
Overview and update in developments for the treatment of depression

An Overview of
Depression By: Stephanie Grange, Michelle Taylor, Kylie Hintze
1

Table of Contents
Definition 3
Types of Depression 3
Diagnosis 7
Characteristics 8
Symptoms 9
Progression 9
Treatment 9
Tests and Medication 9
Equipment 10
Special Needs 11
TR implications 12
Models 13
Resources 14
Personal Examples 19
Works Cited Page 21
2

Definition: “A depressive disorder is not a passing blue mood but rather persistent feelings of sadness and worthlessness and a lack of desire to engage in formerly pleasurable activities.” “Depression (major depressive disorder or clinical depression) is a common but serious mood disorder. It causes severe symptoms that affect how you feel, think, and handle daily activities, such as sleeping, eating, or working.” -National Institute of Mental Health “Depression may be described as feeling sad, blue, unhappy, miserable, or down in the dumps. Most of us feel this way at one time or another for short periods. Clinical depression is a mood disorder in which feelings of sadness, loss, anger, or frustration interfere with everyday life for weeks or more.” -Medline Plus
Types:
1. Major Depression (Also known as Major Depressive Disorder, Chronic
Major Depression or Unipolar Depression) Major Depression is manifested by a combination of symptoms that interferes with the ability to work, study, sleep, eat and enjoy once pleasurable activities. A Major Depressive episode may occur only once; but more commonly, several episodes may occur in a lifetime. Chronic Major Depression may require a person to continue treatment and monitor lifestyle habits on an ongoing basis. This disorder is characterized by the presence of the majority of these symptoms:
Symptoms of Major Depression include:
● Persistent sad, anxious, or “empty” mood most of the day, nearly every day, as indicated by subjective report or observation of others (e.g., appears tearful). In children and adolescents, this may be characterized as an irritable mood.
● Feelings of hopelessness, pessimism ● Feelings of guilt, worthlessness, helplessness ● Loss of interest or pleasure in hobbies and activities that were once
enjoyed, including sex ● Decreased energy, fatigue, being “slowed down” ● Difficulty concentrating, remembering, making decisions ● Trouble sleeping, early-morning awakening, or oversleeping ● Appetite and/or weight changes ● Thoughts of death or suicide, or suicide attempts ● Restlessness, irritability, and/or angry outbursts
3

● Persistent physical symptoms, such as headaches, digestive disorders, and chronic pain, which do not respond to routine treatment
2. Dysthymia
Dysthymia is characterized by an overwhelming yet chronic state of depression, exhibited by a depressed mood for most of the days, for more days than not, for at least 2 years. (In children and adolescents, mood can be irritable and duration must be at least 1 year.) The person who suffers from this disorder must not have gone for more than 2 months without experiencing two or more of the following symptoms:
Symptoms of Dysthymia
● Appetite and/or weight changes ● Trouble sleeping, early-morning awakening, or oversleeping ● Decreased energy, fatigue ● Low self-esteem ● Poor concentration or difficulty making decisions ● Feelings of hopelessness
In addition, no Major Depressive Episode has been present during the first two years (or one year in children and adolescents) and there has never been a Manic Episode, a Mixed Episode, or a Hypomanic Episode, and criteria have never been met for Cyclothymic Disorder. Further, the symptoms cannot be due to the direct physiological effects of use or abuse of a substance such as alcohol, drugs or medication or general medical condition. The symptoms must also cause significant distress or impairment in social, occupational, educational, or other important areas of functioning.
3. Persistent Depressive Disorder Must last for two years, may have episodes of major depression along with
periods of less severe symptoms 4. Perinatal depression Much more serious than the “baby blues” that many women experience after
giving birth, full-blown major depression during pregnancy or after delivery (postpartum depression). The feelings of extreme sadness, anxiety, and exhaustion that accompany perinatal depression may make it difficult for these new mothers to complete daily care activities for themselves and/or for their babies.
5. Psychotic depression Occurs when a person has severe depression plus some form of psychosis, such
as having disturbing false fixed beliefs (delusions) or hearing or seeing upsetting things
4

