An Assessment of Cardiovascular Risks of a Low ......David Diamond, Ph.D. Departments of Psychology,...
58
David Diamond, Ph.D. Departments of Psychology, Molecular Pharmacology and Physiology USF Neuroscience Collaborative University of South Florida Tampa, Florida, USA An Assessment of Cardiovascular Risks of a Low Carbohydrate, High Fat Diet
Transcript of An Assessment of Cardiovascular Risks of a Low ......David Diamond, Ph.D. Departments of Psychology,...

David Diamond, Ph.D.
Departments of Psychology, Molecular Pharmacology and Physiology
USF Neuroscience Collaborative
University of South Florida
Tampa, Florida, USA
An Assessment of Cardiovascular Risks of a Low
Carbohydrate, High Fat Diet
David Diamond, Ph.D.
Departments of Psychology, Molecular Pharmacology and Physiology
USF Neuroscience Collaborative
University of South Florida
Tampa, Florida, USA
An Assessment of Cardiovascular Risks of a Low
Carbohydrate, High Fat Diet
Low Carb Diet-Induced
Increase in LDL
The Ultimate Bogeyman

Disclosure #1: 1997 – 2007
My High TG and Low HDL Carried the Highest Risk for a Heart Attack
Relative Risk
of MI
Low TG
High HDL
High TG
Low HDL
0
3
6
9
12
15
18

Disclosure 2: My sources of information on diet, cholesterol and
cardiovascular disease
Gary Taubes* Nina Teicholz*, Jimmy Moore*
Ivor Cummins* Ann Childers Cate Shanahan*
Uffe Ravnskov* Paul Rosch* Jeff Volek*
Stephanie Seneff* Carlos Monteiro* Barry Groves*
Luca Mascitelli* Richard Feinman* Michel De Lorgeril*
Malcolm Kendrick* Kevin Kip* Aseem Malhotra*
Sherif Sultan* David Brownstein* Harumi Okuyama*
Douglas Schocken* Paul Leaverton* Joel Kauffman*
Barry Groves* James DiNicolantonio* Abdullah Alabdulgader*
Zoe Harcombe* Eric Westman* Gary/Belinda Fettke*
Tim Noakes* Tom Naughton* Andreas Eenfeldt*
Kilmer McCully* David Ludwig* Sarah Hallberg*
Robert Lustig* Robert DuBroff* Anthony Colpo*
William Davis Bruce Fife Fred Kummerow
Nicolai Worm* Edward H. Ahrens Mark Cucuzella*
Colin Champ Alana/Peter Langsjoen* Maryanne Demasi*
John Abramson John Yudkin Steve Phinney
Beatrice Golomb Marcia Angell Sally Fallon/Mary Enig
Rita Redberg Jason Fung Hussein Dashti
George Mann Verner Wheelock Maria Luz Fernandez
Robert Atkins Jay Wortman Georgia Ede*
Dwight Lundell David Perlmutter Marika Sboros
Mark Hyman Dave Feldman* Jeff Gerber*
Michael Eades Ted Naiman Amber O’Hearn

Disclosure 3: My Neuroscience Research Program (1978 – Present)
Support: Dept. of Veterans Affairs, Navy, NIH, DoD, NSF, Drug Companies
Diet/Cardiovascular Disease Research: Unfunded
Gary Taubes* Nina Teicholz*, Jimmy Moore*
Ivor Cummins* Ann Childers Cate Shanahan*
Uffe Ravnskov* Paul Rosch* Jeff Volek*
Stephanie Seneff* Carlos Monteiro* Barry Groves*
Luca Mascitelli* Richard Feinman* Michel De Lorgeril*
Malcolm Kendrick* Kevin Kip* Aseem Malhotra*
Sherif Sultan* David Brownstein* Harumi Okuyama*
Douglas Schocken* Paul Leaverton* Joel Kauffman*
Barry Groves* James DiNicolantonio* Abdullah Alabdulgader*
Zoe Harcombe* Eric Westman* Gary/Belinda Fettke*
Tim Noakes* Tom Naughton* Andreas Eenfeldt*
Kilmer McCully* David Ludwig* Sarah Hallberg*
Robert Lustig* Robert DuBroff* Anthony Colpo*
William Davis Bruce Fife Fred Kummerow
Nicolai Worm* Edward H. Ahrens Mark Cucuzella*
Colin Champ Alana/Peter Langsjoen* Maryanne Demasi*
John Abramson John Yudkin Steve Phinney
Beatrice Golomb Marcia Angell Sally Fallon/Mary Enig
Rita Redberg Jason Fung Hussein Dashti
George Mann Verner Wheelock Maria Luz Fernandez
Robert Atkins Jay Wortman Georgia Ede*
Dwight Lundell David Perlmutter Marika Sboros
Mark Hyman Dave Feldman* Jeff Gerber*
Michael Eades Ted Naiman Amber O’Hearn
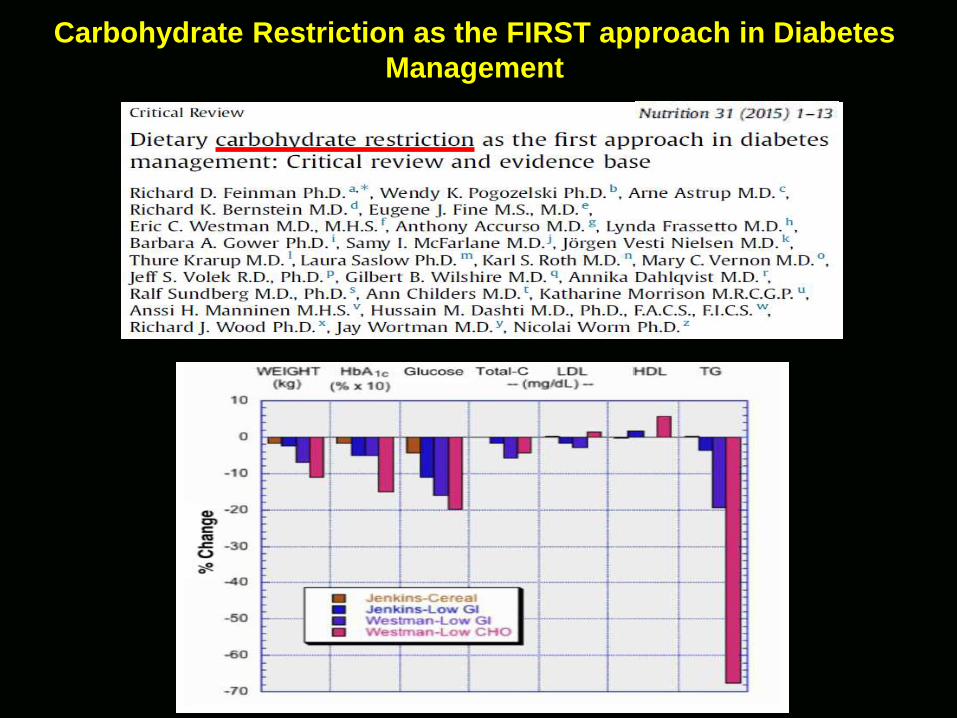
Carbohydrate Restriction as the FIRST approach in Diabetes
Management

The Elephant in the Conference Room: Even a Small Increase in
LDL (Bad Cholesterol) Increases One’s Risk of a Heart Attack
You lost weight, lowered your
BP/TGs, increased your HDL, but I’m worried about your
LDL

“saturated fat … increases blood cholesterol, damages arteries
and leads to coronary disease.”
Ancel Keys, 1961
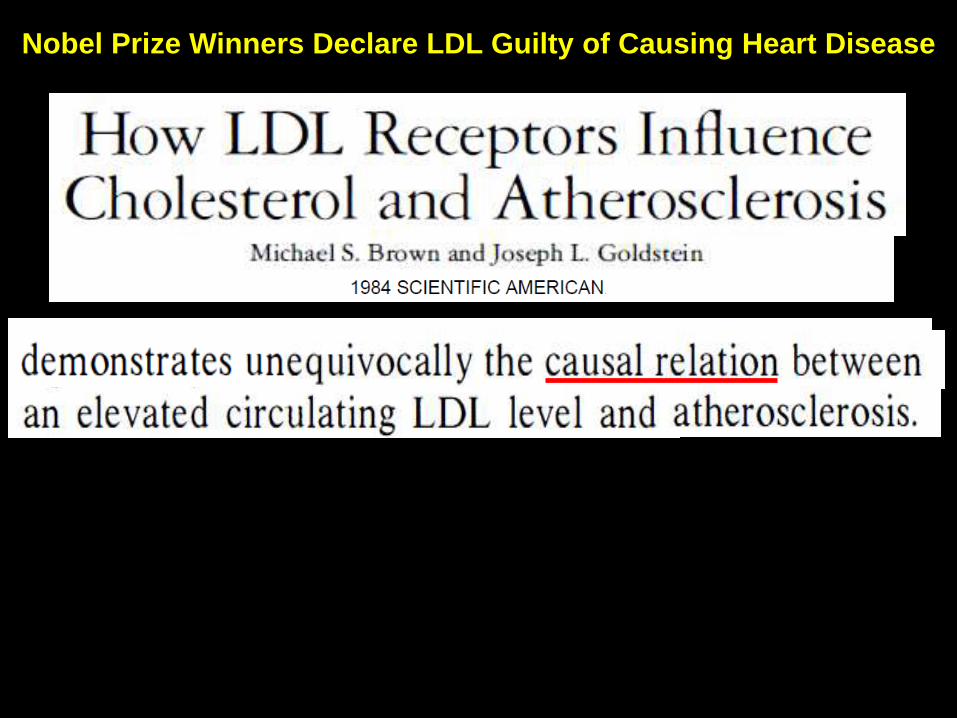
Nobel Prize Winners Declare LDL Guilty of Causing Heart Disease

