AMALGAM RESTORATIONS
47
AMALGAM RESTORATIONS INTRODUCTION An Amalgam is an alloy that contains Hg as one of its constituents. American National Standards Institute (ANSI) / American dental Association (ADA) specification NO. 1 requires that amalgam alloys contain predominantly silver and tin. Unspecified amounts of other elements for eg Cu, Zn, Au and Hg are allowed in concentrations less than silver or tin content. Alloys containing zinc in excess of 0.01% are zinc containing alloys. There is no specification of low or high copper alloy per se. Historically, amalgam alloys contain 65 wt % silver 29 wt % tin <6 wt % copper a composition close to that recommended by G V Black in 1896. During 1970s high copper amalgams were developed. The clinical success of amalgam restoration is based on meticulous attention to detail. Each manipulative step from the time the cavity is prepared until the restoration has been polished can have an effect on the physical and chemical properties of amalgam and the success and failure of restoration violation of the fundamental principles of cavity preparation has contributed substantially to failure.
-
Upload
drshivanim -
Category
Documents
-
view
210 -
download
4
Transcript of AMALGAM RESTORATIONS

AMALGAM RESTORATIONS
INTRODUCTION
An Amalgam is an alloy that contains Hg as one of its constituents.
American National Standards Institute (ANSI) / American dental Association (ADA) specification NO. 1 requires that amalgam alloys contain predominantly silver and tin.
Unspecified amounts of other elements for eg Cu, Zn, Au and Hg are allowed in concentrations less than silver or tin content.
Alloys containing zinc in excess of 0.01% are zinc containing alloys. There is no specification of low or high copper alloy per se.
Historically, amalgam alloys contain65 wt % silver29 wt % tin<6 wt % copper
a composition close to that recommended by G V Black in 1896.
During 1970s high copper amalgams were developed.
The clinical success of amalgam restoration is based on meticulous attention to detail. Each manipulative step from the time the cavity is prepared until the restoration has been polished can have an effect on the physical and chemical properties of amalgam and the success and failure of restoration violation of the fundamental principles of cavity preparation has contributed substantially to failure.
PERTINENT MATERIAL QUALITIES AND PROPERTIES
Strength
Compressive strength
Tensile strength
Longevity

Ease of use
Clinically proven success.
* Amalgam is the only restorative material with an interfacial seal that improves over time.
INDICATIONS
The following is a list of clinical indication for amalgam restorations in Classes I, II, and VI.
1) Moderate to large restoration
2) Restorations that are not in highly esthetic areas of mouth.
3) Restorations that have heavy occlusal contacts.
4) Restorations that can’t be well isolated.
5) Restorations that extends onto root surfaces
6) Foundations
7) Abutment teeth for R PD
8) Temporary of caries control restorations.
CONTRAINDICATIONS
1) Esthetically prominent areas of post teeth
2) Small to moderate Class I & II restorations that can be well isolated.
3) Small Class VI restorations

ADVANTAGES
1) Ease of use
2) High tensile strength
3) Excellent wear resistance
4) Favourable long term clinical research results
5) Lower costs than for composite
6) Bonded amalgam have ‘bonding’ benefits
DISADVANTAGES
The primary disadvantages of amalgam relate to
Esthetics
Increased tooth structure removal
Other are
1) Non insulating
2) Weakens tooth structure unless bonded.
3) More technique sensitive if bonded
4) More difficult tooth preparation
5) Initial microleakage
(LCTE 2.5 times greater than tooth).

AMALGAM RESTORATIONS
CLINICAL TECHNIQUE
INITIAL CLINICAL PROCEDURES
A complete examination diagnosis and treatment plan must be finalized.
Assessment of operative site and assessment of occlusion
Local Anesthesia Profound anesthesia contributes to a comfortable and uninterrupted operative and usually results in a marked reduction in salivation.
ISOLATION OF THE OPERATING SITE Isolation for amalgam restorations can be accomplished with a rubber dam or cotton rolls.
OTHER PREOPERATIVE CONSIDERATIONS For eg , wedge for restoring a posterior proximal surface
TOOTH PREPARATION FOR AMALGAM RESTORATIONS
Because of amalgam’s physical properties It
1) Must be Placed in a tooth preparation that provides for or 90 degree or greater restoration angle at cavosurface margin.
2) Should have minimum thickness of 0.75 to 2 mm.
3) Should be placed into a prepared undercut form in the tooth in order to be mechanically retained.
CONSERVATIVE CLASS I AMALGAM RESTORATIONS
Conservative preparation is recommended to