that others cannot hear or see (hallucinations). The psychotic symptoms typically have a depressive “theme,” such as delusions of guilt, poverty, or illness.
6. Seasonal affective disorder Characterized by the onset of depression during the winter months. This
depression generally lifts during spring and summer. Winter depression, typically accompanied by social withdrawal, increased sleep, and weight gain, predictably returns every year in seasonal affective disorder.
7. Bipolar disorder
Another type of depressive illness is bipolar disorder (in the past described as manic-depressive illness). Bipolar disorder is characterized by cycling mood changes: severe highs (mania) and lows (depression), often with periods of normal mood in between. Sometimes the mood switches are dramatic and rapid, but usually they are gradual. When in the depressed cycle, an individual can have any or all of the symptoms of depression. When in the manic cycle, the individual may be overactive, over-talkative, and have a great deal of energy.
Bipolar disorder is characterized by more than one bipolar episode. There are four basic types of bipolar disorder.
1. Bipolar I Disorder
The primary symptom presentation is manic, or rapid (daily) cycling episodes of mania and depression that last at least seven days. Manic episodes may be so severe that the individual may require hospitalization. Depressive episodes typically last at least two weeks.
2. Bipolar II Disorder
The primary symptom presentation is recurrent depression accompanied by hypomanic episodes (a milder state of mania in which the symptoms are not severe enough to cause market impairment in social or occupational functioning or need for hospitalization, but are sufficient to be observable by others).
3. Bipolar Disorder Not Otherwise Specified
Symptoms of the disorder exist, but do not meet diagnostic criteria for either Bipolar I or II. However symptoms are well out of normal range for the individual.
4. Cyclothymic Disorder
A chronic state of cycling between hypomanic and depressive episodes that do not reach the diagnostic standard for bipolar disorder but have been present for at least two years.
Mania often affects thinking, judgment, and social behavior in ways that cause serious problems. For example, the individual in a manic phase may feel elated, full of grand
5

