Analysis of long-term care transitions: Examples in the dementia care context
54
1 ANALYSIS OF LONG-TERM CARE ANALYSIS OF LONG-TERM CARE TRANSITIONS: TRANSITIONS: EXAMPLES IN THE DEMENTIA CARE EXAMPLES IN THE DEMENTIA CARE CONTEXT CONTEXT Joseph E. Gaugler, Ph.D. Joseph E. Gaugler, Ph.D. Associate Professor Associate Professor School of Nursing School of Nursing University of Minnesota University of Minnesota
Transcript of Analysis of long-term care transitions: Examples in the dementia care context

1
ANALYSIS OF LONG-TERM CARE ANALYSIS OF LONG-TERM CARE TRANSITIONS: TRANSITIONS:
EXAMPLES IN THE DEMENTIA CARE EXAMPLES IN THE DEMENTIA CARE CONTEXTCONTEXT
Joseph E. Gaugler, Ph.D.Joseph E. Gaugler, Ph.D.
Associate ProfessorAssociate Professor
School of NursingSchool of Nursing
University of MinnesotaUniversity of Minnesota

ACKNOWLEDGEMENTS
Funding Agencies (as PI)• National Institute on Aging (R21 AG026525)
Collaborators • Steven H. Zarit, Ph.D., Penn State University• Leonard I. Pearlin, Ph.D., University of Maryland• Robert Kane, M.D., University of Minnesota• Rosalie Kane, Ph.D., University of Minnesota• Robert Newcomer, Ph.D., University of California-San
Francisco• Mary Mittelman, DrPH, New York University• Ken Hepburn, Ph.D., Emory University• Mike Williams, Ph.D., CaringFamily, LLC

SPECIFIC AIMS
Who am I?
Discuss transitions in informal dementia care
Nursing home admission (NHA) in dementia caregiving• Predicting NHA in dementia
• Analyzing caregivers’ emotional and psychological adaptation to NHA
• Identifying interventions to facilitate adaptation to NHA

4
Longitudinal implications of
informal long-term care
Effectiveness of psychosocial interventions
Social integration in residential long-
term care
OTHERS OTHERS Dementia Demonstration Project (VA); Nursing Home Training to Impact CMS Dementia Demonstration Project (VA); Nursing Home Training to Impact CMS
Indicators (NIA R42);The Memory Club (Alzheimer’s Association Indicators (NIA R42);The Memory Club (Alzheimer’s Association collaboration); Nursing Home Diversion Project (MN-BoA)collaboration); Nursing Home Diversion Project (MN-BoA)
NIA R01 AG022066 NIA R01 AG022066 Comprehensive Comprehensive
Support for AD CGs Support for AD CGs (2005-2010)(2005-2010)
NIA R21 AG026525 NIA R21 AG026525 CG Outcomes Post CG Outcomes Post
NH Placement NH Placement (2007-2009)(2007-2009)
NIA K02 NIA K02 ADS Use and ADS Use and
Outcomes: MM Outcomes: MM (2008-2013)(2008-2013)
NINR R41 NR010642 NINR R41 NR010642 Communication in Communication in
the NH the NH (2008; Co-PI)(2008; Co-PI)
NIA R21 AG026525 NIA R21 AG026525 CG Outcomes Post CG Outcomes Post
NH Placement NH Placement (2007-2009)(2007-2009)

WHAT IS A TRANSITION?

WHAT IS A TRANSITION?
Life course perspective (e.g., Glen Elder): “A change in social roles or responsibilities” (Wethington, 2000; p. 116)
• Can also be thought of as a significant change to an existing role (e.g., caregiving and institutionalization)
• Transitions as unexpected and/or positive (onset in dementia caregiving; Gaugler et al., 2003)
• Also, “turning points:” “major transitions associated with major life changes or breaks in ongoing trajectories” (Wethington, 2000: p. 116)
Nursing perspective: “Transitions are both a result of and result in change in lives, health, relationships, and environments.” (Meleis et al. 2000)
• Meleis’ Middle Range Theory of Transitions (Meleis et al., 2000)

Wethington. E. (2000). An overview of the life course perspective: Implications for health and nutrition. Journal of Nutrition Education and Behavior, 37, 115-120. (p. 116)

