An Evaluation of the Greater Glasgow & Clyde Osteoporosis and Falls Strategy Dr Dawn Skelton & Fiona...
70
An Evaluation of the Greater Glasgow & Clyde Osteoporosis and Falls Strategy Dr Dawn Skelton & Fiona Neil, School of Health
-
Upload
kory-sanders -
Category
Documents
-
view
215 -
download
0
Transcript of An Evaluation of the Greater Glasgow & Clyde Osteoporosis and Falls Strategy Dr Dawn Skelton & Fiona...

An Evaluation of the Greater Glasgow & Clyde Osteoporosis
and Falls Strategy
Dr Dawn Skelton & Fiona Neil,
School of Health

The Process
• Jan 2008, Fiona Neil, OT within the Falls Service, was seconded to the GCAL 0.5 FTE for one year.
• Visits to representatives of all parts of the service (Jan 2008-Aug 2008)– Record current Protocols and Processes– Discuss and gather previous audits– Discuss potential data collection – Advise on relevant up to date guidelines/evidence base
• Any previously gathered audit or outcome information (for presentations at conferences etc) was collected as well as raw data where possible.
• Data blinded by the relevant service, permission sought from the Caldicott Guardian for NHSGGC.
• Some small audit projects and 2 Masters Project (GCU OT & PT student, with full NHS ethical approval)

CFPP• Specialist falls service which aims to prevent further falls by
providing a comprehensive falls screening, health education, exercise, rehabilitation and onward referral
• The service is available to individuals who are over 65, live at home and have had a fall in the last year
• 221 referrals a month in 2008
• Telephone triage completed within 24 hours of receiving referral
• Home screening completed within 5 working days of triage
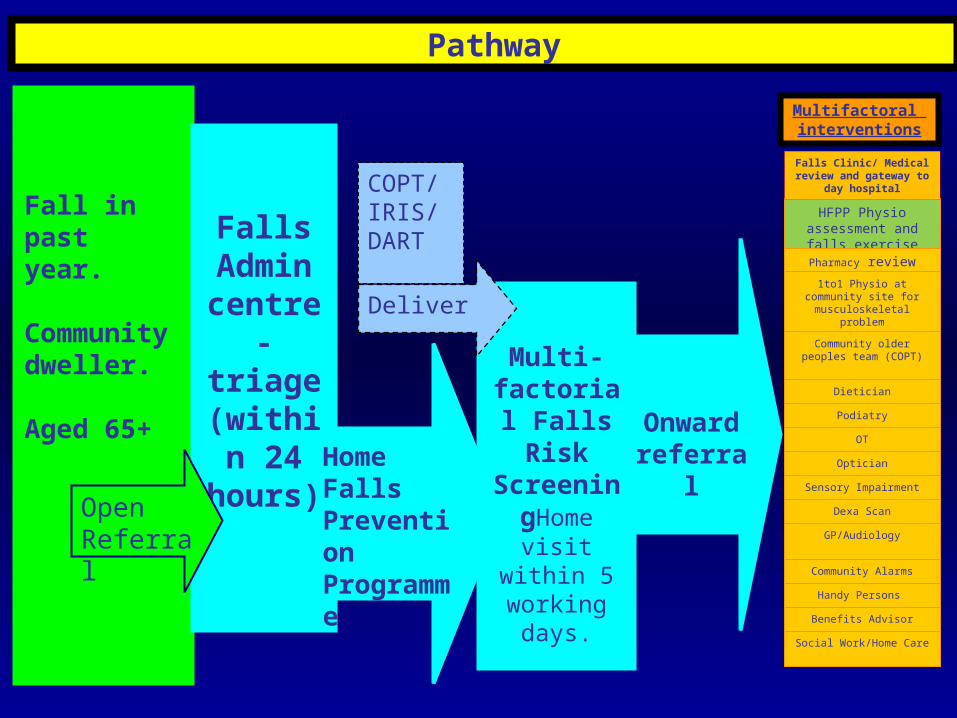
Onward referral
Fall in past year.
Community dweller.
Aged 65+
FallsAdmin centre-triage (within 24
hours)
Open Referral
Multi-factorial
Falls Risk
ScreeningHome visit
within 5 working days.
HFPP Physio assessment and
falls exercise classesPharmacy review
1to1 Physio at community site for
musculoskeletal problem
Community older peoples team (COPT)
Dietician
Podiatry
OT
Optician
Sensory Impairment
Dexa Scan
GP/Audiology
Community Alarms
Handy Persons
Benefits Advisor
Social Work/Home Care
Falls Clinic/ Medical review and gateway
to day hospital
Multifactoral interventions
COPT/IRIS/DART
Pathway
Home Falls Prevention Programme
Deliver

INTEGRATED PLANS
Fracture
Osteoporosis Falls
> 95% hip fractures due to a fall
> 90% of hip fractures
due to osteoporosis
Falls, Fragility & Fractures, Cryer & Patel, 2002

NICE Falls CG: specialist integrated service model, 2004

ABS/BGS Guidelines 2001
Assessment
History of falls
Medications & Medical Conditions
Vision
Gait and Balance
Lower Limb Joints (assistive devices)
Neurological (sensory) & Continence
Cardiovascular
Multifactorial intervention(as appropriate)
Gait, balance and exercise programmes
Medication modification
Postural Hypotension Treatment
Environmental Hazard Modification
Cardiovascular disorder treatment
AGS/BGS GuidelinesJ Am Geriatr Soc 2001; 49: 664 – 672.
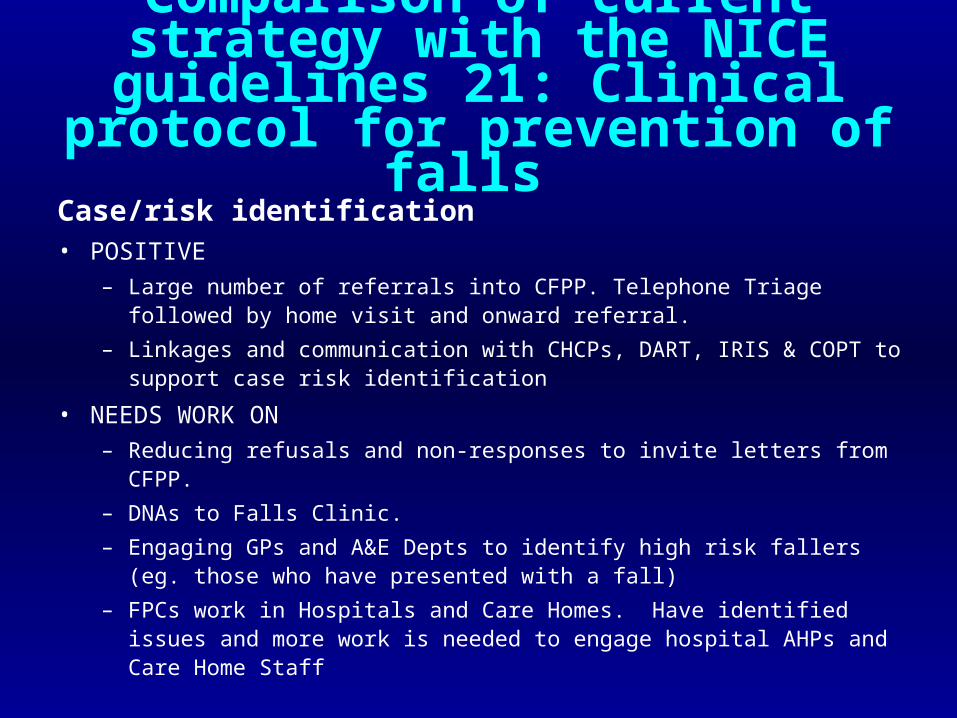
Comparison of current strategy with the NICE guidelines 21: Clinical protocol for prevention of falls
Case/risk identification
• POSITIVE– Large number of referrals into CFPP. Telephone Triage followed
by home visit and onward referral.
– Linkages and communication with CHCPs, DART, IRIS & COPT to support case risk identification
• NEEDS WORK ON– Reducing refusals and non-responses to invite letters from CFPP.
– DNAs to Falls Clinic.
– Engaging GPs and A&E Depts to identify high risk fallers (eg. those who have presented with a fall)
– FPCs work in Hospitals and Care Homes. Have identified issues and more work is needed to engage hospital AHPs and Care Home Staff