Serum Cholesterol (mg/dl)
150 175 187 198 208 216 226 238 243 > 2900.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
Relative Risk
of Death from
CHD
Serum Cholesterol (mg/dl)
150 175 187 198 208 216 226 238 243 > 2900.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
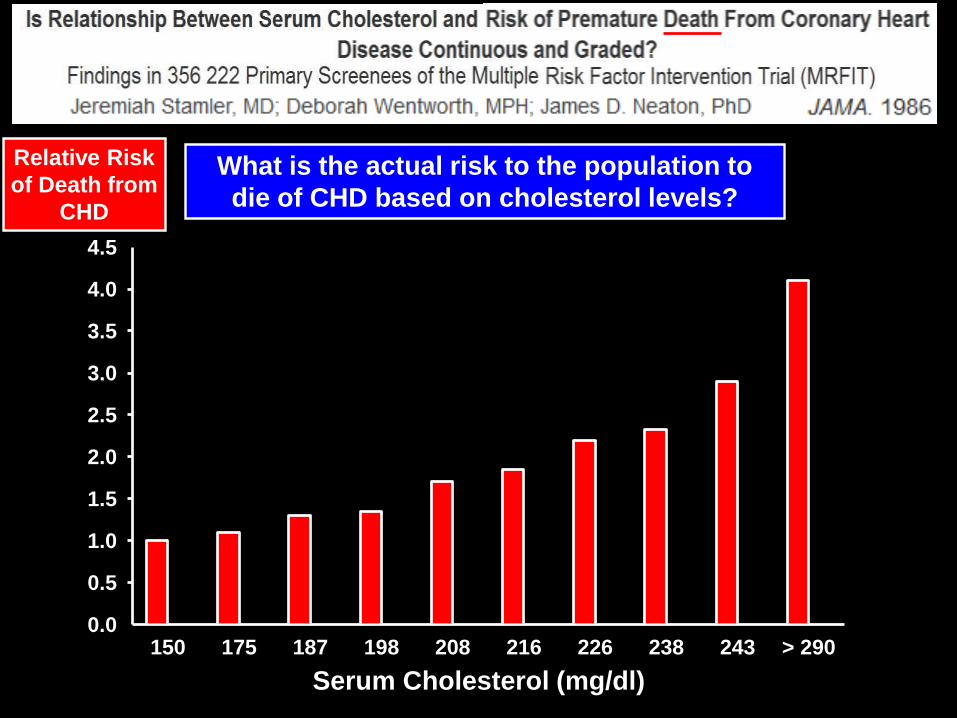
What is the actual risk to the population to
die of CHD based on cholesterol levels?
Relative Risk
of Death from
CHD
Serum Cholesterol (mg/dl)
150 175 187 198 208 216 226 238 243 > 2900.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
What is the actual risk to the population to
die of CHD based on cholesterol levels?
150 175 187 198 208 216 226 238 243 > 2900.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
0
20
40
60
80
100
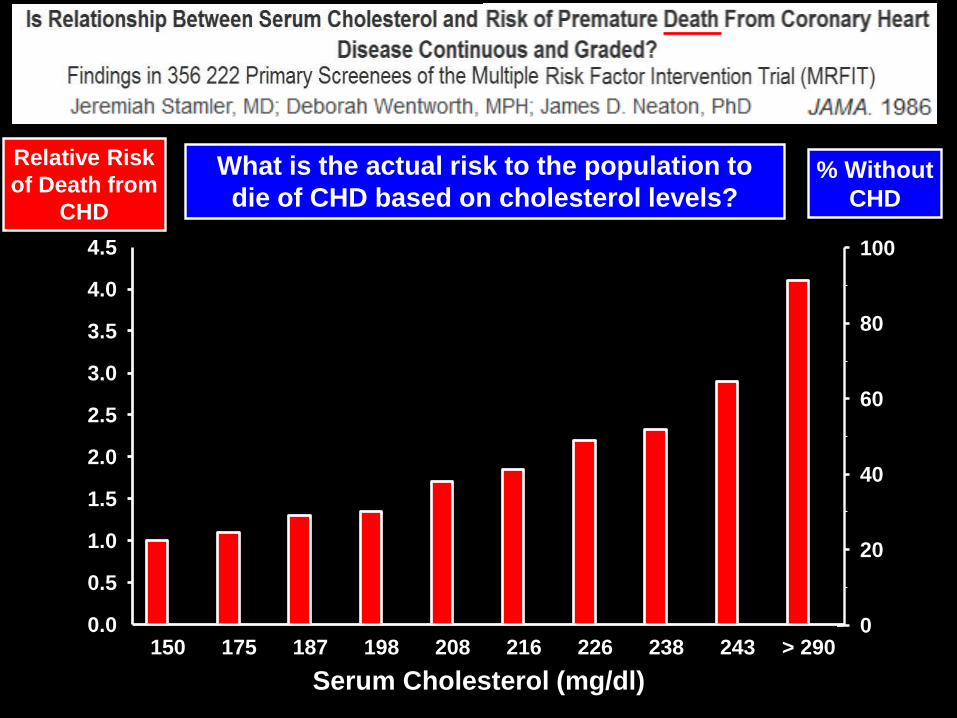
% Without
CHD
Relative Risk
of Death from
CHD

Serum Cholesterol (mg/dl)
% Without
CHD
150 175 187 198 208 216 226 238 243 > 2900.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
0
20
40
60
80
100
What is the actual risk to the population to
die of CHD based on cholesterol levels?
Relative Risk
of Death from
CHD

Serum Cholesterol (mg/dl)
% Without
CHD
150 175 187 198 208 216 226 238 243 > 2900.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
0
20
40
60
80
100
What is the actual risk to the population to
die of CHD based on cholesterol levels?
Relative Risk
of Death from
CHD
Serum Cholesterol (mg/dl)
150 175 187 198 208 216 226 238 243 > 2900.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
0
20
40
60
80
100
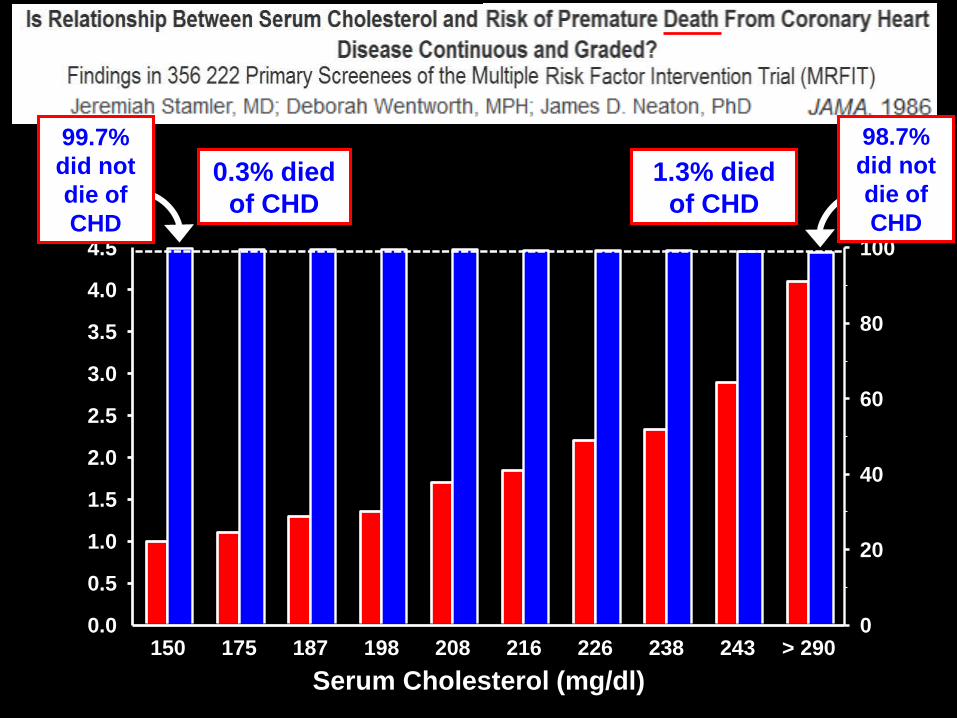
98.7%
did not
die of
CHD
99.7%
did not
die of
CHD
0.3% died
of CHD
1.3% died
of CHD

