
Analysis of Gut Microbiome and Diet Modification in ... · SOJ Microbiology & Infectious Diseases....
13
*Corresponding author email: [email protected] Symbiosis Group Symbiosis www.symbiosisonline.org www.symbiosisonlinepublishing.com Analysis of Gut Microbiome and Diet Modification in Patients with Crohn’s Disease Sumathi Sankaran Walters 1 *, Antonio Quiros 2,3 , Matthew Rolston 1 , Irina Grishina 1 , Jay Li 1 , Anne Fenton 1 , Todd Z. DeSantis 4 , Anne Thai 2 , Gary L Andersen 5 , Peggy Papathakis 6 , Raquel Nieves 7 , Thomas Prindiville 2 and Satya Dandekar 1 1 Department of Medical Microbiology and Immunology, University of CA Davis, USA 2 Department of Internal Medicine, University of CA Davis, Sacramento, USA 3 Division of Pediatric Gastroenterology MUSC Children’s Hospital, Charleston, SC, 4 Department of Bioinformatics, Second Genome, San Bruno, CA 94066. 5 Ecology Department, Lawrence Berkeley National Laboratory, Berkeley, CA 94720 6 Department of Nutrition, California Polytechnic State University, San Luis Obispo, CA, USA 7 Department of Pediatrics, David Grant Medical Center, Travis Air Force Base, California, 94535 SOJ Microbiology & Infectious Diseases Open Access Research Article Bowel Disease • The gut microbial balance can be altered by modifying the diet. • Taken together, the goal of this study was to follow changes in the gut microbiota by longitudinally analyzing the fecal microbiome in patients with IBD. What are the new findings? • The study has identified restricted microbial diversity associated with IBD. • Our study has demonstrated, for the first time, an enrichment of microbial diversity following the use of the specific carbohydrate diet. How might it impact on clinical practice in the foreseeable future? • Diet modification will be an important means to reduce symptoms and improve mucosal healing • Additional microbial modification using Probiotics could be beneficial. • Expansion of this study model can provide a definitive means to improve microbial diversity and mucosal health in IBD patients. Introduction Human intestine harbors trillions of diverse communities of commensal bacteria that are beneficial for the human health [1-4]. It has been estimated that over 100 trillion microbes belonging to over 500 species co-exist in the human colon [5]. Changes in the composition of intestinal microbiota have been observed in disease involving infectious and non-infectious Abstract Objective: The human intestine harbors trillions of commensal microbes that live in homeostasis with the host immune system. Changes in the composition and complexity of gut microbial communities are seen in inflammatory bowel disease (IBD), indicating disruption in host-microbe interactions. Multiple factors including diet and inflammatory conditions alter the microbial complexity. The goal of this study was to develop an optimized methodology for fecal sample processing and to detect changes in the gut microbiota of patients with Crohn’s disease receiving specialized diets. Design: Fecal samples were obtained from patients with Crohn’s disease in a pilot diet crossover trial comparing the effects of a specific carbohydrate diet (SCD) versus a low residue diet (LRD) on the composition and complexity of the gut microbiota and resolution of IBD symptoms. The gut microbiota composition was assessed using a high-density DNA microarray PhyloChip. Results: DNA extraction from fecal samples using a column based method provided consistent results. The complexity of the gut microbiome was lower in IBD patients compared to healthy controls. An increased abundance of Bacteroides fragilis (B. fragilis) was observed in fecal samples from IBD positive patients. The temporal response of gut microbiome to the SCD resulted in an increased microbial diversity while the LRD diet was associated with reduced diversity of the microbial communities. Conclusion: Changes in the composition and complexity of the gut microbiome were identified in response to specialized carbohydrate diet. The SCD was associated with restructuring of the gut microbial communities. Keywords: IBD; Crohn’s Disease; Fecal microbiome; Diet Modification; PhyloChip Received: February 24, 2014; Accepted: June 24, 2014; Published: June 27, 2014 *Corresponding author: Sumathi Sankaran Walters, Department of Medical Microbiology and Immunology, University of CA Davis, 5605A GBSF, One Shields Ave, Davis, CA 95616, USA, Ph: 530-754-7242; Fax: 530-754-7240, E-Mail: [email protected] Summary What is already known about this subject? • The interplay between the gut microbiota and mucosal health is of great importance especially in Inflammatory
Transcript of Analysis of Gut Microbiome and Diet Modification in ... · SOJ Microbiology & Infectious Diseases....
*Corresponding author email: [email protected] Group
Symbiosis www.symbiosisonline.org www.symbiosisonlinepublishing.com
Analysis of Gut Microbiome and Diet Modification in Patients with Crohn’s Disease
Sumathi Sankaran Walters1*, Antonio Quiros2,3, Matthew Rolston1, Irina Grishina1, Jay Li1, Anne Fenton1, Todd Z. DeSantis4, Anne Thai2, Gary L Andersen5, Peggy Papathakis6, Raquel
Nieves7, Thomas Prindiville2 and Satya Dandekar1
1Department of Medical Microbiology and Immunology, University of CA Davis, USA2Department of Internal Medicine, University of CA Davis, Sacramento, USA
3Division of Pediatric Gastroenterology MUSC Children’s Hospital, Charleston, SC, 4Department of Bioinformatics, Second Genome, San Bruno, CA 94066.
5Ecology Department, Lawrence Berkeley National Laboratory, Berkeley, CA 947206Department of Nutrition, California Polytechnic State University, San Luis Obispo, CA, USA
7Department of Pediatrics, David Grant Medical Center, Travis Air Force Base, California, 94535
SOJ Microbiology & Infectious Diseases Open AccessResearch Article
Bowel Disease
• Thegutmicrobialbalancecanbealteredbymodifyingthediet.
• Taken together, the goal of this study was to followchangesinthegutmicrobiotabylongitudinallyanalyzingthefecalmicrobiomeinpatientswithIBD.
Whatarethenewfindings?
• The study has identified restricted microbial diversityassociatedwithIBD.
• Our study has demonstrated, for the first time, anenrichmentofmicrobialdiversityfollowingtheuseofthespecificcarbohydratediet.
Howmight it impact on clinical practice in the foreseeablefuture?
• Dietmodificationwillbean importantmeans toreducesymptomsandimprovemucosalhealing
• AdditionalmicrobialmodificationusingProbioticscouldbebeneficial.
• Expansion of this studymodel can provide a definitivemeanstoimprovemicrobialdiversityandmucosalhealthinIBDpatients.
IntroductionHuman intestine harbors trillions of diverse communities
ofcommensalbacteriathatarebeneficial forthehumanhealth[1-4]. It has been estimated that over 100 trillion microbesbelonging toover500 species co-exist in thehuman colon [5]. Changes in the compositionof intestinalmicrobiotahavebeenobserved in disease involving infectious and non-infectious
AbstractObjective: Thehumanintestineharborstrillionsofcommensal
microbes that live in homeostasis with the host immune system.Changes in the composition and complexity of gut microbialcommunitiesareseenininflammatoryboweldisease(IBD),indicatingdisruption in host-microbe interactions. Multiple factors includingdietandinflammatoryconditionsalterthemicrobialcomplexity.Thegoalofthisstudywastodevelopanoptimizedmethodologyforfecalsample processing and to detect changes in the gutmicrobiota ofpatientswithCrohn’sdiseasereceivingspecializeddiets.
Design:FecalsampleswereobtainedfrompatientswithCrohn’sdisease in a pilot diet crossover trial comparing the effects of aspecificcarbohydratediet(SCD)versusalowresiduediet(LRD)onthecompositionandcomplexityofthegutmicrobiotaandresolutionof IBD symptoms. The gut microbiota composition was assessedusingahigh-densityDNAmicroarrayPhyloChip.
Results: DNA extraction from fecal samples using a columnbasedmethodprovidedconsistentresults.ThecomplexityofthegutmicrobiomewaslowerinIBDpatientscomparedtohealthycontrols.An increased abundance of Bacteroides fragilis (B. fragilis) wasobservedinfecalsamplesfromIBDpositivepatients.Thetemporalresponse of gut microbiome to the SCD resulted in an increasedmicrobialdiversitywhiletheLRDdietwasassociatedwithreduceddiversityofthemicrobialcommunities.
Conclusion: Changes in the composition and complexity ofthe gut microbiome were identified in response to specializedcarbohydratediet.TheSCDwasassociatedwithrestructuringofthegutmicrobialcommunities.
Keywords: IBD; Crohn’s Disease; Fecal microbiome; DietModification;PhyloChip
Received: February 24, 2014; Accepted: June 24, 2014; Published: June 27, 2014
*Corresponding author: Sumathi Sankaran Walters, Department of Medical Microbiology and Immunology, University of CA Davis, 5605A GBSF, One Shields Ave, Davis, CA 95616, USA, Ph: 530-754-7242; Fax: 530-754-7240, E-Mail: [email protected]
SummaryWhatisalreadyknownaboutthissubject?
• The interplay between the gutmicrobiota andmucosalhealthisofgreatimportanceespeciallyinInflammatory

Page2of13Citation:WaltersSS,QuirosA,RolstonM,GrishinaI,LiJ,etal.(2014)AnalysisofGutMicrobiomeandDietModificationinPatientswithCrohn’sDisease.SOJMicrobiolInfectDis2(3):1-13.DOI:http://dx.doi.org/10.15226/sojmid/2/3/00122
Analysis of Gut Microbiome and Diet Modification in Patients with Crohn’s Disease Copyright: © 2014 Walters et al.
etiologies [6-10]. Diet is known to cause changes in fecalMicrobiota [11,12]. Three predominant enterotypes have beenshowntobepresentinthehumangutmicrobiome:Bacteroides, Prevotella andRuminococcus [13]. Severalstudiessuggest thateach individual harbors his or her own distinctive pattern ofintestinalmicrofloracompositionthatisnotnecessarilydistinctbut isagradientmicrobialcommunity [14].Thispattern tendsto remain constant across timewith the exception of possibleage and Body Mass Index (BMI) related changes [15-17]. IBDandgastrointestinalcancersarethoughttoaffectthemicrofloracomposition and recent data supports such association [9,18-21]. Human feces provide a complex microbial niche and arereflectiveofthemicrobiotathatispresentinthelargeintestine[22-25]. Thus, analysis of the bacterial communities in humanfecesiswidelyutilizedtodeterminethechangesininfectiousornon-infectiousdiseases.
