An update on vitamin D as related to nephrology practice: 2003
6
Kidney International, Vol. 64, Supplement 87 (2003), pp. S125–S130 An update on vitamin D as related to nephrology practice: 2003 JACK W. COBURN The Medical and Research Services, Veterans Affairs Greater Los Angeles Healthcare System, West Los Angeles, and Department of Medicine, David Geffen School of Medicine at UCLA, Los Angeles, California An update on vitamin D as related to nephrology practice: 2003. In this article, an up-to-date consideration of vitamin D therapeutics in nephrology is reviewed. The condition of vita- min D insufficiency is defined as the level of serum 25(OH)- vitamin D at which vitamin D 2 or D 3 supplementation leads to a reduction of levels of parathyroid hormone (PTH). The risks of such vitamin D insufficiency in the normal population and likely risks in individuals with chronic kidney disease (CKD) stages 3 and 4 are reviewed. The potential for its safe treatment and prevention using moderate supplements of vitamin D 2 or vitamin D 3 are outlined. The role of altered “vitamin D nutri- tion” in leading to the observed greater incidence of secondary hyperparathyroidism in African Americans with ESRD com- pared to other racial groups is considered. The actions of active vitamin D sterols to augment intestinal absorption of both calcium and phosphorus, the effect to reduce levels of PTH, and to be a factor contributing to the rising incidence of low bone turnover (adynamic bone) are discussed. Growing evi- dence for contributions of elevated levels of serum calcium, serum phosphorus, and the calcium phosphorus product as factors contributing to vascular and cardiac calcification in ESRD patients are cited. Questions are raised about whether the current practice of vitamin D usage in ESRD patients might be a contributing factor to such vascular abnormalities. The economic factors that likely affect the usage of intravenous vitamin D sterols in the United States are reviewed. It is recom- mended that potential adverse vascular effects of vitamin D sterols related to the increments of serum Ca and P be carefully evaluated. This review focuses on several aspects of the clinical use of vitamin D sterols, which include: (1 ) the recent data regarding vitamin D nutrition as a factor leading to osteoporosis and the potential role of impaired vita- min D nutrition in patients with chronic kidney disease (CKD); (2 ) the clinical actions of the active vitamin D sterols, including the newer active analogs of calcitriol used in the management of secondary hyperparathyroid- ism in ESRD; (3 ) the economic factors that may affect vitamin D usage in the United States; and (4 ) a consider- Key words: renal osteodystrophy, vitamin D, calcitriol. 2003 by the International Society of Nephrology S-125 ation of clinical practices of vitamin D usage that could, indeed, be harmful. The data derived from study of the elderly and of those with osteoporosis have provided important implications regarding patients with kidney disease. The changes of vitamin D metabolism during the development of vita- min D deficiency, as studied in dogs fed a low calcium and vitamin D-deficient diet for two years [1], are pertinent. Serum iPTH levels rose within days with accompanying hypophosphatemia; however, serum 1,25-dihydroxyvita- min D (calcitriol) levels rose even as 25-hydroxyvita- min D levels fell. These adaptations maintained normal ionized Ca levels for 6 months. Subsequently, hypocal- cemia appeared, 1,25(OH) 2 D levels fell (although remain- ing within the normal range), and 25(OH)D levels de- creased further to very low levels. Thus, the serum level of 25-hydroxyvitamin D, not the level of 1,25-dihydroxy- vitamin D, provides an indication of the body stores of vitamin D. 25-Hydroxyvitamin D, which circulates at a concentration 1000-fold higher than that of 1,25-dihydroxy- vitamin D or calcitriol, has a plasma half-life of 25 to 30 days, and the measurement of 25(OH)D levels provides a means to detect vitamin D deficiency or insufficiency, even in those with kidney disease [2, 3]. The measure- ment of plasma 1,25(OH) 2 D levels can be useful to iden- tify unusual causes of hypercalcemia or hyperphosphate- mia, but its measurement provides no indication of nutritional vitamin D-deficiency [4]. The maintenance of normal or even elevated serum levels of 1,25(OH) 2 D in severe secondary hyperparathyroidism due to vitamin D-deficiency occurs because of the highly efficient con- version of 25(OH)D to 1,25(OH) 2 D, even when the con- centration of the former is markedly reduced [5]. A modest reduction in the serum level of 25(OH)D, the substrate for the generation of 1,25(OH) 2 D, leads to mild secondary hyperparathyroidism in those with normal kidney function [6, 7] and may aggravate second- ary hyperparathyroidism in those with chronic kidney disease and reduced renal function [8, 9]. True vitamin D deficiency, with hypocalcemia and osteomalacia, is rare
Transcript of An update on vitamin D as related to nephrology practice: 2003

Kidney International, Vol. 64, Supplement 87 (2003), pp. S125–S130
An update on vitamin D as related tonephrology practice: 2003
JACK W. COBURN