Serum Cholesterol (mg/dl)
150 175 187 198 208 216 226 238 243 > 2900.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
0
20
40
60
80
100
98.7%
did not
die of
CHD
99.7%
did not
die of
CHD
1.3/0.3 = 4.13
>400% Increase
in Deaths
0.3% died
of CHD
1.3% died
of CHD
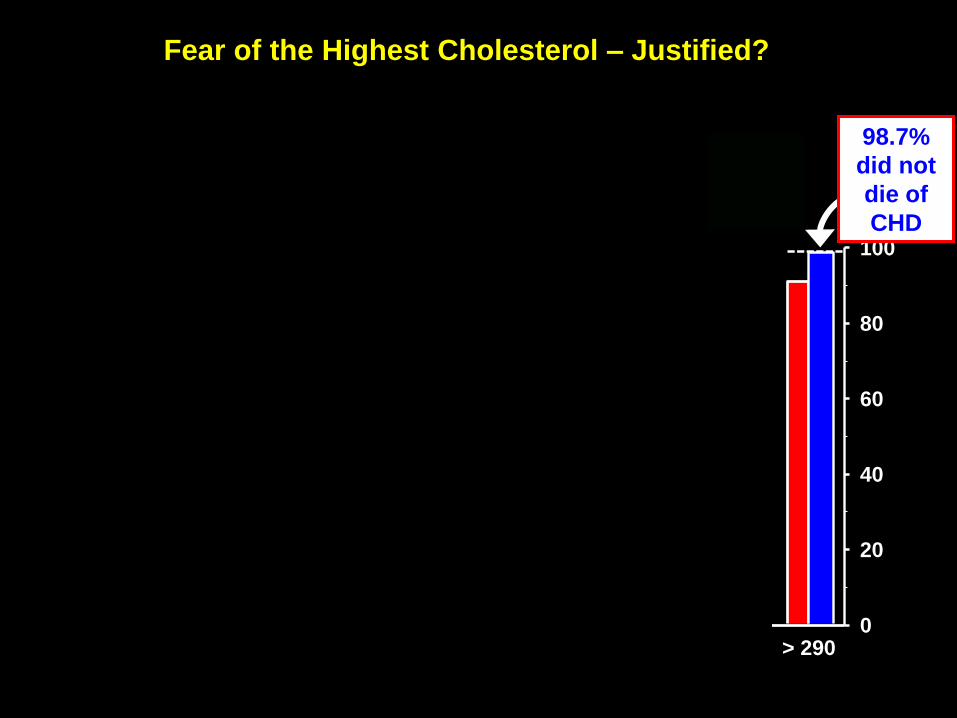
Fear of the Highest Cholesterol – Justified?
150 175 187 198 208 216 226 238 243 > 2900.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
0
20
40
60
80
100
98.7%
did not
die of
CHD

Familial Hypercholesterolemia:
An Inevitable Early Coronary Death Sentence?

Tests of the Hypothesis That Cholesterol Causes Atherosclerosis
1 – There should be a high rate of premature death in people
with Familial Hypercholesterolemia
2 – Pharmacological reduction of cholesterol should reduce
the rate of coronary events and mortality
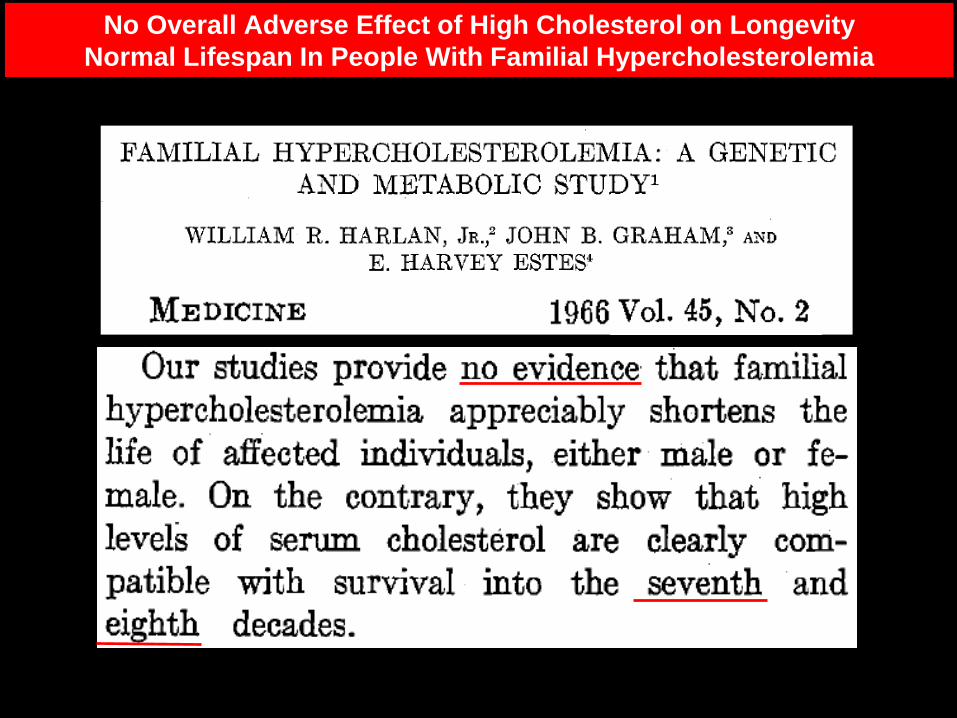
No Overall Adverse Effect of High Cholesterol on Longevity
Normal Lifespan In People With Familial Hypercholesterolemia
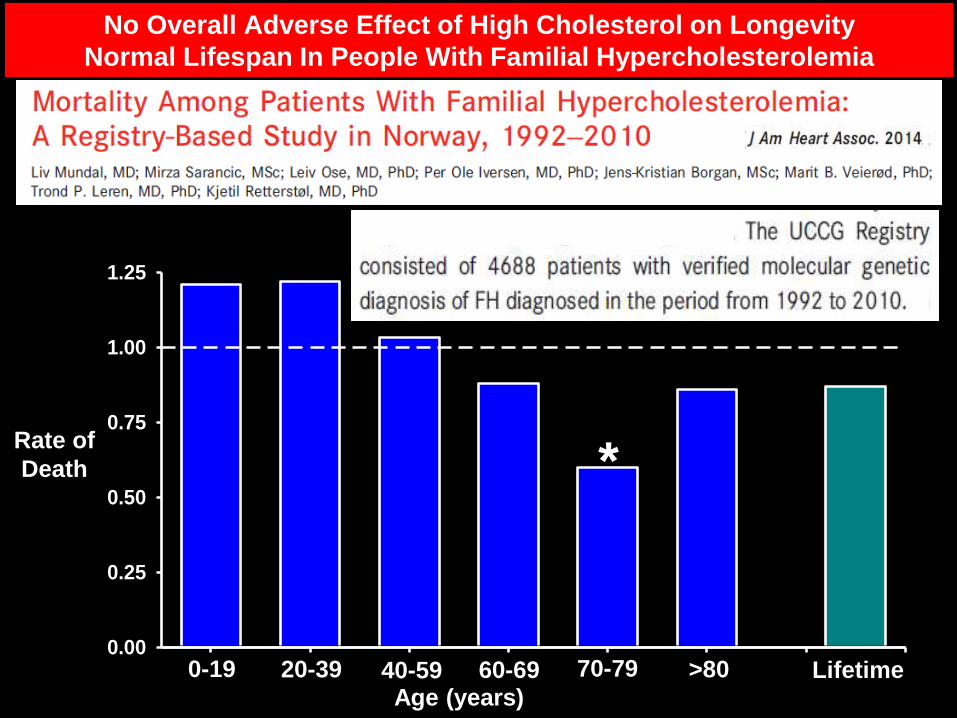
No Overall Adverse Effect of High Cholesterol on Longevity
Normal Lifespan In People With Familial Hypercholesterolemia
0-19 20-39 40-59 60-69 70-79 >80 Lifetime0.00
0.25
0.50
0.75
1.00
1.25
Age (years)
Rate of
Death *

0-19 20-39 40-59 60-69 70-79 >80 Lifetime0.00
0.25
0.50
0.75
1.00
1.25
No Overall Adverse Effect of High Cholesterol on Longevity
Normal Lifespan In People With Familial Hypercholesterolemia
Age (years)
Rate of
Death *