schemes that might range from unwise business decisions to romantic sprees and unsafe sex. Mania, left untreated, may worsen to a psychotic state. Manic episodes are characterized by:
A. A distinct period of abnormally and persistently elevated, expansive, or irritable mood, lasting at least one week (or any duration if hospitalization is necessary)).
B. During the period of mood disturbance, three or more of the following symptoms have persisted (4 if the mood is only irritable) and have been present to a significant degree:
Symptoms of Mania
● Abnormal or excessive elation ● Unusual irritability ● Decreased need for sleep (e.g., feels rested after only 3 hours of
sleep) ● Grandiose notions or increased self-esteem ● Increased talking or pressure to keep talking ● Flight of ideas or subjective experience that thoughts are racing ● Excessive involvement in pleasurable activities that have a high
potential for painful consequences (e.g., engaging in unrestrained purchasing sprees, sexual indiscretions, or foolish business investments).
● Markedly increased energy ● Poor judgment ● Inappropriate social behavior ● Distractibility (i.e., attention easily drawn to unimportant or irrelevant
external stimuli) 8. Substance Induced Mood Disorder (abuse or dependence)
Substance-Induced Mood Disorder is a common depressive illness of clients in substance abuse treatment. It is defined in DSM-V-TR as “a prominent and persistent disturbance of mood…that is judged to be due to the direct physiological effects of a substance (i.e., a drug of abuse, a medication, or somatic treatment for depression, or toxin exposure). The mood can manifest as manic (expansive, grandiose, irritable), depressed, or a mixture of mania and depression.
Generally, substance-induced mood disorders will only present either during intoxication from the substance or on withdrawal from the substance and therefore do not have as lengthy a course as other depressive illnesses. However, substance use disorders also frequently co-occur with other depressive disorders. Research has revealed that people with alcoholism are almost twice as likely as those without alcoholism to also suffer from major depression. In addition, more than half of people with bipolar disorder type I (with severe mania) have a co-occurring substance use disorder.
6
Men are more likely than women to report alcohol and drug abuse or dependence in their lifetime; however, there is debate among researchers as to whether substance use is a “symptom” of underlying depression, or a co-occurring condition that more commonly develops in men. Nevertheless, a substance use can mask depression, making it harder to recognize depression as a separate illness that needs treatment.
Diagnostic criteria:
DSM 5 Major Depressive Disorder A. Five (or more) of the following symptoms have been present during the same 2-week period and represent a change from previous functioning; at least one of the symptoms is either (1) depressed mood or (2) loss of interest or pleasure. Note: Do not include symptoms that are clearly attributable to another medical condition. 1. Depressed mood most of the day, nearly every day, as indicated by either subjective report (e.g., feels sad, empty, hopeless) or observation made by others (e.g., appears tearful). (Note: In children and adolescents, can be irritable mood.) 2. Markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day (as indicated by either subjective account or observation.) 3. Significant weight loss when not dieting or weight gain (e.g., a change of more than 5% of body weight in a month), or decrease or increase in appetite nearly every day. (Note: In children, consider failure to make expected weight gain.) 4. Insomnia or hypersomnia nearly every day. 5. Psychomotor agitation or retardation nearly every day (observable by others, not merely subjective feelings of restlessness or being slowed down). 6. Fatigue or loss of energy nearly every day. 7. Feelings of worthlessness or excessive or inappropriate guilt (which may be delusional) nearly every day (not merely self-reproach or guilt about being sick). 8. Diminished ability to think or concentrate, or indecisiveness, nearly every day (either by subjective account or as observed by others). 9. Recurrent thoughts of death (not just fear of dying), recurrent suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide. B. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
7
C. The episode is not attributable to the physiological effects of a substance or to another medical condition. Note: Criteria A-C represent a major depressive episode. Note: Responses to a significant loss (e.g., bereavement, financial ruin, losses from a natural disaster, a serious medical illness or disability) may include the feelings of intense sadness, rumination about the loss, insomnia, poor appetite, and weight loss noted in Criterion A, which may resemble a depressive episode. Although such symptoms may be understandable or considered appropriate to the loss, the presence of a major depressive episode in addition to the normal response to a significant loss should also be carefully considered. This decision inevitably requires the exercise of clinical judgment based on the individual’s history and the cultural norms for the expression of distress in the contest of loss. D. The occurrence of the major depressive episode is not better explained by schizoaffective disorder, schizophrenia, schizophreniform disorder, delusional disorder, or other specified and unspecified schizophrenia spectrum and other psychotic disorders. E. There has never been a manic episode or a hypomanic episode. Note: This exclusion does not apply if all of the manic-like or hypomanic-like episodes are substance induced or are attributable to the physiological effects of another medical condition. Characteristics Many factors may play a role in depression, including genetics, brain biology and chemistry, and life events such as trauma, loss of a loved one, a difficult relationship, an early childhood experience, or any stressful situation. Depression can happen at any age, but often begins in the teens or early 20s or 30s. Most chronic mood and anxiety disorders in adults begin as high levels of anxiety in children. In fact, high levels of anxiety as a child could mean a higher risk of depression as an adult. Depression can co-occur with other serious medical illnesses such as diabetes, cancer, heart disease, and Parkinson’s disease. Depression can make these conditions worse and vice versa. Sometimes medications taken for these illnesses may cause side effects that contribute to depression. A doctor experienced in treating these complicated illnesses can help work out the best treatment strategy.
8

Overall Symptoms Decreased energy or fatigue Moving or talking slowly Restless Difficulty concentrating remembering and making decisions Aches and pains, headaches, cramps, digestive problems without a clear cause Appetite and weight changes Pessimism Thoughts of death or suicide Difficulty sleeping Sad, anxious, empty feelings Hopelessness Loss of interest Loss of pleasure in hobbies and activities
Progression: Depressive symptoms typically develop over 2 or 3 weeks before the onset of a major depressive episode. Untreated depressive episodes can last from 6 to 18 months, but average is about 8 months. Treated episodes typically last from 6 weeks to 3 months. Depression often is a chronic disease that relents periodically; depressed people may experience 1 to 2 years of mental health, without symptoms, between episodes. Depression can occur in people of all ages. Typical age of onset for both men and women is 25-44 and least common for those 65 and older.
Treatment
Tests
- To know if you or someone else has depression, be familiar with the symptoms! If you have been experiencing many of them, it is possible you have depression.
- When you go to the doctor, they will ask you specific questions to assess whether or not you have depression.
- Doctors will also do physical assessments in order to rule out a physical cause for depression. They will try to identify major health concerns that may be contributing to symptoms of clinical depression. Blood tests are common to check for things such as anemia, thyroid, other hormone, calcium, and vitamin D levels.
- A depression diagnosis is often difficult to make because clinical depression can manifest in so many different ways. For example, some clinically depressed individuals seem to withdraw into a state of apathy.
9