Comparison of current strategy with the NICE guidelines 21: Clinical protocol for prevention of falls
Multifactorial Falls Risk Assessment
• POSITIVE
– Excellent links with Fracture Liaison Service and Direct Access DEXA Scan and Pharmacy to ensure bone health is also considered
• NEEDS WORK ON
– Urinary Incontinence, Fear of falling, anxiety and depression and Vision assessment is minimal.
– Roll out of DADS into Clyde

Comparison of current strategy with the NICE guidelines 21: Clinical protocol for prevention of falls
Multifactorial Interventions • POSITIVE
– Evidence based exercise delivery continuum. – Good OT input to CFPP interventions.– Excellent links with Fracture Liaison Service & Pharmacy
• NEEDS WORK ON– dedicated support time for CFPP (& Falls Clinics) Clinical
Psychology – Hospital based OTs to ensure home visits before discharge – Equitable access to services across GG&C (eg syncope clinic for
potential cardiac pacing). – long-term support of home exercise programmes and primary
prevention programmes – No “tie-up” or follow up after interventions (Falls Clinics, CFPP,
Little evidence of exercise or other multi-factorial interventions occurring in care homes (apart from FPCs currently raising awareness)

Comparison of current strategy with the NICE guidelines 21: Clinical protocol for prevention of falls
Patient Engagement
• POSITIVE– Evidence of patient satisfaction questionnaires in some parts of
the service
• NEEDS WORK ON– Falls Clinics need to engage patients to understand reasons for
DNAs

Comparison of current strategy with the NICE guidelines 21: Clinical protocol for prevention of falls
Case/risk identification
• POSITIVE– Large number of referrals into CFPP. Telephone Triage followed
by home visit and onward referral.– Linkages and communication with CHCPs, DART, IRIS & COPT to
support case risk identification
• NEEDS WORK ON– Reducing refusals and non-responses to invite letters from CFPP. – DNAs to Falls Clinic. – Engaging GPs and A&E Depts to identify high risk fallers (eg.
those who have presented with a fall) – FPCs work in Hospitals and Care Homes. Have identified issues
and more work is needed to engage hospital AHPs and Care Home Staff

Comparison of current strategy with the AGS/BGS Guidelines
Assessment
History of falls
Medications & Medical Conditions
Vision
Gait and Balance
Lower Limb Joints (assistive devices)
Neurological (sensory) & Continence
Cardiovascular
Multifactorial intervention(as appropriate)
Gait, balance and exercise programmes
Medication modification
Postural Hypotension Treatment
Environmental Hazard Modification
Cardiovascular disorder treatment
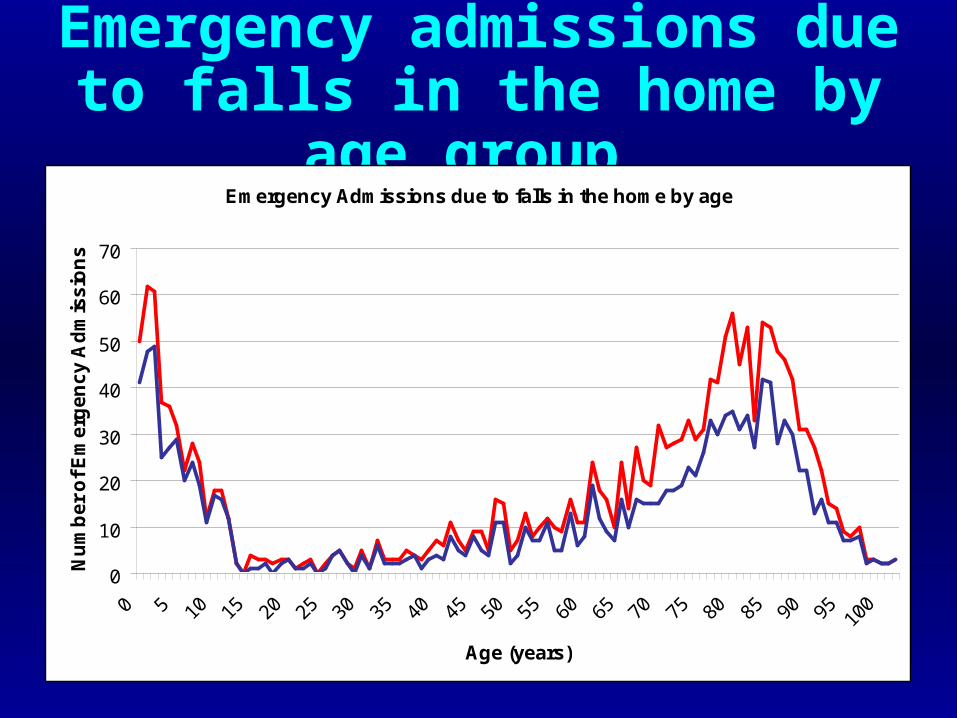
Emergency admissions due to falls in the home by age group
Emergency Admissions due to falls in the home by age
0
10
20
30
40
50
60
70
Age (years)
Nu
mb
er
of
Em
erg
en
cy
Ad
mis
sio
ns
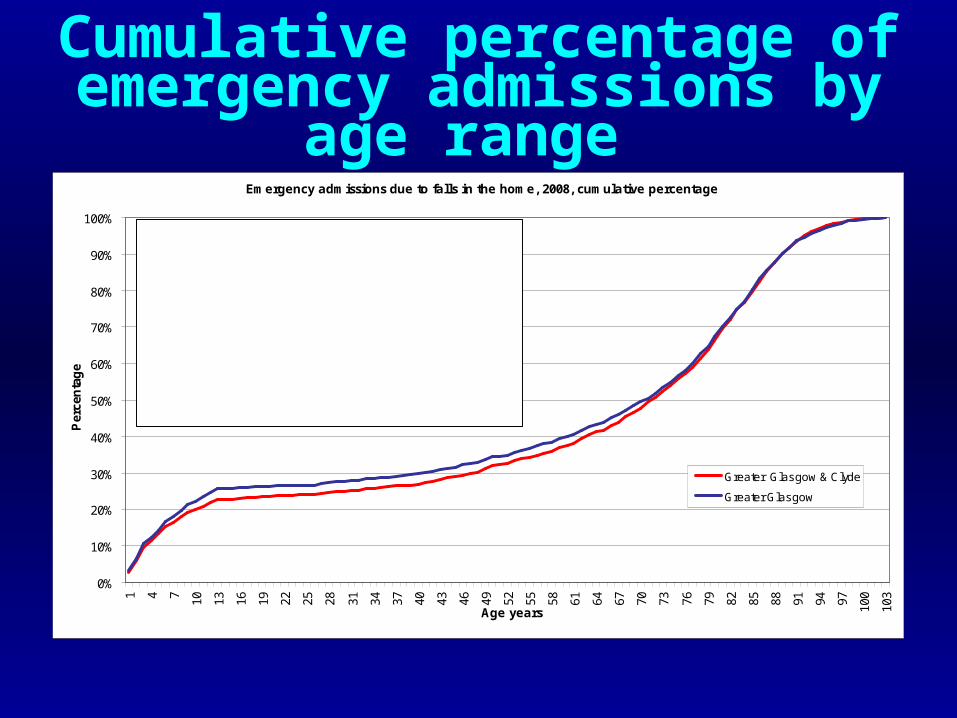
Cumulative percentage of emergency admissions by age
range Emergency admissions due to falls in the home, 2008, cumulative percentage
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1 4 7 10 13 16 19 22 25 28 31 34 37 40 43 46 49 52 55 58 61 64 67 70 73 76 79 82 85 88 91 94 97 100
103
Age years
Per
cen
tag
e
Greater Glasgow & Clyde
Greater Glasgow
Greater Glasgow & ClydePatients aged 65+ account for 57% of admissionsPatients aged 75+ account for 43% of admissionsPatients aged 80+ account for 31% of admissionsPatients aged 85+ account for 17% of admissionsGreater GlasgowPatients aged 65+ account for 55% of admissionsPatients aged 75+ account for 42% of admissionsPatients aged 80+ account for 30% of admissionsPatients aged 85+ account for 17% of admissions
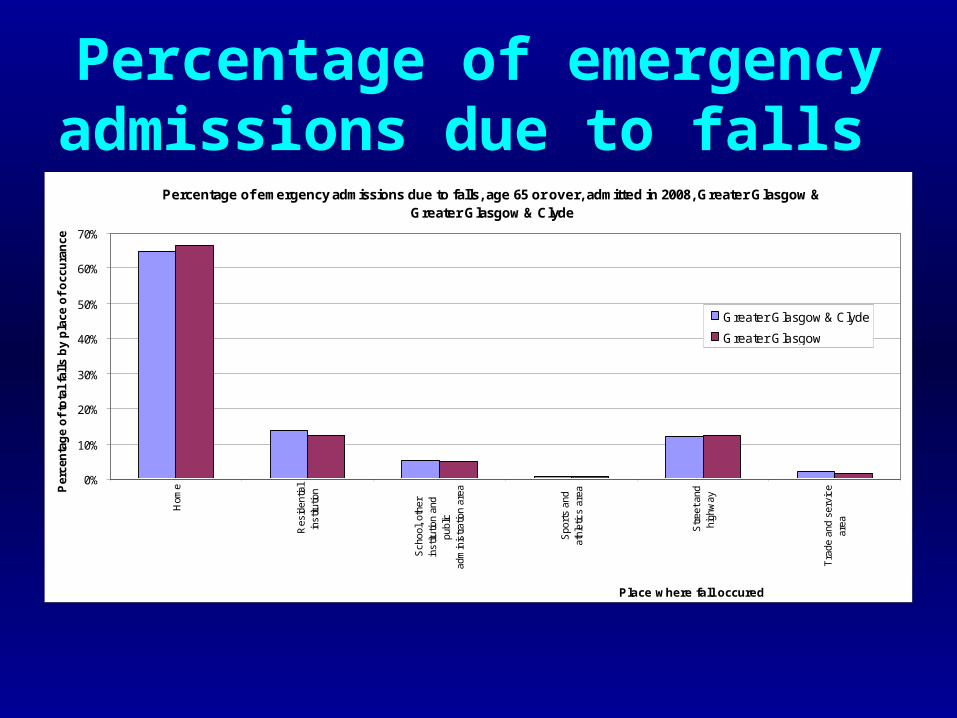
Percentage of emergency admissions due to falls
Percentage of emergency admissions due to falls, age 65 or over, admitted in 2008, Greater Glasgow & Greater Glasgow & Clyde
0%
10%
20%
30%
40%
50%
60%
70%
Hom
e
Res
iden
tial
inst
itutio
n
Sch
ool,
othe
rin
stitu
tion
and
publ
icad
min
istr
atio
n ar
ea
Spo
rts
and
athl
etic
s ar
ea
Str
eet a
ndhi
ghw
ay
Tra
de a
nd s
ervi
cear
ea
Place where fall occured
Per
cen
tag
e o
f to
tal
fall
s b
y p
lace
of
occ
ura
nce
Greater Glasgow & Clyde
Greater Glasgow