Higher LDL is Associated with Equal or Greater Longevity
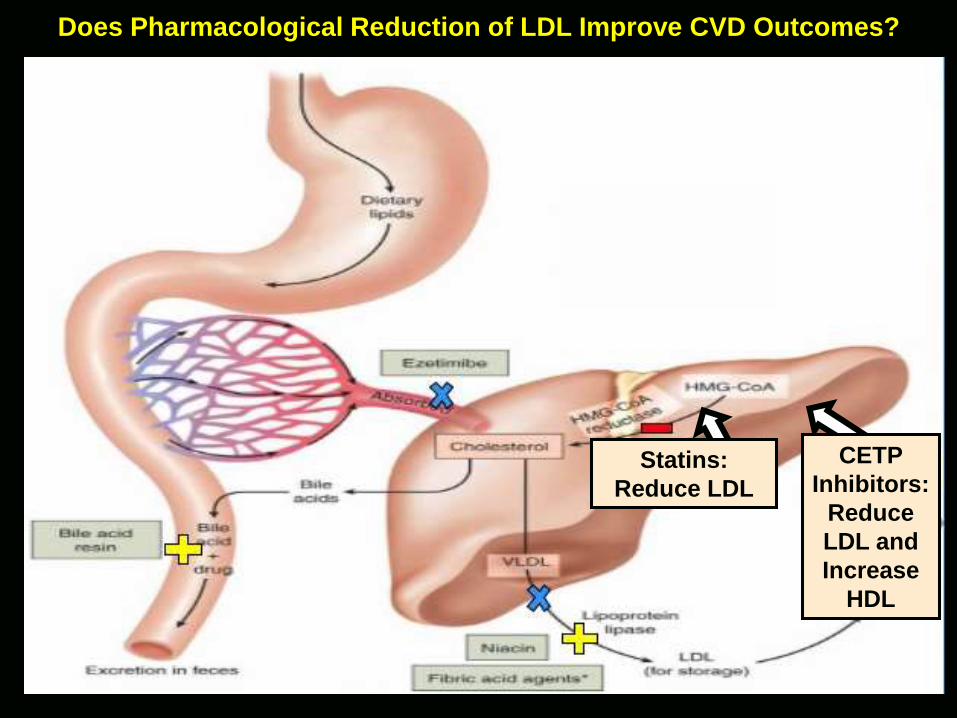
Does Pharmacological Reduction of LDL Improve CVD Outcomes?
Statins:
Reduce LDL
CETP
Inhibitors:
Reduce
LDL and
Increase
HDL
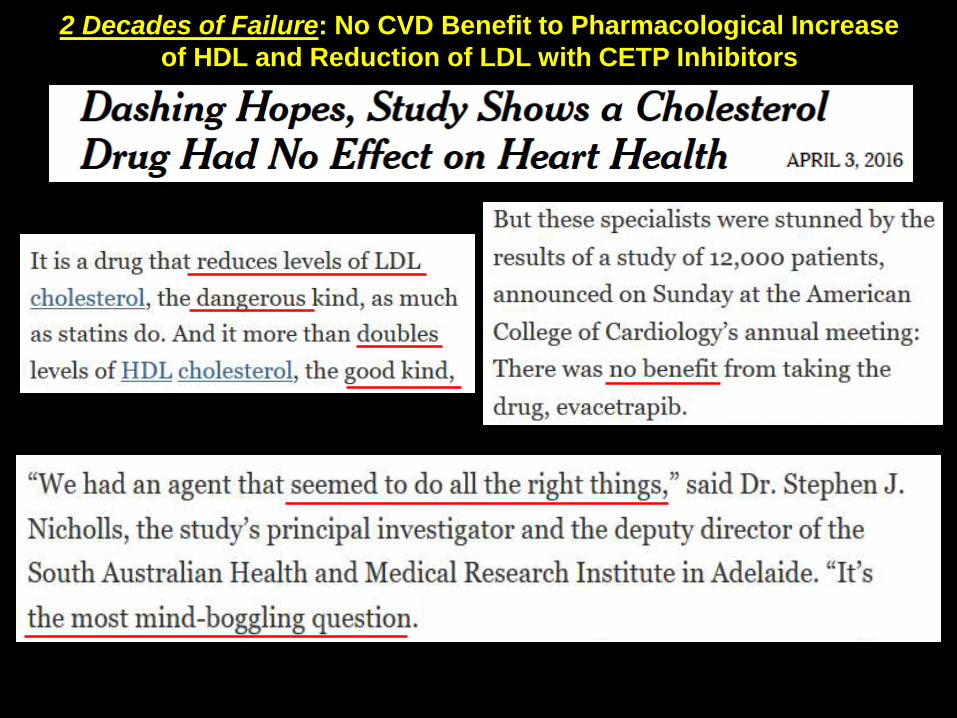
2 Decades of Failure: No CVD Benefit to Pharmacological Increase
of HDL and Reduction of LDL with CETP Inhibitors
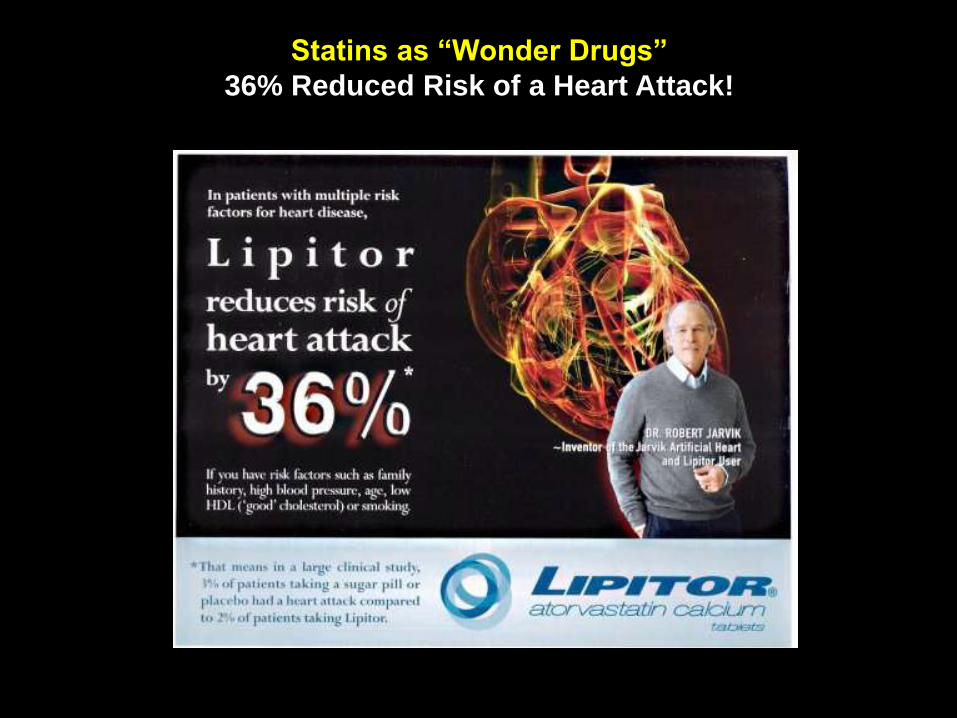
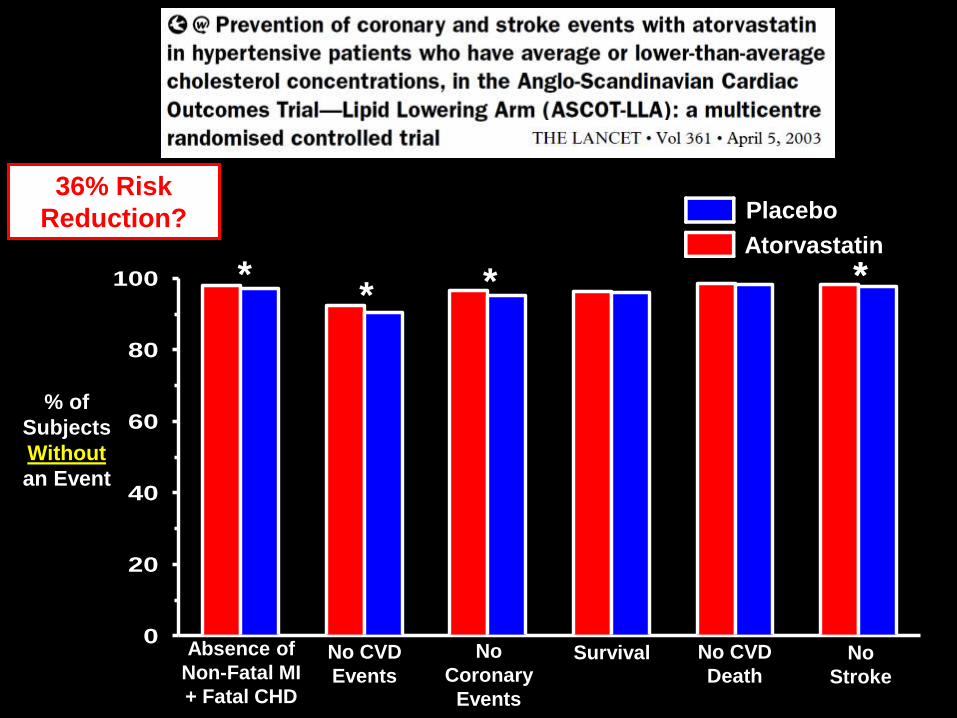
Statins as “Wonder Drugs”
36% Reduced Risk of a Heart Attack!

