Anaesthessia for EYE Surgery Ramprasad
57
ANAESTHESIA FOR EYE SURGERY Dr Ramprasad Gorai PGT, Department of Anaesthesia, Critical Care & Pain R.G.Kar Medical College
-
Upload
ramprasad-gorai -
Category
Health & Medicine
-
view
580 -
download
1
Transcript of Anaesthessia for EYE Surgery Ramprasad
ANAESTHESIA FOR EYE SURGERY
Dr Ramprasad Gorai
PGT, Department of Anaesthesia, Critical Care & Pain
R.G.Kar Medical College
Anatomy of Eye , Physiology Of IOP
Anaesthetic Ramification of Ophthalmic Drugs
Pre-op Evaluation
Anaesthtic Management Of Specific Situation
Post-op Complications
We will discuss on-
History---
Karl Koller
Karl Koller Austrian ophthalmologist
introduced cocaine as a local
anaesthetic for eye surgery.
Koller was reputedly nick named
"Coca Koller" for his association with the drug.
Hermann Jakob Knapp
1st Describe Needle Based Ophthalmic Regional Anaesthesia.
Atkinson,introduced the retrobulbar block in early 20th
century.

Orbit
ORBIT-1.Eye ball2.Optic Nerve3.Extra-Ocular Muscles4.Vessels5.Fat6.Ciliary Ganglion7.Occulomotor,Trochlear,Abducent Nerves.8.Lacrymal,Frontal,nasociliary br of Trigeminal Nerve.
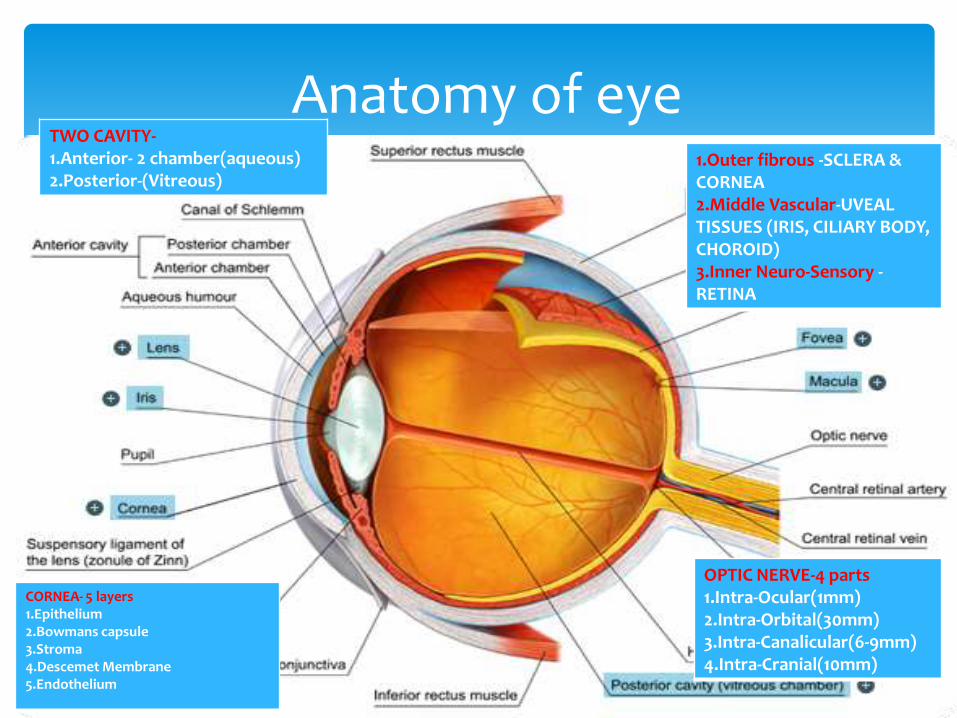
Anatomy of eye1.Outer fibrous -SCLERA & CORNEA2.Middle Vascular-UVEAL TISSUES (IRIS, CILIARY BODY, CHOROID)3.Inner Neuro-Sensory -RETINA
TWO CAVITY-1.Anterior- 2 chamber(aqueous)2.Posterior-(Vitreous)
CORNEA- 5 layers1.Epithelium2.Bowmans capsule3.Stroma4.Descemet Membrane5.Endothelium
OPTIC NERVE-4 parts1.Intra-Ocular(1mm)2.Intra-Orbital(30mm)3.Intra-Canalicular(6-9mm)4.Intra-Cranial(10mm)
Cont..
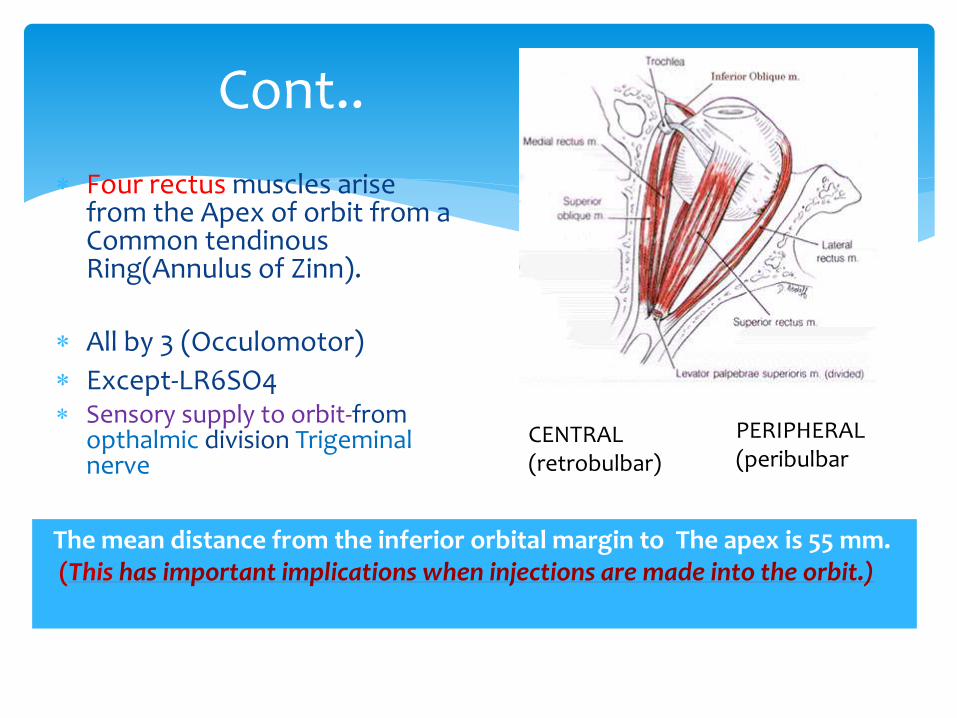
Four rectus muscles arise from the Apex of orbit from a Common tendinousRing(Annulus of Zinn).
All by 3 (Occulomotor)
Except-LR6SO4 Sensory supply to orbit-from
opthalmic division Trigeminal nerve
PERIPHERAL(peribulbar
CENTRAL(retrobulbar)
The mean distance from the inferior orbital margin to The apex is 55 mm. (This has important implications when injections are made into the orbit.)

