An Account of the Development of the Conceptual Basis of Osteopathy Course at the British School of...
9
Click here to load reader
-
Upload
petrakas-petrix -
Category
Documents
-
view
215 -
download
0
Transcript of An Account of the Development of the Conceptual Basis of Osteopathy Course at the British School of...

7/30/2019 An Account of the Development of the Conceptual Basis of Osteopathy Course at the British School of Osteopathy
http://slidepdf.com/reader/full/an-account-of-the-development-of-the-conceptual-basis-of-osteopathy-course 1/9
An account of the development of the conceptual basis of
osteopathy course at the British School of Osteopathy
K. Nash*, S. Tyreman
British School of Osteopathy, 275 Borough High Street, London SE1B 1JE, UK
Received 10 January 2005; received in revised form 11 February 2005; accepted 11 February 2005
Abstract
Background: The historical background to the teaching of ‘The Principles or Concepts of Osteopathy’ from the foundation of the
British School of Osteopathy (BSO) in 1917 to the present is briefly described in order to provide a context for a curriculum review
that occurred between 2003 and 2004.
Objectives: The objective for the review of ‘The Concepts of Osteopathy’ curriculum change was to develop a clinically relevant
course, which reflected both the historical foundations of osteopathy, current philosophy in health care and contemporary scientific
developments.
Methods: Focus groups were held with members of the BSO faculty in order to ascertain their views about what should be taught
within ‘Concepts of Osteopathy’ curriculum. Additional contributions were received from an online discussion group of BSO faculty
members and through discussions with the members of the teaching faculty. This information was analysed and utilised in
developing the revised curriculum.
Results: Commonly occurring themes which participants felt should be reflected in the concepts course were: (1) it is the osteopathic
concepts that distinguish us from other physical therapists, (2) there are different models of osteopathy being practiced and taught
within the BSO, the UK and internationally and (3) it is the practical application of osteopathic concepts that is important.Discussion: Despite the fact that osteopathy as currently practiced is clinically diverse, there was a considerable measure of
agreement amongst the osteopaths who participated in this focus group exercise. Particular challenges exist in developing the
curriculum content because of both the broad theoretical basis on which the course operates and the importance of presenting the
content in such a way that students are able to apply it to clinical situations.
Conclusion: Further development of the curriculum will be informed by feedback from students, internal faculty and examiners; and
revised to reflect contemporary developments in health care and scientific knowledge.
Ó 2005 Elsevier Ltd. All rights reserved.
Keywords: Education; Principles of osteopathy; Osteopathic medicine; Health care concepts
1. Introduction
The teaching of ‘The Principles of Osteopathy’ or
‘Conceptual Basis of Osteopathy’ (CBO), occupies
a unique place in health care education. No other
main-stream healthcare professions have an equivalent
subject, and even within osteopathy there appear to be
considerable differences between the ways various
teaching institutions manage this part of the curriculum.
This paper reviews some of the changes that have taken
place in teaching Principles or Concepts at the British
School of Osteopathy (BSO), the rationale behind the
changes and the challenges that face this subject area.
From 1917, when the BSO was founded, until
through to the 1950s, The Principles of Osteopathy to* Corresponding author.
E-mail address: [email protected] (K. Nash).
1746-0689/$ - see front matter Ó 2005 Elsevier Ltd. All rights reserved.
doi:10.1016/j.ijosm.2005.02.005
International Journal of Osteopathic Medicine 8 (2005) 29e37
www.elsevier.com/locate/ijosm

7/30/2019 An Account of the Development of the Conceptual Basis of Osteopathy Course at the British School of Osteopathy
http://slidepdf.com/reader/full/an-account-of-the-development-of-the-conceptual-basis-of-osteopathy-course 2/9
a large extent equated to the whole of the osteopathy
course. Principles of Osteopathy was taught without the
subject demarcations that are familiar in the contempo-
rary tertiary education environment. As the course
expanded over the years, both in terms of the number of
students and the scope of the academic syllabus, the
need to divide content into manageable areas of studybecame apparent. An unexpected consequence of this
development was that three separate ‘cultures’ devel-
oped within the school, namely academic faculty,
technique and clinic. This separation may in part arise
because of the different teaching expertise and structures
of working demanded by these curriculum areas. During
2003 and 2004, the BSO undertook a review of the CBO
subject area in order to further develop the course.