Culture-independent molecular methodologies havefacilitated more accurate and rapid detection of changes inmicrobial communities during various disease states [26,27].Thedetectionofabroad-rangeofcommensalbacteria isbasedonclassifyingheterogeneous16Sgenesamplifiedbypolymerasechainreaction(PCR)usingprimerswithbroadspecificity[28-30].Priorto2010thegeneralmethodofsamplingandcategorizingDNA from complex samples has been to clone or otherwisesegregate individual amplicons, then sequence a subset ofthem [28-30]. However, the number of sequences required toadequatelyquantifythepopulationlevelsofeachtaxainasampleis unwieldy. Additionally, newer high throughput sequencingtechnology has been used to study bacterial populations usingthe 16S sequences. While this technology is readily availablethecomplexanalyticaltoolsandexpertisenecessarytoanalyzethe data is not as readily available. Recent development of ahigh density microarray consisting of probes complementing16S genes has enabled researchers to performprofiling of themicrobesinagivensampleformonitoringchangesinthebacterialcommunities ina simpleand timeefficientmanner [31]. Thesemicroarrayshavebeenused inmonitoringmicrobes indiverseenvironmentsandindiseaseandareabletoprovideafingerprintof characterized sequences [32-34]. Specific microbiomesignature changes have been reported in inflammatory boweldisease,obesityand infectiousdiseasesandare considered forthediagnosisandmonitoringofthesedisorders. Thisprovidesanopportunitytodevelopmorenovelbiomarkersformonitoringdiseaseprogressionortherapeuticoutcomes.
Theuseofprobiotics,dietarypatternsandintakeofvariousnutrients can change profiles of fecal microflora [12, 35-37].Specific diets have been implicated to play a role in Crohn’sdisease.Thus,effortsweremadetoutilizespecializeddiets,suchas theSpecificCarbohydrateDiet™(SCD)and theLowResidueDiet (LRD), for restoring the gut microbiome and to improveintestinal health [38-41]. The SCD restricts theuse of complexcarbohydrates and has been advocated in the symptomaticmanagementofceliacdiseaseformanyyearssince1955[42-45].TheLRDisalowfiberdietandservestoprolongintestinaltransittime. This has been suggested to be beneficial in alleviating
Crohn’s disease symptoms with varying results [46]. Furtherinvestigationsareneededtogaininsightsintothecomplexityanddynamicsofthehumanmicrobiotainthecontextofvariousdietsformanaginggutinflammation.
Inthisstudy,weinvestigatedseveralmethodsoffecalsampleprocessingfortheirutility inprovidingthebestrepresentationof the fecal microbiome diversity. The aim of this study wasto demonstrate changes in the complexity of the microbiomein the longitudinal fecal samples following diet modificationusing culture independent high-density microarrays, the 16SPhyloChip.WeexaminedtheimpactofIBDaswellastheSCDorLRDdietmodificationontherestructuringofthegutmicrobiota.
MethodsStudy subjects and experimental design
This studywasdesigned inpart to investigate the effect ofDNAextractionmethodsontheabilitytodetectchanges inthecomplexityoffecalmicrobiomeofhealthycontrolsandpatientswith Crohn’s disease and to investigate the effects that diethas on restoring the gutmicrobial complexity in patientswithCrohn’sdisease.TheSCDandLRDwereselected to investigatetheir effects on the alleviation of the clinical symptoms ofCrohn’s disease. Previous anecdotal reports suggested a wideuseofLRDbypatientsandapotentialofenhancedrelief fromclinicalsymptomsofCrohn’sdiseasewiththeuseofSCD[47-49].ParticipantswereenrolledinthestudyatthepediatricandadultIBDclinicsatUCDavisMedicalCenter(Sacramento,CA)asperIRBapprovedprotocols.
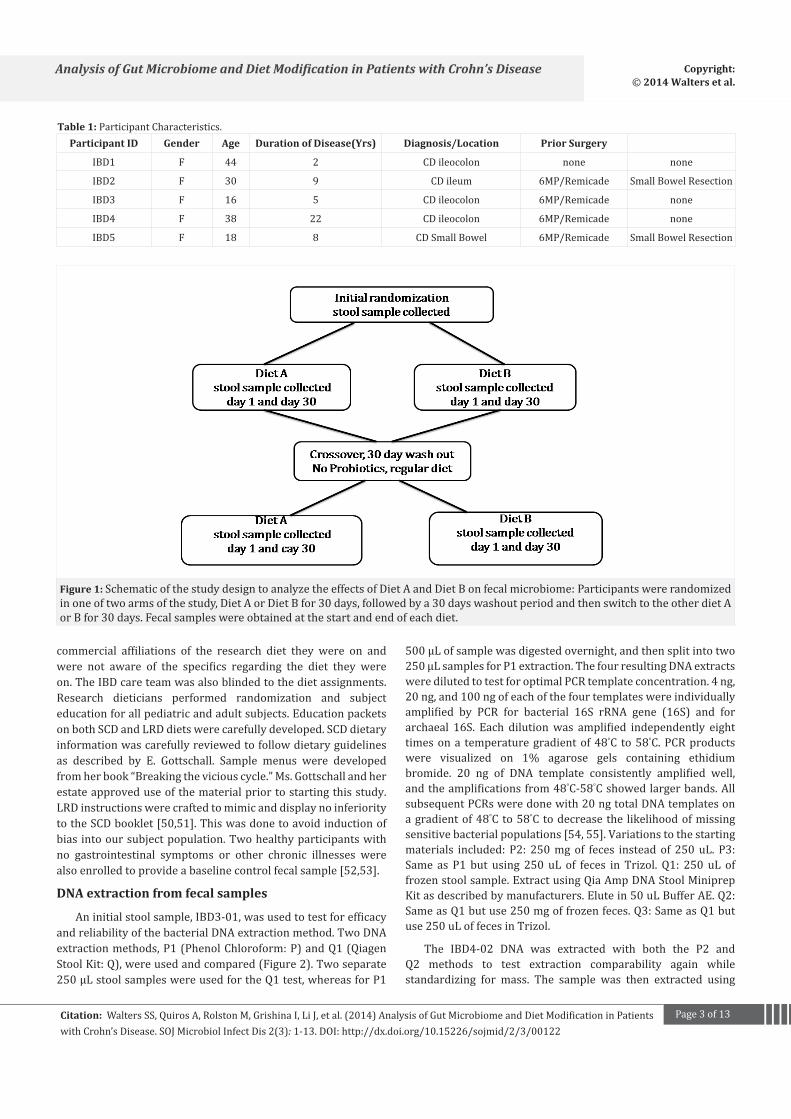
Eightparticipants,aged16-50years(Table1)whomet theinclusion criteria were enrolled in this study. All participantswere Caucasian. Two participantswere healthy controlswhilesixparticipantshadadiagnosisofCrohn’sdisease(CD).Inclusioncriteria for the CD cohort included: 1) confirmed diagnosis ofCD,2) in clinical remission3)noProbioticsuseand4)willingto sign consent form for enrollment into the trial. Exclusioncriteriaincluded:1)failuretomeetanyoftheinclusioncriteria,2) poor compliance with the diet during the study phase, 3)failuretosubmitstoolsamplesasindicatedateachphaseofthestudy,and4)needforantibioticuseduringthestudy.Subjectswere randomized to either diet A (LRD) or diet B (SCD) andan education booklet was provided to them describing theresearchdiet and samplemenus. Stool sampleswere collectedonday1and30(Figure1).Atwentyfour-hourdietaryrecallwasperformedby the traineddietitiansover thephone.After theirinitial30dayperiod,patientswentona“washout”phasefor30days.Duringthisperiodtheparticipantsresumedtheirnormalpre-studydiet.Afterwashoutperiod,patientsreturnedtoclinicand the second 30-day trial period began. Stool sampleswerecollected again at the beginning and after 30 days on the trialdiet.StandardIBDquestionnaires(IBDQ)werecollectedfromallsubjectsatthebeginningandendofthestudytoaccessclinicaloutcome.Lossofcomplianceorworseningoftheclinicaldiseasestateautomaticallyexcludedthemfromcontinuingthestudy.
All patients were blind to the specific names and any
Page3of13Citation:WaltersSS,QuirosA,RolstonM,GrishinaI,LiJ,etal.(2014)AnalysisofGutMicrobiomeandDietModificationinPatientswithCrohn’sDisease.SOJMicrobiolInfectDis2(3):1-13.DOI:http://dx.doi.org/10.15226/sojmid/2/3/00122
Analysis of Gut Microbiome and Diet Modification in Patients with Crohn’s Disease Copyright: © 2014 Walters et al.
Participant ID Gender Age Duration of Disease(Yrs) Diagnosis/Location Prior Surgery
IBD1 F 44 2 CD ileocolon none none
IBD2 F 30 9 CD ileum 6MP/Remicade SmallBowelResection
IBD3 F 16 5 CD ileocolon 6MP/Remicade none
IBD4 F 38 22 CD ileocolon 6MP/Remicade none
IBD5 F 18 8 CDSmallBowel 6MP/Remicade SmallBowelResection
Table 1:ParticipantCharacteristics.
Figure 1: SchematicofthestudydesigntoanalyzetheeffectsofDietAandDietBonfecalmicrobiome: Participantswererandomizedinoneoftwoarmsofthestudy,DietAorDietBfor30days,followedbya30dayswashoutperiodandthenswitchtotheotherdietAorBfor30days.Fecalsampleswereobtainedatthestartandendofeachdiet.
commercial affiliations of the research diet they were on andwere not aware of the specifics regarding the diet they wereon.TheIBDcareteamwasalsoblindedtothedietassignments.Research dieticians performed randomization and subjecteducationforallpediatricandadultsubjects.EducationpacketsonbothSCDandLRDdietswerecarefullydeveloped.SCDdietaryinformationwascarefullyreviewedtofollowdietaryguidelinesas described by E. Gottschall. Sample menus were developedfromherbook“Breakingtheviciouscycle.”Ms.Gottschallandherestateapproveduseofthematerialpriortostartingthisstudy.LRDinstructionswerecraftedtomimicanddisplaynoinferioritytotheSCDbooklet[50,51].Thiswasdonetoavoidinductionofbias intooursubjectpopulation.Twohealthyparticipantswithno gastrointestinal symptoms or other chronic illnesses werealsoenrolledtoprovideabaselinecontrolfecalsample[52,53].