The blood supply to the retina and optic nerve depends on the intraocular perfusion pressure(IPP).
IPP=MAP-IOP
Normal IOP = 10-20 mm of Hg
IOP varies 1 to 2 mm Hg with each cardiac contraction. Also, a diurnal variation of 2-5 mm Hg is observed
High IOP—1.Impair blood supply, 2.prolapse intraocular content in open eye—> Permanent vision loss.
Physiology of Intra Ocular Pressure-
How aqueous humour formed?
Two third (2/3)-is formed in the posterior chamber by the ciliarybody in an active secretory process involving both the carbonic anhydrase and the cytochrome oxidase systems
The remaining third (1/3)- is formed by passive filtration from the vessels on the anterior surface of the iris
Rate of Production?
@ 2 μL/min.
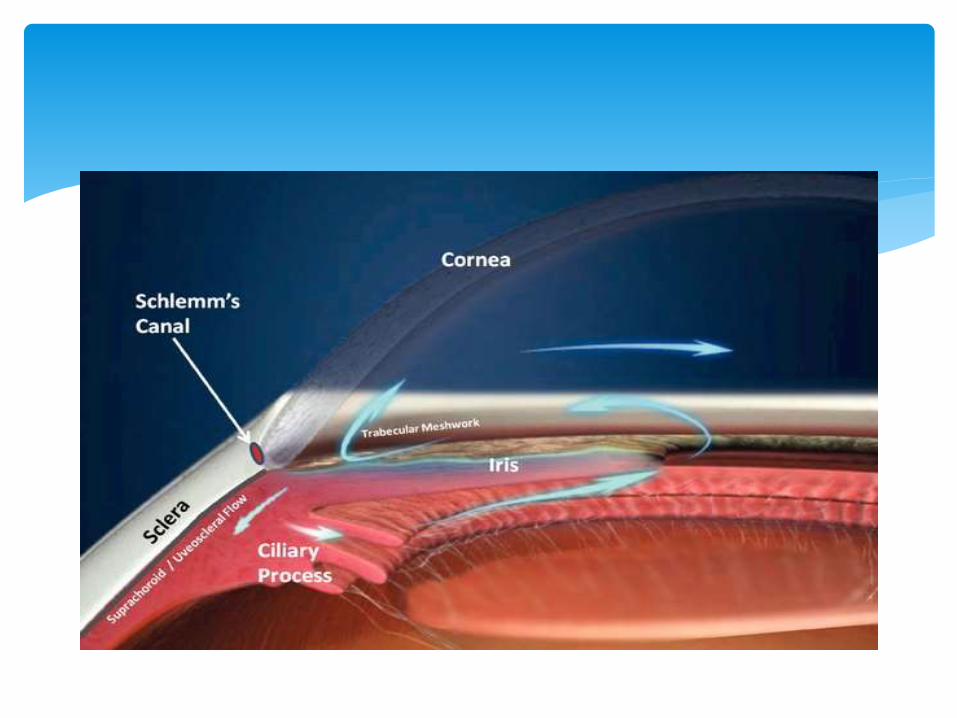
Pathway?
Aqueous humour flow from posterior to anterior chamber through Pupil & then drain out by 2 route- 1.Trabecular outflow(90%) 2.Uveo-scleral outflow(10%).
Mainly-Trabeular meshwork—Schlemms canal– episcleral vein.
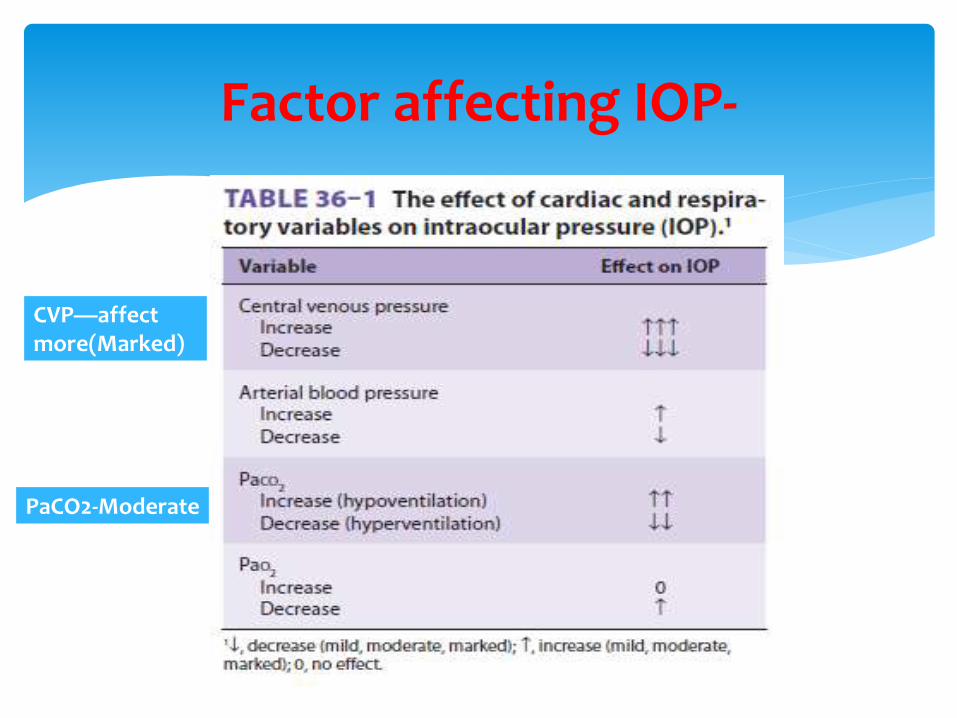
Factor affecting IOP-
CVP—affectmore(Marked)
PaCO2-Moderate