Number of admissions due to falls in relation the number of medical
conditions diagnosed Number of different conditions that persons aged 65 or more, admitted as the result of a fall in 2008, have had
recorded on previous admissions, Greater Glasgow & Clyde
0
100
200
300
400
500
600
700
800
1 2 3 4 5 6 7 8 9 10
Number of admissions
Nu
mb
er o
f p
atie
nts

Emergency admissions and bed days occupied from falls
Injuries to Hip and Thigh Injuries to the Head
Emergency Admissions for falls(number)
% total adm. for falls
Bed Days(average number)
% total bed days for falls admissions
Emergency Admissions for falls(number)
% total adm. for falls
Bed Days (average number)
% total bed days for falls admissions
Greater Glasgow and Clyde
376 35.6% 33.5 51.1% 178 16.8% 10.5 7.6%
Greater Glasgow 271 36.7 % 32.8 52.6% 128 17.3% 11.7 8.8%

Relationship between emergency admissions and deprivation
Greater Glasgow & ClydeRate per 100,000 persons having had an emergency admission due to a fall in the home, persons aged 65 or
more, 2006
0
100
200
300
400
500
600
1 - Least Deprived 2 3 4 5 - Most Deprived
Deprivation quintile
Rat
e p
er 1
00,0
00 p
op
ula
tio
n

Deaths due to falls by deprivation index
Rate per 100,000 population of deaths in Scotland of people aged 65 or more who died as the result of a fall, 2006
0
10
20
30
40
50
60
70
80
90
1 - LeastDeprived
2 3 4 5 - MostDeprived
1 - LeastDeprived
2 3 4 5 - MostDeprived
Deprivation quintile
Ra
te p
er
10
0,0
00
po
pu
lati
on
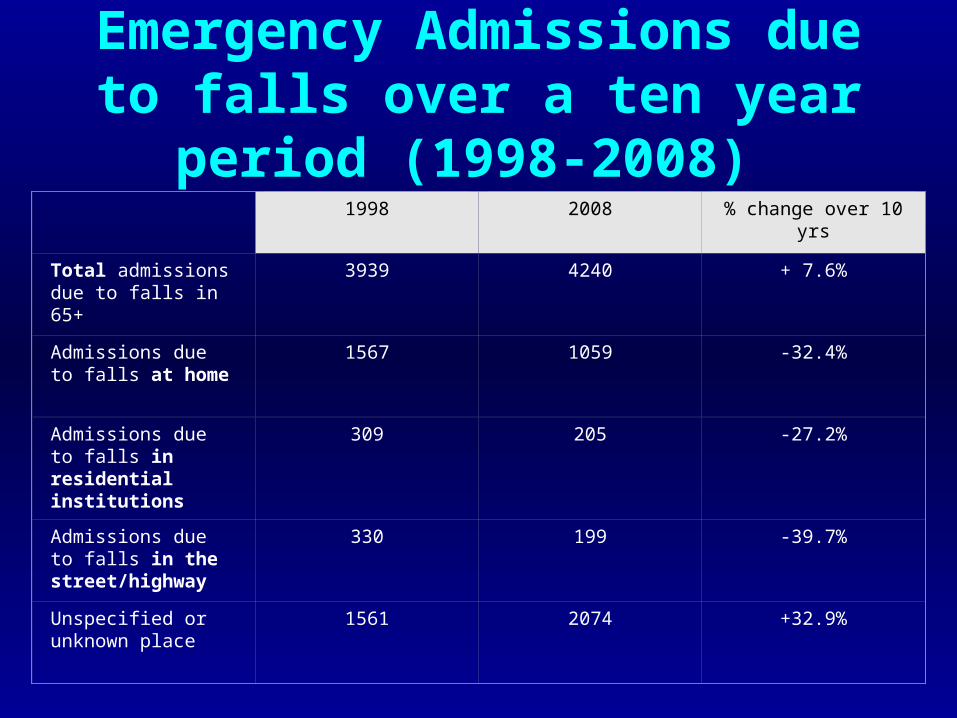
Emergency Admissions due to falls over a ten year period (1998-2008)
1998 2008 % change over 10 yrs
Total admissions due to falls in 65+
3939 4240 + 7.6%
Admissions due to falls at home
1567 1059 -32.4%
Admissions due to falls in residential institutions
309 205 -27.2%
Admissions due to falls in the street/highway
330 199 -39.7%
Unspecified or unknown place
1561 2074 +32.9%

