sented with a large symptomatic apical periodontitis lesion associated with the maxillary left lateral incisor that persisted in spite of previous nonsurgical and surgical endodontic treatment. Root canal retreatment was accomplished, but the lesion only showed a slight decrease in size after 18 months. Forty-six months after retreatment, the patient returned because of reemer- gence of symptoms. Radiographically, the lesion re- mained relatively unaltered. Periradicular resurgery was performed, and a biopsy specimen consisting of the lesion and the apical part of the root was collected for analysis. Radiographic and clinical reevaluation after 4 years revealed complete healing. Histopathologic and histobacteriologic observations demonstrated that the lesion was a cyst, and that the probable reason for failure was the occurrence of bacteria within dentinal tubules and in a lateral canal slightly coro- nal to the amalgam root-end filling. This case report clearly illustrates the difficulties imposed by ana- tomic complexities in attaining a disinfection level that is compatible with periradicular tissue healing. (J Endod 2008;34:1249 –1254) Key Words Apical periodontitis, endodontic infection, periradicular surgery, root canal retreatment E radication or at least reduction of the microbial burden in the root canal system has been regarded as essential to the success of both nonsurgical and surgical endodon- tic treatment (1, 2). Despite meticulous canal cleaning, shaping, disinfection, and obturation, endodontic treatment might still fail in some cases, and the causes for the unsuccessful outcome are mostly related to bacterial persistence in the apical canal in areas unaffected by treatment procedures (3, 4). In this regard, anatomic irregularities and/or pathologic entities such as calcifications might hinder the ability to achieve the desired treatment goals (4–6). This article describes several nonsurgical and surgical attempts to treat a tooth with persistent apical periodontitis. This clinical case typically exemplifies the limita- tions imposed by anatomic complexities in achieving adequate disinfection during nonsurgical root canal treatment. Case Report A 28-year-old woman was referred from a general clinician who had performed periradicular surgery for “removal of a cyst” around the root apices of the maxillary left lateral and central incisors. Two months after surgery, the patient presented with severe pain and swelling in the vestibule. Oral examination revealed vestibular swelling as well as a scar on the mucosa as a result of previous surgery (Fig. 1A). Radiographic analysis showed that the left lateral and central incisors had been subjected to both nonsurgical and surgical endodontic procedures. Amalgam root-end fillings were present, and a large radiolucency encompassed both root ends and extended to the adjacent left canine (Fig. 1B). The canine responded to sensitivity testing (thermal and electric pulp tests) within normal limits. Both left lateral and central incisors were tender to percus- sion and palpation and exhibited mobility grade 1. The patient was taking amoxicillin (2 g per day) for the current distress. Clinically, the soft tissue swelling was nonfluctuant and not amenable to incision and drainage, and continuation of the antibiotic therapy was considered. One week later, the patient was asymptomatic, and decision was made to nonsurgically re-treat the lateral incisor because the lesion was mostly centered around its root apex, whereas the apex of the central incisor was only partly involved. In addition, the quality of previous treatment in the lateral incisor was apparently low. Therefore, it appeared reasonable that the lesion was maintained by the lateral incisor. The tooth was isolated with a rubber dam, the canal was accessed, and gutta- percha filling was removed with hand instruments. Working length was established to the root-end filling (Fig. 1C), and the canal was cleaned and shaped with Gates-Glidden burs and Hedström files. Three bigger file sizes were used after the first instrument that fit at the working length. Accordingly, the final file used for apical preparation at the working length was a #100 K-file. Irrigation was carried out with 1% sodium hypochlo- rite (NaOCl). The canal was then filled with chemically pure calcium hydroxide powder and temporized with IRM (Dentsply DeTrey GmbH, Konstanz, Germany). Three weeks later, calcium hydroxide was removed, and the canal was cleaned and medicated once again as before. This approach was repeated 2 more times until the patient was symptom-free. After 75 days of calcium hydroxide medication, the canal was instrumented once again and filled with laterally compacted gutta-percha and sealer (Fig. 1D). During retreatment, a portion of the amalgam root-end filling was slightly displaced into the periradicular tissues. Finally, the tooth crown was restored with composite resin. The patient was reexamined after 6 months, and the tooth was comfortable. At the 18-month follow-up examination, the radiolucency had slightly decreased in size and From *Private practice, Rome, Italy; and † Department of Endodontics, Faculty of Dentistry, Estácio de Sá University, Rio de Janeiro, Brazil. Address requests for reprints to Dr Domenico Ricucci, Piazza Calvario 7, 87022 Cetraro (CS), Italy. E-mail address: [email protected]. 0099-2399/$0 - see front matter Copyright © 2008 American Association of Endodontists. doi:10.1016/j.joen.2008.07.002 Case Report/Clinical Techniques JOE — Volume 34, Number 10, October 2008 Persistent Infection Leading to Failure 1249
Transcript of Anatomic and Microbiologic Challenges to Achieving Success ... · Anatomic and Microbiologic...