* * *
0
20
40
60
80
100
% of
Subjects
Without
an Event
*
No
Stroke
No CVD
DeathSurvivalNo
Coronary
Events
No CVD
Events
*
Placebo
Atorvastatin
Absence of
Non-Fatal MI
+ Fatal CHD
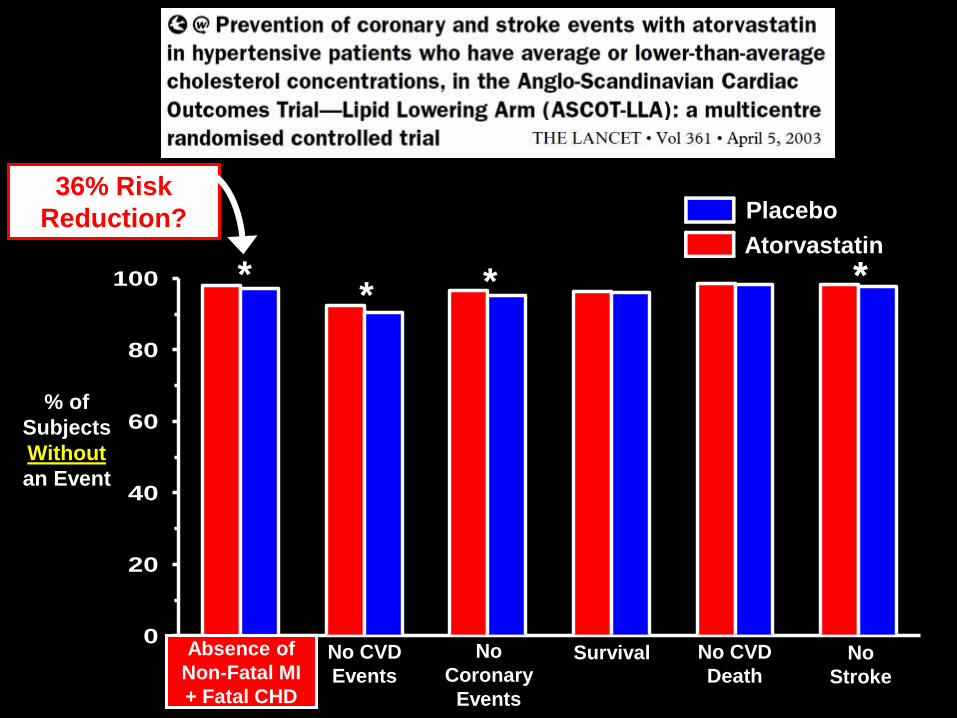
36% Risk
Reduction?
* * *
0
20
40
60
80
100
% of
Subjects
Without
an Event
*
Absence of
Non-Fatal MI
+ Fatal CHD
No
Stroke
No CVD
DeathSurvivalNo
Coronary
Events
No CVD
Events
*
Placebo
Atorvastatin
36% Risk
Reduction?
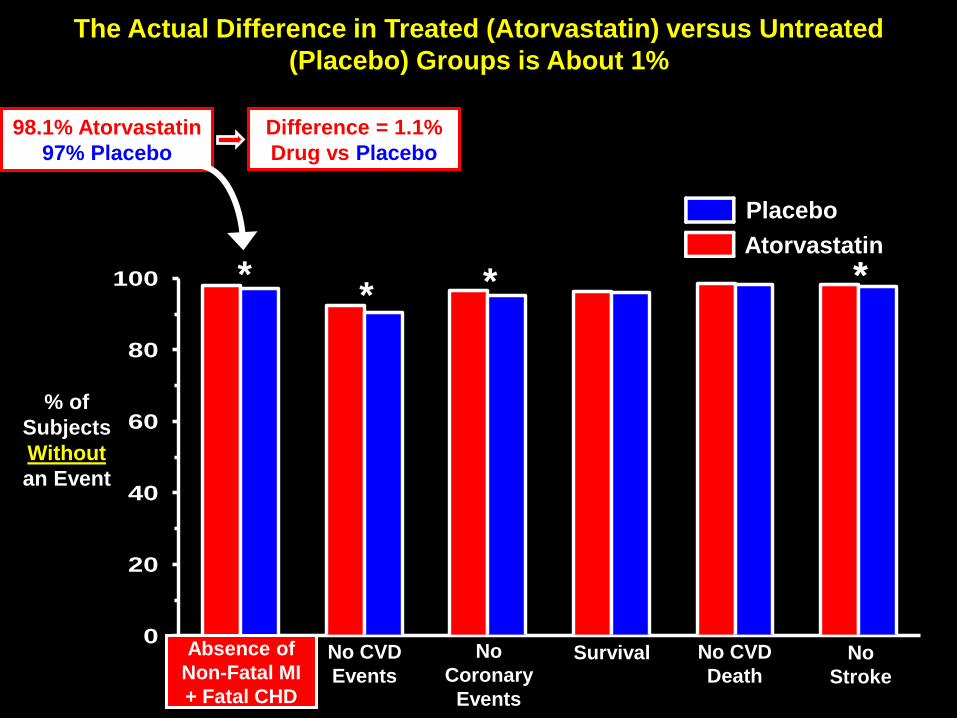
The Actual Difference in Treated (Atorvastatin) versus Untreated
(Placebo) Groups is About 1%
98.1% Atorvastatin
97% Placebo
Difference = 1.1%
Drug vs Placebo
* * *
0
20
40
60
80
100
% of
Subjects
Without
an Event
**
Placebo
Atorvastatin
No
Stroke
No CVD
DeathSurvivalNo
Coronary
Events
No CVD
Events
Absence of
Non-Fatal MI
+ Fatal CHD

How Can the Effect be 1.1% as well as 36%?(read the fine print)
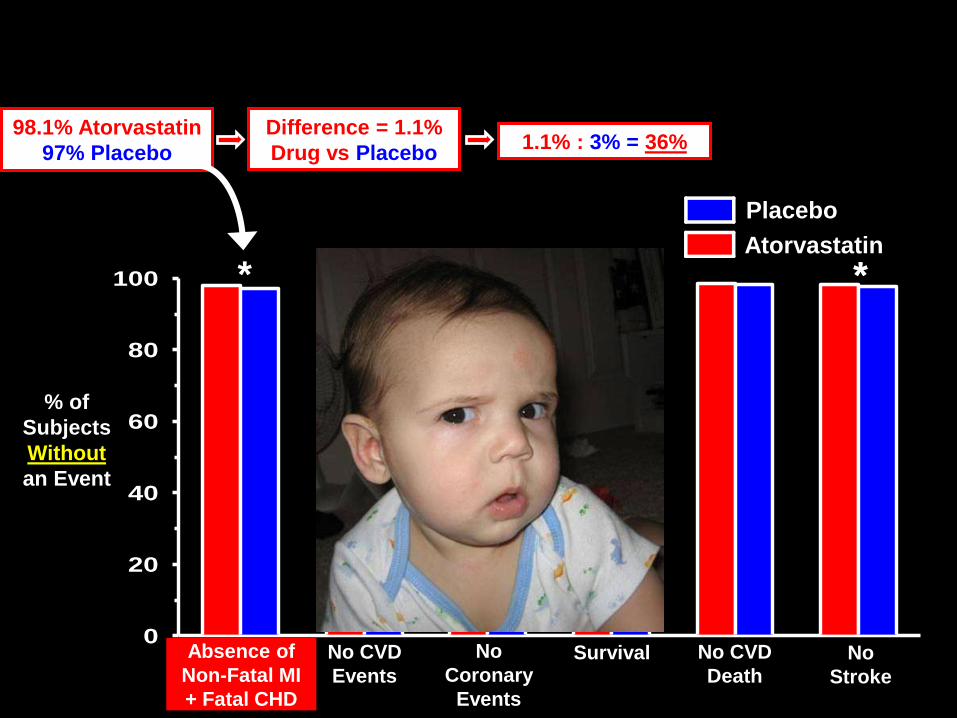
98.1% Atorvastatin
97% Placebo
Difference = 1.1%
Drug vs Placebo1.1% : 3% = 36%
* * *
0
20
40
60
80
100
% of
Subjects
Without
an Event
**
Placebo
Atorvastatin
Absence of
Non-Fatal MI
+ Fatal CHD
No
Stroke
No CVD
DeathSurvivalNo
Coronary
Events
No CVD
Events

