Anal Abuse - WordPress.com€¦ · 06.10.2013 · Anal Abuse Clinical Forensic ... 89 children < 18...
69
Anal Abuse Clinical Forensic Medicine Clinical Forensic Medicine MATLA A BANA 2011
Transcript of Anal Abuse - WordPress.com€¦ · 06.10.2013 · Anal Abuse Clinical Forensic ... 89 children < 18...

Anal AbuseClinical Forensic MedicineClinical Forensic Medicine
MATLA A BANA
2011

Marcus X
• This is the horrific story of Marcus X who
fell prey to the lusts of his bachelor uncle
• This lecture is a tribute to the woes of a
child who did not ask to be abused
• The psychological damages done were far
worse than the physical trauma

Marcus X – 5 Years old

Family Structure
GrandpaGrandma
Mother Father Uncle
Bachelor
Marcus

Marcus Presented with:
• Sexual Play – other children
• Encircling genitals in magazines
ALARM BELLS:
• Encircling genitals in magazines
• Recalls the taste of semen
• “Uncle put his ‘tottie’ in my mouth”
• Refused to visit farm he was fond of
• Examined
• Referred to a Clinical Psychologist

12:00
03:0009:00
06:00
01:00
NOTES: Marcus (5 years) was seen approximately 5 months after alleged
sodomy
The position of examination was KNEE-CHEST
He had a definite scar PERI-ANAL in the 01:00 position
No dilatation could be demonstrated
Note the fecal soiling in the midline

Outline
• Introduction
• Anatomy• Anatomy
• Approach to the anus
• Normal versus Abnormal
• Fissures; Dilatation; Cupping; Funneling
• Tire sign
• Adams Classification
Introduction
IMPORTANCE:
• CORRECT EXAMINATION PROCEDURE• CORRECT EXAMINATION PROCEDURE
• CORRECT INTERPRETATION OF FINDINGS
1987:
CLEVELAND (ENG) 125 CHILDREN REMOVED ON BASIS
OF REFLEX ANAL DILATATION - ALL THESE CHILDREN
WERE PLACED BACK
• TRAGIC EVENT

ANAL ANATOMYANAL ANATOMYTHE ESSENTIALS

C
R
O
SS
SS
E
CT
I
ON

Anal Sphincters

Anatomy And Physiology
TWO SPHINCTERS:
A. INTERNAL - Smooth MuscleA. INTERNAL - Smooth Muscle
Involuntary
B. EXTERNAL - Pelvic Floor
Voluntary

Anal Reflexes:
A. CUTANO-ANAL REFLEX
External sphincters contracts when the skin of the buttocks is touched. Under voluntary control it can buttocks is touched. Under voluntary control it can relax to prevent pain or injury
B. RECTO-ANAL REFLEX
Internal sphincter relaxes when rectum is distended.
The external sphincter can override this process
NEVER EXAMINE THE ANUS WHEN STOOLS FILL THE RECTUM


Anal Mucosa
Rectal Rectal Rectal Rectal mucosamucosamucosamucosa
PectenPectenPectenPecten
Anal VergeAnal VergeAnal VergeAnal Verge

ANAL EXAMINATIONANAL EXAMINATIONAN APPROACH

How to examine the anus:
• SUPINE KNEE CHEST POSITION
• LEFT LATERAL POSITION• LEFT LATERAL POSITION
• PRONE KNEE CHEST POSITION
Gently part the buttocks. Examine for signs of abuse.
Anal verge as well as the rugae should be inspected.
Internal examination is rarely necessary unless a PR
bleeding is observed.

