
An analysis of the burden of bipolar disorder and related suicide...
56
Bipolar disorder: Costs An analysis of the burden of bipolar disorder and related suicide in Australia An Access Economics Report for SANE Australia 2003
Transcript of An analysis of the burden of bipolar disorder and related suicide...

Bipolar disorder: CostsAn analysis of the burden of bipolar disorder and related suicide in Australia
An Access Economics Reportfor SANE Australia 2003


Bipolar disorder: CostsAn analysis of the burden of bipolar disorder and related suicide in Australia
An Access Economics Reportfor SANE Australia 2003

Disclaimer and Acknowledgements
This report was prepared by Access Economics for SANE Australia,funded by an unrestricted grant from GlaxoSmithKline Australia PtyLtd who had no part in the direction, analysis or findings contained inthis report. Access Economics would like to acknowledge withappreciation the comments, previous research and expert input from:
Professor Michael BerkProfessor of Psychiatry, Barwon Health and Geelong Clinic,University of Melbourne
Ms Barbara HockingSANE Australia
Professor Nicholas KeksProfessor of Psychiatry, Monash University,Director of Psychiatry, Box Hill Hospital
Professor Pat McGorryProfessor of Psychiatry,University of Melbourne,Director, ORYGEN Youth Health
Professor Philip MitchellHead, School of Psychiatry, University of New South Wales
Dr Paul MorganSANE Australia
Dr Jenny ThomasGeneral Practitioner, Adelaide
Professor Harvey WhitefordProfessor of Psychiatry, University of Queensland,Mental Health Advisor to the World Bank
Suggested referenceAccess Economics; SANE Australia (2003). Bipolar disorder: Costs:An analysis of the burden of bipolar disorder and related suicide inAustralia. Melbourne.
While every effort has been made to ensure the accuracy of this document, theuncertain nature of economic data, forecasting and analysis means that AccessEconomics Pty Ltd is unable to make any warranties in relation to the informationcontained herein. Access Economics Pty Ltd, its employees and agents disclaimliability for any loss or damage which may arise as a consequence of any personrelying on the information contained in this document.
© SANE Australia, 2003 ISBN 1 875182 60 8

Contents1 Executive Summary ........................................................................................................................... 22 Bipolar Disorder and Suicide............................................................................................................. 3
2.1 Bipolar disorder – a clinical picture; health and social impacts............................................................ 3Table 1: Weighted prevalence of comorbid 12-month DSM-IV disorders, Australia, 2003....................................................... 7Table 2: Impact of bipolar disorder symptoms on employment, 1992 and 2000....................................................................... 8
2.2 Suicide ............................................................................................................................................................ 9Table 3: Inadequacy of treatment prior to suicide for people with bipolar disorder, Australia, 1993-2001............................. 10Box 1: Personal story: Suicide is Painless?.............................................................................................................................. 10
2.3 Prevention, treatment and care................................................................................................................. 11
3 Prevalence and Direct Health Costs................................................................................................. 173.1 Prevalence of bipolar disorder........................................................................................................................... 17
Table 4: One-year prevalence of bipolar disorder in Australia, by gender & age, 2003.......................................................... 17
3.2 Prevalence of suicides related to bipolar disorder......................................................................................... 18Chart 1: Increase in age-standardised suicide rates 1921-2001, and rates by age & gender 2001, Australia ...................... 18Table 5: Suicides, Australia, by age & gender, 2001................................................................................................................ 19Table 6: Estimated suicides due to bipolar disorder, Australia, 2003 ...................................................................................... 19
3.3 Direct costs of bipolar disorder: 2003............................................................................................................... 21Table 7: Direct costs of bipolar disorder and other mental disorders, Australia, 1993-94, top-down ..................................... 21Table 8: Direct costs of bipolar disorder and depression, 1993-94 and 2003, top-down........................................................ 22Table 9: Direct costs of bipolar disorder per treated person, 2003, bottom-up........................................................................ 24Table 10: Direct costs of bipolar disorder, 2003, consolidated................................................................................................. 24Chart 2: Components of bipolar disorder costs, 2003 .............................................................................................................. 25Table 11: Costs of suicide and self-inflicted injuries including those due to bipolar disorder, Australia, 2003....................... 25
3.4 Projections to 2013 .............................................................................................................................................. 26Table 12: Projected numbers of people with bipolar disorder and their suicides, Australia, 2013.......................................... 26Table 13: Projected components of direct health costs for bipolar disorder, 2013 (2003 prices)........................................... 27
4 Indirect Costs and Burdens .............................................................................................................. 284.1 Loss of earnings................................................................................................................................................... 28
Table 14: Potential earnings and tax revenue lost due to bipolar disorder, 2003.................................................................... 28
4.2 Carer payments .................................................................................................................................................... 29Table 15: Value of carers of people with bipolar disorder, 2003.............................................................................................. 30
4.3 Cost of welfare payment ..................................................................................................................................... 30Table 16: Cost of welfare payments, bipolar disorder, 2003.................................................................................................... 31
4.4 Cost related to forensic issues .......................................................................................................................... 31Table 17: Prison costs of bipolar disorder, 2003....................................................................................................................... 32
4.5 Burden of disease ................................................................................................................................................ 32Table 18: Burden of disease from bipolar disorder including suicide, 2003 ............................................................................ 33Chart 3: Disease burden (DALYs) of bipolar disorder and other mental disorders ................................................................. 33
5 Conclusions....................................................................................................................................... 34Table 19: Summary of direct and indirect costs of bipolar disorder, 2003............................................................................... 34Chart 4: Distribution of bipolar costs, Australia 2003................................................................................................................ 35Table 20: Comparison with one UK study; direct and indirect costs of bipolar disorder ......................................................... 35
Methodology......................................................................................................................................... 39Table 21: Population and prevalence rates by cohort, Australia, 2003.................................................................................... 39
References............................................................................................................................................ 45
Access Economics | SANE Australia Bipolar disorder: Costs
2
1 Executive SummaryThe direct and indirect costs of bipolar disorder and associated suicides are substantial. Real financial costs total$1.59!billion in 2003, 0.2% of GDP and over $16,000 on average for each of nearly 100,000 Australians with theillness. Around half of this cost is borne by people with the illness and their carers.
– Direct health system costs are estimated at $298!million in 2003, with two-thirds being hospital expenditure, 13%medical expenditure (GPs and specialists), 11% residential care, 2% pharmaceuticals and the remainder onallied health, pathology, research and administration.
– This represents only $3,007 per person with bipolar disorder, even less than spending on the averageAustralian’s health care and 0.43% of national health spending.
– 42% of costs relate to depression, 36% to mania or hypomania and 22% to prophylaxis.
– Real indirect costs are estimated at $833 million, including $464!million of lost earnings from people unable towork due to the illness, $145!million due to premature death (the net present value of the mortality burden),$199!million of carer costs and $25!million of prison, police and legal costs.
– Transfer payments are estimated at $224!million of lost tax revenue (patients and carers) and $233!million inwelfare and care payments, primarily comprising disability support pensions.
Moreover, the burden of disease – the pain, suffering, disability and death – is greater for bipolar disorder than forovarian cancer, rheumatoid arthritis or HIV/AIDs, and similar to schizophrenia and melanoma.
– 24,001 years of healthy Australian life are estimated to be lost to the illness in 2003, including 4,843 years lostdue to suicide and self-inflicted injury – 56% of the burden of disease being borne by males and 90% by youngpeople aged 15-34 years.
Suicide is the pre-eminent cause of death – the lifetime risk of suicide for people with bipolar disorder is 15%.This year an estimated 298 Australians with bipolar disorder will take their lives, 12% of all suicides.
These tragic figures reflect both the serious nature of the illness, which will affect 1.2% of Australians in their lifetime,as well as serious problems of under-treatment and under-diagnosis in Australia.
– Of those who suicide, 60% are estimated to have received inadequate treatment. One third of people with bipolardisorder receive no treatment, 40% are not taking medications and only 17% access psychosocial rehabilitationprograms.
– Average treatment levels are less than one quarter of what is considered ‘best practice’. Although lithium iseffective in reducing suicide risk, there are problems in accessing treatment.
– Over two thirds of people with bipolar disorder are likely to be misdiagnosed, on average 3.5 times, with theaverage time from onset to accurate diagnosis over ten years.
– Comorbid substance abuse (at least 39% in a year and higher over a lifetime), anxiety disorders (52%) and otherconditions are confounding issues.
Bipolar disorder suffers from ‘orphan syndrome’ relative to unipolar depression. Bipolar disorder is largelymisdiagnosed and undertreated, leading to unacceptably high rates of suicide and costs to society. Public fundingstreams worthy of more dedicated investment in the future, to reduce expensive hospitalisations and improve qualityof life, include:– health worker education for better diagnosis, especially differential diagnosis, and earlier intervention;– enhanced suicide prevention and community awareness programs;– support, education and training programs, for people with bipolar disorder, their family and carers;– greater adherence to medications and use of psychotherapies, in particular through assertive community
psychiatric intervention and augmentation of specialist outpatient services;– treatment of comorbid substance abuse and other disorders; and– research for cause, cure and care.
Without such investment, in the coming decade real direct health costs alone for bipolar disorder willapproach $400!million per annum, with the indirect costs of lost productivity, carer burden and welfarepayments outnumbering these costs fourfold. Moreover, if the gross under-treatment of Australians withbipolar disorder is not addressed, its heavy suicide toll will persist, and those who survive will continue tosuffer from the ‘orphan syndrome’ in Australian mental health care.

Access Economics | SANE Australia Bipolar disorder: Costs
3
‘When you’re high, you think you cantake on anything. You’re so perceptive
and sharp, your mind is racing athousand miles ahead of everyone else.
I’d give all my money away. I’d seepeople in the street who needed moneyand give it to them, pay people’s fines,
give endless free help. I ended up gettingmy young son to cut up my credit cards
so I couldn’t get into more debt.
I’d go home and be up all night scrubbingmy flat, polishing my car 15 times to seekabsolute perfection. I’d sit in the beanbag,
smoking and staring at the TV set allnight, thinking really bad, suicidal
thoughts. When I got really low, all colourwould go from what I saw, everything was
black and grey.
I was not correctly diagnosed for years.When I was finally diagnosed and startedon medication, it was sheer relief. I felt acalmness I’d never experienced before.
I felt I’d been given my life back.Neil Cole
‘For about 12 months I used to say I hadlost my feelings. I couldn’t feel anything.
If somebody that I love or one of myfamily members had got run over…
I wouldn’t have reacted. I used todescribe it as being a shell of a person –everything inside me died and I had just
my physical body that I was walkingaround in. It’s total emotional shutdown.
My face was like a mask.It had no expression.’
Carole
2 Bipolar Disorder and Suicide
2.1 Bipolar disorder – a clinical picture; health and social impacts2.1.1 What is bipolar disorder? 1
Bipolar disorder (once called manic depression) is a medical condition that affects the brain, causingextreme changes in mood, thoughts and activity, much more severe than normal ‘highs’ or ‘lows’. Typicallythe fluctuations, which can be known as ‘episodes’ or ‘cycles’, are characterised by the followingsymptoms, without reason:
Mania– Increased energy, activity and restlessness– ‘High’, euphoric mood– Racing thoughts and speech, jumping between ideas– Distractibility, poor concentration– Little sleep required– Unrealistic beliefs in one's abilities and powers– Lasting period of behaviour that is different from usual– Poor judgment– Spending sprees– Increased sexual drive– Abuse of drugs, particularly cocaine, alcohol, and
sleeping medications– Extreme irritability– Provocative, intrusive, or aggressive behaviour– Denial that anything is wrong
Mania episode is diagnosed if elevated mood occurs withthree or more other symptoms most of the day, nearlyevery day, for one week or longer. If mood is irritable, fouradditional symptoms must be present (NIMH, 2001).
Mild to moderate mania is hypomania, which may feelgood and include enhanced functioning and productivity.Hence the person may deny that anything is wrong, even iffamily and friends recognize the mood swing. Withoutproper treatment, however, hypomania can become severemania in some people or can switch into depression.
Depression symptoms include:– Lasting sad, anxious, or empty mood– Feelings of hopelessness or pessimism– Feelings of guilt, worthlessness, or helplessness– Loss of interest or pleasure in activities once enjoyed– Decreased energy, fatigue, ‘slowing down’– Restlessness, irritability– Sleeping too much, or can't sleep– Change in appetite and/or unintended weight loss/gain– Difficulty concentrating, remembering, making decisions
1 Australians with bipolar disorder who tell their stories in Kelly (2000) are cited throughout to the original story-teller, eg ‘Rachel’.

Access Economics | SANE Australia Bipolar disorder: Costs
4
– Chronic pain or other persistent physical symptoms not caused by physical illness or injury– Thoughts of death or suicide (suicidal ideation) or suicide attempts
Depression is diagnosed if five or more of these symptoms last most of the day, nearly every day, for aperiod of two weeks or longer (NIMH, 2001).
Sometimes, severe episodes of mania or depression include psychotic symptoms such as hallucinations(hearing, seeing or otherwise sensing the presence of things not actually there) and delusions (false,strongly-held beliefs not influenced by logical reasoning or explained by a person's usual culturalconcepts). In bipolar disorder, psychotic symptoms tend to reflect the extreme mood state at the time.For example, delusions of grandiosity, such as believing one has special powers, wealth or status, mayoccur during mania; delusions of guilt or worthlessness, such as believing one is ruined, penniless or hascommitted some terrible crime, may appear during depression.
Bipolar mood states can be depicted as a spectrum withsevere depression at the low ‘pole’, above which ismoderate depression and then mild low mood—‘theblues’ when short-lived but ‘dysthymia’ when chronic.Normal or balanced mood lies in the middle, abovewhich is hypomania and then severe mania at the highpole.
The length, intensity and pattern of fluctuations varies from one person to another. As many as 40-48% ofpeople experience mixed states, where some symptoms of depression are mixed with some symptoms ofmania (Goodwin and Jamison, 1990, p101). Symptoms of a mixed state often include agitation, troublesleeping, change in appetite, psychosis, and suicidal thinking. A person may have a very sad, hopelessmood while at the same time feeling extremely energized.
Sometimes there can be ‘rapid cycling’ between the two states, defined as four or more cycles in a year,compared to the ‘average’ of 0.4 to 0.7 (Mitchell et al, 2003). Some people experience multiple episodes ina single week, or even in a day. Rapid cycling tends to develop later in the course of illness (NIMH, 2001),occurs in 5–20% of adults with bipolar disorder, and is more common in women than men – up to 72%compared to 28% (Suppes et al, 2000).
2.1.2 Diagnosis and disease progressionLike other mental illnesses, bipolar disorder cannot yet be identified physiologically – for example, througha blood test or brain scan. Diagnosis is therefore made on the basis of symptoms, course of illness and,when available, family history. Diagnostic criteria for bipolar disorder are described in the Diagnostic andStatistical Manual for Mental Disorders, fourth edition (DSM-IV). Two types of bipolar disorder aredistinguished from three other major mood disorders in the DSM-IV with characteristics as follows:– Bipolar affective disorder Type I: at least one manic or mixed episode, with depressive episodes;– Bipolar affective disorder Type II: depressive episodes with hypomania (no mania);– Major depressive disorder: depression without mania or hypomania;– Cyclothymia: hypomania and mild depression– Dysthymic disorder: persistent mild depression.
Onset of bipolar disease symptoms can be as early as childhood or teenage years. Some children andadolescents with bipolar disorder can be more prone than adults to mixed symptoms, to rapid moodswings many times a day and to irritability and destructive tantrums in mania, rather than to being elated.Bipolar disorder can be difficult to recognise and accurate diagnosis can take some years, in part due toproblems of differential diagnosis. For young people, it is necessary to distinguish bipolar from attentiondeficit hyperactivity disorder (ADHD), conduct disorder or oppositional defiant disorder. In adults andadolescents, it is important to distinguish bipolar from depression, schizophrenia, drug-induced psychosesand eating, anxiety or personality disorders. Women are most likely to be misdiagnosed with depression,

Access Economics | SANE Australia Bipolar disorder: Costs
5
69% of people with bipolardisorder are mis-diagnosed, onaverage 3.5 times. On average,
it takes 10.2 years and 4doctors to obtain a correctdiagnosis (DMDA, 2001).
and men most likely to be misdiagnosed with schizophrenia (DMDA,2001). There are a number of useful diagnostic tools, including theStructured Clinical Interview for DSM-IV (SCID), Schedule for AffectiveDisorders and Schizophrenia (SADS) and the Mini-Mental State Exam(MMSE), which all require extensive clinician training for optimal use andare not suitable for screening. A new screening questionnaire – the MoodDisorders Questionnaire (MDQ) – is now available, shown to be bothspecific and sensitive in distinguishing bipolar disorder from otherpsychiatric conditions (Hirschfeld, 2002).
Spike Milligan (1918-2002) lived withbipolar disorder for most of his life.
There is extensive documentation of the under-diagnosis (delayed diagnosis and misdiagnosis) andunder-treatment of bipolar disorder. A US longitudinal survey found that one third of people with bipolardisorder wait at least ten years before seeking help (DMDA, 2001), with an average of 4.5 years fromonset to seeking help and an average of 10.2 years from onset to accurate diagnosis. From seeking helpto diagnosis takes more than 10 years for 35% of people, between 5 and 10 years for 15% of people andbetween 3-5 years for 11% of people. 69% of the 600 participants were initially misdiagnosed, with anaverage of 3.5 misdiagnoses and consultation of four physicians prior to obtaining an accurate diagnosis.Sixty per cent were misdiagnosed with depression, 26% withanxiety disorder, 18% with schizophrenia and 17% withborderline personality or antisocial personality disorders. Ina smaller US study, 42% of people with bipolar disordercarried other diagnoses, 90% being unipolar depression(Ghaemi et al, 1997). Screening for bipolar before providingwomen with a diagnosis of depression, or men with adiagnosis of schizophrenia, could be beneficial. Treatmentgaps and non-adherence are discussed more in Section 2.3.
Episodes of mania and depression typically recur across the life span. Between episodes, most peoplewith bipolar disorder are free of symptoms, but as many as one third of people have some residualsymptoms. Full symptom resolution may occur in 26% of patients and functional recovery may occur in24% (Mitchell et al, 2003). A small percentage of people experience chronic unremitting symptoms despitetreatment (Hyman and Rudorfer, 2000).
Earlier diagnosis means earlier access to treatment and support. Without treatment the natural course ofbipolar disorder tends to worsen. Over time a person may experience more frequent and severe episodes(Goodwin and Jamison, 1990). With treatment, however, most people experience reduced frequency andseverity of episodes, recover well from episodes of illness and have enhanced quality of life.
‘I was diagnosed as anorexic depressive and paranoid schizophrenic… I knew I wasn’t anorexic… I justdidn’t eat because I wasn’t hungry. They did those psychological tests on me… as a result of that theydecided I was paranoid schizophrenic. I ended up in a private psychiatric hospital. I was only diagnosedwith manic depression a couple of years after that.’
Mary

Access Economics | SANE Australia Bipolar disorder: Costs
6
2.1.3 AetiologyThe causes of bipolar disorder are not fully understood. It seems there is no single cause for bipolardisorder — rather, many factors act together to produce the illness.
Because bipolar disorder tends to run in families, genetic research has for decades attempted to isolatethe gene or genes that create a vulnerability to develop bipolar disorder. Areas that have been identifiedas possible interacting contributors are chromosomes 4, 12, 18, 21, 22 and X (Hyman, 1999).Researchers at the University of California San Diego School of Medicine recently identified a mutation inG protein receptorkinase 3 (GRK3), occurring in part of the gene called the ‘promoter’ that regulates whenthe gene is turned on. This gene regulates sensitivity to brain neurotransmitters such as dopamine, andthe research suggests that the mutation may contribute to bipolar disorder in as many as 10% of cases(Barrett et al, 2003).
At least 50% of people with bipolar disorder have a parent with a mood disorder, most often majordepressive disorder. A person has a 30% chance of inheriting a mood disorder if one parent has bipolardisorder, and a 60% chance if both parents have it. Research has found an even greater risk among twins,especially identical twins, who have a parent with bipolar disorder (NIMH Genetics Workgroup, 1998).A person with high penetrance – how strongly a gene is expressed – has a high probability of developingbipolar disorder when a stressor of sufficient strength is experienced, whereas a person with lowpenetrance exposed to that same stressor or environment may not develop bipolar disorder.
New brain-imaging techniques and studies are helping to identify what goes wrong in the brain to producebipolar disorder and other mental illnesses (Soares and Mann, 1997a and b). These techniques includemagnetic resonance imaging (MRI), positron emission tomography (PET) and functional magneticresonance imaging (fMRI). Areas being researched include the systems controlled by the hypothalamusand pituitary gland (adrenal, thyroid and reproductive systems) and the limbic system (emotional centre),communication between the right and left hemispheres, parts of the cerebellum and the temporal lobe andthe function of two neurotransmitters involved in bipolar disorder – serotonin and dopamine (Kelly, 2000).
Viruses and the immune system are also under investigation as possibly contributing to bipolar disorder.Antibodies to viruses that cause glandular fever, cold sores and some other conditions have beenidentified in the bloodstream of people with bipolar disorder, whether or not they have symptoms of thoseillnesses (Goodwin and Jamison, 1990, p534). People with chronic asthma and hayfever, which are alsoassociated with bipolar disorder, have gained relief from lithium. People with multiple sclerosis – an auto-immune disease – have a higher incidence of bipolar disorder than the general population.
Dangerous environmental triggers include relationship difficulties and work pressures, especially duringthe early stage of the illness. Sleep disturbance – disruption to circadian rhythms – may be a contributoras well as a symptom of bipolar disorder. In women, hormones associated with puberty, the menstrualcycle, pregnancy (including miscarriage and termination), childbirth and menopause can trigger episodes(Parry, 1996). New mothers with bipolar disorder have a 30% to 50% risk of an episode during the firstmonth after childbirth (Kelly, 2000).