Coughing, straining, or vomiting- can increase IOP to 30 to 40 mm Hg.
Endotracheal intubation can cause similar increases. These increases are transient and are relatively innocuous in a closed eye. In an open eye, (such as after traumatic injury or during cataract surgery) these increases can lead to loss of intraocular contents, hemorrhage, and permanent vision loss.
Extrinsic compression of the eye-also increases the IOP.
A normal blink increases the IOP by 10 mm Hg.
A forceful lid squeeze can increase IOP to more than 50 mm Hg.
A poorly placed anesthesia mask can put enough pressure on the eye to reduce blood flow to zero.
Other factor affecting IOP-

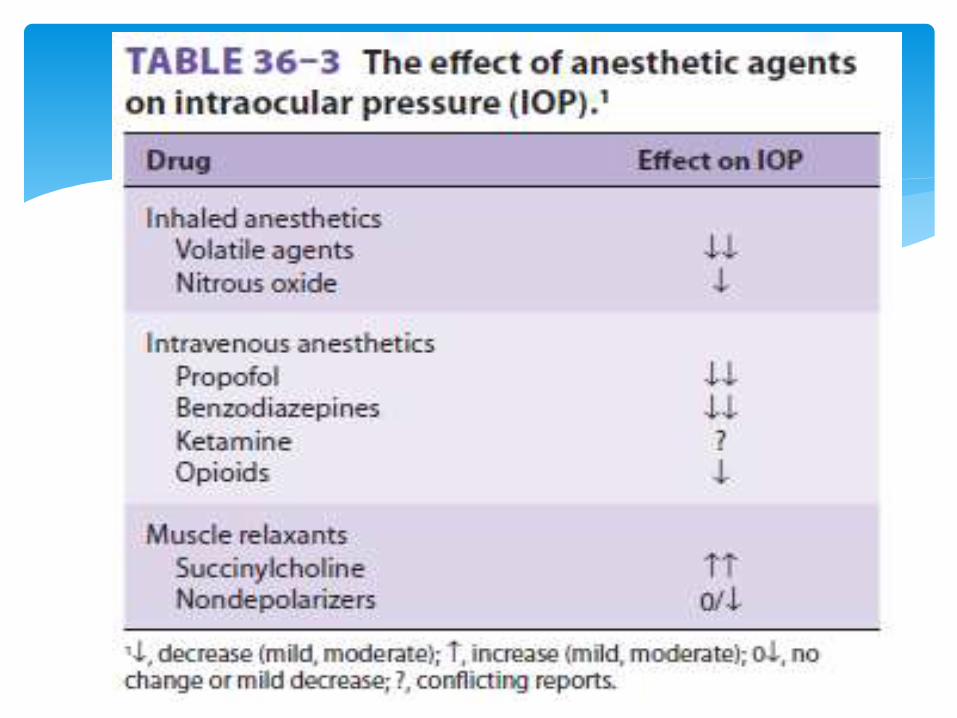
Deep inhaled or intravenous (e.g., propofol) anesthesia -causes a dose-related reduction in IOP by 30% to 40%.
Opioids have little effect.
Atropine (usual dose)-do not cause a significant increase in IOP, even in patients with open-angle glaucoma.
Ketamine – Controversy
Succinylcholine causes IOP to increase by 6 to 12 mm Hg; this lasts for 5 to 10 minutes
Anesthesia Drug & IOP-
ketamine initially was believed to increase IOP significantly,
as measured by indentation tonometry.
More Recent Study using applanation tonometry, shows no
significant rise in IOP (after 2mg/kg IV Ketamine in adult &
8mg/kg IM ketamine in Pediatric patient).
Rather Ketamine may cause Nystagmus & Blepharospasmwhich limit its use in Eye surgery.
Effect of Ketamine-
Nondepolarizing- 2 effect
Direct-Lower IOP by Relaxing Extraocular muscles.
Indirectly-Paralysis of respiratory muscles causes alveolar hypoventilation which increase IOP.
Depolarizing-
Succinylcholine increase IOP about 8 mm Hg within 1-4 Minute & return to baseline within 7 min due to-
1.Tonic contraction of Extraocular muscles,
2.Choroidal Vascular dilation,
3.Relaxation of orbital smooth muscles.
Muscle Relaxant-