Approach to the anus
Supine knee- chest Prone knee-chest

Supine knee-chest

Prone Knee Chest

The Anus
• What can go wrong with the anus:
– During and after Abuse?– During and after Abuse?
– During and after Normal Processes?
– During and after Pathological Processes?
– Congenital abnormalities

Abuse Related - Acute
• Tears peri-anal
• Ecchymoses - bruising• Ecchymoses - bruising
• Abrasions
• Redness
• Swelling

Abuse Related - Chronic
• Scar Tissue formation
• Hypertrophy of peri-anal skin• Hypertrophy of peri-anal skin
• Infections
– Gonorrhoea & Lues
– Warts [C Accuminata]
• Dilatation – spontaneous
– Cupping or Funnelling

Normal Processes
• Constipation Related:
– Fissure formation– Fissure formation
• Midline Tears – 12:00 & 06:00
– Tag formation [Sentinel Piles]

Pathological
• Chron’s Disease:
– Peri-anal scars– Peri-anal scars
– Diarrhoea
– Mucoid stools
– Family history
– > 15 years

Congenital
• Fusion defects

Its Normal to be Abnormal
1989 - McCann - 267 Non Abused Children:
• Erythema [Redness] - 40,5%• Erythema [Redness] - 40,5%
• Pigmentation [Darkening]- 29,5%
• Venous Congestion - 7% - 52% - 73%
• Smooth midline areas - 26% (06:00 & 12:00)
• Anal tags - Midline = Normal
• Sphincter Dilatation [See next page]

Sphincter Dilatation
• Dilatation occurred in 49% of children and mean
diameter was 10mm ( 1mm - 25mm)
• In 91% of children examined the maximums were • In 91% of children examined the maximums were
less than 20mm and the mean diameter 5,7mm
• 30% before 30 seconds
• 55% before 2 minutes
• 5% After 5 minutes
• 38% stayed open and
• 68% opened intermittently
Controversial issues
Hobbs survey (1989) - 337 children:
• Reckon ERYTHEMA, FISSURES, VENOUS
CONGESTION is positive for abuse. Anal CONGESTION is positive for abuse. Anal
DILATATION seen in only 4%

Controversial issues
Various Studies on reflex anal dilatation:
• Ellis-Fraser and Wright in 1987 - 8,5% of Abuses
• Stanton and Sunderland 1989 - 14% of non-abused• Stanton and Sunderland 1989 - 14% of non-abused
• Priestly 1989 - 4% of all children
• Agnerrson, Evans et al 1990 - 18% with constipation
• Claydon 1988 - 15% of severe constip.
Anal dilatation is more common in abuse, but fits abused and non-abused

Common Denominators
Reflex anal dilatation:
• More in abuse
• More in constipation
• Associated with Crohn’s
• More with sedating drugs (benzodiasepines)

Homosexuals
Study amongst those active in anal intercourse:
• Tenesmus in 56% - most common complaint• Tenesmus in 56% - most common complaint
• Resting anal pressure slightly reduced
• Squeeze pressure unchanged
• None had dilatation

Anal fissures [Constipation]
versusversusPenetration injuries
[Abuse]

Definition of a Fissure
• It is an elongated ulcer in the long axis of the lower anal canalof the lower anal canal

Location
• The position of anal fissures are in the 06:00
position and to a lesser extent in the 12:00
position
• In males the ratio is Anterior : Posterior –
10% : 90%
• In females the distribution is 40% : 60%

