Analogs as a Focus Bruce W. Bode, MD, FACE Atlanta Diabetes Associates Atlanta, Georgia.
42
Analogs as a Focus Bruce W. Bode, MD, FACE Atlanta Diabetes Associates Atlanta, Georgia
-
Upload
phillip-robinson -
Category
Documents
-
view
214 -
download
0
Transcript of Analogs as a Focus Bruce W. Bode, MD, FACE Atlanta Diabetes Associates Atlanta, Georgia.

Analogs as a Focus
Bruce W. Bode, MD, FACE
Atlanta Diabetes Associates
Atlanta, Georgia

ADA. Clinical Practice Recommendations. 2001.
Goals of Intensive Diabetes Management
• Near-normal glycemia
— HbA1c <6.5% to 7.0%
• Avoid short-term crisis
— Hypoglycemia
— Hyperglycemia
— DKA
• Minimize long-term complications
• Improve QOL

ACE/AACE Targets for Glycemic Control
HbA1c <6.5%
Fasting/preprandial glucose <110 mg/dL
Postprandial glucose <140 mg/dL
ACE/AACE Consensus Conference. Washington, DC. August 2001.

Insulin
The Most Powerful Agent We Have to Control Glucose

Fred Banting (1891-1941) Charles H. Best (1899-1978) John J.R. McLeod (1876-1935)Fred Banting (1891-1941) Charles H. Best (1899-1978) John J.R. McLeod (1876-1935)
James B. CollipJames B. Collip(1892-1965)(1892-1965)
Marjorie (?-?)Marjorie (?-?)
The Discovery of Insulin (Toronto 1921)

Patient J.L., December 15, 1922 February 15, 1923
The Miracle of Insulin

Comparison of Human Insulins/Analogs
Insulin Onset of Duration ofPreparations Action Peak Action
Regular 30-60 min 2-4 h 6-10 h
NPH/lente 1-2 h 4-8 h 10-20 h
Ultralente 2-4 h Unpredictable 16-20 h
Lispro/aspart 5-15 min 1-2 h 4-6 h
Glargine 1-2 h Flat ~24 h

4:00 16:00 20:00 24:00 4:00
Breakfast Lunch Dinner
8:0012:008:00
Time
Pla
sma
insu
lin
Ideal Basal/Bolus Insulin Absorption Pattern

Rapid-acting Insulin Analogs: Medical Rationale
• Administration at mealtime
• Mimic physiologic insulin profile
• Improved postprandial glycemic control
• Lower risk of late hypoglycemia
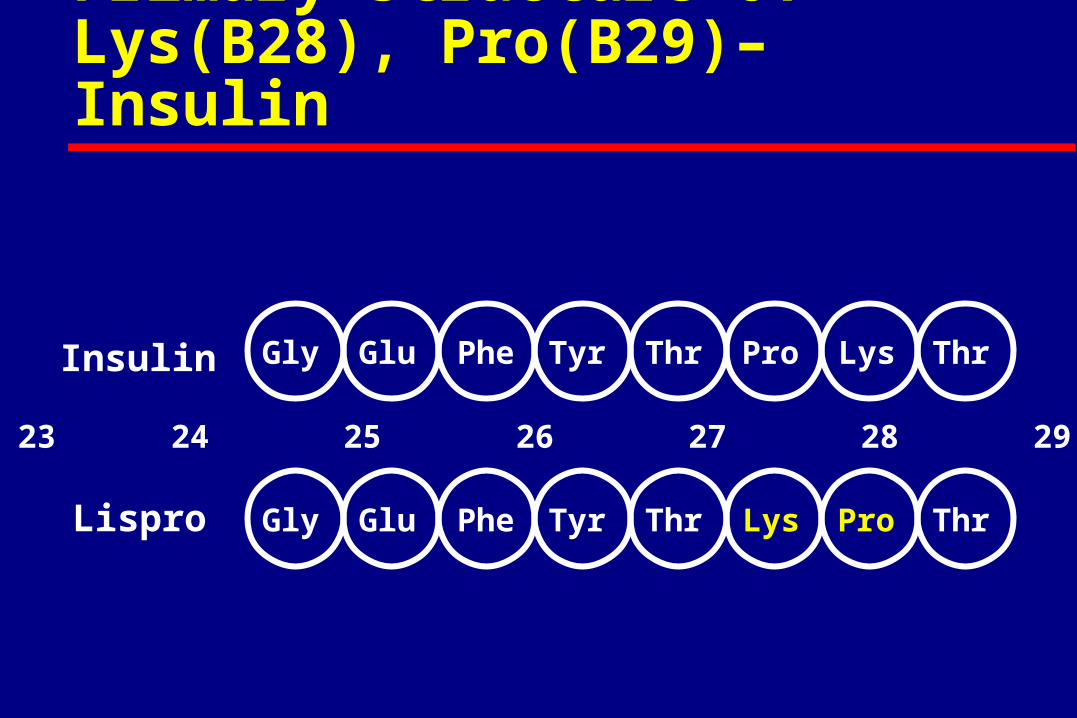
Gly ThrGlu Phe Tyr Pro Lys Thr
Gly ThrGlu Phe Tyr Lys Pro Thr
23 24 25 26 27 28 29 30
Insulin
Lispro
Primary Structure of Lys(B28), Pro(B29)–Insulin

