
An Integrated Clinic-Community Partnership for Child ...
12
ARTICLE An Integrated Clinic-Community Partnership for Child Obesity Treatment: A Randomized Pilot Trial Jessica Hoffman, BS, a Leah Frerichs, PhD, b Mary Story, PhD, RD, c Jason Jones, CPRP, CPO, d Kiah Gaskin, MSW, MPH, e Annie Apple, BS, e Asheley Skinner, PhD, f Sarah Armstrong, MD e BACKGROUND AND OBJECTIVES: Effective treatment of childhood obesity remains elusive. Integration of clinical and community systems may achieve effective and sustainable treatment. However, the feasibility and effectiveness of this integrated model are unknown. METHODS: We conducted a randomized clinical trial among children aged 5 to 11 presenting for obesity treatment. We randomized participants to clinical care or clinical care plus community-based programming at a local parks and recreation facility. Primary outcomes were the change in child BMI at 6 months and the intensity of the program in treatment hours. Secondary outcomes included health behaviors, fitness, attrition, and quality of life. RESULTS: We enrolled 97 children with obesity, and retention at 6 months was 70%. Participants had a mean age of 9.1 years and a mean baseline BMI z score of 2.28, and 70% were living in poverty. Intervention participants achieved more treatment hours than controls (11.4 vs 4.4, SD: 15.3 and 1.6, respectively). We did not observe differences in child BMI z score or percent of the 95th percentile at 6 months. Intervention participants had significantly greater improvements in physical activity (P = .010) and quality of life (P = .008). CONCLUSIONS: An integrated clinic-community model of child obesity treatment is feasible to deliver in a low-income and racially diverse population. As compared with multidisciplinary treatment, the integrated model provides more treatment hours, improves physical activity, and increases quality of life. Parks and recreation departments hold significant promise as a partner agency to deliver child obesity treatment. abstract a School of Medicine, c Global Health Institute, e Department of Pediatrics, and f Clinical Research Institute, Duke University, Durham, North Carolina; b Center for Health Equity Research, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina; and d Durham Parks and Recreation, Durham, North Carolina; Ms Hoffman was involved in the project design, designed the database and managed data collection, recruited participants, conducted baseline and follow-up assessments of participants, and drafted the initial manuscript; Dr Frerichs conceptualized and designed the study, designed the data collection instruments, conducted feasibility subanalyses, conducted initial analyses, and reviewed and revised the manuscript; Dr Story was involved in the project design, served as a mentor throughout the study, and reviewed and revised the manuscript; Mr Jones was involved in the project design and reviewed and revised the manuscript; Ms Gaskin and Ms Apple were involved in the project design, supervised the intervention delivered at the community site, and reviewed and revised the manuscript; Dr Skinner was involved in the project design, conducted all initial and final analyses, and reviewed and revised the manuscript; Dr Armstrong conceptualized and designed the study, coordinated and supervised data collection at the clinical site, and critically reviewed and revised the manuscript; and all authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work. This trial has been registered at www.clinicaltrials.gov (identifier NCT02573142). PEDIATRICS Volume 141, number 1, January 2018:e20171444 WHAT’S KNOWN ON THIS SUBJECT: Childhood obesity treatment guidelines are challenging to deliver in real-world settings. Integrated clinic- community partnerships may increase the intensity of treatment, yet little is known about the feasibility and effectiveness of these integrated models. WHAT THIS STUDY ADDS: When compared with clinical obesity treatment alone, an integrated clinic-community model, delivered at a parks and recreation facility, is engaging among a low-income, racially diverse population and is associated with improvements in physical activity and quality of life. To cite: Hoffman J, Frerichs L, Story M, et al. An Integrated Clinic-Community Partnership for Child Obesity Treatment: A Randomized Pilot Trial. Pediatrics. 2018;141(1):e20171444 by guest on November 5, 2021 www.aappublications.org/news Downloaded from
Transcript of An Integrated Clinic-Community Partnership for Child ...
Article
An Integrated Clinic-Community Partnership for Child Obesity Treatment: A Randomized Pilot TrialJessica Hoffman, BS, a Leah Frerichs, PhD, b Mary Story, PhD, RD, c Jason Jones, CPRP, CPO, d Kiah Gaskin, MSW, MPH, e Annie Apple, BS, e Asheley Skinner, PhD, f Sarah Armstrong, MDe
BACKGROUND AND OBJECTIVES: Effective treatment of childhood obesity remains elusive. Integration of clinical and community systems may achieve effective and sustainable treatment. However, the feasibility and effectiveness of this integrated model are unknown.METHODS: We conducted a randomized clinical trial among children aged 5 to 11 presenting for obesity treatment. We randomized participants to clinical care or clinical care plus community-based programming at a local parks and recreation facility. Primary outcomes were the change in child BMI at 6 months and the intensity of the program in treatment hours. Secondary outcomes included health behaviors, fitness, attrition, and quality of life.RESULTS: We enrolled 97 children with obesity, and retention at 6 months was 70%. Participants had a mean age of 9.1 years and a mean baseline BMI z score of 2.28, and 70% were living in poverty. Intervention participants achieved more treatment hours than controls (11.4 vs 4.4, SD: 15.3 and 1.6, respectively). We did not observe differences in child BMI z score or percent of the 95th percentile at 6 months. Intervention participants had significantly greater improvements in physical activity (P = .010) and quality of life (P = .008).CONCLUSIONS: An integrated clinic-community model of child obesity treatment is feasible to deliver in a low-income and racially diverse population. As compared with multidisciplinary treatment, the integrated model provides more treatment hours, improves physical activity, and increases quality of life. Parks and recreation departments hold significant promise as a partner agency to deliver child obesity treatment.
abstract
aSchool of Medicine, cGlobal Health Institute, eDepartment of Pediatrics, and fClinical Research Institute, Duke University, Durham, North Carolina; bCenter for Health Equity Research, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina; and dDurham Parks and Recreation, Durham, North Carolina;
Ms Hoffman was involved in the project design, designed the database and managed data collection, recruited participants, conducted baseline and follow-up assessments of participants, and drafted the initial manuscript; Dr Frerichs conceptualized and designed the study, designed the data collection instruments, conducted feasibility subanalyses, conducted initial analyses, and reviewed and revised the manuscript; Dr Story was involved in the project design, served as a mentor throughout the study, and reviewed and revised the manuscript; Mr Jones was involved in the project design and reviewed and revised the manuscript; Ms Gaskin and Ms Apple were involved in the project design, supervised the intervention delivered at the community site, and reviewed and revised the manuscript; Dr Skinner was involved in the project design, conducted all initial and final analyses, and reviewed and revised the manuscript; Dr Armstrong conceptualized and designed the study, coordinated and supervised data collection at the clinical site, and critically reviewed and revised the manuscript; and all authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
This trial has been registered at www. clinicaltrials. gov (identifier NCT02573142).
PEDIATRICS Volume 141, number 1, January 2018:e20171444
What’s KnoWn on this subject: Childhood obesity treatment guidelines are challenging to deliver in real-world settings. Integrated clinic-community partnerships may increase the intensity of treatment, yet little is known about the feasibility and effectiveness of these integrated models.