Bringing these cultures together is one of the challenges
this curriculum review sought to address. A second
challenge was how to ensure that students were able to
apply the taught component of CBO into patient
management. This challenge was apparent to Colin
Dove, a lecturer at the BSO, who taught the course
between 1960 and 1980, and it provided the impetus for
this current review.
2. Historical development of the course
John Martin Littlejohn, who founded the BSO in
1917, published a series of lectures on the subject of
Psycho-physiology in 1899.1 He had given these lectures
to students at the American School of Osteopathy. In
the preface to this work he writes:
‘‘The aim is to make the Psychology entirely physiolog-
ical and in this way to lay down a basis for the treatment
of Psycho-pathology and therapeutics, so that the field
of Medicine covered by Osteopathy may be all inclusive,
including means and methods of dealing with the entire
organism of the body and mind.’’
We will further discuss Littlejohn’s lectures again
later in this article. There is some mention in later
works2 that Littlejohn considered ‘mental’ or ‘psycho-
logical’ factors as being contained within the ambit of
‘osteopathic’ lesions. He may well have considered
adjustment (a term that is now commonly associated
with chiropractic) as addressing many levels of a pa-
tient’s life, not simply a technique to address musculo-
skeletal problems. However, in later osteopathic
writings, (for example those of Webster-Jones3 from
the early 1950s), there seems to have been more
concentration on anatomy, physiology, pathology and
treatment plans for specific conditions. These areas were
presented in the context of osteopathic principles: for
example, the role of ‘vital force’ in the preservation of
health, and disease as an effect of imbalance or mala-
djustment. Diagnosis and the technique of adjustment
were seen as synonymous terms and taught together. It
is difficult to ascertain to what extent Littlejohn
incorporated psychology or any of the philosophy and
humanities that he had studied prior to osteopathy, into
his teaching at the BSO. If he did, it may have been that
for his students these insights became implicit.
Shilton Webster-Jones who followed Littlejohn asPrincipal of the BSO, taught a Principles of Osteopathy
course in the 1950s. Webster-Jones’ hand written
Principles of Osteopathy notes, undated, but probably
written in the early 1950s, contain a mix of the current
subject boundaries in osteopathy. Some of the content
includes: a discussion of the defining features of
osteopathy, namely; the significance of the ‘vital force’
in health; function; the self healing properties of the
body and maladjustment as the cause of disease; are all
ideas that are still discussed in the concepts course
today. However, Webster-Jones also includes evalua-
tion, diagnosis, technique, and treatment and manage-
ment for specific conditions under the umbrella of
‘principles’.
In the mid 1950s, Jocelyn Proby4 took over the
teaching from Webster-Jones for about a year. Proby
taught a very structurally based course, looking at
‘triangles of forces’. In his book The Mechanics of the
Spine and Pelvis (undated) he describes this work as
based on lectures given at the BSO in 1934, and based
on research carried out by Littlejohn in 1900. Proby also
shared his interest in naturopathic ideas with the
students, for example the role of diet.