Access Economics | SANE Australia Bipolar disorder: Costs
7
In a year, 39% of Australianswith bipolar disorder have
comorbid substance abuse;lifetime prevalence is even
higher.
2.1.4 Morbidity, socioeconomic impacts and mortalityBipolar disorder can cause substantial suffering, disruption to quality of life and premature death.Its functional impairment in Australia has been shown to be even more devastating than that of depression(Mitchell, Slade and Andrews, 2003), including marital break-ups, destruction of personal relationships, jobloss, alcohol and drug abuse, other significant comorbidities and suicide.
Alcohol and substance abuse: Studies show that substance abuse comorbidity is very high, andsubstantially more likely to occur with bipolar disorder than with other mental illness, includingschizophrenia, depression, anxiety or eating disorders, or any other DSM-IV ‘Axis I’ disorder (Brady andGoldberg, 1996). Many factors contribute to substance abuse comorbidity, including self-medication ofsymptoms, mood symptoms either brought on or perpetuated by substance abuse, and common riskfactors (Strakowski and DelBello, 2000). Factors that may increase the risk of comorbid substance abuseare family history of substance use, an early age of onset of bipolar disorder and the presence of mixedepisodes. Treatment for co-occurring substance abuse, when present, is an important part of the overalltreatment plan for someone with bipolar disorder.
Different studies show different levels of alcohol and substance abuse comorbidity – for example, 30-60%(Brady and Goldberg, 1996), 40% (Lish et al, 1994) and 60% (NIMH). Evans (2000) distinguishes 46% ofpeople dependent on alcohol and 40% with drug abuse or dependency, noting that substance abuse canexacerbate symptoms and/or precipitate episodes. In Australia, Mitchell, Slade and Andrews (2003) foundthat for one-year prevalence, 38.9% of people with bipolar disorder have a substance abuse disorder,including 26.4% with drug abuse/dependence and 28.9% with alcohol abuse/dependence, compared withgeneral rates in the population of 6.7%, 2.4% and 5.2% respectively. Table 1 shows various comorbidities,comparing bipolar disorder to major depressive disorder as well as to the ‘rest of the sample’ (the generalpopulation). The results show that bipolar disorder has greater comorbidity than depression. Lifetimeprevalence is likely to be much higher.
Table 1: Weighted prevalence of comorbid 12-month DSM-IV disorders, Australia, 2003Bipolar disorder Major depressive
disorderRest of the
sample
Comorbid Disorders % (SE) % (SE) % (SE)Model 1: Individual disordersDysthymia 7.8 (3.0) 11.6 (1.2) 0.3 (0.1)Panic disorder with or w/out agoraphobia 26.3 (6.0) 12.4 (1.4) 1.1 (0.1)Agoraphobia 6.2 (3.4) 7.9 (1.0) 1.1 (0.1)Social phobia 19.1 (6.3) 14.5 (1.3) 1.3 (0.1)Generalized anxiety disorder 25.3 (5.7) 25.9 (2.2) 1.9 (0.2)Obsessive-compulsive disorder 9.5 (3.7) 5.5 (0.9) 0.3 (0.1)Post traumatic stress disorder 10.6 (5.1) 12.4 (1.1) 0.5 (0.1)Drug abuse/dependence 26.4 (5.5) 7.6 (1.1) 2.4 (0.2)Alcohol abuse/dependence 28.9 (6.2) 16.4 (1.2) 5.2 (0.2)Model 2: Disorder groupAny affective disorder1 7.8 (3.0) 11.6 (1.2) 0.3 (0.1)Any anxiety disorder 52.0 (8.7) 45.9 (2.3) 5.2 (0.3)Any substance use disorder 38.9 (6.8) 21.3 (1.2) 6.7 (0.2)Any personality disorder 44.3 (10.6) 28.5 (2.2) 4.7 (0.3)Any medical condition2 44.5 (12.1) 46.4 (1.9) 37.9 (0.6)Model 3: Number of disordersOne other disorder 16.9 (9.0) 25.8 (1.5) 8.9 (0.4)Two or more other disorders 47.7 (9.2) 31.6 (2.1) 2.3 (0.2)Model 4: Any other disorder 65.3 (10.3) 62.6 (2.0) 14.1 (0.5)1. Made up of one disorder – dysthymia2. Medical conditions include asthma, chronic bronchitis, amaemia, high bloodpressure, heart trouble, arthritis, kidney disease, diabetes, cancer, stomach orduodenal ulcer, chronic gallbladder or liver trouble, hernia or rupture.Source: Mitchell, Slade and Andrews (2003), part of Table 3.

Access Economics | SANE Australia Bipolar disorder: Costs
8
52% of Australians withbipolar disorder have a
comorbid anxiety disorder
Other Australian data (collated by Professor Patrick McGorry at the University of Melbourne) suggest that,in young people, the rate of comorbid substance abuse may be as high as 70%.
Other comorbidities and disability: Anxiety disorders, such aspost-traumatic stress disorder (PTSD) and obsessive-compulsivedisorder, may be common in people with bipolar disorder (Mueseret al, 1998), with PTSD reported by the NIMH as high as 43%.Co-occurring anxiety disorders may respond to the treatmentsused for bipolar disorder, or they may require separate treatment(Strakowski et al, 1998). Panic disorder, social phobia and impulse control disorders (e.g. pathologicgambling, kleptomania) may also be more common. Mitchell, Slade and Andrews (2003) show fromAustralian data that people with bipolar disorder are ten times more likely to have an anxiety disorder –52% compared to 5.2% in the general population. The figures also show elevated risk of personalitydisorder (44.3% compared to 4.7%), although this may be an artefact of the interview system, and ofdysthymia (7.8% compared to 0.3%). Although prevalence of other medical conditions was elevated(44.5% compared to 37.9%), this was not statistically significant.
Disability: Mitchell, Slade and Andrews (2003) also show that people with bipolar disorder in Australia aremore disabled as assessed by a number of measures of disability, including days of disability, rolefunctioning, mental scale assessment and neuroticism. People with bipolar were on average 4 to 5 timesmore disabled than the general population by all measures.
Relationships: The intimate relationships of those with bipolar disorder tend to suffer. Lish et al (1994)found that 57% to 73% of patients with bipolar disorder were divorced or had past marital difficulties.DMDA (2001) found that 65% of people responding to their survey in 2000 reported difficulties in theirmarriage or intimate relationships because of bipolar disorder. 60% said they had difficulty maintaininglong-term friendships (both increases on 1992) and 64% said their illness had a negative impact on theirrelationships with their children (a new question). In Australia, Mitchell et al (2003) cite double the divorcerate for people with bipolar disorder, while Mitchell, Slade and Andrews (2003) show rates of beingseparated, divorced or widowed as 3.1 times higher than the general population, and of never marrying as3.0 times higher.
Employment impacts: Days lost from work, loss of employment and difficulty regaining employment canall contribute to the disruption caused by the disorder. Lish et al (1994) found that only 43% percent ofpatients with bipolar disorder were employed six months after discharge from a psychiatric hospital, andonly 21% were functioning at their expected level of employment. Zwerling et al (2002), using data fromover 11,000 respondents in the US National Health Interview Survey, found that people with bipolardisorder were only 60% as likely to work. DMDA results are shown in Table 2, indicating a worsening from1992 to 2000.
Table 2: Impact of bipolar disorder symptoms on employment, 1992 and 20001992 2000
Base (total responding)Those who agree strongly or somewhat with statement
500%
600%
The illness affected my abilities to perform job duties 83 88*My career aspirations were lower 74 75I found it necessary to change jobs more frequently than my peers 58 65*I found it necessary to totally change careers/professions 55 60I was treated differently from other employees 52 63*I quit working outside the home 47 58*I was passed up for a promotion 47 65*I was given decreased responsibility in job duties 40 48*My mania increased my productivity before having a negative impact on my performance - 79* Significantly greater than 1992 at 95% confidence level.Note: Question—‘Please rate the impact of your symptoms on your employment, by indicating how much you agree or disagreewith each of the following statements when the illness was not being managed effectively’.Source: DMDA (2001), Table 9.

Access Economics | SANE Australia Bipolar disorder: Costs
9
1 in 6 Australians withbipolar disorder die by
their own hand.Over 1 in 4 attempt
suicide, nearly twicethe rate of Australians
with depression.Two-thirds contemplate
suicide.
60% of Australians withbipolar disorder who
completed suicidereceived inadequate
treatment prior to theirdeath.
Australian data show people with bipolar disorder are 15 times more likely than average to be in the lowestincome earning category and their occupational status is twice as likely to deteriorate (Mitchell, 2001).Mitchell, Slade and Andrews (2003) found that unemployment rates were 2.1 times higher for people withbipolar disorder although workforce participation was higher and there was no significant difference in theemployment rate. Because these data were not age-standardised, these results reflect the concentrationof people with bipolar disorder of workforce age (see Section 3.1).
Mortality: Death rates for untreated bipolar disorder are higher than those for most types of heart diseaseand some types of cancer (Bowden, 1997) and are two to three times higher than those of the generalpopulation (Muller-Oerlinghausen et al, 2002). Elevated rates of mortality and morbidity are due to suicide,cardiovascular and other diseases, which can sometimes be related to other comorbidities, such as liverdysfunction (Bourgeois and Verdoux, 1997). By far the largest source of preventable premature death forpeople with bipolar disorder is suicide.
‘Manic-depression distorts moods and thoughts, incites dreadful behaviours, destroys the basis of rationalthought, and too often erodes the desire and will to live. It is an illness that is biological in its origins, yetone that feels psychological in the experience of it; an illness that is unique in conferring advantage andpleasure, yet one that brings in its wake almost unendurable suffering and, not infrequently, suicide. I amfortunate that I have not died from my illness, fortunate in having received the best medical care available,and fortunate in having the friends, colleagues, and family that I do.’ Dr Kay Redmond Jamison (1995), p6.
2.2 SuicideThe lifetime risk of suicide for people with bipolar disorder is around15% (Goodwin and Jamison, 1990). In Australia, empirical evidenceshows 10% to 19% of people with bipolar disorder suicide (Mitchell etal, 2003).2 The figures may be higher as in many cases cause of deathis unknown – such as single vehicle accidents. Those at highest risktend to be young men in an early phase of illness, especially thosewho have made a previous suicide attempt, those abusing alcohol,and those recently discharged from hospital. Risk is also increased inpatients who are in the depressed phase, who have mixed states, orwho have psychotic mania. Lithium prophylaxis appears to decreasesuicide attempts (Simpson and Jamison, 1999).
Australians with bipolar disorder are more likely than average to havethoughts about suicide or to make a suicide attempt – 26% will attemptsuicide during their lifetime, much higher than the 14% of Australianswith depression and the 2% of Australians overall (Mitchell, Slade andAndrews, 2003, and consistent with Kessler et al, 1997). Sixty-five percent will contemplate suicide compared to 49% with depression and11.6% in the general population (Mitchell, Slade and Andrews, 2003).
A pivotal Australian study was recently conducted by Keks et al (2003),which provides demographic and risk factor analysis for Victorians withbipolar disorder who suicided between 1993 and 2001. More detail ofthis study is provided in Section 3.2. However, a critical finding of the study is highlighted here – themajority (60%) of bipolar suicides in the series did not receive management at or above a recognisedbenchmark standard. In the year prior to suicide, prescription of antidepressants was inadequate in 40% of
2 The WA linked database shows 15% (Coghlan et al, 2001). Muller-Oerlinghausen et al (2002) cite 10-20% of people with bipolardisorder take their own life, and nearly one third admit to at least one suicide attempt. Jamison (2000) cites at least 25% to 50%attempting suicide at least once.

Access Economics | SANE Australia Bipolar disorder: Costs
10
people, and of mood stabilisers in 40%; psychosocial intervention was unsatisfactory in 45% (seeTable!3).3
Table 3: Inadequacy of treatment prior to suicide for people with bipolar disorder, Australia, 1993-2001Clinical panel ratings on selected psychiatric autopsy questions Yes
(%)No(%)
Uncertain(%)
Was medical intervention adequate in the 12 months prior to suicide (apart fromlast 4 weeks)? 28.6 57.1 14.3Was medical intervention adequate in the 4 weeks prior to suicide? 34.3 60.0 5.7Was clinician use of mood stabilisers adequate in 12 months prior to suicide? 42.9 40.0 17.1Was clinician use of antidepressants adequate in the 12 months prior to suicide? 45.7 40.0 14.3Was clinician use of antipsychotics adequate in the 12 months prior to suicide? 62.9 25.7 11.4Was patient adherence to treatment satisfactory in the 4 weeks prior to suicide? 44.1 47.1 8.8Source: Keks et al (2003).
Box 1: Personal story: Suicide is Painless?‘Suicide is painless, it brings on many changes’. These lyrics from the M*A*S*H theme had stuck in my mindever since I had started to watch the TV show and of course, the original film. It seemed to me that the secondpart of the phrase was patently true, but was the first part? Until the late 1990s it was only a theoretical questionto me but then things changed dramatically in what felt to me to be a very short time.
At the time I was working in a job I hated, under a lot of pressure in it. I had financial problems because I hadresigned from another job at short notice without securing an alternative one previously and just felt that nothingI did was any good or worthwhile… I had reached the end of my tether. I just couldn't go on any longer. My wifeand family and everyone I knew would be far better off without me. If I was dead, the insurance money wouldsolve the financial problems and my wife and family wouldn't have to put up with a loser like me. So I started,coolly and rationally, to plan my options for a successful exit. I had just resigned from the job I hated so I hadplenty of time to check things out. The last thing I wanted was to be unsuccessful so the method chosen had tohave a high probability of success without the danger of being thwarted at the last minute. At the end of thesedeliberations I decided to shoot myself and as I had two rifles at home, the means were readily at hand. I thengot myself ready, checked out my rifle and decided where I would do it.
That's the point where I found out that suicide isn't painless! Oh, I wouldn't feel much, I knew all about whereexactly to place the round to be removed from the pain and worthlessness I was feeling… and having worked inthe emergency services for over 16 years I knew plenty about the results of self-inflicted injuries for it towork…Then it struck me! I remembered the sight of my first fatality and how messy a violent death is to thosehaving to deal with it. I had a vision of my wife and kids coming into the room and finding me and I saw the lookthat would have been on their faces. That is what saved me. I unloaded the rifle and put the round away andwent for a walk. During that walk aimlessly around, I found myself at the medical surgery where my wifeworked, walked in and found that there was a spare appointment with a doctor that I had never seen. That wasthe turning point – it led to initial treatment for depression and eventually to a bipolar diagnosis and treatment.
No! Suicide isn't painless! Those you leave behind suffer for the rest of their lives wondering why. Often notunderstanding how it could happen, what they had done or not done, for you to think that this was your onlyoption.
Graham Brown, October 20024
3 The study was conducted in Victoria using ‘psychiatric autopsy’ method to identify, from the total 3,752 suicides over the period,35 people with bipolar disorder (22 men, 13 women) aged an average 40.3 years (SE=1.8). Duration of illness averaged 11.9years (SE=1.1). The expert panel used APA Guidelines as the benchmark.4 Graham’s personal story is available on www.bipolarworld.net/Stories/graham.htm Graham has lived in Australia since age 16and was diagnosed with bipolar disorder at age 51 after three decades of undiagnosed symptoms.

Access Economics | SANE Australia Bipolar disorder: Costs
11
‘I felt good, because I felt that I wasin safe hands and that Dr Z would
know what to do.’
Jonathon, on receiving diagnosis
One third ofAustralians withbipolar disorder
do not receiveany treatment.
2.3 Prevention, treatment and careWith early and ongoing treatment, people with bipolar disorder can live in the community and leadrelatively normal lives. However, treatment of bipolar disorder can be difficult, due to the complexity andvariability of the illness (Muller-Oerlinghausen et al, 2002). Treatment goals include rapid, effectiveamelioration of acute episodes, prevention of recurrences, enhancement of social and vocationalfunctioning and reduction in the incidence of suicidal acts.To this end, the following sections look briefly at preventiveinterventions (including earlier diagnosis and prophylacticinterventions), pharmacotherapies, medical and specialistservices including psychotherapy and electroconvulsivetherapy (ECT), hospital services— both inpatient andoutpatient, community mental health services and otherpsychosocial and allied health services, such as counsellingand occupational therapy.
However, many people with bipolar disorder in Australia are not accessingtreatment. The Australian Bureau of Statistics 1998 report, Mental Health andWellbeing – Profile of Adults, Australia, found that as many as 60% of peoplewith mental illness are not using the services available.5 Mitchell, Slade andAndrews (2003) report that 32% of people with bipolar disorder are notreceiving any treatment (including information about mental illness, medicines,psychotherapy, CBT, counselling or other non-specific treatments).
Barwon Health conducted an Australian study of prescription patterns in bipolar disorder, and found thateven in academic setting, there was substantial divergence of treatment from established guidelines,particularly with regard to underutilisation of mood stabilisers. Their findings are currently submitted forpublication. Australian expert Professor Michael Berk comments:
I believe that bipolar is perhaps one of the most difficult disorders to treat. However, currently,Australians with bipolar disorder are prone to 'fall between the stools' in accessing treatmentservices. Part of the reason for this is that the public system tends to focus on the treatment ofsevere psychosis, such as schizophrenia (which ironically has a very simple therapeuticalgorithm), while the private system is more geared to treating affective disorders such asdepression. As a consequence, people with bipolar disorder can find themselves 'pingponging'between the sectors, with problems resulting in continuity of care. This can lead to problems withadherence to treatment and other difficulties, reinforcing the undertreatment cycle. Furthermore,the policy of devolving responsibility for the care of mood disorders into the primary care sectordoes not serve people with bipolar disorders well at present, particularly because of diagnosisproblems.
2.3.1 Preventive interventionsPrimary prevention to reduce the onset of bipolar disorder is limited because causation and risk factorsare not sufficiently understood. More research is required in this area. Where possible, those with a familyhistory of the illness should be informed of the risk, symptoms and treatability of the disorder, to enable anearly diagnosis to be made if required and rapid symptomatic relief to be attained.
Secondary prevention aims at early diagnosis of bipolar disorder as well as early detection andtreatment of episodic triggers. Long term preventive (prophylactic) treatment is almost always indicated,including adhering to medication, to prevent recurrence of episodes and minimise their severity. Manysuccessful psychosocial strategies for secondary prevention are also available such as wellness
5 In the US, people who receive treatment for mental illness are estimated to comprise only 15% of people with mental illness(US Department of Health and Human Services, 1999).

Access Economics | SANE Australia Bipolar disorder: Costs
12
monitoring (eg, sleep hygiene and exercise) and avoidance of jet lag. Kelly (2000) in a practical chapterentitled ‘The Art of Rollercoaster Riding’ outlines a five-step self-help strategy for staying well:
– Step 1: Telling the difference between illness and a ‘bad day’ – utilising a checklist approachmonitoring factors such as caffeine, alcohol, tobacco, weather, hormonal cycle and other stressors;
– Step 2: Using mood, activity and thinking to identify ‘signposts’ – these need to be concrete andspecific, recorded and evaluated, and ‘signpost-spotting with a trusted friend’ is recommended;
– Step 3: Creating brakes and safety nets – set these up when well so that if/when signposts becomeevident, intervention can begin straight away, for example increasing medication doses, avoiding ‘high-risk’ stressors, taking time off work, getting home help or healing therapy and practical steps such asmaking a list and not doing anything not on the list (mania) or calling emergency help numbers(depression);
– Step 4: Strategies for staying well – ‘get regular sleep; eat a balanced diet; stop drinking to killpain/restlessness/isolation; pay attention to physical health and seek treatment from medical andalternative therapies; get enough exercise; get involved in important issues, jobs or your personalvision; pay attention to the spiritual dimension if relevant; and get into some mainstream activities’;
– Step 5: Let time do its work – each individual must learn from their own unique experience how toapply brakes and set up safety nets; ‘let the passing of time teach you your recovery’.
Suicide prevention: Suicide is one of the top three causes of death for people aged 15-35. Suicide rateshave increased 60% worldwide in the past 45 years, with one death now every 40 seconds. Suicideattempts are 20 times more frequent (one every two seconds) than completed suicides. Moreover, mentaldisorders are associated with 90% of suicides (WHO, 2002).
For people with bipolar disorder, there is substantial evidence of lower suicidal risk during long-termlithium treatment. However, diagnosis and timely therapeutic interventions reach only a minority of peoplewith bipolar disorder at risk for suicide (Baldessarini and Jamison, 1999). It is thus important to adopt:
– multi-sectoral approaches – eg, community crisis centres, crisis phone lines, GP training, school-basedinterventions, mentoring programs, family involvement (often it is only family or friends who are awareof risk factors emerging, such as talking about suicide);
– education and awareness programs – eg, crisis management, self-esteem enhancement, coping skills,healthy decision-making, group therapies; in the case of bipolar disorder, improved public andprofessional awareness of risk factors for suicide and of high risk times and people;
– restriction of access to common methods of suicide eg, firearms (and avoidance of media reporting ofthe detail of suicides);
– adequate and early access to clinical assessment and to safe and effective treatments forcomorbidities such as alcohol and substance abuse; and
– research to clarify specific benefits and risks of medical treatments and social interventions aimed atpreventing suicide.
2.3.2. PharmacotherapiesTreatment of bipolar disorder involves pharmacotherapy (with psychotherapies), in both acute episodes(antipsychotic/antidepressant therapy possibly with ECT) and during prophylaxis. Antipsychotics arecommonly and appropriately used as adjuncts to the mood stabilisers in all phases of the illness.The treatment algorithm is illustrated in the following box diagram.