* protect the pulp
* presence the strength of tooth
* reduce deterioration of amalgam restoration
Features of conservative preparations are
* minimal extension of tooth preparations
* supra gingival margins
* rounded internal angles
INITIAL TOOTH PREPARATION (establishing the outline form by extension of external walls to sound tooth structure, while maintaining a specified limited depth and providing resistance and retention form )
The outline form for Class I occlusal amalgam tooth preparation should include only the faulty occlusal pits & fissures.
Resistance principles include
1) Extending around the cusps to conserve tooth structure and prevent internal line angles from approaching the pulp horns too close.
2) Keeping the facial and lingual margin extension as minimal as possible between central groove and cusp tips.
3) Extending the outline to include fissures thereby placing the margins on relatively smooth sound tooth structure.
4) Minimally extending into marginal ridges without removing the dentinal support.
5) Eliminating a weak wall of enamel by joining two outlines that come close together (i.e. less than 0.5 mm apart)
6) Extending the outline form to include enamel undermined by caries
7) Using enameloplasty on the terminal ends of shallow fissure to conserve tooth structure
8) Establishing an optimal, conservative depth of the pulpal wall.

BUR RECOMMENDED →
# 245 bur
- head length = 3 mm- tip diameter = 0.8 mm - slightly convergent towards shank- slightly rounded corners of the end.
# 330 bur - for smaller cavities
- pear shaped version of # 245 bur
Procedure:Enter the deepest or most carious pit with a punch cut using No. 245 bur of high speed with water spray long axis of bur in kept parallel to long axis of tooth. * Depth of 1.5 mm is measured at central fissure * Depth of prepared external walls will be 1.5 – 2 mm .* Desired pulpal depth is 0.2 mm into DEJ. * Faciolingual width of no more than 1 mm
If entering distal pit, bur is tilted distally to prevent undermining the marginal ridge. (not more than 10 degrees).
The distance from the margin of such an extension to proximal surface should not be less than
* 1.6 mm for premolar
* 2 mm for molars.
Maintain the burs orientation and depth while moving from central tissue towards the mesial pit.
Care should be taken to not to undermine the marginal ridges.
If these fissures require extensions of more than a few tenths of millimeter,
* Change the bur size to smaller one.
Eg. # 169 L

# 329 L
* Use enameloplasty
Pulpal floor should follow DEJ to maintain a more uniform pulpal floor depth.
If fissure extends to marginal ridge, the long axis of bur should be changed to have slight occlusal divergence to mesial wall, otherwise marginal ridge will be devoid of dentinal support.
The strongest an ideal enamel margin should be made up of full length enamel rods resting on sound dentin, supported on the preparation side by shorter rods , also resting on sound dentin .
Direction of mesial and distal walls is influenced by remaining thickness of marginal ridge as measured from distal or mesial margin
Effect of various extensions in tooth preparation on tooth’s resistance to fracture
1. By crossing one marginal ridge at ¼ the intercuspal distance, there is almost 10% loss of a tooth’s resistance to splitting.
2. BY crossing two marginal ridges at ¼ the intercuspal distance, there is almost 15% of a tooth’s resistance to splitting.

3. By crossing one marginal ridge at 1/3 the intercuspal distance, there is almost 30% loss of a tooth’s resistance to splitting.
4. By crossing two marginal ridges by 1/3 the intercuspal distance, there is almost 35% loss of a tooth’s resistance to splitting.
5. By crossing one marginal ridge at ½ the intercuspal distance, there is almost 40% loss of tooth’s resistance to splitting.
6. By crossing two marginal ridges at ½ the intercuspal distance, there is almost 45% loss of a tooth’s resistance to splitting.
7. By crossing a crossing ridge at ¼ the intercuspal distance, there is almost 20% loss of a tooth’s resistance to splitting.
8. By crossing a crossing ridge at 1/3 the intercuspal distance, there is almost 35% loss of a tooth’s resistance to splitting.
9. By crossing a crossing ridge at ½ the intercuspal distance, there is almost 45% loss of a tooth’s resistance to splitting.
* Mesial and distal walls must CONVERGE OCCLUSALLY when distance is greater than 1.6 mm in premolars * Mesial and distal walls must DIVERGE OCCLUSALLY if only 1.6 mm distance is left

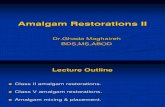
ENAMELOPLASTY
Enameloplasty refers to eliminating the developmental fault by removing with the side of flame shaped diamond stone. The surface left by enameloplasty should meet the tooth preparation wall preferably with a cavosurface angle 80-100 degrees.
If enameloplasty is unsuccessful in eliminating mesial fissure extending to Marginal Ridge, three alternatives are there
Make no further changes in the outline form
Extend through the marginal ridge when margins will be lingual to contact.
Include the fissure in conservative Class II tooth preparation.
Enameloplasty.
A, Developmental fault at terminal end of fissure. B, Fine-grit diamond stone in position to remove fault.
C, Smooth surface after enameloplasty.
D,Cavosurface angle should not exceed 100 degrees, and marginal-amalgam angle should not be less than 80 degrees. Enamel external surface (e) before enameloplasty When the remaining fissure is no deeper-than one quarter to one third the thickness of enamel, enameloplasty is indicated.
If enameloplasty is unsuccessful in eliminating mesial fissure extending to Marginal Ridge, three alternatives are there

