Anaplastic Sarcoma of the Kidney With Chromosomal Abnormality

of 5
-
Upload
jose-alejandro-inciong -
Category
Documents
-
view
9 -
download
0
description
Anaplastic Sarcoma of the Kidney With Chromosomal Abnormality
Transcript of Anaplastic Sarcoma of the Kidney With Chromosomal Abnormality
-
dney with chromosomalcytouetagMD,
bDivision of Hemato-oncology, Kanagawa Children's Medical Center, Yokohama, 232-8555 Japan
A 12-year-old Japanese girl presented at a regional
Human Pathology (2010) 41, 14951499 Corresponding author. Division of Pathology, Kanagawa Children'sMedical Center, Yokohama City, Kanagawa Prefecture, 232-8555, Japan.ASK. Chromosomal analysis revealed the karyotype of the tumor cells to be 46, XX, +8, 10, der (18) t(10; 18) (q21; p11.2). The thyroid tumor was removed later and diagnosed as adenomatous goiter. Toour knowledge, this is the first case of ASK with chromosomal abnormality and may provide newinsight into the molecular biologic basis of this rare renal tumor. 2010 Elsevier Inc. All rights reserved.
1. Introduction
Anaplastic sarcoma of the kidney (ASK) is a rare andnewly recognized renal neoplasm, first described by Vujanicet al in 2007 [1]. According to their report, ASK mainlyoccurs in children or adolescents younger than 15 years andis histologically characterized by widespread anaplasticchanges such as pleomorphic cells and highly atypicalmitotic figures, polyphenotypic mesenchymal differentia-tion, and absence of blastemal element, neoplastic epithelialstructure, and nephrogenic rest. The only subsequent case
report describing ASK [2] does not discuss cytogeneticabnormality in ASK. ASK was previously diagnosed asvarious types of tumor, most often as anaplastic nephro-blastoma, and was treated accordingly, with relatively goodoverall outcome [1]. To better understand the nature of ASK,further molecular studies are desirable. Here, we report theclinicopathological findings of a new case of ASK withchromosomal abnormality.
2. Clinical case0dKeywords:Anaplastic sarcoma ofkidney;
Renal tumor;Children;Chromosomal abnormalitycDivision of Surgery, Kanagawa Children's Medical Center, Yokohama, 232-8555 JapandDivision of Radiology, Kanagawa Children's Medical Center, Yokohama, 232-8555 Japan
Received 6 January 2010; revised 22 February 2010; accepted 11 March 2010
Summary We report a case of anaplastic sarcoma of the kidney (ASK) with cytogenetic findings. A 12-year-old Japanese girl presented with buttock pain and urinary incontinence. Radiological investigationsrevealed a right renal tumor with multiple distant metastases and multicystic thyroid tumor. Sheunderwent radical right nephrectomy and subsequently received chemotherapy and radiation therapy.Histologically, the renal tumor demonstrated admixture of various types of mesenchymal elements:cellular spindle cells with anaplastic features, cartilage, and rhabdomyoblastic cells consistent withaDivision of Pathology, Kanagawa Children's Medical Center, Yokohama, 232-8555 JapanCase study
Anaplastic sarcoma of the kiabnormality: first report onKiyoshi Gomi MD, PhDa,, Satoshi HamanMasae Matsumoto MD, PhDb, Norihiko KiNoriko Aida MD, PhDd, Hisato KigasawaE-mail address: [email protected] (K. Gomi).
046-8177/$ see front matter 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.humpath.2010.03.008ogenetic findingsMD, PhDb, Mio Tanaka MD, PhDa,
awa MD, PhD c, Tetsu Niwa MD, PhDd,PhDb, Yukichi Tanaka MD, PhDawww.elsevier.com/locate/humpathhospital with buttock pain and urinary incontinence. No past
-
history was relevant. Her mother underwent subtotalthyroidectomy for diffuse hyperplasia of the thyroid at theage of 17 years. Magnetic resonance imaging revealed tumorin the sacral bone with extension into the surrounding softtissue. After open biopsy, Ewing sarcoma family tumor wassuspected. The patient was transferred to our hospital, whereextensive imaging studies revealed a right renal mass andmetastases to the lungs (multiple, up to 1 cm in diameter),sacral bone, pubic region, and right femur. The biopsiedsacral bone lesion was considered a metastatic lesion. Amulticystic tumor was also noted in the right lobe of thethyroid gland. Right radical nephrectomy was performedimmediately. Under the diagnosis of unclassified sarcoma,the patient received postoperative intensive chemotherapyfor Ewing sarcoma family tumors and radiation therapy. Sixmonths later, the thyroid tumor was resected and diagnosedas adenomatous goiter. At follow-up at 28 months, the lungand bone metastases showed a significant decrease in size,and there was no sign of local recurrence or newly developeddistant metastasis.