Bed days, emergency admissions and mean stay due to falls in the home in
the 65+ age group 1998-2008 Greater Glasgow Greater Glasgow & Clyde
YearBed
DaysNumber of
admissionsMean Stay
Bed Days
Number of admissions
Mean Stay
1998 34248 1173 29.2 48261 1567 30.8
2008 16909 740 22.9 24624 1059 23.3
% Change 1998 to 2008 -50.6% -36.9% -21.7% -49.0% -32.4% -24.5%
% Change 2005 to 2008 -31.5% -8.5% -25.1% -30.2% -10.5% -22.1%

Number of emergency admissions due to falls in the home
Number of emergency admissions due to falls in the home, Greater Glasgow and Greater Glasgow & Clyde
0
200
400
600
800
1000
1200
1400
1600
1800
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Year of admission
Nu
mb
er o
f em
erg
ency
ad
mis
sio
ns
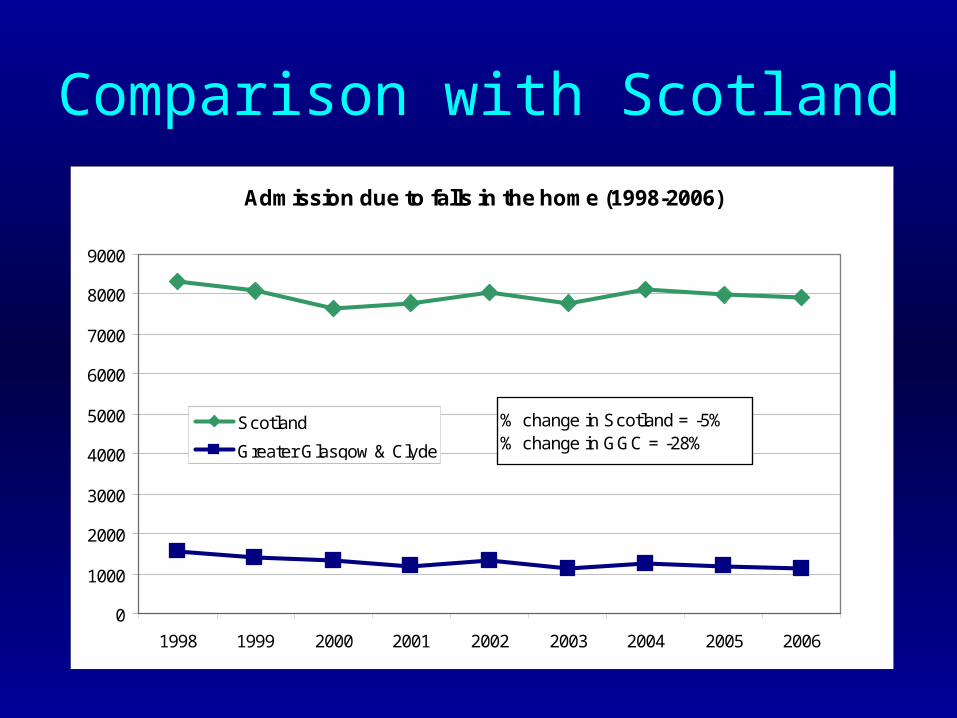
Comparison with Scotland
Admission due to falls in the home (1998-2006)
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
1998 1999 2000 2001 2002 2003 2004 2005 2006
Scotland
Greater Glasgow & Clyde
% change in Scotland = -5% % change in GGC = -28%

Falls Admissions in England related to frailty in over 60 year olds 1999-2008
Codes W00, W01, W04-8, W010, W018-19
0
50,000
100,000
150,000
200,000
250,000
98-99 99-00 00-01 01-02 02-03 03-04 04-05 05-06 06-07 07-08
Growth 5.6% per year

Bed days due to admission for falls in the home Emergency admissions due to falls in the home, aged 65 or over, bed days
0
10000
20000
30000
40000
50000
60000
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Year of admission
Bed
day
s
Greater Glasgow
Greater Glasgow & Clyde

Bed-days in England for frailty related falls in over 60 year olds 1999-2007
Codes W00, W01, W04-8, W010, W018-19
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
98-99 99-00 00-01 01-02 02-03 03-04 04-05 05-06 06-07 07-08
Estimated from proportion of FCEs by age groupGrowth 1.7% per year

Hip fracture admissions in over 65s
Emergency Admissions due to Hip Fractures CodesS.72.0-72.2 (1998-2008) for
0
500
1,000
1,500
2,000
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Greater Glasgow & Clyde
Greater GlasgowNo change –0.4%

Admissions for Hip Fractures in England (ICD S72.0, 72.1 and 72.2)
50,000
52,000
54,000
56,000
58,000
60,000
62,000
64,000
66,000
1998-1999 1999-2000 2000-01 2001-02 2002-03 2003-04 2004-05 2005-06 2006-07 2007-08
Growth 1.8% per year

In a bit more depth…
• CFPP referrals and interventions– Any parts of the process that need work?
• Strength and Balance Interventions– Do they improve balance?– Do they reduce fear of falling, improve balance confidence and
quality of life?– Why do people not necessarily progress from rehab-led to
instructor-led classes?
• Assessment of bone health in Falls Clinics– Can we use a “tool” and not do DEXA scans?

