
Analgesics in dentistry
24
Vivek Narayan Oral Medicine & Radiology ANALGESICS IN DENTISTRY
-
Upload
medicinist -
Category
Health & Medicine
-
view
595 -
download
0
Transcript of Analgesics in dentistry
Vivek NarayanOral Medicine & Radiology
ANALGESICS IN DENTISTRY
IASP defines pain as an unpleasant sensory and emotional experience associated with actual or potential
tissue damage or described in terms of such damage.
Pain – definition

Algesia/algia – pain.
Neuralgia - Pain in one or more nerves
and is described as electric shock like
pain with presence of trigger zones.
Neuropathic pain - Constant burning
type of pain without presence of trigger
zones.
Allodynia - Pain due to a stimulus which
does not normally provoke pain.
Hyperalgesia - Extreme reaction to a
stimulus which is normally painful.
Pain terminologies
Medical management.
Physiatry/physiotherapy.
TENS.
Acupuncture.
Low level laser therapy.
Cognitive behavioral therapy.
Hypnosis.
Pain control

Analgesic – pain reliever, pain killer.
Analgesics
1. NSAIDS (non opioid analgesics) –
mild to moderate pain.
2. Opioid analgesics – severe pain.
Analgesic

Arachidonic acid pathway.
COX converts arachidonic acid
to produce,
1. Prostaglandins
2. Thromboxane
3. Prostacyclin
COX 1 – secretion of mucus,
hemostasis & renal functions –
house keeping functions.
COX 2 – induced by cytokines &
other stimuli of inflammation.
Cyclo-oxygenase (COX)Mediators of pain &
inflammation

NSAIDS
NSAIDS
Non selective COX inhibitors
AspirinIndometh
acinIbuprofenDiclofenacPiroxicamKetorolac
Preferential COX 2 inhibitors
Nimesulide
Meloxicam
Nabumetone
Selective COX 2 inhibitors
CelecoxibRofecoxib
Analgesics with poor anti-
inflammatory action
Acetaminophen
Nefopam

Acetyl salicylic acid.
Converted to salicylic acid by the body.
Acts on peripheral pain receptors.
Hyperglycemia at toxic doses.
Hyperventilation, asthma.
GI irritant, ulcers.
Prolonged bleeding.
Dosage - 325 to 650 mg orally every 4
hours as needed, not to exceed 4 g/day
Aspirin

Less effective than aspirin.
Inhibits PG synthesis.
Prolongs bleeding time.
Gastric discomfort.
Nausea & vomiting.
Precipitates asthma.
Indicated in RA, osteoarthritis, soft tissue
injuries & after tooth extraction.
Dosage – 400mg q4 – 6h. Maximum
2.4g.
Ibuprofen
Has all analgesic, antipyretic & anti-
inflammatory actions.
Inhibits PG synthesis.
Short lasting anti platelet action.
Good tissue penetration.
Concentration is 3 times the plasma t1/2 in
synovial fluid .
Nausea, headache & dizziness.
Used in arthritis, ankylosing spondyltits.
Dosage – 50mg – 100mg q4 – 6h not to
exceed 150mg.
Diclofenac
Paracetamol.
Central action & increases pain
threshold.
Good antipyretic.
Poor anti-inflammatory.
No significant adverse effects.
Used as analgesic for headache &
musculoskeletal pain, osteoarthritis.
Dosage – 500mg – 1000mg q4 – 6h
not to exceed 4g.
Acetaminophen

Locally acting NSAIDS.
Inhibits prostaglandin synthetase.
Has analgesic & local anesthetic
properties.
Used for inflammatory conditions
of mouth & throat.
Contraindicated in hypersensitivity.
Oral tissue numbness & stinging
sensation may occur.
Dosage – 0.15% mouthwash to be
used TID.
Available as TANTUM ORAL RINSE.
Benzydamine hydrochloride

OPIOIDS
Acts on the CNS produces
depression.
Otherwise called narcotic analgesics.
Morphine is the prototype drug &
principal opium alkaloid .
Morpheus – ‘god of dreams’
Indicated for severe pain conditions.
Sedation, mental clouding,
constipation, respiratory depression,
tolerance & dependence.
Opioid analgesics

Opioid analgesics
Natural alkaloids
Morphine Codeine
Semisynthetic opiates
HeroinPholcodeine
Hydrocodon
e Oxycodone
Synthetic opioids
PethidineFentanyl
Tramadol
Methyl morphine.
Converted to morphine by the
body.
Effective cough suppressant.
Constipation occurs.
Used after extraction along with
NSAIDS.
Dosage – 30mg – 60mg q4 – 6h.
Codeine
To treat moderate to severe pain.
As an antitussive to suppress
cough.
Effect starts after 30 mins & lasts
for 4 – 8hrs.
Common side effects are nausea,
vomiting, constipation, drowsiness,
dizziness, lightheadedness.
Dosage – 5mg – 10mg q4 – 6h.
Hydrocodone & oxycodone
Synthetic centrally acting
analgesic.
Indicated for moderate to
severe pain.
Nausea, vomiting, drowsiness,
sedation & fatigue.
50mg – 100mg q4 – 6h
maximum 400mg.
Tramadol