Access Economics | SANE Australia Bipolar disorder: Costs
13
Acute mania is treated with a mood stabiliser. The first-line mood stabiliser is lithium, where evidence foreffectiveness is strong and confirmed in several meta-analyses and where the response rate is around79% (Compton & Nemeroff, 2000). Lithium salts also have well documented anti-suicidal effects (Muller-Oerlinghausen et al, 2002).
The benefits of lithium as a treatment for bipolar were discovered in 1948 by Australian psychiatrist DrJohn Cade. By the 1970s lithium had become the mainstay of treatment for bipolar disorder. The USNational Institute of Health estimate that lithium treatment for bipolar disorder saves over US$9!billion peryear in hospital spending there (NIH, 2000).
People on lithium therapy should have both their serum lithium concentration and thyroid functionmonitored and, to avoid toxic effects6, the lithium dose should be titrated to achieve a desirable serumconcentration. Two anticonvulsants, valproate and carbamazepine, are of similar efficacy to lithium;olanzapine is more effective than placebo and possibly also valproate (Mitchell et al, 2003). Because ofthe lagged effect (around one week) of mood stabilisers, administration of an antipsychotic (eg,risperidone, olanzapine, chlorpromazine, thiorodazine, haloperidol) or benzodiazepine (eg, diazepam,clonazepam, lorazepam7) is used in the interim.
The best evidence for treatment of mixed episodes is valproate, evidence for carbamazepine is weak andlithium may also be used as second-line therapy if the person is refractive to anticonvulsants. Olanzapinecan also be effective (Mitchell et al, 2003).8 Following resolution of the manic or mixed episode, the anti-psychotic is withdrawn but the mood stabiliser should be continued for at least six months.
For depression, lamotrigine is currently the only agent approved for use in the prevention of depressiveepisodes in patients with bipolar disorder. For breakthrough episodes, lithium is again first-line therapy.If unsuccessful, lamotrigine (also sometimes a first-line therapy) or valproate (especially in rapid cycling)are trialled. For people who are not psychotic, suicidal or hospitalised, a mood stabiliser may be sufficient,although slow onset of action may require interim administration of an antidepressant. Concurrentantidepressant use can enhance efficacy; Mitchell et al (2003) recommend selective serotonin reuptakeinhibitors (SSRIs) and venlafaxine as the first-line choice, with monoamine oxidase inhibitors (MAOIs) andtricyclic antidepressants (TCAs) as second-line. Antidepressant monotherapy may induce mania or rapidcycling, so if this is a risk a second mood stabiliser can be added instead (lamotrigine at reduced dose).On remission, antidepressants are tapered to minimise the risk of switching.
6 Signs of toxicity include loss of appetite, nausea/vomiting, abdominal pain, diarrhoea, staggering, slurred speech, marked tremorand agitation. Side-effects of lithium itself include slowed thinking, weight gain, poor coordination, dry skin/acne, thirst, a sense of‘flatness’, blunted creativity, thyroid problems and urinary frequency (Kelly, 2000, p43-44). Many people find lithium’s side-effectsunacceptable so do not comply with long term treatment (Simpson and Jamison, 1999).7 Clonazepam and lorazepam may be helpful adjuncts for insomnia.8 If the person with bipolar disorder initially fails to respond to pharmacological intervention in a manic or mixed episode, optionsare to increase the dose, to switch to another mood stabiliser, to combine mood stabilisers or to add an adjunctive anti-psychotic.The strongest evidence is for the last, augmenting the mood stabiliser with risperidone or haloperidol, with the second-line optionbeing combination therapy (Mitchell et al, 2003).
Mania/Hypomania
Depression
Prophylaxis
Mania/Hypomania
Depression
Acute Treatment
for breakthroughepisodes
Bipolar disorder
No Bipolar disorder

Access Economics | SANE Australia Bipolar disorder: Costs
14
40% of Australians withbipolar disorder are not
receiving medication.
Notwithstanding under-treatment, Australians with
bipolar disorder use over tentimes the average number of
mental health services
In the prophylactic period, two meta-analyses (including one Cochrane) strongly support lithium’susefulness for people who are not rapid cycling (Mitchell et al, 2003). For people who are rapid cycling,there is no convincing trial evidence that mood stabilisers are robustly effective, although valproate hasthe most evidence. Renal function should be monitored every 3-6 months and thyroid function every 6-12months. If lithium is to be discontinued, it should occur slowly over 1-2!months.
People with bipolar disorder have a high rate of non-adherence topharmacotherapy, estimated at 32–45% of treated patients(Rothbaum & Astin, 2000). Mitchell, Slade and Andrews (2003)found that 40% of Australians with bipolar disorder are not receivingmedication.
2.3.3 Medical, family and other psychosocial interventionsEffective treatment for people with bipolar disorder and their carers includes ongoing clinical support(primary and specialist psychiatric care, hospital and community services), education about the illness andhow to deal with it, psychosocial rehabilitation and a range of other services to enable independent living.
Medical services: Australians with bipolar disorder in Australia are significantly more likely to consult ahealth professional, including specialists (Mitchell, Slade and Andrews, 2003). 70% of people with bipolardisorder were consulting a doctor, specialist, nurse, mental health team, chemist, counsellor or otherhealth professional for their mental health problem, as opposed to 7.2% in the population generally.Thirty-three per cent were specifically consulting a mental health professional for their mental healthproblem, as opposed to 1.7% in the general population.
In Australia the GP is often the first contact for a person withbipolar disorder, although GPs can face constraints in beingable to accurately diagnose bipolar disorder, as well as withongoing treatment and care, particularly suicide preventionstrategies. Specialist and community mental health supportservices and education for GPs, as well as removal of theremunerative disincentives for longer consultations in the MBSstructure, could be beneficial.
Psychiatrists are referred to for specialist diagnosis and for ongoing pharmacological, psychosocial andother care management, particularly in acute phases, together with the GP and/or other carers. Combiningpsychotherapy with pharmacotherapy can assist in increasing the patients’ adherence to prescribedmedication, may reduce the number and length of hospitalisations and relapses, increase socialfunctioning, improve quality of life and reduce the person’s suicide risk (Rothbaum and Astin, 2000).There are different psychotherapeutic approaches, appropriate to different stages, which can includepsychoeducation, cognitive behavioural therapy (CBT), family interventions, group therapy and therapyspecific to an individual case, such as therapy for substance abuse (see below).
Electroconvulsive therapy (ECT) can be helpful in treating severe depression and/or mixed mania thatdoes not respond to medications, or for people who are especially delusional or at a high risk of suicide.Today ECT is administered after an injection of a muscle relaxant and a general anaesthetic, so it nolonger resembles the barbaric unsedated practice first introduced to Australia in the 1940s. Nonetheless,there can still be temporary unwanted effects on memory and other brain functions and ECT remains verylow in most treatment algorithms, due to ongoing public concerns (Compton & Nemeroff, 2000).Kelly (2000) colourfully describes a variety of personal responses to ECT treatment in Australia, rangingfrom unhelpful to: ‘Next time I get depressed, no mucking around. I’m having ECT straight away, it worksso fast’ (Mary). Lithium treatment is not recommended with ECT as it may be neurotoxic.
Community mental health services: It is generally preferable for people to be treated in their homesurroundings under the care of a Community Mental Health Service, with a specialist local clinic andmobile teams of mental health workers. If needed, longer term support providing help with day-to-day

Access Economics | SANE Australia Bipolar disorder: Costs
15
activities may also be available, and is often supplied by community organisations (see SANE Australia,2003, p16). Non-residential services provide assessment, treatment, rehabilitation and care for non-admitted patients. Residential services are 24-hour staffed units established in community settings thatprovide specialised treatment, rehabilitation or care for people with bipolar disorder or other psychiatricdisability (AIHW, 2002a).9 The increasing reliance on community mental health services and socialsupports goes hand in hand with briefer and fewer hospital admissions.
Hospitalisation is necessary in acute cases of bipolar disorder, with the first episode, during relapse andwhen risk of suicide (or risk to others) is high. A US survey of Depression and Bipolar Support Alliance(DBSA) members found 88% of individuals with bipolar disorder had been hospitalised at least once andthat 66% had been hospitalised twice or more (Lish et al, 1994). In Australia, the average length of stay(ALOS) in hospital for bipolar disorder in Australia is now only 14.8 days10, although some severeepisodes require lengthy hospitalisations.
‘It was the worst depression I’d ever had. I was totally withdrawn… I went back to my parents’ place… andI’d been there five, six, seven days (I don’t really know how long) without eating or drinking. That led to analmighty chase through the bush and I was carted off to Larundel… I was admitted to Larundel onChristmas Eve 1978… I was there for eight months…’ Greg
Psycho-education: aims to help people and their families identify relapse symptoms, develop copingstrategies, understand the course of bipolar disorder, promote treatment adherence, deter drug abuse anddispel stigma. Useful techniques such as constructing a life chart of mood symptoms, medications, and lifeevents may help the person, their carer and their key health care professional to treat the illness optimally.One effectiveness evaluation showed a 50% improvement in lithium compliance and a 60% decrease inhospitalisation (Rothbaum & Astin, 2000).
Cognitive behavioural therapy (CBT): The main aim of CBT is to help a person to adjust negativethought patterns, understand how such patterns contribute to their symptoms and develop techniques toaddress specific thoughts and behaviour. CBT can be useful to help counter suicidal thoughts and, in acombination model with medication, its beneficial impacts are being further studied at the Mood DisordersUnit at the Prince of Wales Hospital, Sydney (University of New South Wales, 2002).
Family therapy: Family and marital interactions may be dysfunctional or strained for people with bipolardisorder, which may impede functioning and trigger relapse. Family therapy aims to assist people and theirfamilies to improve understanding and acceptance of the illness, to enhance social and occupationalfunctioning (eg, through improved communication and problem-solving skills), to manage stressors andunderlying issues (eg, violence, abuse) and to address any post-traumatic symptoms that the patientand/or their family may have after an acute or hospitalised period. Families may be taught to identify signsof a relapse and how to prepare effectively for episodes, including non-judgemental support, boundaries,specific strategies and debriefing (Rothbaum & Astin, 2000).
Group therapy helps decrease stigma, resolve problems and increases support for people with bipolardisorder and their families and carers. People who have combined group therapy and medication canhave a less severe course of illness than people receiving medication alone in terms of family and maritalinteractions and the need for readmission to hospital. One study showed a 15% reduction in the number ofrelapses, in part because of a positive impact on treatment adherence (Rothbaum & Astin, 2000).
Vocational rehabilitation and occupational therapy can assist people with bipolar disorder to retainemployment. Vocational counsellors, through tests and interviews, can help identify issues that causeproblems in attaining educational goals or retaining employment and can suggest techniques formanaging such issues – eg, negotiating more flexible work or study arrangements, such as havingassignments brought to hospital (Kelly, 2000) – or alternative career paths that may prove more positive.
9 Models of 24-hour supported accommodation services and their costs are outlined in SANE Australia (1997).10 AIHW hospital datacubes for U-68B.

Access Economics | SANE Australia Bipolar disorder: Costs
16
Only 17% of people witha psychiatric disabilityaccess psychosocial
rehabilitation programs.
Psychosocial rehabilitation: Rehabilitation refers to the servicesand technologies made available to disabled people so they canadapt to their world, and has three stages – assessment, planningand intervention. Benefits include reduction in the frequency andseverity of symptoms, savings to public health systems, improvedquality of life and respite for carers and support for the carerrelationship. SANE Australia (2001) details two broad approaches to providing rehabilitation – the LivingSkills Centre approach and the Day Program approach, as well as principles for good practice in Australia.State health departments are now the main practical source of funding for such programs, which aim toachieve community integration, independence and rewarding relationships, using social and living skillstraining. SANE Australia’s Gap Project, commissioned by the Commonwealth Government in 1998, foundthat there is a ‘rehabilitation gap’, with over 80% of those who might benefit from psychosocialrehabilitation not attending programs. The study found that in the great majority of cases (92%),psychiatrists did not refer for rehabilitation and indeed only 17% of people with a psychiatric disabilityattended programs. ‘Given the demonstrated effectiveness of rehabilitation, this represents an enormousopportunity to improve the quality of life and health outcomes of a great many people living with mentalillness’ (SANE Australia, 2001, p5).
There is still a great unmet need in Australia for all of these psychosocial interventions for people withbipolar disorder. There is a lack of programs and a lack of choice, particularly outside the Sydney andMelbourne metropolitan areas (Access Economics, 2002).
Access Economics | SANE Australia Bipolar disorder: Costs
17
There are nearly 100,000Australians with bipolar
disorder in 2003, 0.5% ofthe population, declining
with age but roughlyequal across genders.
3 Prevalence and Direct Health Costs
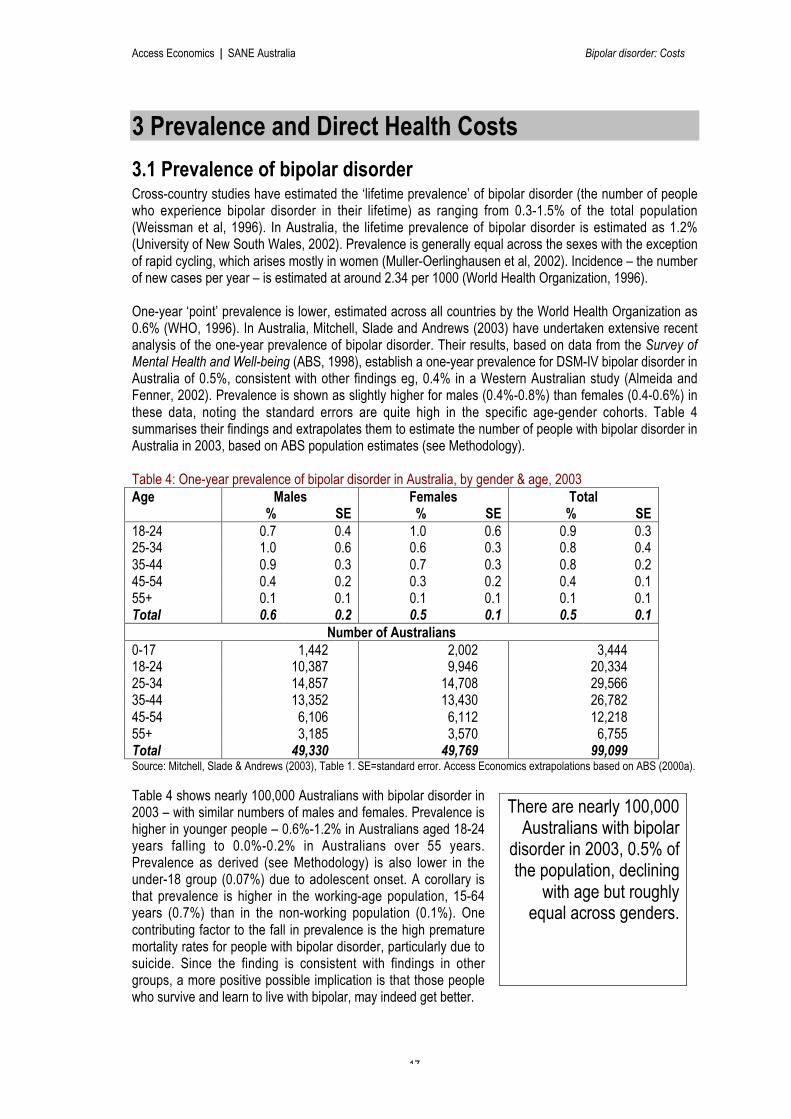
3.1 Prevalence of bipolar disorderCross-country studies have estimated the ‘lifetime prevalence’ of bipolar disorder (the number of peoplewho experience bipolar disorder in their lifetime) as ranging from 0.3-1.5% of the total population(Weissman et al, 1996). In Australia, the lifetime prevalence of bipolar disorder is estimated as 1.2%(University of New South Wales, 2002). Prevalence is generally equal across the sexes with the exceptionof rapid cycling, which arises mostly in women (Muller-Oerlinghausen et al, 2002). Incidence – the numberof new cases per year – is estimated at around 2.34 per 1000 (World Health Organization, 1996).
One-year ‘point’ prevalence is lower, estimated across all countries by the World Health Organization as0.6% (WHO, 1996). In Australia, Mitchell, Slade and Andrews (2003) have undertaken extensive recentanalysis of the one-year prevalence of bipolar disorder. Their results, based on data from the Survey ofMental Health and Well-being (ABS, 1998), establish a one-year prevalence for DSM-IV bipolar disorder inAustralia of 0.5%, consistent with other findings eg, 0.4% in a Western Australian study (Almeida andFenner, 2002). Prevalence is shown as slightly higher for males (0.4%-0.8%) than females (0.4-0.6%) inthese data, noting the standard errors are quite high in the specific age-gender cohorts. Table 4summarises their findings and extrapolates them to estimate the number of people with bipolar disorder inAustralia in 2003, based on ABS population estimates (see Methodology).
Table 4: One-year prevalence of bipolar disorder in Australia, by gender & age, 2003Age Males Females Total
% SE % SE % SE18-24 0.7 0.4 1.0 0.6 0.9 0.325-34 1.0 0.6 0.6 0.3 0.8 0.435-44 0.9 0.3 0.7 0.3 0.8 0.245-54 0.4 0.2 0.3 0.2 0.4 0.155+ 0.1 0.1 0.1 0.1 0.1 0.1Total 0.6 0.2 0.5 0.1 0.5 0.1
Number of Australians0-17 1,442 2,002 3,44418-24 10,387 9,946 20,33425-34 14,857 14,708 29,56635-44 13,352 13,430 26,78245-54 6,106 6,112 12,21855+ 3,185 3,570 6,755Total 49,330 49,769 99,099Source: Mitchell, Slade & Andrews (2003), Table 1. SE=standard error. Access Economics extrapolations based on ABS (2000a).
Table 4 shows nearly 100,000 Australians with bipolar disorder in2003 – with similar numbers of males and females. Prevalence ishigher in younger people – 0.6%-1.2% in Australians aged 18-24years falling to 0.0%-0.2% in Australians over 55 years.Prevalence as derived (see Methodology) is also lower in theunder-18 group (0.07%) due to adolescent onset. A corollary isthat prevalence is higher in the working-age population, 15-64years (0.7%) than in the non-working population (0.1%). Onecontributing factor to the fall in prevalence is the high prematuremortality rates for people with bipolar disorder, particularly due tosuicide. Since the finding is consistent with findings in othergroups, a more positive possible implication is that those peoplewho survive and learn to live with bipolar, may indeed get better.

Access Economics | SANE Australia Bipolar disorder: Costs
18
-
5
10
15
20
25
30
35
40
15-24 25-34 35-44 45-54 55-64 65-74 75+ Allages
De
ath
s p
er
10
0,0
00
Males
Females
Total
-
5
10
15
20
25
30
1921
1925
1929
1933
1937
1941
1945
1949
1953
1957
1961
1965
1969
1973
1977
1981
1985
1989
1993
1997
2001
De
ath
s p
er
10
0,0
00
Total
Males
Females
Rurality: The ABS National Survey of Mental Health and Wellbeing data show no significance differencebetween Australians with bipolar disorder and the general population in terms of whether they live in urbanor rural areas (Mitchell, Slade and Andrews, 2003).
3.2 Prevalence of suicides related to bipolar disorderSuicide continues to be a major public health issue. Across the world, over a million people will die thisyear from suicide. It is one of the top ten causes of death in every country. The psychological, social andfinancial impact of suicide on the family and community is enormous (WHO, 2002).
Over 2,000 Australians committed suicide every year in the 1990s. In 2001 there were 2,454 deaths fromsuicide, with males continuing to outnumber females approximately 4:1 – 1,935 men and 519 women(ABS, 2003b). Chart!1 depicts the growth in Australian suicide rates – which have again reached the highlevels of the 1920s, having risen steadily over the post-war period – together with Australian demographicpattern of suicides. Suicides in the 25-34 age group predominate, followed by those in the 35-44 agegroup. Nearly half (47%) of all suicides are people aged 25-44.
Chart 1: Increase in age-standardised suicide rates 1921-2001, and rates by age & gender 2001, Australia
Source: Derived from ABS (2000b) and ABS (2003b).
The Northern Territory continues to have the highest age-standardised suicide rate in Australia (22.6 per100,000 people), with the lowest rates in Victoria in 2001 (11.0). In 2001, 42.8% of Australian suicideswere by hanging (including strangulation and suffocation), 11.6% by drug poisoning and 20.9% by otherpoisoning (eg!motor vehicle exhaust), 10.7% used firearms (a significant fall over the 1990s) and 14.0%used other methods. For people aged 1 to 75, suicide accounted for 5.5% of male deaths and 2.5% offemale deaths, as well as 4.4% of all potential life lost due to premature death in 2001 (ABS, 2003b).