What this study adds: When compared with clinical obesity treatment alone, an integrated clinic-community model, delivered at a parks and recreation facility, is engaging among a low-income, racially diverse population and is associated with improvements in physical activity and quality of life.
to cite: Hoffman J, Frerichs L, Story M, et al. An Integrated Clinic-Community Partnership for Child Obesity Treatment: A Randomized Pilot Trial. Pediatrics. 2018;141(1):e20171444
by guest on November 5, 2021www.aappublications.org/newsDownloaded from
Childhood obesity is an ongoing health concern1, 2 involving cardiometabolic risk, 3, 4 reduced quality of life, 5 and long-term health consequences.6, 7 In current clinical guidelines, intensive behavioral treatment of children with obesity is recommented.8 The US Preventive Services Task Force (USPSTF) has found a threshold effect to treatment at their recommendation of ≥26 hours of exposure to the intervention.9 Nevertheless, achieving this threshold in clinical settings has been challenged by lack of capacity, 10 poor payment for services, 11 and high rates of attrition, particularly among low-income and racially diverse groups.12 – 14 Effective, accessible, and scalable treatment options are needed.
Integration of clinical and community systems may achieve more effective and sustainable treatment than either system alone.7, 15, 16 The members of the clinical system perform health screenings and medical treatment; the members of the community system provide recreational facilities and staff to deliver fitness programs, cooking classes, and group activities. This integrated model offers several advantages: clinic staff can provide individualized counseling and treatment to address the complications of obesity, and recreation centers are local, accessible, have extended hours, and have staff to provide social support to improve engagement of families.14, 17
Our team has developed an integrated clinic-community treatment model as a partnership between an academic medical center and a municipal parks and recreation agency. The goals of the current study are (1) to describe the implementation of an integrated clinic-community partnership for child obesity treatment and (2) to evaluate the effectiveness of integrated treatment on child BMI and health outcomes. We hypothesize that the integrated model is more
effective in improving BMI and child health behaviors, as compared with clinical treatment alone.
Methods
study design
We used a prospective, 2-group, nonblinded, randomized controlled trial design to compare the integrated clinic-community model with clinic-only treatment. The intervention was 6 months in duration. The clinical treatment in both groups was tertiary-care pediatric weight management, which is currently the most effective standard of care for clinical obesity treatment.9 The Duke Healthy Lifestyles clinic, a pediatric weight management program, served as the recruitment site. Participant enrollment occurred between October 29, 2015 and August 15, 2016, and we collected 6-month follow-up data at the end of the intervention, through March 13, 2017. The institutional review boards from Duke University (Pro00066366) and the University of North Carolina at Chapel Hill (15-1867) approved the study protocol.
study Participants
Participants included a consecutive sample of patients aged 5 to 11 with a BMI ≥95th percentile, referred by their primary care provider to the Healthy Lifestyles clinic, along with each child’s adult primary caregiver (“parent”) aged 18 or older. We excluded children with a medical cause for obesity (hypothyroidism, Cushing’s syndrome, etc), those who lived more than 30 miles from the clinic or planned to move out of the area, and those whose parents could not speak or read English or Spanish. We compensated each parent-child dyad for completing study measurements with gift cards of $10 at baseline, $20 at 3 months, and $30 at 6 months, regardless of participation in programming.
treatment arms
Usual Care (Healthy Lifestyles Clinic)
The Healthy Lifestyles weight management protocol and outcomes have been described previously.18, 19 Briefly, patients with obesity and their families meet monthly with a multidisciplinary team (medical, nutrition, physical therapy, and mental health) to set and monitor lifestyle behavioral goals and manage health conditions. Program details can be found in Supplemental Table 4.
Intervention (Integrated Clinic-Community Model)
The integrated clinic-community model is a partnership between the Healthy Lifestyles pediatric weight management clinic and a recreation center operated by Durham Parks and Recreation. The program, Bull City Fit, has been operational since 2012 and primarily serves racially diverse and low-income families. A shared use agreement outlines the terms of the partnership. Legal representatives from both Duke University and the Durham Parks and Recreation Department review and amend this agreement annually to ensure clear delineation of roles and responsibilities. Bull City Fit is open 6 days per week, from 6 pm to 8 pm on weekdays and 1 pm to 3 pm on weekends (Supplemental Table 4). All members of the immediate household may participate. Activities include structured games and team-building sports (6 days/week), cooking classes (1 day/week), swimming lessons (2 days/week), and peer support (1 day/week). Trained staff supervise and facilitate all activities.
From the beginning of the study, a research assistant texted intervention parents’ mobile devices with daily information about Bull City Fit activities. Starting in May 2016, because of low engagement in Bull City Fit, a research assistant also sent personalized text messages to
HOFFMAN et al2 by guest on November 5, 2021www.aappublications.org/newsDownloaded from

parents to encourage more frequent attendance (Supplemental Table 4).
Procedures
We assigned participants to usual care or intervention with a 1:1 allocation ratio by using a computer-generated randomization (Excel, 2010; Microsoft, Redmond, WA), which we concealed in sequentially numbered envelopes and opened at enrollment. One research assistant generated the allocation sequence, and a different research assistant enrolled participants. We did not blind participants to group assignment. Intervention participants received standard clinical care at Healthy Lifestyles in addition to receiving free, unlimited access to Bull City Fit community-based programming. Control participants received standard clinical care at Healthy Lifestyles, in addition to receiving promotional materials about the local parks and recreation department. We invited control participants to participate in the intervention at the end of the study.
We collected data during routine clinic visits at baseline, 3 months, and 6 months, and we recorded all data in a REDCap database.20 Trained research staff collected all measures, either by administering survey-based instruments or by abstracting data from the medical record. Because of slow enrollment, all measures were translated into Spanish via an American Translators Association–certified translation service that used a process of 2 forward translations by different bilingual and bicultural translators, with discussions to reconcile differences and final approval by the company owner (Bilingual Communications, Inc, Cary, NC). We first enrolled monolingual Spanish-speaking participants in April 2016 (Pacific Interpreters; LanguageLine Solutions Company, Monterey, CA).
Measures
Treatment Intensity
Our primary outcome of treatment intensity was the total number of treatment hours over 6 months, which we calculated on the basis of Bull City Fit attendance and Healthy Lifestyles visits for the intervention and control groups. The details of possible clinical and Bull City Fit hours can be found in Supplemental Table 4. We measured attendance frequency and duration through administrative data in the medical chart and through sign-in software used on-site at Bull City Fit (Volgistics; Red Ridge Software Company, Byron Center, MI). On the basis of treatment hours, we assessed the percentage of participants meeting USPSTF’s recommended intensity for childhood obesity treatment (≥26 hours over 6 months). We measured satisfaction and perceptions of Bull City Fit by using a parent survey completed at 6 months.
Weight, Health, Behavioral, and Psychosocial Outcomes
Our primary health outcome was child BMI. A nurse measured child and parent height by using a stadiometer (Health o meter Professional CE#92977; Health o meter, McCook, IL) and measured weight by using a digital scale (Seca CE#96990; Seca, Chino, CA), which we used to calculate the BMI z score (BMIz) and percent of the 95th percentile for children and the BMI for parents.21 Additional child outcomes included a 1-minute recovery heart rate after a 3-minute stepping test, 22 blood pressure, 23 waist circumference, body fat percentage, 24 and fasting laboratory values, including lipids, glucose, hemoglobin A1c (HbA1c), and insulin.