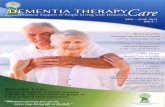
MELEIS TRANSITION MODEL (Meleis et al., 2000; p. 16)
Types and patterns of transitions
Properties of transition experiences
Transition conditions: Facilitators and inhibitors
Process indicators
Outcome indicators
Nursing therapeutics/Clinical intervention

NATURE OF TRANSITIONS
TYPES Developmental
Situational Health/Illness
Organizational
PATTERNS Single Multiple Sequential
Simultaneous Related
Unrelated
PROPERTIES Awareness
Engagement Change & difference Transition time span
Critical points & events
TRANSITION CONDITIONS: FACILITATORS AND INHIBITORS
PERSONAL Meanings
Cultural beliefs & attitudes Socioeconomic status
Preparation & knowledge
COMMUNITY SOCIETY
PATTERNS OF RESPONSE
PROCESS INDICATORS Feeling connected Interacting Location & being
situated Developing confidence &
coping
OUTCOMES Mastery
Fluid integrative identities
NURSING THERAPEUTICS/INTERVENTION
From Meleis, A.I., Sawyer, L.M., Im, E-O., Hilfinger Messias, D.K., & Schumacher, K. (2000). Experiencing transitions: An emerging middle-range theory. Advances in Nursing Science, 23, 12-28. (Figure 1)

TRANSITIONS IN INFORMAL DEMENTIA CARE
Onset, institutionalization, and bereavement (Aneshensel et al., 1995)Montgomery model (Montgomery & Kosloski, 2000):
• When the individual first performs caregiving tasks• Self-identification of “caregiver”• Provision of personal care• Seeking assistance• Formal service use• Considering institutionalization• Actual nursing home use• Termination of caregiving due to bereavement• Recovery of the care recipient• Decision by the caregiver to “quit”

NURSING HOME ADMISSION
It is estimated that 48-55% of nursing home (NH) residents suffer from some form of cognitive impairment (NCHS, 2006).
• 14% residents are estimated as diagnosed with Alzheimer’s disease (Magaziner et al., 2000).
Nursing home entry is associated with rapid declines in health, increased mortality, and emotional challenges for families. Up to 50 million individuals in the U.S. provide informal (unpaid) care to disabled family members Questions when we examine NHA in dementia caregiving
• What potentially predictors NHA in dementia?• How do caregivers adapt to NHA?• Are there clinical approaches that can help caregivers adapt to
NHA?

QUESTION 1: WHAT PREDICTS NHA IN DEMENTIA?
Meta-analyses and systematic reviews identify cognitive impairment as a key precursor to NHA (Gaugler et al., 2007; Miller & Weissert, 2000).
• A systematic review of NHA in dementia does not exist, however.
Providing a synthesis of factors that trigger institutionalization in dementia is important:
• NHA is considered a key clinical marker of the progression of dementia (Winblad, 2000)
– Could lead to enhanced prognostic tools
– Could also inform the targeting of clinical interventions

ANALYSIS 1
Gaugler, J. E., Yu, F., Krichbaum, K., & Wyman, J. F. (in press). Predictors of nursing home admission for persons with dementia. Medical Care.

METHODS
Utilized three-phase approach to obtain, extract, and rate data
Search of the literature • 1950-2006 search of MEDLINE, CINAHL, PSYCINFO,
and Digital Dissertations
• Abstracts screened using set inclusion criteria
• Cross-referenced to the point of saturation
Data extracted in two steps
Quality assessment of studies • A 15-item checklist was created• Post-hoc reliability of the data extraction and quality
assessment tools were established

A positive score of 1 applied if:
1. Study sample is nationally or regionally representative of the U.S. elderly population
2. Inclusion and/or exclusion criteria are formulated
3. The process of data collection is described (e.g., interview, self-report)
4. Mean or median and range or standard deviation of times since dementia diagnosis is given
5. Descriptive data are provided on nursing home admitted (e.g., number of individuals institutionalized, time to admission, etc.)
6. Data included from the following categories: a. Sociodemographic characteristics b. Respondent function c. Respondent cognition d. Informal caregiving dimensions e. Formal service use
7. Categorization of nursing home admission: Long-stay vs. short-stay
8. Categorization of nursing home admission: Facility-type (i.e., nursing home vs. other types of facilities)
9. Objective determination of nursing home admission (i.e., from records other than respondent self-report)
10. Clinical tool used to assess patients’ functional and/or cognitive status
11. Reliability and/or validity of study instruments reported
12. Information on participants lost-to-follow-up
13. Training and quality control methods for interviewers’ techniques
14. One-year or less data collection intervals; 3-year follow-up
15. The degree of selection of the patient sample is described Adapted from Mohls et al. (2005)15 (pp. 2615, Table 1) and Friedenreich (1993)14