Colin Dove commenced teaching the Principles of
Osteopathy in 1960. He had been frustrated by the lackof a scientific basis in the teaching he had received as
a student, and turned to research into the neurophys-
iological effects of the osteopathic lesion, which was
being published by American osteopaths and associated
researchers around this time. In particular, Dove was
impressed by Irvin Korr’s work on spinal cord
facilitation and the concept of the ‘neurological lens’,
which was based on Denslow’s research begun in the
1940s.5 Dove also incorporated the work of Barry
Wyke, a neurophysiologist who had investigated the role
of joint receptors,6 as well as Melzack and Wall’s gate
control theory of pain.7 In 1967, Dove was invited to
give the Littlejohn Memorial Lecture in which he
outlined Korr’s work and signalled a major change in
the way that the Principles of Osteopathy would be
taught at the BSO.8 The course, which was mostly
neurophysiology from an embryological perspective
focused on neurological links between the somatic and
visceral structures. By 1970, he no longer taught ‘theory
of the osteopathic lesion’, because in common with BSO
faculty member Audrey Smith, he felt it was restricting
students’ ability to achieve a complete evaluation of the
patient. Instead, the idea of somatic dysfunction, which
Colin Dove considered to be just another term for the
30 K. Nash, S. Tyreman / International Journal of Osteopathic Medicine 8 (2005) 29e37

7/30/2019 An Account of the Development of the Conceptual Basis of Osteopathy Course at the British School of Osteopathy
http://slidepdf.com/reader/full/an-account-of-the-development-of-the-conceptual-basis-of-osteopathy-course 3/9
osteopathic lesion and equally flawed, began to be used
in referring both to a specific segmental phenomenon
capable of detrimentally influencing normal neurologi-
cal patterns, and in a broader whole person sense of
disruption to integrated physiological processes.
At the same time as Dove was starting to focus on
neurophysiology, Audrey Smith was developing anosteopathic diagnostic model based on the ‘pathological
sieve’, which analysed ‘the lesion’ in terms of patholog-
ical changes in specific identifiable tissues. Although
these ideas cross-referenced with changes in the Princi-
ples course, they were not entirely compatible with the
ideas that were being introduced there. On the one hand
the focus was on identifying pathological tissues in
a very specific and localised way, while on the other
it was looking at disruption to complex body-wide
patterns of physiological function. By the time he retired
from teaching the course in 1980, Dove was introducing
the idea of psychological and social stress as important
causal factors in conditions as diverse as cardiac disease,
stomach ulcers and low back pain. This change, as
highlighted earlier, reintroduced ideas that Littlejohn
had considered when he referred to psycho-physiology.
3. The recent era
The ‘Principles course’ was taken on by Kathy
Curtis-Lake (nee Keuls) when Colin Dove retired from
this teaching role in 1980. Curtis-Lake set about
broadening the course content. In particular, she was
interested in the way the health of the musculoskeletalsystem and structural components of the body influence
the general health of the individual in the long term.
Sadly, her tragic death at an early age prevented her
developing her ideas further, and deprived the pro-
fession of a potentially valuable contribution.
Stephen Tyreman took over the Principles course
from Curtis-Lake, and he attempted to build on the
scientific foundations that Dove had established, while
also looking more broadly at other ideas. Tyreman, not
wanting to rely solely on the work of Korr, began to
investigate other research in the area of neurophysiology
which demonstrated integrated and interdependent
neurological effects which could be disrupted by a range
of dysfunctions. In particular, Hans Selye’s9 concept of
stress as an adaptive response of the individual to
changes in their environment began to form an
important part of the course. This focus on stress was
in some ways a return to Littlejohn’s claim that
osteopathy is the ‘‘science of adaptation’’.1
Critically examining and updating traditional osteo-
pathic principals was considered by Tyreman as a key
part of programme development, and early in the
revised course a number of influential thinkers from
the profession were brought together to discuss and
critically review what the fundamental claims of
osteopathy are.
Tyreman started to introduce the work of a number
of important thinkers into the course: the works of
Larry Dossey,10 Rupert Sheldrake,11 Fritjof Capra,12
D’Amico13 and others began to be interpreted in the
context of health and osteopathic care. However,perhaps the most important change came with the
introduction of General Systems Theory into the
course.14,15 General Systems Theory offered a theoret-
ical basis for understanding and analysing the idea that
the body is holistic and needs to be understood as
a whole.
Clive Standen and then Bevis Nathan joined the
faculty of the BSO during the 1980s. In 1989 they, along
with Stephen Tyreman, registered on a Master of Arts
degree programme at the Centre for the Study of
Philosophy and Health Care, University College Swan-
sea. This opened all of them up to ideas from other parts
of health care and to the academic rigour of philosoph-
ical analysis. Clive Standen studied the concept of needs
in contemporary healthcare, Stephen Tyreman became
interested in the Philosophy of Science and the concept
of function in biology and health care, while Bevis
Nathan became interested in touch as a central aspect of
osteopathic practice. These subjects each share obvious
importance to osteopathy.