ASD
AToasltswdrgmplayhtfdnctt(
KAs
Ed
Pd0
d
Case Report/Clinical Techniques
J
natomic and Microbiologic Challenges to Achievinguccess with Endodontic Treatment: A Case Reportomenico Ricucci, MD, DDS,* and José F. Siqueira Jr, DDS, MSc, PhD†
Etouaad
wtn
plpasalcts(ncniaT
ptbfwra
api(dc
bstracthis article describes a case of persistent apical peri-dontitis that required several nonsurgical and surgicalpproaches for resolution. A 28-year-old woman pre-ented with a large symptomatic apical periodontitisesion associated with the maxillary left lateral incisorhat persisted in spite of previous nonsurgical andurgical endodontic treatment. Root canal retreatmentas accomplished, but the lesion only showed a slightecrease in size after 18 months. Forty-six months afteretreatment, the patient returned because of reemer-ence of symptoms. Radiographically, the lesion re-ained relatively unaltered. Periradicular resurgery was
erformed, and a biopsy specimen consisting of theesion and the apical part of the root was collected fornalysis. Radiographic and clinical reevaluation after 4ears revealed complete healing. Histopathologic andistobacteriologic observations demonstrated thathe lesion was a cyst, and that the probable reasonor failure was the occurrence of bacteria withinentinal tubules and in a lateral canal slightly coro-al to the amalgam root-end filling. This case reportlearly illustrates the difficulties imposed by ana-omic complexities in attaining a disinfection levelhat is compatible with periradicular tissue healing.J Endod 2008;34:1249 –1254)
ey Wordspical periodontitis, endodontic infection, periradicularurgery, root canal retreatment
From *Private practice, Rome, Italy; and †Department ofndodontics, Faculty of Dentistry, Estácio de Sá University, Rioe Janeiro, Brazil.
Address requests for reprints to Dr Domenico Ricucci,iazza Calvario 7, 87022 Cetraro (CS), Italy. E-mail address:[email protected]/$0 - see front matter
Copyright © 2008 American Association of Endodontists.oi:10.1016/j.joen.2008.07.002
1
OE — Volume 34, Number 10, October 2008
radication or at least reduction of the microbial burden in the root canal system hasbeen regarded as essential to the success of both nonsurgical and surgical endodon-
ic treatment (1, 2). Despite meticulous canal cleaning, shaping, disinfection, andbturation, endodontic treatment might still fail in some cases, and the causes for thensuccessful outcome are mostly related to bacterial persistence in the apical canal inreas unaffected by treatment procedures (3, 4). In this regard, anatomic irregularitiesnd/or pathologic entities such as calcifications might hinder the ability to achieve theesired treatment goals (4 – 6).
This article describes several nonsurgical and surgical attempts to treat a toothith persistent apical periodontitis. This clinical case typically exemplifies the limita-
ions imposed by anatomic complexities in achieving adequate disinfection duringonsurgical root canal treatment.
Case ReportA 28-year-old woman was referred from a general clinician who had performed
eriradicular surgery for “removal of a cyst” around the root apices of the maxillary leftateral and central incisors. Two months after surgery, the patient presented with severeain and swelling in the vestibule. Oral examination revealed vestibular swelling as wells a scar on the mucosa as a result of previous surgery (Fig. 1A). Radiographic analysishowed that the left lateral and central incisors had been subjected to both nonsurgicalnd surgical endodontic procedures. Amalgam root-end fillings were present, and aarge radiolucency encompassed both root ends and extended to the adjacent leftanine (Fig. 1B). The canine responded to sensitivity testing (thermal and electric pulpests) within normal limits. Both left lateral and central incisors were tender to percus-ion and palpation and exhibited mobility grade 1. The patient was taking amoxicillin2 g per day) for the current distress. Clinically, the soft tissue swelling was nonfluctuant andot amenable to incision and drainage, and continuation of the antibiotic therapy wasonsidered. One week later, the patient was asymptomatic, and decision was made toonsurgically re-treat the lateral incisor because the lesion was mostly centered around
ts root apex, whereas the apex of the central incisor was only partly involved. Inddition, the quality of previous treatment in the lateral incisor was apparently low.herefore, it appeared reasonable that the lesion was maintained by the lateral incisor.