Access Economics | SANE Australia Bipolar disorder: Costs
19
Nearly 1 in 8suicides are ofsomeone with
bipolardisorder.
Table 5: Suicides, Australia, by age & gender, 2001Males Females Total
Number% totaldeaths
Per100,000 Number
% totaldeaths
Per100,000 Number
Per100,000
15-24 276 25% 20.3 63 16% 4.8 339 12.725-34 486 30% 33.9 108 18% 7.4 594 20.635-44 447 20% 30.2 118 9% 7.8 565 18.945-54 311 8% 23.3 106 4% 7.9 417 15.655-64 175 2% 18.9 48 1% 5.3 223 12.165-74 127 <1% 19.9 33 <1% 4.8 160 12.175+ 107 <1% 24.4 38 <1% 5.6 145 13.0All ages 1,935 5.5% 20.1 519 2.5% 5.1 2,454 12.5Source: ABS (2003b).
Suicide rates amongst people with bipolar disorder are at least 12 times higher than those expected in thegeneral population, even higher if comorbid substance abuse is taken into account (Harris andBarraclough, 1997).11 Multiplying the suicide rate by a factor of 12 and then by the number of people withbipolar disorder in 2003 thus provides an estimate of the number of suicides in 2003 due specifically to theillness. This, however, is lower than the number of people with bipolar disorder who suicide – as a result ofcomorbid suicide risk factors including substance abuse and other mental illnesses. Section 2.2 showedlifetime prevalence as 15% or 0.3% annual overall prevalence, assuming an average ‘lifetime’ of theillness of 50 years (see Methodology). Table 6 provides a summary.
Table 6: Estimated suicides due to bipolar disorder, Australia, 2003No. of suicides of people with BD % of total suicides % of total people with BD
Males Females People Males Females People Males Females People 15-24 39 9 48 14% 14% 14% 0.37% 0.09% 0.23% 25-34 91 20 110 19% 18% 18% 0.61% 0.13% 0.37% 35-44 73 19 91 16% 16% 16% 0.54% 0.14% 0.34% 45-54 26 9 34 8% 8% 8% 0.42% 0.14% 0.28% 55+ 11 3 15 3% 3% 3% 0.34% 0.10% 0.22% Total 239 59 298 12% 11% 12% 0.48% 0.12% 0.30%
No. of suicides due to BD only % of total suicides % of total people with BDMales Females People Males Females People Males Females People
15-24 26 6 32 9% 9% 9% 0.24% 0.06% 0.15% 25-34 60 13 73 12% 12% 12% 0.41% 0.09% 0.25% 35-44 48 13 61 11% 11% 11% 0.36% 0.09% 0.23% 45-54 17 6 23 5% 5% 5% 0.28% 0.09% 0.19% 55+ 7 2 10 2% 2% 2% 0.23% 0.06% 0.15% Total 159 40 198 8% 8% 8% 0.32% 0.08% 0.20%
In total there are estimated to be 298 people with bipolar disorder in 2003 whocommit suicide, with 198 (two thirds) of these suicides solely due to the illnessitself. The other 100 deaths can be attributed to comorbid substance abuse andother mental illness in people who have bipolar disorder. Of the total with bipolardisorder, there are an estimated 239 males and 59 females. Over half of thedeaths (55%) are men with bipolar disorder aged 25 to 44, while 48 are peoplewith bipolar disorder under 24 years old, representing 14% of deaths by suicidefor people in this age group. Overall, suicides of people with bipolar disorderrepresent 12% (nearly 1 in 8) of total suicides in Australia; 8% of total suicides aredirectly attributable to the disease.
11 University of New South Wales (2002) cite 15 times the suicide risk for people with bipolar disorder. Meta-analyses by Harrisand Barraclough (1997) found that alcohol abuse/dependence increases the risk of suicide 5.5 times, opioid abuse/dependence10 times and schizophrenia 9 times, among other results.

Access Economics | SANE Australia Bipolar disorder: Costs
20
As noted in Section 2.2, Keks et al (2003) evaluated Victorian data on all deaths by suicide over 1993 to2001 to determine that at least 3512 of the 3,752 people included died due to bipolar disorder.The percentage of women who completed suicide (37%) was higher than in the general population, andthe average age was also higher (40.3 years). The study supports other evidence that risk factors forpeople with bipolar disorder who suicide are:
– a previous suicide attempt (86%);
– depressed (87%) and mixed (10%) episodes, in the 86% of cases where the phase was identified;
– lifetime manifestation of psychosis – 63% compared to 58% overall in bipolar disorder (Goodwin andJamison, 1990);
– alcohol/drug abuse – 63% had abused alcohol and 31% substances in their lifetime; 31% were abusingalcohol and 23% substances in recent history; 29% were intoxicated at the time of suicide;
– recent hospitalisation – 14% were inpatients and 26% suicided within 6 weeks of discharge; treatmentwas assessed as inadequate in 60% of inpatient deaths and in 44% of the latter group; and
– men predominated (63%).
Contrary to previous studies, only 14% suicided in the early stage (first five years) of illness and the meanage (40 years) does not support the contention that young people are over-represented in bipolar suicides.Other characteristics of the people who died were:
– only 17% were in paid employment;
– 31% were in a relationship; 40% had separated; 3% were widowed and 26% had never married;
– 20% had a tertiary qualification and 46% had completed secondary schooling;
– 46% committed suicide by hanging, 20% by carbon monoxide poisoning, 14% by overdose ofprescribed medication, 14% jumped in front of moving vehicles and 6% jumped from a height.
Factors that may have contributed to the death (or failed to prevent it), include:
– prior to death, hopelessness was expressed by 81% and psychomotor agitation observed in 54%;
– significant life stressors for 77% in the 12 months prior to death, and for 46% in the last 4 weeks;
– where insight could be determined, it was at least moderately impaired in 92% of suicides;
– problems of adherence to treatment in 47% in the 4 weeks prior, including inadequatepharmacotherapy (38%) and inadequate follow-up (33%); in cases where mood stabilisers wereneeded but not prescribed, a common reason for non-prescription was an assessment that the patientwould not reliably adhere to treatments; in other cases the doses of prescribed drugs were too low andhad not been appropriately adjusted during treatment.
‘Our study found a high frequency of less than satisfactory treatment in cases of bipolar suicide. Problemswith monitoring clinical state during the terminal phase of illness were particularly striking… The mentalstate of patients during the terminal illness phase was found not to have been adequately monitored in60% of the patients. Changes in patients’ clinical state had also not received adequate clinical interventionin 60% of cases.’
Keks et al (2003).
Treatment implications from these findings are discussed in the Conclusions Section.
12 To be counted, all criteria had to be met, including a recorded robust diagnosis of bipolar disorder and clinical and otherrecords (eg, educational attainment) that could enable a case history to be established. Clearly then, the suicide ‘rate’ (just under1%) is significantly understated.

Access Economics | SANE Australia Bipolar disorder: Costs
21
3.3 Direct costs of bipolar disorder: 2003Direct health system costs can be estimated in one of two ways:
1 the ‘top-down’ approach, which attributes total health expenditures to disease based on availableinformation on the mix of diseases treated and the types of treatment; or
2 the ‘bottom up’ approach, calculated by adding actual (or imputed) average treatment expenditures fora representative cohort of patients.
The advantage of the first approach is that there will be consistency of coverage and estimates acrossdiseases, which can be more helpful for policy makers. In Australia, such attribution has been undertakenby the Australian Institute of Health and Welfare (AIHW) utilising DCIS prevalence-based methodology(see Methodology section). However, the second approach can be useful in identifying up-to-the-minuteestimates for specific diseases, although there can be problems in obtaining representative samples,representative expenditures and in distinguishing between ‘ideal’ treatment patterns and ‘real world’treatment patterns.
In this report, both methods were utilised, generating some interesting results.
3.3.1 The top-down approachTable 7 shows that, using the AIHW’s top-down methodology, affective disorders (depression and bipolardisorder) were the second most expensive mental health item in Australia in 1993-94, after dementia.Separating out diagnosed bipolar disorder from affective disorders shows that expenditure on bipolardisorder in 1993-94 was $82m or 2.7% of all mental health expenditure.
Table 7: Direct costs of bipolar disorder and other mental disorders, Australia, 1993-94, top-down
$m Hospital MedicalPharma-
ceuticals
Otherhealth
services Other Total% ofTotal
Dementia 110 11 2 9 582 714 23.6%Affective disorders 217 141 68 70 148 644 21.3% Of which Bipolar Disorder 41 3 2 16 19 82 2.7%Schizophrenia 275 26 8 106 40 454 15.0%Substance abuse disorders 136 46 12 18 136 348 11.5%Anxiety disorders 24 102 51 25 37 239 7.9%Behavioural syndromes & other mental disorders 17 53 45 9 50 174 5.8%Other non-drug psychosis 63 5 1 6 53 128 4.2%Stress and adjustment disorders 28 27 7 31 19 112 3.7%Disorders of childhood and adolescence 10 9 1 19 16 55 1.8%Personality disorders 24 7 1 12 9 53 1.8%Eating disorders 14 3 0 1 4 22 0.7%Other mental disorders, prevention & screening 20 9 2 29 16 79 2.6%Total 941 438 199 334 1,110 3,022 100.0%
Source: Derived from Mathers, Vos and Stevenson (1999), Table 6.6, p90, and special data request for bipolar disorder.
Projecting health expenditure on diagnosed bipolar disorder as reported by the AIHW to 2003, using apopulation growth factor of 1.110 and a direct health inflation factor of 1.259 over the period, generates theresults shown in Table 8, with depression as a comparator.

Access Economics | SANE Australia Bipolar disorder: Costs
22
Table 8: Direct costs of bipolar disorder and depression, 1993-94 and 2003, top-down1993-94 ($m) 2003 ($m)
Bipolardisorder Depression
Totalaffective
disordersBipolar
disorder Depression
Totalaffective
disordersHospitals inpatients Psychiatric 4.7 80.3 85.1 6.6 112.3 118.9 Public 29.0 58.8 87.9 40.6 82.2 122.8 Private 7.1 37.0 44.1 9.9 51.7 61.7Out-patients 0.5 12.1 12.6 0.7 17.0 17.7GPs 0.6 35.8 36.5 0.9 50.1 51.0Specialists 2.1 102.0 104.1 3.0 142.6 145.6Pharmaceuticals 1.9 65.6 67.6 2.7 91.8 94.5Other ambulatory services 15.9 41.4 57.2 22.2 57.8 80.0Allied health 0.5 12.4 12.9 0.7 17.4 18.1Nursing homes 15.7 87.1 102.9 22.0 121.8 143.8Research 0.6 7.0 7.5 0.8 9.7 10.5Other 2.8 22.3 25.1 3.9 31.1 35.1Total direct costs 81.6 562.0 643.6 114.1 785.6 899.7
Source: AIHW special data request. In Table 7, ‘hospital’ expenditure equates to the sum of the first four items in Table 8;‘medical’ in Table 7 equates to the sum of ‘GPs’ and ‘specialists’ in Table 8; ‘other health services’ in Table 7 equates to the sumof ‘other ambulatory services’ (ie, non-outpatient ambulatory services) and ‘allied health’ in Table 8; and ‘other’ in Table 7 equatesto the sum of ‘nursing homes’, ‘research’ and ‘other’ in Table 8.
Table 8 shows that, in 2003, a conservative top-down estimate of direct expenditure on bipolar disorder is$114.1m. With prevalence (from Section 3.1) for bipolar disorder in 2003 of 0.5% (99,099 people), thisequates to an average cost per person of $1,151 pa. This is less than half of average health spending percapita in Australia, and would buy less than three days in hospital per year, with no other medical,pharmaceutical or health services.
The improbably low top-down estimate is likely to be due to the substantial problems of diagnosis and highlevels of comorbidity (as discussed in Section 2.1). It is deemed likely that some expenditure on bipolardisorder may have been included in other categories, most probably ‘substance abuse disorders’, ‘othernon-drug psychosis,’ and ‘disorders of childhood and adolescence’, with potentially misdiagnosed bipolaralso appearing in ‘schizophrenia,’ ‘personality disorders’ and ‘eating disorders’. Because of the likelihoodof under-statement, a bottom-up approach was also investigated.
3.3.2 The bottom-up approachThe bottom-up approach was based on clinicians’ assessments of best-practice quality care for peoplewith bipolar disorder. A panel of Australian experts and published articles on clinical guidelines were used,together with MBS, PBS, AN-DRG hospital and other expenditure data to generate average costs fordepressive and manic episodes and prophylaxis, including people who were rapid cycling. The averagenumber of episodes per year assumed is 0.5 (based on Mitchell et al, 2003) and the percentage of peoplerapid cycling (assumed as four half-length cycles per year) is 10% (derived from US Mayo Clinic data).Critical modelling inputs are summarised below, with further detail in the Methodology section.
Depressive episode– Hospital expenditure: 13 days as an inpatient at $436.37 average cost per day (includes the cost of
secure wards); 4 times average usage of Accident and Emergency, which equates to 0.16 visits overthe 90 day episode at $101 per visit; weekly outpatient sessions once out of hospital for 75% of treatedpatients at an average cost of $200 per session.
– Medical expenditure: 2 Level C and 2 Level B GP consultations at $55.95 and $29.45 eachrespectively; 2 one-hour and 3 35-minute specialist psychiatric consultations at $141.90 and $102.80respectively.
– Pharmaceutical expenditure: 1500mg lithium daily throughout the episode and 375mg valproate onlywhile hospitalised at a daily cost of 41 cents and 43 cents respectively.

Access Economics | SANE Australia Bipolar disorder: Costs
23
– Other ambulatory and allied health expenditure: psychosocial rehabilitation services (living skills,counselling occupational therapy etc) fortnightly out of hospital for 25% of treated patients at anaverage cost of $118 per session; diagnostic/pathology costs (blood and serum lithium tests) of $56.35per episode.
– Nursing home, research and other (mainly administrative) expenditure calculated relative to thepercentage shares from the top-down analysis (see Methodology) – 10.8% and 3.5% respectively.
Manic episode– Hospital expenditure: 13 days as an inpatient at $436.37 average cost per day (includes the cost of
secure wards); 3.5 times average usage of Accident and Emergency, which equates to 0.05 visits overthe 35 day episode at $101 per visit; weekly outpatient sessions once out of hospital for 75% of treatedpatients at an average cost of $200 per session.
– Medical expenditure: 2 Level C and 2 Level B GP consultations at $55.95 and $29.45 eachrespectively; 2 one-hour and 4 35-minute specialist psychiatric consultations at $141.90 and $102.80respectively.
– Pharmaceutical expenditure: 1500mg lithium daily throughout episode (41 cents/day), 6.25mgolanzapine only while hospitalised ($6.59/day), and 4mg risperidone only while hospitalised in 50% oftreated patients ($4.65/day for those taking it).
– Other ambulatory and allied health expenditure: psychosocial rehabilitation services (exercise,counselling, occupational therapy etc) fortnightly out of hospital for 25% of treated patients at anaverage cost of $118 per session; diagnostic/pathology costs (blood and serum lithium tests) of $56.35per episode.
– Nursing home, research and other (mainly administrative) expenditure calculated relative to thepercentage shares from the top-down analysis (see Methodology) – 10.8% and 3.5% respectively.
Prophylaxis– Hospital expenditure: no inpatient expenditure due directly to bipolar disorder13; outpatient visits
averaging once per monthly for 75% of people at a cost of $200/session.– Medical expenditure: 1 Level B GP consultation every 8 weeks at $29.45 each; 1 35-minute specialist
psychiatric consultation every eight weeks at $102.80 each.– Pharmaceutical expenditure: up to 1500mg lithium daily at 41 cents/day.– Other ambulatory and allied health expenditure: psychosocial rehabilitation services (exercise,
counselling, occupational therapy etc) every 8 weeks out of hospital for 25% of treated patients at anaverage cost of $118 per session; one set of diagnostic/pathology tests (blood and serum lithium tests)of $56.35.
– Nursing home, research and other (mainly administrative) expenditure calculated relative to thepercentage shares from the top-down analysis (see Methodology) – 10.8% and 3.5% respectively.
Results are shown in Table 9. Using the bottom-up analysis, average direct health expenditure per personwith bipolar disorder is estimated as $12,946 per annum in 2003. This is about 73% of the expenditure perperson with schizophrenia (Access Economics, 2002)14, which concords with Woods (2000), from the YaleUniversity School of Medicine, that ‘costs to society [from bipolar disorder] appear to be roughly 70% ofthose for schizophrenia’. However, the estimate is over 11 times higher than the top-down approach. If thebottom-up numbers for expenditure per treated case were applied to all people with bipolar disorder(99,099 people), total direct expenditure on the illness in Australia would be $1.3!billion, making it moreexpensive than depression and the second largest mental health item, behind dementia (AccessEconomics, 2003)! The next section looks at reasons for, and a reconciliation of, the top-down andbottom-up estimates of direct costs.
13 This may be an understatement since occasional hospitalisations do occur due to treatment complications during prophylaxis.14 The schizophrenia methodology was based on top-down methodology that concords with bottom-up (Carr et al, 2002).
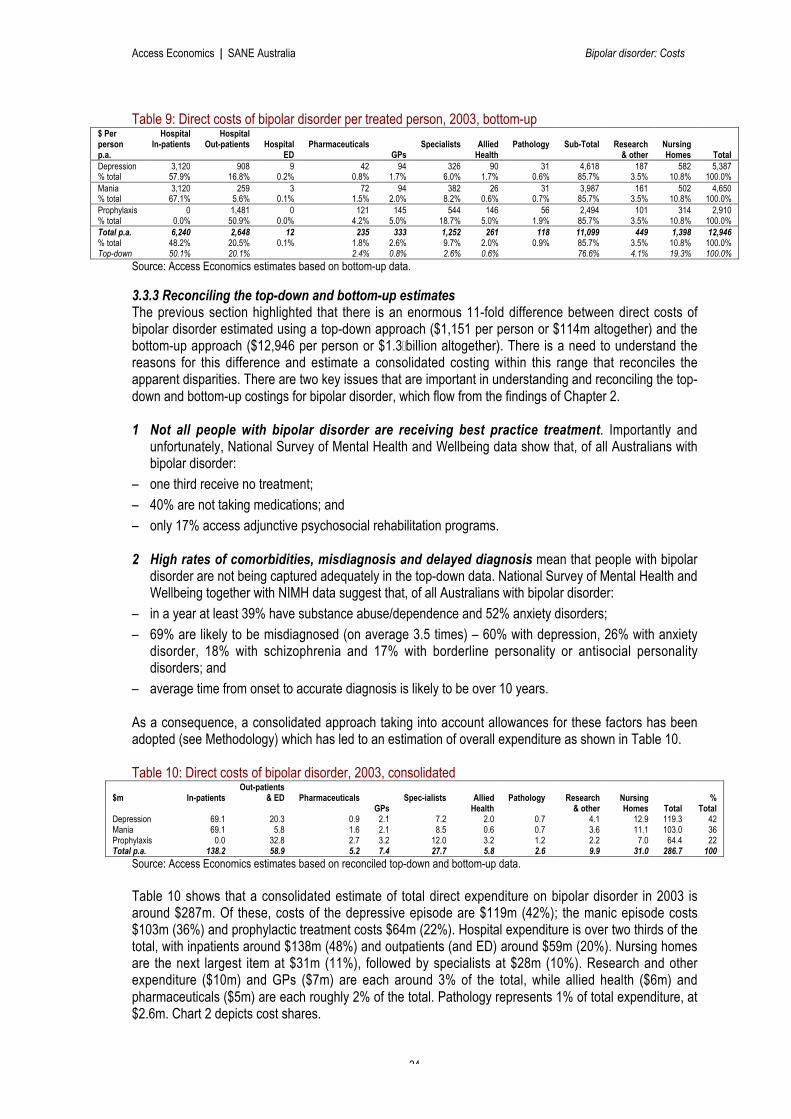
Access Economics | SANE Australia Bipolar disorder: Costs
24
Table 9: Direct costs of bipolar disorder per treated person, 2003, bottom-up$ Perpersonp.a.
HospitalIn-patients
HospitalOut-patients Hospital
EDPharmaceuticals
GPsSpecialists Allied
HealthPathology Sub-Total Research
& otherNursingHomes Total
Depression 3,120 908 9 42 94 326 90 31 4,618 187 582 5,387% total 57.9% 16.8% 0.2% 0.8% 1.7% 6.0% 1.7% 0.6% 85.7% 3.5% 10.8% 100.0%Mania 3,120 259 3 72 94 382 26 31 3,987 161 502 4,650% total 67.1% 5.6% 0.1% 1.5% 2.0% 8.2% 0.6% 0.7% 85.7% 3.5% 10.8% 100.0%Prophylaxis 0 1,481 0 121 145 544 146 56 2,494 101 314 2,910% total 0.0% 50.9% 0.0% 4.2% 5.0% 18.7% 5.0% 1.9% 85.7% 3.5% 10.8% 100.0%Total p.a. 6,240 2,648 12 235 333 1,252 261 118 11,099 449 1,398 12,946% total 48.2% 20.5% 0.1% 1.8% 2.6% 9.7% 2.0% 0.9% 85.7% 3.5% 10.8% 100.0%Top-down 50.1% 20.1% 2.4% 0.8% 2.6% 0.6% 76.6% 4.1% 19.3% 100.0%
Source: Access Economics estimates based on bottom-up data.
3.3.3 Reconciling the top-down and bottom-up estimatesThe previous section highlighted that there is an enormous 11-fold difference between direct costs ofbipolar disorder estimated using a top-down approach ($1,151 per person or $114m altogether) and thebottom-up approach ($12,946 per person or $1.3!billion altogether). There is a need to understand thereasons for this difference and estimate a consolidated costing within this range that reconciles theapparent disparities. There are two key issues that are important in understanding and reconciling the top-down and bottom-up costings for bipolar disorder, which flow from the findings of Chapter 2.
1 Not all people with bipolar disorder are receiving best practice treatment. Importantly andunfortunately, National Survey of Mental Health and Wellbeing data show that, of all Australians withbipolar disorder:
– one third receive no treatment;
– 40% are not taking medications; and
– only 17% access adjunctive psychosocial rehabilitation programs.
2 High rates of comorbidities, misdiagnosis and delayed diagnosis mean that people with bipolardisorder are not being captured adequately in the top-down data. National Survey of Mental Health andWellbeing together with NIMH data suggest that, of all Australians with bipolar disorder:
– in a year at least 39% have substance abuse/dependence and 52% anxiety disorders;
– 69% are likely to be misdiagnosed (on average 3.5 times) – 60% with depression, 26% with anxietydisorder, 18% with schizophrenia and 17% with borderline personality or antisocial personalitydisorders; and
– average time from onset to accurate diagnosis is likely to be over 10 years.
As a consequence, a consolidated approach taking into account allowances for these factors has beenadopted (see Methodology) which has led to an estimation of overall expenditure as shown in Table 10.
Table 10: Direct costs of bipolar disorder, 2003, consolidated
$m In-patientsOut-patients
& ED PharmaceuticalsGPs
Spec-ialists AlliedHealth
Pathology Research& other
NursingHomes Total
%Total
Depression 69.1 20.3 0.9 2.1 7.2 2.0 0.7 4.1 12.9 119.3 42Mania 69.1 5.8 1.6 2.1 8.5 0.6 0.7 3.6 11.1 103.0 36Prophylaxis 0.0 32.8 2.7 3.2 12.0 3.2 1.2 2.2 7.0 64.4 22Total p.a. 138.2 58.9 5.2 7.4 27.7 5.8 2.6 9.9 31.0 286.7 100
Source: Access Economics estimates based on reconciled top-down and bottom-up data.
Table 10 shows that a consolidated estimate of total direct expenditure on bipolar disorder in 2003 isaround $287m. Of these, costs of the depressive episode are $119m (42%); the manic episode costs$103m (36%) and prophylactic treatment costs $64m (22%). Hospital expenditure is over two thirds of thetotal, with inpatients around $138m (48%) and outpatients (and ED) around $59m (20%). Nursing homesare the next largest item at $31m (11%), followed by specialists at $28m (10%). Research and otherexpenditure ($10m) and GPs ($7m) are each around 3% of the total, while allied health ($6m) andpharmaceuticals ($5m) are each roughly 2% of the total. Pathology represents 1% of total expenditure, at$2.6m. Chart 2 depicts cost shares.