To use lower doses of drugs.
Increasing range of action – fast
onset, short acting
(acetaminophen) with a slow
onset, long acting (codeine or
tramadol).
Targeting different pain
pathways simultaneously.
Combination of analgesics

Eliminate the source of pain, if at all
possible.
Individualize regimens based on pain
severity and medical history.
Maximize the non opioid before adding an
opioid.
Optimize dose and frequency before
switching.
For NSAIDs, consider,
1. Preoperative dose.
2. Loading dose.
3. Prescribing round-the-clock.
Avoid chronic use of any analgesic
whenever possible.
Reduce the dose and duration of any NSAID
or opioid in the elderly.
Guidelines for analgesic use
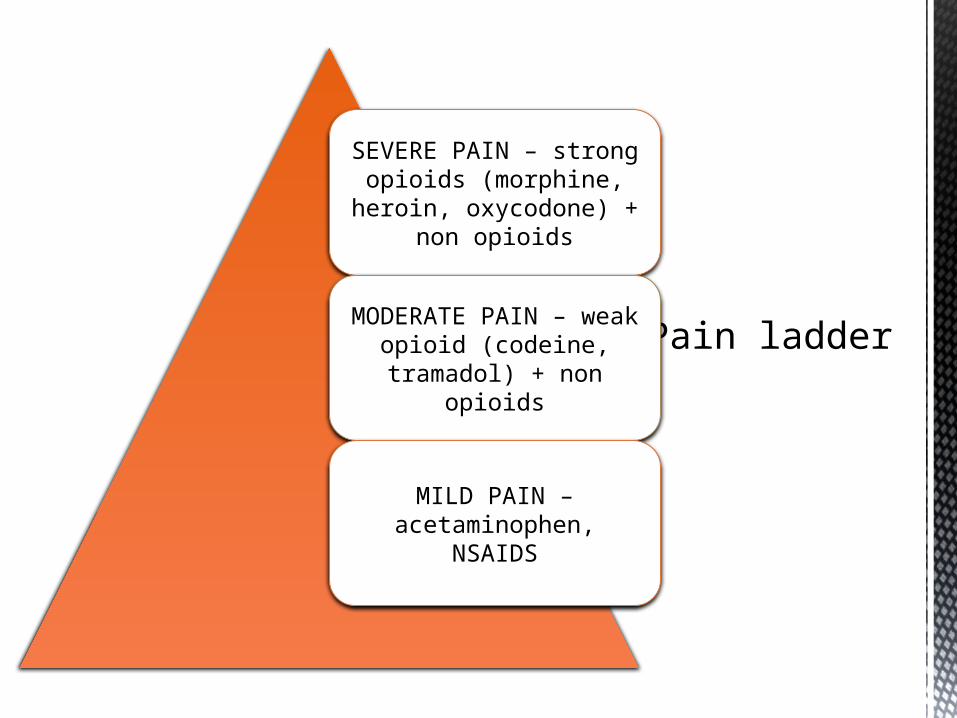
Pain ladder
SEVERE PAIN – strong opioids (morphine, heroin,
oxycodone) + non opioids
MODERATE PAIN – weak opioid (codeine, tramadol) +
non opioids
MILD PAIN – acetaminophen, NSAIDS

Primarily used to treat epilepsy or
seizures.
MOA – reduces neuronal
hyperexcitability that is fundamental
to seizures.
Neuralgic & neuropathic pain is also
because of neuronal hyperexcitability.
Anticonvulsants used,
1. Carbamazepine
2. Oxcarbazepine
3. Phenytoin
4. Valproic acid
5. Lamotrigine
6. Baclofen
Anticonvulsants for pain
Odontogenic infection &
inflammation.
Post extraction, post surgical pain.
Cracked tooth syndrome.
Eagle’s syndrome.
Neuralgias,
1. Trigeminal neuralgia.
2. Glossopharyngeal neuralgia.
3. Post herpetic neuralgia.
Fractures – odontogenic &
osteogenic.
Pain in carcinoma.
Oral mucosal lesions.
Common orofacial pain
conditions






![Knowledge of drug prescription among dental and medical ... · analgesics are essential for management of pain and infection.[7] However, antibiotic prescribing in dentistry is generally](https://static.fdocuments.net/doc/165x107/5ed5c7b83e6f6128a847c2c3/knowledge-of-drug-prescription-among-dental-and-medical-analgesics-are-essential.jpg)