Make no further changes in the outline form
Extend through the marginal ridge when margins will be lingual to contact.
Include the fissure in conservative Class II tooth preparation.
FINAL TOOTH PREPARATION
It includes
(1) Removal of remaining defective enamel and infected dentin on the pulpal floor
(2) Pulp protection
(3) Finishing external walls
(4) Cleaning and inspecting the prepared tooth
Removal of infected dentin is best accomplished by
discoid type spoon excavator
slowly revolving round carbide bur
If the tooth preparation is of ideal shallow depth no liner or base is indicated. In deeper carious excavations place a thin layer of RMGI base.
RMGI should be placed in deeper areas Entire dentin surface should not be covered. Dentin peripheral to liner should be available for bonding and support of restoration.
Occlusal cavosurface bevel is contraindicated in enamel preparations. Butt joint is strongest, i.e.
Cavosurface angle = 90 – 100 degreesAmalgam margins = 80 – 90 degrees
OTHER CONSERVATIVE CLASS I AMALGAM PREPARATION
The facial pit of mandibular molar
The lingual pit of maxillary molar

The occlusal pit of mandibular first premolar
The occlusal pits and fissures of maxillary first molar
The occlusal pit and fissures of the mandibulars second premolars
The preparation may be accomplished with a
- No. 245 bur
- No. 330 or 169 L bur if lesion is very small.
Retention grooves are added with No. ¼ or 33 ½ bur
CLASS I OCCLUSOLINGUAL AMALGAM RESTORATION
On maxillary molars when a lingual fissure connects with distal oblique fissure and distal pit on occlusal surface.
TOOTH PREPARATION
Preparation has occlusal and lingual convergence.
OCCLUSAL PREPARATION
Mesiodistal width of lingual extension should not exceed 1 mm, except when caries are extensive.
Tooth preparation should cut more at the expanse of oblique ridge rather than centering over fissure
On smaller teeth the occlusal portion may have a slight distal tilt to conserve the dentin support of distal marginal ridge.
Margins should extend as little as possible onto oblique ridge, DL cusp and distal marginal ridge
LINGUAL PREPARATION
Lingual extension may be accomplished by two techniques
I Lingual surface is prepared with burs long axis parallel with lingual surface holding the tip of bur at the gingival extent of lingual fissure.

The axial wall should follow the contour of the lingual surface of tooth, with a uniform depth of 0.5 mm inside the DEJ.
II No. 245 bur is held perpendicular to the cusp ridge and lingual surface as it extends the preparation from the occlusal surface gingivally. If it is wider mesiodistally additional retention by preparing locks in mesioaxial & distoaxial line angles.
LOCKS -
*depth of lock at the gingival floor is one half the diameter of No ¼ bur.* The cutting direction of each lock is the bisector of respective line angle. * Locks should diminish in depth towards the occlusal surface, terminating midway along axial wall.
CLASS II AMALGAM RESTORATIONS
CLASS II AMALGAM RESTORATIONS INVOLVING ONLY ONE PROXIMAL SURFACE
OCCLUSAL OUTLINE FORM
The occlusal outline from of a Class II tooth preparation for amalgam is similar to that for Class I tooth preparation .Enter the pit nearest the involved proximal surface.Before extending into the involved proximal marginal ridge, visualize the final location of facial & lingual walls of proximal box relative to the contact area. This will prevent the overextension of occlusal outline form where if joins the proximal box.
PROXIMAL BOX The initial procedure in preparing the outline form of the proximal box is isolation of proximal enamel by proximal ditch cut.
Extend the preparation mesially, stopping approximately 0.8 mm short of cutting through marginal ridge into contact area. 0.5 to 0.6 mm into dentinWith the same orientation of bur, cut the ditch gingivally 2/3 rd at the expense of dentin 1/3rd at the expense of enamel.