In addition to the curriculum developments of this
period, a significant change was made to the title of the
course which was approved as the ‘Concepts of
Osteopathic Health Care’ in an attempt to recognise
that osteopathy has as much, and perhaps more incommon, with other areas of health care and academic
life, and draws on a wide range of disciplines to explain
and understand its practices. The broad theoretical
basis, on which the course operates, has made the
course a particularly difficult one to both teach, and
learn as a student, since it covers a wide range of topic
areas including physiology, psychology, sociology,
philosophy, communication skills, critical thinking as
well as the history of medicine and osteopathy. Because
the course is concerned with ideas and critical analysis
it has always had the effect of polarising student
opinion with respect to the relevance of some of the
material to their chosen career. At least anecdotally,
there is considerable variation in the way students
engage with the material. Some immediately perceive
the relevance to practice. In the focus groups, which
will be described later, several osteopaths commented
that it was only after being in practice that they
realised the relevance of the concepts course. Extensive
written material was generated to support the course.
This was developed out of necessity because it was not
possible to refer the students to a single key text. The
course material was in the main produced by Stephen
Tyreman, with the module on touch authored by Bevis
31K. Nash, S. Tyreman / International Journal of Osteopathic Medicine 8 (2005) 29e37

7/30/2019 An Account of the Development of the Conceptual Basis of Osteopathy Course at the British School of Osteopathy
http://slidepdf.com/reader/full/an-account-of-the-development-of-the-conceptual-basis-of-osteopathy-course 4/9
Nathan. Because of the broad theoretical basis of the
course, developing the course materials proved to be an
extensive and challenging task. It became apparent that
the very comprehensive and eclectic nature of the
material could have a limiting effect on the student’s
independent learning.
With the introduction of the Bachelor of Osteopathydegree at the BSO in 2000, and the reorganisation of the
course, ‘concepts’ became integrated into a larger area
of study that incorporated the history of medicine and
osteopathy, psychology and sociology. The whole sub-
ject area was overseen by Kate Nash. This large and
critical area of study became known as ‘The Conceptual
Basis of Osteopathy’ (CBO). Tyreman reduced his
involvement with teaching the CBO component of the
course in 1997 and this was taken over by a team of
three headed by BSO faculty member Andy Cotton. The
team took on the challenge of improving the clinical
relevance of the material using case histories to highlight
the relevance of the conceptual material. However, by
2003 it became apparent that a major review of the
course needed to be undertaken.
4. Reasons for review
As mentioned in the introduction, the main reason
for the review was the need to structure the CBO course
in such a way that students are enabled to apply the
theoretical content to clinical encounters. Five further
reasons for the CBO course review were identified by the
course team:
1. By 2003, the written material was 10e15 years old
and in urgent need of updating and revision.
2. There had been important changes to the profession
in recent years including the self-regulation of
osteopathy by statute, the introduction of degree
level study in osteopathy, and an increasing in-
volvement by osteopaths in the National Health
Service.
3. During 1998e1999 when the restructuring of the
course from a diploma to a modular degree was
being undertaken, a number of different areas, for
example sociology, psychology, the history of
medicine and the history of osteopathy, in addition
to the formal CBO content, were incorporated into
the CBO area of study. There were insufficient
resources available at that time to integrate these
related disciplines into a coherent whole with clearly
stated inter-relationships.
4. The student feedback from course evaluation data
contained some negative comment. Students were
finding it difficult to perceive the relevance of the
material for their careers as osteopaths. This in part
may have been because in the degree the course CBO
was taught from year 1, as opposed to year 2. It was
intended that by introducing CBO earlier in the
programme, students would be able to apply the
ideas they met in this area of study to other areas of
the curriculum. However, students have little clinical
experience at this stage, so the material needed to be
adapted to be more accessible to Level 1 learners.5. The degree course programme was due for quin-
quennial review in 2005 and the CBO review would
fit into this wider process.