DNA extraction from fecal samples
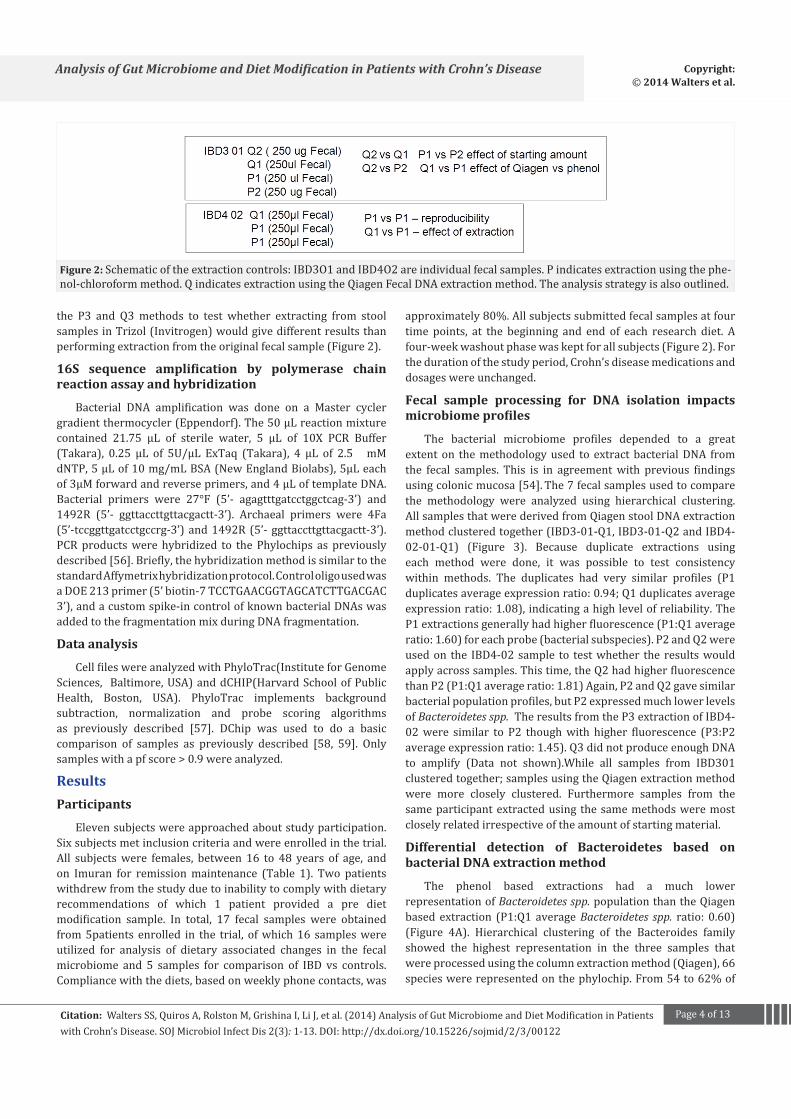
Aninitialstoolsample,IBD3-01,wasusedtotestforefficacyandreliabilityofthebacterialDNAextractionmethod.TwoDNAextractionmethods,P1(PhenolChloroform:P)andQ1(QiagenStoolKit:Q),wereusedandcompared(Figure2).Twoseparate250µLstoolsampleswereusedfortheQ1test,whereasforP1
500µLofsamplewasdigestedovernight,andthensplitintotwo250µLsamplesforP1extraction.ThefourresultingDNAextractsweredilutedtotestforoptimalPCRtemplateconcentration.4ng,20ng,and100ngofeachofthefourtemplateswereindividuallyamplified by PCR for bacterial 16S rRNA gene (16S) and forarchaeal 16S. Each dilutionwas amplified independently eighttimesona temperaturegradientof48°C to58°C.PCRproductswere visualized on 1% agarose gels containing ethidiumbromide. 20 ng of DNA template consistently amplified well,andtheamplificationsfrom48°C-58°Cshowedlargerbands.AllsubsequentPCRsweredonewith20ngtotalDNAtemplatesonagradientof48°Cto58°Ctodecreasethe likelihoodofmissingsensitivebacterialpopulations[54,55].Variationstothestartingmaterials included: P2: 250mgof feces instead of 250uL. P3:Same as P1 but using 250 uL of feces in Trizol. Q1: 250 uL offrozenstoolsample.ExtractusingQiaAmpDNAStoolMiniprepKitasdescribedbymanufacturers.Elutein50uLBufferAE.Q2:SameasQ1butuse250mgoffrozenfeces.Q3:SameasQ1butuse250uLoffecesinTrizol.
The IBD4-02 DNA was extracted with both the P2 andQ2 methods to test extraction comparability again whilestandardizing for mass. The sample was then extracted using
Page4of13Citation:WaltersSS,QuirosA,RolstonM,GrishinaI,LiJ,etal.(2014)AnalysisofGutMicrobiomeandDietModificationinPatientswithCrohn’sDisease.SOJMicrobiolInfectDis2(3):1-13.DOI:http://dx.doi.org/10.15226/sojmid/2/3/00122
Analysis of Gut Microbiome and Diet Modification in Patients with Crohn’s Disease Copyright: © 2014 Walters et al.
Figure 2: Schematicoftheextractioncontrols: IBD3O1andIBD4O2areindividualfecalsamples.Pindicatesextractionusingthephe-nol-chloroformmethod.QindicatesextractionusingtheQiagenFecalDNAextractionmethod.Theanalysisstrategyisalsooutlined.
the P3 and Q3methods to test whether extracting from stoolsamplesinTrizol(Invitrogen)wouldgivedifferentresultsthanperformingextractionfromtheoriginalfecalsample(Figure2).
16S sequence amplification by polymerase chain reaction assay and hybridization
Bacterial DNA amplification was done on a Master cyclergradientthermocycler(Eppendorf).The50µLreactionmixturecontained 21.75 µL of sterile water, 5 µL of 10X PCR Buffer(Takara), 0.25 µL of 5U/µL ExTaq (Takara), 4 µL of 2.5 mMdNTP,5µLof10mg/mLBSA(NewEnglandBiolabs),5µLeachof3µMforwardandreverseprimers,and4µLoftemplateDNA.Bacterial primers were 27°F (5’- agagtttgatcctggctcag-3’) and1492R (5’- ggttaccttgttacgactt-3’). Archaeal primers were 4Fa(5’-tccggttgatcctgccrg-3’)and1492R(5’-ggttaccttgttacgactt-3’).PCRproductswerehybridized to thePhylochips as previouslydescribed[56].Briefly,thehybridizationmethodissimilartothestandardAffymetrixhybridizationprotocol.ControloligousedwasaDOE213primer(5’biotin-7TCCTGAACGGTAGCATCTTGACGAC3’),andacustomspike-incontrolofknownbacterialDNAswasaddedtothefragmentationmixduringDNAfragmentation.
Data analysis
CellfileswereanalyzedwithPhyloTrac(InstituteforGenomeSciences, Baltimore,USA)anddCHIP(HarvardSchoolofPublicHealth, Boston, USA). PhyloTrac implements backgroundsubtraction, normalization and probe scoring algorithmsas previously described [57]. DChip was used to do a basiccomparison of samples as previously described [58, 59]. Onlysampleswithapfscore>0.9wereanalyzed.
ResultsParticipants
Elevensubjectswereapproachedaboutstudyparticipation.Sixsubjectsmetinclusioncriteriaandwereenrolledinthetrial.All subjectswere females, between 16 to 48 years of age, andon Imuran for remissionmaintenance (Table 1). Two patientswithdrewfromthestudyduetoinabilitytocomplywithdietaryrecommendations of which 1 patient provided a pre dietmodification sample. In total, 17 fecal samples were obtainedfrom5patients enrolled in the trial, ofwhich16 sampleswereutilized for analysis of dietary associated changes in the fecalmicrobiome and 5 samples for comparison of IBD vs controls.Compliancewiththediets,basedonweeklyphonecontacts,was
approximately80%.Allsubjectssubmittedfecalsamplesatfourtime points, at the beginning and end of each research diet. Afour-weekwashoutphasewaskeptforallsubjects(Figure2).Forthedurationofthestudyperiod,Crohn’sdiseasemedicationsanddosageswereunchanged.
Fecal sample processing for DNA isolation impacts microbiome profiles
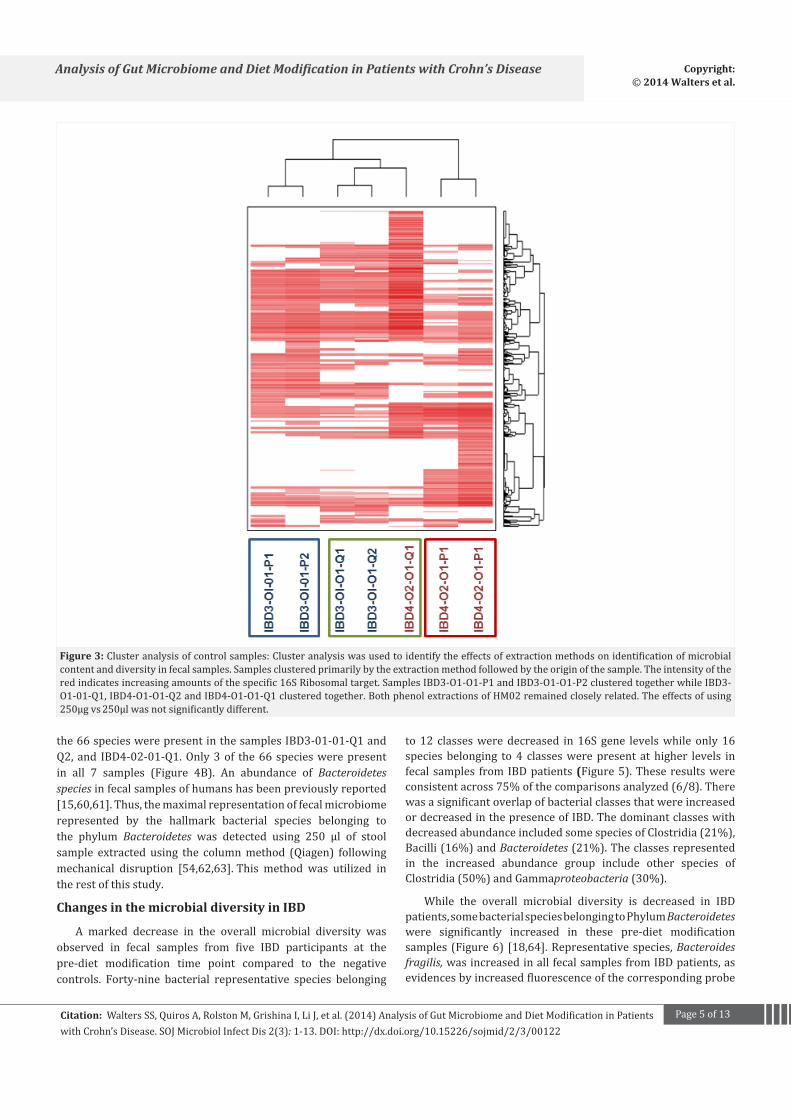
The bacterial microbiome profiles depended to a greatextenton themethodologyused to extractbacterialDNA fromthe fecal samples. This is in agreementwith previous findingsusingcolonicmucosa[54]. The7fecalsamplesusedtocomparethe methodology were analyzed using hierarchical clustering.AllsamplesthatwerederivedfromQiagenstoolDNAextractionmethodclusteredtogether(IBD3-01-Q1,IBD3-01-Q2andIBD4-02-01-Q1) (Figure 3). Because duplicate extractions usingeach method were done, it was possible to test consistencywithin methods. The duplicates had very similar profiles (P1duplicatesaverageexpressionratio:0.94;Q1duplicatesaverageexpressionratio:1.08),indicatingahighlevelofreliability.TheP1extractionsgenerallyhadhigherfluorescence(P1:Q1averageratio:1.60)foreachprobe(bacterialsubspecies).P2andQ2wereusedon the IBD4-02sample to testwhether the resultswouldapplyacrosssamples.Thistime,theQ2hadhigherfluorescencethanP2(P1:Q1averageratio:1.81)Again,P2andQ2gavesimilarbacterialpopulationprofiles,butP2expressedmuchlowerlevelsofBacteroidetes spp. TheresultsfromtheP3extractionofIBD4-02were similar to P2 thoughwith higher fluorescence (P3:P2averageexpressionratio:1.45).Q3didnotproduceenoughDNAto amplify (Data not shown).While all samples from IBD301clusteredtogether;samplesusingtheQiagenextractionmethodwere more closely clustered. Furthermore samples from thesameparticipantextractedusing thesamemethodsweremostcloselyrelatedirrespectiveoftheamountofstartingmaterial.