The tooth was isolated with a rubber dam, the canal was accessed, and gutta-ercha filling was removed with hand instruments. Working length was established to
he root-end filling (Fig. 1C), and the canal was cleaned and shaped with Gates-Gliddenurs and Hedström files. Three bigger file sizes were used after the first instrument that
it at the working length. Accordingly, the final file used for apical preparation at theorking length was a #100 K-file. Irrigation was carried out with 1% sodium hypochlo-
ite (NaOCl). The canal was then filled with chemically pure calcium hydroxide powdernd temporized with IRM (Dentsply DeTrey GmbH, Konstanz, Germany).
Three weeks later, calcium hydroxide was removed, and the canal was cleanednd medicated once again as before. This approach was repeated 2 more times until theatient was symptom-free. After 75 days of calcium hydroxide medication, the canal was
nstrumented once again and filled with laterally compacted gutta-percha and sealerFig. 1D). During retreatment, a portion of the amalgam root-end filling was slightlyisplaced into the periradicular tissues. Finally, the tooth crown was restored withomposite resin.
The patient was reexamined after 6 months, and the tooth was comfortable. At the
8-month follow-up examination, the radiolucency had slightly decreased in size andPersistent Infection Leading to Failure 1249
wowc
tr
Fsrmistf
Case Report/Clinical Techniques
1
as focused almost exclusively on the lateral incisor; however, marginsf the original radiolucency were now well-delimited and accentuatedith a heavy sclerotic, radiopaque line (Fig. 1E). The patient was en-
A
D E
G H
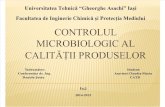
igure 1. Patient presenting with a flare-up 2 months after periradicular surgerhows a large apical periodontitis lesion. Both central and lateral incisors hadetreatment was performed in the lateral incisor, with the working length establedication. Note that the amalgam root-end filling was slightly displaced into the
n size but now exhibited sclerotic margins. The tooth was asymptomatic. (F) Tevere pain. (G) Radiograph showing that lesion size remained substantially unhe apical portion with the lesion attached to it was resected and submitted to fuollow-up radiograph shows healing of the apical periodontitis lesion.
ouraged to return for further yearly evaluations. r
250 Ricucci and Siqueira
Twenty-eight months later (46 months after retreatment), the pa-ient returned because of abscess formation in the previously operatedegion (Fig. 1F). A radiograph showed that the lesion size had remained
C
I
removal of a cyst”. (A) A linear scar is evident on the mucosa. (B) Radiographpicoectomized, and amalgam root-end fillings were present. (C) Nonsurgical
at the root-end filling. (D) Root canal filling after 75 days of calcium hydroxidedicular tissues. (E) Eighteen-month follow-up evaluation. The lesion decreasedears and 10 months after retreatment, the patient presented with swelling andd when compared with (E). (H) Periradicular resurgery was performed, andnalysis. A new retrocavity was prepared and filled with amalgam. (I) Four-year
B
F
y “forbeen aishedperirahree yaltere
rther a
elatively unaltered (Fig. 1G). The patient was given an additional
JOE — Volume 34, Number 10, October 2008

cst
mrrThpn
T
bofwpthaiuuhmtwtrdt
H
Bna2c
(tvbc
doAIe3a
paOc
tadBie(tctpb
pdspc(itfbvhf
smhadrilHelsirptcbt
ciblrldagr(tp
Case Report/Clinical Techniques
J
ourse of amoxicillin. Incision for drainage was not necessary becausepontaneous drainage was evident at that point. After remission of symp-oms periradicular surgery was scheduled.