The Medical and Research Services, Veterans Affairs Greater Los Angeles Healthcare System, West Los Angeles,and Department of Medicine, David Geffen School of Medicine at UCLA, Los Angeles, California
An update on vitamin D as related to nephrology practice:2003. In this article, an up-to-date consideration of vitamin Dtherapeutics in nephrology is reviewed. The condition of vita-min D insufficiency is defined as the level of serum 25(OH)-vitamin D at which vitamin D2 or D3 supplementation leads toa reduction of levels of parathyroid hormone (PTH). The risksof such vitamin D insufficiency in the normal population andlikely risks in individuals with chronic kidney disease (CKD)stages 3 and 4 are reviewed. The potential for its safe treatmentand prevention using moderate supplements of vitamin D2 orvitamin D3 are outlined. The role of altered “vitamin D nutri-tion” in leading to the observed greater incidence of secondaryhyperparathyroidism in African Americans with ESRD com-pared to other racial groups is considered. The actions of activevitamin D sterols to augment intestinal absorption of bothcalcium and phosphorus, the effect to reduce levels of PTH,and to be a factor contributing to the rising incidence of lowbone turnover (adynamic bone) are discussed. Growing evi-dence for contributions of elevated levels of serum calcium,serum phosphorus, and the calcium � phosphorus productas factors contributing to vascular and cardiac calcification inESRD patients are cited. Questions are raised about whetherthe current practice of vitamin D usage in ESRD patients mightbe a contributing factor to such vascular abnormalities. Theeconomic factors that likely affect the usage of intravenousvitamin D sterols in the United States are reviewed. It is recom-mended that potential adverse vascular effects of vitamin Dsterols related to the increments of serum Ca and P be carefullyevaluated.
This review focuses on several aspects of the clinicaluse of vitamin D sterols, which include: (1) the recentdata regarding vitamin D nutrition as a factor leadingto osteoporosis and the potential role of impaired vita-min D nutrition in patients with chronic kidney disease(CKD); (2) the clinical actions of the active vitamin Dsterols, including the newer active analogs of calcitriolused in the management of secondary hyperparathyroid-ism in ESRD; (3) the economic factors that may affectvitamin D usage in the United States; and (4) a consider-
Key words: renal osteodystrophy, vitamin D, calcitriol.
2003 by the International Society of Nephrology
S-125
ation of clinical practices of vitamin D usage that could,indeed, be harmful.
The data derived from study of the elderly and of thosewith osteoporosis have provided important implicationsregarding patients with kidney disease. The changes ofvitamin D metabolism during the development of vita-min D deficiency, as studied in dogs fed a low calcium andvitamin D-deficient diet for two years [1], are pertinent.Serum iPTH levels rose within days with accompanyinghypophosphatemia; however, serum 1,25-dihydroxyvita-min D (calcitriol) levels rose even as 25-hydroxyvita-min D levels fell. These adaptations maintained normalionized Ca levels for 6 months. Subsequently, hypocal-cemia appeared, 1,25(OH)2D levels fell (although remain-ing within the normal range), and 25(OH)D levels de-creased further to very low levels. Thus, the serum levelof 25-hydroxyvitamin D, not the level of 1,25-dihydroxy-vitamin D, provides an indication of the body stores ofvitamin D. 25-Hydroxyvitamin D, which circulates at aconcentration 1000-fold higher than that of 1,25-dihydroxy-vitamin D or calcitriol, has a plasma half-life of 25 to 30days, and the measurement of 25(OH)D levels providesa means to detect vitamin D deficiency or insufficiency,even in those with kidney disease [2, 3]. The measure-ment of plasma 1,25(OH)2D levels can be useful to iden-tify unusual causes of hypercalcemia or hyperphosphate-mia, but its measurement provides no indication ofnutritional vitamin D-deficiency [4]. The maintenanceof normal or even elevated serum levels of 1,25(OH)2Din severe secondary hyperparathyroidism due to vitaminD-deficiency occurs because of the highly efficient con-version of 25(OH)D to 1,25(OH)2D, even when the con-centration of the former is markedly reduced [5].
A modest reduction in the serum level of 25(OH)D,the substrate for the generation of 1,25(OH)2D, leadsto mild secondary hyperparathyroidism in those withnormal kidney function [6, 7] and may aggravate second-ary hyperparathyroidism in those with chronic kidneydisease and reduced renal function [8, 9]. True vitamin Ddeficiency, with hypocalcemia and osteomalacia, is rare

Coburn: An update on vitamin DS-126
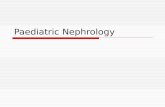
Fig. 1. Changes from baseline of serum calcium levels during therapywith either paricalcitol (solid bars) or intravenous doxercalciferol (cross-hatched bar) observed in controlled trials that employed only calcium-based phosphate-binding agents. The data are mean � SE when suchinformation can be calculated or shown without an “error” bar whenvariance of the data was not provided. “No.” indicates the number ofsubjects receiving the sterol in the trial.