3. Materials and methods
The resected tissue samples were fixed in 10% formalinand embedded in paraffin. Serial paraffin sections (3-4 m
thick) were cut from the blocks and stained with hematoxylinand eosin. Immunohistochemical study was performed usingantibodies against the antigens, as shown in Table 1, and theindirect immunoperoxidase method. Frozen section tumorsamples were studied for EWS-FLI1, EWSR1-ERG,EWSR1-WT1, ETV6-NTRK3, SS18-SSX, PAX3-FOXO1A,and PAX7-FOXO1A chimeric transcripts, as describedpreviously [3-7]. Chromosomal preparations of disaggre-gated tumor cells were made after 3 days culture usingstandard methods. The choromosomes were G-banded withtrypsin and Giemsa. Karyotype descriptions were madeaccording to the International System of CytogeneticNomenclature of 1995.
4. Results
4.1. Pathological findings
The right kidney measured 17 9.5 8.5 cm and weighed985 g. A well-demarcated tumor (15 8 5.5 cm) waslocated in the superior portion. Cut sections revealed a graycolored, friable tumor tissue with multifocal necrosis, cysticdegeneration, and a large subcapsular hematoma (Fig. 1).The tumor exhibited focal invasion into the renal pelvis, andno extension beyond the renal capsule was noted.
Table 1 Results of immunohistochemistry
/Anticellslls
WCytokeratin CAM5.2 BDB 1:1/MWCytokeratin AE1/AE3 NCR 1:1/MW
treattreatreatedWated ++
++ated
reated
W
W
o, CABMDan Di, nodex.
1496 K. Gomi et al.EMA E29 DC 1:50/MWSynaptophysin SY38 DC 1:20/MWS-100 protein 2A10 IBL 1:800/unGFAP 6F2 DC 1:100/unMuscle specific actin HHF-35 ENZ 1:50/untDesmin D33 DC 1:100/MMyoglobin polyclonal BMD 1:1/untreMyogenin F5D DC 1:25/MWCD34 NU-4A1 NCR 1:1/untreCD56 (N-CAM) 123C3 IVG 1:1/MWCD99 (MIC-2) 12E7 DC 1:50/untBcl-2 DAKO124 DC 1:50/MWBeta-catenin 14 TDL 1:100/MBAF47 (INI-1) 14 BDT 1:300/ACWT-1 6F-H2 DC 1:25/ACKi-67 MIB-1 DC 1:100/M
DC, DAKO Cytomation Glostrup Denmark; BDB, BD Bioscience, SandiegLaboratories, Takasaki, Japan; ENZ, Enzo Life Science International;Transduction Laboratories, Lexington, KY; BDT, BD Transduction labs, Susing a 500-W oven; AC, autoclave in 0.01 mol/L citrate buffer (pH 6.0);cells; +++, 50%-90% of positive cells; N.E, not examined; LI, labeling inAntibodies to Antibodyclone
Source Dilutionretrievaltissue ce
Vimentin V9 DC 1:100/M +++ +++ +++ LI: 20-30% N.E N.E
; NCR, Nichirei Biosciences Inc, Tokyo, Japan; IBL, Immuno-Biological, Biomeda Corp; IVG, Zymed-Invitrogen Corp, Carlsbad, CA; TDL,ego, CA; MW, microwave treatment in 0.01 mol/L citrate buffer (pH 6.0)positive cell; +, less than 10% of positive cells; ++, 10%-50% of positivegen Reactivity for tumor cells
Spindlecells
Cartilaginoustissue
Rhabdomyoblasticcells
+++ +
ed ++ ed
+ +++ ++
-
Histologically, the tumor revealed fascicular growth ofoval or short spindle cells having hyperchromatic nuclei withcoarse chromatin and inconspicuous nucleoli. The tumorcells showed frequent mitotic figures and karyorrhecticappearances. Anaplastic features, such as large irregular-shaped nuclei, atypical or multipolar mitoses, and bizarremultinucleated giant cells, were commonly found (Fig. 2A).Throughout the tumor, there existed scattered foci of hyalinecartilaginous tissue with various atypical features (Fig. 2B)and clusters of brightly eosinophilic, rounded/elongatedrhabdomyoblastic cells occasionally displaying straplike
Fig. 2 Microscopic findings of ASK (hematoxylin-eosin). A,Anaplastic features are present, including pleomorphic cells, bizarremultinucleated giant cells, and atypical mitotic features (originalmagnification 400). B, Chondroid differentiation: note the islandsof hyaline cartilaginous tissue (original magnification 200). C,Rhabdomyoblastic differentiation: rounded or elongated rhabdo-myoblastic cells are present (original magnification 200) (inset:cross-striations are seen in some cells [red arrowheads]; originalmagnification 1000).