Compared to Other Falls Services
• SDO Report 2007 – services in England– 231 services reported back - median new attendances
p.a = 180 (range 10–1700) at a cost of £32 million! – 116 Community based services
• Average cost £110k• see on average 195 pts p.a
– 110 Acute based services• Average cost £171k • see on average 269 pts p.a
– 5 A&E based services• Average cost £363k • refer on average 1000 pts p.a to GP etc.
• CFPP GGC sees 2652 pts p.a – at unknown cost
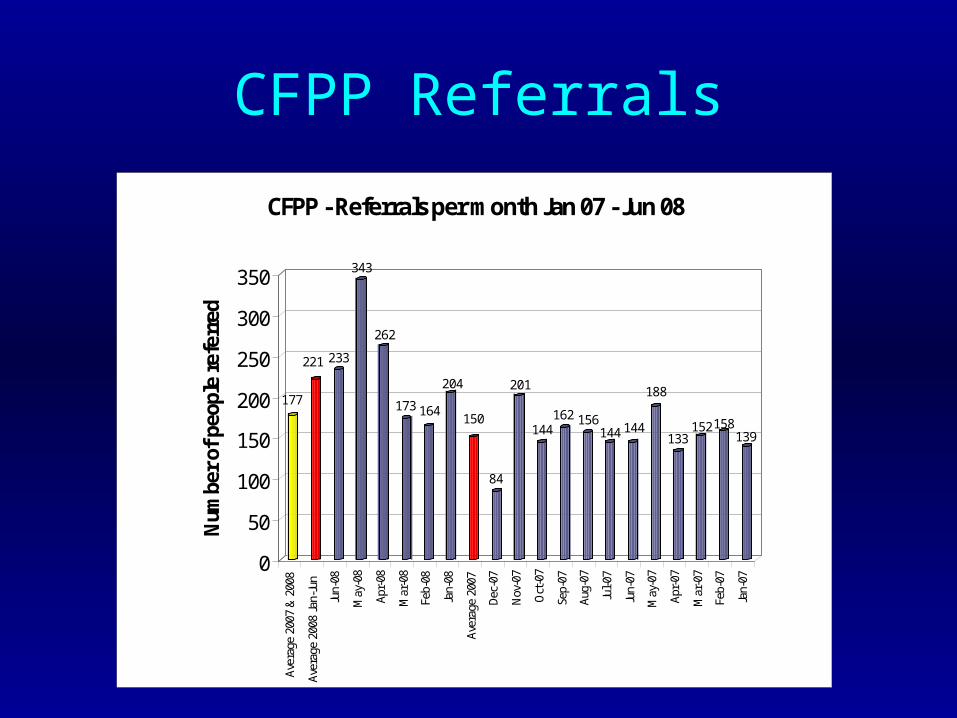
CFPP Referrals
177
221 233
343
262
173 164
204
150
84
201
144162 156
144 144
188
133152158
139
0
50
100
150
200
250
300
350
Num
ber o
f peo
ple
refe
rred
Aver
age
2007
& 2
008
Aver
age
2008
Jan-
Jun
Jun-
08
May
-08
Apr-
08
Mar
-08
Feb-
08
Jan-
08
Aver
age
2007
Dec-
07
Nov
-07
Oct
-07
Sep-
07
Aug-
07
Jul-0
7
Jun-
07
May
-07
Apr-
07
Mar
-07
Feb-
07
Jan-
07
CFPP - Referrals per month Jan 07 - Jun 08
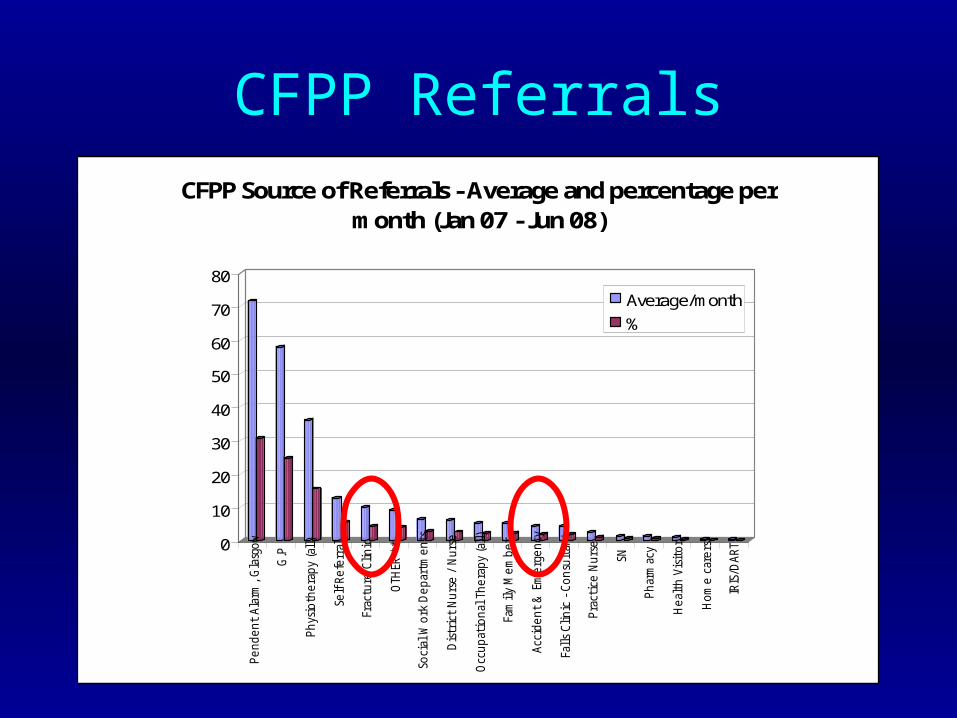
CFPP Referrals
0
10
20
30
40
50
60
70
80P
en
de
nt
Ala
rm,
Gla
sgo
w
G.P
Ph
ysio
the
rap
y (a
ll)
Self
Re
ferr
al
Frac
ture
Cli
nic
OTH
ER *
*
Soci
al W
ork
De
par
tme
nts
Dis
tric
t N
urs
e /
Nu
rse
Occ
up
atio
nal
Th
era
py
(all
)
Fam
ily
Me
mb
er
Acc
ide
nt
& E
me
rge
ncy
Fall
s C
lin
ic -
Co
nsu
ltan
t
Pra
ctice
Nu
rse
SN
Ph
arm
acy
He
alth
Vis
ito
r
Ho
me
car
ers
IRIS
/DA
RT
CFPP Source of Referrals - Average and percentage per month (Jan 07 - Jun 08)
Average/month%