in the United States; it is associated with 25(OH)D levelsbelow 5 to 7 ng/mL. However, levels of 25(OH)D from7 to 30 ng/mL, which are within the “reference range”of 7 to 80 ng/mL, are indications of vitamin D insuffi-ciency. The latter is recognized because modest supple-ments of vitamin D2 or D3 can lower serum iPTH levels[10, 11]. Patients over 60 years of age with hip fractureshave lower 25(OH)D levels than age-matched individu-als with no fracture, and “normal” elderly subjects with25(OH)D levels �30 ng/mL have lower bone mineraldensity than those with higher levels [12, 13]. The onlydisagreement is the upper value of serum 25(OH)D levelat which one does not encounter significant numbersof patients with mild elevations of serum iPTH levels,indicating that 25(OH)D levels should be maintained athigher levels. Evidence for the importance and frequencyof vitamin D-insufficiency is indicated by results of pla-cebo-controlled prospective studies in New England [14],Europe [15], and the United Kingdom [16] that demon-strated significant reductions in fracture incidence inindividuals over 60 to 65 years given supplements ofvitamin D3 or D2, 600 to 800 units/day. Thus, vitamin Dinsufficiency is characterized clinically by mild secondaryhyperparathyroidism, osteoporosis, and increased risk offracture.
Concerning patients with kidney disease, one study of
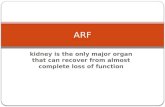
Fig. 2. The percentage of all serum calcium measurements that ex-ceeded various limits is shown on the horizontal axis in two trials usingeither paricalcitol or intravenous doxercalciferol. For some of the limits,the data were not available. For clarity, the percentage is shown in alog10 scale. N is the total number of measurements.
63 non-nephrotic patients with varying levels of renalfunction found median values of 25(OH)D to be 12, 19,and 18 ng/mL in subgroups with glomerular filtration rate(GFR) estimated to be 60 to 90 mL/min, 40 to 60 mL/min, and 20 to 40 mL/min, respectively [17]. Most had25(OH)D values below 30 ng/mL and many had levelsbelow 15 ng/mL [17]. In another study of 76 CKD pa-tients, 37 with diabetic kidney disease and 39 CKD fromother causes [18], the 25(OH)D level averaged 22 � 9.4in the nondiabetic group and 11 � 5.6 pg/mL in thediabetic patients. The serum albumin levels were lowerin the diabetics and 76% had urinary protein concentra-tions above 300 mg/dL compared to only 23% of thenondiabetic group. In another study that included 27patients with GFR of 30 to 70 mL, 79% of patients had25(OH)D levels below 30 ng/mL and the levels werebelow 16 ng/mL in 18% [19]. In a United States studyof 20 patients with GFR of 18 to 70 mL/min, the mean25(OH)D levels were 12 ng/mL in those with nephroticsyndrome, and 20 ng/mL in those lacking nephrotic pro-teinuria. Most subjects in both groups obviously hadsuboptimal levels of 25(OH)D. In a United States studyof medical inpatients, with exclusion of those undergoingdialysis, the presence of impaired renal function was arisk factor for the finding of low levels of 25(OH)D [11].In the two largest series of CKD patients noted above,there were significantly positive correlations between thelevels of 1,25(OH)2D and those of 25(OH)D, with r �0.51 [20] and r � 0.47 [18]. These observations differfrom findings in normal individuals, including those withvitamin D deficiency [5], in whom 1,25(OH)2D levels arenot dependent on the 25(OH)D levels, even in thosewith low levels of 25(OH)D [5]. The normal highly effi-cient renal production of 1,25(OH)2D may be altered in

Coburn: An update on vitamin D S-127
CKD, stages 3 and 4, when the supply of 25(OH)D isreduced. Thus, the levels of 1,25(OH)2D may be depen-dent on the availability of its substrate, 25(OH)D, inpatients with CKD, stages 3 and 4 [4], and in those withESRD [21].
Because of the higher frequency of secondary hyper-parathyroidism in African Americans compared to whitesboth with ESRD [22] and with mild to moderate renalinsufficiency [23], a consideration of vitamin D nutritionin African Americans is pertinent; this is reviewed indetail elsewhere [24]. In normal African Americans liv-ing in temperate climates of Europe and the UnitedStates, the impaired dermal synthesis of vitamin D likelyresults in 25(OH)D levels that are about 50% lower thanthose in whites; the concomitant findings that iPTH levelsare slightly higher and 1,25(OH)D levels are increasedare not surprising. These biochemical features are totallyreversed by the administration of either vitamin D or25(OH)D. When black African individuals moved fromthe Congo to Belgium, there was a fall of mean 25(OH)Dlevels from 50 to 9 ng/mL over two years, a finding thatindicated that sun exposure at latitudes near the equatorled to adequate vitamin D synthesis. It is known thatbone biopsies in healthy African Americans show ero-sion surfaces that are about 50% lower than in whites[25], indicating there is altered skeletal responsivenessto PTH for reasons that are uncertain. It is well knownthat bone density is higher in normal African Americansthan whites, with similar findings in ESRD. Moreover,African Americans with ESRD and of either genderhave a reduced risk of fracture [26]. Nonetheless, pro-gressive secondary hyperparathyroidism is common inAfrican Americans as the duration of dialysis increases.