1497ASK with chromosomal abnormalityFig. 1 Gross appearance of radical nephrectomy specimen. Alarge, encapsulated tumor is noted in the superior portion of theright kidney. The tumor was gray colored and fleshy withmultifocal necrosis and hemorrhage (red arrowheads). A metastaticsatellite nodule (yellow arrowheads) is observed.
-
appearance with distinct cross-striations (Fig. 2C). Noblastemal element, epithelial structure, or nephrogenic restwas identified. Immunohistochemically, the tumor cells werediffusely positive for vimentin and focally positive formuscle-specific actin, desmin, myoglobin, and myogenin(mainly in rhabdomyoblastic cells), or S-100 alpha and S-100 beta (cartilaginous tissue). They were negative forcytokeratin, EMA, synaptophysin, GFAP, CD99, CD34,CD56, nuclear beta catenin, and WT-1. Diffuse and strongnuclear staining for BAF47 was observed. MIB-1 labelingindex was 20% to 30%.
Differential diagnoses included anaplastic nephroblas-toma, synovial sarcoma, and malignant mesenchymoma.Because the tumor showed 2 types of overt malignantmesenchymal differentiation in addition to undifferentiated(rather than blastemal) spindle cell areas, we initiallyconsidered the tumor to be within the spectrum of malignantmesenchymoma. It has been suggested, however, that thediagnosis of malignant mesenchymoma should be removedfrom the classification of soft tissue tumors because this termappears to have become a wastebasket for poorly differen-tiated sarcomas [8]. Thus, our initial diagnosis was
WT1, ETV6-NTRK3, SS18-SSX, PAX3-FOXO1A, and
diagnosis of malignant mesenchymoma was avoided for the
1498 K. Gomi et al.unclassified anaplastic sarcoma with rhabdomyoblastic andcartilaginous differentiation. The diagnosis of ASK wasreached at a later date, following reference to the article byVujanic et al [1]; this diagnosis was subsequently confirmedby Dr Beckwith, who was a coauthor on the original article.
The resected thyroid tumor was adenomatous goiter ratherthan a metastatic lesion.
4.2. Molecular findings
In reverse transcriptase-polymerase chain reaction assay,fusion transcripts for EWSR1-FLI1, EWSR1-ERG, EWSR1-
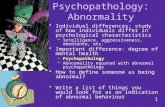
Fig. 3 G-banding karyotype of the tumor cells showing 46, XX, +8,10, der (18) t (10; 18) (q21; p11.2). The red arrow indicatestranslocation between chromosome 10 and 18 and monosomy ofchromosome 10. The blue arrowhead shows trisomyof chromosome 8.reason mentioned in the Pathological Findings section,although there are some case reports of malignant mesench-ymoma arising in the kidney, some of which may correspondto ASK [9-12].
Cytogenetic abnormalities such as specific translocationin chromosome and aberrant genes have never beendescribed in ASK. The present renal tumor demonstratedchromosomal abnormality, that is, 46, XX, +8, 10, der(18) t (10; 18) (q21; p11.2) in 20 of 20 tumor cellsexamined. This type of translocation has not been reportedPAX7-FOXO1A were not detected in the renal tumor tissue.
4.3. Chromosomal analysis
G-banding cytogenetic analysis revealed the karyotype ofthe neoplastic cells (20/20) to be 46, XX, +8, 10, der (18) t(10; 18) (q21; p11.2) (Fig. 3). The patient's karyotype fromlymphocytes from peripheral blood was normal female type,46, XX.
5. Discussion
ASK is a very rare renal neoplasm first described byVujanic et al in 2007 [1], who detected 20 cases of ASKfrom among 3 large pathology collections, including theNational Wilms Tumors Study Pathology Center (7400cases), the International Society of Pediatric Oncology(4000 cases), and the United Kingdom Children's CancerStudy Group (1600 cases). Histologically, all 20 cases ofASK displayed a spindle cell component, which containedeither multiple foci or diffuse, widespread anaplasticchanges with bizarre pleomorphic cells and highly atypicalmitotic features. Chondroid differentiation was seen asislands of hyaline cartilage or chondroid matrix and wasobserved in most cases (16/20, 80%). In a few cases, osteoidcomponent (2/20, 10%), osteoclast-like giant cells (4/20,20%), and rhabdomyoblastic cells (2/20, 10%) were noted.An additional case in a 24-year-old woman has recently beenreported by Labanaris et al [2], without a description of thehistological details.