4248 potentially relevant abstracts and 585 cross-
references identified
4051 studies excluded (e.g., randomized controlled
trial/intervention evaluation; prediction of nursing home admission not considered)
758 studies obtained for further evaluation
24 studies unavailable for retrieval
678 studies excluded● 322 nursing home admission
not outcome● 67 cross-sectional design● 278 not dementia-specific● 9 randomized intervention
included as predictor● 2 repeat studies
80 studies included

RESULTS
The 80 studies represent a total of 39,526 persons with dementia
10,365 persons with dementia were institutionalized.
The sample size in each report ranged from 14 to 5,795.
Thirty-nine studies included U.S. samples.
Length of follow-up ranged from 6 to 240 months.
Average quality score was 6.1 (SD = 1.95; range = 2-12).
• 29 studies were classified as “high” quality (quality score of 7 or above)

Predictor Variable
Direction of Empirical Effect
Negative
Positive
Non-Significant
Sociodemographics: Person with Dementia
Age (n = 37) 0.0% 40.5% 59.5% High quality (n = 19) 0.0% 36.8% 63.2% Gender: Male (n = 25) 8.0% 12.0% 80.0% High quality (n = 13) 7.7% 15.4% 76.9%
Patient is white (n = 12) 8.3% 50.0% 41.7% High quality (n = 6) 16.7% 16.7% 66.7% Marital status: Married (n = 4) 50.0% 0.0% 50.0% High quality (n = 3) 66.7% 0.0% 33.3%
Education (n = 7) 14.3% 0.0% 85.7% High quality (n = 3) 33.3% 0.0% 66.7%
Income (n = 2) 0.0% 0.0% 100.0% High quality (n = 2) 0.0% 0.0% 100.0%
Family income (n = 3) 0.0% 100.0% 0.0%
Medicaid eligible (n = 2) 0.0% 50.0% 50.0%
Patient lives alone (n = 16) 0.0% 31.3% 68.8% High quality (n = 10) 0.0% 40.0% 60.0%

Predictor Variable
Direction of Empirical Effect
Negative
Positive
Non-Significant
Indicators of Dementia Severity
Cognitive impairment (n = 40) 0.0% 65.0% 35.0% High quality (n = 20) 0.0% 65.0% 35.0%
Duration of dementia (n = 6) 0.0% 0.0% 100.0% High quality (n = 3) 0.0% 0.0% 100.0%
Diagnosis of AD (n = 5) 0.0% 80.0% 20.0% High quality (n = 2) 0.0% 100.0% 0.0% WMS: Logical memory (n = 2) 0.0% 50.0% 50.0%
WMS: Orientation (n = 2) 0.0% 50.0% 50.0%
WAIS-R: Digit symbol (n = 2) 0.0% 50.0% 50.0%
WAIS-R: Picture completion (n = 2)
0.0% 50.0% 50.0%
WAIS-R: Information (n = 2) 0.0% 50.0% 50.0%
Language disability (n = 2) 0.0% 50.0% 50.0%
Number of neurological signs (n = 2)
0.0% 100.0% 0.0%

Predictor Variable
Direction of Empirical Effect
Negative
Positive
Non-Significant
Functional Impairment: Person with Dementia
ADL impairment (n = 34) 5.9% 58.8% 35.3% High quality (n = 19) 5.3% 57.9% 36.8%
Incontinence (n = 8) 0.0% 50.0% 50.0% High quality (n = 2) 0.0% 0.0% 100.0%
IADL impairment (n = 6) 16.7% 50.0% 33.3% High quality (n = 2) 0.0% 50.0% 50.0%
Negative physical health (n = 4)b 25.0% 0.0% 75.0%
Behavioral and Psychological Symptoms: Person with Dementia
Behavioral symptoms (n = 36)
2.8% 58.3% 38.9%
High quality (n = 13) 0.0% 53.8% 46.2%
Psychotic symptoms (n = 7) 0.0% 42.9% 57.1% High quality (n = 2) 0.0% 50.0% 50.0%
Depression (n = 6) 0.0% 83.3% 16.7% High quality (n = 2) 0.0% 100.0% 0.0%