It is a proposed recommendation of the Kidney Dial-ysis Outcomes Quality Initiative (K-DOQI) WorkGroup that serum 25(OH)D level be measured in pa-tients with CKD, stages 3 and 4, with elevations of iPTHabove certain limits. If the 25(OH)D levels are below30 ng/mL, replacement with vitamin D is recommended.Because of its pharmaceutical availability, the most con-venient method in the United States is the monthly ad-ministration of ergocalciferol (vitamin D2), 50,000 IUeach month. From a safety standpoint, this monthly doseis less than the upper limit of daily dosage of 2000 IU/day recommended by the Food and Nutrition Board,National Research Council, and National Academy ofSciences. Treatment of overt vitamin D deficiency withevidence of osteomalacia and severe secondary hyper-parathyroidism requires larger doses. A parenteral formof ergocalciferol, with 500,000 IU per mL, is availablefor intramuscular administration. It has been suggestedthat the administration of one single large intramusculartreatment may be curative for vitamin D deficiency [27],avoiding the problem with compliance, particularly indeveloping countries where either limited access to care
and/or cultural differences or customs leads to poor com-pliance and treatment failure [28]. The sterol 25(OH)D3,or calcifediol, has been available for 20 years; there maybe a small pharmaceutical advantage of using calcifediolrather than calciferol or ergocalciferol to treat vita-min D deficiency since calcifediol is available in 20 and50 �g capsules (Calderol�, Organon). However, this prod-uct may not be readily available, and the added cost maynot justify its use. For the prevention or treatment ofvitamin D deficiency or insufficiency as defined by25(OH)D levels, there is no place for the use of calcitriol,alfacalcidol, or any of the newer active vitamin D analogs.
ACTIVE VITAMIN D STEROLS IN ESRD
In conjunction with phosphate-binding agents, theactive vitamin D sterols, calcitriol and alfacalcidol(1�(OH)D3), have been utilized for more than 20 years,with intravenous forms in wide use for 10 years, particu-larly in the United States. The known actions of calcitriolinclude augmentation of intestinal absorption of bothcalcium and phosphorus [29], with a tendency for serumCa and P to rise when kidney function is reduced. Be-cause of calcitriol’s indirect effect to raise serum Ca leveland its direct action to reduce the synthesis of mRNAfor pre- pro-PTH in the parathyroid gland, there is re-duced PTH secretion. There are no conclusive data thattreatment with calcitriol or alfacalcidol has any effect toreverse pre-existing parathyroid hyperplasia.
With the use of intravenous “pulse” therapy, boneturnover is reduced and this is the dominant effect onbone. During intravenous calcitriol therapy, the degreeof reduction of bone formation rate (BFR) seems to begreater than the reduction of PTH levels. This reducedBFR arises due to a reduction of the length of doublelabel, with the apposition rate, or distance between thedouble labels, remaining unchanged [30]. This indicatesthat a major effect of pulse calcitriol on bone is to dimin-ish the number of active osteoblasts. In studies in chil-dren and adolescents, pulse calcitriol therapy has beenshown to lead to the appearance of adynamic bone [31]and, in pre-pubertal children with ESRD, to reduce therate of linear growth [32]. There is indirect evidencethat pulse therapy with calcitriol, combined with thewidespread use of calcium-based phosphate-bindingagents, contributes to the increased prevalence of ady-namic bone. Another change over the last decade hasbeen a change in the relationship between bone turnoverrate, as determined from bone biopsy, and the levels ofintact PTH. In studies of ESRD patients undergoingbiopsies between 1985 and 1990, correlations betweenBFR and iPTH were reasonably good as long as alumi-num-induced bone disease was excluded [33, 34]. In amore recent biopsy series that included some patientswho received pulse vitamin D therapy for varying peri-

Coburn: An update on vitamin DS-128
ods, very poor correlations between iPTH levels andbone turnover were found. Indeed, the level of iPTHdid not distinguish between adynamic bone from bonehaving normal or high turnover when the iPTH levelsranged from 200 to 600 pg/mL [35].