Audit (July-Sept 2008) of A & E attendee’s at
the SGH
32% of all A & E attendee’s over the
age of 65 have had a fall
65 had had a fracture and half of these had
a history of falls
2 were referred to the CFPP direct from A&E!
709Over 65’s
presenting to A+E
227 falls
482Not fall related
6 Admitted or
already inpatient
221 outpatient falls
(Potential referrals to community falls team)
65 #Mean age 68yrs
Median age 76yrs
159 non #
34 History of falls
(18 with previous #)
311st fall
91History of falls
681st fall
66 ♂ (74.9 yrs)
155♀ (77.6yrs)
3 falls with multiple injury
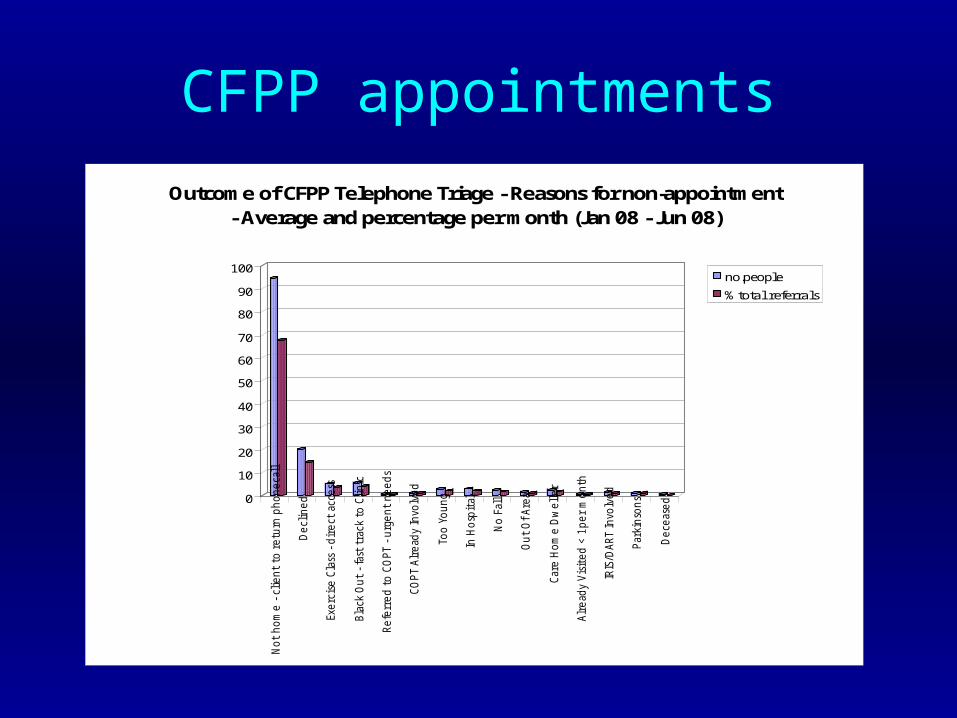
CFPP appointments
0
10
20
30
40
50
60
70
80
90
100N
ot
ho
me
- c
lie
nt
to r
etu
rn p
ho
ne
call
De
clin
ed
Exe
rcis
e C
lass
- d
ire
ct a
cce
ss
Bla
ck O
ut
- fa
st t
rack
to
Cli
nic
Re
ferr
ed
to
CO
PT
- u
rge
nt
ne
ed
s
CO
PT
Alr
ead
y In
volv
ed
Too
Yo
un
g
In H
osp
ital
No
Fal
l
Ou
t O
f A
rea
Car
e H
om
e D
we
lle
r
Alr
ead
y V
isit
ed
< 1
pe
r m
on
th
IRIS
/DA
RT
Invo
lve
d
Par
kin
son
s
De
ceas
ed
Outcome of CFPP Telephone Triage - Reasons for non-appointment - Average and percentage per month (Jan 08 - Jun 08)
no.people
% total referrals
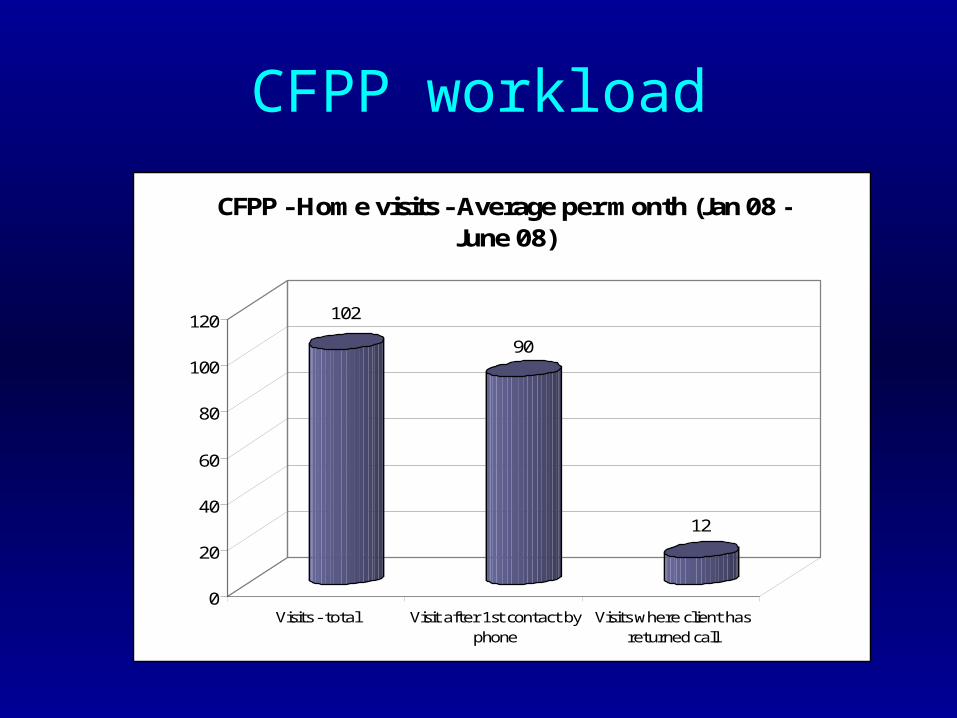
CFPP workload
102
90
12
0
20
40
60
80
100
120
Visits - total Visit after 1st contact byphone
Visits where client hasreturned call
CFPP - Home visits - Average per month (Jan 08 - June 08)
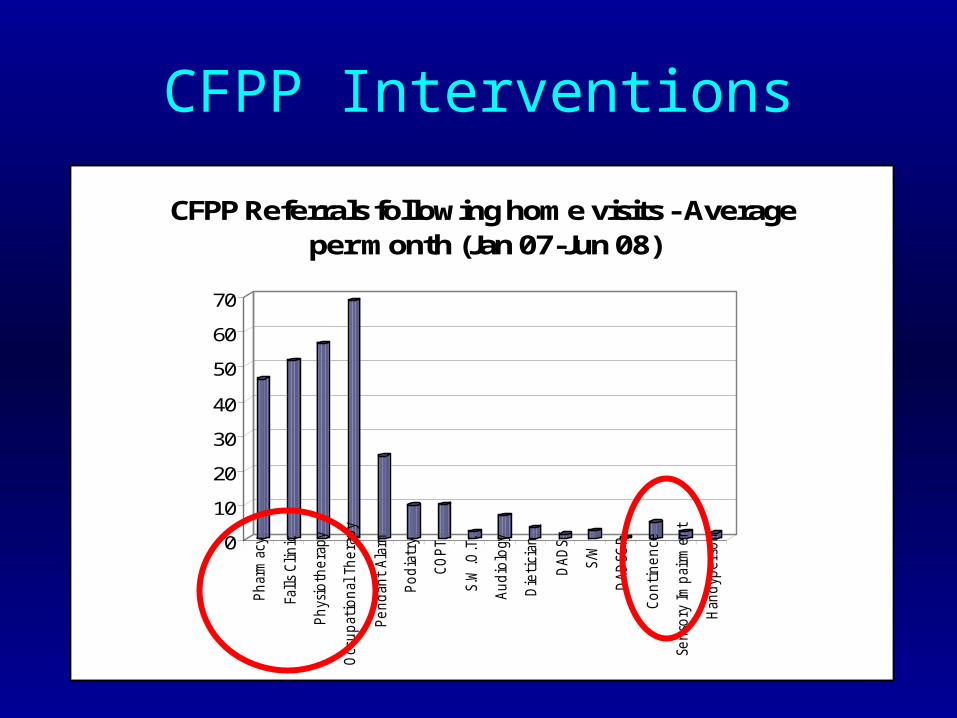
CFPP Interventions
0
10
20
30
40
50
60
70
Ph
arm
acy
Fall
s C
lin
ic
Ph
ysio
the
rap
y
Occ
up
atio
nal
Th
era
py
Pe
nd
ant
Ala
rm
Po
dia
try
CO
PT
S.W
.O.T
.
Au
dio
logy
Die
tici
an
DA
DS
S/W
DA
DSG
P
Co
nti
ne
nce
Sen
sory
Im
pai
rme
nt
Han
dyp
ers
on
CFPP Referrals following home visits - Average per month (Jan 07-Jun 08)

0
10
20
30
40
50
60
70
80
90
100
Home Visit Triggered Interventions - % of clients