Etiology
Stools Force Direction = Backwards
Explains the 06:00 Tears
Fissure Positions
• The constipation related fissures are situated between:situated between:
– Pectinate line and
– Muco-cutaneous junction
• Seldom if ever outside the anal “ring”
• Peri-anal tears are invariably the result of an external penetrative force
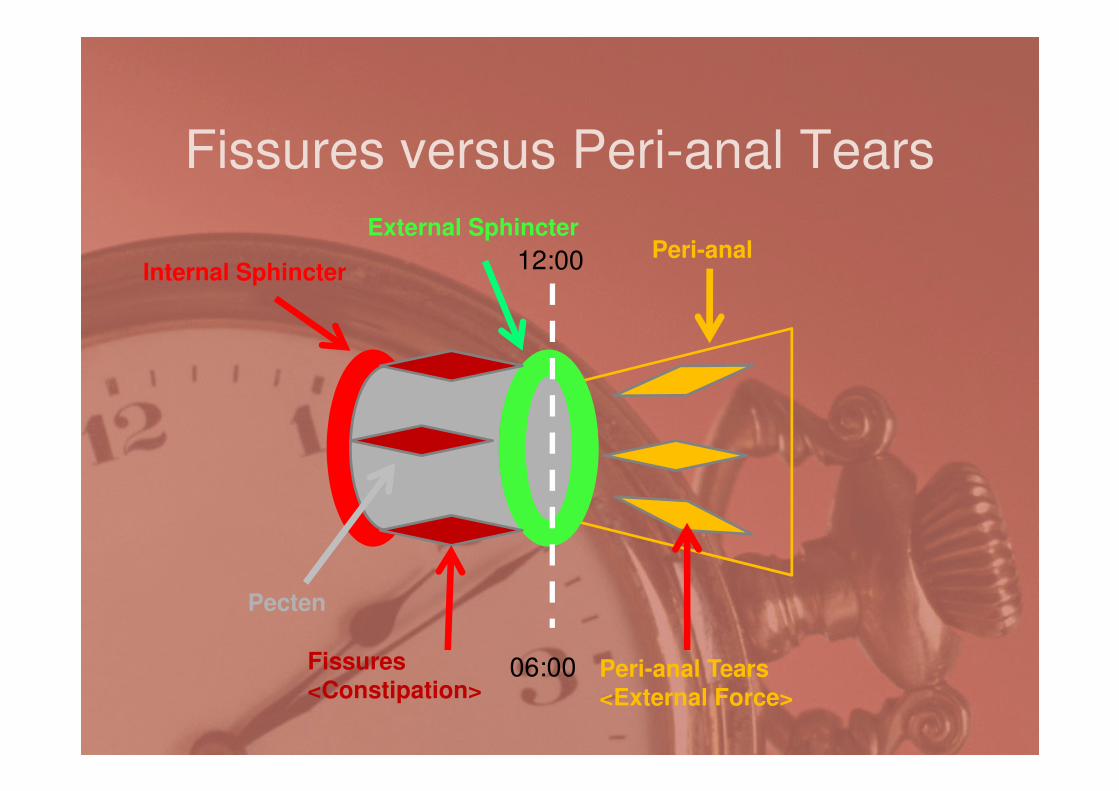
Fissures versus Peri-anal Tears
12:00 Peri-analExternal Sphincter
Internal Sphincter
06:00Fissures
<Constipation>Peri-anal Tears<External Force>
Pecten

Acute Fissures
• Is a deep tear through the anal marginextending into the anal canalextending into the anal canal
• There is little inflammation induration or oedema of its edges
• Associated anal spasm and pain
• Retain stools – vicious cycle
Fissures
• The McCann study - zero fissures
• Berenson (1993) - 89 children < 18 months
• 1 child with fissures
• 3 with anal tags
•CONSTIPATION can cause fissures - The
appearance cannot indicate the causative
mechanism. Small fissures are not consistent with abuse
•Deep fissures will heal with TAG formation

Chronic Fissures
• Has inflamed indurated margins
• The ulcer base is either:• The ulcer base is either:
– Scar tissue
– Internal sphincter muscle
• Is canoe shaped
• Has an anal tag [sentinel pile] inferior
• Piles are in the midline

Peri-anal skin tag
Sentinel Pile

Notes: Tears in the 11:00 and 07:00 [None are midline tears]
Both are in the peri-anal positionBoth are beyond the impact zone of constipated stools

NOTES: Multiple peri-anal tears highlighted with Toluidine Blue dye
These are beyond the anal margin – excluding constipation
fissures
ONLY AN EXTERNAL FORCE CAN BE RESPONSIBLE!!!

