am theDirector of Campaign for New York Health I My name ... · catastrophe or chronic illness. For...
47
Good afternoon, Senators and Assembly Members of the state of New York. First, thank you for holding this hearing. Given the state of healthcare in this state and country, we believe it is long overdue to have this public conversation. We extend our deep appreciation to the Health Committee Chairs for their lead&ship on this issue. My name is Katie Robbins, and I am the Director of the Campaign for New York Health (CNYH), an organization founded to advocate for the right to healthcare in New York State. We firmly believe that a universal, publicly-financed system, or single-payer Medicare-for-All, is the best way to achieve that goal. Today we are releasing a report titled, “From Coverage to Care, A People’s Report on Healthcare in NYS.” Over the last two years, volunteers and partner organizations surveyed over 2,400 New Yorkers from across the state, aiming for a sample representative of the state’s population in regards to gender, age, race, and geographic distribution. Our findings were clear. 50% of respondents reported delaying or skipping basic care entirely because of cost. Even though most people had insurance coverage, they simply couldn’t afford it. One third went on to develop more serious complications from not receiving timely care. When health issues aren’t dealt with promptly it can lead to worse outcomes, and more costly care. Our survey with people across the state went further to capture the stress, fear, and reduction in quality of life so many people experience when navigating the healthcare system. That is why we included testimonials from many different New Yorkers who have lived to tell the tale, speaking about their personal experiences with the system: “Not being able to afford regular dental care cost me my teeth.” -- Becca from Elmira 1
Transcript of am theDirector of Campaign for New York Health I My name ... · catastrophe or chronic illness. For...

Good afternoon, Senators and Assembly Members of the state of New York.
First, thank you for holding this hearing. Given the state of healthcare in this state and
country, we believe it is long overdue to have this public conversation. We extend our
deep appreciation to the Health Committee Chairs for their lead&ship on this issue.
My name is Katie Robbins, and I am the Director of the Campaign for New York Health
(CNYH), an organization founded to advocate for the right to healthcare in New York
State. We firmly believe that a universal, publicly-financed system, or single-payer
Medicare-for-All, is the best way to achieve that goal.
Today we are releasing a report titled, “From Coverage to Care, A People’s Report on
Healthcare in NYS.” Over the last two years, volunteers and partner organizations
surveyed over 2,400 New Yorkers from across the state, aiming for a sample
representative of the state’s population in regards to gender, age, race, and
geographic distribution.
Our findings were clear. 50% of respondents reported delaying or skipping basic
care entirely because of cost. Even though most people had insurance coverage,
they simply couldn’t afford it. One third went on to develop more serious complications
from not receiving timely care. When health issues aren’t dealt with promptly it can
lead to worse outcomes, and more costly care.
Our survey with people across the state went further to capture the stress, fear, and
reduction in quality of life so many people experience when navigating the healthcare
system. That is why we included testimonials from many different New Yorkers who
have lived to tell the tale, speaking about their personal experiences with the system:
“Not being able to afford regular dental care cost me my teeth.” -- Becca from Elmira
1

“1 didn’t have insurance for short periods during my three pregnancies, and the medicaldebt still follows me today” — Sara from Buffalo
“1 stayed at a job that was emotionally and physically exhausting to keep my healthinsurance.” — Frances from Brooklyn
“As a registered nurse who performs bedside care in the hospita4 I have seen patients
delay or refuse healthcare because of cosL “ - David from Orange Co.
Today, you will hear testimony from powerful and wealthy people and institutions,
including the hospital, pharmaceutical, and insurance industries who vehemently
oppose the New York Health Act. Unfortunately, these interests are often incompatible
with healthcare.
In our study, the vast majority of respondents do not view the current healthcare
system favorably. 64% of people felt they do not have a say in decisions about our
healthcare system. Overwhelmingly, people believe that believe that healthcare is a
human right, and most people support a universal, publicly financed, single-payer
system. Frankly, if we didn’t have a crisis in our democratic process, we would very
likely have such a universal system of guaranteed care in place.
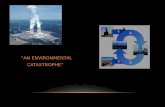
Finally, I am including in my testimony a chart of dates recording when countries
around the world implemented their universal healthcare systems. (Yes, we
understand that not every country with universal healthcare has the single-payer
system we advocate for, which is most similar to Canada, Taiwan, or South Korea. But
what all the systems have in common is strong government regulation of the
healthcare industry -- otherwise you’re left with a system like ours that prioritizes profits
over the collective health of the citizenry). Most of these healthcare systems were
established throughout the middle of the last century. The second chart shows the date
universal healthcare systems around the world ended, failed, or were dismantled. If we
believe the talking points of our opponents about the dangers of a single-payer system
this should surely be an interesting timeline. But in fact you’ll see the second chart is
2

completely blank. No country has ever dismantled their universal healthcare system
once it has been established. In fact, these programs prove wildly popular with their
citizenry, making it very difficult to dismantle once they are in place.
We ask that lawmakers recognize the extraordinary price we are paying to maintain the
status quo, not just in dollars and cents, but the human costs paid in worsening health,
quality of life, and too many tragically unnecessary deaths. The legacy of bringing truly
universal healthcare to a state like New York is on the table. It’s time to pass the New
York Health Act.
Thank you.
County Start Daft County Start Dote
• AustralIa 2.975 ItaJyAustria 1967 JapanBahnTn 1957 KuwaItBelgium 1945 Luxembourg •
Snrnd 1958 Neth.dandsCanada 1966 NnZeaIand -
* Cyp 1980 Norway‘, Denmark 1973 Portugal
FInland 1972 SIngapore 1993Franc, 1974 Slovenla 1972
_________
Germany 1941 South Korea 1988 A
Greece 1983 SpaIn 1986
fl Hang Kong 1993 Sweden 1955[, Eceland 1990 SwIfterfand 1994
Ireland 1977 UnIted Arab EmIrates 19Th1995 UnIted KIngdom 1948
_______
UNIVERSAL HEALTHCARESTART DATES
UNIVERSAL HEALTHCAREEND DATES
2.9781938195019731966193819121979
K’
3



Ii
Carw
egE
tharad
Lev
Tee
Ereecee
fl’yrwiai
Ca,
Esseaseg
Few
+5
8%
Cosi
+2.8%
5a&’rq
+5.5%T
otalA
dditionalC
osts:+
14.1%
Sav
ing
Billions
throughad
rranev
mw
esinphication
andre
dtta
dp
ecesuS
thugs
and
med
cajdoere
s
Heatth
careF
undin
gU
nderT
he
New
York
Health
Act
Total.
543.9B
—N
et=
—511.1
a
Net
Savings:—
3.6%
ryoneW
hileS
avingM
oney
itionalC
osts,N
etSavings
v.Funding
Under
NY
Health
Ad,
RA
ND
Coporation,
Augu
18
;L
eonardR
odberg,Ion’s A
ssessment
oftheN
VH
ealthA
ct,S
eptember
2018.
NE
WY
OR
KH
EA
LT
HA
CT
(A5248,
S3577)
AS
ingleS
tateF
undP
rovid
ing
Com
preh
ensiv
eB
enefits
Covers
ALLm
edicallynecessary
care,Iree
choiceof
provide’,no
more
networks:
Jprim
ary&
specialtycare
,Jlong-term
care&
supponservices
Jhospitalization
Jm
entalhealth
Jprescriptions
4substance
abusetreatm
ent
Jvision,
dental,hearing
4reproductive
care
Sav
ings:
Fam
ilies,N
YS,
Mun
icipalities
&C
ounties
ForIndividuals
andFam
ilies:90%
‘viiipay
lessorm
uchless
—prem
iums,
deductibles,out-of-pocket
costsreplaced
bya
progressivetax
thatonlyincreases
with
income,
notw
ithm
edicalcatastrophe
orchronic
illness.
ForN
YS:
eliminates
administrative
waste
frominsurers
andproviders;
dramatically
reducesdrug
andm
edicaldevice
coststhrough
volume
discounts;reduces
fraudand
controlscosts
without
reducingthe
qualityof
care;reduces
accessinequities
acrossN
t’S.
Municipalities
&C
ountiesw
illsave
15-30%of
budgetlow
eringproperty
taxes:C
ountyM
edicaidcontH
butions:elim
inatedH
ealthcarecosts
forcugent
employees’:
reducedsubstantially
Heatthcare
costsfor
instateretirees*:
eliminated
(‘includingpolice,
firefighters,teachers,
librarians,m
unicipalstaff,
electedreps,
etc.)
Health
carefo
rA
llof
Us
4D
ocorsand
nurses,not
insurar.cecom
panies,willderide
yourcare
—w
ithyou.
4C
orporateprofit
willno
longertake
precedenceover
yourhealth
needsor
publichealth.
4Preventive
carewillbe
covered—
New
Yorkers
canget
carebefore
it’slife-threatening,
4L
ong-Term
Care
willensureperm
anentlyand
temporarily
disabledN
Yers—
andfam
ilyw
honow
carefor
them—
getthe
servicesthey
needto
leadm
oreprodudrve
lives.4
Seniorsw
antingto
ageat
home
willhaveservices
theyneed
forliving
indignity.
Imp
rov
edN
YS
Eco
nom
y
ForB
usinesses:reduces
cost,provides
apredictabe
expense,elim
inatesneed
forbenefits
administration,and
remo’ies
hassle:increases
abilityto
compete
forlabor
andcustom
ers,nationally
andinternationally.
ForN
t’SE
conomy:
improves
productivityw
ithhealthier
worH
orre;ends
“job-lock”;reduces
riskfor
entrepreneursand
start-ups;savings
willcreate2W
,IXIO
newohs.
34%41°!
4%sasings
FederalN
YH
eatrhA
’
010%S
tateG
ovvnmseni
11%O
therF
unds

Let
’sN
ot
Cov
erU
pth
eR
eal
Sto
ryT
hefo
llow
ing
page
sof
fer
stor
ies
told
bypa
tient
s,by
fam
ilym
embe
rsby
phys
icia
ns.
The
yus
ually
begi
nby
desc
ribi
ngco
mfo
rtab
leliv
esem
ploy
edin
sure
d,he
alth
y.
Our
curr
ent
hea
lth
care
pay
men
tsy
stem
isbro
ken
.M
any
who
inte
ract
wit
hit
get
brok
enby
it.M
ed:c
alca
lam
ityha
ppen
sIn
am
om
ent.
Fina
ncia
lan
dem
otio
nal
cala
mity
follo
w.
Avi
ciou
scy
cle
begi
nsw
hew
illne
ssbe
gets
debt
,ex
acer
batin
gill
-hea
lth,j
ob-l
oss,
insu
ranc
eto
ss,
ado
wnw
ard
spira
lof
unst
oppa
ble
angu
ish.
Em
plo
yer
-bas
edin
sura
nce
isn’
tw
ork
ing
—an
dit’
sg
etti
ng
wors
e:
Sky-
rock
etin
gco
sts
have
caus
edem
ploy
ers
tore
duce
the
num
ber
ofco
vere
dw
orke
rs,
dow
n11
%si
nce
2000
,with
less
than
ath
irdof
rece
ntco
llege
grad
uate
sno
wof
fere
dhe
alth
bene
fits
,Th
eco
stof
heal
thbe
nefi
tsex
acer
bate
sag
edi
scrim
inat
ion
amon
gol
der
wor
kers
,an
dis
dAw
ngth
eno
-ben
efits
“gig
econ
omy,
-no
wes
timat
edat
57m
illio
nA
mer
ican
wor
kers
.
Empl
oyer
sha
vein
crea
sing
lysh
ifted
heal
thca
ieco
sts
toem
ploy
ees,
with
high
erem
pfoy
eepr
emiu
mco
ntrib
utio
nsan
din
crea
sed
dedu
clib
les
and
co-p
ays.
Sinc
e2
,em
ploy
erco
nhib
ulio
nsha
vene
arly
tnpl
ed,w
hile
empl
oyee
cont
ribut
ions
have
incr
ease
dal
mos
t5-
fold
—ou
t-of
-poc
ket
dedu
ctib
les
have
incn
ease
dal
mos
tas
mus
h.
Hea
lthca
reco
sts
for
fam
ilyco
vera
geth
roug
hem
ploy
men
tha
veris
enfro
m13
%of
the
med
ian
wag
ein
2001
toal
mos
t50
%to
day.
The
aver
age
fam
ilysp
ends
mol
eon
prem
ium
cont
ribu
tions
than
onfo
odfo
ra
yeaç
mor
eon
heaf
thca
repr
emiu
ms
plus
out-
of-p
ocke
tth
anon
hous
ing.
Phy
sici
ans
also
suff
er:
Sinc
e20
10,
over
half
ofkm
enca
ndo
ctor
sm
port
sym
ptom
sof
bum
-out
—wi
sh10
%of
criti
cal c
are
and
fam
ilyph
ysic
ians
repo
rtin
gsu
icid
alid
eatio
n.A
cros
sth
ede
velo
ped
wor
ld,
only
Ger
man
MD
s(w
hoal
sost
rogg
lew
ithhu
ndre
dsof
insu
ranc
epo
lides
ihav
efe
wca
reer
satis
fact
ion
than
Psne
rican
MD
s,ca
nadi
anM
Ds,
unde
rsi
ngle
-pay
er,
repo
rtsa
tisfa
ctio
n;th
eyfo
cus
onpa
tient
s,w
ithou
tins
urem
inte
rfer
ing,
with
out c
osts
thre
aten
ing
lives
that
doct
ors
have
save
d.
Our
syst
emis
chan
ging
how
doct
ors
prac
tice
med
icin
e:fe
wca
naf
ford
priv
ate
prac
tice
whe
nfo
r-pr
ofit
insu
rers
offe
rre
imbu
rsem
entl
ess
than
Med
icar
e,w
hen
billi
ng/r
eim
burs
emen
tre
quir
essi
gnifi
cant
offic
est
affa
ndph
ysic
ian
time,
whe
ndo
ctor
sca
rry
anav
erag
eof
200t
Qye
arin
unpa
idde
btfm
min
sure
rs.
Nar
row
ing
netw
orks
also
redu
ceco
ntin
uity
ofca
re,
mak
ing
care
few
pers
onaf
,fe
win
form
ed. T
hese
amre
ason
sw
hym
ostd
octo
rssu
ppor
tasi
ngle
-pay
erpa
ymen
tsy
stem
,lik
eth
eNY
Hea
lthA
ct.
For
-pro
fit
insu
rers
intr
ud
ein
too
ur
do
cto
r-p
atie
nt
rela
tionsh
ips,
and
har
mour
hea
lth
:
Mos
tkne
rica
nsha
vea
fam
ilym
em
ber
who
has
avoi
ded
doct
ors
and
skim
ped
onm
edic
atio
ns;
dela
yed
cam
oft
en
requ
ires
mor
eco
mpl
extr
eatm
ent
and
criti
cal
care
.Am
eric
anhe
alth
met
rirs
,am
ong
the
wom
tin
the
deve
lope
dw
orld
, am
wor
seni
ng.
One
U.S
.dem
ogra
phic
has
outc
omes
appr
oach
ing
the
glob
atry
heat
thie
slan
dlo
nges
t-liv
ing:
seni
ors
who
have
been
onM
edic
are
for
atfe
asl
ade
cade
,
Uni
vers
al,c
ompr
ehen
sive
heal
thca
rew
ithno
fear
offin
anci
alru
inhe
lps
outs
enio
rsge
tan
dst
ayhe
alth
yM
edic
are
offe
rsac
cess
tow
orld
-cla
ssm
edic
alca
re—
afte
ra
Iitti
me
offe
w,
W,th
rega
rdto
Med
icar
e,se
nior
sre
joic
e(w
ithM
auri
ceC
heva
lier
):“I
’mso
gla
dI’
mnot
yo
un
gan
ym
ore
,”
Cov
erin
gE
very
one
Whi
leS
avin
gM
oney
Tota
lpr
ojec
ted
stal
usqu
oS
pend
ing
in20
22:
$311
B
fle
ed
eedxea
Sdk
h1
n,r
aM
OS
Pw
xhas
’rg
Ad,
,,,it
upla
lra
re,g
,ceas
Aà,
i.i
S—
6,5%
CI
—6%
—5,
2%
Totaf
Savi
ngs:
—17
.7%
Tof a
t—
555,
1B
NY
Hea
lth
Will
Cov
erE
v
Sour
ces
ofSa
ving
s,A
d
Cur
rent
Sour
ces
ofFu
ndin
Sour
ces:JI
Uu,
etaL
,An
Ass
ess
me
ofth
eNY
Hea
kSu
mm
a,y
and
Eva
luat
ion
oft
he
RA
ND
cara
t-
The
NYH
ealth
Tax
repl
aces
priv
ate
insu
ranc
e,ou
t-of
-poc
ket
cost
s,&
coun
tyM
edic
aid
cotf
s
Cur
rent
Sour
ces
ofH
eatt
hca
reF
undIn
g
Pri
vate
Insu
ranc
e
31%
34%
Fed
er&
Gov
ernm
ent
1%
11%
Oia
tt/
10%
Sla
teG
over
nmen
tPo
cket
3%11
%C
ount
yO
ther
Fun
dsG
over
nmen
t