Differential detection of Bacteroidetes based on bacterial DNA extraction method
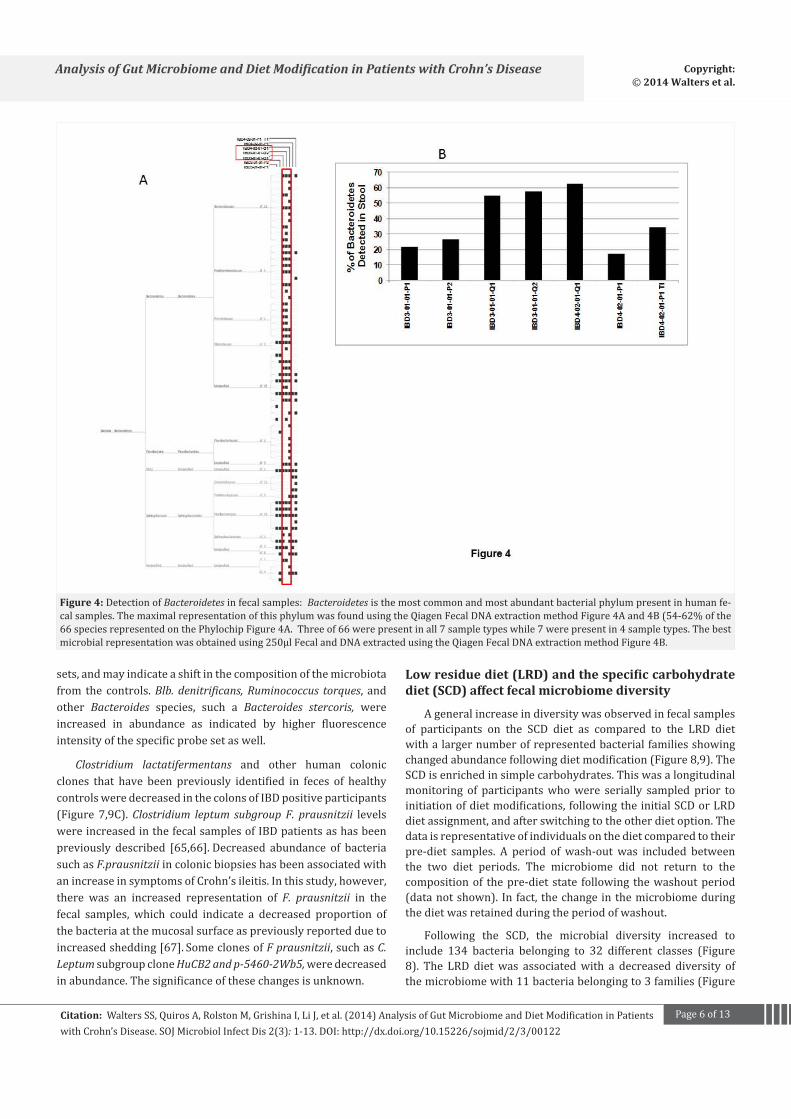
The phenol based extractions had a much lowerrepresentationofBacteroidetes spp.populationthantheQiagenbased extraction (P1:Q1 averageBacteroidetes spp. ratio: 0.60)(Figure 4A). Hierarchical clustering of the Bacteroides familyshowed the highest representation in the three samples thatwereprocessedusingthecolumnextractionmethod(Qiagen),66specieswererepresentedonthephylochip.From54to62%of
Page5of13Citation:WaltersSS,QuirosA,RolstonM,GrishinaI,LiJ,etal.(2014)AnalysisofGutMicrobiomeandDietModificationinPatientswithCrohn’sDisease.SOJMicrobiolInfectDis2(3):1-13.DOI:http://dx.doi.org/10.15226/sojmid/2/3/00122
Analysis of Gut Microbiome and Diet Modification in Patients with Crohn’s Disease Copyright: © 2014 Walters et al.
Figure 3: Clusteranalysisofcontrolsamples:Clusteranalysiswasusedtoidentifytheeffectsofextractionmethodsonidentificationofmicrobialcontentanddiversityinfecalsamples.Samplesclusteredprimarilybytheextractionmethodfollowedbytheoriginofthesample.Theintensityoftheredindicatesincreasingamountsofthespecific16SRibosomaltarget.SamplesIBD3-O1-O1-P1andIBD3-O1-O1-P2clusteredtogetherwhileIBD3-O1-01-Q1,IBD4-O1-O1-Q2andIBD4-O1-O1-Q1clusteredtogether.BothphenolextractionsofHM02remainedcloselyrelated.Theeffectsofusing250µgvs 250µlwasnotsignificantlydifferent.
the66specieswerepresentinthesamplesIBD3-01-01-Q1andQ2,and IBD4-02-01-Q1.Only3of the66specieswerepresentin all 7 samples (Figure 4B). An abundance of Bacteroidetes speciesinfecalsamplesofhumanshasbeenpreviouslyreported[15,60,61].Thus,themaximalrepresentationoffecalmicrobiomerepresented by the hallmark bacterial species belonging tothe phylum Bacteroidetes was detected using 250 µl of stoolsample extracted using the columnmethod (Qiagen) followingmechanical disruption [54,62,63]. This method was utilized intherestofthisstudy.
Changes in the microbial diversity in IBD
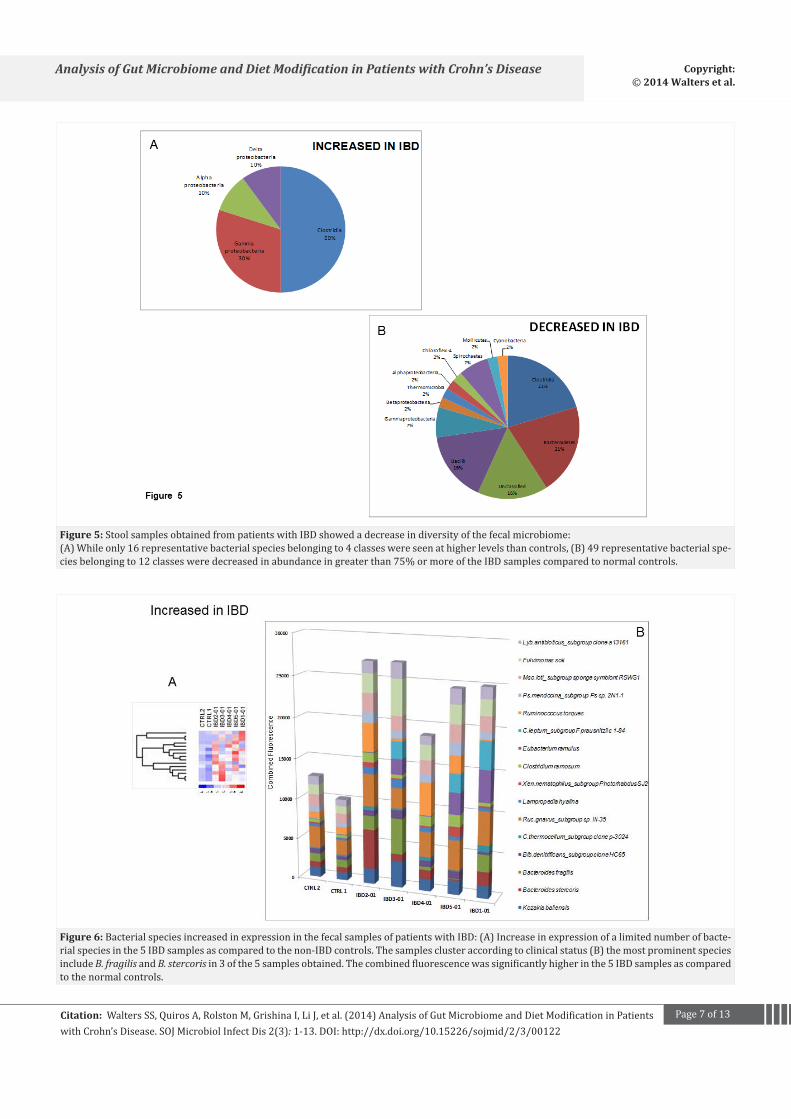
A marked decrease in the overall microbial diversity wasobserved in fecal samples from five IBD participants at thepre-diet modification time point compared to the negativecontrols. Forty-nine bacterial representative species belonging
to12 classesweredecreased in16S gene levelswhile only16speciesbelonging to4 classeswerepresent at higher levels infecal samples fromIBDpatients (Figure5).Theseresultswereconsistentacross75%ofthecomparisonsanalyzed(6/8).TherewasasignificantoverlapofbacterialclassesthatwereincreasedordecreasedinthepresenceofIBD.ThedominantclasseswithdecreasedabundanceincludedsomespeciesofClostridia(21%),Bacilli(16%)andBacteroidetes(21%).Theclassesrepresentedin the increased abundance group include other species ofClostridia(50%)andGammaproteobacteria(30%).