5. Process of the review
Focus groups were held in September and October
2003. All faculty members at the institution were invited
to attend. Material outlining the current aims and
content of the CBO course was distributed with the
invitation. Attendance was voluntary. Five separate
focus groups were organised, with one on each day of
the week in order to allow all staff to attend even if they
only worked one day a week. Four groups were
convened and varied in size from 6 to 10 participants.
There was active involvement and open expression of
views in all the groups regardless of the size. On the fifth
day, only one participant was available. They were
interviewed by the facilitator, so that their views could
be included. Each group had one facilitator and
a designated note taker. Two of the facilitators had
attended a training course in focus groups. A week
before the focus groups were held the facilitators met fora training session. All focus group discussions were
recorded on audio tape so that matters of accuracy from
the written notes could be verified. The members of each
group were informed that their contribution would be
confidential, but given the nature of a small institution
like the BSO, where individuals may be known for
particular views, their anonymity could not be assured.
The opening question posed by the facilitator to the
group was: ‘‘What do you think students need to know
about the conceptual basis of osteopathy in order to be
able to practice.’’
To facilitate discussion a variety of cards were placed
on the table with titles of topics currently taught on the
CBO course, as well as topics that could potentially be
included. Participants were invited to sort these cards
according to their perceived importance.
The follow up question posed by the facilitator for
group discussion was: ‘‘Are there any other topics which
you feel should be included in the CBO course?’’
The notes taken at the group were distributed to all
members for comment as to whether they accurately
represented the discussions before further analysis took
place. Thirty-seven individuals in total were involved in
the focus groups. The researcher then analysed the
32 K. Nash, S. Tyreman / International Journal of Osteopathic Medicine 8 (2005) 29e37

7/30/2019 An Account of the Development of the Conceptual Basis of Osteopathy Course at the British School of Osteopathy
http://slidepdf.com/reader/full/an-account-of-the-development-of-the-conceptual-basis-of-osteopathy-course 5/9
notes for themes. This process was shared with the
facilitators.
6. Analysis
There was considerable diversity of opinion ex-pressed by participants. In fact for each opinion
expressed the opposite stance was argued, either within
the group or across the groups. Not all the participants
trained as osteopaths at the BSO, which may in part
account for the rich mix of views. However, there were
some themes that occurred commonly irrespective of
training, and others that were expressed by several
participants.
6.1. Commonly occurring themes
1. It is our osteopathic concepts that distinguish usfrom other physical therapists
No uniformity arose out of the focus groups as to what
these concepts were, a finding that also emerged from
Corson’s survey of osteopaths.16 There was acknowl-
edgement from the majority of participants for the need
to be clear about the nature of evidence we as teachers put
forward to support osteopathic concepts.
2. There are different models of osteopathy being
practiced and taught within the BSO, within the
UK and internationally.
There was a clear expression of the need to be more
open about differences in opinion amongst osteopaths
teaching both the BSO and also more broadly within the
wider profession. Students quickly become aware of
these differences and can lose confidence if the diversity
of views amongst the faculty is not expressed in an open
way within a culture of critical thinking. It was also
recognised as being important to develop at least some
common ground that all faculty members at the BSO
may broadly accept even though they may disagree on
some of the finer points.
3. It is the practical application of osteopathic concepts
that is important.
This theme, which relates to one of the reasons for
carrying out the review, led to passionate expression of
views. A key question posed by one of the participants
was:
‘‘How can we translate to the novice learner the
unconscious expression of a conceptual framework
that the experienced practitioner is able to do un-
consciously?’’
This relates to another key question posed by another
participant:
‘‘How can we ensure that conceptual material is
delivered in a way that has practical application for
students and their patients?’’