Our
Heathcare
Heroes
Health
careS
tories
From
NY
C
Gary
Axelbank,
‘Mr.
Bronx”
publisherof
ThisIs
theB
ronxand
producerof
Bronx
Talk:For
yourgenerosity
inm
akingspace
fora
yearof
weekly
storiesdelineating
Healthcare
inA
merica,”
andyour
unfailingcom
mitm
entto
spotlightinghealthcare
disparitiesin
ourborough
andstate.
Richard
Gotifried,
Foryour
championing
theN
YH
ealthA
ctsince
1992,steadfastly
advancingand
improving
thisgroundbreaking
legislation,inspiring
usto
staythe
moral
highground,
andthereby
bringingvictory
within
reach.
Gustavo
Rivera,
NY
Senator
fromthe
Bronx
since2010
andchair
ofthe
Health
Com
mittee:
Foryour
flairand
passionatededication
toerasing
healthinequity
inlaw
andin
fact.
Legislative
Sponsors:
Foryour
courageto
dothe
rightthing
forconstituents.
Katie
Robbins,
NY
HC
ampaign
leaderextraordinaire:
Foryour
graceand
steel,strategic
visionand
boundlessjoy.
NY
SN
ursesA
ssociation,For
your24/7/36S
caringw
henw
ereat
ou
rlow
est,for
initiallyadvocating
single-payerto
AM
Gotifried,
andfor
25years
ofunw
eariedefforts
tobring
qu&ity
healshcareto
everyN
ewY
orker.
PNH
PN
YM
etroT
eam:
eachof
youjoins
reasonw
ithhum
anity,and
we
particularlynose,
Dr.
LenR
odberg:For
yourgenerosity
soall
corners,exceeded
onlyby
yourtalent
forelucidating
financialand
conceptualcom
plexitiespellucidly.
Henry
Moss:
Foryour
championship
oflong-term
careand
yourpatience
when
dispellingconfusion
ondetails
esoteric,technical,
andsom
etimes
justplain
arbitrary.
NY
SL
ettersT
eam:
them
osteloquent,
responsive,generous
peoplew
eknow
,W
alterC
arpenterFor
yourunflagging
advocacyof
single-payerin
New
York—
andacross
theUS.
SarahO
utterson.Murphy:
Foryour
compassion,
organization,and
devotionto
improving
livesU
rsulaR
ozum:
Foryour
humor,
patience,and
disciplinein
mobilizing
tom
akea
dfference.Farris
Thom
as:Foryour
business-sav’,personal
insighis,and
deepm
oralpassion.
Madeline
Zevon:
ForyourinexhausU
bleadvocacy
andleadership
aoossyour
countyand
ourstate.
Dr.C
atherineC
.Wolf,
1947-2018,beloved
mem
berof
ourL
ettersT
eam,
who
wrote
byusing
hereyebrow
tocontrol
aco
mp
uter
foryour
courageous,contagious
optimism
andyour
righteousadvocacy
forN
YH
ealth,“the
most
important
battleof
my
life.”
1.F
inancier.W
ellInsured.
Motorcycle
Hit
Him
.B
ank
rup
t
Under
NY
HA
:o
Medical
bankruptciesand
debt:elim
inated—
likep
eersaround
thew
orld.
•E
veryN
ewY
orkerw
illbe
fullycovered
automatically
—w
omb
totom
b.
2.E
mployed
&Insured.
Pregnancy
Com
plications.N
oJob.
Three
Livesat
Risk
Under
NY
HA
:
*Y
ourchildren
will
always
havehealthcare.
Sow
illyou.
*A
utomatic
pre-nataland
post-partumcare
will
helpreverse
risingm
aternalm
ortality.
3.ER
Doctor:
For-ProfitInsurance
IsN
otG
oodE
noughor
SafeE
noughU
nderN
YH
A:
•ER
patientsfacing
deathcan
focuson
medical
needs,not
theirw
allets.
oD
octorscan
savelives,
without
savagingpatient
finances.
4.P
re-Existing
Conditions.
InsidiouslyC
urtailingC
areersU
nderN
YH
A:
•H
ealthcarecosts
won’t
discouragehiring.
*O
lderw
orkersm
aysee
lessage
discrimination
when
job-hunting.
5.C
auseof
death:For-Profit
Insurance.F
ortune100
FiresC
hiefL
itigatorU
nderN
YH
A:
•N
oone
will
diew
aitingfor
Medicare.
No
onew
illdie
becauseof
losinga
job.•
CO
BR
Apaym
entsw
on’tdestroy
finances,
6.T
errifyingN
ightmares:
“My
Wife
Will
Be
Hom
eless!”U
nderN
YH
A:
oH
ospitalizedloved
onescan
focuson
healing,not
fearinghom
elessness.o
Medical
billsw
on’tleave
families
indeb
tor
strugglingw
ithcollection
agencies.
7.Fully
Em
ployed.G
otSick.
Lost
Job.L
ostinsurance.
Haggled
forH
isLife
Under
NY
HA
:o
You’ll
neverhaggle
foryour
life,like
youhaggle
fora
car.•
Unlike
currentjob-based
benefits,you’ll
becovered.
Fully.O
e&gned
byK
eiayC
ast
keiseyaclar*2Ogm
ailcwn
Questions?
NY
RA
Lsierr?Jesitgrnall
cornW
rnA
EsW
.q@grna,rrom
M/2
Ol9

Sen
ator
Bia
ggi:
Con
stan
tFo
rmul
ary
Cha
nges
Wor
ryM
yP
aren
ts
Cos
t-S
hari
ngH
arm
sH
ealt
h
My
fam
’’y
isty
frca
tof
man
yof
my
cons
titu
ents
inD
istr
ict
34
Sinc
e20
12w
hen
my
dad
was
diag
nose
dw
ithPa
rkin
son’
sdi
seas
e.lh
enu
mbe
rof
pills
heta
kes
each
mon
thha
sfl
uctu
ated
depe
ndin
gon
how
wel
lhe
’sdo
ing
My
dad
ison
my
mont
heal
thin
sura
nce
plan
.an
dad
ding
pres
crip
tion
drug
sis
very
expe
nsiv
e.
Som
yda
d,w
hois
over
65,p
ays
prem
ium
sfo
rM
edic
are
Part
Dfo
rpr
escr
iptio
ndr
ugs
Even
with
his
heal
thin
sura
nce
and
my
mom
’s,
my
pare
nts
still
pay
som
eo
ut
of-p
ocke
tco
sts
form
yda
dsm
edid
ne.
Each
mon
th,
pills
are
chan
ged.
One
kind
ofpi
llca
nhe
$500
one
mon
th,
and
I40
0sh
ene
xtm
onth
Am
onth
late
r,m
aybe
it’s$2,.
Hig
h-Q
uali
tyL
ong-
Ter
mC
are
Ext
ends
Qua
lity
Live
s
Iwas
fort
unat
eth
atm
ygr
andp
aren
tsliv
edun
tilth
eir
tate
eigh
ties
and
nine
ties
Wat
chin
gth
emag
ew
asbo
thw
onde
rful
and
diff
icul
tbe
caus
edi
ffer
ence
sin
thei
rec
onom
icst
atus
dete
rmin
edth
eki
ndof
tare
they
wer
eab
leto
acce
ss—
and,
byex
tens
ion,
thei
rqu
ality
oflif
edi
ffer
ed.
My
gran
dfat
her
had
24-h
our
care
inhi
sho
me,
whe
rehe
lived
until
age
97.
get
tin
gg
oo
dC
are
can
exte
nd
the
leng
than
dqu
alit
yof
your
life
Dyco
ntra
st,
both
ofm
ygr
andm
othe
rsw
ent
tonu
rsin
gho
mes
whe
rene
tthe
rw
asfe
dT
hat
may
sotm
dcr
azy.
but
it’s
true
.T
henu
rs’n
gho
mes
did
put
food
infr
ont
otth
em,
but
both
cran
dmot
he,s
had
suff
ered
stro
kes
and
coul
dn’t
use
the,
rba
nds.
Iiw
ason
’yaf
ter
seve
ral
wee
ksth
atw
ele
arne
dth
eyw
ere,
quit
elit
eral
ly.
star
ving
.M
ypa
rent
sno
tice
dm
ygr
andm
othe
rsge
ttin
gth
inan
dm
oved
them
from
whe
reth
eyw
ere
inup
stat
eN
ewY
ork
into
near
byB
ronx
nurs
ing
hom
es.
My
dad
has
paid
dose
atte
ntio
nto
thes
ech
ange
s—
eati
nghi
sin
sura
nce
com
pani
esto
ques
tion
cost
s.H
eha
sbe
ento
’don
em
onth
isis
Sch
edul
eI,
the
next
mon
thit
isS
ched
ule
2.E
ach
mon
thit
tsa
diff
eren
tco
stsh
are.
Sohe
rew
eha
vetw
ove
rysm
art
peop
le,
my
mom
who
wor
ksin
apu
btic
hosp
ital
inm
ydi
stri
ctan
dm
yda
dw
hois
aIa
vrye
r,ha
ving
ave
rydi
ffic
ult
time
navi
gatin
gth
eco
sts
ofhi
spr
escn
ptio
ndr
ugs
Now
,th
isis
prog
ress
ive
dise
ase
and,
astim
ego
eson
,th
eykn
owth
eyw
iltha
veso
unde
rsta
ndad
diti
onal
thin
gslik
eto
ng-t
erm
care
and
chat
they
can
affo
rd.
I kno
ww
eca
ndo
som
uch
bet
ter
The
NY
HA
will
relie
vest
ress
for
som
any
fam
ilies
acro
ssth
est
ate.
As
my
fam
ily’s
expe
rien
cesh
ows,
gett
ing
good
care
can
exte
ndth
ele
ngth
and
qual
ityof
your
life.
Des
pite
the
chal
leng
esw
eha
d,m
yfa
m,ty
was
luck
yto
beab
leto
affo
rdth
eca
rem
ygr
andp
aren
tsne
eded
.Li
ving
atho
me
was
ahu
gepo
sitiv
efo
rm
ygr
andf
athe
r’s
men
tal
heal
than
dw
ett-
bein
gB
utho
mec
are
ofte
nm
eans
afa
mily
mem
ber
mus
tst
opw
orki
ngor
get
trai
ning
.Si
nce
tong
.term
care
ina
New
Yor
knu
rsin
gfa
cilit
yca
nco
st$1
00,0
00pe
rye
aror
mor
e,fo
rm
ost
fam
ilies
anu
rsin
gho
me
isou
tof
reac
hun
tilth
ere
itno
othe
rpa
thbu
t“s
pend
ing
dow
n”al
lsa
ving
s.
We
mus
t...
thin
kab
ou
tth
ew
ayth
epo
lici
esan
dla
ws
we
pass
affe
cthu
man
bei
ng
s
Itis
xat
that
at5N
ewY
orke
rsca
nag
ew
ithdi
gniv
yW
em
ust
mak
esu
rew
ear
eta
king
care
ofon
ean
othe
r,th
atw
eth
ink
abou
tth
ew
ayth
epo
licie
san
dla
ws
vie
pass
affe
cthu
man
bein
gs.
Ale
ssan
dra
Bia
yyt
isS
tair
Srn
a!o
’(t
orn
d:st
rict
33.
8.N
oM
edic
are.
No
Med
icai
d.N
Y’s
Mos
tA
t-R
isk
Pop
ulat
ion:
Und
erse
rved
Und
erN
YH
A:
•A
mbu
lanc
eco
sts
won
’tle
ave
abr
oken
back
ona
clin
icfl
oor.
öP
ost-
surg
ery
care
will
decr
ease
suff
erin
gan
dhe
lphe
al.
9.Sm
all
Bus
ines
sO
wne
r:N
eeds
NY
HA
toA
ttra
ctT
opT
alen
tU
nder
NY
HA
:o
Top
tale
ntw
on’t
bejo
b’lo
cked
—yo
uca
nre
crui
tth
em.
oS
tart
-ups
will
have
heal
thca
re—
even
the
heal
thy
suff
erac
cide
nts.
10.
Dua
l—In
com
e.G
ood
Insu
ranc
e.L
ost
jobs
.L
ost
Eve
ryth
ing
Und
erN
YH
A:
oH
ard-
wor
king
NY
ers
who
get
sick
won
’tfa
cepe
nury
.•
Wom
en’s
heal
thne
eds
will
befu
llyco
vere
d,
11.
Em
ploy
er-B
ased
Insu
ranc
eT
hrea
tens
My
Son
sLi
feU
nder
NY
HA
:o
“Con
tinu
ity
ofC
are”
will
beth
eno
rm,
not
the
drea
m.
oC
hang
ing
jobs
won
’tth
reat
enyo
urch
ild’s
life.
12.
Act
ive.
Hea
lthy.
Sud
den
Chr
onic
Illn
ess.
For
mul
ary
Hel
l.W
illIS
urvi
ve?
Und
erN
YH
A:
•D
rug
pric
esw
illno
long
erex
trac
tex
tort
iona
tepr
ofit
s.o
NY
ers
with
chro
nic
dise
ases
will
get
nee
ded
med
s;th
eyw
illre
mai
npr
oduc
tive
.
13.
Del
ays
Upd
atin
gIn
sura
nce.
Bar
ely
Esc
aped
Ban
krup
tcy
Und
erN
YH
A:
•A
utom
atic
enro
llm
ent
inth
ebe
stpl
an,
alw
ays
affo
rdab
le,
alw
ays
ther
e.0
Pre
-exi
stin
gco
ndit
ions
won
’tdi
mfu
ture
job
pros
pect
s.
14.
The
Hos
pita
lIs
“in
Net
wor
k.”
Sur
pris
elT
heD
octo
rIs
Not
Und
erN
YH
A:
0N
osu
rpri
sebi
lls,
noco
sts
atpo
int
ofse
rvic
e.•
All
NY
hosp
ital
sar
e“i
nne
twor
k,”
and
soar
eth
eir
doct
ors,
)We
won
’tfa
teob
stac
les
toge
ttin
gne
eded
pres
crip
tion
s.
Hom
eLT
CK
ept
My
Gra
ndfa
ther
Aliv
eL
onge
r
zo
oW
e’ll
age
atho
me,
wit
hdi
gnit
y.