While the overall microbial diversity is decreased in IBDpatients,somebacterialspeciesbelongingtoPhylumBacteroidetes were significantly increased in these pre-diet modificationsamples(Figure6) [18,64].Representativespecies,Bacteroides fragilis,wasincreasedinallfecalsamplesfromIBDpatients,asevidencesbyincreasedfluorescenceofthecorrespondingprobe
Page6of13Citation:WaltersSS,QuirosA,RolstonM,GrishinaI,LiJ,etal.(2014)AnalysisofGutMicrobiomeandDietModificationinPatientswithCrohn’sDisease.SOJMicrobiolInfectDis2(3):1-13.DOI:http://dx.doi.org/10.15226/sojmid/2/3/00122
Analysis of Gut Microbiome and Diet Modification in Patients with Crohn’s Disease Copyright: © 2014 Walters et al.
Figure 4: DetectionofBacteroidetesinfecalsamples: Bacteroidetesisthemostcommonandmostabundantbacterialphylumpresentinhumanfe-calsamples.ThemaximalrepresentationofthisphylumwasfoundusingtheQiagenFecalDNAextractionmethodFigure4Aand4B(54-62%ofthe66speciesrepresentedonthePhylochipFigure4A.Threeof66werepresentinall7sampletypeswhile7werepresentin4sampletypes.Thebestmicrobialrepresentationwasobtainedusing250µlFecalandDNAextractedusingtheQiagenFecalDNAextractionmethodFigure4B.
sets,andmayindicateashiftinthecompositionofthemicrobiotafrom the controls.Blb. denitrificans, Ruminococcus torques, andother Bacteroides species, such a Bacteroides stercoris, were increased in abundance as indicated by higher fluorescenceintensityofthespecificprobesetaswell.
Clostridium lactatifermentans and other human colonicclones that have been previously identified in feces of healthycontrolsweredecreasedinthecolonsofIBDpositiveparticipants(Figure 7,9C).Clostridium leptum subgroup F. prausnitzii levelswereincreasedinthefecalsamplesofIBDpatientsashasbeenpreviously described [65,66]. Decreased abundance of bacteriasuch as F.prausnitziiincolonicbiopsieshasbeenassociatedwithanincreaseinsymptomsofCrohn’sileitis.Inthisstudy,however,there was an increased representation of F. prausnitzii in thefecal samples, which could indicate a decreased proportion ofthebacteriaatthemucosalsurfaceaspreviouslyreportedduetoincreasedshedding[67]. SomeclonesofF prausnitzii,suchasC. Leptum subgroup clone HuCB2 and p-5460-2Wb5, weredecreasedinabundance.Thesignificanceofthesechangesisunknown.
Low residue diet (LRD) and the specific carbohydrate diet (SCD) affect fecal microbiome diversity
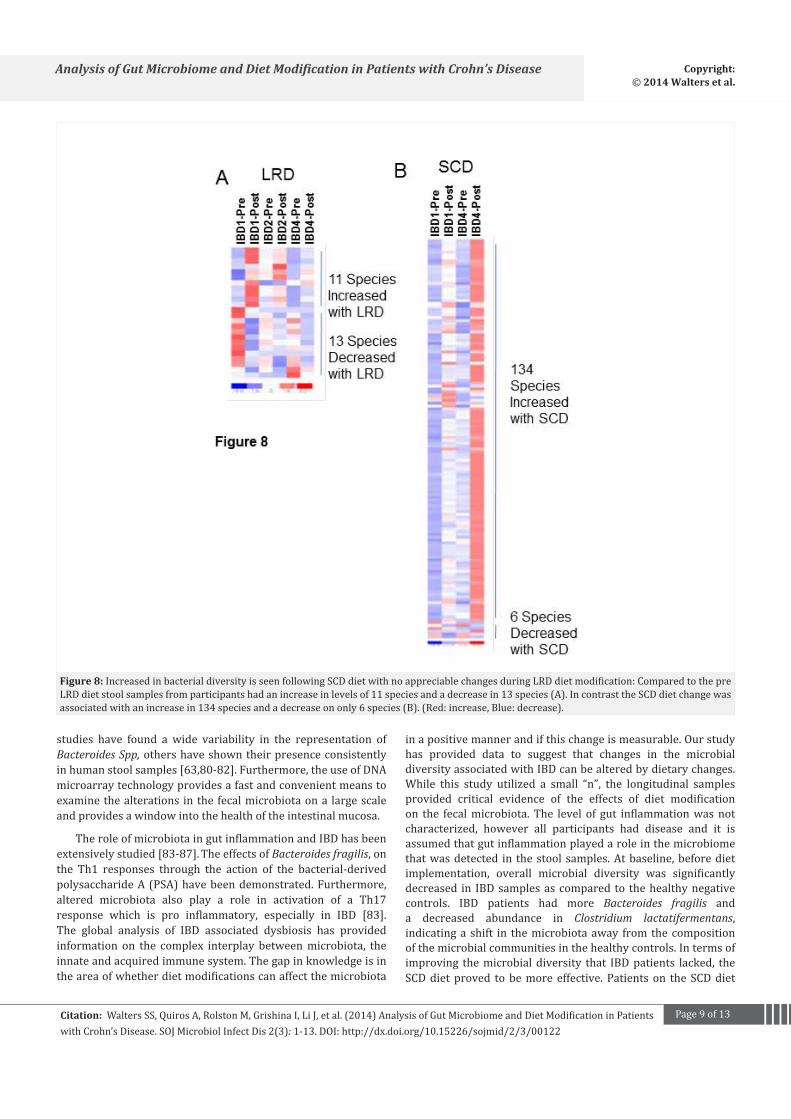
Ageneralincreaseindiversitywasobservedinfecalsamplesof participants on the SCD diet as compared to the LRD dietwithalargernumberofrepresentedbacterialfamiliesshowingchangedabundancefollowingdietmodification(Figure8,9).TheSCDisenrichedinsimplecarbohydrates.Thiswasalongitudinalmonitoring of participantswhowere serially sampled prior toinitiationofdietmodifications,followingtheinitialSCDorLRDdietassignment,andafterswitchingtotheotherdietoption.Thedataisrepresentativeofindividualsonthedietcomparedtotheirpre-diet samples. A period of wash-outwas included betweenthe two diet periods. The microbiome did not return to thecompositionof thepre-dietstate following thewashoutperiod(datanotshown). In fact, thechange inthemicrobiomeduringthedietwasretainedduringtheperiodofwashout.
Following the SCD, the microbial diversity increased toinclude 134 bacteria belonging to 32 different classes (Figure8). The LRD dietwas associatedwith a decreased diversity ofthemicrobiomewith11bacteriabelongingto3families (Figure
Page7of13Citation:WaltersSS,QuirosA,RolstonM,GrishinaI,LiJ,etal.(2014)AnalysisofGutMicrobiomeandDietModificationinPatientswithCrohn’sDisease.SOJMicrobiolInfectDis2(3):1-13.DOI:http://dx.doi.org/10.15226/sojmid/2/3/00122
Analysis of Gut Microbiome and Diet Modification in Patients with Crohn’s Disease Copyright: © 2014 Walters et al.
Figure 5: StoolsamplesobtainedfrompatientswithIBDshowedadecreaseindiversityofthefecalmicrobiome:(A)Whileonly16representativebacterialspeciesbelongingto4classeswereseenathigherlevelsthancontrols,(B)49representativebacterialspe-ciesbelongingto12classesweredecreasedinabundanceingreaterthan75%ormoreoftheIBDsamplescomparedtonormalcontrols.
Figure 6: BacterialspeciesincreasedinexpressioninthefecalsamplesofpatientswithIBD:(A)Increaseinexpressionofalimitednumberofbacte-rialspeciesinthe5IBDsamplesascomparedtothenon-IBDcontrols.Thesamplesclusteraccordingtoclinicalstatus(B)themostprominentspeciesincludeB. fragilis andB. stercorisin3ofthe5samplesobtained.Thecombinedfluorescencewassignificantlyhigherinthe5IBDsamplesascomparedtothenormalcontrols.
Page8of13Citation:WaltersSS,QuirosA,RolstonM,GrishinaI,LiJ,etal.(2014)AnalysisofGutMicrobiomeandDietModificationinPatientswithCrohn’sDisease.SOJMicrobiolInfectDis2(3):1-13.DOI:http://dx.doi.org/10.15226/sojmid/2/3/00122
Analysis of Gut Microbiome and Diet Modification in Patients with Crohn’s Disease Copyright: © 2014 Walters et al.
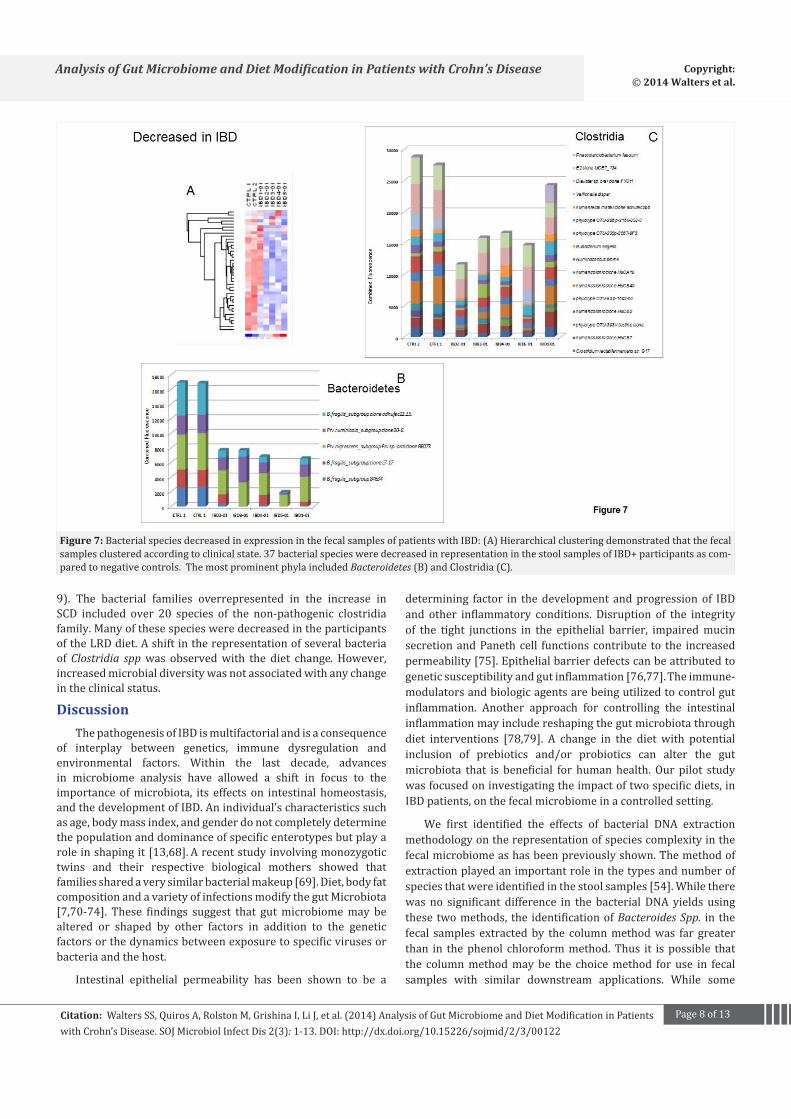
Figure 7: BacterialspeciesdecreasedinexpressioninthefecalsamplesofpatientswithIBD:(A)Hierarchicalclusteringdemonstratedthatthefecalsamplesclusteredaccordingtoclinicalstate.37bacterialspeciesweredecreasedinrepresentationinthestoolsamplesofIBD+participantsascom-paredtonegativecontrols.ThemostprominentphylaincludedBacteroidetes (B)andClostridia(C).