We measured child dietary intake with 43 items from the Food Frequency Questionnaire, in the domains of fruit, vegetable, sugar-sweetened beverage, and sweet snack
intake, which was completed by the parent on behalf of the child.25 We measured child physical activity with a modified version of the Physical Activity Questionnaire, which involved a parent-assisted interview with the child.26 A research assistant interviewed the child by using Sizing Me Up, an obesity-specific instrument that measures quality of life, divided into 5 subscales with scaled scores out of 100: emotional, teasing/marginalization, physical, social avoidance, and positive attributes.27 We assessed parent motivation with the Parent Motivation Inventory.28
Analysis
According to power calculations, a sample size of 100 participants would provide >80% power to detect a mean treatment difference of −0.14 in BMIz by using a 2-sided α = .05, assuming an SD of 0.20 and a 30% attrition rate. Given emerging evidence of the limitations of BMIz among children with severe obesity, we also included an exploratory analysis of the changes in the percent of the 95th percentile for BMI.29 We used intent-to-treat analysis for all participants, regardless of their engagement level in the intervention. We used descriptive statistics to report baseline findings. We compared intervention and control groups at 3 and 6 months by using paired t tests. We performed statistical analyses using Stata 14.1 (StataCorp, College Station, TX).
Results
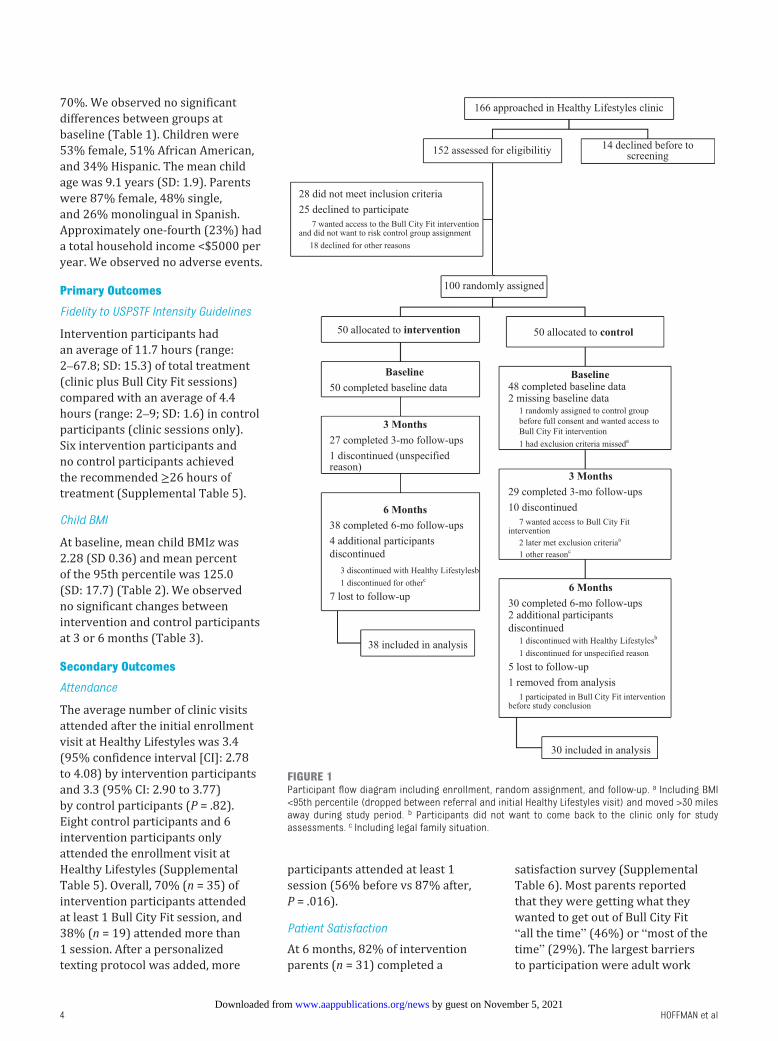
We randomly assigned 100 child-parent dyads to intervention (n = 50) or control (n = 50) and collected baseline data from 97 child-parent dyads. Approximately 60% (n = 56) of child-parent dyads completed 3-month assessments, and 70% of child-parent dyads (n = 68) completed 6-month assessments (see the Consolidated Standards of Reporting Trials diagram, Fig 1). The total retention rate at 6 months was
PEDIATRICS Volume 141, number 1, January 2018 3 by guest on November 5, 2021www.aappublications.org/newsDownloaded from
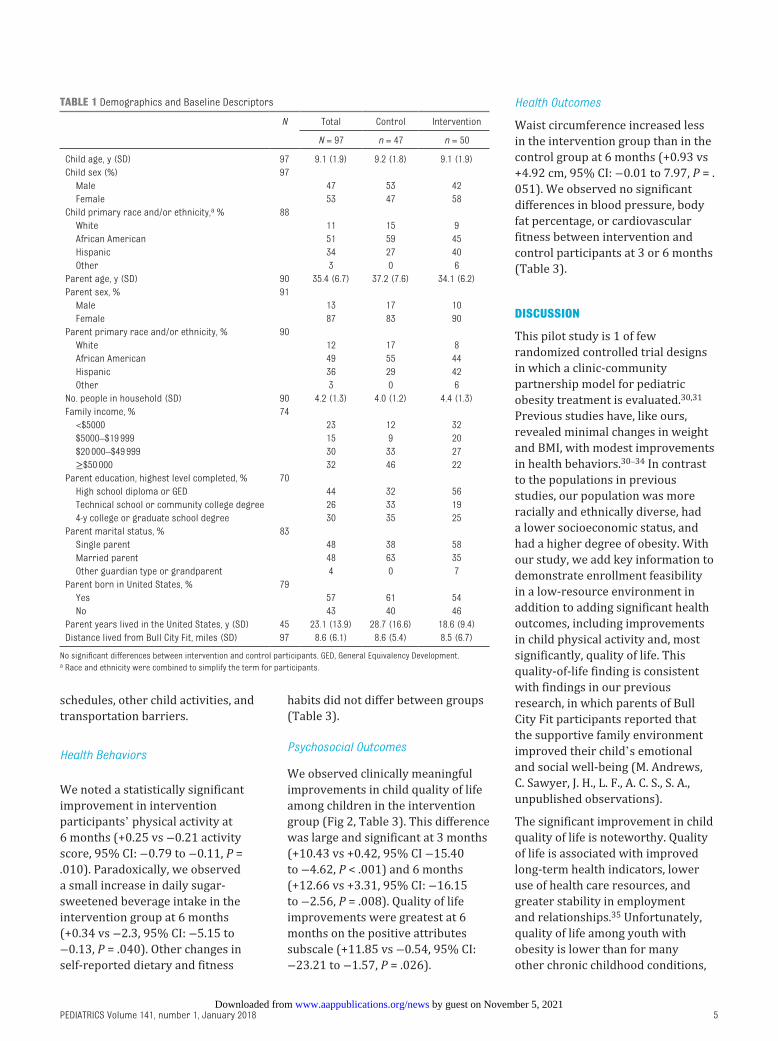
70%. We observed no significant differences between groups at baseline (Table 1). Children were 53% female, 51% African American, and 34% Hispanic. The mean child age was 9.1 years (SD: 1.9). Parents were 87% female, 48% single, and 26% monolingual in Spanish. Approximately one-fourth (23%) had a total household income <$5000 per year. We observed no adverse events.
Primary outcomes
Fidelity to USPSTF Intensity Guidelines
Intervention participants had an average of 11.7 hours (range: 2–67.8; SD: 15.3) of total treatment (clinic plus Bull City Fit sessions) compared with an average of 4.4 hours (range: 2–9; SD: 1.6) in control participants (clinic sessions only). Six intervention participants and no control participants achieved the recommended ≥26 hours of treatment (Supplemental Table 5).