Anaesthetic Ramifications of Ophthalmic Drugs
Systemic absorption of topical ophthalmic drugs may occur
from either the conjunctiva or the nasal mucosa after the
drainage through the nasolacrimal duct.
Occluding the nasolacrimal duct by pressing on the inner
canthus of the eye for a few minutes after each instillation
greatly decreases systemic absorption ,thereby systemic side effects.

Carbonic anhydrase inhibitor with Renal tubular effect
Popular Antiglaucoma drug.
It also induces an alkaline diuresis that can result in potassium depletion.
Patients taking acetazolamide should have electrolytes checked preoperatively.
Acetazolamide

Atropine E/D-Used for Mydriasis & Cycloplegia.
can cause tachycardia, dry skin, fever, and agitation.
Overdose can be treated with incremental doses of physostigmine.
Timolol maleate – Non-selective topical β-blocker
Popular anti glaucoma drug.
Systemic absorption causes-bradycardia, bronchospasm,exacerbation of congestive heart failure (especillyin COPD pts) ,execerbation of Myasthenia gravis.
Betaxolol- Beta 1 blocker, More Oculospeific, Minimal Systemic Effect.
Long acting topical anticholin-esterase drug
Used- to maintain miosis in the treatment of glaucoma.
Systemic absorption leads to total body inhibition of plasma cholinesterase.
Subsequent administration of succinylcholine can cause prolonged muscle paralysis.
Inhibition of the metabolism of ester-type local anestheticsmay predispose to local anesthetic toxicity.
Echothiophate is a long-acting. A return toward normal enzyme activity can take 4 to 6 weeks after discontinuation of the drug.
Echothiophate
Phenylephrine is an α-adrenergic agonist
Applied topically to dilate the pupil.
Systemic absorption of the 10% solution is associated with severe hypertension,Headache,Tachycardia
In CAD patient ,10% drop application may cause MI .
Pilocarpine and acetylcholine are cholinergic drugs used to constrict the pupil.
can cause bradycardia and acute broncho-spasm

Mannitol is an osmotic diuretic that causes a decrease in IOP lasting 5 to 6 hours. (Dose= 1.5 gm/kg given over 30-60 min)
Patients who receive mannitol during surgery may need a urinary catheter to avoid over-distention of the bladder.
Mannitol causes an increase in the circulating blood volume, which can lead to congestive heart failure (in patients with poor ventricular function),Pulmonary edema,Hypo or Hypertension,Myocardial ischemia,Renal faliure.