During the surgical procedure, cortical bone was carefully re-oved, and soft tissue was curetted after the apical root portion was
esected to obtain an intact specimen for biopsy and evaluation. A newoot-end cavity was prepared and then filled with amalgam (Fig. 1H).he apical biopsy was immersed in fixative and prepared for routineistopathologic evaluation. Reevaluation after 4 years showed that theatient was asymptomatic, and the lesion was completely replaced byewly formed bone (Fig. 1I).
issue ProcessingThe biopsy specimen was immediately immersed in 10% neutral
uffered formalin and fixed for 48 hours. Demineralization was carriedut in an aqueous solution consisting of a mixture of 22.5% (vol/vol)ormic acid and 10% (wt/vol) sodium citrate for 3 weeks. The end pointas determined radiographically. At the end of the demineralizationrocess, amalgam was carefully removed from the apical seat and fromhe soft tissue. The biopsy specimen was washed in running water for 48ours, dehydrated in ascending grades of ethanol, cleared in xylene,nd infiltrated and embedded in paraffin (melting point 56°C) accord-ng to standard procedures. With the microtome set at 4 –5 �m, metic-lous longitudinal serial sections were taken on a buccolingual planentil the specimen was exhausted. Every fifth slide was stained withematoxylin-eosin for screening purposes and for assessment of inflam-ation. Particular care was taken to locate those sections in such a way
hat the apical cavity and the root canal could be seen in a continuumith the pathologic periradicular tissue. A modified Brown and Brenn
echnique for staining bacteria (7) was used for selected slides. Accu-acy of the bacterial staining method was tested by using the protocolescribed by Ricucci and Bergenholtz (8). Slides were examined underhe light microscope.
istopathologic and Histobacteriologic ObservationsLow magnification sections stained with the modified Brown and
renn technique disclosed the presence of a lateral canal slightly coro-al to the amalgam root-end filling. This ramification could be followedlong its way from the root canal wall to the periodontal ligament (Fig.A-D). Necrotic tissue and bacterial colonies were seen in this lateral
ommunication (Fig. 2 C).Bacterial colonization of the dentinal tubules was also observed
Fig. 2D–F). Bacteria (blue bodies) were clearly distinguishable fromhe residual amalgam (black particles) (Fig. 2E, F). Cross-sectionaliew of some dentinal tubules allowed a better visualization of intratu-ular bacterial colonization (Fig. 2D). Bacteria were not found in theystic cavity and in the surrounding pathologic tissue.
On the basis of hematoxylin-eosin–stained sections, the lesion wasiagnosed as an apical cyst. Serial sections revealed that the cyst actuallyccupied only approximately one half of the whole lesion diameter.pical cysts are frequently lined by stratified squamous epithelium (9).n the present case, a stratified nonkeratinized cylindrical or cubicalpithelium was present (Fig. 3A–C), with a distinct basal layer (Fig.D). More superficially, degenerating epithelial cells were seen exfoli-ting into the cyst lumen (Fig. 3E).
DiscussionFailure of nonsurgical root canal treatment is usually related to the
resence of residual bacteria (persistent infection) or reinfection of anlready disinfected root canal environment (secondary infection) (1).f these conditions, it appears that persistent infections are the most
ommon cause of post-treatment apical periodontitis (10). For bacteria rOE — Volume 34, Number 10, October 2008
o survive and be involved in persistent infections, they have to (A) resistntimicrobial intracanal procedures and (B) manage to survive in arastically changed environment in which nutrients are scarce (11).acteria located in anatomic complexities such as dentinal tubules,
rregularities, isthmuses, and ramifications can be protected from theffects of instruments and chemical substances used in the main canal12). For surviving bacteria to maintain or induce apical periodontitis,hey must (A) adapt to the new environment represented by the filledanal, (B) have a steady source of nutrients (tissue remnants are usuallyemporary, but fluid seeping via ramifications and leakage channels areermanent), (C) have available space to multiply, and (D) reach num-ers high enough to elicit tissue damage.