Others may become irritable or even agitated. Eating and sleeping patterns can be exaggerated. Clinical depression may cause a person either to sleep or eat to excess or almost eliminate those activities.
- Observable or behavioral symptoms of clinical depression also may sometimes be minimal despite a person experiencing profound inner turmoil. Depression can be an all-encompassing disorder, and it affects a person's body, feelings, thoughts, and behaviors in varying ways.
Medications There are a plethora of medications for depression, and finding the right one or combination can be a process for every individual. Here are some examples of types of medications.
- Selective serotonin reuptake inhibitors (SSRIs) - These are the most commonly prescribed class of antidepressants. An imbalance of serotonin may play a role in depression. These drugs fight depression symptoms by decreasing serotonin reuptake in the brain. This effect leaves more serotonin available to work in your brain.
- Serotonin and norepinephrine reuptake inhibitors (SNRIs) - SNRIs help improve serotonin and norepinephrine levels in the brain. This may reduce depression symptoms.
- Tricyclic antidepressants (TCAs) - TCAs are often prescribed when SSRIs or other antidepressants don’t work. It isn’t fully understood how these drugs work to treat depression.
*Common side effects for depression medication include: drowsiness, weakness, lightheadedness, weight gain, blurry vision, and dry mouth. For a more specific list refer to the following website: http://www.healthline.com/health/depression/medication-list#Otherdrugs5
Equipment Light therapy boxes can offer an effective treatment for seasonal affective disorder (SAD). Features such as light intensity, safety, cost and style are important considerations. Therapy Seek professional help
- e.g. doctors, therapists, recreational therapists - don’t be afraid to ask for help medication
10

Mindfulness exercises - e.g. mandalas or deep breathing - anything that will help you clear your mind or focus your thoughts
Social support - Be genuine with your emotions and authentic to those who are close to
you - Don’t keep everything to yourself; open up to someone you trust
Exercise - Clinically proven that exercise can be as effective in treating mild to
moderate depression as antidepressants Nutrition
- Eating enough protein and having a good diet can go a long way Sleep
- Get adequate sleep at night and take naps when necessary Keeping a mood journal
- Can be cathartic and insightful
Special needs
- Strong support group: those who struggle with depression often feel alone, misunderstood or that they are a burden to others. The caring and loving support of friends, family, and professionals can help ease this distress.
- Patience: it can require a great deal of energy for those who struggle with depression to perform even the simplest tasks like getting out of bed. It is important to be understanding of the extra time they may take to do things or even give them space for a day.
- Support them in seeking professional help: although an invisible disorder, depression is real and often needs to be treated medically. With so much social stigma surrounding mental illness many who struggle with depression are hesitant to seek help. Do not perpetuate the stigma and never judge someone for seeking help.
- Validate: those who struggle with depression experience a different world than those without depression. It can be frustrating and cause people to feel alone if they are the only ones experiencing this reality. It is helpful to validate their feelings so they can know they are being heard and understood.
11