A key connecting theme here was that students foundit difficult to recognise physiology as a link between
evaluation and care. Emotional and psycho-social envi-
ronments cause physiological changes that may lead to
palpably different tissue states. The following quote
from Littlejohn1 in which he explores the relationship
between environment, mental state and physical func-
tion is pertinent to this discussion:
‘‘While the body is a machine, it is not a machine that
is wound up and capable of going for a number of
years wholly under external influence. The moulding
and shaping of the body is from within. Mental
function is at the basis of every physical function.Behind the physical acts involved in digestion,
respiration and circulation there is a mental state
which determines the body condition. It is a notorious
fact that civilization has increased disease and body
weakness. This is due to the fact that along with
civilisation comes a mental excitement that is not
conducive to body health. There is involved a higher
mental effort, a greater struggle for existence which
causes the normal development of mind and body to
be lost sight of and involves the body in numberless
disturbed conditions and diseases.’’
7. Issues to do with content
There was general agreement that ‘Philosophy of
Science’ and ‘General Systems Theory’ were given too
much emphasis and should be in the course more as
background or as a context within which to understand
holism. However, there were extremes of opinion
expressed, some participants feeling that Philosophy of
Science was absolutely essential while others felt it
should be dispensed with altogether.
There was a strong feeling that students should
have a foundation in critical thinking and be clear
about the hierarchy of evidence in relation to
osteopathy. While accepting that we need to give
students confidence in their chosen career, they do
need to be introduced to the idea that practice is
uncertain and evidence may not be produced in some
areas.17
There was strong support for the notion that the
History of Medicine, the History of Osteopathy and
some understanding of Complementary and Alternative
Medicine (CAM) therapies should be taught in a more
integrated manner. Interestingly, this integration had
33K. Nash, S. Tyreman / International Journal of Osteopathic Medicine 8 (2005) 29e37

7/30/2019 An Account of the Development of the Conceptual Basis of Osteopathy Course at the British School of Osteopathy
http://slidepdf.com/reader/full/an-account-of-the-development-of-the-conceptual-basis-of-osteopathy-course 6/9
been the case when Colin Dove taught this subject in the
1980s.
There was discussion as to the content of the CBO
course as a whole. There were many topics that some
participants felt were important for students to be
introduced to, but they felt there was potential for the
size of the CBO curriculum to become unmanageable.
There was also concern that there was some overlap
between different areas of study and that students might
be being over-taught.
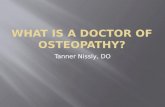
V E R T I C A L T H E M E S R E P R E S E N T T H E T A U G H T C O N T E N T A T L E V E L 2
C O N T E X T U A L I S I N G O
S T E O P A T H Y - a
b r o a d o v e r v i e w
I N T R O D U C T I O N
T O C
R I T I C A L T H I N K I N G A
N D
E P I S T E M O L O G Y
T H E H I S T O R I C A L D E V E L O P M E N T O F
O S T E O P A T H Y – i n r e l a t i o n t o t h e h i s t o r y o f m e
d i c i n e
H E A L T H
C A R E C O N C E P T S - h o w
i s o s t e o p a t h y s i m i l a r o r d i f f e r e n t f r o m o
t h e r f o r m s o f h
e a l t h c a r e ?
H E A L T H
B E L I E F S A N D
B E H A V I O U R S
P S Y C H O L O G I C A L A N D
E M O T I O N A L D E V E L O P M E N T T H R O U G H
T H E L I F E C O U R S
E
S O C I O L O G I C A L A S P E C T S O F H E A L T
H
I N T E G R A T I O N
APPLICATION OF THEORY TO PRACTICE
AWARENESS OF DIVERSITY
AWARENESS OF UNCERTAINTY-
Openness to debate and differences of opinion within osteopathy
LEVELS OF EVIDENCE
Intuition---------------------------------------------------------------------Randomised Double-Blind Trials
CRITICAL THINKING
HORIZONTAL THEMES REPRESENT THEMES THAT UNDERPIN THE WHOLE COURSE
Fig. 1. Schematic representation of conceptual basis of osteopathy curriculum at Level 1 (1st year level).