The ideal dentinal depth of axial wall of proximal box should be 0.5 to 0.6 mm. When extension places the margin in cementum, the initial pulpal depth should be 0.7 mm to 0.8 mm
REVERSE CURVE
Developing the mesiofacial wall perpendicular to the enamel rod direction and conserving the facial cusp structure results in reverse curve in occlusal outline of Class II preparation.
It permits 90 o amalgam at mesiofacial margins and yet curves around the mesial portion of facial cusp.
ADVANTAGES * mesiaofacial wall is perpendicular to the enamel rod direction* conserves the facial tooth structure
ISTHMUS WIDTH
One fourth the distance between the pulp tips
Extension of Margins
Facial/ lingual: Clearance of 0.2 – 0.3 mmGingival: clearance of 0.5 mm
The proximal ditch cut may be diverged gingivally to ensure the Faciolingual extension at gingival is greater than occlusal
A, Bur position to proximal ditch cut.

B, Proximal ditch in extended gingivally to desired level of gingival wall (i.e., floor). C, Variance in pulpal depth of axiolingual line angle as extension of gingival varies: a, at minimal gingival extension; b: at moderate extension; c, at extension that places gingival margin in cementum, whereupon pulpal depth is 0.75 to 0.8 mm and bur may shave side of wedge.
D, Proximal ditch cut results in axial wall that follows outside contour of proximal surface. E, Position of proximal walls (i.e., facial, lingual, gingival) should not be overextended with No. 245 bur, considering additional extension provided by hand instruments once remaining spurs of enamel are removed
MODIFICATION FOR CLASS II
IN TAPERED TEETH
In tapered teeth in which gingival margin of the proximal portion of preparation is located so far gingivally that preparing the regular facial and lingual retentive grooves will undermine tooth structure at axial angle of the tooth, one of the two types of grooves can be created.
(a) In line with axio pulpal line angle facially and lingually a groove is prepared on each of the facial and lingual walls, respectively. Each groove is started at the axio pulpal line angle and continues occlusally to the occlusal surface.
(b) Facial or lingual dentinal grooves may be prepared at the expense of facial or lingual walls of proximal portion, but having their maximum dimension at the pulpal floor level, tapering to a point termination at the bucco-gingivo-axial point angles i.e. the reverse arrangement of the regular retentive groove
In a narrow proximal lesion it is permissible not to extend. The Outline of the proximal box facially or lingually beyond the proximal contact to conserve the tooth structure.

To prevent the bur from marring the proximal surface of the adjacent tooth.
(a) Matrix band may be used around adjacent tooth
(b) A thin proximal enamel is spared which can be fractured out with a spoon excavator.
→ If the gingival cavosurface margin is in enamel, it will usually require a slight bevel.
PRIMARY RETENTION FORM
(1) The pulpal and gingival walls being relatively flat and perpendicular to forces directed with long axis of tooth
(2) Restricting extension
(3) Restricting occlusal outline form to areas receiving minimal occlusal contacts.
(4) Reverse curve
(5) Slightly rounding the internal line angles to reduce stress concentration
(6) Providing enough thickness of restorative material.
(7) Occlusal convergence of facial and lingual walls and occlusal dovetail.
SECONDARY RETENTION AND RESISTANCE FOR
RETENTION LOCKS

Bur: # 169 L Bur ( with air coolant & reduced speed. )
* Position: Axiofacial & axio lingual line angles 0.2 mm inside the DEJ
* Translation: direction of movement of axis of bur
* Depth: extent of translation (0.5 mm at gingival floor)
* Occlusogingival orientation: Tilt of bur which dictates occlusal height of the lock. (should disappear midway between enamel margin and dentin
Four characteristics of retentive locks. A, Occlusal view of MO preparation before placement of retention locks. B, Proximal view of MO preparation. C and D, position, transition, and depth. E, and F, Occlusogingival orientation

The use of retention locks in proximal boxes is controversial.
With high copper amalgam and dovetail design retention locks are unnecessary
VARIATION OF ONE PROXIMAL SURFACE TOOTH PREPARATIONS
Mandibular first premolar
When preparing the occlusal portion, bur is tilted occlusally (leading to facial inclination of pulpal wall). Otherwise it will weaken the lingual cusp.
Excessive extension in facial direction could approach and expose facial cusp.
Maxillary first molar
Extension into enamel oblique ridge is avoided whenever possible to maintain the cross splinting strength it provides to the tooth
When the occlusal fissure extends into the facial cusp ridge defect should be eliminated by extension of tooth preparation, accomplished by tilting the bur to create an occlusal divergence of facial wall, while maintaining the dentinal support.
In disto-occlusal tooth preparation an extension onto lingual surface should be prepared only after disto-lingual proximal margin is established. It is accomplished by preparing the lingual fissure extension more at the expense of mesio lingual cusp
Maxillary First Premolar
Mesiofacial embrasure is esthetically prominent therefore Class II mesial preparation requires special attention. The Occluso-gingival preparation of facial wall of mesial box should be parallel to long axis of tooth rather than converging occlusally to minimize unesthetic display of amalgam at faciogingival corner of restoration. The facial extension should minimally clear the contact.
If mesial proximal involvement
* is limited to a fissure in marginal ridge.
* is not treatable with enameloplasty
* doesn’t involve the proximal contact