Child BMI
At baseline, mean child BMIz was 2.28 (SD 0.36) and mean percent of the 95th percentile was 125.0 (SD: 17.7) (Table 2). We observed no significant changes between intervention and control participants at 3 or 6 months (Table 3).
secondary outcomes
Attendance
The average number of clinic visits attended after the initial enrollment visit at Healthy Lifestyles was 3.4 (95% confidence interval [CI]: 2.78 to 4.08) by intervention participants and 3.3 (95% CI: 2.90 to 3.77) by control participants (P = .82). Eight control participants and 6 intervention participants only attended the enrollment visit at Healthy Lifestyles (Supplemental Table 5). Overall, 70% (n = 35) of intervention participants attended at least 1 Bull City Fit session, and 38% (n = 19) attended more than 1 session. After a personalized texting protocol was added, more
participants attended at least 1 session (56% before vs 87% after, P = .016).
Patient Satisfaction
At 6 months, 82% of intervention parents (n = 31) completed a
satisfaction survey (Supplemental Table 6). Most parents reported that they were getting what they wanted to get out of Bull City Fit “all the time” (46%) or “most of the time” (29%). The largest barriers to participation were adult work
HOFFMAN et al4
FiGuRe 1Participant flow diagram including enrollment, random assignment, and follow-up. a Including BMI <95th percentile (dropped between referral and initial Healthy Lifestyles visit) and moved >30 miles away during study period. b Participants did not want to come back to the clinic only for study assessments. c Including legal family situation.
by guest on November 5, 2021www.aappublications.org/newsDownloaded from
schedules, other child activities, and transportation barriers.
Health Behaviors
We noted a statistically significant improvement in intervention participants’ physical activity at 6 months (+0.25 vs −0.21 activity score, 95% CI: −0.79 to −0.11, P = .010). Paradoxically, we observed a small increase in daily sugar-sweetened beverage intake in the intervention group at 6 months (+0.34 vs −2.3, 95% CI: −5.15 to −0.13, P = .040). Other changes in self-reported dietary and fitness
habits did not differ between groups (Table 3).
Psychosocial Outcomes
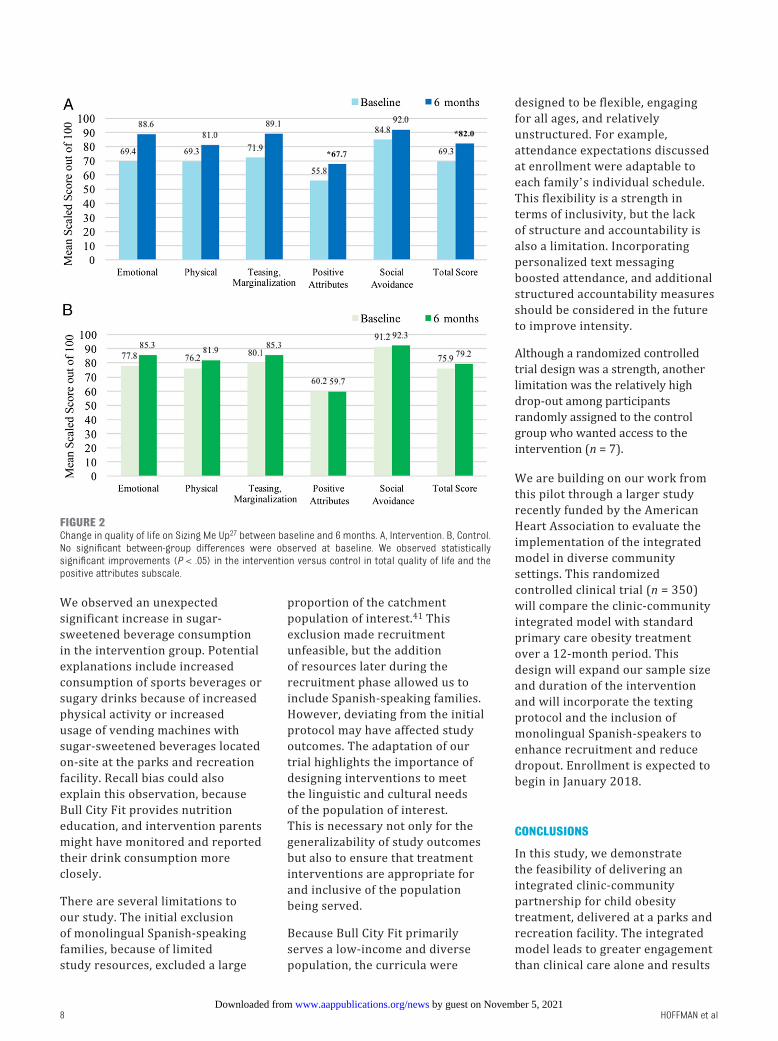
We observed clinically meaningful improvements in child quality of life among children in the intervention group (Fig 2, Table 3). This difference was large and significant at 3 months (+10.43 vs +0.42, 95% CI −15.40 to −4.62, P < .001) and 6 months (+12.66 vs +3.31, 95% CI: −16.15 to −2.56, P = .008). Quality of life improvements were greatest at 6 months on the positive attributes subscale (+11.85 vs −0.54, 95% CI: −23.21 to −1.57, P = .026).
Health Outcomes
Waist circumference increased less in the intervention group than in the control group at 6 months (+0.93 vs +4.92 cm, 95% CI: −0.01 to 7.97, P = . 051). We observed no significant differences in blood pressure, body fat percentage, or cardiovascular fitness between intervention and control participants at 3 or 6 months (Table 3).
discussion
This pilot study is 1 of few randomized controlled trial designs in which a clinic-community partnership model for pediatric obesity treatment is evaluated.30, 31 Previous studies have, like ours, revealed minimal changes in weight and BMI, with modest improvements in health behaviors.30 – 34 In contrast to the populations in previous studies, our population was more racially and ethnically diverse, had a lower socioeconomic status, and had a higher degree of obesity. With our study, we add key information to demonstrate enrollment feasibility in a low-resource environment in addition to adding significant health outcomes, including improvements in child physical activity and, most significantly, quality of life. This quality-of-life finding is consistent with findings in our previous research, in which parents of Bull City Fit participants reported that the supportive family environment improved their child’s emotional and social well-being (M. Andrews, C. Sawyer, J. H., L. F., A. C. S., S. A., unpublished observations).
The significant improvement in child quality of life is noteworthy. Quality of life is associated with improved long-term health indicators, lower use of health care resources, and greater stability in employment and relationships.35 Unfortunately, quality of life among youth with obesity is lower than for many other chronic childhood conditions,
PEDIATRICS Volume 141, number 1, January 2018 5
table 1 Demographics and Baseline Descriptors
N Total Control Intervention
N = 97 n = 47 n = 50
Child age, y (SD) 97 9.1 (1.9) 9.2 (1.8) 9.1 (1.9)Child sex (%) 97 Male 47 53 42 Female 53 47 58Child primary race and/or ethnicity, a % 88 White 11 15 9 African American 51 59 45 Hispanic 34 27 40 Other 3 0 6Parent age, y (SD) 90 35.4 (6.7) 37.2 (7.6) 34.1 (6.2)Parent sex, % 91 Male 13 17 10 Female 87 83 90Parent primary race and/or ethnicity, % 90 White 12 17 8 African American 49 55 44 Hispanic 36 29 42 Other 3 0 6No. people in household (SD) 90 4.2 (1.3) 4.0 (1.2) 4.4 (1.3)Family income, % 74 <$5000 23 12 32 $5000–$19 999 15 9 20 $20 000–$49 999 30 33 27 ≥$50 000 32 46 22Parent education, highest level completed, % 70 High school diploma or GED 44 32 56 Technical school or community college degree 26 33 19 4-y college or graduate school degree 30 35 25Parent marital status, % 83 Single parent 48 38 58 Married parent 48 63 35 Other guardian type or grandparent 4 0 7Parent born in United States, % 79 Yes 57 61 54 No 43 40 46Parent years lived in the United States, y (SD) 45 23.1 (13.9) 28.7 (16.6) 18.6 (9.4)Distance lived from Bull City Fit, miles (SD) 97 8.6 (6.1) 8.6 (5.4) 8.5 (6.7)
No significant differences between intervention and control participants. GED, General Equivalency Development.a Race and ethnicity were combined to simplify the term for participants.
by guest on November 5, 2021www.aappublications.org/newsDownloaded from
including cancer.36 Long-term studies have revealed that obesity interventions that improve quality of life lead to improvements in weight status.37 It is possible, therefore, that the short duration of our study did not allow us to observe longer-term changes in weight status.