Access Economics | SANE Australia Bipolar disorder: Costs
25
Health care costs forpeople with bipolar
disorder are around$300m in 2003.
The two thirds ofAustralians with bipolar
disorder who are treated,are receiving on average
one third of optimaltreatment levels.
Chart 2: Components of bipolar disorder costs, 2003
Source: Access Economics.
Suicide attempts and self-inflicted injury also impose costs on the Australian health system. In 2001 theestimated value of these was $104m or 3% of expenditure on all Australian injuries and accidents (AccessEconomics, 2002). Table 11 extrapolates this expenditure to 2003 – $112m – and shows the componentdue to bipolar disorder – $9m – based on 8% of total suicides being due to bipolar disorder (see Section3.2). Hospitalisation represents two thirds of direct health expenditure due to suicide attempts and self-injury (Access Economics, 2002) – with $6m in hospital expenditure due to bipolar disorder.
Table 11: Costs of suicide and self-inflicted injuries including those due to bipolar disorder, Australia, 2003
$m Hospital MedicalPharma-ceuticals Other Total
Suicide and self-inflicted injury 74.5 17.1 6.2 17.1 111.8Bipolar suicide & self-inflicted injury 6.0 1.4 0.5 1.4 9.0Source: Access Economics based on AIHW data.
In estimating the full health system costs of bipolar disorder, there is an additional small element forprevention and management ($2m), which forms part of the ‘Other mental disorders, prevention &screening’ category in Table 7.
In summary, Access Economics estimates the total health systemexpenditure for bipolar disorder as $298m in 2003, comprised of:– direct health system expenditure of $287m;– suicide and self-inflicted injury due to bipolar disorder ($9m);– suicide prevention and management ($2m).
Allowing for the one third of Australians with bipolar disorder whoreceive no treatment, there are an estimated 66,397 receiving sometreatment. Health care expenditure thus averages $4,484 pertreated person with bipolar disorder – 1.5 times the spending on theaverage Australian’s health care. This is possibly still a conservativeestimate, at 0.43% of national health system expenditure and 0.04%GDP.
Inpatients47%
Pharmaceuticals2%
GPs3%
Specialists10%
Nursing Homes11%Research & other
3%
Outpatients & ED21%
Allied Health2%
Pathology1%

Access Economics | SANE Australia Bipolar disorder: Costs
26
However, the most telling implication of the direct cost estimate is the difference between officialtop-down estimated expenditure on treatment and that derived in the bottom-up analysis as ‘bestclinical practice’ ($12,946 per person p.a.). The implication is that, on average, the 66,397 receivingtreatment are receiving one third of what is considered optimal. The conclusion must be thatunder-treatment of Australians with bipolar disorder is a serious problem.
Comparisons with the UK and the USFinnern, Lothgren and Gandhi (2002) estimate direct health expenditure on bipolar disorder in the UKbetween £3,371 and £8,230 per person (A$9,000-22,000). Our Australian estimate falls at the lower end ofthis range. Hospital expenditure in the UK study was between 49% and 76% of the total whilepharmaceutical expenditure was 6-7%; these parities are reconcilable with our findings given that the UKstudy did not include the same breadth of costs (eg,!research and nursing homes). Key differences werethat the UK study assumed 1.1-1.2 episodes per year, longer periods of hospitalisation – 65 days formania, 46 for mixed and 36 for depressive episodes – and subsequently higher expenditure associatedwith manic episodes relative to depressive episodes.
In the US, Wyatt and Henter (1995) estimate expenditure on bipolar disorder as US$3,416 per person in1991. Converting to Australian dollars and allowing for health inflation and population growth wouldsuggest an average expenditure per person of around A$8,952 by 2003, somewhat lower than ourAustralian estimates. The key reasons for this may be lower hospital utilisation in the US and to a lesserextent the impact of the rising costs of pharmacotherapies on health costs since 1991, not captured in theWyatt and Henter estimates. Meletiche, Bolge and Lasser (2002) claim total health expenditure on bipolardisorder to the US economy in 2000 as US$7.6!billion. If there were 0.5% prevalence in the US, therewould be 1.4m Americans with bipolar disorder, with average expenditure of US$5,430 (A$8,140) perperson p.a. (no year referenced).
3.4 Projections to 20133.4.1 Projected prevalence of bipolar disorder and related suicidesBased on demographic growth of cohorts, the prevalence of bipolar disorder will increase by 6% – over5,500 additional people with the illness – to 104,644 over the coming decade. Most of this growth is in theoldest cohort – 32% growth in number of people with bipolar disorder over 55 years – due to demographicageing. Conversely, overall prevalence in the youngest cohort declines by 3%, as a result of lowernumbers of people in this age-group. Because of the age distribution of bipolar disorder, its totalprevalence is projected to fall slightly from 0.50% of the population to 0.48% over the decade (Table 12).
Table 12: Projected numbers of people with bipolar disorder and their suicides, Australia, 2013Males Females Total % change
0-17 1,710 1,621 3,332 -3% Suicides Males Females Total18-24 10,914 10,457 21,371 5% 15-24 41 9 5025-34 14,918 14,626 29,543 0% 25-34 91 19 11035-44 13,970 13,927 27,896 4% 35-44 76 20 9545-54 6,753 6,828 13,582 11% 45-54 28 10 3855+ 4,256 4,664 8,920 32% 55-64 14 4 19Total 52,521 52,123 104,644 6% Total 251 62 312
0.49% 0.48% 0.48%Source: Access Economics projections.
Table 12 also estimates the likely number of people with bipolar disorder who will commit suicide in 2013.In total, there are estimated to be 312 suicides – 251 males and 62 females. Suicides of people withbipolar disorder are estimated to grow in line with prevalence of the illness itself, in the absence of anypolicy changes.

Access Economics | SANE Australia Bipolar disorder: Costs
27
3.4.2 Projected direct health costsProjected growth in health inflation – based on trends in the Health and Community Services GDP deflator– together with greater prevalence, will lead to higher expenditure on bipolar disorder by 2013 (seeMethodology). All other things being equal, real direct health expenditure on bipolar disorder will grow 33%to $396m over the coming decade. Table 13 shows a breakdown of projected costs, assuming a policy-neutral environment.
Table 13: Projected components of direct health costs for bipolar disorder, 2013 (2003 prices)Hospital in-
patientsOutpatients &
EDPharmaceuticals
GPsSpec-ialists Allied Health inc
pathologyResearch &
otherNursingHomes
Total
Depression 91.9 27.0 1.2 2.8 9.6 3.5 5.5 17.1 158.6
Mania 91.9 7.7 2.1 2.8 11.3 1.7 4.8 14.8 136.9
Prophylaxis 0.0 43.6 3.6 4.3 16.0 6.0 3.0 9.3 85.7
Subtotal 183.7 78.3 6.9 9.8 36.9 11.2 13.2 41.2 381.2
Suicide 5.6 2.4 0.7 0.4 1.4 0.3 0.4 1.2 12.3
Prevention 0.7 0.3 0.0 0.1 0.3 0.2 0.2 0.8 2.7
Total p.a. 190.1 81.0 7.6 10.3 38.6 11.7 13.8 43.1 396.2
Source: Access Economics projections.
Clearly, these projections are highly sensitive to future policy and environmental changes. Some of theseare discussed below. If under-treatment issues were addressed, we might expect the proportion ofhospital inpatient expenditure to decline and expenditure on other components to increase by a proportionof the reduction. Section 2.3.3 lists studies that show the cost-effectiveness of psychoeducation, cognitivebehaviour therapy and family therapy interventions.
Pharmaceutical spending: The development of and access to newer pharmacotherapies may increasethe share of pharmaceuticals in total health expenditure. However, there would be expected to be anoffsetting effect on other health items, in particular hospitalisations.
Accommodation and rehabilitation programs: If inadequacies in these components are addressed in asignificant way, there may be compositional and other effects on projected direct expenditure (for examplethe nursing home component). A number of studies offer evidence of mental health and indirect costsavings from psychosocial rehabilitation, flowing from better health outcomes that diminish demand forclinical services and increase the likelihood of gaining employment. The Adelaide Study, conducted for theSouth Australian Health Commission, identified a range of savings including reduced frequency ofpsychiatric appointments (Ireland and Morgan, 1996).
Support, education and training: Programs that provide support, education and training for people withbipolar disorder and their families and carers have enormous potential to alter the cost structure andoverall burden of bipolar disorder in the years ahead. Access Economics (2003) found that investment insuch programs avoids institutionalisation for people with dementia and provides returns to investment ofaround 7:1.
Early intervention and diagnosis: Improvements in these areas are particularly important for people withbipolar disorder, as misdiagnosis is currently so common and because untreated illness elevates the riskof suicidality. In Australia, the Early Psychosis Prevention and Intervention Centre (EPPIC) in the westernmetropolitan region of Melbourne, has been able to demonstrate the cost-effectiveness of their model ofearly intervention and care for people aged 16 to 25 with emerging psychotic disorders. Treatmentoutcomes were far better in the EPPIC sample even when less money was used, through a reduction ofexpensive inpatient and other services as well as an improvement in productivity through treatmentoutcomes that permit return to work or study (Access Economics, 2002).

Access Economics | SANE Australia Bipolar disorder: Costs
28
4 Indirect Costs and Burdens
In addition to the direct health system expenditure estimated in the previous chapter, there are two typesof indirect costs of bipolar disorder estimated in this chapter:– financial costs, which include earnings (and taxation) forfeited due to the disabling nature of the illness
and its premature mortality, as well as carer costs, welfare expenditures and forensic costs, eachestimated individually; and
– non-financial costs from loss of healthy life – the pain, premature death and loss of life quality thatresults from the disease; these are more difficult to measure, but can be analysed in terms of the yearsof healthy life lost, both quantitatively and qualitatively, known as the ‘burden of disease’.
4.1 Loss of earningsLower participation/employment: Mitchell, Slade and Andrews (2003) found that, without agestandardisation, the employment rate of people with bipolar disorder is roughly equivalent to (but theunemployment rate is 2.1 times higher than) that of the general population. This is a result of the agedistribution of people with bipolar disorder as well as their functional disability. To correct for the agedistribution, we therefore use the employment rate (48.1%) of the population, and 2.1 times the populationunemployment rate (3.1%), which equals 6.5%, for people with bipolar disorder. If people with bipolardisorder participated in the workforce at the same rate as the ‘average’ Australian aged 15-64, theiremployment rate would be 57.9% and unemployment rate 6.1% (ABS, 2003a). All other things beingequal, there would be an extra 10,088 people in the workforce in 2003, with average weekly earnings(AWE) of $714.40 per week (see Methodology), generating $375.5m in extra income.
This figure is a conservative estimate of the true loss as many people may reduce their workload ratherthan stop work completely, as a result of the health impacts of bipolar disorder. Income losses of carers ofpeople with bipolar disorder who reduce or give up work in order to care for the person with the illness areidentified in the next section.
Absenteeism: There are an estimated 47,677 people with bipolar disorder employed in 2003, earning anestimated $1.77 billion at AWE of $714.40 per week. The percentage of time lost due to absenteeism forpeople with psychotic illnesses (such as schizophrenia) was shown in the Low Prevalence DisordersStudy to be 8% on average (Access Economics, 2002). For people with bipolar disorder, whose functionalimpairment can be similar, a conservative estimate of 5% is assumed in the absence of other robust data,amounting to $88.7m of lost production in 2003.
In total, the loss of earnings from loss of employment and absenteeism is estimated for 2003 as $464.2m.
Potential tax revenue foregone: There are two sources of lost tax revenue that result from the lowerearnings above – the potential income tax foregone and the potential indirect (sales) tax foregone. Thelatter is lost because, as income falls, so does consumption of goods and services. Table 14 summarisesthe tax losses of $129m in 2003, comprising $99m (77%) of personal income tax and $30m of indirect tax(23%).
Table 14: Potential earnings and tax revenue lost due to bipolar disorder, 2003Potential Earnings Lost $464.2m
Average personal income tax rate# 21.28%
Potential personal income tax lost $98.8m
Average indirect tax rate # 12.51%
Potential indirect tax lost $29.8m
Total potential tax revenue lost $128.6m
# Source: AEM Model, Access Economics.

Access Economics | SANE Australia Bipolar disorder: Costs
29
Mortality burden: In addition to income foregone due to those with bipolar disorder in the communitybeing unable to work because of their illness, there is also the income foregone of those who have died.This section provides an estimate of this ‘mortality burden’ of suicides related to bipolar disorder,assuming that if those who died had lived and not had the illness, they would have been employed at thesame rate as the general population – 172 people in all. The average age of suicide is estimated as 40.3years (Keks et al, 2003) – ie with 24.7 years to retirement – and the income stream is discounted at theaverage real growth rate in AWE (0.8% p.a.). This yields the net present value of the mortality burden as$144.6m.The NPV of taxation revenue sacrificed for the mortality burden is $40.1m in 2003.
4.2 Carer paymentsAlthough people with bipolar disorder receive treatment through the medical and mental health servicesavailable in the community as discussed in Section 2.3, the provision of day-to-day care and support,particularly during acute episodes, is left very much to family carers and friends (Schene et al, 1996).Society, and our public sector health and welfare budget, relies heavily on the support that carers provide.
Carers Australia estimates there are at least 2.3m Australians (one in every five households) providingcare for family members or friends with a disability, chronic condition or who are frail aged. Nearly 20%(450,900) of these are ‘primary’ carers, of whom 70% are female. The ‘invisible workforce’ saves theeconomy around $16!billion annually and is the major provider of community care services, delivering 74%of all services to people needing care and support. The Home and Community Care (HACC) Program,worth over $1.1billion nationally, meets only 9% of this need. 78% of primary carers are of workforce age(15 to 64 years) yet 59% are not attached to the workforce. Over one-half of all full time carers reportedincomes of less than $200 per week, while also experiencing the increased expenses of looking afteranother person. 40% of primary carers have been providing care for a decade or more, and 68% for morethan 5 years. Care is mostly for a partner (43%), child (25%) or parent (21%), and most primary carers(54%) said that they provided care either because alternative care was unavailable or too costly, orbecause they consider they have no choice. Carers suffer from generally worse physical health, tiredness,stress, back/muscle problems, depression, anxiety and lack of respite.15
For carers of people with bipolar disorder, specific stressors may include:– mourning the losses of the person with bipolar disorder (see Kelly, 2000, pp104-5);– feeling ashamed of the illness and possibly guilty that they may in some way have contributed to it;– difficulty dealing with the demanding behaviours and mood swings of the person and, at times, possibly
even being afraid for their own safety;– fear of leaving the person alone, of taking holidays or having visitors to stay; and– strain on marriages and relationships.
There can also be substantial effects on siblings of people with bipolar disorder, as the illness has animpact on the whole family. Siblings may experience stress-related problems, guilt, anger, pressure to dowell, and isolation/shame from stigma (eg, in relation to bringing friends home), as well as other issues.Whole family therapy may be indicated.
Counselling, education, support and respite services are essential for carers, result in improved healthoutcomes for people with bipolar disorder, and reduce demand on clinical mental health services,especially hospitalisations.
A comprehensive assessment of carer costs in Australia would require detailed survey work to assess theneeds for care of all levels of people with bipolar disorder across the spectrum of self-care – personalhygiene, cleaning, cooking, washing, shopping and house/garden maintenance. Wherever these tasks areoutsourced (to hired assistants, home services and most often volunteer carers), the value should beattributed as disease cost. Where disease severity is higher, with commensurate greater reliance on 15 Sources: AIHW, Australia's Welfare: 1999 Services and Assistance; Carers Australia, Caring Costs, 1998, Australian Bureau ofStatistics, Disability, Ageing and Carers: Summary of Findings, 1998. Cited on Carers Australia website.