Physiotherapy Intervention
• 12 Strength & Balance Classes • Classes locally delivered• Free transport service (70% utilise)• 12-18 week attendance• Home Exercises• Partnership working with Day hospital and
Leisure services (Glasgow Culture & Sport)
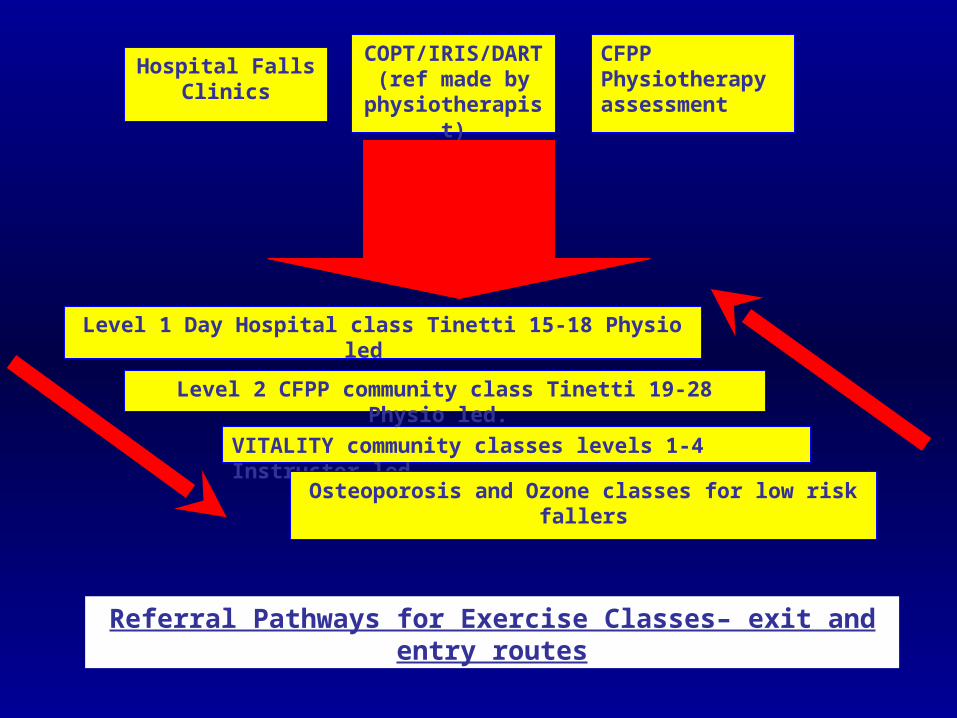
Hospital Falls Clinics
COPT/IRIS/DART (ref made by
physiotherapist)
CFPP Physiotherapy assessment
Level 1 Day Hospital class Tinetti 15-18 Physio led
VITALITY community classes levels 1-4 Instructor led
Level 2 CFPP community class Tinetti 19-28 Physio led.
Osteoporosis and Ozone classes for low risk fallers
Referral Pathways for Exercise Classes– exit and entry routes

Strength & Balance Programmes
• Evidence based exercises– (Skelton 2005; Robertson 2001; Campbell 1999)
• Evidence based “deliverers”– Physiotherapists and trained Postural Stability
Instructors (Skelton 2004)
• Evidence based duration– Dose of 50 hours of balance challenging
exercise (Sherrington 2008)


Attendance at classes
277
17 15
245
0
50
100
150
200
250
300
Number of people
Total
atten
dees/m
onth
New Patients
Assesse
d at C
FPP
New Patients
Starti
ng Class
Regular a
ttendees
CFPP Exercise Class Attendance- average per month citywide 2007

Evaluation of effect• N= 274 clients considered over a time period in 2007.• Attended on average 11.9 (sd 3.8) weeks• Outcome measures:
– Duration of attendance– Functional tests
• Tinetti Mobility and Balance Score• Timed Up and Go• 180 degree turn• Functional Reach• Confidence in Maintaining Balance• Tinetti’s Falls Efficacy Scale (FES)
– Patient Satisfaction Questionnaires (N=91)
• Same assessor throughout - not all tests completed on all clients

Outcome measures
Test
Mean (sd)
Number of clients
Before exercise sessions
After exercise sessions
P-value
Tinetti Balance Score
274 23.1 (3.3) 24.8 (3.1) 0.000
180 deg turn (deg) 253 5.5 (1.9) 5.0 (1.6) 0.000Functional Reach (cm)
112 19.2 (5.9) 20.9 (6.9) 0.000
TUAG (sec) 137 18.6 (6.7) 16.3 (5.9) 0.000ConFBal 162 19.4 (3.9) 16.9 (3.4) 0.000Tinetti FES 43 29.3 (16.5) 21.5 (11.6) 0.0002

Balance improvements are duration dependent
• The Tinetti Mobility and Balance Score showed considerable improvement, but the change was dependent on duration of exercise attendance.
• Those attendees that drop out of sessions before 12 weeks are unlikely to see clinically significant changes in their balance.
• This is in line with the recent systematic review of exercise (Sherrington et al. 2008) where a dose of at less than 50 hours confers little benefit to fall risk reduction.

Client Satisfaction
• Satisfaction forms at week 10 of their exercise programme (n=117 issued).
• 91 patients returned the forms (response rate 78%). • 85% had received information about the class before the sessions
started and most (83%) found the pre-class information useful. • Only 1% thought the class was not in a suitable location; the staffs
were not helpful; the exercises were rushed, too short or not well explained (showing a high degree of satisfaction with facilities and delivery).
• 98% felt the exercise classes were beneficial and 94% thought the sessions were good or very good.
• Open response questions showed good improvements to wellbeing (see next slide) however, many people just wrote “enjoyed” in this section!

Open responses to feedback
Open responses to any improvements felt as a result of exercise sessions (n=91)
0
5
10
15
20
25
30
35
Improvement/Benefit
Nu
mb
er o
f p
atie
nts
Confidence /wellbeing / mood
Balance
Walking / stamina /fitness / mobility
Strength / muscletone
Social benefits
Flexibility
Summary
• The CFPP exercise service to prevent falls in Glasgow does improve many of the known risk factors for falls
• The benefits are duration dependent – clients should be encouraged to adhere for at least 12 weeks,
ideally to the maximum 18 weeks and then to move into normal community exercise sessions for older people to maintain the improvements
• High degree of client satisfaction (though questionnaire could have been designed better)

WHAT ARE THE EFFECTS OF THE GGC FALLS EXERCISE
SESSIONS ON FEAR OF FALLING, BALANCE CONFIDENCE AND
QUALITY OF LIFE IN GLASWEGIAN FALLERS?
Gaynor McGrath
MSc Rehabilitation Science
Glasgow Caledonian University
Submitted Oct 2009
Aims and Methods
• Objectives: To examine whether a 12 week strength and balance exercise class improved an individual’s perception of their fear of falling, balance confidence and quality of life and whether there was an inter-relationship between outcome measures pre and post the exercise intervention.
• Methods: Prospective cohort study. • Participants: Female fallers (n=13) aged >=65 years
• Questionnaires specific to fear of falling (SFES-I), balance confidence (CONFbal) and quality of life (SF-12) were completed prior to and on completion of the 12 week exercise intervention.

Results and Conclusion
• Results: following completion of the 12 week exercise intervention there was a significant reduction in fear of falling (p<0.05) together with a significant improvement in balance confidence (p<0.05) and quality of life (p<0.05). However, the only significant inter-relationship between outcome measures was between fear of falling and balance confidence post exercise intervention (p<0.05).
• Conclusion: An exercise intervention is effective in reducing fear of falling
whilst improving balance confidence and quality of life in community dwelling older females 65 years and older. It also improves the inter-relationship between fear of falling and balance confidence post intervention.