I ama
24-year-oldm
edicaistudent
in1.Y
C.M
yoverw
helming
deere
isto
healpeople,
particularlythose
who
arem
ostvulnerable
Our
complex
‘nealshcaresystem
oftenfails
showw
honeed
itm
ost.A
sboth
apatient
anda
fusuiephys:cian
I’veseen
that.even
forthose
wish
healthinsuiance,
accessand
Cots
remain
problemasrc.
We
actuallyhave
separatebuildings
forpallenss
with
private(for
profit)and
publicM
edraid
andM
edicare)health
insurancea,
theN
YC
Teaching
hospitalw
hereI w
ork.Faca!ty
mem
berssee
patientsw
ithp
ivaleinsurance,
titlea
rotatingcast
ofresidents
Idoctoisin
traininglsee
shoaew
ishpublic
assurance.T
hosew
ithouthealth
insurancearen’t
teenat
all—
unlessthey
goto
thesrudens-m
nclinic,
where
medical
studentspractice
onand
treatthem
.
evenfor
those
with
healthinsurance,
accessand
costrem
ainpro
blem
atic
My
hospitalclaim
sthat
patientson
publicand
privateinsurance
receivecom
parablecare
but,as
historyhas
shown
us,T
heparasebut
equal”is
unequal.Pasienss
atshe
publicclinic
wait
longer(or
appointments,
andshetr
doctorschange
continuallyas
residentsgraduate
andnew
doctorsin
trainingtake
over.
Patientsw
hoconsistently
seethe
same
do
no
rhave
adistinct
advantageover
thosew
hodon’t,
thosew
hosee
anew
rotationof
physicianseach
time
theyare
treatedor
hospilalized.C
onstantrelation
preventspatients
fromgening
shecontinuity
ofcate
requitedfor
qualityinterjenijor.s.
Inconsistencyincreates
theodds
thatlong-standing
conditionsare
overlookedor
ynored,often
thedifference
between
lifeand
deathM
edicinerelies
onresident
laboras
ateaching
tool,hut
thissegregated
systemskew
sthe
dstributionof
resourcesby
income,
Data
demonstrates
thissystem
createsde
factoracial
segregation.In
NY
C.
over80%
ofpatients
onM
edicaididentify
atB
lackor
Latino,
while
only30%
ofprivately
insuredpatients
do.In
practice,this
means
I canguess
whether
apatient
will
receivethe
higherlevel
ofcare
asthe
privateclinic
lustby
lookingas
thecolor
ofhislner
skin.
Sadly,such
dispansiesextend
tonearly
everyaspect
ofour
hospitaland
medical
school.O
nthe
08/
GY
Nservice,
patientsw
ithpublic
inturanceare
teenon
adifferent
floorw
iihfew
eram
enitiesthan
shephvately’inaured
patientsN
ewborns
atthe
hospisalare
separatedaccording
toInsurance
status,ensuring
that
thesehealthcare
inequitiesam
presentfrom
ea&baoy’s
firstbreash.
At
them
edicalschool,
it’sw
e]know
nthat
arotation
atthe
pabl:ccity
hosditalm
eansgett:ng
todo
more
andhav.ng
more
autonomy
when
practctngon
patients1en
I triedso
make
apoontrnenta
form
yow
ncare,
Ihada
hardtim
efinding
physiciansasm
yhospital
who
acceptM
edicaid.
these
health
careinequities
arep
resent
fromeach
baby’sfirst
breath
Being
aM
edicaidpatient
meant
rece’.vi nglow
erqual.iy
ofcare
where
Iwork,
solsought
careat
aclinic
thatsarvet
everyone,regardless
olinsurance
stalus.tam
fortunateto
hen
goodhealth
endto
havethe
tootsand
resourcesto
make
informed
dectsionsabout
my
own
healthcare;fly
most
vulnerablepatients
donot.
Thisunequal
systempenalizes
low-incom
epatients
anddelivers
substandardcare
topeople
who
desperatelyneed
qualitym
edicalattention
fromskilled
diagnosticians.W
orse,this
segregationis
entirelylegal.
Because
itis
bated
onhealth
insurancestatus,
notrace,
hospitalsthroughout
shecity
segregatepatients.
While
thissystem
hasdubious
financialbenefits,
ithas
veryreal
healthconsequences.
Our
medical
schoolleaches
usto
valueevery
human
life,In
treatall
patientsas
equals,care
forthem
with
dignity,com
passion,and
shehighest
clinicaltiandardt,
butthis
systemrens
contraryto
everythingw
e’vebeen
taughl,underm
iningit.
Our
med
icalsch
ool
teaches
us
to
valu
eev
eryhum
anlife
but
this
system
runs
contrary
toev
eryth
ing
we’v
eb
eentau
ght,
underm
inin
git
Thism
ulti.t,ered.incom
e-basedsystem
isn’tfair.
It’snot
fairso
patients—
orto
med;cal
students,w
honeen
healshcareto
become
doctorsand
who
needquality
superv:uonto
doright
bythe,r
current(and
future)patients.
.dit’s
notfair
todoctors
who
tryso
giveeach
patienttheir
fullattention
andbest
care—
regardlessof
havingtheir
feesdeterm
inedby
theirpatients’
,ncome.
We
needto
levelthe
playingfield
onhealthcare
—for
patientsand
forproviders.
NYH
ealihw
illm
akea
difference.
SerenaC
a,uileis
am
edicalstudentas
am
ajorN
eivYork
teachinghospital.
We’ll
dismantle
“separate
but
NO
Tequal”
healthcare.
•‘ h
in
I1
?rn
1cn
rm
iliinviIcun
;mP
ir.f’lI
I15.
Authorizations:
Designed
toK
eepP
rovidersFrom
Patients,
Patients
FromC
are
Under
NY
HA
:Y
ourprovider
andyou
chooseyour
care.N
oinsurer
denials.
•A
llfinancial
obstaclesto
care:elim
inated.
16.B
adM
igraine.Scary
Prognosis.
InsuranceT
raps.S
carierD
ebt
Under
NY
HA
:
•N
ohassles:
allinsurance
trapselim
inated.
oIf
youneed
thecare,
it’5covered.
Rationing
basedon
income
will
end.
17.H
ealthcareC
ostsD
estroyD
reams.
Discourage
Entrepreneurs
Under
NY
HA
:
0E
ntrep
reneu
rsW
illflourish,
creating
200
000
newjobs.
oSm
allbusinesses
will
havehealthcare
risksresolved.
18.S
uddenIllness.
Great
Insurance.M
onthsof
Stress
Over
Paperw
orkand
Bills
Under
NY
HA
:o
No
hassleson
bills,ev
er—th
erearen’t
any.
•N
etwork
issues,questions
abouttests,
confusingpaperw
ork—
allgone.
19.M
edS
tudent.E
xperiences“S
eparatebut
Equal”
Healthcare
inN
YC
Under
NY
HA
•E
liminating
tieredservices
will
begindism
antling“separate
butN
OT
equal.
0D
octo
rsan
dhosp
italsw
on’tbe
paidless
fortreating
lower-incom
epatients.
20.S
enatorB
iaggi:C
onstantF
ormulary
Changes
Worry
My
Parents:
Long
Term
Care
Kept
My
Grandfather
atH
ome
andA
liveL
onger
Under
NY
HA
:o
We
won’t
faceobstacles
togetting
theprescriptions
we
need.
•M
ostof
usw
illbe
ableto
ageat
home
—m
uchlonger,
andw
ithdignity.
Online
versionsof
thesestones
—and
more
—are
availableat
tfsisistlsebronx.info/sveekday.magazine’healthcare’in’arnerica
(Author’s
Nam
e)
19