Access Economics | SANE Australia Bipolar disorder: Costs
30
community services and volunteer carers, the value of the community service and income sacrifice of thecarer plus the value of the carer’s work in a paid setting should also be attributed as disease cost.
The methodology used here is based on data from the 1997-98 Australian Low Prevalence DisordersStudy (LPDS), which included 11.8% of people with bipolar disorder and/or mania, who had experiencedat least one psychotic episode (which nearly two thirds of people with bipolar disorder experience). Thisstudy is used as it provides an estimate of the proportion of Australians with bipolar disorder with carers(9.3% or 9,216 people) who stay at home in order to fulfil their caring role full time (Jablensky et al, 1999,p44). If these carers participated in employment at the same rate as the general population, there wouldbe an additional 5,336 people working, earning at AWE an estimated $198.6m p.a. (Table 15).
Table 15: Value of carers of people with bipolar disorder, 2003People with carers at home (9.3%, LPDS) 9,216Carers who may work otherwise (57.9%) 5,336Carers lost earnings @ AWE $198.6mTransfer paymentsTax foregone on carers’ earnings $55.0mCarer payment and carer allowance $17.1mSource: Access Economics estimates utilising LPDS and ABS data.
The tax foregone on these earnings is $55.0m in 2003. Other relevant transfer payments include the CarerPayment ($214.70 for singles and $179.20 each for couples per week in the first half of 2003) is a means-tested government payment to people who provide full-time care to a person. Carer Allowance is a lowerpayment ($43.85 per week) that is not means-tested. Allowing for access constraints (see Methodology),the estimated amount of Carer Allowance and Carer Payment transferred to carers of people with bipolardisorder is $17.1m.
The costing in Table 15 is conservative as it ignores the many hours of care provided part-time or not by‘designated carers at home’, as well as the many hours of care provided by goodwill non-governmentorganisations, churches and others. The amount and type of care provided for people with bipolar disorderwould be a useful area for further research.
4.3 Cost of welfare paymentEighty-five per cent of people with psychotic illnesses in Australia are reliant on welfare benefits as theirmain source of income (Jablensky et al, 1999). The Disability Support Pension is received by 79% ofthose on a benefit, Newstart or other unemployment benefits by 11.8% and Sickness Allowance by 5%.
Disability support pension is the main means of income support in Australia for people over 16 yearswho have physical, intellectual or psychiatric impairment that prevent them from working, or for peoplewho are permanently blind.
Sickness Allowance provides assistance for people who are employed and who are temporarily unableto work due to a medical condition or, in some situations, unable to continue their full-time study.
Newstart Allowance is the main means of income support in Australia for people over 21 who areunemployed or temporarily unable to work due to illness, injury or disability, to assist them while they arelooking for work and allow them to participate in activities designed to increase their chances of findingwork. Youth allowance and Work for the Dole are also available but not significant for people with bipolardisorder and so are excluded from this analysis.
In addition to these payments, the Pharmaceutical Allowance assists people in buying prescriptionmedicines available through the Pharmaceutical Benefits Scheme, while Rent Assistance assists peopleon lower incomes who rent privately.
Table 16 provides a summary of the estimated costs to government attributable to each of these transferpayments for people with bipolar disorder (see Methodology). The largest item is the Disability Support

Access Economics | SANE Australia Bipolar disorder: Costs
31
Pension at $189m, with Sickness Allowance $12m, Rent Assistance $9m and Pharmaceutical Allowance$2m. Unemployment payments included are only $4m, reflecting the fact that, although there were 5,467people with bipolar disorder unemployed in 2003, only 386 were ‘extra’ to the number expected due to thegeneral population unemployment rate. Welfare payments estimated here are thus $216m in total.
Table 16: Cost of welfare payments, bipolar disorder, 2003DisabilityPension
SicknessAllowance
Unemployment(Newstart etc)
PharmaceuticalAllowance
RentAssistance
Average weekly payment ($) 196.95 193.86 193.86 2.18 42.45# people receiving payment 18,459 1,168 386* 15,440 4,006Total cost ($m) 189.4 11.8 3.9 1.7 8.9Total welfare payments 215.7* Only those above the general unemployment rate included here.Source: Access Economics estimates utilising LPDS data.
4.4 Cost related to forensic issuesPeople with bipolar disorder are more at risk of criminality – both male and female prisoners are morelikely to have bipolar disorder than the general population. Fazel and Danesh (2002) show the over-representation in the prison system of people with bipolar disorder, with other psychoses and with majordepressive disorder – ‘disorders that may be risk factors for suicide’ (p548) – bringing together the resultsof 62 international surveys. They conclude that, in Western countries, people with these disorders areover-represented 2 to 4-fold, which would imply that in Australia the prevalence rate of bipolar disorder inprisons is around 1.5%.
The World Health Organization (2000) is concerned that inmates have higher suicide rates than theircommunity counterparts – in pre-trial facilities suicide rates are ten times the outside population, and threetimes greater in facilities holding sentenced prisoners. Suicide is often the single most common cause ofdeath in correctional settings, that often struggle with the problem of preventing suicide. Key contributingfactors are untreated mental illness (particularly in young males with substance abuse) combined with thepsychological stress impact of arrest and incarceration, poor access to mental health services,overcrowding and poor sanitation. There is a very high period of risk within the first 24 hours of beingdetained (especially if intoxicated) and a second period around the time of the court appearance,especially if a guilty verdict or harsh sentencing is anticipated. Other periods of risk are after 4-5 years ofincarceration in older prisoners, especially after a conflict or family break-up, victimisation, or after anegative legal disposition such as loss of an appeal or denial of parole. Completed suicides tend to occurin isolation or segregation cells, mostly by hanging, often at night or on weekends when staffing is lowest.Key warning signs are voiced feelings of hopelessness, shame or guilt, and psychotic episodes.
Prevention involves post-intake observation and monitoring strategies (eg, video surveillance), screeningof high-risk inmates, training of and clear procedures for correctional staff, social interventions, eg trained‘inmate buddies’, removal of means (eg, eliminating hanging points in cells or dorms) and, veryimportantly, access to mental health treatment. WHO (2002, p10) concludes, ‘criminal justice, mentalhealth and health systems must be integrally linked in the service of suicide prevention in correctionalsettings . . . This may require multi-agency cooperative service arrangements with general hospitals,emergency services, psychiatric facilities, community mental health programmes and addictionprogrammes’.
The US National Advisory Mental Health Council estimates that people with psychotic illness spend twiceas much time in prison, and are more likely to commit suicide there. On average, each incarceration in theUS costs US$50,000 p.a., including prison, court and police costs but not including the cost of damages toproperty, totalling US$15!billion per year for all those with serious psychotic disorders (TreatmentAdvocacy Center, 2002).
In Australia, the LPDS found that 10% of people with psychotic illnesses were arrested during the 12months prior to the interview and 18% reported being a victim of violence. ABS (2003c) estimates the

Access Economics | SANE Australia Bipolar disorder: Costs
32
Australian prison population in 2002 as 22,492 in total, with 21,008 males (93.4%) and 1,484 females(6.6%). Because growth in the prison population has been very small (less than 1% p.a.), these statisticsare used conservatively to estimate the 2003 Australian prison population. To this is applied theprevalence estimate of bipolar disorder in Australian prisons, from above, of 1.5% – 315 males and 22females with the illness.
Total prison expenditure in 2001 was $1.265!billion (Productivity Commission, 2002) from which averageexpenditure per inmate ($56,341) are derived (Access Economics, 2002). By 2003, using general inflationrates of 2.3%!p.a., these costs are estimated to have reached $58,963 per prisoner. The total prison costsfor males and females with bipolar disorder are thus $18.6m and $1.3m respectively. An estimate can alsobe derived for the total prison, legal and police costs for the illness based on the American TreatmentAdvocacy Center data, which suggest the average expenditure per inmate in Australia for all these itemswould be nearly $75,000 and hence the total bill would be over $25m.
Table 17: Prison costs of bipolar disorder, 2003Males Females Total
All prisoners (number) 21,008 1,484 22,458
Prevalence of BD (3 times 0.5%) 1.5% 1.5% 1.5%
Prisoners with BD (number) 315 22 337
Prison costs of BD ($m) 18.6 1.3 19.9
Prisons, legal & police costs ($m) 23.6 1.7 25.3
Source: Access Economics estimates utilising ABS (2003c), Fazel and Danesh (2002), Productivity Commission (2002)and Treatment Advocacy Center (2002).
4.5 Burden of diseaseIn 2003, an estimated 298 Australians with bipolar disorder committed suicide. Thousands of otherssuffered from the disabling symptoms of the illness and its pervasive impacts on loved ones.
Disease imposes burdens on patients that go well beyond the financial costs. The internationallydeveloped ‘Burden of Disease’ approach (see Methodology) has earned recognition in Australia andoverseas as a useful way of estimating the pain, suffering and premature death in terms of the years ofhealthy life lost due to a disease. This method uses DALYs – or ‘disability adjusted life years’ – as themeasuring stick. DALYs have two components:– the years of life lost (YLL) due to premature death – the mortality burden; and– the years of healthy life lost due to disability (YLD) – the morbidity burden.
The World Health Organization estimates suicide to be responsible for 1.8% of the total global burden ofdisease and injury and 2.3% in high-income countries like Australia – equal to the burden due to wars andhomicide, and roughly twice the burden of diabetes (WHO, 2000). WHO also identified bipolar disorder asthe sixth leading cause of DALYs in the world among people aged 15 to 44 years.
DALYs, YLLs and YLDs provide indicators that are useful in measuring the impact of disease andexploring the effectiveness of health spending in terms of purchasing years of healthy life. The AustralianInstitute of Health and Welfare has provided some excellent analysis in this area. Mathers, Vos andStevenson (1999) estimate the burden of disease in 1996 for a variety of disease and injury categories.Two of these are ‘bipolar affective disorder’ and ‘suicide and self-inflicted injury’. Table 18 extrapolatestheir estimates for these categories to 2003 based on an estimated increase in total prevalence over theperiod of 8.2%.

Access Economics | SANE Australia Bipolar disorder: Costs
33
Table 18: Burden of disease from bipolar disorder including suicide, 2003
Bipolar disorderSuicide & self-inflicted injury due to
bipolar disorderBipolar disorder inc.
suicide & self-inflicted injuryDALYs YLL YLD DALYs YLL YLD DALYs YLL YLD
Males 9,522 - 9,522 3,856 3,834 22 13,378 3,834 9,5440-14 - - - 20 20 0 20 20 015-34 9,522 - 9,522 2,042 2,025 18 11,564 2,025 9,53935-54 - - - 1,353 1,350 3 1,353 1,350 355-74 - - - 378 377 1 378 377 175+ - - - 63 63 0 63 63 0Females 9,636 40 9,595 987 968 19 10,623 1,008 9,6140-14 - - - 18 18 0 18 18 015-34 9,595 - 9,595 409 395 13 10,004 395 9,60935-54 - - - 432 427 5 432 427 555-74 21 21 - 110 109 0 130 130 075+ 19 19 - 19 19 0 38 38 0Total 19,157 40 19,117 4,843 4,802 41 24,001 4,842 19,1580-14 - - - 38 38 1 38 38 115-34 19,117 - 19,117 2,451 2,420 31 21,568 2,420 19,14835-54 - - - 1,785 1,777 8 1,785 1,777 855-74 21 21 - 487 486 1 508 507 175+ 19 19 - 82 81 0 101 101 0Source: Access Economics estimates utilising data from Mathers, Vos and Stevenson (1999).
In Australia in 2003, the burden of disease attributable to bipolar disorder was estimated as 24,001DALYs, of which 19,157 (80%) was due to the illness itself and 4,843 (20%) was due to suicide related tothe illness. Interestingly the components of YLD and YLL were in almost exactly the same proportions.Morbidity was the major source of burden (19,158 YLDs, 80%) although, clearly, mortality was dominant inthe suicidal component (4,802 YLLs or 99%). Males bore 56% of the overall burden of disease – 50% ofthe burden due to the disease itself and 80% of the burden due to suicide and self-inflicted injury. Most(90%) of the burden of disease was borne by young people aged 15-34 years.
Mathers, Vos and Stevenson (1996) show the burden of disease from bipolar disorder (not including theimpact of suicide and self-inflicted injury) was greater than that due to ovarian cancer, epilepsy,rheumatoid arthritis, HIV/AIDS or homicide and violence, and of similar magnitude to brain tumour,schizophrenia, cirrhosis of the liver and skin cancer (melanoma). Bipolar disorder comprised 1.6% of themorbidity burden (YLD) of all disease and injury in Australia and 5.3% of all mental illness DALYs(Chart!3).
Chart 3: Disease burden (DALYs) of bipolar disorder and other mental disorders
Source: Access Economics, utilising data from Mathers, Vos and Stevenson (1999). Total is 333,901 DALYs.
Schizophrenia5%
Eating disorders3%Borderline personality
disorder5%
Bipolar disorder5%
Childhood conditions6%
Anxiety disorders23%
Substance abuse24%
Other 1%
Major depression28%

Access Economics | SANE Australia Bipolar disorder: Costs
34
5 Conclusions
The direct and indirect costs of bipolar disorder in Australia in 2003 are substantial. Financial costs of theillness total $1.59!billion, about 0.2% of GDP, with indirect costs and transfer payments outweighing directhealth system expenditure by 4:1. Real indirect costs (mainly lost earnings) total $0.83!billion, whiletransfer payments for bipolar disorder (tax foregone and welfare payments) amount to $0.46!billion (0.06%of GDP). Direct health expenditure is estimated as $3,007 per person with bipolar disorder, while realindirect costs are a further $11,410 and transfer payments $4,606. Most tragically, bipolar disorder costsAustralians 24,001 healthy life-years in 2003, including 298 lives lost through suicide. Table!19summarises the costs as estimated in this report.
Table 19: Summary of direct and indirect costs of bipolar disorder, 2003Real costs Transfer
paymentsTotal
Direct health costsHospital 204Other 94Direct costs ($m) 298 298Direct costs per person with illness 3,007Indirect costsLoss of earnings 375Absenteeism 89Mortality burden NPV 145Tax foregone, patients 169Subtotal patient earnings 609 169 777Carer costs 199Tax foregone, carers 55Care payments 17Subtotal carers 199 72 271Disability support pension 189Other welfare payments 26Subtotal welfare 216 216Prison costs 20Police and legal costs 5Subtotal criminality 25 25Indirect financial costs ($m) 833 456 1,289Indirect cost per person with illness 8,403 4,606 13,009TOTAL FINANCIAL COSTS ($m) 1,131 456 1,587% of GDP 0.15% 0.06% 0.20%Cost per person with disease $11,410 $4,606 $16,016Cost per capita $57 $23 $80
Burden of disease BD RelatedSuicides
Total
YLL 40 4,802 4,842YLD 19,117 41 19,158DALYs 19,157 4,843 24,001Deaths 5 298 303Source: Access Economics estimates.
Chart!4 shows the distribution of costs. Broadly, 19% are health system expenditures, dominated byhospitals (13% of the total); 28% are lost earnings and a further 29% are transfer payments – 14%government tax foregone and 15% welfare pensions. The net present value of the ‘mortality burden’ – theproductive income streams lost due to premature death – is 9%, with the remaining costs for carers (13%)and criminality (2%). The total size of the ‘pie’ is $1.59 billion.

Access Economics | SANE Australia Bipolar disorder: Costs
35
Chart 4: Distribution of bipolar costs, Australia 2003
Source: Access Economics. * Tax and welfare costs (including carer payment) are transfer payments.
Comparison of results with other studiesThe results of this study are compared with similar studies in the UK and US. In the UK, Das Gupta andGuest (2002) have estimated the annual cost of resource use attributable to managing bipolar disorder,including indirect societal costs. Their study did not include estimates of carer costs or of transferpayments, although there is a good deal of comparability otherwise. Results are shown in Table 20 below.
Table 20: Comparison with one UK study; direct and indirect costs of bipolar disorderUK £m % total Aust $m % total
Direct health costs (NHS) 199 69.8% Hospital inpatients 69.0 24.2% 143.0 48.0% Hospital outpatients 28.5 10.0% 60.9 20.4% Psychiatric day hospitals * 28.9 10.1% 29.0 9.7% High security hospitals 2.7 0.9% - 0.0% GPs 5.2 1.8% 7.7 2.6% Pharmaceuticals 8.5 3.0% 5.7 1.9% Pathology 1.2 0.4% 2.6 0.9% Community mental health ** 53.2 18.7% 16.7 5.6% Residential care 67.8 23.8% 32.4 10.9% Non-NHS day care 18.1 6.4%Total direct (NHS and other) 285 13.9% 298 32.9%Indirect productivity costs 1,770 86.1% 609 67.1% Employment 1510 85.3% 375 61.7% Absenteeism 152 8.6% 89 14.6% Mortality 109 6.2% 145 23.8%Total 2,055 100.0% 907 100.0%No. of people with BD 297,000 99,099Direct per person £959 A$2,591 A$3,007Indirect per person £5,960 A$16,098 A$6,143 A$11,410#Total per person £6,919 A$18,690 A$9,150 A$16,016#Source: Access Economics with UK data from Das Gupta and Guest (2002) A$1=UK£0.3702* Compared with specialist costs in Australia ** In Australia includes research and other# Including carer costs and transfer costs
Points of note include:– Direct expenditure per person (£959 of $2,591) was slightly higher in Australia than in this essentially
top-down UK study; however, another UK contemporary study – Finnern, Lothgren and Gandhi (2002)– put the UK costs much higher than in Australia (see Section 3.3.3 – £3,371 to £8,230 per person)perhaps due to the same top-down/bottom-up under-treatment issue highlighted in this paper.
Hospital13%
Other health costs6%
Lost earnings28%
Carer costs13%
Forensic2%
Tax foregone*14%
Welfare payments*15%
Mortality NPV9%

Access Economics | SANE Australia Bipolar disorder: Costs
36
– Within direct expenditure, hospital spending was a smaller share (one third of direct costs) in the UKthan in Australia (two thirds); conversely, community mental health and residential care representedlarger shares in the UK than in Australia.
– GPs, pharmaceuticals and pathology were just over 5% altogether in both countries, while specialistspsychiatric services were around 10% in both countries.
– Unemployment of people with bipolar disorder appears more of a problem in the UK (46% of theirsample were unemployed, compared to 3% in the general UK population), thus representing a higherabsolute level and higher share of indirect and total costs than in Australia – productivity losses fromunemployment, absenteeism and premature mortality were A$16,098 in the UK compared to A$6,143in Australia.
– The higher productivity costs and lower direct expenditure in this UK study make the ratio of indirectproductivity costs to direct costs even higher in the UK (6:1) than in our Australian study (2:1).
– Including our estimates of carer costs and transfer payments, per capita comparisons are in fact quitesimilar A$18,690 in the UK compared to A$16,016 in Australia.
In the US, expenditures related to affective disorders in the US were an estimated US$20.8 billion in 1985,with direct expenditure comprising 58.4% of the total that year. By 1990, the total associated costs hadincreased to US$30.4 billion (Rice and Miller, 1995). A 1991 report from the National Institute of MentalHealth (Wyatt and Henter, 1995) produced much higher results, with 1991 total costs for bipolar disorderalone estimated at a staggering US$45 billion. Direct costs (US$7 billion) consisted of expenditures fortreatment-related inpatient and outpatient care, as well as nontreatment-related costs such as use of thecriminal justice system. The US$38 billion in indirect costs (5:1) included the lost productivity of wage-earners (US$17 billion), homemakers (US$3 billion), those who have been institutionalised (US$3 billion),individuals who committed suicide (US$8 billion), and caregivers of manic-depressive family members(US$6 billion). Even with a high prevalence estimate of 2 million Americans with bipolar disorder, thissuggests an average cost per person of US$22,500 in 1991 or A$58,961 in 2003 per person p.a., which ismore than the total cost per person of schizophrenia – A$49,597 in 2001 (Access Economics, 2002) – andwhich would appear to be at the extreme end of the spectrum. Moreover it seems out of line with otherofficial US (1990) estimates of the indirect costs of all mental illness of US$79-81 billion, of which majordepression was US$49!billion16.
Severe mental disorders, ie, schizophrenia, manic-depressive (bipolar) disorder, and severe forms ofdepression, panic disorder and obsessive compulsive disorder affect nearly 3% of the adult population –nearly 5 million people – and account for 25% of all Federal disability payments . . . For bipolar (manic-depressive) disorder, effective preventative medications (such as the mineral salt lithium carbonate and,for lithium resistant patients, anticonvulsants), often used in combination with supportive psychotherapy,allow 75 to 80% of manic-depressive patients to lead essentially normal lives. Without treatment, patientstypically spend one-fourth of their adult life in the hospital and fully one-half of their lives disabled. Since itsadvent as a treatment for bipolar disorder in 1970, lithium has saved the U.S. economy more than $40billion – $13 billion in direct treatment costs and $27 billion in such indirect costs as lost productivity.
American Psychiatric Association
The way aheadOver the past century, thanks in large part to research-based public health innovations, the lifespan of theaverage Australian has nearly doubled. Today, our nation’s physical health – as a whole – has never beenbetter. Illnesses of the body are increasingly becoming treatable, survivable, even curable ailments. Yet,despite the increase in public education, the lessening of stigma and the great advances in neuroscience,
16 US$79 billion cited on www.healthchoices.org/GettingBetter/2.asp. US$81 billion sourced to American Psychiatric Association:‘In 1990, the nation's health bill was $670 billion; direct cost of treating all mental disorders was 10% of that total, or $67 billion.There are hidden costs of mental disorders too, though: loss of income and loss of productivity to name a few. This tacks anadditional $81 billion onto the direct costs, bringing the total mental illnesses cost to the nation each year to $148 billion. Add thebill for the direct and indirect costs of substance abuse, and the total comes to over $270 billion. Compare this to the annual costof diseases of the cardiovascular system – $159 billion – and you have some idea of the effect of mental illnesses on America'seconomy every year. Fortunately, psychiatrists and other mental health professionals have sophisticated methods of diagnosisand treatment at their disposal to stem this tide.’