TR implications “Can you teach someone to be happy?”
Examples of specific skills that we can teach:
- Goal setting and achieving - Developing healthy relationships - “Play” and fun in a safe environment - Communicating appropriate and effectively - Functioning abilities
. . . It’s all about the process!
Ideas for TR interventions: - Sports: because exercise has proven mental health benefits especially through
its release of endorphins, therapeutic recreation activities that are active can be very effective.
- Passion: because those who struggle with depression often struggle to see a point to their lives, help them to find something they can live for.
- Service: find ways to help them feel needed. They could be a leader in a group or help plan things so they know they are important and contributing.
- Creative: any type of artistic activity can be a good outlet and way for people to express their emotions in a healthy way. This can include painting, writing, music, dance, etc.
- Empowering: people with depression often feel worthless and have no sense of their individual value. Activities where they can be stretched and see what they are capable of may help them develop confidence.
- Group and individual activities: people with depression definitely need a support group, but may also get overwhelmed and need space. It is important to consider in what situations group or individual activities may be best.
- Involve family: depression not only affects the person, but everyone around them, especially the family. No matter how informed and involved the family is, it takes a toll on the relationship. Find ways to include family members or other loved ones.
- Intrinsic motivation: those who struggle with depression often have a hard time being motivated to do day to day tasks. By finding something that will intrinsically motivate them can be hard, but it is important to work toward this so they can continue this activity even when they don’t have you to help them.
12
- Nature: mindfulness and meditation can be very helpful for people with depression. Finding activities that involve being out in nature can provide a peaceful setting to help them feel centered.
- New skills: those with depression may have missed out on opportunities to learn different skills because they were not in a mental state that allowed them to be on a soccer team or go skiing, etc. Helping them to understand what recreation opportunities are available can help them find their passion (leisure education)
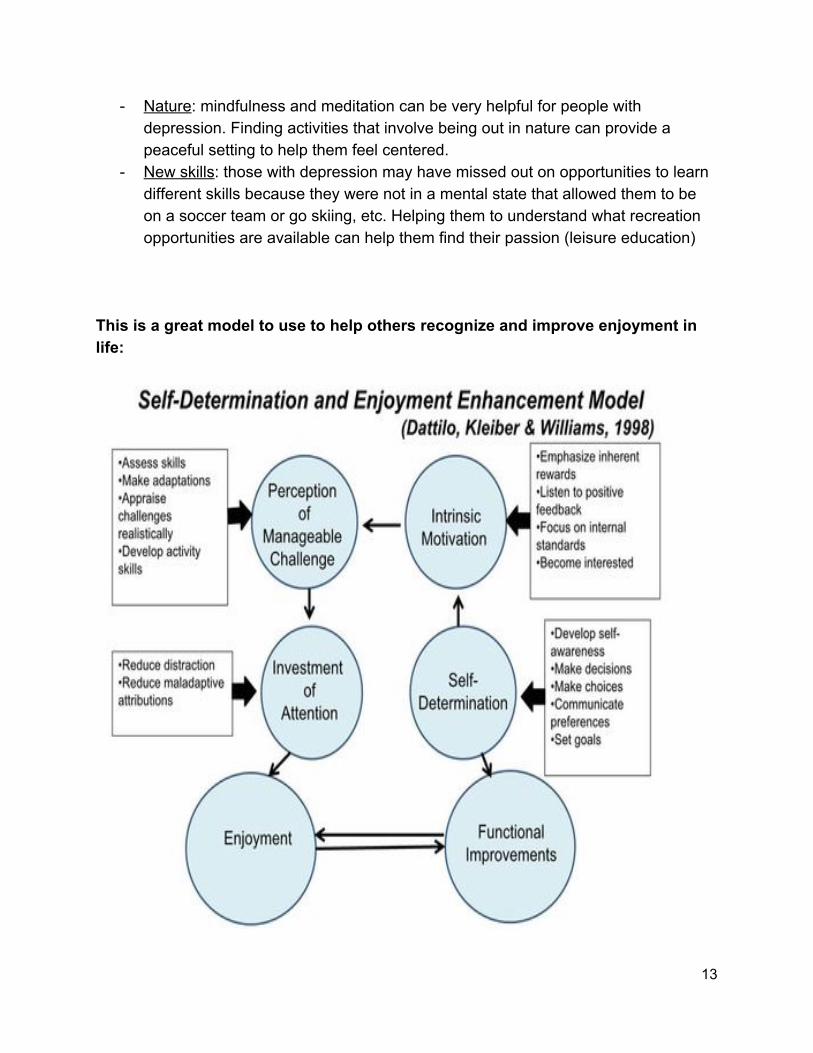
This is a great model to use to help others recognize and improve enjoyment in life:
13

Resources Local New Haven
Saratoga Springs Campus 228 W 400 N, Saratoga Springs, UT 84045
Spanish Fork Campus 2172 E 7200 S, Spanish Fork, UT 84660
Hobble Creek Campus 266 South Left Fork, Springville, UT 8463 Phone 801-794-1218
Crystal Vail Adolescent Services Program
Phone 385-262-5044 Depression and Bipolar Support Group Alliance: Utah County - Support Group
1034 N 500 W Provo, UT 84604 385-200-0613
BYU Counseling and Psychological Services
https://caps.byu.edu Psychology Today: Psychologists in Provo, UT
https://therapists.psychologytoday.com/rms/state/UT/Provo.html Utah County Crisis Line
801-691-LIFE www.crisislineuc.org
State Utah State Hospital
Ush.utah.gov 801-583-4171 1300 E Center Street
14