The authors of previous studies of clinic-community models for
child obesity treatment have incompletely assessed child quality of life. Of the 5 comparable trials, only 1 included the measurement of health-related quality of life.30 –34 The authors of this study measured quality of life by using a different scale and found a significant improvement; however, a prospective cohort design was used, which limited the conclusion
that quality-of-life changes were caused by the intervention.32 Our randomized controlled design is supportive of the conclusion that a clinic-community model enhances the lives of children in meaningful ways by directly improving quality of life.
We also demonstrated the feasibility of delivering child obesity treatment in collaboration with parks and recreation departments. The National Recreation and Park Association and its member organizations are well-suited partners for community-based wellness programming. The National Recreation and Park Association is a nonprofit organization that promotes public parks, recreation, and conservation; their 3 pillars are “conservation, health/wellness, and social equity.” 38 Parks and recreation departments are nearly ubiquitous in communities across the United States, with 1 recreation center for every 26 650 residents offered within its member communities, 38 and centers are typically located in low-resource communities.
In addition to delivering a child obesity program, the partnership with parks and recreation departments provides mutual benefit to the clinic and the parks and recreation agency. In our previous studies, clinic staff report high satisfaction with the ability to “refer” patients to a free, local fitness program. Durham Parks and Recreation leadership reported that, since the partnership began in 2012, the recreation center hosting Bull City Fit has become the most highly used parks and recreation facility in the city. Because of high volume, this center receives a higher proportion of city appropriations, which can be used to add staff, equipment, and complete needed repairs to the facility.
HOFFMAN et al6
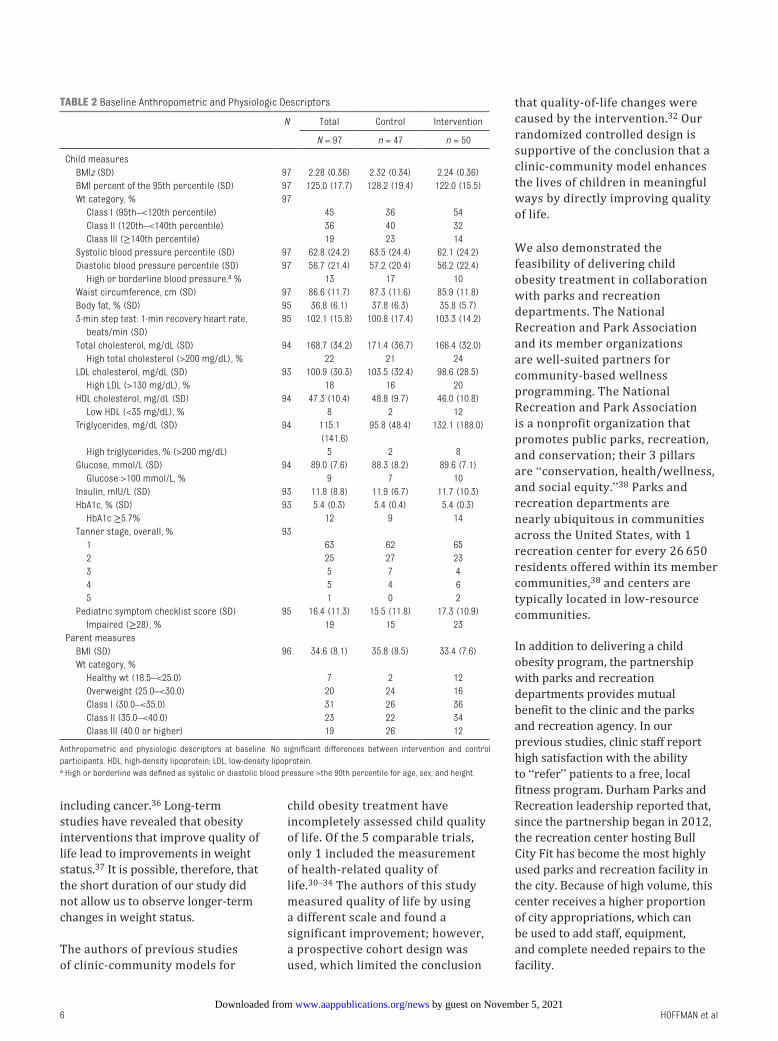
table 2 Baseline Anthropometric and Physiologic Descriptors
N Total Control Intervention
N = 97 n = 47 n = 50
Child measures BMIz (SD) 97 2.28 (0.36) 2.32 (0.34) 2.24 (0.36) BMI percent of the 95th percentile (SD) 97 125.0 (17.7) 128.2 (19.4) 122.0 (15.5) Wt category, % 97 Class I (95th–<120th percentile) 45 36 54 Class II (120th–<140th percentile) 36 40 32 Class III (≥140th percentile) 19 23 14 Systolic blood pressure percentile (SD) 97 62.8 (24.2) 63.5 (24.4) 62.1 (24.2) Diastolic blood pressure percentile (SD) 97 56.7 (21.4) 57.2 (20.4) 56.2 (22.4) High or borderline blood pressure, a % 13 17 10 Waist circumference, cm (SD) 97 86.6 (11.7) 87.3 (11.6) 85.9 (11.8) Body fat, % (SD) 95 36.8 (6.1) 37.8 (6.3) 35.8 (5.7) 3-min step test: 1-min recovery heart rate,
beats/min (SD)95 102.1 (15.8) 100.8 (17.4) 103.3 (14.2)
Total cholesterol, mg/dL (SD) 94 168.7 (34.2) 171.4 (36.7) 166.4 (32.0) High total cholesterol (>200 mg/dL), % 22 21 24 LDL cholesterol, mg/dL (SD) 93 100.9 (30.3) 103.5 (32.4) 98.6 (28.5) High LDL (>130 mg/dL), % 18 16 20 HDL cholesterol, mg/dL (SD) 94 47.3 (10.4) 48.8 (9.7) 46.0 (10.8) Low HDL (<35 mg/dL), % 8 2 12 Triglycerides, mg/dL (SD) 94 115.1
(141.6)95.8 (48.4) 132.1 (188.0)
High triglycerides, % (>200 mg/dL) 5 2 8 Glucose, mmol/L (SD) 94 89.0 (7.6) 88.3 (8.2) 89.6 (7.1) Glucose >100 mmol/L, % 9 7 10 Insulin, mIU/L (SD) 93 11.8 (8.8) 11.9 (6.7) 11.7 (10.3) HbA1c, % (SD) 93 5.4 (0.3) 5.4 (0.4) 5.4 (0.3) HbA1c ≥5.7% 12 9 14 Tanner stage, overall, % 93 1 63 62 65 2 25 27 23 3 5 7 4 4 5 4 6 5 1 0 2 Pediatric symptom checklist score (SD) 95 16.4 (11.3) 15.5 (11.8) 17.3 (10.9) Impaired (≥28), % 19 15 23Parent measures BMI (SD) 96 34.6 (8.1) 35.8 (8.5) 33.4 (7.6) Wt category, % Healthy wt (18.5–<25.0) 7 2 12 Overweight (25.0–<30.0) 20 24 16 Class I (30.0–<35.0) 31 26 36 Class II (35.0–<40.0) 23 22 34 Class III (40.0 or higher) 19 26 12
Anthropometric and physiologic descriptors at baseline. No significant differences between intervention and control participants. HDL, high-density lipoprotein; LDL, low-density lipoprotein.a High or borderline was defined as systolic or diastolic blood pressure >the 90th percentile for age, sex, and height.