In the case reported in this article, even after chemomechanicalreparation with NaOCl as an irrigant and application of calcium hy-roxide for a total of 75 days, bacteria persisted in the apical root canalystem within dentinal tubules and in a lateral canal to be the mostrobable cause of failure. Chemomechanical procedures do not suc-eed in rendering root canals bacteria-free in about one half of the cases13–15). Although supplementing disinfection by calcium hydrox-de interappointment dressing can increase the incidence of nega-ive cultures, bacteria are still detected in some cases (13, 15). Theailure of calcium hydroxide to eliminate bacteria in dentinal tu-ules and ramifications might relate to its low solubility and inacti-ation by dentin, tissue fluids, and organic matter, all of which canamper the diffusion and further pH-dependent antimicrobial ef-
ects of calcium hydroxide (16, 17).Noteworthy in this case was that the apical periodontitis lesion
howed decreased size at 18-month follow-up evaluation after retreat-ent, but after a given period it stabilized, and no further indication of
ealing was evident because it remained unaltered at 46-month evalu-tion. Because the size of apical periodontitis lesion is correlated to theiversity and density of bacteria in the canal (18, 19), the probableeason for initial decrease in size was reduction in the load of bacterialrritants within the canal by retreatment procedures. A short-term fol-ow-up evaluation would erroneously interpret this lesion as healing.owever, persistence and stabilization of the lesion after long-termvaluation indicated that bacteria were not completely eradicated or ateast reduced to levels compatible with complete resolution of the le-ion. In other words, because the lesion size is related to the level ofnfection, if the latter is reduced but not eliminated, the former can alsoeduce but not to heal completely. This was apparently the case in theresent report, in which instruments and substances used during re-
reatment might have affected bacteria occurring in the main canaloronary to the root-end filling but were not able to reach and eradicateacteria located in the very apical ramification and within tubules along
he dentinal walls of the retrocavity.Periradicular surgery exhibits a failure rate of about 10% of the
ases (20 –23). Persistent apical periodontitis after surgical treatments usually related to the inability to eliminate or at least seal residualacteria in the root canal system to deny them access to the periradicu-
ar tissues. In the present case report, frank communication betweenesidual bacteria and the periradicular tissues might have been estab-ished by many ways: (A) bacteria in the apical ramification were inirect contact with the periradicular tissues, from which they might havecquired nutrients to survive, proliferate, and then maintain tissue ag-ression; (B) infected dentinal tubules might have been exposed afteroot-end resection and/or made patent by cementum resorption; andC) finally, poor sealing ability of amalgam might have allowed leakageo occur, providing nutrients for remaining bacteria and creating aathway through which bacteria and/or their products might have
eached the periradicular tissues and maintained inflammation (24).Persistent Infection Leading to Failure 1251

yrtsii
toh
ht
Ftscdsiob
Case Report/Clinical Techniques
1
Amalgam was the most used material for root-end fillings for manyears (2), but it has significantly decreased in popularity because of itseported limitations, especially poor clinical performance (25). Al-hough amalgam has also problems of biocompatibility (26), corro-ion, and staining (27), the poor clinical performance associated withts use in periradicular surgery is very likely to be related to deficiencies
A
C
E F
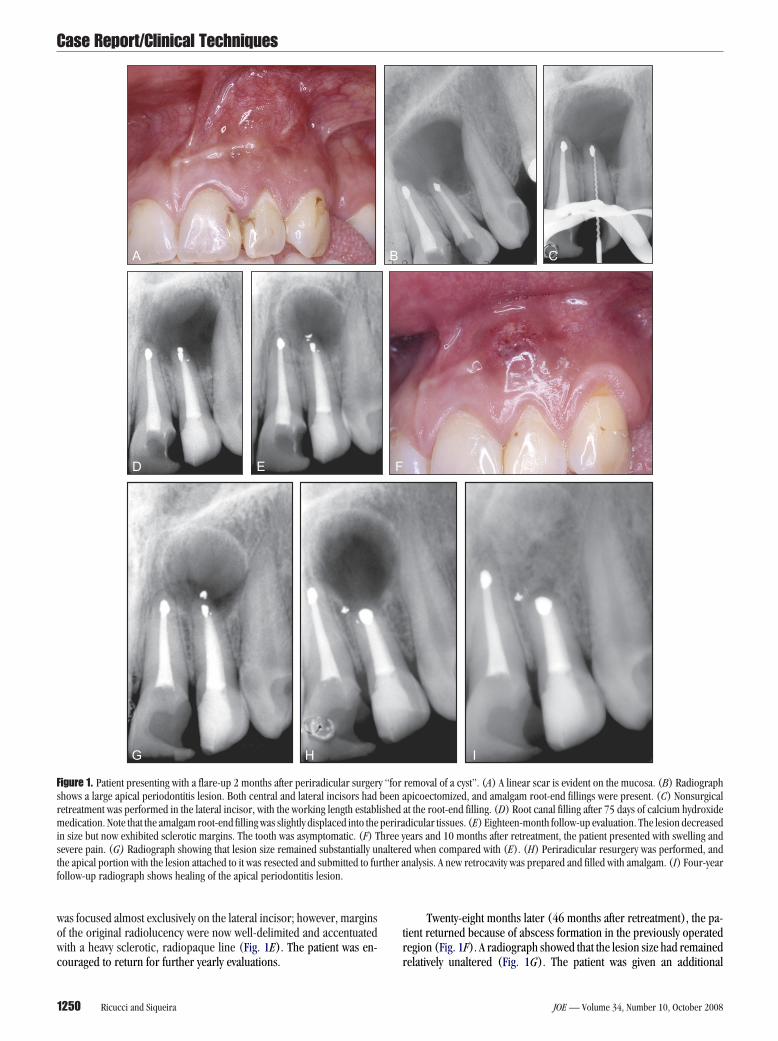