Provo, UT 84606 Just for Youth
justforyouth.utah.gove/health/mental-health/ Foundations Recovery Network: Utah Treatment Center
855-673-7174 www.rehabandtreatment.com/utah-treatment-center
Pathways Real Life Recovery Resources
pathwaysreallife.com/depression-treatment-utah/ 8706 S 700 E #205 Salt Lake City, UT 84111 Phone 801-895-3006
Turning Point Centers
1-888-576-HEAL turningpointcenters.com/dual-diagnosis/depression/
The Bridge: Health Recovery Center
thebridgerecoverycenter.com/depression-treatment-recover-center.html Located in St George, UT 877-885-9567
Salt Lake Behavioral Health www.saltlakebehavioralhealth.com/major-depressive-disorder 3802 S 700 E Salt Lake City, UT 84106 Phone 877-264-6000
Outback Therapeutic Expeditions
50 N 200 E Lehi, UT 84043 800-817-1899
Wasatch Mental Health
750 N 200 W Provo, UT 801-373-4760
15

National National Alliance on Mental Illness:
1-800-950-NAMI (1-800-950-6264) https://www.nami.org
Anxiety and Depression Association of America:
1-240-485-1001 http://www.adaa.org
National Institute of Mental Health:
1-866-615-6464 http://www.nimh.nih.gov
Centers for Disease Control and Prevention: Division of Mental Health
1-800-CDC-INFO (1-800-232-4636) http://www.cdc.gov/mentalhealth
American Psychological Association:
1-800-374-2721, http://www.apa.org
American Psychiatric Association:
1-703-907-7300 http://www.psychiatry.org
American Foundation for Suicide Prevention:
1-800-273-TALK (1-800-273-8255), https://afsp.org
Depression and Bipolar Support Alliance: 1-800-826-3632, http://www.dbsalliance.org
Families for Depression Awareness:
1-781-890-0220, http://familyaware.org
16
To Write Love On Her Arms: 1-800-273-TALK (1-800-273-8255), https://twloha.com
Global World Health Organization
www.who.int/mental_health/en/ International Society for Mental Health Online
Ismho.org World Federation for Mental Health
Wfmh.com World Mental Health Survey Initiative
www.hcp.med.harvard.edu/wmh/ Basic Needs
www.basicneeds.org Manas
manas.org.in
Patient Blogs
Lawyers With Depression: http://www.lawyerswithdepression.com
Daisies and Bruises:
http://daisiesandbruises.com
Time to Change: http://www.time-to-change.org.uk/category/blog/depression
Postpartum Progress:
http://www.postpartumprogress.com
17

Depression Marathon: http://depressionmarathon.blogspot.com
Transcript of “I Had a Black Dog His Name Was Depression”: I had a black dog. His name was depression. Whenever the black dog made an appearance, I felt empty and life seemed to slow down.
He could surprise me with a visit for no reason or occasion. The black dog made me look and feel older than my years. When the rest of the world seemed to be enjoying life, I could only see it through the black dog. Activities that usually brought me pleasure, suddenly ceased to. He liked to ruin my appetite. He chewed up my memory and ability to concentrate. Doing anything or going anywhere with the back dog required super human strength. At social occasions, he would sniff out any confidence I had and chase it away.
My biggest fear was being found out. I worried that people would judge me. Because of the shame and stigma of the black dog. I was constantly worried that I would be found out. So I invested vast amounts of energy into covering him up. Keeping up an emotional lie is exhausting.
Black dog could make me think and say negative things. He could make me irritable and difficult to be around. He would take my love and bury my intimacy. He loved nothing more than to wake me with highly repetitive and negative thinking. He also liked to remind me how exhausted I was going to be the next day. Having a black dog in your life isn’t so much about feeling a bit down, sad or blue…at it’s worst it’s about being devoid of feeling altogether.
As I got older the black dog got bigger and he started hanging around all the time. I’d chase him off with whatever I thought may send him running. But more often than not he’d come out on top. Going down became easier than getting up again. So I became rather good at self medication…which never really helped. Eventually I felt totally isolated from everything and everyone. The black dog had finally succeeded in hijacking my life. When you lose all joy in life, you can begin to question what the point of it is.
Thankfully this was the time that I sought professional help. This was my first step towards recovery and a major turning in my life. I learned that it doesn’t matter who you are, the black dog affects millions and millions of people. It is an equal opportunity mongrel. I also learned that there was no silver bullet or magic pill. Medication can help some and others might need a different approach altogether.
18