Pre Operative Evaluation
Comorbidity-DM/HTN/IHD/COPD/OSA.
Fasting Status
Allergies & Drug Hypersensitivity.
Current Daily Medication.
Anticoagulant use.
HISTORY-
Stage 3 of severe hypertension is defined as a systolic BP ≥180 mm Hg or
diastolic BP ≥110 mm Hg .
Elective procedures in patients with sustained stage 3 hypertension should be delayed until after 2 weeks of antihypertensive therapy.
What to do if patient is Hypertensive?
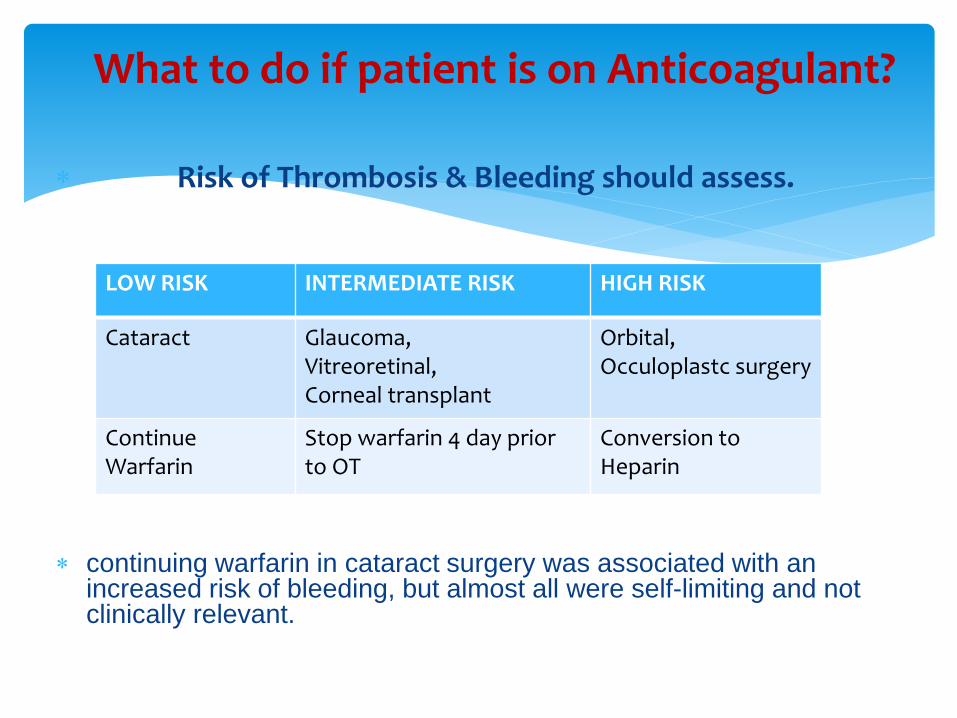
Risk of Thrombosis & Bleeding should assess.
continuing warfarin in cataract surgery was associated with an increased risk of bleeding, but almost all were self-limiting and not clinically relevant.
What to do if patient is on Anticoagulant?
LOW RISK INTERMEDIATE RISK HIGH RISK
Cataract Glaucoma,Vitreoretinal,Corneal transplant
Orbital,Occuloplastc surgery
ContinueWarfarin
Stop warfarin 4 day prior to OT
Conversion to Heparin
Delay Elective Surgery –for at least-
4-6 weeks ---if Bare Metal Stent
12 Months ----if Drug Eluting Stent
What to do if patient have Stent?
ASA task force on preoperative evaluation concluded that
Routine preoperative tests are commonly not useful in
assessing and managing patients’ perioperative experience.
Recent Multi-centric Study----“routine” testing does not
improve patient safety or outcome in cataract surgery.
So, patients having cataract surgery need no preoperative
evaluation.
What Preoperative Investigation to do?
Anaesthesia for Ophthalamic Surgery
Surgeon work near to airway/Head-end.
Most patient are Elderly age gr having associated Comorbidity (DM/HTN/CAD/COPD etc)
Wide Fluctuation of Intraocular Pressure by multiple factors.
Risk of aspiration (eg-Full stomach open globe injury).
Systemic effect of Ophthalmic Drugs.
Problems in Ophthalmic Anaesthesia
Akinesia
Analgesia
Minimal Bleeding
Awareness of drug interactions
Regulation of intraocular pressure
Prevention of the oculocardiac reflex
Management of oculocardiac reflex
Control of intraocular gas expansion
Smooth emergence
Goal of Ophthalmic Anaesthesia-
Types of ocular anaesthesia
General anaesthesia
Local anaesthesiaTopical
Regional
Peribulbar block
Retro-bulbar block
Episcleral or Sub-Tenons block
Facial block
Frontal block
The choice of general v/s local anesthesia is madeon the basis of
the duration of the surgery,
the relative risks and benefits of each techniquefor the patient,
patient preference.
Neither technique has been shown to be safer.
GENERAL VERSUS LOCAL ANESTHESIA

GENERAL ANAESTHESIAFOR OCULAR SURGERY
INDICATION:1. In children and infant2. Anxious & uncooperative
patient3. Mentally retarded adult4. Patient’s preference
ADVANTAGES:
1. safe operative environment
2. Complete akinesia
3. Controlled intra-ocular pressure
4. For bi-lateral surgery
5. Avoiding complications of L/A

Nitrous oxide presents a special problem in some vitreoretinalProcedures-where fluid-gas exchange technique used (surgeon injects an intra-vitreal poorly soluble bubble to tamponade the retina against the wall of the globe).
Sulfur hexafluoride is a poorly soluble agent used commnly.Nitrousoxide diffuses and causes bubble expansion & potential for dangerous increases in IOP. Nitrous oxide should be shut off for 15 minutes before placing the sulfur hexafluoride bubble and should be avoided for 7 to 10 days thereafter.
newer drug, perfluoropropane (C3F8) can persist for weeks. In this case, nitrous oxide should be avoided for at least 1 month, or until the bubble is resorbed.
Nitrous Oxide in Vitreoretinal Surgery-
acts by- producing reversible block to the transmission of peripheral nerve impulses.
Advantages-1.It avoids the potential complications of retrobulbar and peribulbar
injection/GA. 2.most rapid visual rehabilitation,
Disadvantages –1.eye movement during surgery, 2.patient anxiety and discomfort.
Drugs-Tetracaine 0.5% and lignocaine 4%.
Patient Selection-A confident, calm, and cooperative patient usually does well. A nervous, hypersensitive patient may be a better candidate for
another technique.
TOPICAL ANAESTHESIA

