AML IN OLDER PATIENTS Whenever possible, intensive ... · Hematopoietic precursors are...
22
AML IN OLDER PATIENTS Whenever possible, intensive induction therapy should be considered Charles A. Schiffer, M.D. Karmanos Cancer Institute Wayne State University School of Medicine Detroit, MI
Transcript of AML IN OLDER PATIENTS Whenever possible, intensive ... · Hematopoietic precursors are...

AML IN OLDER PATIENTS Whenever possible, intensive induction therapy should be considered
Charles A. Schiffer, M.D. Karmanos Cancer Institute Wayne State University School of Medicine Detroit, MI

WHY ARE MOST SUBTYPES OF AML SO DRUG RESISTANT?
•
Hematopoietic precursors are “designed”
to survive repeated exposure to multiple types of natural toxins
•
Most resistance mechanisms have been shown to be amplified in undifferentiated precursors
•
They can survive exposure to huge doses of chemotherapeutic agents in vitro (marrow “purging”)Therefore,It is not surprising that leukemias which derive from hematopoietic stem cells are particularly resistant (eg - Ph chromosome pos diseases, MDS, MPD, FAB M0)

HOW TO DEFINE AML
and
WHO IS BEING TREATED ON THESE TRIALS?

OLDER ELDERLY
“REAL” AML WHO – MDS/AML

Burnett et al, Cancer 109:1114, 2007
MRC – LOW DOSE ARA-C vs.SUPPORTIVE CARE – MEDICALLY“UNFIT” PATIENTS
~ 15% CR

S0432: Overall Survival by Tipifarnib Regimen
Erba et al Blood 2007; 110: 136a (abstract 440)

THE ISSUE OF “UNFIT” FOR “INTENSIVE” THERAPY
•
Very subjective and difficult to definePS, “comorbidities”, karyotype
•
Implications for clinical trials •
Critical in making recommendations for individual patients
•
Implications for new drug assessment/approval
Control arm?

Azacitidine Treatment Prolongs Overall Survival in Higher-Risk MDS Patients
Compared with Conventional Care Regimens: Results of the AZA-001 Phase III Study
Azacitidine Treatment Prolongs Overall Azacitidine Treatment Prolongs Overall Survival in HigherSurvival in Higher--Risk MDS Patients Risk MDS Patients
Compared with Conventional Care Compared with Conventional Care Regimens: Results of the Regimens: Results of the AZAAZA--001 Phase III Study001 Phase III Study
P Fenaux, MD, GJ Mufti, MD, V Santini, MD, C Finelli, MD, P Fenaux, MD, GJ Mufti, MD, V Santini, MD, C Finelli, MD, A Giagounidis, MD, R Schoch, MD,A List, MD, S Gore, MD, A Giagounidis, MD, R Schoch, MD,A List, MD, S Gore, MD, J Seymour, MD, E HellstromJ Seymour, MD, E Hellstrom--Lindberg, MD, J Bennett, MD, Lindberg, MD, J Bennett, MD,
J Byrd, MD, J Backstrom, MD, L Zimmerman, BSN, J Byrd, MD, J Backstrom, MD, L Zimmerman, BSN, D McKenzie, MS, CL Beach, PharmD and L Silverman, MD D McKenzie, MS, CL Beach, PharmD and L Silverman, MD
on behalf of the International Vidaza Highon behalf of the International Vidaza High--Risk MDS Risk MDS Survival Study GroupSurvival Study Group

