An Introduction to Minimally Invasive Surgery II Advanced Laparoscopy and...
54
An Introduction to Minimally Invasive Surgery II Advanced Laparoscopy and Thoracoscopy Philipp Mayhew BVM&S, MRCVS, DACVS Assistant Professor, Small animal surgery University of California-Davis Taiwan College of veterinary surgeons - Taiwan 2011
Transcript of An Introduction to Minimally Invasive Surgery II Advanced Laparoscopy and...

An Introduction to Minimally Invasive Surgery IIAdvanced Laparoscopy and Thoracoscopy
Philipp Mayhew BVM&S, MRCVS, DACVSAssistant Professor, Small animal surgery
University of California-Davis
Taiwan College of veterinary surgeons - Taiwan 2011

Laparoscopic cholecystectomy Main indication: Uncomplicated gall bladdermucocelesCase selection criteria:
-NO evidence of extra-hepatic biliary tractobstruction-NO evidence of bile peritonitis-Good candidates for anesthesia andpneumoperitoneum -Dogs over ~4kg
•
•

Illustration courtesy of Kip Carter! UGA
Patient positioningand port placementfor LC
Dorsal recumbency
Slighttrendelenburg
4 port technique
10mm port onmidline
One 5mm port forretractor on farleft side at mid-abdominal level
•
•
•
•
•

Ligatingthe cysticduct
Illustration courtesy of Kip Carter! UGA

Dissection around the cystic duct


Lap chole - GB removal

Laparoscopicadrenalectomy
Laparoscopic adrenalectomy (LA) isstandard of care in humans
Provides advantage of a lateral approachwithout the painful paramedian incision
Case selection is critical for success
Perioperative management is key to success just as it is with “open” adrenal surgery
•
•
•
•

Case selection forlaparoscopic adrenalectomy
Must rule out vascular invasion bydiagnostic imaging:
-Ultrasound: sensitivity 80%, specificity 90%(Kyles et al. 2003)
-Computed tomography (CT): Sensitivity 92%specificity 100% (Schulz et al. 2009)
If vascular invasion present do “open”approachTumor size:
-If diameter >3-4cm probably not suitable forLC
•
•
•

Case selection for LA Imaging: Ultrasound
Poor case for LA: Tumor with vascular invasion
into the caudal vena cava

Case selection for LAImaging: Computed Tomography
Non-invasive Left-sided Pheochromocytoma
Moving cranial to caudal

Case selection for LAComputed Tomography
Left-sided tumor invading phrenicoabdominal veinand vena cava

Surgicalapproach for LA
Right approach
Left approach
Patient positioned inlateral or near lateralrecumbency with theaffected side up
3-4 port technique in triangulating pattern around adrenal
•
•

Left sided LADissect into retroperitoneum over gland.
Dissect out as much as possible of thesurrounding fat.
Identify phrenicoabdominal vein (PV) andligate/clip
Take care to observe
renal vein
Once PV is dissected off
then dissect dorsally
•
•
•
•
•

Left sided adrenalectomy

Laparoscopicureteronephrectomy
Case selection – key to successSuggested indications:
- small circumscribed neoplasms - idiopathic renal hematuria - renal dysplasia - mild hydronephrosis ± infection
Suggested contraindications: - large neoplasms - active pyelonephritis with extensionbeyond capsule
If in doubt use advanced imaging (CT orMRI)
••
•
•

Surgical technique
Early dissection of theureter is helpful
Be careful to accuratelyidentify the ureter and notconfuse this with otherstructures
Ureter can then be graspedand used as a handle forelevation of the kidneyduring artery and veindissection
•
•
•

Lap UreteronephrectomyRetroperitoneal dissection
The technique begins with dissection of theretroperitoneal attachments of the kidneyusing a vessel-sealer
•

Artery and vein dissectionMust dissect out all of the soft tissue around
the renal artery and veinTake care to dissect adrenal gland off the
kidneyUse right angle dissector to get around the
vesselsFor ligation of artery and vein:
-small dogs and cats: vessel-sealer, hemoclips-Larger dogs: Hemoclips, EndoGIA
•
•
•
•