Most popular now a days
AIM:
Injected into peribulbar space
Spreads to lid and other spaces
Produces globe and orbicularis akinesia and anaesthesia.
L/A agent :
o Lignocaine 2%
o Bupivacaine 0.75%
o Ropivacaine
Along with
o Hyaluronidase 3-7 IU/ml( Hydrolyse connective tisssue polysaccharides---
Better spread)
o Adranaline 1: 200,000 (reduced bleeding + prolong anesthesia)
PERIBULBAR BLOCK
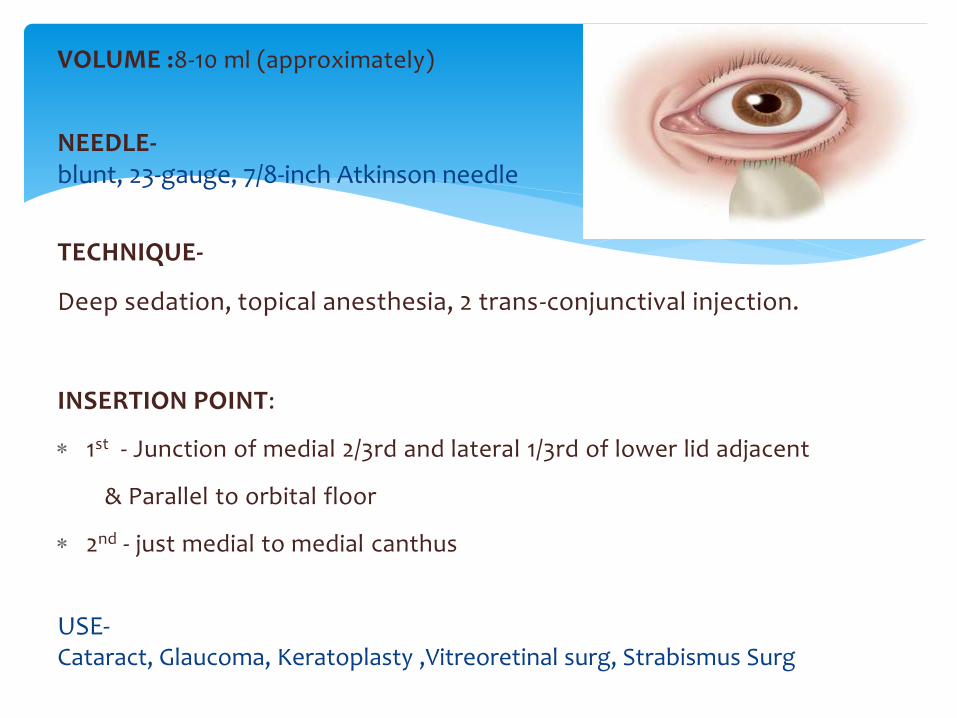
VOLUME :8-10 ml (approximately)
NEEDLE-blunt, 23-gauge, 7/8-inch Atkinson needle
TECHNIQUE-
Deep sedation, topical anesthesia, 2 trans-conjunctival injection.
INSERTION POINT:
1st - Junction of medial 2/3rd and lateral 1/3rd of lower lid adjacent
& Parallel to orbital floor
2nd - just medial to medial canthus
USE-Cataract, Glaucoma, Keratoplasty ,Vitreoretinal surg, Strabismus Surg
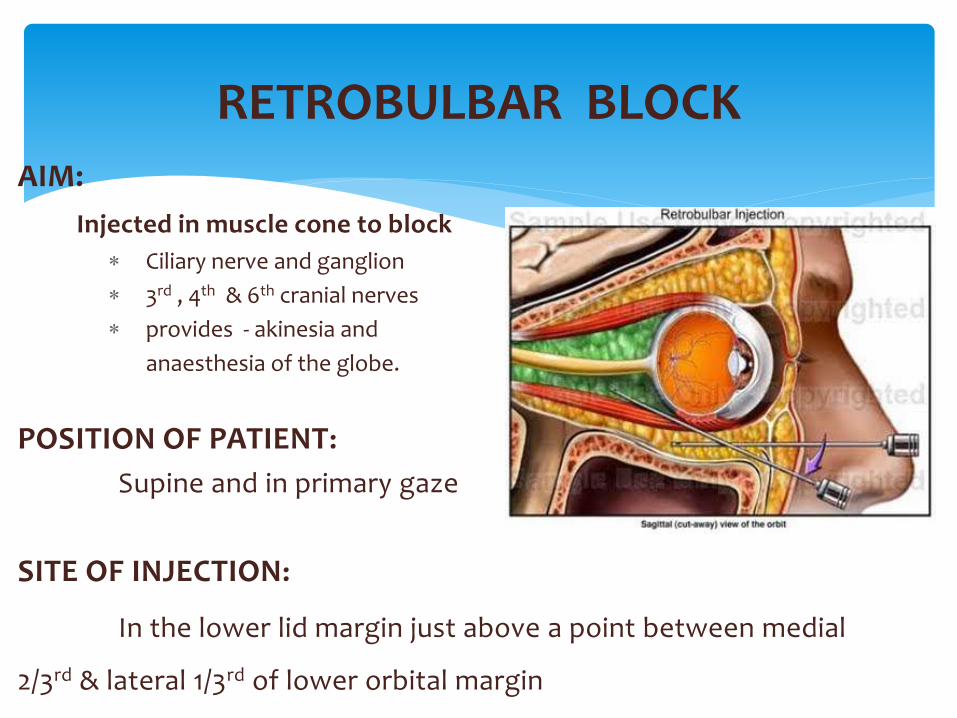
AIM:
Injected in muscle cone to block
Ciliary nerve and ganglion
3rd , 4th & 6th cranial nerves
provides - akinesia and
anaesthesia of the globe.
POSITION OF PATIENT:
Supine and in primary gaze
SITE OF INJECTION:
In the lower lid margin just above a point between medial
2/3rd & lateral 1/3rd of lower orbital margin
RETROBULBAR BLOCK