The present tumor showed diffuse anaplastic changes,islands of cartilage (with or without atypia), and rhabdo-myoblastic cells. Rhabdomyoblastic cells with cross-stria-tion, which were not observed in the 21 published cases ofASK, were also found. The present tumor lacked blastemalcells positive for CD56 or WT-1, neoplastic epithelialcomponents, and a nephrogenic rest; these findings areinconsistent with nephroblastoma. Based on molecularstudies using reverse transcriptase-polymerase chain reactionassay, synovial sarcoma, congenital mesoblastic nephroma(cellular variant), Ewing sarcoma family of tumor, anddesmoplastic small round cell tumor were also excluded. The
-
in any other tumor, and the relationship between ASK andthis chromosomal abnormality remains unknown. Althoughfurther molecular genetic studies are required, this novelchromosomal translocation may play a critical role in thepathogenesis of ASK.
Vujanic et al reported that the patients with ASK weretreated according to different therapeutic protocols and evendifferent diagnoses, but with reasonably good overalloutcome, and appeared to have responded well to treatmentgiven to anaplastic nephroblastoma [1]. The present case wasstage IV, but the patient is alive, with disease, 2 years afterthe onset, after chemotherapy against the Ewing sarcomafamily of tumors. More appropriate treatment, however,should be obtained based on an understanding of themolecular characters of the tumor.
In conclusion, this study is the first to report ASK withchromosomal findings, including rearrangement between10q21 and 18p11.2. Further molecular analysis, with a focuson 10q21 and 18p11.2, could be helpful in clarifying thepathogenesis of this unusual renal tumor.
Acknowledgments
References[1] Vujanic GM, Kelsey A, Perlman EJ, et al. Anaplastic sarcoma of the
kidney: a clinicopathologic study of 20 cases of a new entity withpolyphenotypic features. Am J Surg Pathol 2007;31:1459-68.
[2] Labanaris AP, Zugor V, Smiszek R, et al. Anaplastic sarcoma of thekidney. Sci World J 2009;9:97-110.
[3] Kato K, Kato Y, Ijiri R, et al. Ewing's sarcoma family of tumor arisingin the adrenal gland-possible diagnostic pitfall in pediatric pathology:histologic, immunohistochemical, ultrastructural, and molecular study.HUM PATHOL 2001;32:1012-6.
[4] Wang LL, Perlman EJ, VujanicGM, et al. Desmoplastic small round celltumor of the kidney in childhood. Am J Surg Pathol 2007;31:576-84.
[5] Argani P, Fritsch M, Kadkol SS, et al. Detection of the ETV6-NTRK3chimeric RNA of infantile fibrosarcoma/cellular congenital mesoblas-tic nephroma in paraffin-embedded tissue: application to challengingpediatric renal stromal tumors. Mod Pathol 2000;13:29-36.
[6] Argani P, Faria PA, Epstein JI, et al. Primary renal synovial sarcoma:molecular and morphologic delineation of an entity previouslyincluded among embryonal sarcoma of the kidney. Am J Surg Pathol2000;24:1087-96.
[7] Kato K, Tanaka Y. Molecular diagnosis of rhabdomyosarcoma(In Japanese, English abstract). Jpn J Pediatr Surg 2001;34:434-9.
[8] Weiss SH, Goldblum JR. Enzinger and Weiss's soft tissue tumors.5th ed. Philadelphia: Mosby; 2008.
[9] Faria PA, Zerbini MC. Dedifferentiated cystic nephroma withmalignant mesenchymoma as the dedifferentiated component. PediatrPathol Lab Med 1996;16:1003-11.
[10] Bulkley GJ, Drinker HR. Malignant mesenchymoma of the kidney:case report. J Urol 1957;77:583-8.
[11] Mead JH, Herrera GA, Kaufman MF, et al. Case report of primary
1499ASK with chromosomal abnormalityHuman anatomy, Loma Linda University and School ofMedicine, for confirming our diagnosis and Ms YukariHasegawa, Ms Takako Yokomori, and Ms Sayuri Oda fortheir valuable technical assistance.cystic sarcoma of the kidney, demonstrating fibrohistiocytic, osteoid,and cartilaginous components (malignant mesenchymoma). Cancer1982;50:2211-4.
[12] Reed HM, Poppiti Jr R, Sivina M. Malignant mesenchymoma ofkidney and inferior vena cava. Urology 1983;22:297-9.The authors thank Dr Beckwith JB, Pathology and
Anaplastic sarcoma of the kidney with chromosomal abnormality: first report on cytogenetic find.....IntroductionClinical caseMaterials and methodsResultsPathological findingsMolecular findingsChromosomal analysis
DiscussionAcknowledgmentsReferences