by guest on November 5, 2021www.aappublications.org/newsDownloaded from
One of our key primary outcomes was intensity of the program in terms of treatment hours and meeting current USPSTF recommendations (≥26 hours over 6 months). We designed the program to address known barriers to achieving this goal, including being open 6 days per week, with after-school and work access hours,
free programming, engaging group activities, family participation, digital support through mobile devices, incentives and/or prizes for participation, and geographic location within the community. Although the intervention did lead to increased hours of treatment (11.7 vs 4.4 in the clinic-only group), only 6 intervention
participants, and no control participants, achieved ≥26 hours of treatment. This is consistent with findings in previous studies that have revealed difficulty meeting recommended treatment hours, 39, 40 which suggests that meeting time-specific treatment targets may be poorly feasible in low-resource communities.
PEDIATRICS Volume 141, number 1, January 2018 7
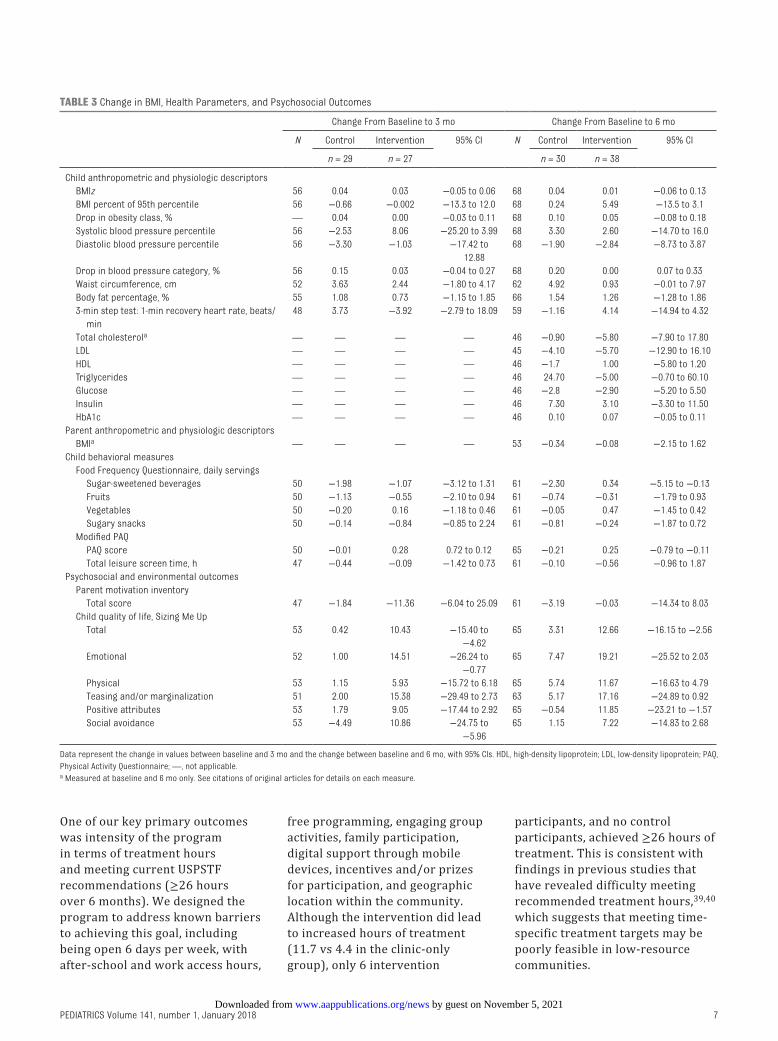
table 3 Change in BMI, Health Parameters, and Psychosocial Outcomes
Change From Baseline to 3 mo Change From Baseline to 6 mo
N Control Intervention 95% CI N Control Intervention 95% CI
n = 29 n = 27 n = 30 n = 38
Child anthropometric and physiologic descriptors BMIz 56 0.04 0.03 −0.05 to 0.06 68 0.04 0.01 −0.06 to 0.13 BMI percent of 95th percentile 56 −0.66 −0.002 −13.3 to 12.0 68 0.24 5.49 −13.5 to 3.1 Drop in obesity class, % — 0.04 0.00 −0.03 to 0.11 68 0.10 0.05 −0.08 to 0.18 Systolic blood pressure percentile 56 −2.53 8.06 −25.20 to 3.99 68 3.30 2.60 −14.70 to 16.0 Diastolic blood pressure percentile 56 −3.30 −1.03 −17.42 to
12.8868 −1.90 −2.84 −8.73 to 3.87
Drop in blood pressure category, % 56 0.15 0.03 −0.04 to 0.27 68 0.20 0.00 0.07 to 0.33 Waist circumference, cm 52 3.63 2.44 −1.80 to 4.17 62 4.92 0.93 −0.01 to 7.97 Body fat percentage, % 55 1.08 0.73 −1.15 to 1.85 66 1.54 1.26 −1.28 to 1.86 3-min step test: 1-min recovery heart rate, beats/
min48 3.73 −3.92 −2.79 to 18.09 59 −1.16 4.14 −14.94 to 4.32
Total cholesterola — — — — 46 −0.90 −5.80 −7.90 to 17.80 LDL — — — — 45 −4.10 −5.70 −12.90 to 16.10 HDL — — — — 46 −1.7 1.00 −5.80 to 1.20 Triglycerides — — — — 46 24.70 −5.00 −0.70 to 60.10 Glucose — — — — 46 −2.8 −2.90 −5.20 to 5.50 Insulin — — — — 46 7.30 3.10 −3.30 to 11.50 HbA1c — — — — 46 0.10 0.07 −0.05 to 0.11Parent anthropometric and physiologic descriptors BMIa — — — — 53 −0.34 −0.08 −2.15 to 1.62Child behavioral measures Food Frequency Questionnaire, daily servings Sugar-sweetened beverages 50 −1.98 −1.07 −3.12 to 1.31 61 −2.30 0.34 −5.15 to −0.13 Fruits 50 −1.13 −0.55 −2.10 to 0.94 61 −0.74 −0.31 −1.79 to 0.93 Vegetables 50 −0.20 0.16 −1.18 to 0.46 61 −0.05 0.47 −1.45 to 0.42 Sugary snacks 50 −0.14 −0.84 −0.85 to 2.24 61 −0.81 −0.24 −1.87 to 0.72 Modified PAQ PAQ score 50 −0.01 0.28 0.72 to 0.12 65 −0.21 0.25 −0.79 to −0.11 Total leisure screen time, h 47 −0.44 −0.09 −1.42 to 0.73 61 −0.10 −0.56 −0.96 to 1.87Psychosocial and environmental outcomes Parent motivation inventory Total score 47 −1.84 −11.36 −6.04 to 25.09 61 −3.19 −0.03 −14.34 to 8.03 Child quality of life, Sizing Me Up Total 53 0.42 10.43 −15.40 to
−4.6265 3.31 12.66 −16.15 to −2.56
Emotional 52 1.00 14.51 −26.24 to −0.77
65 7.47 19.21 −25.52 to 2.03
Physical 53 1.15 5.93 −15.72 to 6.18 65 5.74 11.67 −16.63 to 4.79 Teasing and/or marginalization 51 2.00 15.38 −29.49 to 2.73 63 5.17 17.16 −24.89 to 0.92 Positive attributes 53 1.79 9.05 −17.44 to 2.92 65 −0.54 11.85 −23.21 to −1.57 Social avoidance 53 −4.49 10.86 −24.75 to
−5.9665 1.15 7.22 −14.83 to 2.68
Data represent the change in values between baseline and 3 mo and the change between baseline and 6 mo, with 95% CIs. HDL, high-density lipoprotein; LDL, low-density lipoprotein; PAQ, Physical Activity Questionnaire; —, not applicable.a Measured at baseline and 6 mo only. See citations of original articles for details on each measure.