DIRECTION OF NEEDLE-backward , upwards and medially towards apex of orbit
SUCCESS- successful retrobulbar block is accompanied by anesthesia, akinesia, and abolishment of the oculocephalic reflex (ie, a blocked eye does not move during head turning).
VOLUME: 2 – 5 ml usually
ADVANTAGES:
Complete akinesia
Dilatation of pupil
Adequate and quicker anaesthesia
Minimal amount of agent required.
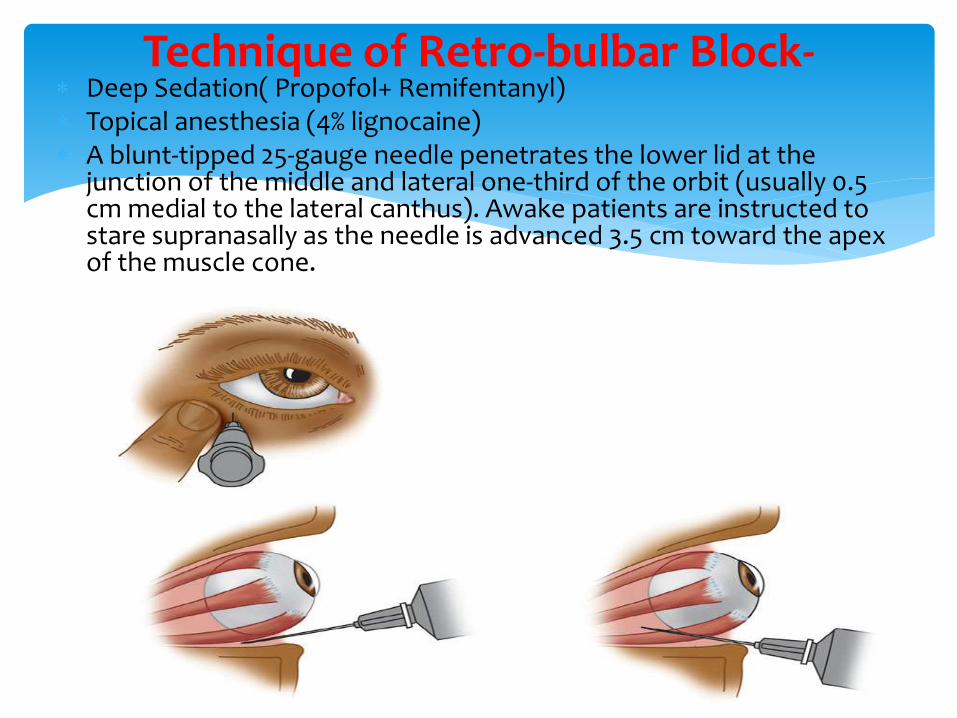
Deep Sedation( Propofol+ Remifentanyl) Topical anesthesia (4% lignocaine) A blunt-tipped 25-gauge needle penetrates the lower lid at the
junction of the middle and lateral one-third of the orbit (usually 0.5 cm medial to the lateral canthus). Awake patients are instructed to stare supranasally as the needle is advanced 3.5 cm toward the apex of the muscle cone.
Technique of Retro-bulbar Block-
Tenon’s fascia surrounds the globe and extraocular muscles.
Local anesthetic (3-4 ml) injected beneath it into the episcleral space spreads circularly around the sclera and to the extraocular muscle sheaths .
A special blunt 25-mm or 19-gauge curved cannula is used for a sub-Tenon block.
After topical anesthesia, the conjunctiva is lifted along with Tenon’s fascia in the inferonasal quadrant with forceps. A small nick is then made with blunt-tipped scissors, which are then slide underneath to create a path in Tenon’s fascia.
Sub-Tenon’s (Episcleral) Block

Performed when complete akinesia desired(as in squint surg).
Techniques-
1.modified van Lint,
2.Atkinson,
3.O’Brien,
4.Nadbath-Rehman block
FACIAL NERVE BLOCK
Complication