During the last five years, two new vitamin D sterolshave been introduced in Japan and two in the UnitedStates. For two sterols, 22-oxa-calcitriol (maxicalcitol)and paricalcitol (1,25(OH)2-19-nor-vitamin D2), thereare studies in experimental animals showing little or noaugmentation of intestinal calcium absorption, whilethere were potent actions to suppress PTH levels inde-pendent of increments in serum Ca [36, 37]. The presentdiscussion will be limited to paricalcitol and doxercalcif-erol, two newer sterols used in the United States. Doxer-calciferol (1�(OH)D2), like alfacalcidol, is a prohormonethat is 25-hydroxylated in the liver before inducing itsactions. In vitamin D deficiency animals, doxercalciferoland alfacalcidol are equally potent in curing rickets; how-ever, when given in larger doses, doxercalciferol had farless calcemic action [38]. In an animal model of osteopo-rosis produced by ovariectomy, doxercalciferol protectedagainst bone loss without increasing urinary Ca, whilethe other sterols tested, including 1�(OH)D3, caused sub-stantial hypercalciuria when given in doses that protectedagainst bone loss [39]. In osteoporotic women, the ad-ministration of doxercalciferol in doses up to 5 �g/daydid not produce hypercalciuria [40], while much smallerdoses of (1�(OH)D3) produced significant hypercalciuria[41].
The clinical data analyzed for the effects of paricalcitoland doxercalciferol are limited to reports of prospectivestudies in comparison to placebo [42–45]. For paricalcitolcompared to calcitriol, a large blinded comparison ofintravenous paricalcitol to intravenous calcitriol hasbeen reported. In all of these trials, only calcium-basedphosphate-binding agents were employed. Both parical-citol [42] and doxercalciferol [46] were highly effectivein lowering iPTH levels, although the trials with oraldoxercalciferol included a substantial fraction with iPTHlevels above 1200 pg/mL [47].
Clinical trials with both paricalcitol and doxercalcif-erol showed modest increments in both serum calciumand phosphorus, and there are no studies with eithersterol, such as have been reported with calcitriol, thatmeasured intestinal absorption of calcium and phospho-rus using either balance techniques or radiolabeled cal-cium. The observation that hypercalcemia was morelikely to occur in trials with paricalcitol when the serumiPTH levels were reduced below 100 pg/mL suggests thatsuch patients likely had oversuppression of PTH withadynamic bone [48], with the lack of bone buffering, ashas been documented in patients with biopsy demonstra-tion of adynamic bone [49]. Since all the studies citedfor comparison employed only calcium-based phosphate-
binding agents, any effect of the sterol to augment intesti-nal absorption would be amplified by the high calciumintake.
In this comparison of the effects of these sterols toraise serum calcium, there are five controlled studiesusing paricalcitol [42, 43, 44, 45] with data that permitthe determination of the relative increase of serum cal-cium, and one trial with intravenous doxercalciferol [46](Fig. 1). With paricalcitol, the rise of serum calcium was3% to 4% in three trials [42, 43], while the rise wasgreater in two studies with far fewer patients in the stud-ies [44, 45]. In the trial using intravenous doxercalciferol,the increment of calcium averaged 4% at eight weeksof therapy [46]. In two trials reporting data on the frac-tions of serum calcium measurements that exceeded lev-els from �10.5 to �12.0 mg/dL, no differences could beseen between the two sterols (Fig. 2). The mean incre-ments of serum phosphorus (data not shown) variedfrom 6.6 to 12.6% in three trials using paricalcitol [42, 43]and were 10.1% in the trial using doxercalciferol [46].Although not direct comparisons, such data suggest thereis little difference between the sterols with regard to theireffect to raise the levels of serum calcium or phosphorus.
The large double-blind trial that compared intrave-nous paricalcitol with intravenous calcitriol [50] is nota-ble. With intravenous paricalcitol, iPTH levels fell morerapidly than was observed in the group receiving intrave-nous calcitriol, possibly related to a ratio of dosing of4:1 for paricalcitol:calcitriol. The fraction of patientsshowing a lowering of iPTH by �50% was 62% withparicalcitol and 54% with calcitriol (P � NS). With re-gard to side effects, 68% of the calcitriol group and 64%of the paricalcitol group had at least one episode ofhypercalcemia (corrected calcium �11.5 mg/dL) or aCa � P product �75 (P � NS). However, in the assess-ment of more prolonged side effects, defined as twosuccessive serum calcium levels �11.5 mg/dL or foursuccessive elevations of the serum Ca � P product �75(with serum calcium and phosphorus measured twiceweekly), the results favored paricalcitol; thus, 18% ofparicalcitol patients compared to 33% of the calcitriolgroup fulfilled these criteria (P � 0.01). Neither the over-all incidence of hyperphosphatemia nor the percentageincrements of serum calcium or phosphorus were re-ported, but inspection of graphic data, provided by Dr.S. Sprague, revealed significant increments in both treat-ment groups. Nonetheless, this large study suggests theremay be some benefit of paricalcitol over calcitriol, withboth given intravenously. A recent report of a retrospec-tive analysis indicates that the mortality of ESRD pa-tients who initiated therapy with intravenous calcitriolwas higher than the mortality of patients given paricalci-tol initially [51]. However, the assignment of patients toone sterol or the other was not random, and it is possible

Coburn: An update on vitamin D S-129
that factors other than the type of vitamin D sterol con-tributed to the difference.