Then the proximal portion of the tooth is prepared by extending through the fault with # 245 bur so that margins are lingual to contact.
Often this means that the proximal box will be the Faciolingual width of the bur and gingival floor may be at the same depth as pulpal floor.
If proximal caries is limited to mesiolingual embrasure , do not involve the mesial proximal contact in the tooth preparation.
BOX ONLY PREPARATION
When restoring a small, cavitated proximal lesion in a tooth with neither occlusal fissures nor a previously inserted occlusal restoration, a proximal box preparation without an occlusal step has been recommended.
To maximize retention, preparations facial and lingual wall should oppose each other
Retention locks are necessary
SLOT PREPARATION FOR ROOT CARIES
This is indicated if caries are appreciably gingival to proximal contact. The tooth preparation is usually approached from facial and has a form of slot.
* Bur: No. 2 or No. 4
* Dimensions: 0.75 to 1 mm at the gingival aspect
1 – 1.25 mm at the occlusal wall
axial depth: 0.5 mm inside DEJ if Occlusal margin is in enamel.
* Retention grooves with a No. ¼ burs are prepared into occlusoaxial & gingivoaxial line angles 0.2 mm inside the DEJ or 0.3 – 0.5 mm inside the cementoenamel cavosurface margin.
The depth of these grooves is one half the diameter of bur head.
Ideally the direction of occlusal groove is slightly more occlusal than axial, and the direction of an gingival groove would be slightly more gingival than axial.

ROTATED TEETH
The outline form for a MO teeth preparation on the rotated mandibular second premolar has its proximal box displaced facially because proximal caries include mesiofacial line angle of crown.
If lesion is small consideration must be given to slot preparation.
UNUSUAL OUTLINE FORM
* Dovetail is not required unless a fissure emanating in occlusal step is involved in preparation.
* The occlusal fissure segmented by coalesced enamel should be treated with individual amalgam restoration if preparations are separated by approximately. 0.5 mm or more sound tooth structure.
ADJOINING RESTORATIONS
Where two restoration adjoin care should be taken that outline of second restoration doesn’t weaken the amalgam margin of first. The intersecting margins of two restorations should be at right angles as much as possible. A weak wall of enamel joining two outlines that are less than 0.5 mm apart should be removed.
CLASS II LESION CONTIGUOUS WITH CLASS V LESION
Class II lesion prepared and restored before preparing Class V lesion. This avoids condensation problems which are encountered if both the lesions are prepared first.
ABUTMENT TEETH FOR REMOVABLE PARTIAL DENTURE
The facial and lingual proximal walls and respective occlusal margins must be extended so that entire rest seat can be prepared in amalgam without encroaching the occlusal margins.

There should be minimum 0.5 mm of amalgam between rest seats and margins
LARGER CLASS II RESTORATION
Often a larger Class II restoration may require greater extension of occlusal surface outline form. This may include
Extending grooves that are fissured Capping cusps that are undermined. Extending the outline form up the occlusal inclines.
These extensions occur at same initial pulpal depths and follow DEJ. Alteration in orientation of bur is also required, by tilting lingually while extending facially and vice-versa.
CUSP REPLACEMENT
Rule for cups capping: * If extension from a primary groove toward the cusp is no more than half the distance, then no cusp capping; * If this extension is from one half to two thirds of the distance, then consider cusp capping: * If the extension is more than two thirds of the distance, then usually cap the cusp
If indicated, cusp replacement increases the resistance form of tooth.
PROXIMAL EXTENSIONS:
Large proximal box preparations also need secondary retention features. When proximal extension around a line angle is necessary, it is usually
associated with a reduction in involved cusp.
Class III Amalgam Restorations
INDICATIONS
Distal surface of maxillary and mandibular canine if
(1) Preparation is extensive with only minimal facial involvement
(2) Gingival margin involves primarily cementum
(3) Moisture control is difficult.