Predictor Variable
Direction of Empirical Effect
Negative
Positive
Non-Significant
Medication Use Tacrine/Cholinesterase inhibitors (n = 6)
50.0% 33.3% 16.7%
High quality (n = 2) 50.0% 0.0% 50.0%
Rivastigimine use vs. no drug (n = 2)
50.0% 50.0% 0.0%

Predictor Variable
Direction of Empirical Effect
Negativea
Positivea
Non-Significant
Caregiver Sociodemographics Caregiver is spouse (n = 11) 38.5% 0.0% 61.5% High quality (n = 4) 25.0% 0.0% 75.0% Caregiver is wife (n = 2) 0.0% 0.0% 100.0% High quality (n = 2) 0.0% 0.0% 100.0%
Caregiver is husband (n = 2) 0.0% 0.0% 100.0% High quality (n = 2) 0.0% 0.0% 100.0% Caregiver is adult child (n = 3) 33.3% 0.0% 66.7%
Caregiver is related to patient (n = 2)
0.0% 50.0% 50.0%
High quality (n = 2) 0.0% 50.0% 50.0%
Caregiver age (n = 11) 9.1% 36.4% 54.5% High quality (n = 6) 0.0% 66.7% 33.3% Caregiver education (n = 9) 22.2% 0.0% 77.8% High quality (n = 4) 25.0% 0.0% 75.0% Caregiver is female (n = 8) 12.5% 0.0% 87.5% High quality (n = 4) 0.0% 0.0% 100.0% Caregiver income (n = 5) 20.0% 40.0% 40.0% High quality (n = 2) 50.0% 50.0% 0.0% Duration of caregiving (n = 5) 60.0% 0.0% 40.0% High quality (n = 3) 33.3% 0.0% 66.7% Caregiver is employed (n = 2) 0.0% 0.0% 100.0%

Predictor Variable
Direction of Empirical Effect
Negative
Positive
Non-Significant
Caregiving Stressors Caregiver stress (n = 16) 0.0% 68.8% 31.2% High quality (n = 5) 0.0% 80.0% 20.0% Caregiver desire to institutionalize (n = 6)
0.0% 100.0% 0.0%
High quality (n = 2) 0.0% 100.0% 0.0% Role overload (n = 4) 0.0% 25.0% 75.0% High quality (n = 2) 0.0% 0.0% 100.0% Role captivity (n = 4) 0.0% 100.0% 0.0% High quality (n = 2) 0.0% 100.0% 0.0% Caregiver unmet need (n = 3) 0.0% 33.3% 66.7% Caregiving hours (n = 3) 0.0% 66.7% 33.3% High quality (n = 2) 0.0% 50.0% 50.0% Caregiver economic strain (n = 2)
50.0% 0.0% 50.0%
Caregiver reaction to behavioral symptoms of dementia (n = 2)
0.0% 50.0% 50.0%

Predictor Variable
Direction of Empirical Effect
Negative
Positive
Non-Significant
Caregiver Well-Being Caregiver psychological distress (n = 15)
6.7% 26.7% 66.7%
High quality (n = 6) 0.0% 25.0% 75.0% Caregiver health (n = 12) 50.0% 8.3% 41.7% High quality (n = 6) 50.0% 16.7% 33.3% Caregiving Psychosocial Resources
Social support (n = 11) 18.2% 18.2% 63.6% High quality (n = 4) 25.0% 50.0% 25.0% Family help to caregivers (n = 6)
16.7% 16.7% 66.7%
High quality (n = 2) 0.0% 0.0% 100.0% Uplifts/satisfaction with caregiving (n = 6)
16.7% 16.7% 66.7%
High quality (n = 4) 25.0% 25.0% 50.0% Quality of caregiver-patient relationship (n = 5)
40.0% 0.0% 60.0%
High quality (n = 2) 50.0% 0.0% 50.0% Caregiver satisfaction with leisure (n = 3)
33.3% 0.0% 66.7%
Caregiver coping: Active (n = 2) 0.0% 50.0% 50.0% Caregiver mastery (n = 2) 50.0% 50.0% 0.0%