Abuse & the anusAbuse & the anus

The anus in abuse
Frequency of anal involvement
– ♂ 40 – 83%– ♂ 40 – 83%
– ♀ 10 – 29%
– Penis 62%
– Repeated abuse 68%
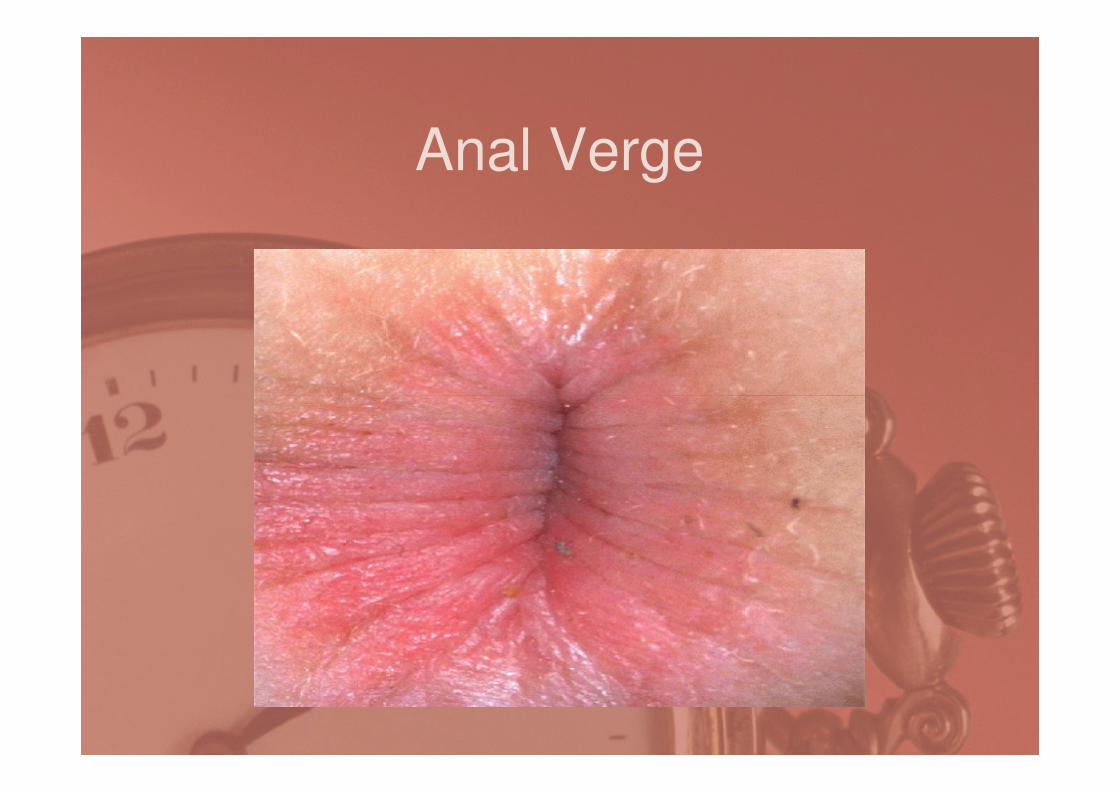
Anal Verge

Anal Rugae

Pecten Line
Pecten Line
Anal Verge
Pecten

Midline Fusion Defect

Peri-anal Tears
Child had been
gone for 24 gone for 24
hours – was
found without
panties
This was the
clinical picture

Peri-anal Hypertrophy
1 Year old child with
hypertrofied peri-anal
skin
The father confessed
to sodomy

Anal fissures
2 yr old with
history of history of
chronic
constipation.
Exam shows &
midline fissure &
skin tag

Tear Scar

Peri-anal Abrasions

Peri-anal Redness

Anal Dilatation
NORMAL
External sphincter
Internal sphincter
Column/Pecten
FUNNELING DILATATION

Cupping/Funneling
External sphincter- dilated
Internal sphincter- contracted
ColumnDilated