Fin
anci
er.
Wel
lIn
sure
d.M
otor
cycl
eH
itH
im.
Ban
krup
tS
udde
nIl
lnes
s.M
onth
sof
Str
ess
Ove
rP
aper
wor
kan
dBi
llsI
My
life
chan
ged
fore
ver
onM
arch
31st
2009
whi
lecr
ossL
ngth
est
reet
asp
eedi
ngm
otor
cycl
ehi
tm
e.T
heim
pact
sent
me
flyin
g25
feet
,br
eaki
ngev
ety
bone
onm
yri
ght
tide
,fr
omm
ycl
avic
leIn
my
toes
.
amgr
atef
ulto
mod
ern
med
icin
eso
beal
ice.
The
trau
ma
was
cata
stro
phic
.Se
ven
open
frac
ture
sto
my
leg,
nine
brok
ennb
sp
erci
ngm
ylu
ngs,
and
abr
oken
clav
icle
.M
any
surg
enes
.so
me
mar
eth
an14
hour
slo
ng,
rebu
iltth
eng
hted
eof
my
body
.
I was
rep
ute
dam
on
gth
eb
est
inm
yfi
eld,
the
sub
ject
oftw
odocu
men
tari
esan
da
WS
JC
olu
mn
3pro
file
Mon
ths
ofph
ys’c
alth
erap
yan
dpr
ivat
enu
rses
foilo
wed
.Ih
adto
lear
nto
viac
agai
n,to
mov
em
yar
ms
upan
dar
ound
,to
feed
and
bath
em
yte’
lT
heva
scul
artr
aum
ato
my
legs
was
soex
tens
ive
I hav
eha
d11
surg
erie
son
my
left
leg,
the
mos
tre
cent
Sm
onth
,ag
o.M
yw
orld
beca
me
incr
easi
ngly
smal
l—
aw
orld
ofdo
ctor
s,th
erap
ists
,nu
rses
,ai
des
and
mnr
enu
rses
and
flar
eth
erap
ists
.
whe
reIo
nce
foun
dfu
lfill
men
tin
build
ing
com
pani
esan
dse
rvin
gon
the
boar
dsof
num
erou
sor
gani
zatio
ns,
exig
ency
requ
ired
tota
lfo
cus
onca
ring
for
wou
nd,
and
lear
ning
basi
csk
ills
ofse
llca
re.
Shor
tlybe
fore
the
acci
dent
,m
yin
sura
nce
brok
erar
rive
dw
ithfo
rms
soco
mpl
ete.
Itho
ught
we
wer
em
axim
izin
gco
vera
geof
dam
ngo
odin
sura
nce.
I was
actu
ally
sett
ing
unim
agin
able
cove
rage
limits
.A
fter
the
first
seve
n’fi
gure
s,m
yin
sura
nce
ende
d.Bi
llsco
ntin
ued
toar
nve,
for
year
s.A
fter
mor
ebi
llsre
ache
dse
ven
digi
ts,
Pwas
foic
edto
life
for
bank
rupt
cy
Her
eI
was
:ban
kru
pt.
Ife
ltsh
amed
For
thre
ede
cade
sI’d
kno’
.ni
mys
elf
asa
high
lyie
gard
edpr
ofes
sion
al.
Iwas
repe
ted
amon
gth
ebe
stin
my
fiel
d,th
esu
bjec
tof
two
docu
men
tari
esan
da
WSJ
Col
umn
3pr
ofle
.B
uthe
reIw
as,
bank
rupt
.‘f
elt
sham
ed.
Sloe
ly.
Ilea
rned
our
heal
thca
resy
stem
isso
brok
enth
attw
o.th
i,ds
ofba
nkru
ptci
esar
em
edic
al.
Dun
ngth
istim
e,Ia
pp
ted
for
Lon
g.T
erm
Dis
abili
ty.
A,
ofte
nha
ppen
s,m
yfir
stap
plic
atio
nw
asde
nied
.Ir
eapp
’ied
.M
yfil
ew
aslo
st—
tw;c
e.Ju
stbe
fore
my
first
cour
the
arin
g,m
yat
torn
eyw
asho
spit
aliz
edw
ithhi
sow
nm
edic
alem
erge
ncy.
Whe
nm
yse
cond
hear
ing
date
arri
ved,
the
Judg
ew
asca
lled
toan
othe
rco
urt.
Fina
lly,
the
thir
dda
lear
rive
d:I w
asaw
arde
dL
ong.
Ter
mD
isab
ility
.
Nat
ural
ly,
Iexp
ecte
da
chec
k.A
lter
wai
ting
mon
ths
and
dilig
ently
chec
king
with
Soci
alSe
curit
y,th
em
anag
erof
the
New
Yor
kof
fice
calle
dth
em
asag
erof
she
Chi
cago
offi
ceto
requ
est
anex
pedi
ted
shed
.It
was
.Si
xw
eeks
late
rB
utth
esi
zeot
the
awar
dne
cess
ilat
edtn
ree
inst
allm
ents
.Fi
naK
y.af
ter
mor
eth
an2
year
s,m
ySo
cial
Secu
rity
Ois
abil.
fych
eck
was
paid
infu
ll,m
ost
go:n
gto
over
due
med
,ral
b:lls
The
Tom
Ikne
wfo
r50
year
sis
nolo
nger
.la
mst
illge
ttin
gto
know
the
new
Tom
.So
me
days
feel
frag
ile;
othe
rfe
elst
rong
.T
heN
ewTo
ml.v
esw
ithch
roni
cp&
n.In
my
prio
rlif
e,Is
erve
don
she
boai
dsof
soci
alse
rv.c
eag
ende
s,e’
way
shi
nd.r
aiur
rg.
Toda
y,‘a
ma
clie
n:,
and
etem
ally
grat
eful
tosa
,cis
orga
niza
t:ons
and
rne:
rdo
nors
.
life
asw
eknow
itca
ntu
rnin
anin
stan
t,
fore
ver
and
un
alte
rab
lych
anged
Iam
activ
ein
supp
ort
grou
psw
here
we
help
one
anot
her
navi
gate
this
New
Nor
mal
.Ea
chof
usha
sa
full
plal
eof
stre
ss,
man
yso
the
poin
tof
over
load
.
I’ve
lear
ned
afe
wpr
ofou
ndtr
uths
inm
yjo
urne
y:
•Fi
rst,
life
asw
ekn
owis
can
turn
inan
inst
ant,
fore
ver
and
unal
tera
bly
chan
ged.
Seco
nd.
heal
ing
take
stim
e,lin
ancr
atly
,em
otio
nally
,ph
ysic
ally
—le
avin
gus
inva
ried
stag
esof
prep
ared
.ne
ssan
daw
kwar
dnes
san
dcI
umsi
nrss
.It
take
stim
eto
embr
ace
the
new
you,
shen
ewm
e.
Third
,w
ear
eou
rbr
othe
r’s
keep
er—
we
owe
itto
ours
elve
san
dso
one
anoi
he,
lobe
ther
efo
rea
choT
her.
Mos
tas
sure
dly
this
iidude,
heat
tfsc
are.
Wor
tyin
gab
out
payi
ngfo
rhe
alth
care
shou
ldne
ver
bin
onan
yone
’spt
ate
Hea
lshc
are
isa
mor
algo
od,
not
am
eans
for
exto
rtin
gpr
ofits
.
Farr
is‘i’
omT
hom
as,
once
asen
aIe
ntre
pren
eura
ndac
irce
inph
itant
hmpy
,is
now
anac
t,.C
r,t,
a,ie
er
Bill
ing
com
poun
dsSe
riou
sH
ealth
Con
ditio
n
Ten
year
sag
o,on
anev
enin
gin
Febr
uary
,th
esc
hool
whe
reIt
each
mus
icca
lled
toco
nfirm
my
plac
eon
anex
citin
gsc
hool
trip
toC
hina
.Bu
sIm
iste
dth
eca
ll:Iw
asbe
ing
rush
edso
the
hosp
ital
with
abr
ain
infe
ctio
n,so
ondi
agno
sed
asen
ceph
aliti
sac
com
pani
edby
ase
irue.
I’dco
me
hom
efr
omsc
hool
not
feel
ing
wel
l.tc
rais
led
into
bed.
My
husb
and
was
relie
ved
that
for
once
,I
was
givi
ngin
tobe
ing
sick
,so
hele
tm
est
eep.
But
the
next
day,
hetr
ied
tow
ake
me.
my
eyes
wer
eop
enbu
tun
seei
ng,
fdid
not
resp
ond
toan
ylhr
nghe
said
.H
eca
:led
911.
wor
ried
for
my
LIe,
my
elde
rda
ught
erfle
win
from
Sro
slan
d‘w
aslo
stin
aki
ndof
daik
ness
.O
nce
itse
emed
likel
yIw
ould
surv
ive,
my
doct
ors
expe
cted
Iwou
’dne
edm
onth
sin
she
hosp
;lal
tore
cove
r.B
utI
surp
rise
dm
yne
urol
ogis
tby
the
spee
dw
i5h
whi
chIs
naup
edba
ckfr
omth
ein
itial
sym
ptom
s,an
dIw
asai
low
eolo
go
hom
eaf
ter
ten
days
.
Enc
epha
liti
spr
esen
tsa
pani
cula
rty
trick
yre
cove
rybe
caus
esh
ein
stru
men
tyo
uus
eso
eval
uate
and
inte
rpre
tyo
urse
lfan
dth
ew
orld
Isda
mag
edE
mot
iona
lre
cove
ryto
oklo
nger
than
phys
ical
and
men
Ial
func
tions
.C
omin
gto
term
sw
ithw
hat
happ
ened
look
abou
tB
year
s.Is
isha
rdto
dist
ingu
ish
whe
ther
ther
eis
perm
anen
tda
mag
efr
omw
ork
arou
ndbr
ain
deve
lopm
ent
orev
enag
ing.
Ihad
very
good,
and
very
exp
ensi
ve,
heal
thin
sura
nce
Ihad
very
good
,an
dve
ryex
pens
ive,
heal
thin
sura
nce
—ha
lfpa
idby
my
empl
oyer
and
half
bym
e.To
give
me
she
best
poss
ible
chan
ceof
reco
very
,m
yex
cell
ent
neur
olog
ist
refe
rred
me
for
neur
o’ps
ych
test
ing
with
anot
her
exce
llen
tdo
ctor
.Si
nce
the
hosp
ital
took
my
insu
ranc
e,w
eas
sum
edth
esp
ecia
list
wou
ld.
Inm
yve
ryda
mag
edm
enta
lst
ate,
Idid
n’s
ask
abou
tpa
ymen
t.Is
turn
edou
tth
ispa
rtic
ular
donor
was
n’t
onm
yrn
sura
nce
so,
afte
rne
gota
fion
s,th
ebi
Bfo
rte
stin
gw
asso
met
h:ng
Ike
54,5
03.
Dea
ling
wis
hR
ecov
erin
g.R
ecov
erin
gfr
omB
illin
g
Kno
win
gw
hat
ape
rtec
s:on
’st
and
wor
kaho
licla
m,
my
neur
olog
ist
insi
sted
‘tak
esh
efu
ll3
mon
ths
ofd’
sabi
t.ty
leav
eof
fere
dby
my
scho
ol.
Iwas
sorr
yto
mis
sw
ork,
and
my
stud
ents
mis
sed
me,
too.
But
Iw
asgr
afef
ulfo
rsh
ele
ave
beca
use
Inee
ded
lime
tone
goti
ate
heal
thca
repa
ymen
tis
sues
.
Wis
ileit’
sha
rden
ough
tode
alw
ithhe
alsh
care
bills
and
insu
ranc
eco
mpa
nies
with
ahe
alth
ybr
ain,
heat
thca
rebi
lls(w
hich
don’
tw
ail
for
you
sore
cove
r)ar
eR
EALt
Ydi
ffic
ult
with
ada
mag
edbr
ain.
And
the
bills
wou
tdn’
cgo
away
.Is
till
felt
conf
uted
,lik
eIn
eede
dal
lm
yst
reng
thju
stto
put
mys
elf
bask
toge
ther
.T
here
was
alo
tof
back
and
fonh
with
the
hosp
ital
and
she
insu
ranc
eco
mpa
ny;
itw
asex
haus
ting
,st
ress
ful,
and
time-
cons
umin
g.Ire
mem
ber
gett
ing
sofr
ustr
ated
that
she
hillr
ngof
fice
kept
felli
ngm
efo
wed
mor
em
oney
than
‘thought’
ahou
ld.
The
insu
ranc
eco
mpa
nyan
dbh
ling
offi
ceke
ptbo
unci
ngm
eba
ckan
dfo
rth.
And
the
bills
wou
ldn’
tgo
away
.Is
till
felt
conf
used
...
ftw
asex
hau
stin
g,
stre
ssfu
l,an
dti
me-
cons
umin
g
Icl
ea’ly
rem
embe
rse
lling
anem
ploy
eein
the
bitli
igof
fice
that
Iwou
ldpa
yso
me
amou
nt,
even
thou
gh‘t
houg
htit
was
n’t
fair,
ifw
eco
uld
lust
bedo
new
ithif,
The
yva
ere
givi
ngm
ea
runa
roun
dab
out
havi
ngto
chec
kit
out,
but
thei
rsu
perv
isor
over
hear
dif
from
anot
her
room
—an
dca
me
runn
ing
in,
sayi
ngth
ey’d
take
my
mon
eyan
dcl
ose
the
case
.M
yre
cove
ryth
enco
ntin
ued
with
out
the
adde
dw
orry
ofhi
ghbi
lls.
Ires
umed
tow
ork
Ilov
edth
enan
dco
ntin
ueto
enjo
yno
w.
Med
ical
bank
rupt
cies
and
deb
t:E
lim
inat
ed.
118
Iam
ast
rong
supp
orte
rof
the
Nes
vY
ork
Hea
lthA
ctbe
caus
eIw
ant
ever
yone
toha
vehe
alth
care
cove
rage
that
itas
good
as(o
rbet
ter
than
)m
ine
—bu
tw
ithou
tst
ress
ful
nego
tiat
ions
with
bure
aucr
acy,
bills
,pa
perw
ork,
prio
rap
prov
als,
nego
tiat
ions
,an
dth
eta
rge
sum
sgo
ing
to“m
iddl
emen
”th
atou
rty
tsem
requ
ires
.
Jady
Flet
cher
,w
holiv
esin
the
Dro
ne, i
sa
rrolin
isf,
teac
her,
envir
onm
enta
landpolr
ticat
anie
’st.
No
hass
les
onbi
lls,
ever
—th
ere
aren
’tan
y.