9). The bacterial families overrepresented in the increase inSCD included over 20 species of the non-pathogenic clostridiafamily.ManyofthesespeciesweredecreasedintheparticipantsoftheLRDdiet.AshiftintherepresentationofseveralbacteriaofClostridia sppwas observedwith the diet change. However,increasedmicrobialdiversitywasnotassociatedwithanychangeintheclinicalstatus.
DiscussionThepathogenesisofIBDismultifactorialandisaconsequence
of interplay between genetics, immune dysregulation andenvironmental factors. Within the last decade, advancesin microbiome analysis have allowed a shift in focus to theimportanceofmicrobiota, its effects on intestinal homeostasis,andthedevelopmentofIBD.Anindividual’scharacteristicssuchasage,bodymassindex,andgenderdonotcompletelydeterminethepopulationanddominanceofspecificenterotypesbutplayaroleinshapingit[13,68]. Arecentstudyinvolvingmonozygotictwins and their respective biological mothers showed thatfamiliessharedaverysimilarbacterialmakeup[69].Diet,bodyfatcompositionandavarietyofinfectionsmodifythegutMicrobiota[7,70-74]. These findings suggest that gutmicrobiomemay bealtered or shaped by other factors in addition to the geneticfactorsorthedynamicsbetweenexposuretospecificvirusesorbacteriaandthehost.
Intestinal epithelial permeability has been shown to be a
determining factor in thedevelopment andprogressionof IBDand other inflammatory conditions. Disruption of the integrityof the tight junctions in the epithelial barrier, impairedmucinsecretionandPanethcell functionscontribute to the increasedpermeability[75].Epithelialbarrierdefectscanbeattributedtogeneticsusceptibilityandgutinflammation[76,77]. Theimmune-modulatorsandbiologicagentsarebeingutilizedtocontrolgutinflammation. Another approach for controlling the intestinalinflammationmayincludereshapingthegutmicrobiotathroughdiet interventions [78,79]. A change in the diet with potentialinclusion of prebiotics and/or probiotics can alter the gutmicrobiota that is beneficial for humanhealth.Our pilot studywasfocusedoninvestigatingtheimpactoftwospecificdiets,inIBDpatients,onthefecalmicrobiomeinacontrolledsetting.
We first identified the effects of bacterial DNA extractionmethodologyontherepresentationofspeciescomplexityinthefecalmicrobiomeashasbeenpreviouslyshown.Themethodofextractionplayedanimportantroleinthetypesandnumberofspeciesthatwereidentifiedinthestoolsamples[54].Whiletherewas no significant difference in the bacterial DNA yields usingthese twomethods, the identificationofBacteroides Spp. in thefecal samples extractedby the columnmethodwas far greaterthan in thephenol chloroformmethod.Thus it ispossible thatthe columnmethodmaybe the choicemethod for use in fecalsamples with similar downstream applications. While some
Page9of13Citation:WaltersSS,QuirosA,RolstonM,GrishinaI,LiJ,etal.(2014)AnalysisofGutMicrobiomeandDietModificationinPatientswithCrohn’sDisease.SOJMicrobiolInfectDis2(3):1-13.DOI:http://dx.doi.org/10.15226/sojmid/2/3/00122
Analysis of Gut Microbiome and Diet Modification in Patients with Crohn’s Disease Copyright: © 2014 Walters et al.
Figure 8: IncreasedinbacterialdiversityisseenfollowingSCDdietwithnoappreciablechangesduringLRDdietmodification:ComparedtothepreLRDdietstoolsamplesfromparticipantshadanincreaseinlevelsof11speciesandadecreasein13species(A).IncontrasttheSCDdietchangewasassociatedwithanincreasein134speciesandadecreaseononly6species(B).(Red:increase,Blue:decrease).
studies have found a wide variability in the representation ofBacteroides Spp, othershaveshowntheirpresenceconsistentlyinhumanstoolsamples[63,80-82].Furthermore,theuseofDNAmicroarraytechnologyprovidesafastandconvenientmeanstoexaminethealterations in the fecalmicrobiotaona largescaleandprovidesawindowintothehealthoftheintestinalmucosa.
TheroleofmicrobiotaingutinflammationandIBDhasbeenextensivelystudied[83-87]. TheeffectsofBacteroides fragilis,onthe Th1 responses through the action of the bacterial-derivedpolysaccharideA(PSA)havebeendemonstrated.Furthermore,altered microbiota also play a role in activation of a Th17response which is pro inflammatory, especially in IBD [83]. The global analysis of IBD associated dysbiosis has providedinformation on the complex interplay betweenmicrobiota, theinnateandacquiredimmunesystem.Thegapinknowledgeisintheareaofwhetherdietmodificationscanaffectthemicrobiota
inapositivemannerandifthischangeismeasurable.Ourstudyhas provided data to suggest that changes in the microbialdiversityassociatedwithIBDcanbealteredbydietarychanges.While this study utilized a small “n”, the longitudinal samplesprovided critical evidence of the effects of diet modificationon the fecalmicrobiota.The level of gut inflammationwasnotcharacterized, however all participants had disease and it isassumedthatgutinflammationplayedaroleinthemicrobiomethatwasdetected in thestool samples.Atbaseline,beforedietimplementation, overall microbial diversity was significantlydecreased in IBDsamplesascompared to thehealthynegativecontrols. IBD patients had more Bacteroides fragilis anda decreased abundance in Clostridium lactatifermentans,indicatinga shift in themicrobiotaaway fromthecompositionofthemicrobialcommunitiesinthehealthycontrols.Intermsofimproving themicrobialdiversity that IBDpatients lacked, theSCDdietproved tobemoreeffective.Patientson theSCDdiet
Page10of13Citation:WaltersSS,QuirosA,RolstonM,GrishinaI,LiJ,etal.(2014)AnalysisofGutMicrobiomeandDietModificationinPatientswithCrohn’sDisease.SOJMicrobiolInfectDis2(3):1-13.DOI:http://dx.doi.org/10.15226/sojmid/2/3/00122
Analysis of Gut Microbiome and Diet Modification in Patients with Crohn’s Disease Copyright: © 2014 Walters et al.
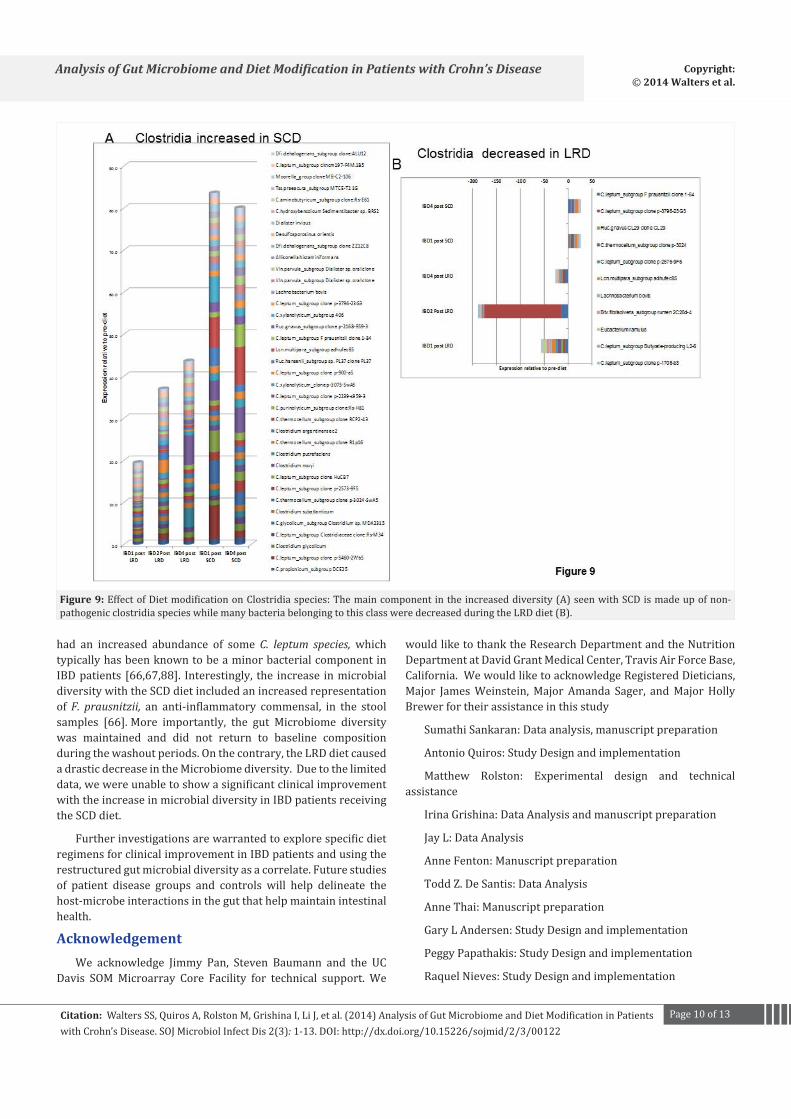
Figure 9: EffectofDietmodificationonClostridiaspecies:Themaincomponentintheincreaseddiversity(A)seenwithSCDismadeupofnon-pathogenicclostridiaspecieswhilemanybacteriabelongingtothisclassweredecreasedduringtheLRDdiet(B).
had an increased abundance of some C. leptum species, which typicallyhasbeenknowntobeaminorbacterialcomponentinIBDpatients [66,67,88]. Interestingly, the increase inmicrobialdiversitywiththeSCDdietincludedanincreasedrepresentationofF. prausnitzii, an anti-inflammatory commensal, in the stoolsamples [66]. More importantly, the gut Microbiome diversitywas maintained and did not return to baseline compositionduringthewashoutperiods.Onthecontrary,theLRDdietcausedadrasticdecreaseintheMicrobiomediversity.Duetothelimiteddata,wewereunabletoshowasignificantclinicalimprovementwiththeincreaseinmicrobialdiversityinIBDpatientsreceivingtheSCDdiet.