Access Economics | SANE Australia Bipolar disorder: Costs
37
genetics and behavioral science research, there has been little improvement in many areas of mentalhealth, and notably in the diagnosis and treatment of bipolar disorder.
Multiple epidemiologic studies suggest a lifetime prevalence of bipolar disorder of around 1%, making it acommon illness. Bipolar illness is not only common, but for those affected, it is a significant source ofdistress, disability, loss of life through suicide, costs (both direct and indirect) and burden for relatives andother caregivers. Despite the costs and burdens imposed by bipolar disorder and the availability of cost-effective treatments, many people with the illness in Australia continue to face significant barriers to care.The findings of this paper underline the under-treatment of bipolar disorder and the need for action.
The orphan syndrome: In recent years, improved focus on people with unipolar depression has assistedin providing those people with better access to services and improved quality of life. There isoverwhelming evidence that individuals with bipolar depression are also seriously undertreated and thetime has come now to focus also on these people. Greater public awareness of bipolar disorder isimportant to ensure early, accurate diagnosis and treatment, which in turn has a substantial impact on thequality of people’s lives. Keks et al (2003) describe bipolar depression as suffering from the ‘orphansyndrome’ as it is usually excluded from studies of depression, since treatment is less defined and morecomplex (Tondo et al, 1998). Research neglect precipitates a vicious circle since less robust trial evidencemeans less growth in knowledge of how to best treat the illness, and hence continuation of sub-optimaltreatments, non-adherence and greater suicide risk.
RecommendationsThere is an urgent need to improve the current level of under-treatment for people with bipolar disorder,particularly those at high risk of suicide, through cost-effective interventions, including:
– Diagnosis and early intervention: Improved diagnostic services and screening programs are needed,especially for GPs and primary mental health services, such as greater use of the Mood DisordersQuestionnaire (MDQ) for screening. Screening for bipolar particularly before providing women with adiagnosis of depression, or men with a diagnosis of schizophrenia, could be beneficial. A diagnosis ofdepression should never be made without first ruling out the possibility of bipolar disorder, in particularthrough a thorough investigation for a possible history of mania, especially in light of the fact thatpeople tend to under-report manic symptoms.
– Education and awareness programs: There is a need to counter the ‘orphan syndrome’ experiencedin the treatment of bipolar disorder through education and awareness programs for both the generalcommunity and healthcare professionals. This would also assist with diagnosis and interventionstrategies.
– Community mental health services: Comprehensive and assertive community psychiatricintervention is needed to augment specialist outpatient services (Keks et al, 2003; Hoult, 1993) with anemphasis on education to enhance suicide prevention. There is a particular need to address the highlevels of comorbid substance abuse for people with bipolar disorder.
– Improving access to treatment: Treatment targets should be introduced, especially where suiciderisk is high, to address the inadequate monitoring of mental state in 60% of patients who suicide, theone third of people who receive no treatment and the majority of the remainder who receive sub-optimal treatment. Focus should be on cost-effective pharmacological and psychosocial interventionsidentified by research, including treatment with lithium, other mood stabilisers and antipsychotics asrequired, psychosocial rehabilitation programs, and carer education and training.
– Data: There is a need for improved itemisation of bipolar disorder (distinct from comorbid illnesses andconditions) in top-down expenditure data, for evaluative purposes.

Access Economics | SANE Australia Bipolar disorder: Costs
38
– Suicide prevention strategies: Suicide is the pre-eminent cause of death for people with bipolardisorder, with a lifetime risk of completed suicide of 15%. Identification of high risk people together witheffective prevention strategies are essential to reducing mortality and its burdens – equivalent to$21,550 on average for each person-year saved from suicide, and around 25 years of healthy life.
– Research: The impact of combination treatments on suicide risk is unknown and, in general, long termstudies evaluating the usefulness of the range of available treatment strategies are urgently needed forbipolar disorder (Keks et al, 2003). Moreover, more research is required to understand the causationand risk factors associated with bipolar disorder and thus to reduce its onset and improve its treatment.Little is known about the cost-effectiveness in Australia of carer interventions for bipolar disorder, andthis would also be a useful area for further research.
Without such investment, in the coming decade real direct health costs alone for bipolar disorderwill approach $400!million per annum, with the indirect costs of lost productivity, carer burdenand welfare payments outnumbering these costs fourfold. Moreover, if the gross under-treatmentof Australians with bipolar disorder is not addressed, its heavy suicide toll will persist, and thosewho survive will continue to suffer from the ‘orphan syndrome’ in mental health care.

Access Economics | SANE Australia Bipolar disorder: Costs
39
MethodologyPrevalenceSection 3.1 provides sources for the international and Australian lifetime prevalence estimates cited, aswell as the cross-country one-year prevalence of 0.6% and the Australian prevalence of 0.5%. The latterestimate from Mitchell, Slade and Andrews (2003) is based on the ABS National Survey of Mental Healthand Well-being, a stratified, age and gender matched sample of 10,641 Australian adults from privatedwellings in rural and urban areas in all States and Territories (a response rate of 78.1%). The sample didnot include people in hospitals, nursing homes, hotels or gaols, or in remote areas. As such, aboriginalpeople may have been under-sampled and the estimate of bipolar disorder may be slightly conservative.Further details of the sampling method, screening and other questions used and comparisons with similarstudies are provided in Mitchell, Slade and Andrews (2003), ABS (1998) and, in particular, ABS (1999).ABS (2000a) provides details of the methodology for population projections.
The total number of Australians with bipolar disorder is derived simply by applying the 0.5% prevalencerate to the Australian population estimate from ABS (2000a) Series II. For the cohorts over 18, due to therelatively high standard errors and rounding in the gender breakdown, the total age cohort percentage ismultiplied by each respective ABS age-gender population cohort, to generate results more in line withinternational findings of the rough parity across the sexes. Moreover, there is clearly a small amount ofrounding and/or sampling error in the totals since, otherwise, the 0-18 category would be improbably large.To adjust for this, one half of the standard error is added to the total age cohort percentage in deriving thedemographic splits. For example, for the 18-24 cohort, the number of males with bipolar disorder isestimated as 1.05% multiplied by the 989,300 young men in that cohort. The difference between the totalnumber of people with bipolar disorder (99,099) and the sum of the cohorts aged 18-24 so derived(95,655) thus provides the estimate of the number of people under 18 with bipolar disorder (3,444), withan associated prevalence rate relative to the number of children in that cohort (4.7326m) of 0.07%, or0.42% of 15-17 year olds.17 The gender cohorts under 18 are also derived as residuals from theirrespective totals (for example, 49,330 minus 47,888 = 1,442 boys). Table 21 summarises the populationcohort numbers and prevalence rates used.
Table 21: Population and prevalence rates by cohort, Australia, 2003Age Males Females Total Prevalence
’000 ’000 ’000 (%)
0-18 2,427.2 2,305.4 4,732.6 0.0718-24 989.3 947.3 1,936.5 1.0525-34 1,485.7 1,470.8 2,956.6 1.0035-44 1,483.6 1,492.3 2,975.8 0.9045-54 1,356.9 1,358.1 2,715.1 0.4555+ 2,123.4 2,379.9 4,503.3 0.15Total 9,866.0 9,953.8 19,819.9 0.50
Suicide is defined in this paper as the deliberate taking of one’s life: to be classified as a suicide, a deathmust be recognised as due to other than natural causes and must also be established by coronial enquiryas resulting from a deliberate act of the deceased with the intent of ending his or her own life (ABS,2003b). Suicides of people due to bipolar disorder are estimated as 12 times the specific Australiansuicide rates (from ABS, 2003b) of each age-gender cohort multiplied by the number of people with bipolardisorder in that cohort (as derived above). For the 55+ cohort, the 55-64 suicide rate is applied, which isvery slightly conservative as the suicide rate is bimodal and increases marginally in the 65+ group,although there are few people with bipolar disorder in this age group. Consistent with ABS (2003b), thereare assumed to be no suicides of people aged under 15, and an insignificant number of people with 17 Sawyer et al (2000) found that 14% of Australian children and adolescents have mental health problems, including rates for anumber of possibly BD-related problems (somatic, delinquency, attention, aggression, social, withdrawn, anxious/depressed andthought problems) averaging 4.9% of 13-17 year olds. This suggests that BD could be associated with 9% of these symptoms.
Access Economics | SANE Australia Bipolar disorder: Costs
40
bipolar disorder under 15. Suicides of people who have bipolar disorder are higher (in fact, derived as 18times the specific Australian suicide rates) because of the high levels of comorbid suicide risk factors.For lifetime prevalence of 15% – for which there is a considerable body of international and Australianevidence as noted in Section 2.2 – and assuming (once again conservatively) that an ‘average’ lifetimewith bipolar disorder is 50 years, annual suicide risk must average 0.3% across all age groups. The samedemographic pattern of suicides is then applied to this larger group.
Direct cost estimationThe top-down approach is based on the methodology developed by the Australian Institute of Health andWelfare (AIHW), in collaboration with the National Centre for Health Program Evaluation (NCHPE) for theDisease Costs and Impact Study (DCIS). This major study measures health services utilisation andexpenditure for specific diseases and disease groups in Australia, in accordance with the Ninth Revision ofthe International Classification of Disease (ICD-9) published by the World Health Organization (WHO).The DCIS methodology has been gradually refined to estimate direct expenditure on hospitals, GP andspecialist medical services, allied professionals, pharmaceuticals, nursing homes, research and otherexpenditure (such as administration), primarily from hospital morbidity data, case mix data and theNational Health Survey (NHS), as well as other sources. The ‘health system’ is defined as the sum of allspending in these areas, regardless of whether that spending is financed by the Commonwealth or othergovernments, or by the private sector. DCIS methodology is detailed in Mathers et al (1998).
Data on bipolar disorder were provided by the AIHW in response to a specific data request. 1993-94 datawas projected to 2003 using a population growth factor of 1.110 and a health inflation factor of 1.259based on Austats population data and growth in health inflation as reported in AIHW (2002b), Table 5.
The bottom-up approach was based partially on responses to a questionnaire circulated to ten Australianclinical specialist experts in April 2003 with questions as follows.
DEPRESSIVE EPISODE1. Average length of cycle (days)—please estimate.2. GP consultations required during episode—please estimate eg, ‘1 Level B plus 1 Level C’3. Specialist consultations required during episode—please estimate eg, ‘4 psychiatric 1-hour appointments’4. Firstline drug therapy—please provide details eg, what you would usually prescribe (provided in and out of hospital) –please include dosage (mg/day), no. of days of treatment etc.5. Monitoring tests performed—please provide details of what would normally be required.6. Hospitalisation for depressive episode6a) Please estimate average number of days and type of hospitalisation – eg, “21 days in general psychiatric ward”.6b) How often are ‘secure’ wards used? Are they likely to be more costly? Please provide details.6c) How frequently would you estimate that people with BD use A&E services relative to average use? Perhaps supply a factor2x, 3x, 0.75x or provide a descriptive response.7. Outpatient services—please estimate and provide details of hospital outpatient services that may be required during theepisode8. Other health care—please estimate and provide details of other health care eg, psychosocial interventions such asoccupational therapy, dietary supplements etc during the episode.MANIC EPISODE1. Average length of cycle (days)—please estimate2. GP consultations required during episode—please estimate eg, ‘1 Level B plus 1 Level C’3. Specialist consultations required during episode—please estimate eg, ‘4 psychiatric 1-hour appointments’4. Firstline drug therapy—please provide details eg, what you would usually prescribe (provided in and out of hospital) –please include dosage (mg/day), no. of days of treatment etc5. Monitoring tests performed—please provide details of what would normally be required6. Hospitalisation for manic episode6a) Please estimate average number of days and type of hospitalisation – eg, ‘21 days in general psychiatric ward’.6b) How often are ‘secure’ wards used? Please provide details.6c) How frequently would you estimate that people with BD use A&E services relative to average use? Perhaps supply a factor2x, 3x, 0.75x or provide a descriptive response.7. Outpatient services—please estimate and provide details of hospital outpatient services that may be requiredduring the episode8. Other health care—please estimate and provide details of other health care eg, psychosocial interventions such asoccupational therapy, dietary supplements etc during the episode
Access Economics | SANE Australia Bipolar disorder: Costs
41
PROPHYLAXIS1. Average number of prophylactic (‘normal’) periods per annum—please estimate, as well as the number of complete‘cycles’ per annum, if different. Please also estimate the average frequency of ‘rapid cycling’ and any other relevant informationabout the standard deviation around the mean (the shape of the distribution) eg, about 25% of people with BD have 4 cycles p.a.,about 20% have 3 cycles, about 20% have 5 cycles, about 20% have less than 3 cycles and the remainder have more than 5cycles.2. GP consultations required during prophylaxis—please estimate eg, ‘1 Level B per month’3. Specialist consultations required during prophylaxis—please estimate eg, ‘1 psychiatric appointment per month’4. Firstline drug therapy—please provide details eg, what you would usually prescribe including dosage (mg/day), no. of daysof treatment etc5. Monitoring tests performed – please provide details of what would normally be required6. Hospitalisation – it is assumed no hospitalisation is required due to BD during prophylaxis; if there are exceptions to thisassumption, please provide details7. Outpatient services – please estimate and provide details of hospital outpatient services that may be required duringprophylaxis8. Other health care – please estimate and provide details of other health care eg, psychosocial interventions such asoccupational therapy, dietary supplements etc during the periodOTHERSuicide attempts/completions1a) Please estimate average frequency of suicide attempts eg, ‘in one year, 2% of all people with BD would attempt suicide’.1b) Please estimate average frequency of completed suicides eg, ‘of attempted suicides, 1 in 5 are completed for women onaverage, 1 in 2 for men with BD’.1c) Do suicide attempts occur only in the depressive episode? If not, please estimate the average proportions that occur (i) in thedepressive episode; (ii) in the manic episode, if any and (iii) between episodes/during prophylaxis1d) Please estimate average additional hospitalisation and health services required for suicide attempts– eg, ‘3 days in intensivecare, an additional 20% recovery period in general psychiatric ward relative to the average for depressive episodes, 2 additionalspecialist visits, weekly counselling for two months, etc’Accidents1a) Please estimate average frequency of accidents due to BD eg, ‘In one year, 1% of all people with BD have an accidentprimarily caused by BD and requiring expert medical attention’.1b) Please estimate average frequency of accidental death for people with BD. Are accidents more common for men thanwomen and what are the average associations?1c) Do accidents occur mainly in the manic episode? If not, please estimate the average proportions that occur (i) in thedepressive episode; (ii) in the manic episode and (iii) between episodes/during prophylaxis.1d) Please estimate average additional health services required for accidents –!eg, ‘2 days in intensive care, an additional 10%recovery period in general psychiatric ward (relative to the average for manic episodes), an additional GP visit, two counsellingsessions, etc’.Lifetime BD prevalence of 1.2% and one-year prevalence of 0.5% from recent WA data will be used, as well as a global estimateof lifetime prevalence of 0.3% to 1.5%. Are these estimates compatible with your experience? Are you aware of any additionalrecent Australian data on gender and age distribution of prevalence? Are there any other comments or information which youbelieve would be relevant for costing BD episodes and overall?Thank you very much for your time.
Reponses were consolidated and related to other data from a variety of published sources to derive thecosts detailed in Section 3.2.2.
– The Medical Benefits Schedule was used to derive costing for specialist consultations (Items 304, 306,314, 316, 320), GP consultations (Items 23 and 36) and pathology services (MBS Items 65070, 66515and 66611).
– The Pharmaceutical Benefits Schedule was used to derive indicative drug costs (3059B Tablet 250mg200 Lithicarb, 8290H Tablet 450mg 200 Quilonum SR, 2294R Tablet 100mg 200 Epilim, 2289L Tablet200mg Vaplro 200, 2290M Tablet 500mg 200 Valpro 500, 8185T Tablet 5mg 30 Zyprexa, 8186WTablet 7.5mg 30 Zyprexa, 3170W Tablet 1mg 60 Risperdal and 3172 Tablet 4mg 60 Risperdal).
– Hospital expenditure was derived from the AIHW hospital data cubes online and from a special AIHWdata request for AN-DRG U63-B cost per separation and ALOS and Accident and Emergencyseparations and average costs.
– Allied health costs were derived from telephone sampling five providers in the ACT, New South Walesand Victoria, for a range of case management, exercise and relaxation, physiotherapy, occupationaltherapy and counselling services.
Reconciliation of the top-down and bottom-up approaches involved inflation of the top-down data by 50%to allow for comorbidity, by 34% to allow for delay in diagnosis, and by 25% to allow for misdiagnosis.Treated prevalence was assumed to be two thirds of estimated prevalence.

Access Economics | SANE Australia Bipolar disorder: Costs
42
Projections to 20132013 population estimates were obtained through Austats from the ABS midpoint Series II projections forAustralia (ABS, 2000). Prevalence rates for each demographic cohort of people with bipolar disorder wereprojected on the 2013 population, to reflect the effects on one-year prevalence of change in the populationstructure. More comprehensive Australian age of onset and remission data would enhance theseprojections.
The numbers of people with bipolar disorder who suicide, in the absence of policy changes, is thenprojected as 18 times the suicide prevalence rates by cohort (ie, including suicides due to comorbidconditions). It is hoped, however, that policy interventions may reduce the numbers of suicides over thedecade.
Direct expenditure projections were based on the prevalence growth (5.6% overall) together with projectedgrowth in the Health and Community Services GDP deflator. The latter is expected to grow by 25.9% from2003 to 2013 based on projections of historical growth over 1997-98 to 2000-01, which averaged 2.9%p.a. (AIHW, 2002b). The upside risk of pharmaceutical spending, together with the various policysensitivities outlined in Section 3.4.2, make the expenditure projections very much open to policy choicesand directions of today.
Indirect costsThe World Health Organisation and cost of illness studies in the past have typically classed indirect costsas all those costs that are not health system expenditures, the approach adopted here. A distinction ismade here between real indirect costs and transfer payments, where the latter do not represent real goodsand services but, rather, monetary transfers from one economic unit to another through the government,such as taxation and welfare payments. Measurement of indirect costs remains a matter of some debateand controversy.
Lost earnings and production (‘human capital’): This focuses on the loss of production or earningsassociated with illness and premature death. In this analysis it is reasonably assumed that, in the absenceof illness, people with bipolar disorder would participate in the labour force and obtain employment at thesame rate as other Australians, and earn the same average weekly earnings – based on ABS AverageWeekly Earnings (Cat. 6302.0 released May 2003, most recent available), end-February 2003 of $714.40per week, including full and part time earnings across all occupations and regions (‘all employees totalearnings’) seasonally adjusted. The implicit economic assumption is that the numbers of such peoplewould not be of sufficient magnitude to substantially influence the overall clearing of the labour market.
Labour force statistics (ABS, 2003a) show that in May 2003 (most recent available) there were 9.535mAustralians employed and 0.613m unemployed, making 9.672m in the workforce, in a population of19.82m. From this is derived the population-wide employment rates used in Section 4.1 (48.1% foremployment and 3.1% for unemployment), which of course are lower than the ratios published relative tothe working age population, namely 57.9% and 6.1% respectively in ABS (2003a). The population-wideestimates are necessary to age-standardise the findings of Mitchell, Slade and Andrews (2003). Ininternational studies of bipolar disorder, employment rates tend to be lower and unemployment rateshigher than those in Australia, so this may be a conservative estimate of loss of earnings.
Mortality burden: The mortality burden makes similar assumptions to those above if, in the absence ofthe illness, those people with the illness do not die (including from suicide) in 2003, but rather are well andparticipate in the labour force similarly to average Australians, and for the same expected duration. Theaverage age of suicide is 40.3 years (Keks et al, 2003); with retirement assumed to be at age 65, thisimplies 24.7 years to retirement. The discount rate for the net present value (NPV) of the future incomestream – 0.81% – is based on the 30-year average growth of real AWE (with the Consumer Price Index asthe deflator) for the period 1981-92 to 2011-12, including forecasts from the Access EconomicsMacroeconomic Model. A long-term average is required due to the sensitivity of the results to the discountrate. Then:

Access Economics | SANE Australia Bipolar disorder: Costs
43
NPV = _Y/(1+r)i where Y=$37,220, r=0.81% and i=0,1,2………25 = $0.839m
The number of people with bipolar disorder who suicide under the age of 65 (assumed to be all of the 298)is multiplied by the employment rate (57.9%) to give the number of people (172) who suicide who would, ifthey were well, have been employed. This is possibly a conservative estimate since males are over-represented in suicides and in employment rates. Overall, 172*$0.839m = $144.6m, the mortality burden.Average annual earnings ($37,220) multiplied by 172 divided by 298 gives $21,550 benefit per life saved(plus 25 years of life, undiscounted) as per the Conclusions section.
Potential tax revenue foregone: People with bipolar disorder who work less or retire early will not onlyforego income, but will also pay less personal income tax. The income tax foregone is a product of theaverage personal income tax rate and the foregone income. With bipolar disorder and lower income, therewill be less consumption of goods and services, estimated up to the level of the disability pension(averaging $196.95 per week in the first half of 2003 – see Social welfare payments below). Withoutbipolar disorder, it is conservatively assumed that consumption would comprise 90% of income (thesavings rate may well be lower than this). The indirect tax foregone is a product of the foregoneconsumption and the average indirect tax rate, as per the Access Economics macroeconomic model(AEM) incorporating changes from A New Tax System from 1 July 2000. Tax revenue sacrificed isincluded as a transfer payment (not a real economic cost) – interesting in terms of the overall governmentbudget position.
Carer costs: For many illnesses such as bipolar disorder, the patient is supported and cared for by aspouse, parent, family member or significant other. Placing a value on the cost of volunteer care andcommunity services is the one of the most difficult aspects of disease costing. It is nonetheless a hugelyimportant indirect cost, and becoming more so as, in Australia, we increasingly cap hospital inpatientbeds, discharge patients earlier, and move people with disabilities out of the hospital system. Greateremphasis is being placed on partnerships with community organisations, such as the Home andCommunity Care (HACC) program, and the proliferation of paid home help and domiciliary care services.
Two elements of Carer Costs are made in this analysis. First, an estimate of their lost earnings, the simplemethodology for which has been described in the main body of the text (Section 3.2) and, as discussedthere, errs on the conservative side because of the nature of the questions in the Low PrevalenceDisorders Study. Second, the Carer Allowance and Carer Payment are derived from the Centrelinkwebsite, the latter a simple average of the weekly rates for couples (each) and singles, averaging $196.95as per the disability pension. Access constraints relate to the payment criteria which, for Carer Payment,involve proof of providing full-time care to a person, of caring for the person in their own home, of notgetting another social security pension or benefit, or a Veterans' Affairs Service Pension or PartnerService Pension, and of meeting residence requirements. The person/s needing care must:– be at least 16 years old and, because of a severe physical, intellectual or psychiatric disability, qualify
the carer under the Adult Disability Assessment Tool; or be a child with a profound disability under theage of 16 years; or be two or more children with a disability under 16 years who, together, require alevel of care that is at least equivalent to the level of care required by a child with a profound disability;or be a person with a disability and their child (who is less than six years old, or less than 16 years oldand attracting Carer Allowance), and
– need this care permanently or for an extended period of at least six months (less if they have aterminal illness); and
– be getting a full or part social security pension or benefit, or a Veterans' Affairs Service Pension orPartner Service Pension; or be ineligible for a social security pension or benefit, or a Veterans' AffairsService Pension or Partner Service Pension solely because they have not lived in Australia longenough to qualify; or not be getting a social security pension or benefit, or a Veterans' Affairs ServicePension or Partner Service Pension and satisfy specific income and assets tests; and
– meet residence requirements.