WHAT ARE OLDER PEOPLE’S VIEWS ON THEIR FORTHCOMING
TRANSITION BETWEEN THE PHYSIOTHERAPY-LED FALLS
PREVENTION EXERCISE CLASS AND THE INSTRUCTOR-LED
FALLS PREVENTION EXERCISE CLASS?
Aisling O’Connor
MSc Rehabilitation Science
Glasgow Caledonian University
31st January 2009

Falls Intervention Programme
• GG & C – tiered exercise programme: Physiotherapist-led community class (12-18 weeks)
Postural Stability Instructor (PSI)-led class
Benefits of Falls Prevention Exercise Programmes (Hauer et al., 2003; Skelton et al., 1995; Narici et al., 2004; Mazzeo & Tanaka, 2001)
Exercise intervention greater than 6 months in duration is necessary (Skelton, 2007).
PSI-led class: low uptake & high drop-out rates
Aims
• Explore older people’s views on falls exercise classes
• Transition from physiotherapist-led classes to PSI-led
classes
• Motivators & Barriers to the uptake and adherence
• Increase attendance rates at PSI-led classes

Methods – Qualitative Research
• Design: Principles of grounded theory.
• Sample: 5 participants from physiotherapist-led class (saturation point reached)
• Recruitment: Visit by researcher to classes
• Data Collection: Semi-structured interviews: 7 open questions
• Analysis of data: Transcription of interviews- Open coding >> axial coding >> selective coding (+ memo writing)
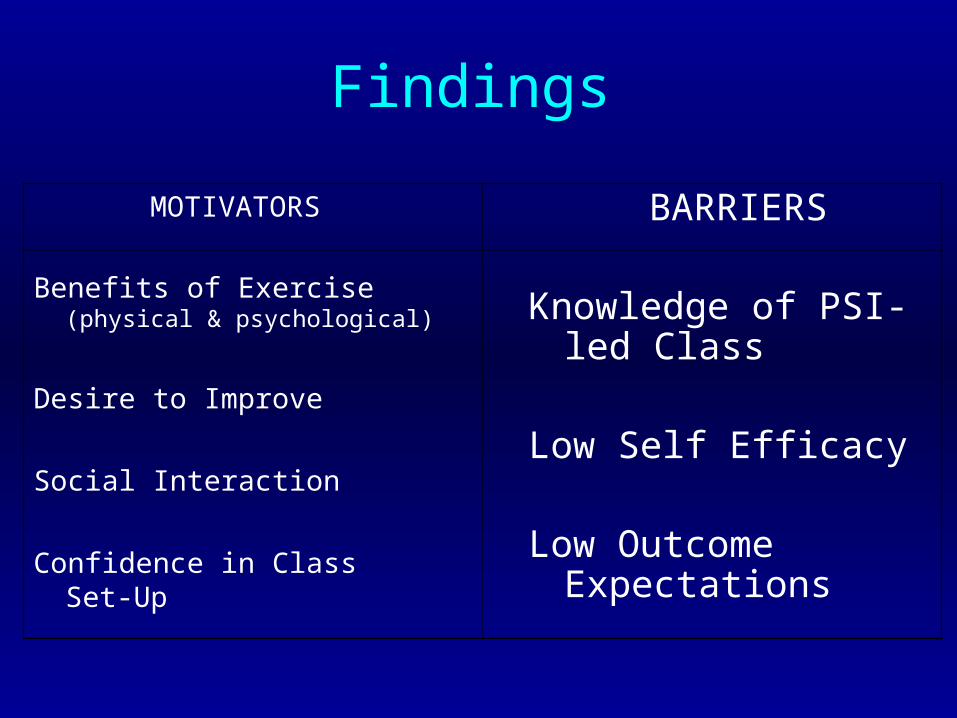
Findings
MOTIVATORS
Benefits of Exercise (physical & psychological)
Desire to Improve
Social Interaction
Confidence in Class Set-Up
BARRIERS
Knowledge of PSI-led Class
Low Self Efficacy
Low Outcome Expectations

New themes.…Motivator
CONFIDENCE IN CLASS SET-UP
- Not previously discussed in the literature
- “...But I mean these people, whether it’s this class or the next advanced class, presumably they are experts in their own field.” (P4, pg.10, L358-360)

New themes….Barrier
KNOWLEDGE OF PSI-LED CLASS
Not previously discussed in the literature
“…What’s this other class?” (P1, pg.1, L5-6)
“...What time would it be?” (P2, pg.3, L109)
“...Where would I have to go in the first place?”(P5, pg.11, L419)

Clinical Implications
• Lack of knowledge of PSI-led classes
• Increase awareness of Falls Prevention Services
- booklet?
- DVD?
- reinforce information every week?
• Essential if attendance rates at PSI-led classes are to be increased and the risk of falling reduced

Future Research…
• …on the transition between classes with larger sample sizes
& bigger geographical area
• …strategies to encourage older people with low self efficacy
But most importantly…
• Effective strategy to inform older people of their options
within Falls Prevention Programmes urgently needed!
How useful is the fracture Risk Assessment Tool (FRAX) in a falls
clinic population?
McCarthy C, Skelton DA, Gallacher S, Mitchell LE
Abstract presented at 10th National Conference on Postural Stability and Falls, Blackpool, 07/09/09

So what about case finding for bone fragility?
Used to determine 10 year fracture risk in community dwelling adults – then NOGG suggests guidance on treatment

NOGG Advice based on FRAX
Research Questions
• What are the implications of using FRAX / NOGG in a falls clinic Setting?
• Can they identify those patients who would benefit from BMD assessment?
• Can they be used to determine treatment without the use of DEXA?

Methods
• 44 consecutive patients (33 F) attending a falls clinic– Mean age 78.0 (sd 6.0) years
• BMD measured – Lunar Prodigy, L2-L4 and neck of femur
• FRAX and NOGG assessed• Statistics
– Sensitivity, specificity, negative predictive values, positive predictive value, false negative and false positive rate for each FRAX cut off and NOGG advice to treat or not – before and after BMD measurement

Demographic Results
• After DEXA– Total 29.5% (n=13) had Osteoporosis (T < -2.5)– 4 at hip and spine, 1 at spine alone, 8 at hip alone – A further 47% (n=21) had Osteopenia at spine and/or hip (T < -1)
Mean St Dev
Tinetti (score) 20.2 5.4
TUG (sec) 19.7 8.1
FRAX score major OP (%)
17.2 8.6
FRAX score hip (%) 7.8 5.9
BMD at Spine -0.5 1.8
BMD at hip -1.7 1.1

Results pre-DEXA
• NOGG advice (DEXA or treat) followed:
– 46% (n=6) of those with OP at either spine and/or hip would not be treated or advised a DEXA
– Of those where DEXA was advised (n=18), 72% did not have osteoporosis (n=13)
– Treatment advised in 2 patients both of whom had osteoporosis on subsequent DEXA

FRAX and NOGG not good in falls clinic at predicting need for DEXA and treatment
Pre-FRAX
NOGG
Advice
Sensitivity
%
Specificity
%
NPV
%
PPV
%
FP
%
FN
%
DXA advised
and has OP53.9 58.1 75.0 35.0 41.9 46.2
DXA advised
and has OP or OS
42.9 55.6 20.0 79.0 44.4 57.1
The Benefits
• ‘Loss leader’ that has led to a strong relationship– Access and willingness to work on research within
various parts of the service• Masters students data projects x 2 • 2 large NIHR outline bids, dementia and physical activity,
visual impairment and falls
– Memorandum of Agreement to increase research capacity within Specialist Registrars
• Footwear and balance in wards• FRAX and BMD in Falls Clinic Attenders