Under ideal Conditions only 1/100 patients will Benefit

Statins Lose Their Appeal When the Real
Effectiveness Data is Shown

JUPITER Study – Crestor
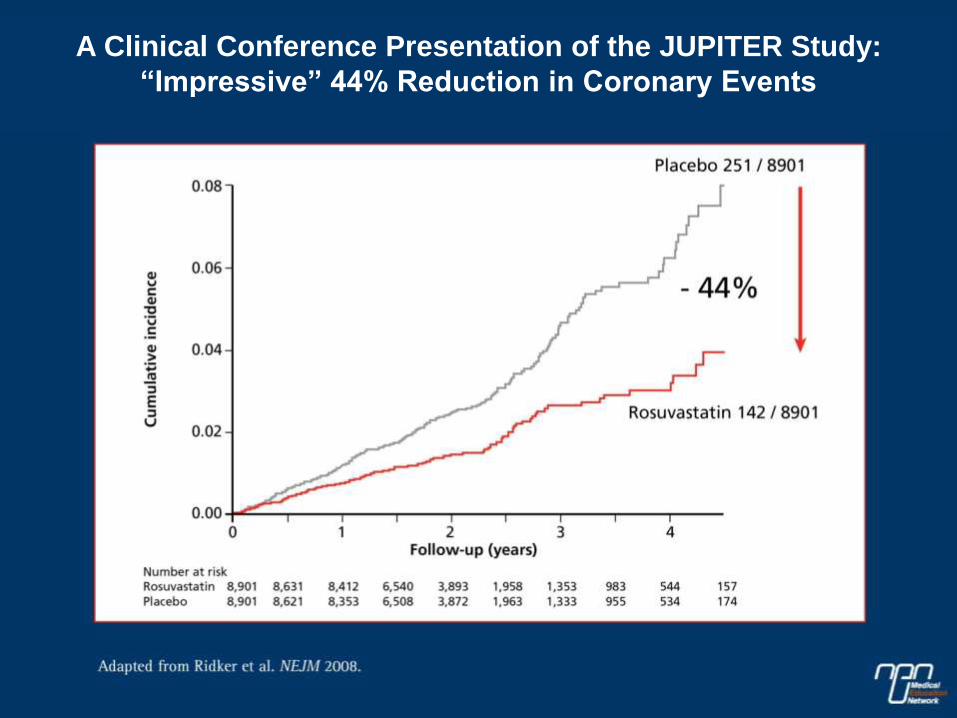
Little if Any Evidence of an All-Cause Mortality BenefitA Clinical Conference Presentation of the JUPITER Study:
“Impressive” 44% Reduction in Coronary Events
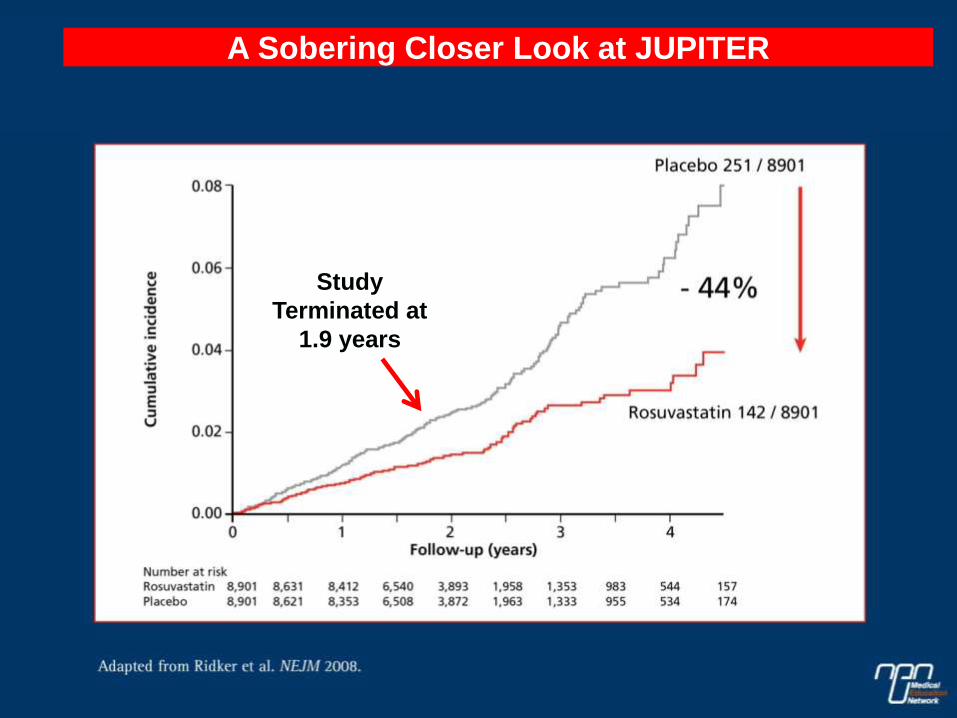
Little if Any Evidence of an All-Cause Mortality BenefitA Sobering Closer Look at JUPITER
Study
Terminated at
1.9 years
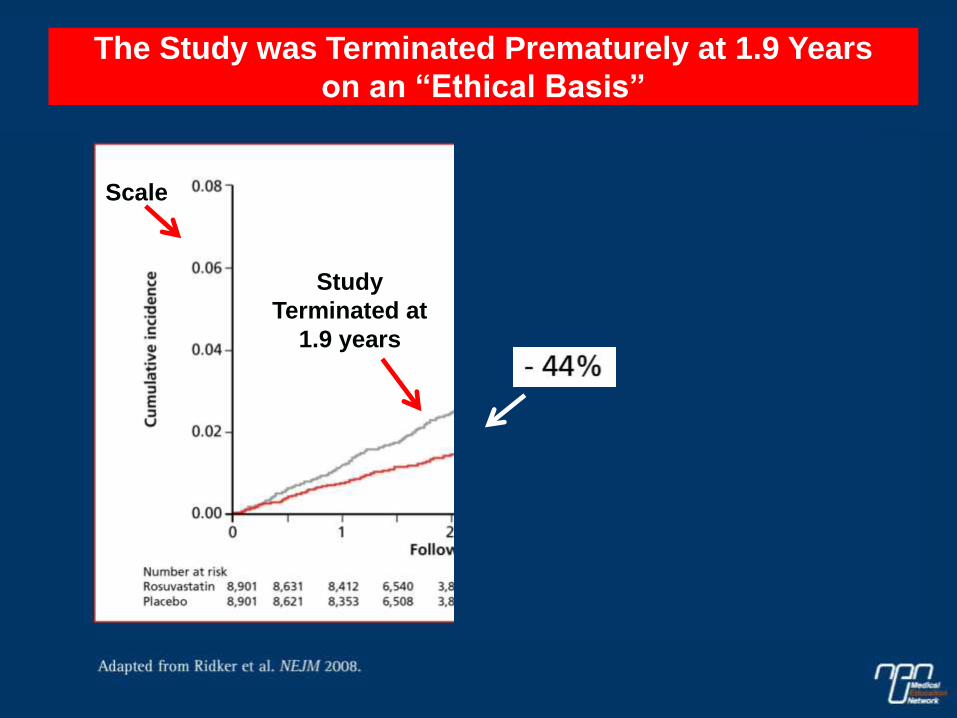
Scale
The Study was Terminated Prematurely at 1.9 Years
on an “Ethical Basis”
Study
Terminated at
1.9 years
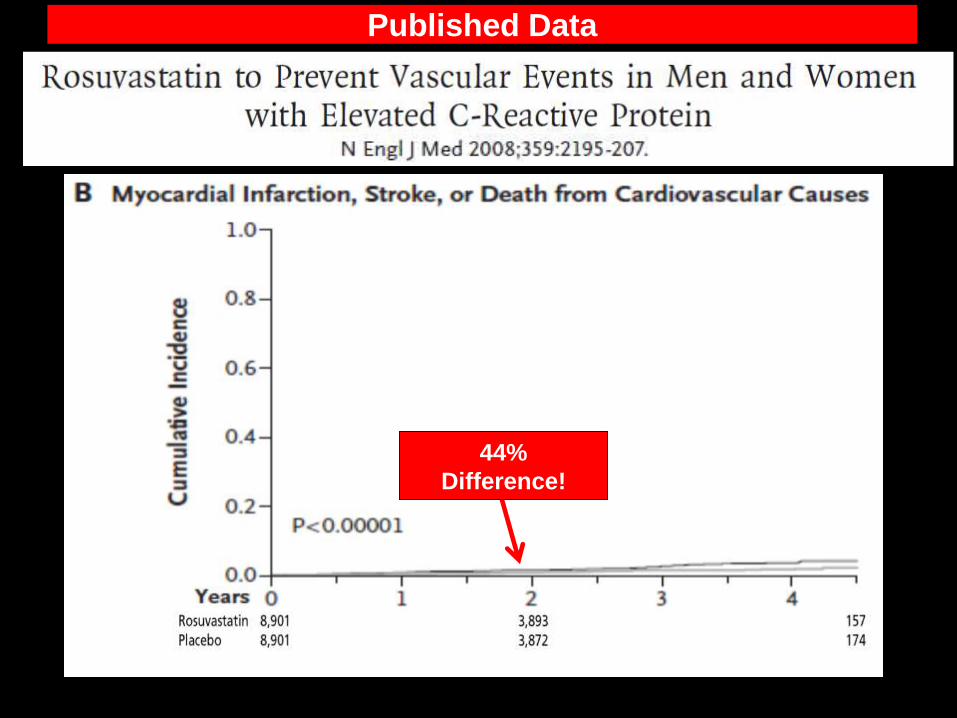
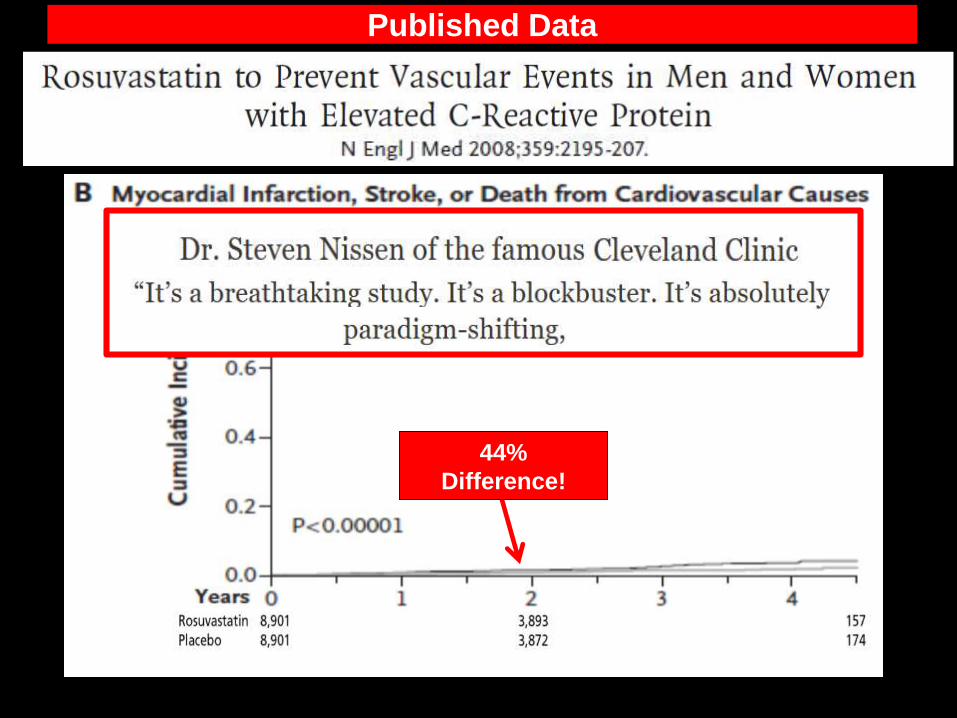
Published Data
44%
Difference!
44%
Difference!
Published Data