34 K. Nash, S. Tyreman / International Journal of Osteopathic Medicine 8 (2005) 29e37

7/30/2019 An Account of the Development of the Conceptual Basis of Osteopathy Course at the British School of Osteopathy
http://slidepdf.com/reader/full/an-account-of-the-development-of-the-conceptual-basis-of-osteopathy-course 7/9
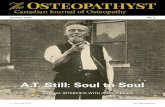
An overview of the musculoskeletal system
The body as a unit from 2 perspectives:
1. physiologically 2. philosophically (holism)
Adaptation to the environment:
1, structure, function and agency 2. posture, gait and response to injury 3. emotional and
psychological adaptation
Stress and the social environment
Stress and the Autonomic Nervous System
Stress and Immunity
Fluid Dynamics
Pain
Palpation
TOUCH
Physiological and psychological aspects of touch
Looking at the individual from
different psychological
perspectives
Concepts and theories of osteopathic treatment and their mechanism of effect
Evidence for the ‘whole person’ approach to treatment
The placebo and ‘nocebo’ effect
Patient empowerment
How do we understand osteopathic theory in the light of current evidence?
INTEGRATION
EVALUATION
TREATMENT
MANAGEMENT
Fig. 2. Schematic representation of conceptual basis of osteopathy curriculum at Level 2 (2nd year). The diagram should be read from above downwar
including touch are particularly relevant to patient evaluation. Elements that appear below touch and including touch have particular relevance for tre

7/30/2019 An Account of the Development of the Conceptual Basis of Osteopathy Course at the British School of Osteopathy
http://slidepdf.com/reader/full/an-account-of-the-development-of-the-conceptual-basis-of-osteopathy-course 8/9
8. Further development
After the material was transcribed and analysed for
themes, a further meeting was held of focus group
leaders, lecturers on the CBO course and any other
interested parties to begin development of a curriculum
outline with reference to the themes that had emergedfrom the focus groups. There were further contributions
by members of faculty who had not contributed to the
focus groups made via an on-line discussion group. At
least five very different models emerged from this
process. However, there were three common themes:
(1) that students should begin with a broad introduction
to osteopathy, (2) that they should be taught how to
apply CBO in a clinical context and (3) that they should
be introduced to different models of osteopathy later in
their clinical career. For example, models of osteopathy
in this context might include osteopathy as an alterna-
tive to orthodox medicine, osteopathy as therapy for
specialising in musculoskeletal conditions, visceral
osteopathy, and osteopathy in the cranial field.
Further discussions with the CBO faculty led to
making a distinction between horizontal themes that
underpinned and informed the course throughout all
years and vertical themes that represented content. The
horizontal themes included: (1) Application of Theory
to practice (2) Awareness of Diversity (3) Awareness of
Uncertainty (3). The Hierarchy of Evidence (from
Intuition through to Randomised Controlled Trials
and Meta-Analyses) (4) Critical Thinking. A model of
the Level 1 course is shown in Fig. 1.
Two major challenges in developing and delivering thecourse were to make the curriculum clinically relevant
and make clear the physiological interface between
evaluation and treatment. The Model for the Level 2
(second year curriculum) curriculum is shown as Fig. 2. In
this model, ‘Touch’ is seen as central because it informs
both patient evaluation and treatment. Perhaps this could
be seen as distantly mirroring Littlejohn’s belief that
diagnosis and the technique of adjustment are synony-
mous. The curriculum is arranged as a clinical encounter
working through content that is relevant to osteopathic
evaluation and content that relates to osteopathic
treatment and management. Psychology and sociology
are seen as inter-relating with this approach at all levels.
In addition we have attempted to integrate physiology
and psychology where possible. So for example, adapta-
tion is not taught simply as a structural adaptation to
physical circumstance but alongside positive and negative
psychological adaptive mechanisms.
9. A note on Level 3 of the CBO course
The Level 3 (year 4) of the CBO course did not form
part of the curriculum review, but we briefly discuss it
here for completeness. In the degree course CBO is
taught at Level 3 in students’ final year, the Pre-
professional Phase. By this stage, it is intended that
students are able to integrate the various components of
the degree course, and subject boundaries are less
relevant. For this reason, the taught component of
CBO is combined with two other areas of study:‘Professional Capability’ which is primarily clinical
work, and ‘Applied structure e Function’. As part of
Level 3 assessment, students are required to prepare
a written case study and 10 min oral presentation based
on a patient they have been treating in clinic, which
demonstrates their understanding and application of
CBO.