Heaithcare
Costs:
Destroy
Dream
s.D
iscourageE
ntrepreneurs‘reg
nan
cyC
omplications.
Three
Lives
atR
iskI
I vividlyrem
ember
thataw
fulday.A
ugust4th
2014.t.o
riand
Ihadbean
married
lessthan
ayear.
Shehad
recentlyquit
hercorporate
financejob,
goneback
toschool
andstarted
herow
nbusiness.
Thai
daythe
woke
up,turned
tom
e,and
said,“I
can’tfeel
my
arms
andlegs.”
Shew
as28
yearsold.
There
isno
adequatew
ayto
descriheshe
fear,the
piercingdread,
thatw
ashesthrough
youw
henthe
wom
anyou
lovesays
something
likethat,
gatheredher
upand
droveto
shehospital
ER. After
admitting
hero
nan
outpatientbasis,
theyw
heeledher
tothe
radiologydepartm
entfor
anM
Rl.T
heydirected
me
tothe
billingdepanm
ent.W
ethought
we
hadgreat
inaeraece,just
likew
ethought
we
were
youngand
healthy,but
theyw
anted$5,000.
On
thespot.
Inthe
mom
entw
ew
erem
ostvulnerable,
inshe
mom
entm
yw
ife’shealth
was
moss
unclear,she
systemrequired
$5,000.Im
mediately.
Part
ofm
ew
ondered
maybe
we
weren’t
worthy
otcare
ifw
ecouldn’t
pay.Ican
stillfeel
sliatpanic
Ithoughtthere
must
besom
em
istake.N
aively,I
thoughtthey
must
nothave
runthe
insurancecard
correctly.R
unit
again,I urged.
But,
no,they
were
right—
ourdeductible
was
$5,000.Ihad
two
creditcards
inm
yw
allet.T
heanxiety
I feltunnerved
me,
Panof
me
was
surethey
would
providecare
evenif
bothcards
were
denied.Pan
ofm
ew
onderedm
aybew
ew
eren’tw
orthyof
careifw
ecouldn’t
pay.Ican
stillFeel
thatpanic.
Consider:
thisw
asdespite
knowing
we
hadinsurance.
Good
insurance,
Looking
back,I know
we
wem
lucky.Ihad
two
creditcards,
andboth
were
paidup.
But
when
“luckyin
Am
enca”m
eansyou
havethe
capacityto
accruepotentially
vastm
edicaldebt,
we
inA
merica
havea
seriousproblem
.Tw
oyears
ofstruggle
followed
thisinitial
hospitalvisit.
Two
yearsof
doctorvisits,
latenight
callsto
insurers,everyday
battlesto
demand
thatthe
carem
yw
ileneeded
anddeserved
was
thecare
shegot
—and
two
yearsof
debtthat
almost
buriedus
financially,alm
ostcost
ourfam
ilyall
we
had,
We
leftN
ewY
orkfor
New
Ham
pshireand
moved
inw
ithm
yA
unt,W
ew
eregrateful
forher
help:w
ecouldn’t
affordm
edicalbills
pluscredit
cardbills
plusrent
ontop.
Our
strugglew
asn’tunique
then.It’s
notunique
now,
Healthcare
inA
merica
isbroken.
It’sa
systemthat
demands
peopleem
ptytheir
wallets
andstress
theircredit
—w
henthey
arecom
pletelyvulnerable,
paralyzedw
ithfear,
andgrievously
worried
aboutthe
fateof
someone
theylove,
Our
lawm
akersm
ustlisten
tothose
who
votefor
them,
ratherthan
shethousands
oflobbyists
spendingm
illionsof
dollarsto
keepthe
statusquo.
Healthcare
istoo
expensive.Its
costis
destroyingtoo
many
Am
encanfam
ilies.Y
es,of
course,it’s
am
oralissue.
But
it’salso
afiscal
issue.M
dan
economic
issue—
forindividuals,
families,
comm
unities,states,
andour
country,
When
we
investin
healthcare,w
eare
investingin
Am
erica...
bigthinkers
andsm
allbusiness
owners
Families
who
arestm
gglingevery
dayto
payfor
foodand
rentend
medical
billsare
tootired
andw
ordedto
work
ontheir
dreams.
How
canm
eexpect
themto
beinventive?
Entrepreneurial?
Tostart
theirow
nbusinesses?
When
we
investin
healshcare,w
eare
investingin
Am
erica—
invetsingin
anA
merica
thatrew
ardsbig
thinkersand
small
businessow
ners,people
who
starttheir
own
business,create
newjobs,
andbuild
valuefor
ourcom
munities.
People
who
fearlosing
theirhealth
coverage,w
hoknow
thattheir
currentjob,s
theonly
way
theycan
afford
insurance,those
peopledon’t
leavejobs
evenifthey
hatethem
,even
if thehealth
insurancekeeps
theirw
ageslow
,even
ifthey
yearnto
transformtheir
bigidea
intoa
business.
People
who
fearlosing
theirhealth
coveragedon’t
leavejobs
—even
ifthey
hatethem
,even
ifhealth
insurancekeeps
theirw
ageslow
TtseR
andC
orporationrecently
analyzedthe
NYH
ealthA
ct,and
concludeditw
ouldcover
everyNY
residentfor
lessthan
what
NY
iscurrensly
paying—
andthat
savingsw
ouldstim
ulatethe
NYeconom
y,m
akeN
Ybusinesses
more
competitive,
unleashentrepreneurship,
raisew
ages,and
crease200,000
more
jobs.O
urgovem
ment
needsshe
fiscalprudence
ofsingle’payer
healthcare.Fam
iliesneed
besterand
more
affordablehealthcare,
Law
makers
needto
hearconstituent
voicesthat
understandthe
issuesfacing
ordinaryA
mericans,
small
businessow
ners,and
families.
I’veseen
firsthand
abroken
systemthat
failsfam
iliesw
hoare
experiencingthe
scariestweeks
andm
onthsof
theirlives.
It’stim
eour
representativesrepresent
ourvoices
andour
future.
Oeagtan
McE
achernm
oved(m
mN
Yback
tofam
ilyin
NH
afterruinous
medicalbills;he
works
inrechnotogy
andnow
adrocareafor
unirersal haalthcam.
rat’sI:
My
lifeexplodes
intohealthcaro
nightmare
Diagnosed
with
preeclampsia
andsevere
ante’nataldepression.
Prescription:total
bedrest.
Here
Iwas,
ina
high’riskpregnancy
shascan
leadto
HEI.LP
syndrome,
aIife.threatening
complication
thathad
almost
killeda
goodfriend.
The
ideaof
leavingm
yth
reeold
erchildren
mo
therless
terrifiedm
e
I knewA
merican
wom
encan
anddo
diefrom
this;it’s
partof
why
theUS
isshe
onlycountry
with
risingm
aternalm
ortality.Iknew
Ineededm
edicalcare
tosave
my
baby—
andso
savem
yow
nlife.
The
ideaof
leavingm
ythree
olderchildren
motherless
terrifiedm
e.R
atherthan
givingm
em
edicalleave,
my
schoolterm
inatedm
e—
which
terminated
my
healshinsurance,
andthe
healthinsurance
ofm
ychildren.
Iwasn’t
eI:giblefor
unemploym
entbecause
Icouldn’tlock
foia
job:com
pletebed
rest
•Iw
asn’teligible
forIperm
anenildisability
becausehigh’risk
pregnancyis
temporary
lehennot
lethal)•
Iwasn’t
eligiblefor
COBRA
,sincem
yem
ployerdidn’t
processm
yterm
inationas
Iasked
•Iwas
scared,and
notjust
form
e
Yes,
Iwas
inthe
moss
dangeroustrim
esterof
ahigh’
riskpregnancy,
butm
yrw
een,recently
diagnosedw
ithsevere
emotional
disabilityand
suicidaldepression,
hadjust
beenaccepted
intoan
inp
atient
program.
When
Ilostm
yhealth
insurance,she
was
terminated
fromher
program.
Her
needsw
ereserious,
andIhad
now
ayto
helpher.
I’dlike
every
local,state
and
natio
nal
represen
tative
tosp
end
afew
day
sw
aiting
among
those
need
ing
ben
efits
My
desperationfor
my
kidsovercam
eshe
profoundsham
edeepening
my
depression:I decided
toapply
forM
edicaid.Itw
asm
ean.spirited,B
yzantine:
Youm
ustapply
inperson
ata
localSocial
ServicesO
ffice.They
openata
00am
,giveyou
anum
beras
youenter,
andthen
youw
ait.
Thetine
outsideform
slong
befom800a.m
.because
youneed
tobe
atthehead
ofshequeue
toget
alow
number.
Irushedto
leavem
ykids
atschool
eadyto
anisebefore
8.00am
,and
nevergot
alow
numher
Because
Ihadto
pickup
my
kidsafter
school,Ih
adto
leaveat 3:00
pmso
Ilostm
yplace.They
lockthe
doomat
3:00or
330,
soyou
can’tcom
eback,
Ifyouleave,you
haseto
returnagain
thenest
morning.
‘Who
made
thesem
les?D
on’sallm
oms
haveto
carefor
kids?People
who
needSocial
Servicesfor
urgent,scary,
Iife.threaseningreasons
havecom
plicatedlives.
Isit
likethis
sodiscourage
people?
I’dlike
everylocal,
stateand
nationalrepresensative
tospend
afew
daysnailing
among
thoseneeding
benefits:every
oneof
ushad
assory,
some
farw
orsethan
mine.
Ifinallygot
my
Medicaid
cardat
38w
eeks.
Who
made
these
rules?D
on’tall
mom
shave
tocare
forkids?
People
who
needSociel
Services
for..,
life•threateningreasons
havecom
plicatedlives
We
mere
allincredibly
fortunatethat
Ididn’tfall
intosuch
adebilitating
depressionthat
Icouldn’tleave
my
bed,although
Icame
close.In
short,as
anguishinglyhorrible
asit w
as,w
eall
survived.
rertII:
The
nightmare
subsidesinto
HC
limbo
Bus,
jutslike
life,m
ystory
continues—
notyet
asgood
asitw
asbefore
thepreeclam
pssa,but
som
uchbetter
thenthose
threem
onths.Ilive
ina
stateof
uncertaintyabout
boshem
ployment
andhealthcare,
Tom
akem
yselfeven
more
attractive—
Iamgaining
additionalcertification
som
yschool
canuse
me
ina
greatervariety
ofsub1ecrs
with
agreater
varietyof
students.I
likethis
school,and
Iloveteaching.
With
NY
HA
my
termination
would
nothave
sodesperately
worried
me
aboutleaving
my
childrenorphans.
And
my
daughtercould
havecontinu
edthe
excellentprogram
she’dentered
ratherthan
interruptingitto
returnto
afam
ilyin
crisisw
itha
mother
who
was
almost
asdepressed
asshe
was,
Under
NY
Health,
I wouldn’t
todaybe
soconsum
edw
ithpatching
togethercontinuing
coveragew
ithas
fewgaps
aspossible.
Instead,I could
focuson
doingthe
bessoh
Icanfor
my
studentsand
colleagues.U
nderN
YH
ealthI’llbe
happyto
paym
orew
henm
yincom
erises.
Carm
enLyre
isa
rpeoaleducation
teacherand
them
oiharof fourchildren,
Entrepreneurs
will
flourish,creatIng
200,000new
jobs.17
Your
childrenw
illalw
ayshave
healthcare.So
willyou.

ERD
oc:
For-
Prof
itIn
sura
nce
Isn’
tG
ood
Eno
ugh
Mig
rain
e.S
cary
Pro
gnosi
s.S
cari
erD
ebt
The
Cas
tof
Hea
rtac
he
Sto
pr
brou
ght
life-
savi
ngpr
epto
ade
adha
lt.
Aw
oman
inhe
rSO
sla
yon
agu
rney
inth
eER
whe
reI
aman
atse
ndin
gph
ysio
an.
Imet
her
EKG
befo
rem
ethe
r,no
ting
the
omin
ous
tom
bsto
nex
patt
ern.
wen
tto
med
ical
scho
olto
heal
peo
ple
,not
tohav
efi
nanc
ial
dis
cuss
ions
about
indic
ated
care
The
wom
anw
aspa
le,
swea
ty,
hold
ing
her
ches
t,co
mpl
aini
ngof
crus
hing
pain
,an
dIt
old
her
she
was
‘hav
ing
ahe
art
atta
ck’
—a
diag
nosi
sIh
ave
mad
eov
er10
0tim
es.
We
calle
dfo
ra
STE
Ml
Ale
rt”
whi
chm
obili
zes
ate
amto
perf
orm
aca
rdia
cca
thet
erpr
oced
ure
—sa
ying
“STA
T”is
redu
ndan
t.
sMie
nan
EKG
show
sa
hear
tat
tack
inp’
ogre
ss,
we
live
byth
em
antz
a‘F
me
isM
uscl
e.”
Ope
ning
tnat
clog
ged
arte
ryin
her
hear
tw
.thin
90m
inut
esof
the
pati
ent
ente
ring
the
ERis
the
geld
stan
dard
.ii
’e
90m
inut
esm
ayso
und
like
fore
ver,
prep
ping
isno
tsi
mpl
e:th
ere
are
nom
inut
esto
spar
e.W
est
ripp
edhe
rcl
othe
s,ch
ecke
dvi
tals
,in
sert
edlV
s,dr
ewbl
ood,
atta
ched
mon
itor
s.
..
Like
api
tne
wat
ara
cetr
ack.
asw
arm
ofdocs
or,
nurs
es,
and
tech
nici
ans
tryto
beat
she
dock
.T
hesc
ene
may
look
chao
tic,
bus
ever
ype
rson
isfo
cuse
dan
dfa
ston
anes
sent
ial
job
—to
keep
the
patie
nt’s
hear
tm
uscl
eal
ive,
tosa
vehe
rlif
e.
And
then
cam
eth
esc
ream
that
stop
ped
ever
ythi
ng,
the
entir
eER
shoc
ked
byou
rem
erge
ncy
card
iac
pati
ent
shou
ting
,“S
topl
Stop
l”‘I
need
my
phon
e.In
eed
my
insu
ranc
eca
rd,
Are
you
inm
yne
twor
k?l”
The
team
froz
e.Iw
alke
dto
the
head
ofth
egu
rney
.A
sw
em
ade
eye
cont
act,
she
blur
ted,
“Iha
vein
sura
nce,
but
it’s
ahi
ghde
duct
ible
plan
.M
ysp
ouse
pass
edaw
ay.
Ihav
ea
teen
aged
daug
iste
r.Id
on’t
know
ifIc
anaf
ford
this
.”
Inw
hat
was
likel
yth
em
ost
vuln
erab
lem
omen
tin
her
lile
from
ahe
alth
care
pers
pect
iee.
she
was
NO
Tfn
ghte
ned
byw
hat
was
happ
en;n
gin
her
body
orth
at,
with
out
emer
genc
ytr
eatm
ent,
she
mig
htdi
e—
that
min
utes
ofde
lay
coul
dca
use
al,f
etim
eof
disa
bilit
y.H
erfo
cus
was
onth
eco
st,
abou
tbe
ing
the
only
supp
ort
for
her
teen
aged
daug
htec
The
team
look
edba
ckat
me,
anxi
ousl
yey
eing
the
cloc
k.Ic
an’t
adeq
uate
lyde
scri
beho
wth
issi
tuat
ion
mak
esm
efe
el.
V,’h
enpa
tien
tsbr
,ng
upco
st,
espe
cial
lyin
such
anun
com
prom
isin
gly
emer
gent
cond
itio
n,w
here
the
med
ical
deos
ion
iscr
ysta
lcl
ear.
IFin
dm
ysel
ffe
elin
ga
dee
ppi
tof
ange
r,di
sgus
t,an
dpa
inin
my
own
hear
t.Si
nce
Ifirs
tst
arte
dm
edic
alsc
hool
in20
01,
I’ve
know
nm
edic
albi
llsar
eth
ele
adin
gca
use
ofpe
rson
alba
nkru
ptcy
inA
mer
ica,
mos
tw
ish
priv
ate
insu
ranc
e.It
wor
nes
me
that
the
care
Idel
iver
—an
dev
enth
efiv
esw
esa
ee—
too
ofte
nal
sode
liver
scr
ippl
ing
cost
s.
love
putt
ing
my
year
sof
trai
ning
and
clin
ical
expe
rien
ceto
wor
k—
but
whe
nla
mfo
cuse
don
savi
nga
patie
nt’s
futu
rehe
alth
,Ih
ave
noad
diti
onal
men
tal
band
wid
th.
Itol
dhe
rw
ew
ante
dto
keep
her
aliv
e,th
athe
rfif
ew
asw
orth
savi
ng,
that
not
trea
ting
her
now
coul
dki
llhe
ror
leav
ehe
rdi
sabl
ed.
I tol
dhe
rth
ere
was
now
ay,
inth
isli
fe-t
hrea
teni
ngst
uati
on,
whe
rese
cond
sm
atte
r,th
atI c
ould
figu
reou
tco
sts
4r,d
I ass
ured
her
the
hosp
ital
wou
ldw
ork
w,th
her
and
her
insu
rer
She
let
uspm
ceed
.T
hela
bin
sene
da
sten
t.
Med
ical
lysa
vin
gli
ves
can
fina
ncia
lly
ruin
tfse
m
Icen
tto
med
ical
scho
olto
heal
peop
le,
not
toha
vefi
nanc
ial
d,sc
uss,
ons
abou
tin
dica
ted
care
,B
utth
ecu
rren
tst
ate
ofA
nsei
ican
heal
shca
refi
nanc
ing
has
crea
ted
ado
uble
-edg
edsw
ord:
Med
catly
savi
ngliv
esca
nfi
nanc
ially
ruin
them
Ou
rcu
rren
tIs
ealt
hca
resy
stem
has
tota
lly
cois
spro
mis
edth
edoct
or.
pat
ient
rela
tio
nsh
ip.
It’s
hea
rt-b
reak
ing.
And
frust
rati
ng
Isup
port
the
NY
Hea
lthA
ct,
sing
le.p
ayer
heal
thca
m—
whi
chw
illco
vera
lles
sent
ial
care
for
all
NY
resi
dent
s—
with
nopa
ymen
tat
poin
tof
serv
ice.
Mos
tdo
ctor
sag
ree
onth
is,
Inee
dsi
ngle
’pay
erhe
alth
care
soth
atI
can
final
lyte
llm
ypa
tien
ts,
and
may
beev
enyo
uw
hoar
ere
adin
gth
isan
dm
ight
one
day
bem
ypa
tien
t:“D
on’t
wor
ryab
out
the
cost
s.T
hey’
reco
vere
d.Y
oune
edth
istr
eatm
ent
.n
ow
.”B
us
Ican
’t.
Our
cure
ent
heal
thca
msy
stem
has
lota
9yco
mpr
omis
edth
edo
ctor
-pat
ient
rela
tions
hip.
It’s
frus
trat
ing.
And
hear
tbre
akin
g.
Dc
Dan
iel
Lega
ssy
can
ERphys’c
:an
at
3N
YC
hosp
itals
arid
abo
ard
mee
ter,
rtiy
srda
nsfo
r aN
ario
natH
ealth
Pmcr
nn,
NY
Met
roC
hapt
er.
pes’
wny
mef
mor
g.n
jf’catp
eg
nO
’g
At
age
29,
win
abl
ood
clot
atth
ebat
eof
my
brai
n,Iw
asho
sp;t
aliz
edfo
rth
ree
days
in20
15.1
had
tobe
cons
tant
lym
onit
ored
for
stro
kes
orse
izur
esso
.du
ero
ala
ckof
avai
labl
eho
spit
albe
ds,
Iwas
inth
eIC
Ufo
rth
ree
stra
ight
days
.
‘ini
tially
wen
tto
the
ERw
ithw
hat
Itho
ught
was
anet
cept
iona
lly
awfu
l,m
ulti-
day
mig
rain
e.W
hen
the
ERdo
ctor
ran
into
my
curt
aine
doH
area
toas
kfl
had
hit
my
head
(Iha
dn’t
)be
caus
eth
eC
Tsc
ande
mon
stra
ted
blee
ding
,Iw
aste
rrif
ied.
Ihad
tobe
tran
spor
ted
byam
bula
nce
toa
larg
erho
spita
lw
here
anM
RIco
uld
bedo
neon
Satu
rday
afte
rnoo
n.
Iwas
terr
ifie
d,..
nei
ther
ofus
—in
our
pani
c—
thoug
ht
toca
llm
yin
sura
nce
com
pany
Not
hing
like
Ui
5ha
dev
erha
ppen
edto
me
orm
ynu
sbar
tdbe
fore
,so
neit
her
olus
—in
our
pani
c—th
ough
tto
call
my
insu
ranc
eco
mpa
nyto
obta
inpr
e-au
thor
izat
ion
for
all
ofsh
em
edic
alse
rvic
es‘w
ould
need
.W
e&
dn’t
know
how
muc
hw
ould
bene
eded
until
itw
asha
ppen
ingl
Sinc
ew
edi
dro
tca
ll,an
dsi
nce
Ihad
aB
lue
Cro
ssB
lue
Shie
ldhi
gh’d
educ
tibl
epl
an,
man
yaM
,oon
alco
sts
fell
tom
e,an
d‘o
wed
far
mor
eth
anm
yal
read
yhi
ghde
ckic
tible
of$6
,000
.A
lter
leas
ing
the
hosp
ital
,ha
dto
cont
inue
tota
keex
pens
ive
med
icat
ions
sohe
lpbr
eak
dow
nth
ecl
ot.
Tho
ugh
Iwas
dire
cted
tost
art
this
trea
tmen
tth
eda
yIw
asdi
scha
rged
,th
eho
spita
lha
dno
tye
tsu
bmit
ted
itsbi
llsto
BC
BS
with
out
thes
e,as
far
asth
ein
sure
rw
asco
ncer
ned,
I had
not
yet
met
my
dedu
ctib
le,
Iwas
left
with
noch
oice
abou
tpa
ying
hund
reds
ofout
of’p
ocke
tdo
llars
for
my
med
icat
ions
,on
lop
ofm
yho
spita
lbi
lls,
Iwas
left
wit
hno
choi
ceab
out
payi
nghundre
ds
ofou
t-of
-poc
ket
doll
ars
for
med
icat
tons
,on
top
ofm
yho
spit
albi
lls
Ihav
eno
tye
tbe
enab
leto
pay
the
hosp
ital
infu
ll,w
ell
over
two
year
sla
ter.
‘fee
llu
cky
the
hosp
ital
put
me
onan
exte
nded
paym
ent
plan
,an
dIa
mfin
ally
clos
eto
payi
ngof
fm
yor
igin
alho
spita
lbi
lls.
Inde
term
inin
gth
eca
use
ofsh
ebl
ood
clot
,ho
wev
er,
my
doct
ors
foun
da
num
ber
ofun
derl
yng
fact
ors
and
pos&
bte
resi
dual
effe
cts
that
requ
ire
med
ical
atte
nti
on
and
mo
nit
ori
ng
.
Cou
nt’e
ssm
edic
alap
poin
tmen
ts,
anad
diti
onal
hosp
ital
stac
and
anER
visi
tla
te’,
my
med
ical
debt
cont
inue
sto
grow
.
lam
anat
torn
eyin
apu
blic
inle
test
fiel
d(d
isab
ility
righ
tsan
dad
voca
cyl.
Tho
ugh
Iwor
kha
rdan
dlo
vew
hat
I do,
dono
tm
ake
wha
tpe
ople
assu
me
anat
torn
eyw
ould
.It’
sha
rden
ough
tosl
ayaf
loat
fina
ncia
llyw
ithou
tth
ead
diti
onal
med
ical
expe
nses
.T
houg
h‘n
owha
vebe
tter
heal
lhca
reco
vera
ge,
Istil
lha
vesi
gnif
ican
t co’
pays
and
co-i
nsur
ance
.
Cou
ntle
ssm
edic
alap
poin
tmen
ts,
anad
diti
onal
hosp
ital
stay
,an
dan
ERvi
sit
late
r,m
ym
edic
aldeb
tco
ntin
ues
togr
ow
Iwo’
ryth
atth
ere
peal
olth
eA
ffor
dabl
eC
are
Act
’snd
vjdu
alm
anda
tein
the
new
fede
tal
tax
bill
will
leav
em
ew
ithfe
wer
heal
thin
sura
nce
opti
ons
—an
dhi
gh,e
rm
edic
albi
lls.
Like
me.
man
yof
usar
ebu
rden
edw
ithvi
gnif
:can
tliv
ing
expe
nses
and
reti
oact
ive
b:lls
for
our
stud
ent
loan
s.
As
adi
sabi
lity-
righ
tsat
torn
ey,
and
asa
pers
onw
hono
what
spr
e.ex
!stin
gco
nditi
on,
I see
firs
than
dho
wris
ela
ckof
affo
rdab
le,
qual
itym
edic
alca
reaf
fect
spe
ople
ofal
lw
alks
oflif
e,ev
ery
day.
Asi
ngle
.pay
ersy
stem
isne
cess
ary
tom
ake
sum
all
New
Yor
kers
are
able
toco
ntin
ueto
lead
heal
thy,
prod
ucti
veliv
es:
anyo
neco
uld
have
am
edic
alem
erge
ncy
atan
ym
omen
t,an
dno
one
dese
rves
togo
deep
into
debt
beca
use
ofit.
Laur
enG
race
isa
disa
bilit
yrig
hts
atto
rney
and
advo
cate
.Sh
epr
actic
esin
Nei
rYo
rkC
iry
Pat
ient
sfa
cing
deat
hw
on’t
focu
son
thei
rw
alle
ts.
316
All
insu
rer
trap
sel
imin
ated
.
I
‘if