Predictor Variable
Direction of Empirical Effect
Negative
Positive
Non-Significant
Service Use Total service use (n = 8) 0.0% 37.5% 62.5% High quality (n = 3) 0.0% 33.3% 66.7% Caregiver supportive services (n = 6)
0.0% 60.0% 40.0%
Hospitalization (n = 3) 0.0% 33.3% 66.7% Adult day service use (n = 3) 0.0% 33.3% 66.7% In-home service use (n = 3) 33.3% 33.3% 33.3% Assisted living (n = 2) 0.0% 50.0% 50.0%

DISCUSSION
Sociodemographics: Lack of consistent effect
AD diagnosis: What does it mean?
How critical events are assessed (e.g., incontinence)
The importance of caregiving stress • In particular, specific dimensions, such as role captivity
(Pearlin et al., 1990) and desire to institutionalize
CBLTC use: Lack of effect
Limitations

IMPLICATIONS
Intervention • Effectiveness of interventions to delay NHA in dementia
– Many pharmacological interventions do not consider NHA– Long-term use of ACE-inhibitors or Vitamin E may delay
NHA, but studies have methodological flaws
– Caregiver interventions, such as multi-component programs, appear effective (Mittelman et al., 2004); respite or other CBLTC options appear less so
Assessment: Who benefits most from these interventions?
Methodology: Consideration of endogeneity

QUESTION 2: WHAT HAPPENS TO DEMENTIA CAREGIVERS AFTER NHA?
Prior research suggests that caregiver depression and burden are present following a care recipient’s nursing home admission (NHA) (Aneshensel et al., 1995; Gaugler, Pot, & Zarit, 2007; Schulz et al., 2004).
Even recent work in this area rely on relatively small samples or follow-up intervals soon after NHA.
We have access to a multi-regional study of dementia caregiving (Newcomer et al., 1999) that includes data on over 1,000 caregivers who have provided up to 12 months of post-placement data.

ANALYSIS 2
Gaugler, J. E., Mittelman, M. S., Hepburn, K., & Newcomer, R. Predictors of caregiver adaptation across the nursing home transition. Manuscript under review. Psychology and Aging.

RESEARCH QUESTIONS
How does caregiver burden (emotional, social, and financial strain due to care responsibilities; Zarit et al., 1980) and depression change 6- and 12-months following NHA?
• Inconsistent findings in the literature
What factors predict change in caregiver burden and depression 6- and 12-months following NHA?
• Based on factors that predict NHA and prior research that has examined caregiving adaptation (i.e., change in burden and depression following NHA).

METHODS
Data were derived from a sub sample of the Medicare Alzheimer’s Disease Demonstration Evaluation (MADDE).
• 5,831 dementia caregivers were included at baseline from 8 catchment areas in the U.S from 1989-1994.
• Data were collected at 6-month intervals over a 3-year period
Post-placement cohorts were constructed. • 6-month post-placement cohort (pre-placement and
interview up to 6 months after NHA)• 12-month post-placement cohort (pre-placement,
interview up to 6 months post-placement, interview up to 12-months post-placement)

Baseline 6 months 12 months 18 months 24 months 30 months 36 months
5,831 4,707 3,735 2,992 2,397 1,5801,936
704 NHA
524 6
380 12
576 NHA
383 6
350 12
444 NHA
321 6
257 12
372 NHA
268 6
4 12
258 NHA
16 6
149 12
203 NHA
133 6
NOTE: NHA = nursing home admission; 6 = up to 6 months postplacement data; 12 = up to 12 months postplacement data
Number of caregivers with 6-month data on burden or depression: 1610Number of caregivers with 12-month data on burden or depression: 1116

PREDICTIVE DOMAINS
Background characteristics • Kin relationship, living arrangements, ethnicity/race,
duration of care, socioeconomic characteristics, site, time to NHA
Dementia severity (MMSE, Memory and Behavior Problem Checklist)Functional impairment (ADL/IADL dependencies) Formal, informal, and physical resources of caregiverOutcomes
• Zarit Burden Inventory (no established clinical cut-off)• Geriatric Depression Scale (score of >=6 on the GDS is
considered “high” depression; see Lyness et al., 1997; McDowell & Newell, 1996)