CONTRAINDICATIONS
Esthetically prominent areas.
TECHNIQUE
A lingual approach is preferred over facial unless lesion is more facial than lingual.
Using a No. ½, 1, or 2 round bur prepare the outline form extending the external, walls to sound tooth structure while extending pulpally to an initial depth of 0.75 mm.
Groove retention may be necessary groove is prepared 0.25 mm from root surface to a depth of 0.25 mm. Groove is directed as the bisector of the angle formed by function of axial wall and external wall. Usually the outline form includes only proximal surfaces. However a lingual dovetail may be indicated if one existed previously or if additional retention is needed for a larger restoration.
SECONDARY RETENTION FORM
1) gingival groove
2) Incisal cove
(3) lingual dovetail
MODIFICATIONS FOR CLASS III
a) The decay extent may dictate a labial approach, in that case wall anatomy of labial and lingual wall will be reversed.
b) If incisal wall is not bulky enough to accommodate a retentive groove without underlying the distal slope, it may be replaced by a labial and to a lesser extent lingual groove.
c) If horizontal gingival groove cannot be located without perforation to a surface concavity, it can be replaced by deepening the point angle retention groove.
d) If labial or lingual walls is lost it is essential to create a very short wall to try to lock the restoration.
This can be accomplished by deepening the axial wall at its labial or lingual periphery and by establishing a very pronounced axiolabial or axio-lingual line angle

e) In senile decay, where incisal margin of lesion is apical to the contact area the incisal wall will be one planed, inclining gingivodistally making an acute angle with axial walls.

CLASS IV MALGAM RESTORATIONS
INDICATIONS
* Incisal angle is undermined or involved by lesion * Labial and lingual walls are intact and bulky * There is pronounced intact gingival floor * A restoration that replaces the distal slope or Part of it will be subjected to that slope’s mechanical problems
The general shape of cavity preparation is an inverted truncated cone.
Gingival and labial margins are exactly as described for Class III. The lingual margin is located in lingual embrasure just clearing the contact. The incisal margin is located at slope of incisal edge.
MODIFICATIONS OF CLASS IV RESTORATIONS
If labial or lingual walls are not bulky enough to accommodate the retention grooves, it is advisable to make them in two planes
Make them in two planes
* inner, dentinal plane at right angle to axial wall
* outer, enamelo-dentinal plane following the directions of enamel rods.
Sometimes the entire cavity preparation may be inclined inciso-lingually especially in upper canine, resulting in preparation opening partially at its incisal end. In such cases lingual wall must be more slanted in inciso-gingival direction than labial wall.
If retention forms are deficient, and some walls are either partially or totally lost, pins should be used.

CLASS V RESTORATION
The outline form of the Class V amalgam tooth preparation is primarily determined by location and size of caries or old restorative material.
Proper outline form for Class V amalgam tooth preparation results in extending the cavosurface margins to sound tooth structure while maintaining a limited axial depth of 0.5 mm inside the DEJ and 0.75 mm inside the cementum when on root surface.
INITIAL TOOTH PREPARATION
The lesion is entered by a tapering fissure bur. All the walls of the tooth preparation are perpendicular to the external tooth surface, they usually diverge facially. Consequently there is no inherent retention.
Two retention grooves, one along incisoaxial line angle and other gingivoaxial line angle are prepared using No. ¼ bur.
Alternatively, four retention cover may be prepared, one in each of the four axial point angles. – This conserves dentin and reduces the possibility of mechanical pulp exposure.
LARGE PREPARATION THAT INCLUDE LINE ANGLES.
Large lesions on the facial surface may extend beyond the line angles of the tooth. Maxillary molar, particularly second molars are most commonly affected by these extensive defects. If the remainder of the distal surface is sound and distal caries is accessible facially, the facial restoration should extend around the line angle.
MODIFICATIONS OF CLASS V
If most of the facial or lingual surface is involved in a Class V lesion and they are to be part of cavity preparation, the occlusal wall will diverge in occlusal direction. This will decrease the retentive capability of the preparation. It is advisable to make this divergence only at the areas where margin approximates the occlusal surface. In this situation gingival retention grooves should at least be doubled on size, and mesioaxial and disto-axial considerably.
MULTIPLE ISOLATED BOXES
INDICATIONS, There are multiple lesions or defects in gingival third, which are limited in size, with sound tooth structure separating them from each other The general shape of this design is of several preparations which are small, box shaped and with rounded corners.

COMPLEX AMALGAM RESTORATIONS
Complex posterior amalgam restorations should be considered when
(1) large amount of tooth structure is missing
(2) when one or more cusps need capping
(3) increased resistance and retention form are needed.
These are contraindicated if patient has severe occlusal problems or if tooth cannot be properly restored with a direct restoration.
ADVANTAGES
1) Conserves tooth structure
2) Can be completed in one appointment
3) Resistance and retention form is significantly increased
4) It is relatively inexpensive
DISADVANTAGES
1) Preparing pinholes and placing pins may create craze lines or fractures
2) Microleakage around all types of pins has been demonstrated.
3) The tensile strength and horizontal strength of pin retained amalgam restoration is significantly reduced.
PIN RETAINED AMALGAM RESTORATIONS.
Any restoration requiring the placement of one or more pins in dentin to provide adequate resistance and retention form.
Initial tooth preparation