Lap ureteronephrectomyDissecting renal artery and vein

ThoracoscopyHuman literature:
- Less pain, thoracic drainage, hospital stay,sepsis, pneumonia, death
Thoracoscopic procedures described: -Pericardial window -Subphrenic pericardectomy -Cranial mediastinal mass -PDA ligation -Thoracic duct ligation -Vascular ring ligation -Lung biopsy -lung Lobe resection
•
•

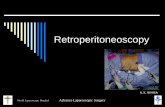
Thoracoscopyinstrumentation
Endoscopic tower
Insufflator not required formost cases
30 degree telescope is best
Thoracic cannulae don’t needone-way valves
•
•
•
•

Thoracoscopyinstrumentation
Suction/irrigation
EndoGIA stapling device
specimenretrieval bags

Anesthesia for thoracoscopyWorking space is provided by apneumothorax after entry of first cannulaThoracoscopy under pneumothorax:
- Ventilate for patient- Monitor oxygenation by pulse oximetry andblood gas analysis- Monitor ventilation by capnography and/orblood gas analysis
To increase working space:
1) insufflate with C02 (generally not welltolerated) 2) One-lung ventilation
•
•
•

Anesthesia for thoracoscopyOne-lung ventilation
! Respiratory rate by ~20%
" Tidal volume by one half
PEEP (2-5cm H20)
Close monitoring
Complications:
-balloon overinflation
-hypoventilation
-V/Q mismatch
-! PaC02
•
•
•
•
•
BronchialBlocker
Selectiveintubation
Double-lumenendobronchial
intubation

OLV: EndobronchialBlocker
Balloon-tipped catheter placedinto right or left mainstembronchusBronchoscopic guidance required
In some cases balloon not bigenough or can move
•
•

OLV: Double-LumenEndobronchial tubes
Tube has two lumens; oneterminates in bronchus andone in trachea
Left and right sided tubes- Can use left sided tubesonlyCan place blind orbronchoscopically guided
•
•
•
RL

Alternating one-lungventilation

Patientpositioning
Lateral recumbency:
-Thoracic duct ligation
-Lung biopsy and lobectomy
-PDA and vascular anomaly
Dorsal recumbency:
-Pericardial window andsubphrenic pericardectomy
-Cranial mediastinal mass
-Lung biopsy and lobectomy
Sternal recumbency
-Thoracic duct ligation
•
•
•

Thoracic access: Port placement
Always use blunt cannulaeDorsal recumbency: Camera portalat subxiphoid locationLateral recumbency: Camera portalintercostally
2-3 instrument portals intercostally
•
•
•
•

Thoracoscopic pericardectomytechniques
Idiopathic or neoplasia-associated pericardial effusion:
-Pericardial window- smallopening in pericardium to drainexcess fluid- 3x3 cm or 4x4cm
Constrictive pericarditis andIdiopathic chylothorax:
-Subphrenic pericardectomy -removal of the pericardiumventral to the level of phrenicn.
•

Patientpositioning andPort placement
Pericardial window:Lateral or dorsalrecumbencySubphrenic
pericardectomy: Dorsalrecumbency
-Subxiphoid camera portal-Instrument ports at 4-6thintercostal spaces locatedvery ventral
•
•

Pericardial resectionCan be done with Scissors sharply but willcause greater hemorrhageUse vessel-sealing device if possibleAlways elevate the pericardium away fromheart before activating vessel-sealer toavoid thermal/electrical injury tomyocardium/coronary vessels
•
•
•

Surgical technique:Pericardial window
Grasp the pericardium over heart apexIncise with vessel-sealing deviceRemove a 4x4cm window of pericardiumPlace in specimen retrieval bag
•
•
•
•

Specimen RetrievalIf specimen is small can be retrievedthrough a large thoracic cannula
If large sample then place in specimenretrieval bag
Port site metastasis has been describedafter pericardium affected withmesothelioma was pulled through anunprotected port incision (Brisson et al. Portal site metastasisof invasive mesothelioma after diagnostic thoracoscopy in a dog JAVMA 2006;229:980-983)
•
•
•