Gly ThrGlu Phe Tyr Pro Lys Thr
Gly ThrGlu Phe Tyr Asp Lys Thr
23 24 25 26 27 28 29 30
Insulin
Aspart
Primary Structure of Asp(B28)-Insulin

Dissociation and Absorption of NovoLog®
Insulin aspart (NovoLog®)
Regular human insulin
Peak time=80-120 min
Peak time=40-50 min
Capillarymembrane
Su
bcu
tan
eou
s ti
ssu
eS
ub
cuta
neo
us
tiss
ue

800
700
600
500
400
300
200
100
0
Se
rum
ins
ulin
(p
mo
l/L)
0.2 U/kg SQTime (h)
0 2 4 6 8 10
Insulin aspartRegular insulin
Heinemann L, et al. Diabetes Care. 1998;21:1910.
Insulin Aspart: Mean Serum Insulin Profiles During Euglycemic Clamp in Healthy Volunteers

Glucose Area Under the Curve
60
70
80
90
100
110
120
130
-30 Fast 30 60 90 120 240
Time (min)
Glucose (mg/dL)
None
RegularAspart

Home PD, et al. Diabetes Care. 1998;21:1904-1909.
BreakfastBreakfast LunchLunch DinnerDinner NPHNPH
mU/LmU/L
8080
6060
4040
2020
00
100100
06:0006:00 12:0012:00 18:0018:00 24:0024:00 06:0006:00
Ser
um
in
suli
nS
eru
m i
nsu
lin
1010
mmol/Lmmol/L
1616
1414
1212
88
66
1818
Pla
sma
glu
cose
Pla
sma
glu
cose
250250
200200
150150
300300
mg/dLmg/dL
Insulin aspart
Human regular
Insulin Aspart vs Human Regular: Glycemic Control

Prandial increment isthe increase in bloodglucose from premeal to 90 minutes postmeal
European trial North American trial
Incr
emen
t (m
mo
l/L
)
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
P<0.001 P<0.001
NovoLog®
Regular human insulin
Raskin P, et al. Diabetes Care. 2000;23:583.Home PD, et al. Diabet Med. 2000;17:762.
Postprandial Blood Glucose Increment (Mean over the 3 Meals at 6 Months)

NovoLog®
Regular human insulin
100
Study 1 Study 2 Study 3 Study 4
0
200
300
400
500
Outliers
Median
Data from: Home. Eur J Clin Pharmacol. 1999;55:199-203.Heinemann. Diabet Med. 1996;13:683-684. Mudaliar. Diabetes Care. 1999;22:1501-1506.Heinemann. Diabetes Care. 1998;21:1910-1914.
Healthy Volunteers
Decreased Interindividual Variability in NovoLog® Values for Tmax
Tm
ax (
min
)