Access Economics | SANE Australia Bipolar disorder: Costs
44
Carer Payment is income and assets tested, while Carer Allowance is not. Carers Allowance is paid if aperson personally provides full-time care on a daily basis for up to two adults who need a lot of additionalcare because of a disability, severe medical condition or because they are frail aged; lives in the samehome as the person they are caring for; and meets residence requirements. Medical eligibility for peopleover 16, as with Carer Payment, is measured by the Adult Disability Assessment Tool (ADAT), whichmeasures the functional ability of the person receiving care. A number of other factors can affectpayments, for example location, rent paid, provision of other information such as proof of identity, having atelephone, or imprisonment.
Taking into account these exclusion criteria, the number of carers who receive Carer Payment and CarerAllowance are assumed to be 13% (1,152 people) and 25% (2,304 people) respectively, relative to thenumber of carers at home as per the LPDS (9,216 in total).
Social welfare payments: The disability pension, sickness benefits and various unemployment benefitspaid to those suffering from disease are costs to the tax-paying community, which could be put toalternative use. These are also income transfer payments rather than real economic costs, but againrelevant to the public financial position. The disability support pension is the main item here for bipolardisorder—this pension was previously known as the invalid pension and was introduced in 1910 as aresult of the Invalid and Old-age Pensions Act 1908.
The average weekly payments in Table 16 for each of the various welfare items included are derived fromthe Centrelink website (www.centrelink.gov.au). Other benefits which may be received by people withbipolar disorder (eg,!Sole Parents Allowance, Age Pension, etc) are not directly related to the illness sonot estimated here as part of the cost of illness. Special Benefit, which may be related to the illness, ispaid in situations of severe financial need due to circumstances outside of a person’s control and decidedat the discretion of the Secretary of the Department of Family and Community Services. However,because Special Benefit is a very small item and there is no data on how many people with bipolardisorder receive it, it is not included.
Jablensky et al (1999) estimated that of the 85% of people in the LPDS who received welfare payments,79% received the Disability Support Pension. These rates are applied only to the people with bipolar whoare not working. For the benefits included, there are various access constraints as there are for CarerPayment and Carer Allowance above, including income and assets tests and other exclusion criteria.Access constraints are assumed to further reduce the number of people receiving the DSP by 39%.For Sickness Allowance, the estimate from Jablensky et al (1999) is 5%. For Newstart Allowance, thedifference between the unemployment rate of the general population (6.1%) and that of people with bipolardisorder (6.5%) is 0.4%, or 386 people. For Pharmaceutical Allowance, 40% of people with bipolardisorder are not receiving medication and additional constraints (in particular copayment levels) areestimated to exclude around 50% of those who are. For Rent Assistance, 30% of those with bipolardisorder who are not working are estimated to rent privately, of whom 50% are estimated to survive otherexclusion criteria (eg, rent limits). Finding a suitable place to live is essential for anyone with bipolardisorder, particularly given the high rate of homelessness of people with chronic mental illnesses.
Burden of disease: The World Health Organisation (WHO), the World Bank and Harvard Universitydeveloped a methodology that provides a comprehensive assessment of mortality and disability fromdiseases, injuries and risk factors in 1990 and projected to 2020 (Murray and Lopez, 1996). This approachhas been adopted and applied in Australia by the AIHW with a separate comprehensive study in Victoria.Mathers, Vos and Stevenson (1999) estimate the burden of disease in 1996. The bipolar disordercomponents did not include associated suicides so these were attributed from the burden of disease datafrom the ‘suicides and self-inflicted injury category’ (Annex tables), on the basis of the proportion ofsuicides due to bipolar disorder as a proportion of total Australian suicides (8%). The YLD and YLLelements were then extrapolated to 2003 on the basis of estimated 8.2% growth in bipolar disorderprevalence over the period. The disability weight used by the AIHW team was 0.176 for bipolar disorderand 0.447 for suicide and self-inflicted injuries. Burden of disease calculation software (DISMOD) isavailable on the WHO website at www.who.org.

Access Economics | SANE Australia Bipolar disorder: Costs
45
ReferencesAccess Economics (2003) The dementia epidemic: Economic impact and positive solutions for Australia.Report for Alzheimer’s Australia, May.
Access Economics (2002) Schizophrenia: Costs: An analysis of the burden of schizophrenia and related suicide inAustralia. Report for SANE Australia, July.
Almeida OP and Fenner S (2002) ‘Bipolar disorder: Similarities and differences between patients with illness onsetbefore and after 65 years of age’ International psychogeriatrics 14:3, 311-322.
American Psychiatric Association (2003) Mental Illness Awareness Guides Reprinted in Monadnock Family Services“Mental Illness Facts and Statistics” available on www.mfs.org/fands.htm
Australian Bureau of Statistics (2003a) Labour Force, Australia, May 2003 Cat. No. 6202.0, June.
Australian Bureau of Statistics (2003b) Information Paper: Suicides Australia, Publication 3309.0.55.001, February.
Australian Bureau of Statistics (2003c) Prisoners in Australia 2002, Cat. No. 4517.0, February.
Australian Bureau of Statistics (2001) Briefing Paper: Suicides 2000, December.
Australian Bureau of Statistics (2000a) Population Projections, Australia, 1999-2101, ABS Cat No. 3222.0, August.
Australian Bureau of Statistics (2000b) Suicides since 1921, ABS Cat. No. 3309.0, March.
Australian Bureau of Statistics (1999) National Survey of Mental Health and Wellbeing of Adults, User’s Guide, 1997,ABS Cat No. 4327.0, January.
Australian Bureau of Statistics (1998) Mental Health and Wellbeing – Profile of Adults, Australia, 1997, ABS Cat No.4326.0, March.
Australian Institute of Health and Welfare (2002a) Mental Health Services in Australia 1999-00, AIHW Cat. No. HSE-19, Canberra.
Australian Institute of Health and Welfare (2002b) Health Expenditure Australia: 2000-01, AIHW Cat. No. HWE 20,September, Canberra.
Baldessarini RJ and Jamison KR (1999) ‘Effects of medical interventions on suicidal behavior’ J Clin Psychiatry60!Suppl 2:117-22.
Barrett TB, Hauger RL, Kennedy JL, Sadovnick AD, Remick RA, Keck PE, McElroy SL, Alexander M, Shaw SH andKelsoe JR (2003) ‘Evidence that a single nucleotide polymorphism in the promoter of the G protein receptor kinase 3gene is associated with bipolar disorder’ Molecular Psychiatry, 8: 546-557.
Bourgeois ML and Verdoux H (1997) ‘Suicidal risk in bipolar disorders’ Encephale Jan:23 Spec No 1:35-41 [article inFrench].
Bowden CL (1997) ‘Update on Bipolar Disorder: Epidemiology, Etiology, Diagnosis, and Prognosis’ MedscapePsychiatry & Mental Health eJournal 2(3).
Brady K and Goldberg J (1996) Substance abuse and bipolar disorder Paper delivered at the Ninth Annual USPsychiatric and Mental Health Congress, November 14-17.
Carr VJ, Neil AL, Halpin SA, Holmes S and Lewin TJ (2003) ‘Cost of Schizophrenia and other Psychoses in UrbanAustralia: Findings from the Low Prevalence (Psychotic) Disorders Study’ Australian and New Zealand Journal ofPsychiatry 37:31-40.
Coghlan R, Lawrence D, Holman D and Jablensky A (2001) Duty to care: Physical illness in people with mentalillness, Departments of Public Health and Psychiatry and Behavioural Science, University of Western Australia.
Compton MT and Nemeroff CB (2000) ‘The treatment of bipolar depression’ J Clin Psychiatry 61(suppl 9):57-67.
Das Gupta R and Guest JF (2002) ‘Annual cost of bipolar disorder to UK society’ CATALYST Health EconomicsConsultants, Middlesex, UK, Br J Psychiatry Mar;180:227-33.
Depressive and Manic-Depressive Association (DMDA) National (2001) ‘Living with bipolar disorder: How far havewe really come?’ Constituency Survey, Chicago, USA.

Access Economics | SANE Australia Bipolar disorder: Costs
46
Evans DL (2000) ‘Bipolar disorder: diagnostic challenges and treatment considerations’ J Clin Psychiatry 61 Supp13:26-31.
Fazel S and Danesh J (2002) ‘Serious mental disorder in 23,000 prisoners: a systematic review of 62 surveys’, TheLancet, 359: 545-50.
Finnern, Lothgren and Gandhi (2002) Direct medical costs for treatment of patients experiencing bipolar disorderepisodes in the UK, European Health Outcomes Research, Eli Lilly and Co, Windlesham UK.
Ghaemi SN, Sachs GS, Chiou AM, Pandurangi AK and Goodwin FK (1997) ‘Is Bipolar Disorder Underdiagnosed?Are Antidepressants Over-utilized?’ Paper for the Second International Conference on Bipolar Disorder, June 19-21,Pittsburgh, Pennsylvania.
Goodwin FK and Jamison KR (1990) Manic Depressive Illness, Oxford University Press, New York.
Harris EC and Barraclough B (1997) ‘Suicide as an Outcome for Mental Disorders: A Meta-Analysis’ Brit J Psychiatry170: 205-228
Hirschfeld RMA (2002) ‘The Mood Disorder Questionnaire: A Simple. Patient-Rate Screening Instrument for BipolarDisorder’ Primary Care Companion, J Clin Psychiatry 4(1).
Hirschfeld RMA, Keller MB, Panico S, Arons BS, Barlow D, Davidoff F, Endicott J, Froom J, Goldstein M, GormanJM, Guthrie D, Marek RG, Maurer TA, Meyer R, Phillips K, Ross J, Schwenk TL, Sharfstein SS, Thase ME and RyattRJ (1997) ‘The national depressive and manic depressive association consensus statement on the undertreatment ofdepression’ Journal of the American Medical Association 277:333-340.
Hoult J (1993) ‘Comprehensive services for the mentally ill’ Current Opinion in Psychiatry 6:238-245.
Hyman SE and Rudorfer MV (2000) Depressive and bipolar mood disorders in Dale DC and Federman DD (eds)‘Scientific American’ Medicine, Healtheon/WebMD Corp, New York, Vol. 3 Sect. 13, p1.
Hyman SE (1999) ‘Introduction to the complex genetics of mental disorders’ Biological Psychiatry; 45(5): 518-21.
Ireland G and Morgan P (1996) A Cost Benefit Analysis of a Clubhouse Program, Report to the South AustralianHealth Commission.
Jablensky A, McGrath J, Herrman H, Castle D, Gureje O, Morgan V, Korten A (1999) ‘People Living with PsychoticIllness: An Australian Study 1997-98’ National Mental Health and Wellbeing Report 4, Commonwealth Department ofHealth and Aged Care, October 1999.
Jamison KR (2000) ‘Suicide and bipolar disorder’ J Clin Psychiatry, 61 Suppl 9:47-51.
Jamison KR (1995) An Unquiet Mind, Knopf, a division of Random House, Inc., New York.
Keks NA, Hill C, Sundram S, Graham A, Bellingham K, Dean B, Opeskin K, Dorissa A and Copolov D (2003) ‘Suicidein treated bipolar mood disorder’ Submitted, pending publication.
Kelly M (2000) Life on a Roller-Coaster: Living well with depression and manic depression, Simon and Schuster,Australia.
Kessler RC, Tubinow DR, Holmes C, Abelson JM and Zhao S (1997) ‘The epidemiology of DSM-III-R bipolar Idisorder in a general population survey’ Psychological medicine 27:1079-1089.
Lish JD, Dime-Meenan S, Whybrow PC et al (1994) ‘The National Depressive and Manic-Depressive Association(DMDA) Survey of Bipolar Members’ J Affect Disorder 31: 281-294.
Mathers C, Stevenson C, Carter R and Penm R (1998) Disease Costing methodology used in the Disease Costs andImpact Study 1993-94, AIHW Cat. No. HWE-7, Australian Institute of Health and Welfare, Canberra.
Meletiche DM, Bolge S and Lasser R (2002) Utilization and cost of resources in bipolar patients receiving atypicalanti-psychotics, Janssen Pharmaceuticals and Princeton University, US.
Mitchell PB, Mahli GS, Redwood BL and Ball J (2003) ‘Summary of guideline for the treatment of bipolar disorder’RANZCP Clinical Practice Guidelines Australasian Psychiatry Vol 11 No.1 March.
Mitchell PB, Slade T and Andrews G (2003) ‘Twelve-month prevalence and disability of DSM-IV bipolar disorder inan Australian general population survey’ Submitted, pending publication.
Mitchell PB (2001) ‘Why are we doing this and how does it work? University of NSW & ARHRF Research Committeepresentation, Sydney, July.
Access Economics | SANE Australia Bipolar disorder: Costs
47
Mueser KT, Goodman LB, Trumbetta SL, Rosenberg SD, Osher FC, Vidaver R, Auciello P and Foy DW (1998)‘Trauma and posttraumatic stress disorder in severe mental illness’ Journal of Consulting and Clinical Psychology,66(3): 493-9.
Muller-Oerlinghausen B, Berghofer A and Bauer M (2002) ‘Bipolar disorder’ Lancet 359(9302):241-7.
Murray CJL and Lopez AD eds (1996) The Global Burden of Disease. Geneva, Cambridge, Mass., Washington.Published by The Harvard School of Public Health, on behalf of WHO and The World Bank, distributed by HarvardUniversity Press.
National Depressive and Manic-Depressive Association (2001) Living with bipolar disorder: How far have we reallycome? Constituency Survey, Chicago US.
National Institute for Mental Health (2001) Bipolar Disorder, NIH Publication No. 02-3679, Hendrix M L revised bySpearing M, Maryland USA.
National Institutes of Health (2000) The Benefits of Medical Research and the Role of the NIH, NIH, US, May.
Neil AN, Lewin TJ and Carr VJ (2003) ‘Allocation of resources and psychosis’ Australian and New Zealand Journal ofPsychiatry 37:15–23.
NIMH Genetics Workgroup (1998) Genetics and mental disorders NIH Publication No. 98-4268, Maryland USA.
Parry B L (1996) ‘Premenstrual and postpartum mood disorders’ Current Opinion in Psychiatry 9:11-16.
Productivity Commission (2002) Report on Government Services, 2002, Chapter 10 ‘Justice’, January 2002,available on www.pc.gov.au
Rice DP and Miller LS (1995) ‘The economic burden of affective disorders’ Br J Psychiatry Suppl Apr(27):34-42.
Rothbaum BO and Astin MC (2000) ‘Integration of pharmacotherapy and psychotherapy for bipolar disorder’ J ClinPsychiatry 61(suppl 9):68-75.
SANE Australia (2003) The SANE Guide to Bipolar Disorder.*
SANE Australia (2001) The Blueprint Guide to Psychosocial Rehabilitation, revised edition.*
SANE Australia (1997) The Blueprint Guide to 24-Hour Supported Accommodation.*
Sawyer MG, Arney FM, Baghurst PA, Clark JJ, Graetz BW, Kosky RJ, Nurcombe B, Patton GC, Prior MR, RaphaelB, Rey J, Whaites LC and Zubrick SR (2000) ‘The Mental Health of Young People in Australia: Child and AdolescentComponent of the National Survey of Mental Health and Wellbeing’ Mental Health and Special Programs Branch,Commonwealth Department of Health and Aged Care, October.
Schene A et al (1996) ‘Caregiving in severe mental illness: conceptualisation and measurement’ 296-316 in Perkins,R and Repper J (1996) Working alongside People with Long-Term Mental Health Problems, Chapman and Hall.
Simpson SG and Jamison KR (1999) ‘The risk of suicide in patients with bipolar disorders’ J Clin Psychiatry,60!Suppl 2:53-6.
Soares JC and Mann JJ (1997a) ‘The anatomy of mood disorders – review of structural neuroimaging studies’Biological Psychiatry, 1997; 41(1): 86-106.
Soares JC and Mann JJ (1997b) ‘The functional neuroanatomy of mood disorders’ Journal of Psychiatric Research,31(4): 393-432.
Strakowski SM and DelBello MP (2000) ‘The co-occurrence of bipolar and substance use disorders’ ClinicalPsychology Review 20(2): 191-206.
Strakowski SM, Sax KW, McElroy SL, Keck PE Jr, Hawkins JM, West SA (1998) ‘Course of psychiatric andsubstance abuse syndromes co-occurring with bipolar disorder after a first psychiatric hospitalisation’ Journal ofClinical Psychiatry, 59(9): 465-71.
Suppes T, Dennehy EB and Gibbons EW (2000) ‘The longitudinal course of bipolar disease’ Journal of ClinicalPsychiatry 61 (Suppl. 9), 23-30.
Treatment Advocacy Center (2002) Fact Sheet: Consequences of Non-Treatment, TAC, Virginia USA, available onwww.psychlaws.org
Tondo L, Baldessarini RJ, Hennen J, Floris G, Silvetti F and Tohen M (1998) ‘Lithium treatment and risk of suicidalbehaviour in bipolar disorder patients’ Journal of Clinical Psychiatry 59:405-414.
Access Economics | SANE Australia Bipolar disorder: Costs
48
University of New South Wales (2002) ‘New treatment for manic depression’ Media, News and Events, 22 April,available on www.unsw.edu.au/news/pad/articles/2002/apr/treatmentmanicdepression.html
US Department of Health and Human Services (1999) Mental Health: A Report of the Surgeon General: ExecutiveSummary, NIMH, Rockville, Maryland.
Weissman MM, Bland RC, Canino GJ, Faravelli C, Greenwald S, Hwu HG, Joyce PR, Karam EG, Lee CK, LellouchJ, Lepine JP, Newman SC, Rubio-Stipec M, Wells JE, Wickramaratne PJ, Wittchen H and Yeh EK (1996) ‘Cross-national epidemiology of major depression and bipolar disorder’ Journal of the American Medical Association, 276,293–299.
Woods SW (2000) ‘The economic burden of bipolar disease’ J Clin Psychiatry 61 Supp 13:38-41.
World Health Organization (2002) Prevention of Suicidal Behaviours: A Task for All, 5!April 2002, onwww.who.int/mental_health
World Health Organization (1996) Bipolar Disorder Prevalence data by M Privett updated 30 September, available onhttp://www.who.int/msa/mnh/ems/ratesold/bipolar.htm
Wyatt RJ and Henter I (1995) ‘An economic evaluation of manic-depressive illness-1991’ Soc Psychiatry PsychiatrEpidemiol 30(5); 213-219.
Zwerling C, Whitten PSS, Sprince NL, Davis CS, Wallace RB, Blanck PD and Heeringa SG (2002) ‘Workforceparticipation by persons with disabilities: The National Health Interview Survey Disability Supplement, 1994 to 1995’Journal of Occupational and Environmental Medicine 44:358-364.
* Available from SANE Australia, PO Box 226 South Melbourne VIC 3205, ph: (03) 9682 5933.See also www.sane.org or email: [email protected]
















![Footnotes for the Infographic Bipolar Drugs: Benefits ... · [2] Weinstock LM et al, Medica.on burden in bipolar disorder: a chart review of pa.ents at psychiatric hospital admission.](https://static.fdocuments.net/doc/165x107/5fc022e521e21211db03524c/footnotes-for-the-infographic-bipolar-drugs-beneits-2-weinstock-lm-et-al.jpg)