* **
98.4% Rosuvastatin
97.2% Placebo
Difference = 1.2%
Drug vs Placebo
Placebo
Rosuvastatin
JUPITER Study – Statistical Alchemy
How to Turn a Miniscule 1.2% Effect into a Spectacular 44% Effect
1.2% : 2.8% = 44%
Absence of
Non-Fatal MI
+ Fatal CHD
0
20
40
60
80
100
No
Stroke
No CVD
DeathNo
Stroke
No
Coronary
Death
No MI
**
% of
Subjects
Without
an
Adverse
Event
1% is better than nothing – right?
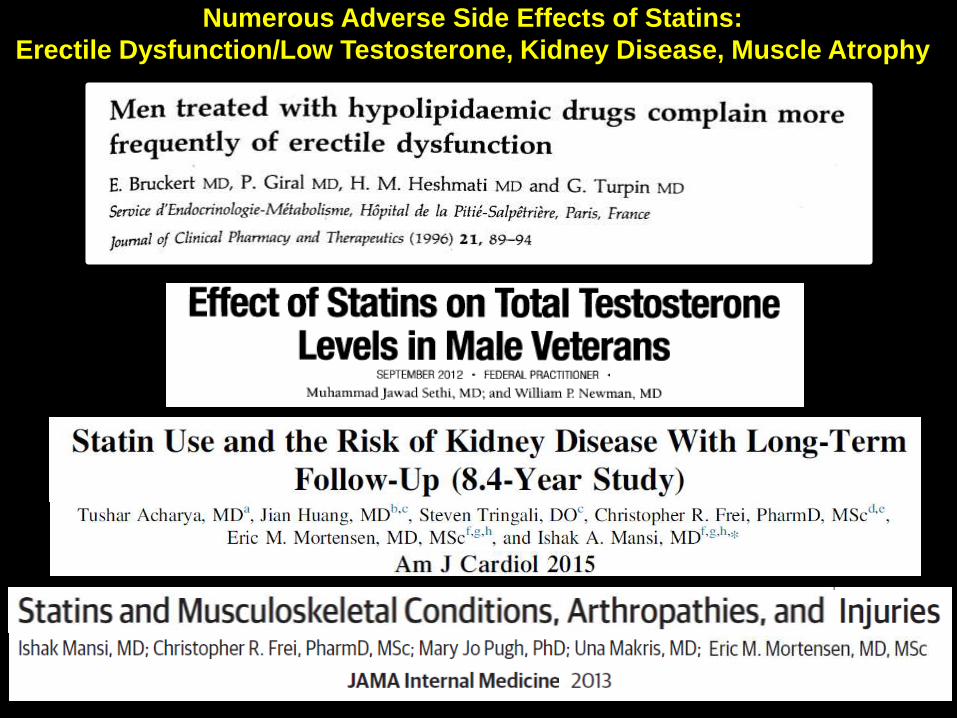
Numerous Adverse Side Effects of Statins:
Erectile Dysfunction/Low Testosterone, Kidney Disease, Muscle Atrophy
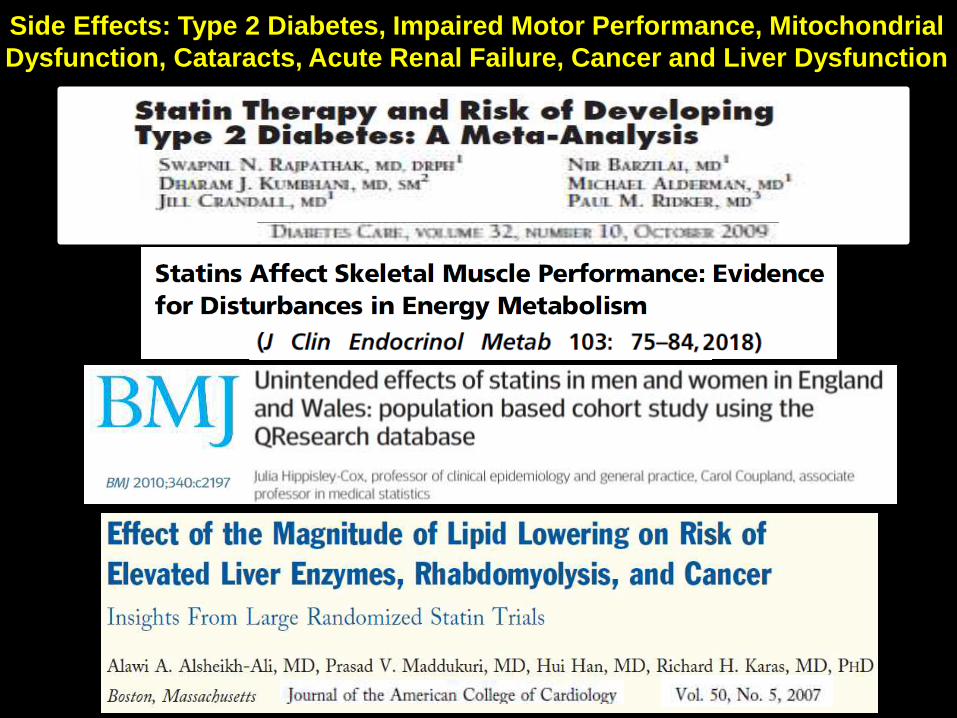
Side Effects: Type 2 Diabetes, Impaired Motor Performance, Mitochondrial
Dysfunction, Cataracts, Acute Renal Failure, Cancer and Liver Dysfunction

0
2
4
6
8
10
12
14
% of
Subjects
With New
Onset
Diabetes
Placebo
44% Increased Risk of Diabetes in People on Statins
Statins
*