Azacitidine Survival StudyAzacitidine Survival StudyAzacitidine Survival Study
AZAAZA 75 mg/m75 mg/m22/d x 7 d q28 d/d x 7 d q28 d
CCRCCRRandomizationRandomization
BSC was included with each armTx continued until unacceptable toxicity or AML transformation or disease progression
•
Best Supportive Care (BSC) only•
Low Dose Ara-C (LDAC, 20 mg/m20 mg/m22/d x 14 d q28/d x 14 d q28--42 d42 d))
•
Std Chemo (7 + 3)
Screening/CentralPathology Review
Investigator CCRTx Selection
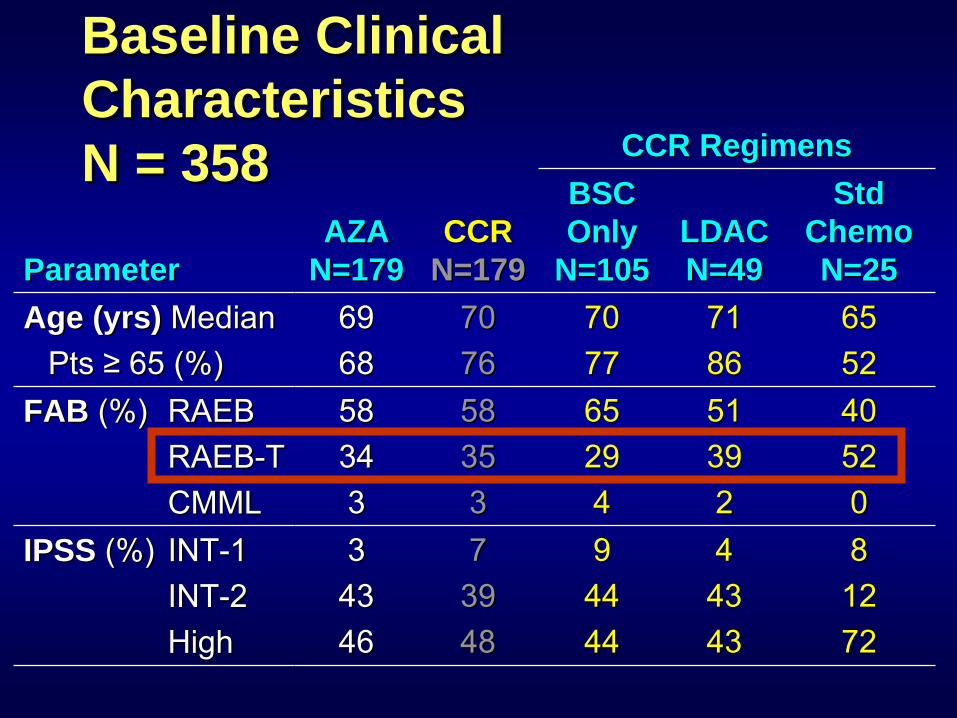
Baseline Clinical Characteristics N = 358
Baseline Clinical Baseline Clinical CharacteristicsCharacteristics N = 358N = 358
ParameterParameterAZA AZA
N=179N=179CCRCCR
N=179N=179
CCR RegimensCCR RegimensBSC BSC Only Only
N=105N=105LDAC LDAC N=49N=49
Std Std Chemo Chemo N=25N=25
Age (yrs) Age (yrs) MedianMedianPts Pts ≥≥
65 (%)65 (%)
69696868
70707676
70707777
71718686
65655252
FAB FAB (%)(%)
RAEBRAEBRAEBRAEB--TTCMMLCMML
5858343433
5858353533
6565292944
5151393922
4040525200
IPSS IPSS (%)(%)
INTINT--11INTINT--22HighHigh
3343434646
7739394848
9944444444
4443434343
8812127272

Overall Survival: Azacitidine vs CCR ITT Population
Overall Survival: Azacitidine vs CCR Overall Survival: Azacitidine vs CCR ITT PopulationITT Population
LogLog--Rank p=0.0001Rank p=0.0001HR = 0.58 [95% CI: 0.43, 0.77]HR = 0.58 [95% CI: 0.43, 0.77] Deaths: AZA = 82, CCR = 113Deaths: AZA = 82, CCR = 113
0 5 10 15 20 25 30 35 40
Time (months) from RandomizationTime (months) from Randomization
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Prop
ortio
n Su
rviv
ing
Prop
ortio
n Su
rviv
ing
CCRCCRAZAAZA
Difference: 9.4 monthsDifference: 9.4 months
24.4 months24.4 months
15 months15 months
50.8%50.8%
26.2%26.2%
And some do OK without treatment


SHOULD OLDER/ELDERLY PATIENTS BE TREATED?
SHOULD OLDER/ELDERLY SHOULD OLDER/ELDERLY PATIENTS BE TREATED?PATIENTS BE TREATED?
•
Not at all - supportive care
•
With standard anthracycline/cytarabine
•
With experimental therapy since it is hard to do “worse” – focus on noncytotoxics

Age, Performance Status and Early Death in AML
N = 437
Age, Performance Status and Age, Performance Status and Early Death in AMLEarly Death in AML
N = 437N = 437Performance
StatusDeath within 30 days
56-60 61-70
71+
0 0% 13% 9%
1 0% 14% 21%2 38% 19% 42%
3 17% 24% 62%
SWOG -
Appelbaum