I also learned that being emotionally genuine and authentic to those who are close to you, can be an absolute game changer. Most importantly, I learn not to be afraid of the black dog and I taught him a few tricks of my own. The more tired and stressed you are the louder he barks, so it’s important to learn how to quiet your mind.
It’s been clinically proven that regular exercise can be as effective for treating mild to moderate depression as antidepressants. So go for a walk or a run and leave the mutt behind. Keep a mood journal, getting your thoughts on paper can be cathartic and often insightful. Also keep track of the things that you have to be grateful for. The most important thing to remember is that no matter how bad it gets… if you take the right steps, talk to the right people, black dog days can and will pass.
I wouldn’t say that I’m grateful for the black dog but he has been an incredible teacher. He forced me to re-evaluate and simplify my life. I learned that rather than running away from my problems it’s better to embrace them. The black dog may always be part of my life but he will never be the beast that he was. We have an understanding. I learned that through knowledge, patience, discipline and humor the worst black dog can be made to heal. If you are in difficulty, never be afraid to ask for help. There is absolutely no shame in doing so. The only shame is missing out on life. Depression. Get Help. Be Helped.
http://www.nobledeedsandhotbaths.com/2014/02/04/i-had-a-black-dog-name-depression-transcript/
Interview responses of two teenage girls who have been diagnosed with depression and gone through treatment for it: Teenager 1 1. What is your definition of depression? Feeling somewhat sad almost always or extremely sad more often than normal (definition is based on my experience) 2. What does it feel like to be depressed? (be as descriptive as possible) I think the feeling of being depressed and the symptoms of depression are different for everyone. For me, feeling depressed consisted of lack of motivation for almost all activities, consistent glum feeling, feeling worthless or not good enough, no confidence, and because of that anxiety about simple things such as ordering food, social interactions and homework and then being sad about being anxious about such simple things Ok so imagine you have a choice between equations. With the first equation, you're already there it's so easy, you have the answer you know what you need to do. With the second equation, I know exactly what I need to do to get there but it's so much work to get to the answer. I would assume most people would choose the first equation for those reasons.
19

3. What are some of the symptoms? I think the "symptoms" of depression are mostly ways of dealing with the depression. For me, the really big things were significantly pulling back socially, self-harm, and disordered eating patterns. The self-harm and social stuff were like tied for number one. I also was just really spaced out and hard to engage with most anything. 4. What has most helped you in dealing with depression or learning to overcome it? Ok so disclaimer: the following statement is not something I believe works for everyone or a solution that I believe that everyone should peruse. Medication has actually really helped me a lot. It was a painful process finding the right stuff and trying different combinations but once we got to what worked it made a really big change for the positive. That said, sometimes you just have a sad day and in those cases I either eat some protein because when I don't have protein I'm like so emotional like seriously it's crazy, or I take a nap because sometimes you just need a break from reality or just do whatever it takes to get to the end of the day because I often feel a lot better in the morning. What other resources are available for people with depression? A lot of other people (and this is all to my understanding I don't wanna speak for others) gain a lot from mindfulness activities such as coloring mandalas or deep breathing. 5. Are there any therapeutic activities or interventions you liked that specifically addressed depression? I suppose like just accepting that the depression is there and not doing anything to try to change it 6. Is there anything else you would like for people to understand about depression or people who experience it? I will always have depression but I will not always be depressed. Teenager 2: 1. What is your definition of depression? For me? The strong desire to lay in bed all day and then kill myself. 2. What does it feel like to be depressed? (be as descriptive as possible) I feel almost dead. 3. What has most helped you in dealing with depression? NOTHING. 4. Are there any recreational therapy activities or interventions you liked that specifically addressed depression? Nope. We literally never had any depression tasks. I was typically unhappy with what the RT department decided to focus on. 5. Is there anything else you would like for people to understand about depression or people who experience it? Um, it's not a joke. It's not a FEELING, it's a diagnosis. Affirmations don't help. It's hard to get through.
20

Works Cited:
https://www.nimh.nih.gov/health/topics/depression/index.shtml http://www.webmd.com/depression/ Anxiety and Depression Association of America http://images.pearsonclinical.com/images/assets/basc-3/basc3resources/DSM5_DiagnosticCriteria_MajorDepressiveDisorder.pdf
21


