Prior
Authorizations:
Designed
toK
eepP
atientsFrom
Care
re-Existin
gC
onditions.Insidiously
Curtailing
Careers
iiIam
aregistered
nursew
orkingin
adoctor’s
officeat
am
ajorN
YC
medical
center
my
woik
with
patientssuffers
fromhaving
tochase
priorauthorizations.
amtrained
totreat
patientsand
certifiedto
doprocedures
onpatients.
Butwhenever
thebest
courseof
treatment
isnot
onthe
‘formulary”
ofan
insurer(w
hichw
orksw
ithstiff
anothercom
panyto
manage
itsm
edicationapprovals),
Ispendhours
deafingw
itha
convofutedsystem
.
Iamnot
atall
surehealth
insuranceis
about
health
Letm
egive
anexam
pleof
what
was
recentlyrequired
toget
apatient
thebest
carepostibfe.
Thispatient
cannotsake
thegeneric
ofa
specificm
edication.It
makes
herill.
Shepays
ajot
ofm
oneyfor
hersupplem
entalinsurance
andneeds
herinsurer
toauthorize
payment,
sinceshe
cannotafford
tobuy
them
edicine.The
sagabegins,
asitoften
does,w
henher
onginalprescription
was
deniedat
thepharm
acy.
amnot
sureevery
doctot’soffice
putsas
much
effortinto
thisas
oursdoes,
feedingm
eto
believethat
insurancecom
paniespuiposefuffy
handletheir
prtorauthorization
processin
thisw
ay.A
syou
readthrough
thesteps
fittedbelow
,keep
inm
indthat
the“benefits”
emptoyees
f deafw
ithhave
nom
edicalknow
ledge,read
scriptedquestions,
haveno
managem
entavailable
attheir
caffcenters
fforappeafing
decisions),and
haveno
connectionbetw
eentheir
company
(which
manages
prtorauthorizations)
andthe
insurancecom
pany.
alengthy
[appealsiprocess
canlead
toex
acerbatio
nof
illness—
andeven
hospitalization..
almost
always
more
expensivethan
medication
Priorauthorizationsate
themselves
obstades,but
havingthe
processbe
soB
yzantineand
time-consum
ingexhausts
thedoctors
officesand
causesm
ostdoctors
togive
up.1en
doctorsoffices
giveup,
patientsusuaffy
dosom
ethingsub-optim
aforjust
gow
ithout.
Rem
ember
thatw
hifew
epursue
thisprocess,
thepatient
goesw
ithouttreatm
ent,aed
afengthy
processcan
leadto
exacerbationof
ilfnest—
andeven
hospitalization.T
hoseare
afmost
afways
more
expensivethan
them
edication.T
heshortsightedness
ofpre-authorization
isastounding.
21S
tepsG
ettingO
neP
atiantN
eeded
Medication:
1.f called
forprior
authorization.2-
That,nitialcalf
was
denied.
I was
thentold
thedenial
was
‘anaccid
ent’
andthat
everyshingw
asok.
No
progress.
4.Iw
aslater
toldIn
eeded
aleo
erof
‘wed
icalnecessity”
which
Icrafted,
detailingthe
reasonsthe
patientn
eeded
the
wedicatioe
andcouldn’t
Lakethe
generic.T
hedocto
rsigned.
5.T
heprior
authorizat,oew
asdenied.
6.fw
astold
theC
ola
code
(classificationof
condiiicnlw
asincorrect;
itw
asn’t.
7.T
hecom
panyth
ensaid
fneed
edan
appeal
a.tfased
theappeal:
Ihave
areceipt
thatit
went
through.
9.W
eheard
nothing:the
secondarycow
panysaid
we
need
edto
callthe
firstieserance
company.
10.T
heinsurance
company
saidthey
didn’tknow
what
thesecondary
company
answered.
11.They
askedm
eto
fatthew
again.
12.fdid.
13.They
didn’tim
mediately
seethe
laxand
toldthe
patientlw
hocalled)
thaithey
didn’thare
anything.14.
Thew
holeprocess
tooksix
weeks.
15Sy
thetiw
efcalled,
theyhad
foundthe
appeal.
16.treq
uested
thatthey
eaped
tethe
appeal.
‘7.They
saidno.
18.1requested
tofire
acow
pfaint.They
said“no”;only
thepatient
cantie
acom
plaint.19.1
requestedthat
thecom
panycalf
thepatient
with
theresult.
20.A
manager
said‘no’;
theycannot
fagthe
syitemin
thatw
ay.
21.Finally,
thepatientw
asable
roget
theprescnption.
Alice
Lovehas
beena
registerednurse
for22yaars.
jsta
flnuw
sr.saR
a4sT
.4ov1D
O’J
My
Dream
tD
erailed
‘Pre’esisting
condition”:heafthcare
lingofor
anillness
youhave
priorto
applyingfor
healthinsurance.
According
nothe
Kaiser
Family
Foundation,
over25%
ofN
ewY
orkersunder
age65
havepre-exittieg
conditions—
suchas
diabetes,cancer
(evenif
cured,cut
out,or
inrem
ission),high
bloodpressure,
depression,allergies,
oranylh:ng
aninsurer
chooses.
You
may
noteven
knowthat
youhave
sucha
condition.Icertainly
hadno
idea.M
ysenior
yearin
college,t w
ona
Fuibrightfellow
shipto
studyLa
Mone
d’Arthur
inE
ngland,C
ertificationrequired
am
edicalexam
.Tom
ysurprise
anddism
ay,the
doctorrefused
tocertify
me:
‘Iabsolutely
cannotlet
yougo
abroad:you
havea
heartm
urmur’
(specifically,a
‘mitral
valveprolapse’).
Ina
highlycom
petitivefield,
universitiesw
erechary
ofhiring
someone
who
might
haveA
IDS
Sothe
deathof
Arthur
became
thedeath
ofa
lifelongdream
tostudy
with
thefam
ousM
aloryscholar.
Disappointed,
Ipursuedless.specialized
graduatestudy.
Over
my
longacadem
iccareer,
Ineveragain
faceda
physicalexam
forany
job:F
ortunate,because
costcalculations
canfuel
agedescrim
ination.
In20)4,
longretired
andon
Medicare,
them
urmur
became
decidedlypronounced.
Open
heartsurgery
repared
thevalve.
Because
IhadM
edicareand
aprivate
policyto
paygaps
inM
edicarecoverage,
Ihadno
additionalcosts.
Another’s
Dream
sD
erailed
Inthe
80s,w
henIw
asD
epartment
Chair
ata
small
college,the
academic
jobm
arketw
asglutted.
Many
veryqualified
peoplew
ithadvanced
degreescobbled
togethercareers
asitinerant
professors,traveling
among
severalcolleges,teaching
oneor
two
coursesat
each,having
nohealth
benefits.T
heyhoped
forcontinued
goodhealth
(andno
carcrashes).
One
day,an
extraordinarycandidate
appliedfor
asudden
pan-time
opening.H
isdissertation
hadw
ona
prizeat
ankq
League
university.H
ehad
publishedarticles
inseveral
first-ratejournals.
He
hada
contractfor
anearly
finishedbook,
Hit
dossierof
recomm
endationspraised
hisw
orkso
theskies,
exceptfor
onetroubling
sentence.A
recognizedscholar
fina
similar
field)spoke
highlyof
thecandidate’s
work,
thenadding:
‘AC
anadiancitizen,
Candidate
Xm
akesfrequent
tripshom
ew
herehe
seeshis
doctorand’s
occasionallyhospitalized.”
How
was
th:srelevant
tohis
schotarshipor
teaching?I felt
adilem
ma:
ShouldIviolate
theconfidentiality
ofthe
writer?
Candidates
were
notsupposed
tosee
theseletters.
But
thisnon’eelevancy
suggestedthe
writer
borehim
some
secretanim
us.In
ahighly
competitive
field,universities
were
charyof
hiringsom
eonew
hom
ighthave
AID
S.
cost
calculatio
ns
canfuel
age
discrim
inatio
n
Isookthe
youngscholar
outto
fundsand
askedhim
aboutthe
professorin
question,“O
hyes,’
hesaid,
“we
write
aboutthe
same
things.”W
ithoutrevealing
anythingof
substance,Isuggested
heask
hisuniversity
Placement
Office
torem
ovethat
letter.The
nextyear,
inan
eventighter
jobm
arket,m
yexcellent
hirereceived
nofew
erthan
3tenure-Irack
offersfrom
major
universities.M
yhunch
hadbeen
correct.
Young
peopletoday
continueso
make
careerdecisions
basedon
whether
(andw
hatquality
oOhealthcare
comes
with
theem
ployment
package.
ElseFisher
isa
(mainly)
retiredprofessor
ofShakespeare.
Your
pro
vid
erand
youchoose
yo
ur
care.15
IH
ealthcarecosts
won’t
discouragehiring.