FurtherinvestigationsarewarrantedtoexplorespecificdietregimensforclinicalimprovementinIBDpatientsandusingtherestructuredgutmicrobialdiversityasacorrelate.Futurestudiesof patient disease groups and controls will help delineate thehost-microbeinteractionsinthegutthathelpmaintainintestinalhealth.
AcknowledgementWe acknowledge Jimmy Pan, Steven Baumann and the UC
Davis SOMMicroarray Core Facility for technical support. We
wouldliketothanktheResearchDepartmentandtheNutritionDepartmentatDavidGrantMedicalCenter,TravisAirForceBase,California.WewouldliketoacknowledgeRegisteredDieticians,Major JamesWeinstein,Major Amanda Sager, andMajorHollyBrewerfortheirassistanceinthisstudy
SumathiSankaran:Dataanalysis,manuscriptpreparation
AntonioQuiros:StudyDesignandimplementation
Matthew Rolston: Experimental design and technicalassistance
IrinaGrishina:DataAnalysisandmanuscriptpreparation
JayL:DataAnalysis
AnneFenton:Manuscriptpreparation
ToddZ.DeSantis:DataAnalysis
AnneThai:Manuscriptpreparation
GaryLAndersen:StudyDesignandimplementation
PeggyPapathakis:StudyDesignandimplementation
RaquelNieves:StudyDesignandimplementation
Page11of13Citation:WaltersSS,QuirosA,RolstonM,GrishinaI,LiJ,etal.(2014)AnalysisofGutMicrobiomeandDietModificationinPatientswithCrohn’sDisease.SOJMicrobiolInfectDis2(3):1-13.DOI:http://dx.doi.org/10.15226/sojmid/2/3/00122
Analysis of Gut Microbiome and Diet Modification in Patients with Crohn’s Disease Copyright: © 2014 Walters et al.
ThomasPrindiville:StudyDesignandimplementation
SatyaDandekar:StudyDesignandimplementation
Funding
This study was supported by grants from the NationalInstituteofHealth(NIH)R01(DK61297,AI43274).Dr.SankaranissupportedbyaBuildingInterdisciplinaryResearchCareersinWomen’sHealthaward(K12HD051958)fundedbytheNICHD,ORWH,andtheNIA.
References1. Yatsunenko T, Rey FE, Manary MJ, et al. Human gut microbiome
viewedacrossageandgeography.Nature.2012;486(7402):222-227.
2. Structure, functionanddiversityof thehealthyhumanmicrobiome.Nature.2012;486(7402):207-214.
3. Ghosh S, Dai C, Brown K, et al. Colonic microbiota alters hostsusceptibilitytoinfectiouscolitisbymodulatinginflammation,redoxstatus,andiontransportergeneexpression.AmJPhysiolGastrointestLiver.Physiol.2011;301(1):39-49.
4. Dave M, Higgins PD, Middha S, et al. The human gut microbiome:current knowledge, challenges, and future directions. Transl Res.2012;160(4):246-57.
5. Lawson RD, Coyle WJ. The noncolonic microbiome: does it reallymatter?CurrGastroenterolRep.2010;12(4):259-262.
6. SchwiertzA, TarasD, SchaferK, et al.Microbiota and SCFA in leanandoverweighthealthysubjects.Obesity(SilverSpring).2010;18(1):190-195.
7. TurnbaughPJ,HamadyM,YatsunenkoT,etal.Acoregutmicrobiomeinobeseandleantwins.Nature.2009;457(7228):480-484.
8. LiM,WangB,ZhangM,etal.Symbioticgutmicrobesmodulatehumanmetabolicphenotypes.ProcNatlAcadSciUSA2008;105(6):2117-2122.
9. Sobhani I, Tap J, Roudot-Thoraval F, et al. Microbial dysbiosis incolorectalcancer(CRC)patients.PLoSOne.2011;6(1):e16393.
10.BalterM.Takingstockofthehumanmicrobiomeanddisease.Science.2012;336(6086):1246-1247.
11. Zimmermann MB, Chassard C, Rohner F, et al. The effects of ironfortificationonthegutmicrobiotainAfricanchildren:arandomizedcontrolled trial in Cote d’Ivoire. Am J Clin Nutr2010; 92(6): 1406-1415.
12. WalkerAW, Ince J,DuncanSH, et al.Dominant anddiet-responsivegroupsofbacteriawithinthehumancolonicmicrobiota.ISMEJ.2011;5(2):220-230.
13. ArumugamM,RaesJ,PelletierE,etal.Enterotypesofthehumangutmicrobiome.Nature.2011;473(7346):174-180.
14. McDonald JA, SchroeterK,FuentesS, et al.Evaluationofmicrobialcommunity reproducibility, stability and composition in a humandistalgut chemostatmodel. Jmicrobiolmethods.2013;95(2):167-174.
15.Gill SR,PopM,DeboyRTetal.Metagenomicanalysisof thehumandistalgutmicrobiome.Science.2006;312(5778):1355-1359.
16.ContrerasM,CostelloEK,HidalgoG,etal.ThebacterialmicrobiotaintheoralmucosaofruralAmerindians.Microbiology.2010;156(11):3282-3287.
17.MagroneT,JirilloE.Theinteractionbetweengutmicrobiotaandage-relatedchanges in immune functionand inflammation. Immunity&ageing.2013;10(1):31.
18.SeksikP,Rigottier-GoisL,GrametG,etal.AlterationsofthedominantfaecalbacterialgroupsinpatientswithCrohn’sdiseaseofthecolon.Gut.2003;52(2):237-242.
19.Marteau P, Lepage P, Mangin I,et al. Review article: gut flora andinflammatory bowel disease. Aliment Pharmacol Ther 2004; 20(4):18-23.
20.WalkerAW,Sanderson JD,ChurcherC,etal.High-throughputclonelibraryanalysisofthemucosa-associatedmicrobiotarevealsdysbiosisand differences between inflamed and non-inflamed regions of theintestineininflammatoryboweldisease.BMCMicrobiol.2011;11:7.
21. KangS,DenmanSE,MorrisonM,etal.Dysbiosisof fecalmicrobiotain Crohn’s disease patients as revealed by a custom phylogeneticmicroarray.InflammBowelDis.2010;16(12):2034-2042.
22. Yildirim S, Yeoman CJ, Sipos M, et al. Characterization of the fecalmicrobiomefromnon-humanwildprimatesrevealsspeciesspecificmicrobialcommunities.PLoSOne.2010;5(11):e13963.
23. PepperJW,RosenfeldS.Theemergingmedicalecologyofthehumangutmicrobiome.TrendsEcolEvol.2012;27(7):381-384.
24. GreenJohnsonJM.Immunologicalresponsestogutbacteria. JAOACInt.2012;95(1):35-49.
25.AshidaH,OgawaM,KimM,etal.Bacteriaandhostinteractionsinthegutepithelialbarrier.NatChemBiol.2011;8(1):36-45.
26.Paliy O, Agans R. Application of phylogenetic microarrays tointerrogation of human microbiota. FEMS Microbiol Ecol. 2012;79(1):2-11.
27.CoxMJ,HuangYJ,FujimuraKE,etal.Lactobacilluscaseiabundanceisassociatedwithprofoundshiftsintheinfantgutmicrobiome.PLoSOne.2010;5(1):e8745.
28.CodlingC,OMahonyL,ShanahanF,etal.Amolecularanalysisoffecalandmucosalbacterialcommunitiesinirritablebowelsyndrome.DigDisSci.2010;55(2):392-397.
29.McKennaP,HoffmannC,MinkahN,etal.Themacaquegutmicrobiomeinhealth,lentiviralinfection,andchronicenterocolitis.PLoSPathog.2008;4(2):e20.
30.O’Keefe SJ. Nutrition and colonic health: the critical role of themicrobiota.CurrOpinGastroenterol2008;24(1):51-58.
31. Godoy-VitorinoF,GoldfarbKC,KaraozU,etal.Comparativeanalysesof foregutandhindgutbacterialcommunities inhoatzinsandcows.ISMEJ.2012;6(3):531-541.
32. Radosevich JL, Wilson WJ, Shinn JH, et al. Development of a high-volume aerosol collection system for the identification of air-bornemicro-organisms.LettApplMicrobiol.2002;34(3):162-167.
33. BrodieEL,DeSantisTZ,ParkerJP,etal.Urbanaerosolsharbordiverseand dynamic bacterial populations. Proc Natl Acad Sci USA. 2007;104(1):299-304.
34. BrodieEL,DesantisTZ,JoynerDC,etal.Applicationofahigh-densityoligonucleotide microarray approach to study bacterial populationdynamics during uranium reduction and reoxidation. Appl EnvironMicrobiol.2006;72(9):6288-6298.
35.Finegold SM, Attebery HR, Sutter VL. Effect of diet on human fecalflora: comparison of Japanese and American diets. Am J Clin Nutr.1974;27(12):1456-1469.
Page12of13Citation:WaltersSS,QuirosA,RolstonM,GrishinaI,LiJ,etal.(2014)AnalysisofGutMicrobiomeandDietModificationinPatientswithCrohn’sDisease.SOJMicrobiolInfectDis2(3):1-13.DOI:http://dx.doi.org/10.15226/sojmid/2/3/00122
Analysis of Gut Microbiome and Diet Modification in Patients with Crohn’s Disease Copyright: © 2014 Walters et al.
36.HillMJ:Dietandcancer.EurJCancerPrev.1995;4(6):443-444.
37.WuGD,ChenJ,HoffmannC,etal.Linkinglong-termdietarypatternswithgutmicrobialenterotypes.Science.2011;334(6052):105-108.