Frequency of events:
7.9
7.8
7.7
7.6
0
Hb
A1
c (
%)
NovoLog® Regularinsulin
NovoLog® Regularinsulin
8.0
8.1
8.20 per year0-10 per year10-30 per year>30 per year
Type 1 Diabetes
*Symptoms or blood glucose <45 mg/dL.Data on file, Novo Nordisk. Studies 035/EU, 036/US.
Study 035/EU Study 036/US
Frequency of Minor* Hypoglycemia Observed by Level of Glycemic Control

NovoLog® Regular human insulin
14
10
0
% Patients with MajorHypoglycemic Episodes
Nighttime
4
12
Daytime
8
6
2
P<0.005 NS
Data on file, Novo Nordisk. Studies 035/EU, 036/US.
Reduced Reporting of Major Nocturnal Hypoglycemia
%

Reduced Risk of Major Nocturnal Hypoglycemia
0.7
0.5
Relative Risk NovoLog Compared with Regular
Human Insulin
NovoLog®
HumanInsulin
(No. of Patients with Events)
Home 8%(54/707)
11%(39/358)
Raskin 4%(24/596)
8%(23/286)
Study 035/EU Study 036/US
Data on file, Novo Nordisk. Studies 035/EU, 036/US.

4:00 16:00 20:00 24:00 4:00
Breakfast Lunch Dinner
8:0012:008:00
Time
Pla
sma
insu
lin
lispro lispro lispro
Aspart Aspart Aspartor oror
Rapid-acting Insulin Analogs Provide Ideal Prandial Insulin Profile

400
350
300
250
200
150
100
MealSC injection
50
00 30 60
Time (min)90 120 180 210150 240
Regular Lispro
500450400350300250
150
50
200
100
00 50 100
Time (min)150 200 300250
Pla
sm
a i
ns
uli
n (
pm
ol/
L)
Pla
sm
a i
ns
uli
n (
pm
ol/
L)
MealSC injection
Heinemann, et al. Diabet Med. 1996;13:625-629.Mudaliar SR, et al. Diabetes Care. 1999;22:1501-1506.
Regular Aspart
Short-acting Insulin Analogs:Lispro and Aspart Plasma Insulin Profiles

Pharmacokinetic Comparison: NovoLog® vs Humalog®
300
350
250
200
150
100
50
0
7 8 9 10 11 12 13
NovoLog®
Humalog®
Fre
e in
sulin
(p
mo
l/L)
Time (h)Hedman CA, et al. Diabetes Care. 2001;24:1120-1121.

Insulin Aspart vs Buffered R vs Insulin Lispro in CSII Study
Bode B, et al. Diabetes Care. 2002;25:439-444.
Insulin aspart
Buffered regular human insulin (Velosulin®)Screening
Insulin lispro
-2 weeks 16 weeks0 weeks
146 patients in the USA; 2-25 years with type 1 diabetes;
7%HbA1c9%; previously treated with CSII for 3 months

Glycemic Control with CSII NovoLog®
Human insulin
Humalog®
7.0
7.2
7.8
8.0
Hb
A1
c (
%) 7.6
7.4
Baseline Week 8 Week 12 Week 160
Bode B. Diabetes. 2001;50(S2):A106.
Type 1 Diabetes

Self-monitored Blood Glucose in CSII
NovoLog® Buffered regular Humalog®
80
100
120
140
160
180
200
220
Blo
od
glu
cose
(m
g/d
L)
* *
*
Bedtime 2 AMBefore and90 min after
breakfast
Before and90 min after
lunch
Before and90 min after
dinner
Type 1 Diabetes
*P<0.01 vs buffered regular insulin.Bode B. Diabetes. 2001;50(S2):A106.

Ep
iso
des
/mo
nth
/pat
ien
t
0
2
4
6
8
10
12
Insulin aspart Human insulin Insulin lispro
PP<0.05<0.05
PP<0.05<0.05
Symptomatic or Confirmed Hypoglycemia
30% relative reduction
Bode B, et al. Diabetes Care. 2002;25:439-444.

0
10
20
30
40
50
Insulin aspartBuffered human insulinInsulin lispro
Pat
ien
ts w
ith
tro
ub
le-f
ree
use
(%
)
Insulin Aspart vs Buffered R vs Insulin Lispro in CSII Study: Pump Compatibility
Data on file, Novo Nordisk. Study ANA 2024.