igure 2. Histobacteriologic analysis of the surgical specimen. Serial sectionechnique). (A) Low magnification shows the exit of a lateral canal on the palataurgery. The amalgam root-end filling was removed after decalcification (origianal extending from the main canal to the external root surface (original magnisplaying necrotic tissue and bacterial colonies (original magnification, �10howing intratubular bacterial colonization (original magnification, �1000).ndicated by the arrow is further magnified in the inset. Longitudinally cut deriginal magnification of the inset, �1000). (F) Higher magnification from therown/black–stained amalgam particles (original magnification, �1000).
n sealing ability (28). The case presented here reinforces this assump- t
252 Ricucci and Siqueira
ion, because infected dentinal tubules were mostly located in the wallsf cavity filled with amalgam, and leakage through the material mightave exerted the effects described above.
It has been postulated that placement of a root-end filling en-ances the outcome of surgical endodontics, particularly when persis-
ent infections are the cause of failure (24). To exert such influence on
cut on a buccolingual plane (Taylor’s modified Brown and Brenn stainingcanal wall. Note the beveled cut of the root tip produced in occasion of the firstgnification, �25). (B–D) Sections taken at different depths showed a lateraln, �25). The inset in (C) is a higher magnification of the lateral canal contenthe inset in (D) is a higher magnification of dentinal tubules in cross-sectionigher magnification of the area demarcated by the rectangle in (A). The areatubules appear heavily colonized by bacteria (original magnification, �100;canal wall. Blue-stained bacterial cells are clearly distinguished from the dark
B
D
s werel rootnal maificatio00). T(E) Hntinal
root
he outcome, it is expected that the root-end filling material seals the
JOE — Volume 34, Number 10, October 2008

cctaat
tcstcrnmr
pdmfqfcc
tompsq
tccacscrslneia
ct
Fl�e
Case Report/Clinical Techniques
J
avity, impeding the influx of protein-rich fluids or exudates into theanal or the egress of bacteria from the canal to the periradicularissues. Because persistent/secondary intraradicular infections are un-rguably the major cause of treatment failure, in the event a surgicalpproach is needed to manage a failed case, a root-end filling shouldhen be placed to enhance the prognosis.
Surgical failures can be managed by nonsurgical root canal re-reatment, surgical retreatment, or a combination of both. The presentase had to be sequentially approached by these 2 modalities to result inuccess. Although the outcome of surgical retreatment is usually poorerhan that of first-time surgery, a reasonable number of cases are stillonverted into success (about 60%) (20, 29). The outcome of the caseeported herein confirms that periradicular resurgery is a good alter-ative to extraction (20). Here, success of the resurgical approach isostly explained by removal of infection after additional cutting of the
oot end.It must be pointed out that the first choice for the management of
ost-treatment apical periodontitis that has not responded to substan-ard nonsurgical root canal treatment should be nonsurgical retreat-ent. In other words, nonsurgical retreatment should always be per-
ormed when it is feasible and can offer a better prognosis because theuality of treatment can be improved. In this context, the option for theirst surgical approach in this case report, where the quality of rootanal treatment was radiographically inadequate and retreatment was
A B
D
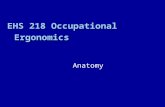
igure 3. Histopathologic analysis of the apical periodontitis lesion (hematoxyumen (original magnification, �50 and �100, respectively). (C) Detail of the c
400). (D) Higher magnification displaying a distinct basal layer (original magnxfoliating into the cyst lumen (original magnification, �1000).
learly feasible, can be regarded as a mistake in treatment plan. About a
OE — Volume 34, Number 10, October 2008
wo thirds of the treatment failures can be converted into success afterrthograde retreatment (30). Even in the event that nonsurgical retreat-ent fails, enhancement of the root canal treatment quality can exert a
ositive impact on surgery outcome, because success for periradicularurgery is considered to be dependent on root canal treatment of gooduality (2, 23, 29).