CONCLUSION
This review will conclude with a brief consideration offactors affecting the administration and dosing of thesevitamin D sterols and consider the possibility of deleteri-ous effects. The initial demonstration [52], and then con-firmation that hyperphosphatemia [53–55] and oral cal-cium loading [56] may contribute to vascular and cardiaccalcifications and to increased mortality in ESRD pa-tients, alters the importance of controlling mineral me-tabolism in ESRD patients. These data causes us to ask,“Does our current usage of vitamin D contribute in anyway to the high mortality in ESRD patients?” Might thepotential clinical benefits of lowering of PTH be offsetby detrimental effects caused by increasing the serumlevels of calcium or phosphorus or of both? The preva-lence of calciphylaxis (uremic calcific arteriolopathy),which had largely vanished 20 to 25 years ago, seemsto have risen over the past 10 to 15 years. Could theadministration of pulse doses of calcitriol or other vita-min D sterols contribute to a presumed higher incidenceof this syndrome? Unfortunately, a diagnosis of calciphy-laxis does not appear in ICD9 codes, so its prevalenceis difficult to document. As anecdotal experience, I amunaware of any de novo cases of calciphylaxis appearingin three dialysis centers that I visit, and the fraction ofpatients receiving intravenous vitamin D, when assessedin the past, was only 40% to 45%. Regarding the preva-lence of vitamin D usage in centers describing multiplecases of calciphylaxis, the use of vitamin D use was statedto be either universal or a much higher percentage. Inthe United States, the profit arising from the reimburse-ment for administration of intravenous drugs, such aserythropoietin or intravenous vitamin D sterols, duringhemodialysis may separate a unit showing a “profit” fromanother with problems meeting its costs. The report indi-cating there may be an excess death rate with use ofintravenous calcitriol must raise a question about theappropriateness of current vitamin D usage in the UnitedStates. If increments in the serum phosphorus, serumcalcium, or the calcium � phosphorus product contributeto cardiovascular mortality, it would seem likely thatincrements associated with use of active vitamin D ste-rols may also exert the same detrimental effect. Furthercareful study of such potential side effects of our therapyseems both appropriate and essential.
Reprint requests to Jack W. Coburn, M.D., Nephrology Section,(111L), West Los Angeles V.A. Medical Ctr., 11301 Wilshire Blvd., LosAngeles, CA 90073.E-mail: [email protected]
REFERENCES
1. Cloutier M, Gascon-Barre M, D’Amour P: Chronic adaptationof dog parathyroid function to a low-calcium-high-sodium-vitaminD-deficient diet. J Bone Miner Res 7:1021–1028, 1992
2. Hollis BW: Detection of vitamin D and its major metabolites, inVitamin D, edited by Feldman D, Glorieux FH, Pike JW, SanDiego, Academic Press, 1997, pp 587–606
3. Bouillon R: Radiochemical assays for vitamin D metabolites:Technical possibilities and clinical applications. J Steroid Biochem19:921–927, 1983
4. Coburn JW, Frazao JM: Vitamin D: Normal physiology and vita-min D therapeutics in normal nutrition and various disease states,in Calcium in Internal Medicine, edited by Morii H, NishizawaY, Massry SG, London, Springer-Verlag, 2002, pp 261–305
5. Papapoulos SE, Fraher LJ, Clemens TL, et al: Metabolites ofvitamin D in human vitamin-D deficiency: Effect of vitamin D3 or1,25-dihydroxy-cholecalciferol. Lancet 2:612–615, 1980
6. Khaw KT, Sneyd MJ, Compston J: Bone density, parathyroidhormone and 25-hydroxyvitamin D concentrations in middle agedwomen. BMJ 305:373–376, 1992
7. Ooms ME, Roos JC, Bezemer PD, et al: Prevention of bone lossby vitamin D supplementation in elderly women: A randomizeddouble blind trial. J Clin Endocrinol Metab 80:1052–1058, 1995
8. Eastwood JB, Harris E, Stamp TCB, De Wardener HE: VitaminD deficiency in the osteomalacia of chronic renal failure. Lancet2:1209–1211, 1976
9. Eastwood JB, Stamp TCB, De Wardener HE, et al: The effectof 25-hydroxyvitamin D3 in the osteomalacia of chronic renal fail-ure. Clin Sci 52:499–508, 1977
10. Chapuy MC, Preziosi P, Maamer M, et al: Prevalence of vitaminD insufficiency in an adult normal population. Osteoporosis Int7:439–443, 1997