Age, Performance Status and Complete Response Rate in AML
Age, Performance Status and Age, Performance Status and Complete Response Rate in AMLComplete Response Rate in AMLPerformance Complete Response
Status 56-60 61-70 +70
0 70% 40% 50%
1 60% 49% 38%
2 25% 38% 27%
3 50% 41% 29%
SWOG -
AppelbaumN = 437

THE MAJOR ADVANCE IN AML THERAPY IN THE
PAST 10-15 YEARS:
ZOFRANAZOLES FOR PREVENTION/TREATMENT OF INFECTIONS WITH MOLDS
LEUCOCYTE DEPLETION TO PREVENT ALLOIMMUNIZATION
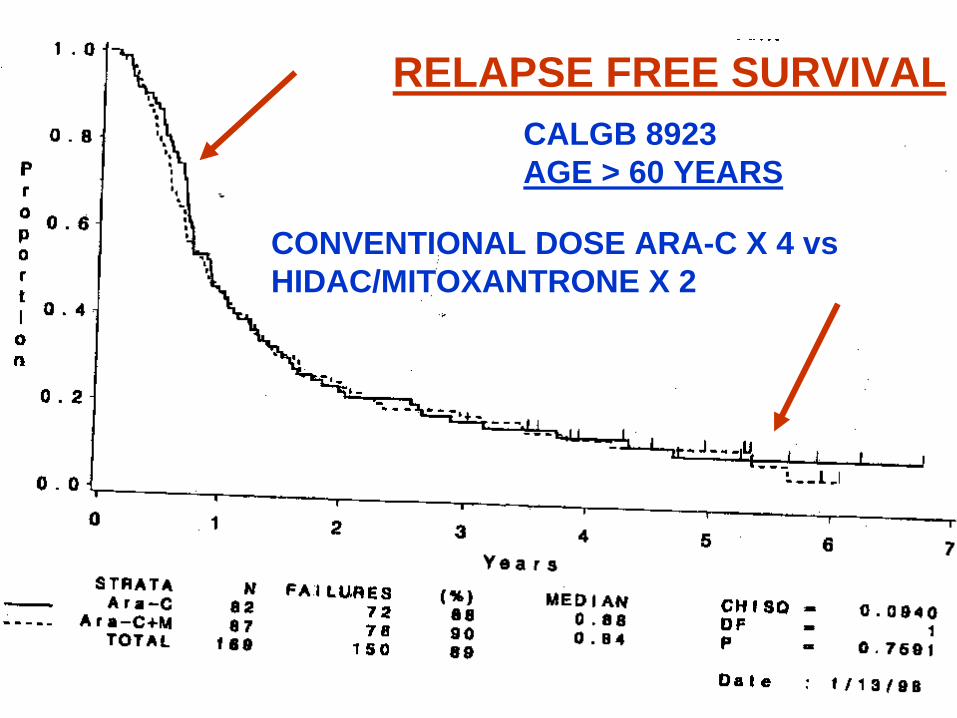
CALGB 8923AGE > 60 YEARS
CONVENTIONAL DOSE ARA-C X 4 vsHIDAC/MITOXANTRONE X 2
RELAPSE FREE SURVIVAL

THE DECISION FROM HELL: MDS PATIENT WITH WORSENING
CYTOPENIAS AND INCREASING BLASTS
•
AML induction therapy – “7 & 3”
•
Decitabine or azacytidine`•
Azacytidine + GO
•
GO•
Clofarabine
•
Low dose Ara-C•
Clinical trials
•
Supportive care

WHAT TO DO TOMORROW FOR POST REMISSION THERAPY FOR PATIENTS
NOT ON A CLINICAL TRIAL•
Assess patient’s goals
•
Individualize•
Conventional dose Ara-C
•
HIDAC for the occasional patient with favorable cytogenetics or NPM1 mutated
•
No maintenance•
Don’t rush into reinduction treatment
•
Consider clinical trials of non- myeloablative allogeneic transplantation


A CRITICAL CHALLENGE: THE DEVELOPMENT OF METHODOLOGY
TO EFFICIENTLY EVALUATE NEW NONCYTOTOXIC THERAPIES
•
Angiogenesis inhibitors•
Tyrosine kinase
inhibitors -
FLT3
•
Farnesyl
transferase
inhibitors•
Modulators of apoptosis
•
Other signal transduction inhibitors•
Immunologic manipulations
•
Histone
deacetylase
inhibitors•
Et al

WHAT TO DO NEXT?
•
1200 -
1500 patients = 1-2 monster phase III studies or….
•
30 phase II exploratory trials-
dose/schedule
-
biologic correlates whenever possiblefocus on responders