Cau
seof
Dea
th:
For
-Pro
fit
Insu
ranc
e.F
ortu
ne10
0F
ires
liti
gat
or
The
Hos
pita
lis
“In
Net
wor
k.’
Sur
pris
e!T
heD
octo
rIs
Not
Cur
able
Can
cer
Kill
s
I mis
sm
ybr
othe
r.A
brill
iant
trial
lavq
er,
wor
king
inth
eG
ener
alC
ouns
els
offi
ceof
aFo
rtun
e10
0co
mpa
ny,
John
nyw
asab
rupt
lyfi
red
fuss
befo
rehe
turn
edsi
xty.
Iam
,of
cour
se,
bias
edab
out
this
trag
ictu
rnof
even
ts:
John
nyha
dar
gued
(and
piev
aile
d)m
ultip
leli
mes
befo
reth
eS
upie
me
Cou
rt(a
ndm
any
US
Cou
rts
olA
ppea
ls)
and
she
com
pany
’sju
dici
alfo
rtun
essu
ffer
edaf
ter
hele
ft,no
tto
men
tion
hs
boss
gett
ing
fire
d,
NY
Cis
too
expe
nsiv
eto
bejo
bles
san
dst
ifl
pay
rent
.N
otw
amti
ngto
die
hom
eles
sin
NY
C
He
took
CO
BR
A.
Itw
asja
w-d
ropp
ingl
yex
pens
ive.
He
look
edfo
ra
new
job.
Age
disc
nmin
atio
nis
real
.P
rosp
ecti
veem
ploy
ers
expl
aine
dth
eyco
uldn
’tpa
yhi
mw
hat
hew
asw
orth
and
they
knew
he’d
ump
ship
ifth
eyof
fere
dw
hat
they
coul
daf
ford
Nev
erm
ind
that
NY
Cis
too
expe
nsiv
eto
bejo
bles
san
dsti
llpa
yre
nt.
Not
wan
ting
0di
eho
mel
ess
inN
YC.
John
nycu
tba
ckon
his
expe
nses
,be
gan
spen
ding
hs
savi
ngs,
took
Soci
alSe
curi
tyea
rly
—an
dth
en,
afte
rge
ttin
ga
phys
ical
,dr
oppe
dhi
she
alth
insu
ranc
e
Aft
erth
eco
lono
scop
y,w
ear
gued
agai
n.T
heG
Ido
ctor
wan
ted
tosc
hedu
leim
med
iate
surg
ery.
“Sur
gery
!H
ell,
not”
tmet
him
afe
wda
ysla
ter
inth
elo
bby
ofN
YPr
esby
teri
an,
‘Sam
!H
ell,
no,’
kept
him
com
pany
for
she
hour
ofpr
e.su
rger
yw
aitin
g,an
dhu
ngou
tin
the
fam
ilylo
unge
—w
onde
ring
why
a45
’min
ute
proc
edur
ew
asta
k’ng
2+ho
urs.
“Cob
rais
eati
ngm
yre
tire
men
tm
oney
!”T
hen
his
surg
eon
arnv
ed,
look
ing
sad,
He’
dre
mov
eda
“mas
sth
es’
reof
ala
rge
lem
on.”
John
nyha
dS
tage
IVco
lon
canc
er.
Mul
tiple
doct
ors
built
ap!
an.
John
nyw
assc
ared
and
said
hew
ould
do“w
hate
ver
itta
kes
:
Six
mon
ths
late
r,af
ter
man
yro
unds
ofch
emo,
whi
chhi
son
colo
gist
kept
sayi
nghe
’d“f
aile
d,’
John
nybe
cam
ede
pres
sed:
itw
ash:
s“f
ault’
hew
asn’
tbe
sser
.Jo
hnny
,w
ho’d
aced
ever
yle
sthe
’dev
erta
ken,
final
lyca
me
toliv
ew
ithm
ebe
caus
ehe
’dfa
iled.
Igot
his
com
pany
and
wit
and
insi
ght,
whi
lehe
got
lood
and
car,r
,g.
Jthnry
d,ed
aye
a’ah
erth
atp
hy
cal,
And
,no
,no
tbe
caus
ehe
’d“f
aile
d.’H
esh
ould
n’t
have
died
.
Had
John
ny’s
canc
erbe
endi
agno
sed
bya
colo
nosc
opy
afS
tage
0or’
,he
mig
htw
ell
beal
ive
toda
y.E
ven
diag
nose
das
Srag
e2
or3,
hem
ight
wel
lbe
aliv
e:S
tage
3Aha
sa
S’ye
arsu
rviv
alra
teof
abou
t90
%,
Imis
sm
ybr
othe
rJo
hnny
,(k
now
hesh
ould
n’t
have
gone
thre
eye
ars
wis
hous
seei
nga
dono
r.Ia
lso
know
hew
ould
n’t
have
been
able
toaf
ford
all
the
trea
tmen
the
got
with
out
heal
thin
sum
nce.
No
one
shou
lddi
ebe
caus
ese
eng
ado
ctor
coul
dle
adto
bank
wot
cy.
FJed
,car
e,ev
enw
ithits
gaps
arid
flaw
s.is
ag
od
srn
dfo
rth
ose
over
65.
We
all
need
“Im
prov
edM
edic
are
for
All
New
Yor
kers
,”NY
Hea
lth,
whi
chw
illsa
veus
mon
ey,
cove
rus
all
—an
dke
epbr
othe
rslik
eJo
hnny
aliv
ean
dsh
rivin
gde
cade
slo
nger
.
Jaha
nna
Bar
dm
oum
iny
she
45,0
00,4
men
cans
who
,fil
mJo
hnny
,di
apr
emat
urel
ybr
caus
eof
rati
oeth
heal
thca
re,
adro
raie
sfo
rN,v
rkH
ealt
han
dSe
a!:h
iust
ice.
Sur
pris
elIt’
sa
hosp
ital
bill!
Ele
ven
p.m
.on
aSa
turd
ayni
ght.
My
wif
ean
dIw
ere
retu
rnin
gho
me
from
ara
reev
enin
gou
t,m
ade
poss
ib!e
byou
rch
ildre
nbe
ing
away
ata
sum
mer
cam
pne
arSi
dney
,NY
.It
had
been
asu
cces
sful
even
ing:
vie
had
disc
over
eda
Mor
occa
n-Is
rael
ica
féon
the
Upp
erW
est
Side
ERdoct
ors
are
eng
aged
bypr
ivat
eco
ntr
act,
the
hosp
ital
told
me
As
soon
atre
ew
alke
d‘n
the
door
,th
ete
leph
one
rang
.It
was
she
russ
ofr
omca
mp
Our
son
was
OK
,se
hurr
ied
inas
sure
us,
but
heha
din
jure
dhi
sfi
nger
and
she
nurs
ew
asas
king
for
our
perm
issi
onto
take
him
toth
eER
ofth
elo
cal
hosp
ital.
Nat
ural
lyw
eag
reed
:Si
dney
is12
5m
iles
and
ath
ree’
hnur
driv
efr
omsh
eB
ronx
,it
wou
ldha
rdly
mak
ese
nse
tobr
ing
our
son
all
the
way
hom
eto
see
ado
ctor
.T
heca
mp
had
our
fam
ilyhe
alth
insu
ranc
ein
form
atio
n,an
dth
eho
spita
lac
cept
edou
rin
sura
nce.
Our
son’
sfi
nger
was
spra
iree
bul
not
brok
en;
isw
asta
ped
and
hew
eet
back
soca
mp.
Mat
ter
clos
edO
rso
isse
emed
,un
tilw
ego
sa
bill
for
$400
from
the
ERd
on
or
(Thi
sw
asin
addi
tion
toth
eco
’pay
men
fto
the
hosp
itaL
!
Itse
ems
the
hosp
.tal
acce
pted
our
insu
ranc
e—
but
she
doct
ordi
dno
t-T
his
isso
met
hing
1co
uld
nor
have
imag
ined
until
Iexp
erie
nced
it,Is
n’t
the
doct
oran
inse
para
ble
pan
ofsh
eho
spit
al?
I ask
edbo
thth
eho
spita
lan
dth
eca
mp
coun
selo
rw
hoac
com
pani
edm
yso
nfo
rde
tail
sof
wha
tsh
edo
ctor
did
tous
tify
this
bilt.
From
wha
tIw
asab
leto
dete
rmin
e,th
edo
ctor
spok
ew
ithm
yso
nbr
iefly
,te
nthi
mfo
ran
x’ra
y,lo
oked
atth
ex’
ray
resu
lts,
and
band
aged
his
fing
er.
At
mos
t,th
edo
ctor
may
have
spen
t5
min
utes
onth
isca
se.
Let’s
see:
5m
inut
esat
£400
—th
at’s
ara
teof
$4,R
00pe
’ho
urN
osba
d;ev
enm
ote
than
a‘s
ir/e
r,It
h:nk
.
Eve
ryon
ew
hoco
mes
into
the
hosp
ital
has
tobe
seen
byth
edoct
or
ondu
ty
Iask
edfh
eho
spita
lw
hy,
ifth
eho
spita
lac
cept
edm
yin
sura
nce,
‘rec
eive
da
bill
rem
the
doct
or.
ERdo
nors
are
enga
ged
bypr
ival
eco
ntra
cf,
the
hosp
ital
told
me,
sepa
rate
from
the
hosp
ilal’
sot
her
care
give
rs.
Ifth
edo
ctor
isno
tpa
rtof
the
hosp
ital,
task
ed,
why
coul
dn’t
my
son
bese
enby
anu
rse?
Aft
eral
l,th
ere
was
noth
ing
abou
thi
sca
sean
RNco
uld
not
take
care
of
The
hosp
ital’
sre
ply:
Eve
ryon
ew
hoco
mes
into
the
hosp
ital
has
tobe
seen
byth
edo
ctor
ondu
ty.
Inot
her
wor
ds,
the
hosp
ital
was
havi
egit
both
way
s-T
hrou
ghfu
rthe
rre
sear
chId
isco
vere
dth
attw
oco
rpor
atio
nsow
nal
mos
taf
Ith
em
edic
alfa
cilit
ies
ina
vast
area
ofce
ntra
lN
ewY
ork
Stat
e.
Sinc
eth
enth
est
ate
pass
eda
law
iequ
idng
hosp
ilal
sto
info
rmpa
tien
tsof
thei
rbi
liing
prac
tice
s,so
paL
en!s
wou
lden
sge
t‘s
urpr
ise’
bills
.
flu!
the
stat
ed’
dro
tou
tlaw
the
prac
tice
ofbi
llir
gse
para
tely
for
the
doct
orSo
Igue
ssw
eca
nco
wst
art
figs
inng
out
how
we’
llpa
yth
ebi
llfo
rou
ri!’
ness
be’o
rew
ear
ecu
red.
Ido
not
keow
ifsh
ela
wre
quir
esho
spita
lem
ploy
ees
toex
plai
nth
eir
billi
ngsy
stem
befo
reth
eyst
art
trea
ting
som
eone
who
com
esin
with
ahe
art
atta
ck,
And
ifth
epa
tien
tis
unco
nsci
ous,
doth
eyha
veto
expl
ain
itri
ght
away
ordo
they
wai
tun
tilth
epa
sien
tha
sre
gain
edco
nsci
ousn
ess?
“Per
vers
e”is
not
too
stro
nga
wor
dto
desc
ribe
this
hea
lthca
re“s
yste
m”
And
ofco
urse
,w
hen
you
have
ase
tiou
sem
erge
ncy
whe
reev
ery
min
ute
coun
ts,
you’
reno
tgo
ing
tooo
toa
hosp
ital
fart
her
away
beca
use
it’s
chea
per,
are
you?
‘Per
vers
e’is
not
too
stro
nga
wor
dto
desc
ribe
th;s
heal
thca
re‘s
yste
m.’
No
one
will
die
wai
ting
for
Med
icar
e.5
14
Ikno
whe
shou
ldn’
tha
vego
neth
ree
year
sw
itho
utse
eing
ado
ctor
He
figu
red
he’d
beon
Med
icar
ew
ithin
3ye
ars.
He
ratio
naliz
edth
athe
’dof
ten
gone
year
sw
ithou
ta
phys
ical
.“N
othi
ngba
dha
ppen
edth
en:
noth
ing
bad
will
happ
enno
w,
And
CO
BR
Ais
eati
ngm
yre
tire
men
tm
oney
!”
He
bega
nha
ving
dige
stio
nis
sues
,bu
tpu
tof
fse
eing
ado
ctor
beca
use
heco
uldn
’taH
ord
anys
h’ng
expe
nsiv
e—
and
“Med
icar
ew
illk,
ckin
soon
,an
dco
ver
wha
teve
rth
eyfi
nd—
and,
mor
elik
ely,
wha
tese
rth
eydo
n’t
find
,do
ing
load
sof
expe
nsiv
ete
sts
“Med
icar
ew
illki
ckin
soon
”
The
nhe
turn
ed65
and
got
his
Med
icar
eca
rd,
His
phys
icia
nha
dre
tired
,so
find
ing
ane
won
eto
oktim
e,H
eca
lled
afte
rth
eap
poin
tmen
tso
com
plai
nth
atth
ene
wgu
yw
asin
sist
ing
ona
colo
nosc
opy.
“whi
chso
unds
nast
y,”
We
argu
ed,
He
mad
eth
eap
poin
tmen
t,
Ron
Weg
sm.n
isa
nonp
rofit
raec
usiv
ean
da
fong
iime
,esi
drnt
ofK
ings
brid
gean
dR
isei
da!e
.
No
surp
rise
bills
,no
cost
sat
po
int
of
serv
ice.