The general concept of tooth preparation for amalgam is followed. The cusps reduction is accomplished during initial tooth preparation only because it improves access and visibility for subsequent steps.
The occlusal contour of the reduced cusp should be similar to normal contour of the unreduced cusps. Final restoration should have restored cusps with minimal thickness of 2 mm for functional cusps and 1.5 mm for non-functional cusps.
Other principles of retention form like converging opposite walls, flat pulpal floors, facial or lingual grooves should also be undertaken.
FINAL TOOTH PREPARATION
Coves (horizontal plane) and locks (vertical plane) are preparation before preparing pinholes and inserting pins
TYPES OF PIN1) Cemented2) Friction locked3) Self threading → Most frequently used
CEMENTED PINS Cemented into pinholes 0.001 – 0.02 inch larger than diameter of pins The cementing media is any standard dental luting agent
FRICTION LOCKED PINS: Diameter of prepared pinhole is 0.001 inch smaller than diameter of pin Pins are tapped into place, retained by resiliency of dentin. These are 2-3 times more retentive than cemented pins
SELF THREADING PINS:
o Diameter of prepared pinhole is 0.0015 inch 0.004 inch smaller than diameter of pin.
o The resiliency of dentin permits insertion of threaded pin into a hole of smaller diameter.
o They do not engage dentin for their entire width. o These are 3-6 more retentive than cemented pins.
Vertical and horizontal stresses generated are maximum in self treading pins.
FACTORS AFFECTING IN RETENTION OF PINS IN DENTIN AND AMALGAM

1) Type: Self threading > Friction locked > cements (from maximum to minimum retentiveness in dentin.)
2) Surface characteristics: Number and depth of serration or threads on pin influence retention of pin in amalgam restoration.
3) Orientation, Number And Diameter Placing pins in a non parallel manner increases their retention. Bending the pins is not desirable, it weakens the pin and risk fracturing the dentin.
In general, increasing the number of pins increases the retention in dentin and amalgam but benefits must be compared with potential problems created like.
* Crazing of dentin * Amount of available dentin between pins, decreases Strength of amalgam restoration decreases
4) Diameter: As diameter increases, retention in dentin and amalgam increases
5) Extension into dentin and amalgam
Retention is not increased significantly when depth of pin into dentin exceeds 2 mm.
PIN PLACEMENT FACTORS AND TECHNIQUE
PIN SIZE : four pin sizes are available with a corresponding colour coding drill.
Determining factors for selecting a appropriate size pin.1) Amount of dentin available2) Amount of retention desired.
Color code Pin dia (INCHES) drill dia (INCHES)1) Regular Gold 0.031 0.0272) Minim Silver 0.024 0.0213) Minikin Red 0.019 0.0174) Minuta Pink 0.015 0.0135
Minikin pins are usually selected to reduce the risk of dentin crazing, pulpal penetration and potential perforation.
Minim are used as backup of pin holes for minikin was over prepared.

Minuta is half to one third retentive as minim. It is too small to provide adequate retention in posterior teeth.
NUMBER OF PINS: one pin for missing line angle is used.
Several factors must be considered (1) amount of missing tooth structure (2) amount of dentin available (3) amount of retention required (4) size of pin.
LOCATION
Several factors aid in determining pinhole locations (1) pulp anatomy and contours of teeth(2) recent radiograph(3) periodontal probe(4) patient age
Consideration must be given to placement of pin in area where greatest bulk of amalgam will occur
A pin placed directly below the occlusal contact weakens amalgam significantly
Occlusal clearance should be sufficient to provide 2 mm amalgam over pin
Caputo & standlee state that ideally, pinholes should be located half way between pulp and DEJ or external surface of tooth root.
Standlee and others have shown that there should at least 1 mm of sound dentin around the circumference of pin hole.
Felton and associates have demonstrated that pin placement providing at least 1 mm of remaining dental thickness from pulp elicits minimal pulp inflammatory response.
But the most practical philosophy is.
In the cervical third of molars and premolars (where most pins are located), pinholes should be located near the line angle of tooth. The pinhole should be positioned no closer than 0.5 to 1 mm to DEJ or no closer than 1-1.5 mm to the external surface of tooth.
As a rule, the pinhole should be parallel to adjacent external surface of tooth.