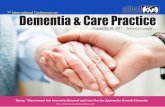
Figure 2. ROC curve for Zarit Burden Inventory at baseline (N = 5,831): “High” depression on GDS.
1.00.80.60.40.20.0
1 - Specificity
1.0
0.8
0.6
0.4
0.2
0.0
Sen
siti
vity
NOTE: Area = .814 (SE = .006) Sensitivity = 77% (screen positive); Specificity = 71% (screen negative)

ANALYSIS
Question 1: How does caregiver burden and depression change prior to and after NHA?
• 6-month post-placement panel: Paired sample T-Test• 12-month post-placement panel: Level 1 growth curve
model
Question 2: What factors predict change in caregiver adaptation following NHA?
• 6-month post-placement panel: Multivariate regression• 12-month post-placement panel: Level 2 growth curve
model

RESULTS: QUESTION 1
6-month post-placement panel• There was significant change in burden (df = 1609; t =
23.43, p < .001) with burden greater at pre-placement than at post-placement (M = 13.76 vs. M = 9.60).
• Depression also decreased significantly in the 6-month post-placement panel (df = 1594; t = 6.40, p < .001) (M = 4.79 at pre-placement vs. M = 4.18 at post-placement).

RESULTS: QUESTION 1
12-month post-placement panel• The Level 1 growth curve trajectories of the 12-month
post-placement panel also indicated significant and considerable decreases in burden following NHA (Mrate of
change = -3.30, p < .001) (M = 13.58 to 6.98)
• Unlike the 6-month panel, mean rate of change in depression was not significant (Mrate of change = 1.80, p > .05).

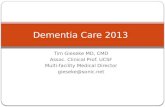
Caregiver healthCaregiver health
Time to NHATime to NHA
PreplacementPreplacementdepressiondepression
PreplacementPreplacementburdenburden
Caregiver ageCaregiver age
Caregiver is femaleCaregiver is female
Site: FloridaSite: Florida
Site: IllinoisSite: Illinois
Site: New YorkSite: New YorkChange in Change in Burden: Burden: PrePre--Post Post
PlacementPlacement
Change in Change in Depression: Depression:
PrePre--Post Post PlacementPlacement
RR2 2 = .36= .36
RR2 2 = .23= .23
df = 78, χ2 =124.70; p = .00;RMSEA = .02; NNFI = .98;CFI = .99; GFI = .99
PostplacementPostplacementhospital usehospital use
.07*.07*
.07*.07*
--.08*.08*--.08*.08*
--.12*.12*
.07*.07*
.05*.05*
.15**.15**
.05*.05*.06*.06*
--.65***.65***
.16*.16*--.50***.50***
.33***.33***
.15**.15**

PreplacementPreplacementCG CG ADLsADLs
Initial status: Initial status: DepressionDepression
Initial status: Initial status: BurdenBurden
Site: Site: OhioOhio
PreplacementPreplacementADLsADLs
Caregiver is Caregiver is spousespouse
Site: Site: FloridaFlorida
Site: Site: New YorkNew York
Rate of Rate of Change: Change: Burden Burden
Rate of Rate of Change: Change:
Depression: Depression:
.11*.11*RR2 2 = .32= .32
RR2 2 = .21= .21
--.16**.16**
--.44***.44***
df = 128 χ2 = 608.26; p = .00;RMSEA = .06; NNFI = .91;CFI = .96; GFI = .95
.26**.26**.26**.26**
.10*.10*--.12**.12**
.09*.09*
.09*.09*
.07*.07*
.09*.09*
--.43***.43***

DISCUSSION
Potential effects of NHA on burden, and over the shorter-term, depression
• Drop in burden appeared clinically relevant in both panels (6-month: M = 13.76 to 9.60; 12-month: M = 13.58 to 6.98)
Predictors to consider• Pre-placement burden, depression: Regression to the
mean, or something else?
• Spousal relationship: 12 months
• Various site differences
• Greater time to NHA, overnight hospital use (6-months)

IMPLICATIONS
Limitations:. • Type of care received in NH or other NH-relevant measures of
caregiver adaptation• Age of data: Emergence of assisted living
Measures to capture challenges specific to NHA• How the decision to institutionalization came about • How helpful the NH was in facilitating the move • Difficulty in finding an appropriate facility • Overall satisfaction with the institutionalization experience
Broadening our understanding of transitions • Assisted living• Transitions leading to other transitions
NHA: Less about prevention, more about finding the right time for the event?