by guest on November 5, 2021www.aappublications.org/newsDownloaded from
We observed an unexpected significant increase in sugar-sweetened beverage consumption in the intervention group. Potential explanations include increased consumption of sports beverages or sugary drinks because of increased physical activity or increased usage of vending machines with sugar-sweetened beverages located on-site at the parks and recreation facility. Recall bias could also explain this observation, because Bull City Fit provides nutrition education, and intervention parents might have monitored and reported their drink consumption more closely.
There are several limitations to our study. The initial exclusion of monolingual Spanish-speaking families, because of limited study resources, excluded a large
proportion of the catchment population of interest.41 This exclusion made recruitment unfeasible, but the addition of resources later during the recruitment phase allowed us to include Spanish-speaking families. However, deviating from the initial protocol may have affected study outcomes. The adaptation of our trial highlights the importance of designing interventions to meet the linguistic and cultural needs of the population of interest. This is necessary not only for the generalizability of study outcomes but also to ensure that treatment interventions are appropriate for and inclusive of the population being served.
Because Bull City Fit primarily serves a low-income and diverse population, the curricula were
designed to be flexible, engaging for all ages, and relatively unstructured. For example, attendance expectations discussed at enrollment were adaptable to each family’s individual schedule. This flexibility is a strength in terms of inclusivity, but the lack of structure and accountability is also a limitation. Incorporating personalized text messaging boosted attendance, and additional structured accountability measures should be considered in the future to improve intensity.
Although a randomized controlled trial design was a strength, another limitation was the relatively high drop-out among participants randomly assigned to the control group who wanted access to the intervention (n = 7).
We are building on our work from this pilot through a larger study recently funded by the American Heart Association to evaluate the implementation of the integrated model in diverse community settings. This randomized controlled clinical trial (n = 350) will compare the clinic-community integrated model with standard primary care obesity treatment over a 12-month period. This design will expand our sample size and duration of the intervention and will incorporate the texting protocol and the inclusion of monolingual Spanish-speakers to enhance recruitment and reduce dropout. Enrollment is expected to begin in January 2018.
conclusions
In this study, we demonstrate the feasibility of delivering an integrated clinic-community partnership for child obesity treatment, delivered at a parks and recreation facility. The integrated model leads to greater engagement than clinical care alone and results
HOFFMAN et al8
FiGuRe 2Change in quality of life on Sizing Me Up27 between baseline and 6 months. A, Intervention. B, Control. No significant between-group differences were observed at baseline. We observed statistically significant improvements (P < .05) in the intervention versus control in total quality of life and the positive attributes subscale.
by guest on November 5, 2021www.aappublications.org/newsDownloaded from
in a meaningful improvement in child quality of life.
acKnoWledGMents
We acknowledge the following important individuals for their assistance in conducting this study: the dedicated, compassionate, and hardworking staff at Healthy Lifestyles, for their accommodation of this research study in clinic and for the excellent care they deliver
to patients; Maria Andrews and Carolyn Sawyer, for their valuable collaboration and hard work in the retrospective analysis of this integrated model that provided the background and framework for this prospective trial; Lisa Watson, for clinic coordination and collaboration and for providing invaluable insight throughout this pilot; Cara Mariani, for help in recruitment; and Jacob Christy, Jasmine Burroughs,
and Sophie Ravanbakht, for help during recruitment and follow-up assessments.
PEDIATRICS Volume 141, number 1, January 2018 9
The satisfaction survey designed by the study team for this trial and completed by parents in the intervention group to assess satisfaction with Bull City Fit and potential barriers to participation.
doi: https:// doi. org/ 10. 1542/ peds. 2017- 1444
Accepted for publication Oct 13, 2017
Address correspondence to Jessica Hoffman, Duke Children’s Healthy Lifestyles, 4020 N Roxboro St, Durham, NC 27704. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2018 by the American Academy of Pediatrics
Financial disclosuRe: The authors have indicated they have no financial relationships relevant to this article to disclose.
FundinG: Supported by the Early Career Award from the Obesity Society, awarded to Dr Frerichs.
Potential conFlict oF inteRest: The authors have indicated they have no potential conflicts of interest to disclose.