11. Thomas MK, Lloyd-Jones DM, Thadhani RI, et al: Hypovitamin-osis D in medical inpatients. N Engl J Med 338:777–783, 1998
12. Krall EA, Sahyoun N, Tannenbaum S, et al: Effect of vitaminD intake on seasonal variations in parathyroid hormone secretionin postmenopausal women. N Engl J Med 321:1777–1783, 1989
13. Lips P, Van Ginkel FC, Jongen MJM, et al: Determinants ofvitamin D status in patients with hip fracture and in elderly controlsubjects. Am J Clin Nutr 46:1005–1010, 1987
14. Dawson-Hughes B, Harris SS, Krall EA, Dallal GE: Effectof calcium and vitamin D supplementation on bone density in menand women 65 years of age and older. N Engl J Med 337:670–676,1997
15. Chapuy MC, Arlot ME, Duboeuf F, et al: Vitamin D3 and calciumto prevent hip fractures in elderly women. N Engl J Med 327:1637–1642, 1992
16. Trivedi DP, Doll R, Khaw KT: Effect of four monthly oral vita-min D3 (cholecalciferol) supplementation on fractures and mortal-ity in men and women living in the community: Randomized doubleblind controlled trial. BMJ 326:469–472, 2003
17. Reichel H, Deibert B, Schmidt-Gayk H, Ritz E: Calcium metabo-lism in early chronic renal failure: Implications for the pathogenesisof hyperparathyroidism. Nephrol Dial Transplant 6:162–169, 1991
18. Ishimura E, Nishizawa Y, Inaba M, et al: Serum levels of 1,25-dihydroxyvitamin D, 24,25-dihydroxyvitamin D, and 25-hydroxy-vitamin D in nondialyzed patients with chronic renal failure. Kid-ney Int 55:1019–1027, 1999
19. Messa P, Vallone C, Mioni G, et al: Direct in vivo assessment ofparathyroid hormone-calcium relationship curve in renal patients.Kidney Int 46:1713–1720, 1994
20. Kanis JA, Russell RGG: Rate of reversal of hypercalcemia andhypercalciuria induced by vitamin D and its 1-alpha hydroxylatedderivatives. BMJ 1:78–81, 1977
21. Ghazali A, Fardellone P, Pruna A, et al: Is low plasma 25(OH)-vitamin D a major risk factor for hyperparathyroidism and Looser’szones independent of calcitriol? Kidney Int 55:2169–2177, 1999
22. Gupta A, Kallenback LR, Zasuwa G, Divine GW: Race is amajor determinant of secondary hyperparathyroidism in uremicpatients. J Am Soc Nephrol 11:330–334, 2000
23. De Boer IH, Gorodetskaya I, Young B, et al: The severity ofsecondary hyperparathyroidism in chronic renal insufficiency is

Coburn: An update on vitamin DS-130
GFR-dependent, race-dependent and associated with cardiovascu-lar disease. J Am Soc Nephrol 13:2762–2769, 2002
24. Mitra D, Bell NH: Racial, geographic, genetic, and body habituseffects on vitamin D metabolism, in Vitamin D, edited by FeldmanD, Glorieux FH, Pike JW, San Diego, Academic Press, 1997, pp521–532
25. Weinstein RS, Bell NH: Diminished rates of bone formation innormal black adults. N Engl J Med 319:1698–1701, 1988
26. Alem AM, Sherrard DJ, Gillen DL, et al: Increased risk of hipfracture among patients with end-stage renal disease. Kidney Int58:396–399, 2000
27. Shah BR, Finberg L: Single day therapy for nutritional vitaminD-deficiency rickets: A preferred method. J Pediatr 125:487–490,1994
28. Lubani MM, Al-Shab TS, Al-Saleh QA, et al: Vitamin D-defi-ciency in Kuwait: The prevalence of a preventable disease. AnnTrop Paediatr 3:134–139, 1989
29. Brickman AS, Hartenbower DL, Norman AW, Coburn JW: Ac-tions of 1�-hydroxy- and 1,25-dihydroxyvitamin D3 on mineralmetabolism in man. I. Effects on net absorption of phosphorus.Am J Clin Nutr 30:1064–1070, 1977
30. Andress DL, Norris KC, Coburn JW, et al: Intravenous calcitriolin the treatment of refractory osteitis fibrosa of chronic renal fail-ure. N Engl J Med 321:274–279, 1989
31. Goodman WG, Ramirez JA, Belin TR, et al: Development ofadynamic bone in patients with secondary hyperparathyroidismafter intermittent calcitriol therapy. Kidney Int 46:1160–1166, 1994
32. Kuizon BD, Goodman WG: Juppner H, et al: Diminished lineargrowth during intermittent calcitriol therapy in children undergo-ing CCPD. Kidney Int 53:205–211, 1998
33. Quarles LD, Lobaugh B, Murphy G: Intact parathyroid hormoneoverestimates the presence and severity of parathyroid-mediatedosseous abnormalities in uremia. J Clin Endocrinol Metab 75:145–150, 1992