Lung Lobectomy in smallanimals
Indications:-Primary lung neoplasms-Metastatic neoplasia if single or confined to onelobe-Chronic consolidation-Pulmonary abscessation-Lung lobe torsion-Pulmonary bullae/blebs
•

TLL: Evidence from humanliterature
TLL is associated with a 4.6-6.7%conversion rate in humansComplication rates (34-39%) and
mortality (1.4-1.6%) are similarTLL is associated with decreased:
-hospital stay-chest tube times-prolonged air leak-renal failure-Sepsis-pneumonia
•
•
•
Villamizar NR et al. Thoracoscopic lobectomy is associated with lower morbidity compared withthoracotomy. J Thorac Cardiovasc Surg 2009;138:418-425

Thoracoscopic lunglobectomy (TLL): CaseSelection
Patient size:Dogs over 20kg best candidatesSmall dogs and cats: difficult due to stapler sizeand OLV
Disease process:-Primary and metastatic neoplastic lesions-Well-circumscribed pulmonaryabscess/consolidated lobes-Pulmonary bullae/blebs
Lesion Characteristics:-Lesion Size: <8-9cm diameter (dogs over 25kg)-Location: lesions away from the pulmonary hilus
•
•
•

TLL: Good case selection
Large mass but well away from Hilus
Large dog...37kg Labrador
•
•

TLL: Poor case selection
Very large massclose to hilus
Small dog...7kgterrier
•

TLL-Patient positioning andport placement
Patient positioning
Single lesions in known lobe: -Lateral recumbency with affected lobe up
Multiple lesions in differenthemithoraces or unknown lesion location:
-Dorsal recumbencyPort Placement
Lateral -Camera portal at level of lung hilus -Instrument portals: triangulate around hilus
Dorsal recumbency: will depend onlesion location
•
•
•
•
•
•

Caudal Lobes: Incision throughpulmonary ligament

TLL: Stapling across theHilus
Use EndoGIA 60mm cartridge with 3.5mmstaples in all medium to large dogs
Will often need a second staple cartridgeto complete the resection
•
•

Lung LobeRetrieval
Always retrieve neoplasticsamples through protectedport incision
•

Idiopathic chylothoraxaccumulation of chyle within the pleural
cavity results in respiratory distress,pleural fibrosis, hypoproteinemiaTreatment options:
-Thoracic duct ligation (TDL)-Pericardectomy (PC)-Cisterna chyli ablation (CCA)-Omentalization-thoracic duct embolization-rutin therapy-drainage techniques (denver shunt, svapplacement)
•
•

Thoracoscopictreatment of idiopathicchylothoraxTDL ONLY -Dogs and cats: ~50% resolution
Open TDL+PC- 10/10 dogs and 8/10 cats resolved(Fossum TW et al. JVIM 2004)
Minimally invasive tdl+PC - 7/8 dogs resolved (Allman et al. Vet Surg2009)
-6/6 Dogs resolved (Mayhew et al. In press)
•
•
•

Technique - TDL 3 ports established at 7-9th ICS in trianguating
pattern around caudal mediastinum~5cm paracostal “port” on right side Lymphangiograms pre and post-operatively can
be usedmethylene blue injected into mesenteric LNTDL performed by clip
application after dissection
•
••
••

TD visualizationExteriorize the lymph nodes around the ileo-cecocolic junctionInject diluted methylene blue
lymph node injections highly effective forhighlighting thoracic duct (Enwiller et al. Vet Surg 2003)
•
•
•

TDL ligation

Most cranial mediastinal masses too large attime of diagnosis for MIShowever if modestly sized may be resectableadvanced imaging very important pre-operatively
•
•
•
Cranial mediastinal massresection


Complications afterthoracoscopic lung surgery
Hemorrhage:
-From pulmonary hilus: Grasp bleeding vessel,clip, re-staple or endoloop
-From Intercostal artery/vein: suture aroundrib
Air leak
-From hilus: use clips or re-staple
-From iatrogenic damage to other lobes
•
•

ConclusionsMany new and exciting developments in the
rapidly growing area of minimally invasivesurgery
Requires a team approach
Case selection, training and the rightequipment are the keys to success
•
•
•

Any Questions?
Yosemite National