QUESTION 3: DOES PSYCHOSOCIAL SUPPORT HELP CAREGIVERS DURING AND AFTER NHA?
Certain types of psychosocial interventions for caregivers can be effective in producing improvements in dementia caregiver outcomes (Gaugler, 2007)
Little research documents the effects of these interventions in easing the transition of NHA for family caregivers.
The goal: determine whether the availability of long-term counseling and support reduces burden and depressive symptomatology across the institutionalization transition.

ANALYSIS 3
Gaugler, J. E., Roth, D. L., Haley, W. E., & Mittelman, M. S. (2008). Can counseling and support reduce Alzheimer’s caregivers’ burden and depressive symptoms during the transition to institutionalization? Results from the NYU Caregiver Intervention study. Journal of the American Geriatrics Society, 56, 421-428.

METHODS
The New York University Aging and Dementia Research Center (NYU-ADRC) has been conducting a pioneering randomized trial of a psychosocial intervention for spouse–caregivers of people with AD since 1987 (NYUCI)
Participants were followed for up to 15.9 years. At least 10 years of follow-up data are available for 12% of the cases (n = 48).
The median times to NHA were 4.8 and 3.3 years after baseline for intervention and control care recipients, respectively.

METHODS
385 spouse caregivers were included; 210 institutionalized during the course of the study
Upon study intake, participants were administered an intensive baseline assessment protocol consisting of structured questionnaires.
Interviews were administered quarterly during the 1st year of participation, and every 6 months thereafter (including after NHA).


NYUCI
The NYUCI consisted of three components: individual and family counseling, support group participation, and ad hoc counseling.
• Counselors with advanced degrees in social work, psychology, counseling, or gerontology delivered the NYUCI.
• During the 4 months after the baseline assessment, spouse caregivers participated in six individual and family sessions with the study counselor.
• Caregivers agreed at intake that, after the 4-month follow-up, they would participate in a support group that met weekly under the auspices of the Alzheimer’s Association.
• The third component, provided throughout the duration of the NYUCI, was ad hoc counseling:
– Caregivers and participating family members were free to contact the study counselors by way of telephone to address any concerns, crises, or other significant changes that occurred.

ANALYSIS
The effects of the NYUCI on burden and depression were estimated and tested using random effects regression growth curve analyses.
A multilevel change model was used.
All analyses were conducted using restricted maximum likelihood estimation as provided by SAS PROC MIXED.
The models were based on 4,193 observations over time.• These included 3,055 observations during the community
caregiving phase and 1,148 observations of caregivers while the care recipients were in the nursing home.



DISCUSSION
Instead of attempting to avoid NHA entirely (or suggesting it too early), good clinical care demands that healthcare providers recognize when NHA is necessary.
The models also emphasize sustained benefit of comprehensive counseling and support for participants continuing to provide at-home care to spouses.
• There is a need to adopt similar long-term treatment strategies when implementing psychosocial interventions to manage the clinical multiyear course of AD.
Limitations

IMPLICATIONS
Balancing policy and family needs • The NYUCI is perhaps one such clinical approach that
can balance these two stakeholder needs.
Continuity of care for families and its benefits
The accumulation of high-quality evidence has made it possible to shift from demonstrations of efficacy to identification of strategies that facilitate translation.

WHERE DO WE GO FROM HERE?
Implementing the NYUCI for adult child caregivers in Minnesota, USA
• R01 AG022066
Developing a psychosocial intervention for families to navigate the NH transition
• R21 AG026525
Enhancing family involvement and interaction in the NH• R41 NR010642
Focusing on other transitions in dementia care: Onset and the early-stage of AD
• The Memory Club, Dementia Demonstration Project

INTERESTED IN COLLABORATING?
Joseph E. Gaugler, Ph.D.
Associate Professor
School of Nursing, Center on Aging
Coordinator of Research Initiatives, Center for Gerontological Nursing
University of Minnesota
Email: [email protected]
Telephone: 612-626-2485