34. Wang M, Hercz G, Sherrard DJ, et al: Relationship betweenintact 1–84 parathyroid hormone and bone histomorphometricparameters in dialysis patients without aluminum toxicity. Am JKidney Dis 26:836–844, 1995
35. Qi Q, Monier-Faugere M-C, Geng Z, Malluche HH: Predictivevalue of serum parathyroid hormone levels for bone turnover inpatients on chronic maintenance dialysis. Am J Kidney Dis 26:622–631, 1995
36. Brown AJ, Finch JL, Lopez-Hilker S, et al: New active analoguesof vitamin D with low calcemic activity. Kidney Int 29(Suppl29):S22–S27, 1990
37. Finch JL, Brown AJ, Kubodera N, et al: Differential effects of1,25-(OH)2D3 and 22-oxacalcitriol on phosphate and calcium me-tabolism. Kidney Int 43:561–566, 1993
38. Coburn JW, Tan AU, JR, Levine BS: 1�-Hydroxy-vitamin D2: Anew look at an ‘old’ compound. Nephrol Dial Transplant 11(Suppl3):153–157, 1996
39. Erben RG, Bante U, Birner H, Stangassinger M: 1�-hydroxy-vitamin D2 partially dissociates between preservation of cancellousbone mass and effects on calcium homeostasis in ovariectomizedrats. Calcif Tissue Int 60(5):449–456, 1997
40. Gallagher JC, Bishop CW, Knutson JC, et al: Effects of increas-
ing doses of 1�-hydroxyvitamin D2 on calcium homeostasis in post-menopausal osteopenic women. J Bone Miner Res 9:607–614, 1994
41. Brickman AS, Coburn JW, Friedman GS, et al: Comparison ofeffects of 1�-hydroxyvitamin D3 and 1,25-dihydroxy-vitamin D3 inman. J Clin Invest 57:1540–1547, 1976
42. Martin KJ, Gonzalez EA, Gellens M, et al: 19-Nor-1-�-25-Dihy-droxyvitamin D2 (paricalcitol) safely and effectively reduces thelevels of intact parathyroid hormone in patients on hemodialysis.J Am Soc Nephrol 9:1427–1432, 1998
43. Martin KJ, Gonzales E, Lindberg JS, et al: Paricalcitol dosingaccording to body weight or severity of hyperparathyroidism: Adouble-blinded, multicenter, randomized study. Am J Kidney Dis38(Suppl.5):S57–S63, 2001
44. Moe SM, Zekonis M, Harezlak J, et al: A placebo-controlled trialto evaluate immunomodulatory effects of paricalcitol. Am J KidneyDis 38:792–802, 2001
45. Sprague SM, Lerma E, Mccormmick D, et al: Suppression of para-thyroid hormone secretion in hemodialysis patients: Comparisonof paricalcitol with calcitriol. Am J Kidney Dis 83(Suppl.5):S51–S56, 2001
46. Maung HM, Elangovan L, Frazao JM, et al: Efficacy and side-effects of intermittent intravenous and oral doxercalciferol (1�-hydroxyvitamin D2) in dialysis patients with secondary hyperpara-thyroidism: A sequential comparison. Am J Kidney Dis 37:532–543,2001
47. Frazao JM, Elangovan L, Maung HM, et al: Intermittent doxer-calciferol (1�-hydroxyvitamin D2) therapy for secondary hyper-parathyroidism: Results of a modified, double blinded, controlledstudy. Am J Kidney Dis 36:550–561, 2000
48. Martin KJ, Gonzalez EA, Gellens ME, et al: Therapy of second-ary hyperparathyroidism with 19-nor-1�,25-dihydroxyvitamin D2.Am J Kidney Dis 32(Suppl. 2):S61–S66, 1998
49. Kurz P, Monier-Faugere M-C, Bognar B, et al: Evidence forabnormal calcium homeostasis in patients with adynamic bonedisease. Kidney Int 46:855–861, 1994
50. Sprague SM, Llach F, Amdahl M, et al: Paricalcitol versuscalcitriol in the treatment of secondary hyperparathyroidism. Kid-ney Int 63:1483–1490, 2003
51. Teng M, Wolf M, Ofsthun N, et al: Survival of patients undergoinghemodialysis with paricalcitol or calcitriol therapy. N Engl J Med349:446–456, 2003
52. Block GA, Hulbert-Shearon TE, Levin NW, Port FK: Associa-tion of serum phosphorus and calcium X phosphate product withmortality risk in chronic hemodialysis patients: A national study.Am J Kidney Dis 31:607–617, 1998
53. Marchais SJ, Metivier F, Guerin AP, London GM: Associationof hyperphosphatemia with haemodynamic disturbances in end-stage renal disease. Nephrol Dial Transplant 14:2178–2183, 1999
54. Guerin AP, London GM, Marchais SJ, Metivier F: Arterialstiffening and vascular calcifications in end-stage renal disease.Nephrol Dial Transplant 15:1014–1021, 2000
55. Blacher J, Guerin AP, Pannier B, et al: Arterial calcifications,arterial stiffness, and cardiovascular risk in end-stage renal disease.Hypertens 38:938–942, 2001
56. Goodman WG, Goldin J, Kuizon BD, et al: Coronary arterycalcification in young adults with end-stage renal disease who areundergoing dialysis. N Engl J Med 342:1478–1483, 2000