38.OmuraK,HiranoK,KanehiraE,etal.Smallamountoflow-residuedietwithparenteralnutritioncanpreventdecreasesinintestinalmucosalintegrity.AnnSurg.2000;231(1):112-118.
39.KogaH,IidaM,AoyagiK,etal.[Long-termefficacyoflowresiduedietfor themaintenanceof remission inpatientswithCrohn’sdisease].NihonShokakibyoGakkaiZasshi.1993;90(11):2882-2888.
40.Chapkin RS, Kamen BA, Callaway ES, et al. Use of a novel geneticmouse model to investigate the role of folate in colitis-associatedcoloncancer.JNutrBiochem.2009;20(8):649-655.
41. MahmudN,WeirDG.TheurbandietandCrohn’sdisease: istherearelationship?EurJGastroenterolHepatol.2001;13(2):93-95.
42. BertiC,RisoP,MontiLD,etal.Invitrostarchdigestibilityandinvivoglucoseresponseofgluten-freefoodsandtheirglutencounterparts.EurJNutr.2004;43(4):198-204.
43. HaasSV,HaasMP.The treatmentof celiacdiseasewith thespecificcarbohydratediet;reporton191additionalcases.AmJGastroenterol.1955;23(4):344-360.
44. ScottKP,Gratz SW, SheridanPO, et al. The influenceof diet on thegutmicrobiota.Pharmacological research: theofficial journalof theItalianPharmacologicalSociety.2013;69(1):52-60.
45.FlintHJ,ScottKP,DuncanSH,etal.Microbialdegradationofcomplexcarbohydratesinthegut.Gutmicrobes.2012;3(4):289-306.
46.Lionetti P, Callegari ML, Ferrari S, et al. Enteral nutrition andmicroflorainpediatricCrohn’sdisease.JPENJParenterEnteralNutr.2005;29(4Suppl):S173-175.
47.Matsui T, Ueki M, Yamada M, et al. Indications and options ofnutritionaltreatmentforCrohn’sdisease.Acomparisonofelementalandpolymericdiets.JGastroenterol.1995;30Suppl8:95-97.
48.Russell RI: Review article: dietary and nutritional management ofCrohn’sdisease.AlimentPharmacolTher.1991;5(3):211-226.
49.AokiY,OhtaM,SakamotoY,etal.Applicationofsolidlowresiduedietsconsistingmainlyofelementaldietincolorectaldiseases.NihonGekaHokan.1986;55(2):358-366.
50.BrownAC,RoyM.Doesevidenceexistto includedietarytherapyinthetreatmentofCrohn’sdisease?Expertreviewofgastroenterology&hepatology.2010;4(2):191-215.
51.Brown AC, Valiere A. Probiotics and medical nutrition therapy.Nutrition inclinicalcare :anofficialpublicationofTuftsUniversity.2004;7(2):56-68.
52.D’AversaF,TortoraA, IaniroG,etal.Gutmicrobiotaandmetabolicsyndrome.Internalandemergencymedicine.2013;8(Suppl1):S11-15.
53.ZoetendalEG,deVosWM.Effectofdietontheintestinalmicrobiotaanditsactivity.CurrOpinGastroenterol.2014;30(2):189-195.
54.P OC, Aguirre de Carcer D, Jones M, et al. The effects from DNAextractionmethodsontheevaluationofmicrobialdiversityassociatedwithhumancolonictissue.MicrobEcol.2011;61(2):353-362.
55.KimM,MorrisonM, Yu Z. Evaluation of different partial 16S rRNAgene sequence regions for phylogenetic analysis of microbiomes.Journalofmicrobiologicalmethods.2011;84(1):81-87.
56.YergeauE,Schoondermark-StolkSA,BrodieEL,etal.EnvironmentalmicroarrayanalysesofAntarcticsoilmicrobialcommunities.ISMEJ.2009;3(3):340-351.
57.SchatzMC,PhillippyAM,GajerP, et al. Integratedmicrobial surveyanalysis of prokaryotic communities for the PhyloChipmicroarray.ApplEnvironMicrobiol.2010;76(16):5636-5638.
58.LiC,HungWongW.Model-basedanalysisofoligonucleotidearrays:model validation, design issues and standard error application.GenomeBiol.2001;2(8):RESEARCH0032.
59.SheddenK,ChenW,KuickR,etal.Comparisonofsevenmethodsforproducing Affymetrix expression scores based on False DiscoveryRatesindiseaseprofilingdata.BMCBioinformatics.2005;6:26.
60.Eckburg PB, Bik EM, Bernstein CN, et al. Diversity of the humanintestinalmicrobialflora.Science.2005;308(5728):1635-1638.
61.Dethlefsen L, Huse S, Sogin ML, et al. The pervasive effects of anantibioticonthehumangutmicrobiota,asrevealedbydeep16SrRNAsequencing.PLoSBiol.2008;6(11):e280.
62.HumanMicrobiomeProjectC.Structure,functionanddiversityofthehealthyhumanmicrobiome.Nature.2012;486(7402):207-214.
63.GollJ,ThiagarajanM,AbubuckerS,etal.Acasestudyforlarge-scalehuman microbiome analysis using JCVI’s metagenomics reports(METAREP).PLoSOne.2012;7(6):e29044.
64.Andoh A, Tsujikawa T, SasakiM, et al. Faecalmicrobiota profile ofCrohn’sdiseasedeterminedby terminal restriction fragment lengthpolymorphismanalysis.AlimentPharmacolTher.2009;29(1):75-82.
65.Martinez C, Antolin M, Santos J, et al. Unstable composition of thefecalmicrobiota in ulcerative colitis during clinical remission.Am JGastroenterol.2008;103(3):643-648.
66.FlanaganP,CampbellBJ,RhodesJM:Bacteriainthepathogenesisofinflammatoryboweldisease.BiochemSocTrans.2011;39(4):1067-1072.
67.Willing BP, Dicksved J, Halfvarson J, et al. A pyrosequencing studyin twins shows that gastrointestinal microbial profiles vary withinflammatory bowel disease phenotypes. Gastroenterology. 2010;139(6):1844-1854.e1.
68.SiezenRJ,KleerebezemM.Thehumangutmicrobiome: areweourenterotypes?MicrobBiotechnol2011;4(5):550-553.
69.ReyesA,HaynesM,HansonN,etal.Virusesinthefaecalmicrobiotaofmonozygotic twins and theirmothers.Nature. 2010; 466(7304):334-338.
70.Gophna U. Microbiology. The guts of dietary habits. Science. 2011;334(6052):45-46.
71.De Cruz P, Prideaux L, Wagner J, et al. Characterization of thegastrointestinalmicrobiotainhealthandinflammatoryboweldisease.InflammBowelDis.2012;18(2):372-390.
72.KlewickaE,CukrowskaB,LibudziszZ,etal.Changesingutmicrobiotain children with atopic dermatitis administered the bacteriaLactobacillus casei DN--114001. Pol J Microbiol. 2011; 60(4): 329-333.
73.TurnbaughPJ,RidauraVK,FaithJJ,etal.Theeffectofdietonthehumangutmicrobiome: ametagenomic analysis in humanized gnotobioticmice.SciTranslMed.2009;1(6):6ra14.
74.Flier JS, Mekalanos JJ. Gut check: testing a role for the intestinalmicrobiomeinhumanobesity.SciTranslMed.2009;1(6):6ps7.
Page13of13Citation:WaltersSS,QuirosA,RolstonM,GrishinaI,LiJ,etal.(2014)AnalysisofGutMicrobiomeandDietModificationinPatientswithCrohn’sDisease.SOJMicrobiolInfectDis2(3):1-13.DOI:http://dx.doi.org/10.15226/sojmid/2/3/00122
Analysis of Gut Microbiome and Diet Modification in Patients with Crohn’s Disease Copyright: © 2014 Walters et al.
75.Hollander D. Crohn’s disease--a permeability disorder of the tightjunction?Gut.1988;29(12):1621-1624.
76.Secondulfo M, de Magistris L, Fiandra R. Intestinal permeability inCrohn’sdiseasepatientsandtheirfirstdegreerelatives.DigLiverDis.2001;33(8):680-685.
77.MurphyMS, Eastham EJ, Nelson R, et al. Intestinal permeability inCrohn’sdisease.ArchDisChild.1989;64(3):321-325.
78.PaturiG,MandimikaT,ButtsCA,etal.Influenceofdietaryblueberryand broccoli on cecalmicrobiota activity and colonmorphology inmdr1a(-/-)mice,amodelofinflammatoryboweldiseases.Nutrition.2012;28(3):324-330.
79.HallerD.NutrigenomicsandIBD:theintestinalmicrobiotaatthecross-road between inflammation and metabolism. J Clin Gastroenterol.2010;44(Suppl1):S6-9.
80.Zubrzycki L, Spaulding EH. Studies on the Stability of the NormalHumanFecalFlora.Journalofbacteriology.1962;83(5):968-974.
81.San Joaquin VH, Griffis JC, Lee C, et al. Association of Bacteroidesfragilis with childhood diarrhea. Scandinavian journal of infectiousdiseases.1995;27(3):211-215.
82.YuanJ,ZengB,NiuR,etal.Thedevelopmentandstabilityofthegenus
BacteriodesfromhumangutmicrobiotainHFAmicemodel.Currentmicrobiology.2011;62(4):1107-1112.
83.IvanovII,FrutosRdeL,ManelN,etal.SpecificmicrobiotadirectthedifferentiationofIL-17-producingT-helpercellsinthemucosaofthesmallintestine.Cellhostµbe.2008;4(4):337-349.
84.Alexander KL, Targan SR, Elson CO, 3rd. Microbiota activation andregulationofinnateandadaptiveimmunity.Immunologicalreviews.2014;260(1):206-220.
85.ComitoD,CascioA,RomanoC.Microbiotabiodiversityininflammatoryboweldisease.Italianjournalofpediatrics.2014;40:32.
86.Ray K. IBD. Understanding gut microbiota in new-onset Crohn’sdisease.NaturereviewsGastroenterology&hepatology.2014;11(5):268.
87.Goldsmith JR, Sartor RB. The role of diet on intestinal microbiotametabolism: downstream impacts on host immune function andhealth, and therapeutic implications. J Gastroenterol. 2014; 49(5):785-798.
88.Flanagan JL, Brodie EL, Weng L, et al. Loss of bacterial diversityduring antibiotic treatment of intubated patients colonized withPseudomonasaeruginosa.JClinMicrobiol.2007;45(6):1954-1962.


