Histopathologic analysis of the apical periodontitis lesion allowedhe diagnosis of apical cyst. Depending on the relationship between theyst cavity and the apical foramen, apical cysts can be histopathologi-ally categorized as true cysts (cavity is completely lined by epitheliumnd is independent of the canal) and bay (or pocket) cysts (cavityommunicates with the canal via apical foramen) (31, 32). It has beenaid that because true cysts have their own dynamics independent of theanal and are thus self-sufficient, they can be refractory to nonsurgicaloot canal treatment (9). However, this statement is speculative and notupported by scientific evidence (33–35). In the present report, theesion was cystic, but detachment of the tissue around the root apex didot allow a distinction to be made between true or pocket cysts. How-ver, this appears to be of no relevance for this particular case, becauset was apparently clear that the reason for the failure was infection in thepical canal system, and the cyst was just a consequence of the infection.
In conclusion, the complex apical canal system displayed in thisase illustrates the difficult task of completely cleaning and disinfectinghe root canal system. It is important to point out that the impact of the
C
sin). (A, B) Cyst cavity lined by epithelium and showing necrotic debris in itsll showing stratified nonkeratinized cubical epithelium (original magnification,on, �1000). (E) Epithelial cells degenerate as they reach the superficial layers,
E
lin-eoyst waificati
natomy on the treatment outcome is mostly observed when it makes it
Persistent Infection Leading to Failure 1253

df
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
Case Report/Clinical Techniques
1
ifficult or even impossible to achieve a status of disinfection necessaryor periradicular tissue healing to occur.
References1. Siqueira JF Jr. Reaction of periradicular tissues to root canal treatment: benefits and
drawbacks. Endod Topics 2005;10:123– 47.2. Gutmann ME, Harrison JW. Surgical endodontics. Cambridge, MA: Blackwell, 1991.3. Fukushima H, Yamamoto K, Hirohata K, Sagawa H, Leung KP, Walker CB. Localization
and identification of root canal bacteria in clinically asymptomatic periapical patho-sis. J Endod 1990;16:534 – 8.
4. Nair PN, Sjogren U, Krey G, Kahnberg KE, Sundqvist G. Intraradicular bacteria andfungi in root-filled, asymptomatic human teeth with therapy-resistant periapical le-sions: a long-term light and electron microscopic follow-up study. J Endod1990;16:580 – 8.
5. Ida RD, Gutmann JL. Importance of anatomic variables in endodontic treatmentoutcomes: case report. Endod Dent Traumatol 1995;11:199 –203.
6. Lin LM, Pascon EA, Skribner J, Gangler P, Langeland K. Clinical, radiographic, andhistologic study of endodontic treatment failures. Oral Surg Oral Med Oral Pathol1991;71:603–11.
7. Taylor RD. Modification of the Brown and Brenn Gram stain for the differentialstaining of gram-positive and gram-negative bacteria in tissue sections. Am J ClinPathol 1966;46:472– 6.
8. Ricucci D, Bergenholtz G. Bacterial status in root-filled teeth exposed to the oralenvironment by loss of restoration and fracture or caries: a histobacteriological studyof treated cases. Int Endod J 2003;36:787– 802.
9. Nair PN. New perspectives on radicular cysts: do they heal? Int Endod J 1998;31:155–60.0. Fabricius L, Dahlén G, Sundqvist G, Happonen RP, Möller AJR. Influence of residual
bacteria on periapical tissue healing after chemomechanical treatment and rootfilling of experimentally infected monkey teeth. Eur J Oral Sci 2006;114:278 – 85.
1. Siqueira JF Jr. Aetiology of root canal treatment failure: why well-treated teeth can fail.Int Endod J 2001;34:1–10.
2. Nair PN, Henry S, Cano V, Vera J. Microbial status of apical root canal system ofhuman mandibular first molars with primary apical periodontitis after “one-visit”endodontic treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2005;99:231–52.
3. Siqueira JF Jr, Guimarães-Pinto T, Rôças IN. Effects of chemomechanical preparationwith 2.5% sodium hypochlorite and intracanal medication with calcium hydroxideon cultivable bacteria in infected root canals. J Endod 2007;33:800 –5.