Little if Any Evidence of an All-Cause Mortality Benefit

3. The small benefits of statins are Offset by their Adverse Effects
2. Deceptive Practices (Use of Relative Risk) Have Created the
Appearance of Statins as “Wonder Drugs”
1. Elevated Levels of Cholesterol, per se, are NOT Inherently
Atherogenic (e.g., elderly with high cholesterol live longer)
0
50
100
150
200
250
300
350
400
0.0
0.5
1.0
1.5
2.0
2.5
3.0
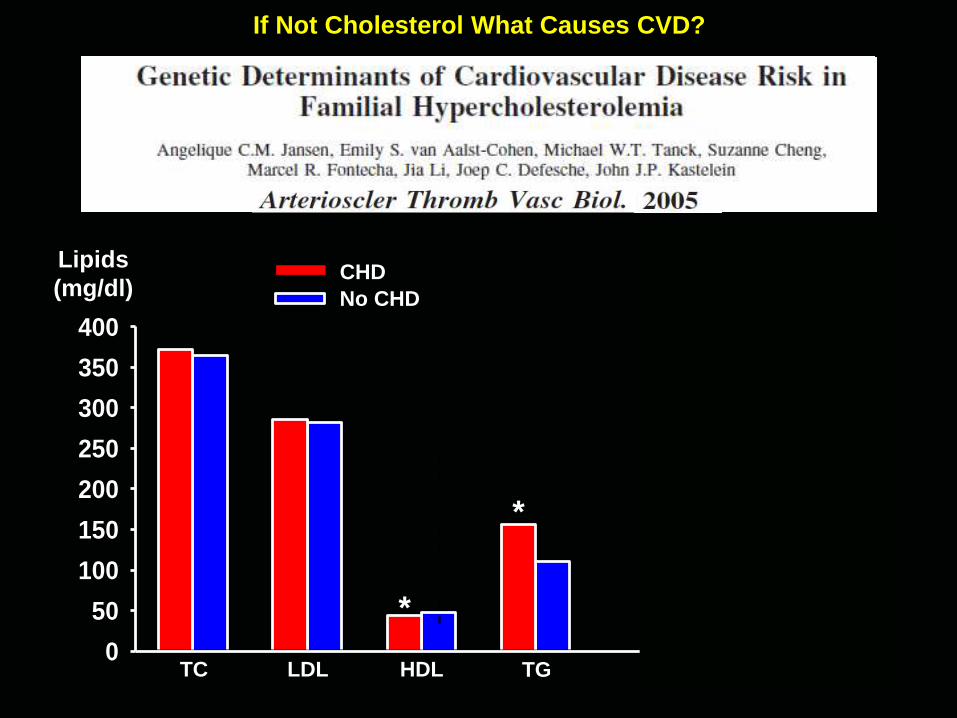
If Not Cholesterol What Causes CVD?
CHD
No CHD
*
Lipids
(mg/dl)
0
50
100
150
200
250
300
350
0
20
40
60
80
100
TC LDL HDL TG
*
*
0
50
100
150
200
250
300
350
400
0.0
0.5
1.0
1.5
2.0
2.5
3.0
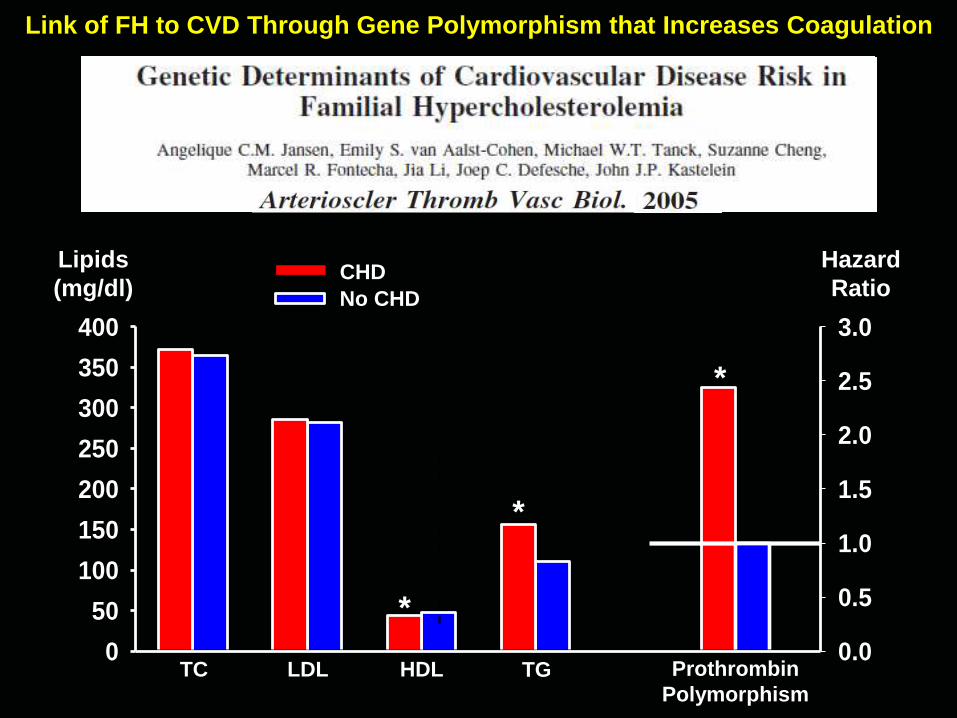
Link of FH to CVD Through Gene Polymorphism that Increases Coagulation
CHD
No CHD
*
Lipids
(mg/dl)
0
50
100
150
200
250
300
350
0
20
40
60
80
100
TC LDL HDL TG
*
*
Prothrombin
Polymorphism
Hazard
Ratio

Activation of Coagulation Factors and/or Reduced Fibrinolysis
Linked to Risk Factors for CVD
Smoking
Advanced Age
Inflammation
Hypertension
Obesity/Metabolic SyndromeHigh Blood Glucose
T2 Diabetes
Psychological
Stress
Subset of Familial
HypercholesterolemiaBacterial
Infection
Clot Formation
and Degradation
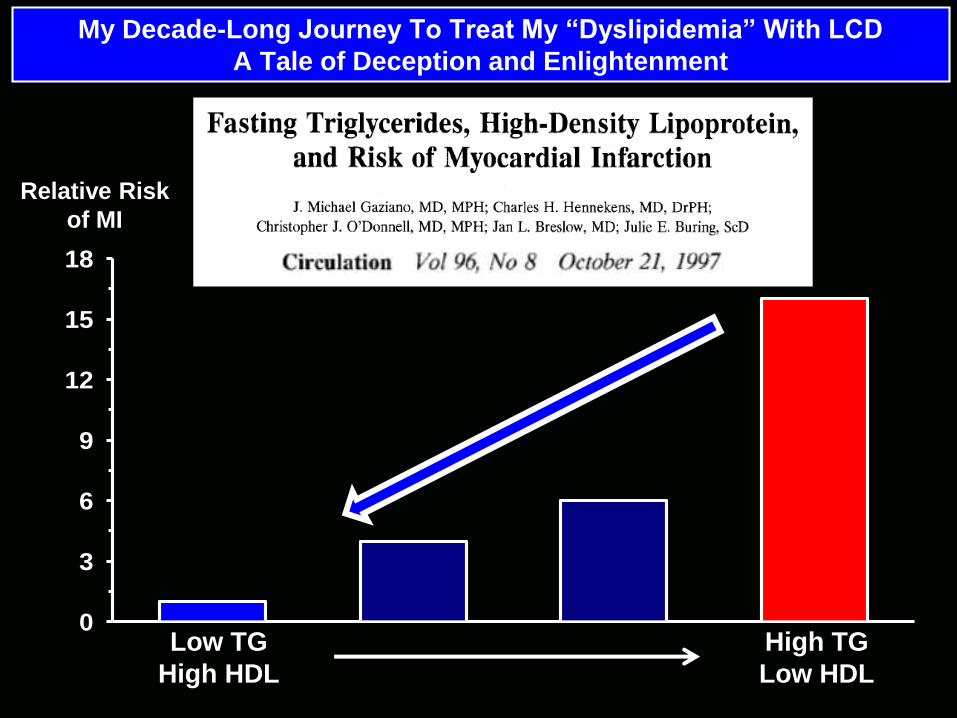
My Decade-Long Journey To Treat My “Dyslipidemia” With LCD
A Tale of Deception and Enlightenment
Relative Risk
of MI
Low TG
High HDL
High TG
Low HDL
0
3
6
9
12
15
18

The Diet-Heart Hypothesis:
Dietary Saturated Fat
Increase in Serum Cholesterol
Cardiovascular Disease
There has been a continuing offensive
against saturated fat and cholesterol
Supported by key opinion leaders
sponsored by food and drug
companies
The Diet-Heart Hypothesis:
Dietary Saturated Fat
Increase in Serum Cholesterol
Cardiovascular Disease
High levels of cholesterol (LDL-C) do not
promote premature death, and are beneficial
toward a reduced rate of morbidity and
death from infection and cancer
There has been a continuing offensive
against saturated fat and cholesterol
Supported by key opinion leaders
sponsored by food and drug
companies
The Diet-Heart Hypothesis:
Dietary Saturated Fat
Increase in Serum Cholesterol
Cardiovascular Disease
High levels of cholesterol (LDL-C) do not
promote premature death, and are beneficial
toward a reduced rate of morbidity and
death from infection and cancer
Despite praise from pharma-supported
researchers, cholesterol reduction
produces miniscule benefits with
offsetting adverse side effects
There has been a continuing offensive
against saturated fat and cholesterol
Supported by key opinion leaders
sponsored by food and drug
companies
The Diet-Heart Hypothesis:
Dietary Saturated Fat
Increase in Serum Cholesterol
Cardiovascular Disease
High levels of cholesterol (LDL-C) do not
promote premature death, and are beneficial
toward a reduced rate of morbidity and
death from infection and cancer
The primary target for CVD protection
should be hypercoagulation, preferably
through optimizing diet and lifestyle
Despite praise from pharma-supported
researchers, cholesterol reduction
produces miniscule benefits with
offsetting adverse side effects
There has been a continuing offensive
against saturated fat and cholesterol
Supported by key opinion leaders
sponsored by food and drug
companies