Long-acting Soluble Insulin Analogs: Medical Rationale
• Mimic basal physiological insulin profile
• Improved glycemic control
• More reproducible insulin delivery
• May be used in insulin pens

Limitations of NPH, Lente,and Ultralente
• Do not mimic basal insulin profile
— Variable absorption
— Pronounced peaks
— Less than 24-hour duration of action
• Cause unpredictable hypoglycemia
— Major factor limiting insulin adjustments

ThrPhe Tyr Pro Lys Thr
25 26 27 28 29 30
InsulinB-chain
Glargine ThrPhe Tyr Pro Lys Thr Arg Arg
AsnLeu Glu Tyr Cys Gly
AsnLeu Glu Tyr Cys Asn
16 17 18 19 20 21
InsulinA-chain
Glargine
Primary Structure of Gly(A21), Arg(B31), Arg(B32)-Insulin

Gly ThrGlu Phe Tyr Pro Lys Thr
Gly ThrGlu Phe Tyr Pro Lys Thr
23 24 25 26 27 28 29 30
Insulin
Detemir
(CH(CH22))44
NHNH
COCO
RR
Primary Structure of Lys(B29)-N--Tetradecanoyl, Des(B30)-Insulin

Basis of Effect of Insulin Glargine
• Isoelectric point change
• Precipitates at neutral tissue pH
— Acid in solution; cannot be mixed with other insulins
• Retarded absorption rate
• Corresponding longer duration of action

0
0
1
2
3
4
5
6
2 4 6 8 10 12 14 16 18 20 22 24 26 28 30
NPH
Glargine
Placebo
0.4 U/kg
Time (h)
Glu
cose
infu
sio
n r
ates
(mg
/kg
/min
)
Linkeschowa R, et al. Diabetes.1999;48(suppl 1):A97.
Insulin Glargine in Nondiabetic Subjects: Pharmacokinetics by Glucose Clamp

Overall Summary: Glargine
• Insulin glargine has the following clinical benefits:
— Once-daily dosing because of its prolonged duration of action and smooth, peakless time-action profile
— Comparable or better glycemic control (FBG)
— Lower risk of nocturnal hypoglycemic events
— Safety profile similar to that of human insulin

Basis of Effect of Acylated Insulin Analogs (Detemir)
• Bind to serum albumin
• Prolonged time in circulation
• Longer duration of action

Injectionsite
Hormone
Blood
Carrierprotein
Carrierprotein Hormonehormone
Carrierprotein
Tissue
Receptor
Receptorhormone
Use of a Serum Carrier Protein (eg, Albumin) to Extend Time of Action

Brunner GA, et al. Exp Clin Endocrinol Diabetes. 2000;108:100-105.
Elapsed time (min)
0.0
0.5
1.0
1.5
2.0
-100 100 300 500 700 900 1100 1300 1500
Detemir - high
Detemir - low
Placebo
Glu
cose
infu
sio
n r
ate
(mg
/kg
/min
)
Insulin Detemir in Nondiabetic Subjects:Pharmacokinetics by Glucose Clamp

4:00 16:00 20:00 24:00 4:00
Breakfast Lunch Dinner
8:0012:008:00
Time
Glargineor
detemir
Pla
sma
insu
lin
Long-acting Insulin Analogs Provide Ideal Basal Insulin Profile

4:00 16:00 20:00 24:00 4:00
Breakfast Lunch Dinner
8:0012:008:00
Time
Glargineor
detemir
lispro lispro lispro
Aspart Aspart Aspartor oror
Pla
sma
insu
lin
Basal/Bolus Treatment Program with Rapid-acting and Long-acting Analogs

Insulin Receptor Affinity (%) IGF-1 Receptor Affinity (%)
Cells Solubilized Cells SolubilizedReceptors Receptors
Relative to human insulin Relative to human insulin
Receptor Binding Affinities
Human insulin 100 100 100 100
Insulin aspart 92 92 69 81
Insulin lispro 102 ND 142 156
Insulin glargine ND 86 ND 641
ND = not determined.

Insulin Analogs
Fulfilling the Promise of Recombinant DNA Technology:
Better BasalBetter Bolus
Better Blood Glucose