4. Sjögren U, Figdor D, Persson S, Sundqvist G. Influence of infection at the time of rootfilling on the outcome of endodontic treatment of teeth with apical periodontitis. IntEndod J 1997;30:297–306.
5. McGurkin-Smith R, Trope M, Caplan D, Sigurdsson A. Reduction of intracanal bac-teria using GT rotary instrumentation, 5.25% NaOCl, EDTA, and Ca(OH) . J Endod
22005;31:359 – 63.
254 Ricucci and Siqueira
6. Siqueira JF Jr, Lopes HP. Mechanisms of antimicrobial activity of calcium hydroxide:a critical review. Int Endod J 1999;32:361–9.
7. Haapasalo M, Qian W, Portenier I, Waltimo T. Effects of dentin on the antimicrobialproperties of endodontic medicaments. J Endod 2007;33:917–25.
8. Sundqvist G. Bacteriological studies of necrotic dental pulps (Odontological Disser-tation no.7). Umea, Sweden: University of Umea, 1976.
9. Siqueira JF Jr, Rôças IN, Paiva SSM, Magalhães KM, Guimarães-Pinto T. Cultivablebacteria in infected root canals as identified by 16S rRNA gene sequencing. OralMicrobiol Immunol 2007;22:266 –71.
0. Gagliani MM, Gorni FG, Strohmenger L. Periapical resurgery versus periapical sur-gery: a 5-year longitudinal comparison. Int Endod J 2005;38:320 –7.
1. Rubinstein RA, Kim S. Long-term follow-up of cases considered healed one year afterapical microsurgery. J Endod 2002;28:378 – 83.
2. Zuolo ML, Ferreira MO, Gutmann JL. Prognosis in periradicular surgery: a clinicalprospective study. Int Endod J 2000;33:91– 8.
3. Grung B, Molven O, Halse A. Periapical surgery in a Norwegian county hospital:follow-up findings of 477 teeth. J Endod 1990;16:411–7.
4. Friedman S. Expected outcomes in the prevention and treatment of apical periodon-titis. In: Ørstavik D, Pitt Ford T, eds. Essential endodontology. Oxford, UK: BlackwellMunksgaard Ltd, 2008:408 – 69.
5. Dorn SO, Gartner AH. Retrograde filling materials: a retrospective success-failurestudy of amalgam, EBA, and IRM. J Endod 1990;16:391–3.
6. Baek SH, Plenk H Jr, Kim S. Periapical tissue responses and cementum regenerationwith amalgam, SuperEBA, and MTA as root-end filling materials. J Endod2005;31:444 –9.
7. Harrison JD, Rowley PS, Peters PD. Amalgam tattoos: light and electron microscopyand electron-probe micro-analysis. J Pathol 1977;121:83–92.
8. Chong BS, Pitt Ford TR, Watson TF, Wilson RF. Sealing ability of potential retrograderoot filling materials. Endod Dent Traumatol 1995;11:264 –9.
9. Wang N, Knight K, Dao T, Friedman S. Treatment outcome in endodontics: the To-ronto Study—phases I and II: apical surgery. J Endod 2004;30:751– 61.
0. Sjögren U. Success and failure in endodontics (Odontological Dissertation no.60).Umea, Sweden: University of Umea, 1996.
1. Nair PN, Pajarola G, Schroeder HE. Types and incidence of human periapical lesionsobtained with extracted teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1996;81:93–102.
2. Simon JH. Incidence of periapical cysts in relation to the root canal. J Endod1980;6:845– 8.
3. Lin LM, Ricucci D, Rosenberg PA. Fate of radicular cysts after nonsurgical root canaltherapy. J Endod 2008; in press.
4. Ricucci D, Pascon EA, Ford TR, Langeland K. Epithelium and bacteria in peria-pical lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:239 – 49.
5. Lin LM, Huang GT, Rosenberg PA. Proliferation of epithelial cell rests, formation ofapical cysts, and regression of apical cysts after periapical wound healing. J Endod
2007;33:908 –16.JOE — Volume 34, Number 10, October 2008










![3.Controlul Microbiologic Al Alimentelor[1]](https://static.fdocuments.net/doc/165x107/55cf9cfe550346d033abd0c6/3controlul-microbiologic-al-alimentelor1.jpg)