In order for students to prepare for this assessment,
and to encourage deeper levels of reflection and thinking
about practical application of CBO from an early stage
in their learning, we are planning to gradually introduce
a workbook to accompany the course over all levels.
This workbook will use clinical vignettes and other
sources of information to demonstrate links between
theory and practice.
10. Conclusion
Developing and implementing a curriculum for the
conceptual basis of osteopathy is a complex task,
because students are completing one curriculum while
the new curriculum is being developed. In addition we
need to reflect changes in scholarship as well as changesin the profession as it continually evolves. We do not
know at this stage whether the new model will achieve
its stated aims. Student feedback and assessment
outcomes are essential components of the development
process, as are contributions from the faculty and the
wider profession. The external examiners report for the
Final Clinical Competence Assessment in 2004 did note
that there was evidence on the whole that students were
attempting to apply osteopathic principles and review-
ing their patients status in a wider psychosocial context.
We will be reflecting on all these sources of information
as we continue to develop the course.
Acknowledgements
We thank Colin Dove for being interviewed about his
experience of being taught and teaching ‘principles’, and
for lending us Webster Jones’ handwritten notes. Hilary
Abbey, Adrian Barnes, Mark Corson and Steven Vogel
for facilitating the Focus Groups. All the members of
the faculty who gave up time to contribute to the
process. Will Podmore, librarian at the BSO for his help.
36 K. Nash, S. Tyreman / International Journal of Osteopathic Medicine 8 (2005) 29e37

7/30/2019 An Account of the Development of the Conceptual Basis of Osteopathy Course at the British School of Osteopathy
http://slidepdf.com/reader/full/an-account-of-the-development-of-the-conceptual-basis-of-osteopathy-course 9/9
References
1. Littlejohn JM. Psycho-physiology. Kirksville, MO: EG Kinney;
1899.
2. Hall TE. The contribution of John Martin Littlejohn to osteopathy.
The British School Osteopathy. The Osteopathic Publishing Co
Ltd; 1952.
3. Webster-Jones S. Handwritten notes, unpublished.4. Proby J. Course notes: the mechanics of the spine and pelvis. The
Maidstone College of Osteopathy; undated.
5. Beal MC editor. Selected papers of John Stedman Denslow, DO.
Indianapolis: American Academy of Osteopathy; 1993.
6. Wyke B. Articular neurology e a review. Physiotherapy 1972;58:
94–9.
7. Melzack R, Wall PD. Pain mechanisms: a new theory. Science
1965;150:971–9.
8. Dove C. A history of the osteopathic vertebral lesion. Br
Osteopath J 1967;3:2–17.
9. Selye H. The stress of life. New York: McGraw Hill; 1976.
10. Dossey L. Beyond illness: discovering the experience of health 1984;.
Boston.
11. Sheldrake AR. A new science of life: the hypothesis of formative
causation. London: Blond and Briggs; 1985.
12. Capra F. The turning point. London: Flamingo; 1982.
13. D’Amico R. Is disease a natural kind? J Med Philos 1995;20:
551–69.
14. Emery FE editor. Systems thinking: 1. Penguin: Harmondsworth;
1981.
15. Von Bertalanffy L. The theory of open systems in physics and
biology. In: Emery FE editor. Systems thinking. Penguin:
Harmondsworth; 1981.
16. Corson M. Unpublished Masters Thesis ‘What makes and
osteopath an osteopath? An investigation into the characteristics
of osteopathy’ completed as part of The Masters in Osteopathic
Health Care at The British School of Osteopathy, 2000.
17. McMullin E. Underdetermination. J Med Philos 1995;20:
233–52.
Further reading
18. Littlejohn JM. Notes on the principles of osteopathy. Maidstone
College of Osteopathy; 1971.
19. Norminton. The Littlejohn companion. Maidstone College of
Osteopathy, undated.
37K. Nash, S. Tyreman / International Journal of Osteopathic Medicine 8 (2005) 29e37