Complications- Retrobulbar haemorrhage
Globe penetration
Optic nerve sheath injury
Optic nerve atrophy
Decrease visual acuity
Retinal vascular occlusion
Brain stem anaesthesia
Frank convulsion
Extra ocular muscle palsy
Trigeminal nerve block
Oculo-cardiac reflex
Respiratory arrest
first described by- Aschner and Dagnini in 1908
Receptor-
1. Traction on the extraocular muscles (mainly Medial Rectus)
2.pressure on the globe.
3.Any stmulation of orbital content even periosteum
Afferent –Short and long ciliary nerve ciliary ganglion ophthalmic division of the trigeminal nerve sensory nucleus of the trigeminal near the fourth ventricle.
Integration Centre-Medulla
Efferent -via the vagus nerve to the heart.
Effect-1.bradycardia, 2.atrioventricular block, 3.ventricular ectopy, or 4.asystole.
Oculocardiac Reflex
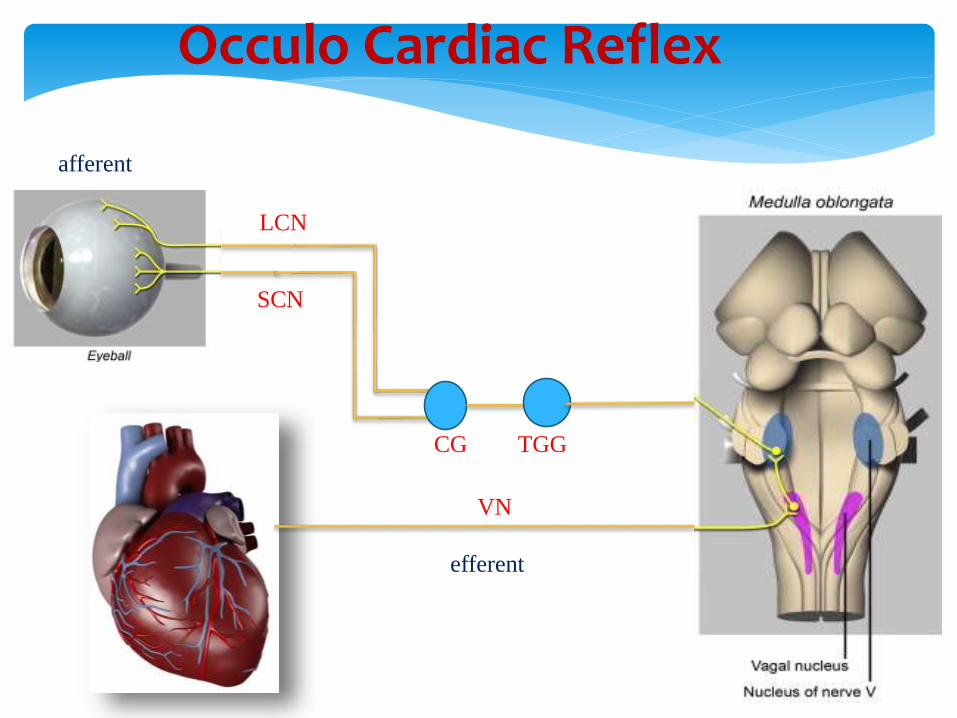
Occulo Cardiac Reflex
LCN
SCN
CG TGG
VN
afferent
efferent
Management-1.first ask the surgeon to stop manipulations.
2.The ventilatory status is assessed.
3.If significant bradycardia persists or recurs, intravenous atropine is administered in 7-μg/kg increments.
4.Rarely, severe bradycardia or asystole require chest compressions(CPR).
Prevention-1.Pre-treatment with intravenous atropine or glycopyrrolate can be effective.
Pre-treatment may be indicated in patients with a history of-1. conduction block, 2.vaso-vagal responses, or 3.β-blocker therapy.
Oculocardiac Reflex
Anaesthtic Management Of Specific Situation
Issues/Problem-
Risk of aspiration against the Risk of blindness
(elevated IOP in injured eye --> extrusion of ocular contents)
Plan of Anesthesia-
Regional anesthesia (eg, retrobulbar block) is relatively contraindicated in patients with penetrating eye injuries because injecting local anesthetic behind the globe increases IOP and may lead to expulsion of intraocular contents.
Therefore, these patients require general anesthesia—despite the increased risk of aspiration pneumonia.
1.Approach to a Patient withan Open Eye & a Full Stomach
1.Exclude other injuries(Skull & Orbital #,ICH,SDH,Abdbleeding)
2.Preop Prophylaxis against Aspiration(H2 Antagonist+ Metoclopramide).
3.Avoid Head down position (which increase IOP).
4.Avoid pressure on eye ball by face mask.
What precaution to take in Open Globe Injury?
5.RSI- Propofol/Thiopentone ,Scoline/Rocuroneum(if Sugamadexavailable)
[Scoline only moderaely increase IOP,Other measures if done appropriately then Scoline induced Increase IOP is Insignificant]
6.Avoid Premature attempt of Intubation as it produce cough,staining& increase IOP .
7.Maintain Deep Plane of anaesthesia
8.Extubate in deep plane with Lignocaine 1.5 mg/kg 90 sec before.
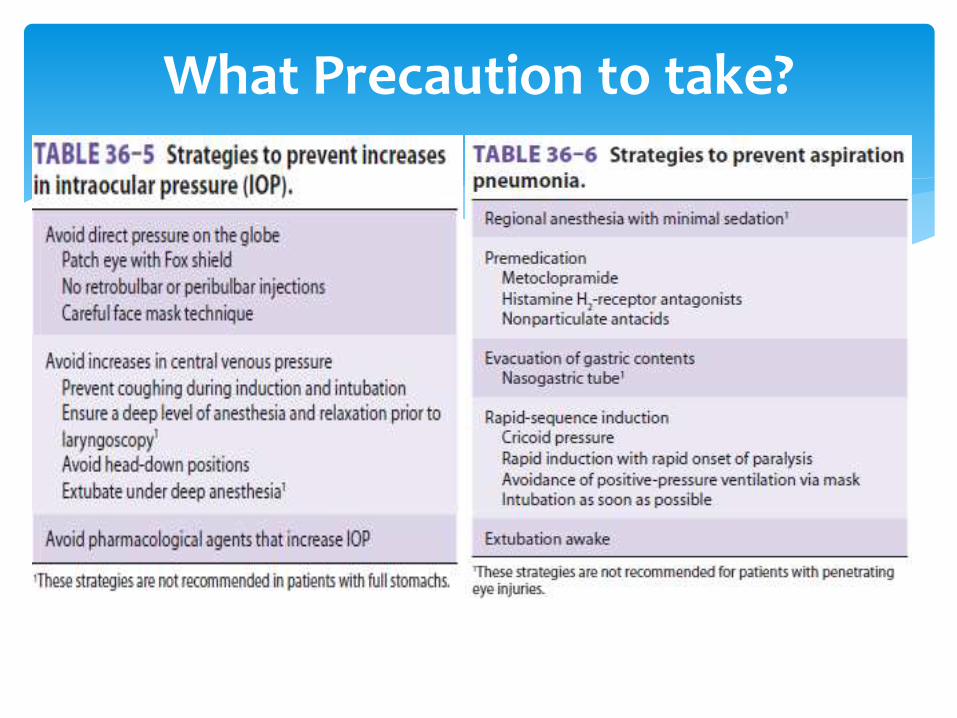
What Precaution to take?
Many Eye Surgery done under Topical & Regional Anaesthesia.
No Preoperative Investigations Required.
Every Patient Should be assess Clinically before OT for Comorbidity & Risk assessment.
Every measure to be taken to prevent rise in IOP.
In Patient with Open Eye & Full stomach-General Anesthesia is preferred regardless of Fasting status but All measure to be taken to prevent Risk of Aspiration and to prevent Rise in IOP.
TAKE HOME MASSAGES

THANK YOU