Tire Sign
External sphincter(contracted/swollen)
Internal sphincter(dilated)
Column
(Dilated)
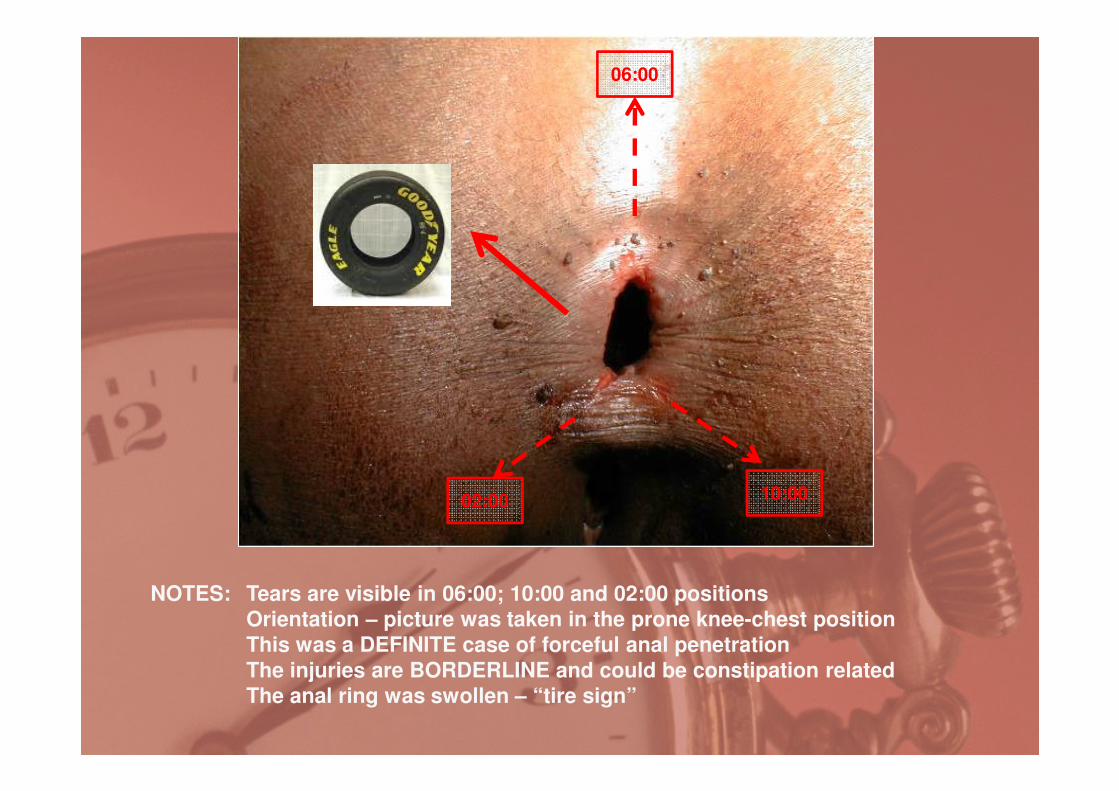
06:00
NOTES: Tears are visible in 06:00; 10:00 and 02:00 positions
Orientation – picture was taken in the prone knee-chest position
This was a DEFINITE case of forceful anal penetration
The injuries are BORDERLINE and could be constipation related
The anal ring was swollen – “tire sign”
10:0002:00

Adams Classification
• Category 1 [No indication of abuse]
– Perianal pigmentation– Perianal pigmentation
– Venous congestion perianal

Adams Classification
• Category 2 [Possible abuse]
– Erythema (redness) perianal– Erythema (redness) perianal
– Vesicular lesions (herpes) perianal
– Warts perianal
– Fissures
– Flattened anal folds
– Anal dilatation

Adams Classification
• Category 3: [Probable Abuse]
– Immediate large anal dilation š stools– Immediate large anal dilation š stools
– Acute abrasions, lacerations, bruising
– Peri-anal scar formation

Adams Classification
• Category 4 [Definite abuse]
– Perianal tears into the external – Perianal tears into the external sphincter
– Sperm or DNA confirmation
– Gonorrhoea;
– Syphilis

Back to Marcus X – 5 Years old

12:00
03:0009:00
06:00
01:00
NOTES: Marcus (5 years) was seen approximately 5 months after alleged
sodomy
The position of examination was PRONE KNEE-CHEST
He had a definite scar PERI-ANAL in the 01:00 position

Outcome of Court Case
• Allegations that peri-anal scar could be:
– Result of Chron’s Disease
– As result of a nail injury when mother inserted a
suppository
• Accused found NOT GUILTY
• No doubt existed that Marcus was abused
• No scientific evidence that would connect the
alleged perpetrator

Note
• Paedophiles do not rehabilitate
• Paedophiles always strike again• Paedophiles always strike again
• The timed bomb is ticking

NO TIME