Pinholes should be prepared on a flat surface that is perpendicular to the proposed direction of the pinhole.
Whenever three or more pinholes are placed, they should be located at different vertical levels on the tooth if possible.
The minimize inter pin distance 3 mm for the manikin 5 mm for minimum
Maximal inter pin distance results in lower level of stress in dentin.
Pinholes on the distal surface of mandibular molars and lingual surface of maxillary molars should be avoided. (Three is abrupt flaring of roots just apical to CEJ).
PIN DESIGN
For each of the four sizes of pins, several designs are available.
Standard
Self shearing
Two in one
Link series
Link plus
The link series and link plus are recommended
TMJ pins are available in Stainless steel plated with gold. Titanium
PIN INSERTION
Two instruments for insertion of threaded pins are available
o Conventional latch type contra angle handpiece
o TMS hand wrenches.
POSSIBLE PROBLEMS WITH PINS

1) FAILURE OF PIN RETAINED RESTORATIONS
i) Restoration fractureii) Pin restoration separationiii) Pin fracturesiv) Pin dentin separation → Most likelyv) dentin fracture
2) BROKEN DRILLS AND BROKEN PINS
o A twist will break if it is stressed laterally or allowed to stop before being removed from the pinhole.
o Sharp twist drills helps eliminate the possibility
o Standard pins may break it turned more than needed to reach the bottom of pinhole
o Pins may break during bonding even
Removal of broken drill and pin is difficult if not impossible and usually should not be attempted.
3) LOOSE PINS
Self threading pins sometimes do not properly engage the dentin because(i) pin hole was inadvertently prepared too large(ii) self shearing pin failed to shear (iii) while shortening, bur is not held perpendicular to pin hole.
4. PENETRATION INTO THE PULP AND PERFORATION OF EXTERNAL TOOTH SURFACE.
Both are obvious if there is hemorrhage in the pin hole following removal of drill.
Usually penetration and perforation can be felt by an abrupt loss of resistance of drill to hand pressure.
PULPAL PENETRATION
In an asymptomatic tooth, a pulpal penetration is treated as any other small mechanical exposure

Ideal treatment of pulpal treatment is endodontic therapy
EXTERNAL PERFORATION * Occlusal to gingival attachment.* Apical to gingival attachment
Treatment options
Occlusal To Gingival Attachment.
Pin can be cut flush off the tooth and no further treatment rendered. Pin can be cut flush off the tooth and preparation for a cast restoration
extending gingivally beyond the perforation. Pin removed external aspect of pin hole enlarged slightly and restored
with amalgam.
Apical To Attachment
(1) reflect the tissue surgically, remove the necessary bone, enlarge the pin hole slightly, restore with amalgam.
(2) perform a crown lengthening procedures, and place the margin of a cast restoration gingival to perforation
SLOT RETAINED AMALGAM RESTORATION
A slot is a retention groove in dentin whose length is in horizontal plane. Slot retention may be used in conjunction with pin retention or as an alternative.
Indications Short clinical crowns
Cusps that have been reduced 2 – 3 mm for amalgam.
DisadvantageCompared with pin placement more tooth structure is removed in preparing slots.
Advantages
Less likely to produce (i) micro fractures (2) external perforation.

Tooth preparation:
Slot may be continuous or segmented
33 ½ No bur is used.
Dimensions
0.5 mm axial to DEJ
0.5 mm in depth
1 mm or more in length
AMALGAM FOUNDATIONS
Definition
A form is an initial restoration of a severely involved tooth. The tooth is restored so that the restorative material will serve in lieu of tooth structure to produce resistance and retention forms during the development of subsequent cast restorations.
Unlike conventional amalgam restoration an amalgam foundation may not depend primarily on remaining coronal tooth structure for support. Instead it may rely mainly on secondary preparation retention features and some what on bonding benefits.
When preparing a tooth for foundation and / or caries control restoration, remaining unsupported enamel may be left, except at the gingival, to aid in forming a matrix for amalgam condensation.
As a rule foundations are placed in preparation for a full crown, especially in endodontic treated teeth.
TOOTH PREPARATION FOR AMALGAM FOUNDATIONS
The technique of tooth preparation for or foundation depends on type of retention that is selected. All techniques have in common the axial location or retention i.e. sufficiently deep axially so that final preparation for subsequent indirect restoration does not compromise the resistance and retention form of foundation.
SUMMARY

Class I & II amalgam restorations are still common procedures, when used correctly and in properly selected cases, amalgam restorations have demonstrated the potential to serve for many years.

ASEMINAR
0N
AMALGAM RESTORATIONS
Presented by : Dr. Shivani Arora

CONTENTS
Introduction Indications Contraindications Advantages Disadvantages Amalgam restorations Initial clinical procedure Tooth preparation for amalgam restorations Conservative class I restoration Enameloplasty Class I occlusolingual preparation Class II amalgam restorations
* for one proximal surface Modifications of class II Variation of one proximal surface tooth preparation Class II restoration involving both proximal surfaces Class III amalgam tooth preparation Modifications for class III restorations Class IV tooth preparation Modifications for class IV preparations Class V preparations Modifications for class V Complex amalgam restorations Pin retained restorations Slot retained amalgam restorations Amalgam foundations