ReFeRences
1. Ogden CL, Carroll MD, Fryar CD, Flegal KM. Prevalence of obesity among adults and youth: United States, 2011-2014. NCHS Data Brief. 2015;(219): 1–8
2. Skinner AC, Perrin EM, Skelton JA. Prevalence of obesity and severe obesity in US children, 1999-2014. Obesity (Silver Spring). 2016;24(5):1116–1123
3. Skinner AC, Perrin EM, Skelton JA. Cardiometabolic risks and obesity in the young. N Engl J Med. 2016;374(6):592–593
4. Freedman DS, Ogden CL, Kit BK. Interrelationships between BMI, skinfold thicknesses, percent body fat, and cardiovascular disease risk factors among U.S. children and adolescents. BMC Pediatr. 2015;15:188
5. Ul-Haq Z, Mackay DF, Fenwick E, Pell JP. Meta-analysis of the association between body mass index and health-related quality of life among children and adolescents, assessed using the pediatric quality of life inventory index. J Pediatr. 2013;162(2):280–286.e1
6. Tirosh A, Shai I, Afek A, et al. Adolescent BMI trajectory and risk of diabetes versus coronary disease. N Engl J Med. 2011;364(14):1315–1325
7. Twig G, Tirosh A, Leiba A, et al. BMI at age 17 years and diabetes mortality in midlife: a nationwide cohort of 2.3 million adolescents. Diabetes Care. 2016;39(11):1996–2003
8. Barlow SE; Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary Report. Pediatrics. 2007;120(suppl 4): S164–S192
9. Whitlock EP, O’Conner EA, Williams SB, Beil TL, Lutz KWUS. Effectiveness of Primary Care Interventions for Weight Management in Children and Adolescents: An Updated, Targeted Systematic Review for the USPSTF. Rockville, MD: Agency for Healthcare Research and Quality; 2010. Evidence Syntheses; No. 76
10. Haemer M, Cluett S, Hassink SG, et al. Building capacity for childhood obesity
prevention and treatment in the medical community: call to action. Pediatrics. 2011;128(suppl 2):S71–S77
11. Slusser W, Staten K, Stephens K, et al. Payment for obesity services: examples and recommendations for stage 3 comprehensive multidisciplinary intervention programs for children and adolescents. Pediatrics. 2011;128(suppl 2):S78–S85
12. Skelton JA, Irby MB, Beech BM, Rhodes SD. Attrition and family participation in obesity treatment programs: clinicians’ perceptions. Acad Pediatr. 2012;12(5):420–428
13. Skelton JA, Irby MB, Geiger AM. A systematic review of satisfaction and pediatric obesity treatment: new avenues for addressing attrition. J Healthc Qual. 2014;36(4):5–22
14. Skelton JA, Martin S, Irby MB. Satisfaction and attrition in paediatric weight management. Clin Obes. 2016;6(2):143–153
15. Innovative Care for Chronic Conditions. Building Blocks for Action - Global
abbReviations
BMIz: BMI z scoreCI: confidence intervalHbA1c: hemoglobin A1cUSPSTF: US Preventive Services
Task Force
by guest on November 5, 2021www.aappublications.org/newsDownloaded from

HOFFMAN et al10
Report. Geneva, Switzerland: World Health Organization; 2002
16. Dietz WH, Solomon LS, Pronk N, et al. An integrated framework for the prevention and treatment of obesity and its related chronic diseases. Health Aff (Millwood). 2015;34(9):1456–1463
17. Skelton JA, Goff DC Jr, Ip E, Beech BM. Attrition in a multidisciplinary pediatric weight management clinic. Child Obes. 2011;7(3):185–193
18. Dolinsky DH, Armstrong SC, Østbye T. Predictors of attrition from a clinical pediatric obesity treatment program. Clin Pediatr (Phila). 2012;51(12):1168–1174
19. Dolinsky DH, Armstrong SC, Walter EB, Kemper AR. The effectiveness of a primary care-based pediatric obesity program. Clin Pediatr (Phila). 2012;51(4):345–353
20. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381
21. Flegal KM, Wei R, Ogden CL, Freedman DS, Johnson CL, Curtin LR. Characterizing extreme values of body mass index-for-age by using the 2000 Centers for Disease Control and Prevention growth charts. Am J Clin Nutr. 2009;90(5):1314–1320
22. Francis K, Feinstein R. A simple height-specific and rate-specific step test for children. South Med J. 1991;84(2):169–174
23. Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents; National Heart, Lung, and Blood Institute. Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: summary report. Pediatrics. 2011;128(suppl 5):S213–S256
24. Nunez C, Rubiano F, Horlick M, Thornton J, Heymsfield SB. Application of
Leg-to-Leg Bioimpedance System in Children. Atlanta, GA: International Life Sciences Institute Center for Health Promotion; 1999
25. Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Questionnaire. Hyattsville, MD: U.S. Department of Health and Human Services, 2015. Available at: https:// wwwn. cdc. gov/ nchs/ nhanes/ ContinuousNhanes/ Default. aspx? BeginYear= 2015. Accessed April 1, 2017
26. Kowalski KC, Crocker PRE, Donen RM. The Physical Activity Questionnaire for Older Children (PAQ-C) and Adolescents (PAQ-A) Manual. Saskatoon, Canada: University of Saskatchewan College of Kinesiology; 2004
27. Zeller MH, Modi AC. Development and initial validation of an obesity-specific quality-of-life measure for children: Sizing Me Up. Obesity (Silver Spring). 2009;17(6):1171–1177
28. Nock MK, Photos V. Parent motivation to participate in treatment: assessment and prediction of subsequent participation. J Child Fam Stud. 2006;15(3):333–346
29. Freedman DS, Butte NF, Taveras EM, et al. BMI z-scores are a poor indicator of adiposity among 2- to 19-year-olds with very high BMIs, NHANES 1999-2000 to 2013-2014. Obesity (Silver Spring). 2017;25(4):739–746
30. Serra-Paya N, Ensenyat A, Castro-Viñuales I, et al. Effectiveness of a multi-component intervention for overweight and obese children (Nereu program): a randomized controlled trial. PLoS One. 2015;10(12):e0144502
31. Savoye M, Shaw M, Dziura J, et al. Effects of a weight management program on body composition and metabolic parameters in overweight children: a randomized controlled trial. JAMA. 2007;297(24):2697–2704
32. Cronk CE, Hoffmann RG, Mueller MJ, Zerpa-Uriona V, Dasgupta M, Enriquez F. Effects of a culturally tailored intervention on changes in body mass
index and health-related quality of life of Latino children and their parents. Am J Health Promot. 2011;25(4):e1–e11
33. Kokkvoll A, Grimsgaard S, Ødegaard R, Flægstad T, Njølstad I. Single versus multiple-family intervention in childhood overweight–Finnmark Activity School: a randomised trial. Arch Dis Child. 2014;99(3):225–231
34. McCormick DP, Ramirez M, Caldwell S, Ripley AW, Wilkey D. YMCA program for childhood obesity: a case series. Clin Pediatr (Phila). 2008;47(7):693–697
35. Gellert GA. The importance of quality of life research for health care reform in the USA and the future of public health. Qual Life Res. 1993;2(5):357–361
36. Schwimmer JB, Burwinkle TM, Varni JW. Health-related quality of life of severely obese children and adolescents. JAMA. 2003;289(14):1813–1819
37. Griffiths LJ, Parsons TJ, Hill AJ. Self-esteem and quality of life in obese children and adolescents: a systematic review. Int J Pediatr Obes. 2010;5(4):282–304
38. National Recreation and Park Association. 2016 NRPA field report: park and recreation agency performance benchmarks. 2016. Available at: www. nrpa. org/ uploadedFiles/ nrpa. org/ Publications_ and_ Research/ Research/ Field- Report. pdf. Accessed April 1, 2017
39. Jasik CB, King EC, Rhodes E, et al. Characteristics of youth presenting for weight management: retrospective national data from the POWER study group. Child Obes. 2015;11(5):630–637
40. Kirk S, Armstrong S, King E, et al. Establishment of the pediatric obesity weight evaluation registry: a National Research Collaborative for identifying the optimal assessment and treatment of pediatric obesity. Child Obes. 2017;13(1):9–17
41. The Latino Migration Project. Durham’s immigrant communities: looking to the future. Available at: http:// isa. unc. edu/ files/ 2013/ 02/ Durhams- Immigrant- Communities. pdf. Accessed April 1, 2017
by guest on November 5, 2021www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2017-1444 originally published online December 13, 2017; 2018;141;Pediatrics
Asheley Skinner and Sarah ArmstrongJessica Hoffman, Leah Frerichs, Mary Story, Jason Jones, Kiah Gaskin, Annie Apple,
Randomized Pilot TrialAn Integrated Clinic-Community Partnership for Child Obesity Treatment: A
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/141/1/e20171444including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/141/1/e20171444#BIBLThis article cites 34 articles, 8 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/public_health_subPublic Healthhttp://www.aappublications.org/cgi/collection/obesity_new_subObesityfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on November 5, 2021www.aappublications.org/newsDownloaded from
DOI: 10.1542/peds.2017-1444 originally published online December 13, 2017; 2018;141;Pediatrics
Asheley Skinner and Sarah ArmstrongJessica Hoffman, Leah Frerichs, Mary Story, Jason Jones, Kiah Gaskin, Annie Apple,
Randomized Pilot TrialAn Integrated Clinic-Community Partnership for Child Obesity Treatment: A
http://pediatrics.aappublications.org/content/141/1/e20171444located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2017/12/11/peds.2017-1444.DCSupplementalData Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2018has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on November 5, 2021www.aappublications.org/newsDownloaded from


