Delays
Updating
Insurance.B
arelyE
scapedB
ankruptcyerrifying
Nightm
ares:“M
yW
ifeW
illB
eH
omelessl”
Thisisa
storyof
howM
argaietalm
ostlost
herlife.
Our
livestogether
areso
intenwined
Icannottell
herstory
without
tellingnine-
Itbegins,
innocentlyenough,
with
Iwo
mistakes.
First,only
oneof
usgot
aflu
shot:m
e.M
argaretIhooght
diedidn’t
needit,
becauseshe
iravelsto
seefam
ilyna
warm
erclim
ate.S
econd. we
hadtrouh’e
updatingour
healthinsurance
becausew
ew
anteda
ointpo:cy
andthen
thoughtw
enad
missed
thew
indowfor
enrollment.
Our
storybegan
lastFebruary
when
my
w.fe
fellterribly
ill.A
fterIposted
aboutit
onF
acebook.as
aw
ayof
keep
ng
myself
saneand
gettingsupport
fromfriends,
apnysicisn
friendIhadn’t
seens:nce
aItS
reunion,20
yearsearlier,
recomm
endedIget
anoxim
eterso
checkM
argaret’sblood
oeygen.H
etold
me
thatifis
fellbelow
90%,
togel
herto
theem
ergencyroom
byam
bulance,
Her
blo
od
oxygen
was
85
%...
73
%39%
...
her
carelikely
cost
over
halfa
million
do
llars
Itw
as85%
.Ihustled
herinto
thecar
toour
localER.
Shew
ashaving
troublew
alkingeven
afew
steps.By
thetim
ethe
ERtniaged
her,her
oxygenw
as73%
—
andthey
hustledto
administer
oxygenin
variousand
successivelym
oreintrusive
ways.
At
3am,
shew
asstill
consciousand
toldm
elo
go
home,
that
the
osy
gen
mask
was
working.
At
lam,
when
I returned,the
ERcoordination
physiciantold
me
sheneeded
lobe
puton
anEC
MO
machine
—w
Inchrem
ovesthe
bloodfrom
anartery
inthe
neck,oxygenates
it,end
returnsitdirectly
sothe
hears.The
ECM
Ois
theH
ailM
arylass
resortfor
breathingissues
thisserious.
Imagine
howI fell,
hearingthat
thism
achinew
asher
onlychance,
thatm
yhospital
didn’thave
onefonly
afew
hospitalsdo),
andthat
thew
asfar
tootick
totravel.
Her
bloodosygen
was
39%.
Our
coordinatingphysician
arrangedfor
Monteliore
Hospital
tosend
ateam
of8
(surgeon,nurses,
technicians),w
hoarrived
within
thehour
andperform
edthe
surgeryw
iththe
machine
theybrought.
The
surgerylook
about90
minutes.
As
sheE
CM
Obegan
tow
ork,she
was
upto
45%,
andthat
was
thebeginning
ofher
longjourney
back.
Margaret
went
throughso
much:
oxygendepivalion
harmed
herheart,
brain,kidneys
andother
organs.She
was
inthe
ICUfor
aw
eek—
beingw
atchedby
two
nurses24/7
—and
ina
coma
fora
month.
Although
everso
much
benernow
,she
hasnot
fullyerovered
andtires
easily.M
argaieslost
herob,
andthis
new
pre.ex
issing
tondL
lion
mak
estied
ing
anew
jobch
allengng.
Com
pan
iesare
reluctan
tto
hirean
yo
ne
likelyto
inuw
xse
lhe.r
insu
rance
costs
Bet,
than
ks
toth
atnag
calm
achin
ean
dtruly
ded
:catedd
octo
rsan
dnurxes
fromco
ohosp
itals,m
yw
ifelees.
Marg
are
tlo
st
her
job,
and
this
new
pre
-existin
gconditio
nm
akes
find
ing
anew
job
challe
ngin
g
Now
forthe
insurancepan.
equallyscary
andw
ithan
equallyhappy
ending.A
dono
rto’d
me
hercaie
t.kelycost
overhalf
am
illiondotxrs.
Fee!:ngiN
myself,
Ihadtried
toapoly
onlinefor
ouro.nl
insurancepolicy.
andhad
gonensw
&w
iththe
forms
sincetw
opolicies
hadto
become
one.T
hen,during
theheight
ofher
illness.Iforgot
tofollow
through.Is
tookm
anycalls
iohe
NY
CH
ealthD
epartment
befove,eached
anagent.
who
fcundour
intialapplication
andallow
edus,
first.to
activatethe
loal
policyand,
second,dale
itback
1°m
yinitialapplication.
The
kindagent
toldm
esve
had1
daysto
make
theale
payment
forFebruary
beforeour
coveragew
ouldbe
cancelled.
We
mig
ht
hav
elo
stev
ery
thin
g—
bu
t
for
the
graceof
onevery
kindarid
patie
nt
NY
SH
Dagent
Imade
thepaym
ent—
alarge
sumfor
us—
andw
ew
eresaved. 1
en
I thinkofw
hatm
ighthave
been.A
ftalf.million.dollardebt
would
haveruined
us.We
might
havelost
everything—
butfor
thegm
ceof
onevery
kindand
patientN
I’SH
Dagent
who
tookthe
lime
tofind
ourfile,
understoodour
situarion,and
made
allthe
coveragehappen.
Ifeel verylucky
indeed,
Iamthe
executivedirector
for anagency
thathelps
homeless
people.providing
shelterand
advocatingfor
affordablehousing
forallN
ewY
orkers.Ironically,the
poorand
homeless
inN
ewY
orkreceive
quiteadequate
camfrom
Medcaid,
butcalamity
almost
tookm
yw
ileand
my
futum—
asudden,
unexpectedhealthcam
calamity, from
which
my
belovedand
I barelyescaped.
NYH
ealthw
ouldhave
preventedm
anyofthe
anxiely.causingaftereffects
ofmy
wife’s
illness.
George
Gross
si execmire
directordan
eteda,thagency
thatad
uocales
forthe
homeless
eN
YC
.
No!
Nol”
my
husband’snightm
ares—
vividchim
erasabout
hism
edicalhills
leavingm
ebankrupt,
without
ahouse,
food,or
safely—
spikedhis
heartrate
andblood
pressure,tngge’ed
alerts,caused
medical
staffto
raceto
hisbed
sde.
They
wou’d
findm
etrying
tow
akehim
toreality,
ashe
grippedm
yhands
gatping,‘A
reyou
sureall
thisit
covered?I can’t
havethre
treatment
.fyou
wont
besafe.’
V/hen
fullyaw
ake,M
ichxelknew
hew
aslucky,
with
Cadiilac’
insurance.D
espitetrus,
we
tegulartygot
billedfor
thousandsof
doilarsO
verfive
years,Ioften
made
callso.sputing
bills:he
was
toosick
local1.
My
hu
sban
dw
orried
about
need
ing
tob
orro
wm
oney,ab
out
dyingbefo
red
ispu
tesw
erereso
lved
Som
etimes
I heardm
issing‘prior
suihorirations,’or
hs
cardnum
berhad
beenre,ected
orinsuranre
hadpaid
Xdollars
andhe
stillow
ed35<.T
henIw
ouldcal
‘benefitsand
beput
onbold,
I stento
music,
geltransferred
around,constanliy
askedfor
me
same
numbers
anddates,
Michael
would
listenfrom
hisbed,
whispering
worned
questions.Per
hisinstructions,
Ikept
anotebook
ofevery
phonenum
berand
personI
talkedto,
andeverything
theysaid.
When
I’dfinally
getthrough
toa
benefitsperson
who
couldhandle
hispolicy,
I’dheat
itwas
coveredbut
thedoctor,
thehospital,
thelab
hadfiled
thew
rongpapenvork.T
oom
anytim
esto
count,w
ereceived
lettersfrom
collectionagencies,
threateninglaw
suits,describing
punitivefinance
charges,w
ritingreally
scarythings.
I respondedto
thesein
writing:
“The
billis
indispute.
Return
itto
theprovider
imm
ediately.”
I always
feltterrib
lew
hend
octo
rs(and
nurses)sp
ent
time
defen
din
gm
edicaldecisions
when
they
need
ed(and
wan
ted)
tosp
end
time
with
patien
ts
My
husband,a
faviryer.would
dictateand
signthese
letters,to
heknew
howm
anydisputes
were
inplay
—
endtheir
repercussions.A
ftersending
theletter,
I would
phonew
hoeversent
thebill
tocollection,
andw
asusually
toldit
hadbeen
sent‘in
ecor.”
My
husbandw
orriedabout
needingto
borrowm
oney.about
dyingbefore
disputesw
ereresolved.
When
home,
hew
aseligible
forv,siling
home
healthcare:each
newperson
requireda
new‘intake
form,’
sometim
eslastng
2hours
orm
ore.Som
eof
them,
heanivss!y,required
himto
answer
everyquestion,
becausehe’s
thepatient,
notyou.’
His
insurershad
noqualm
sab
out
over-rulinghis
doctors’d
iagn
oses
andp
rescriptio
ns
Never
mind
thathe
was
drugged,exhausted,
tootick
torem
ember
everym
edicationor
me
name
andphone
number
ofevery
doctorV
.’o,se,aher
everyhospitalization,
thisintake
formhad
tobe
doneanew
—there
was
now
ayso
carryany
information
overbecause
‘thingshave
changed.’N
othey
hadn’t.T
hem
a,orchange
was
always
thedale.
UIt.m
ately,M
ichael’scare
was
‘tree’—
andw
ew
ereso
gladto
getgood
careand
tohate
itcovered—
butit
was
norw
;thoulcost
som
anyletve,t,
notebooks,and
hoers,so
much
effortand
stresshe
couldhave
spenthealing.
His
insurershad
noqualm
sabout
ov
erruling
hisdonors’
diagnosesand
prescriptions.H
isdoctors,
nurses,and
hospitalinsurance
administrators
allspent
hourson
thephone
andcom
puterstrying
toget
approvalsand
permissions,
checkingbilling
codesand
FDA
sites,persuading
bureaucrats.
I always
feltterrible
when
doctorsfand
nurseslspent
lime
defendingm
edicaldecisions
when
theyneeded
(andw
anted)to
spendtim
ew
ithpatients.
The
hasslescaused
byhis
Cadillac
insurancem
adelife
almost
asgm
esome
ashis
illness.B
utIknow
hegot
superbcare
despitefor’pm
fi trnsurance,N
OT
becauseof
it.
All
ofus
needa
simpler,
more
user.friendly,less
costlypaym
entsystem
.It’s
onereason
why
single.payerN
YH
ealthw
illbe
better
Donors
will
diagnoseand
prescribeaccording
toevidence.based
protocolsdefined
bydoctors
—and
getpaid,
promptly.
All
thetim
enow
spentarguing?
New
lyavailable
forpatient
care.A
ndm
ydarling
husband—
andyour
lovedones
—w
on’tw
onyabout
bankruptingtheir
families,
orleaving
themhom
elessbecause
ofunpaid
medical
bills.T
heycan
concentrateon
gettingw
ell.
JudithU
ebenlost
herhusband
after580
days0f
hospiralizaiion.In
hishonor,
sheadrosates
forN
VH
ealth—
toelim
inatefinancial obstacles
tohealthcare
forall
New
Vortem
.
Au
tom
aticen
rollm
ent
inth
ebest
plan,alw
aysth
ere.13
Loved
onescan
focuson
healing,notfearing
homelessness.

Got
Sick
.L
ost
Job.
Los
tIn
sura
nce.
Hag
gled
for
His
Life
Sud
den
Chr
onic
Illn
ess.
For
mul
ary
Hel
l.W
illIS
urvi
ve?
IIa
imos
tti
edel
even
year
sag
o.In
itial
ly,
Ihad
ajo
bw
ithin
sura
nce
but
illne
ssco
stm
em
yjo
b.L
osin
gm
yta
bco
stm
em
yin
sura
nce-
Not
bein
gab
leto
affo
rdhe
alth
care
alm
ost
kille
dm
e.M
yst
ory
isa
vici
ous,
like
-thr
eate
ning
cycl
e.I’v
ele
arne
dth
athu
ndre
dsof
thou
sand
sof
Am
sric
ans
have
sim
ilar
stor
ies.
now
my
job
didn
’tin
clud
ehe
alth
insu
ranc
e.N
otal
ljo
bsdo
,ev
enso
me
that
recr
uit
you
wit
hpr
omis
esof
heal
thin
sura
nce
Afe
wye
ars
earl
ier,
Ihad
my
first
epis
ode
ofbi
liary
du
nob
stru
ctio
nan
ddi
dn’t
gel
sosi
ck.
My
insu
ranc
eco
mpa
nypa
id$1
,500
for
ach
olec
yste
ctom
yan
d,af
ter
wee
ksof
reco
very
,Iw
asal
mos
tba
ckto
norm
al,
livin
gm
yl,t
ean
ddo
ing
my
job,
but
now
my
job
did
nt
incl
ude
heal
thin
sura
nce.
Not
all
jobs
do,
even
som
eth
atre
crui
tyo
uw
ithpr
omis
esof
heal
thin
sura
nce.
Soth
ere
Isva
sel
even
year
sag
o,w
oik:
ngev
ery
day.
The
nI g
otre
ally
sick
—in
tens
ebl
oatin
g,ja
undi
ce,
afa
natic
alitc
h’ng
that
kept
me
from
slee
ping
far
four
mon
ths.
Itw
asco
nsta
ntev
ery
hour
ofev
ery
day.
Nonst
op
.Iw
asin
such
mis
ery.
Ilos
tw
eigh
t.Iw
asha
llow
edojr
.
One
fnen
dsa
idIl
ooke
dlik
ea
“dea
dm
anw
alki
ng.”
The
hosp
ital
told
me
$20,
000
br
the
sam
etr
eatm
ent
they
’dch
arge
dsh
ein
sure
r$1
,500
for
afe
wye
ars
earl
ier.
I was
dum
bfou
nded
.W
hyw
asth
eca
stso
high
for
me
whe
nIn
olo
nger
had
heal
thin
sura
nce?
$1,5
00w
ould
have
been
diff
icul
t,bu
s$2
0,00
0w
asun
imag
inab
le.
Iwon
dere
d,sh
ould
tjus
tgi
veup
and
die?
S20
,000
was
unim
agin
able
...S
houl
dI j
ust
give
upan
ddi
e?to
ldth
eho
spita
lad
min
istr
ator
that
the
grav
e“a
sbe
ckon
ing
sinc
eId
idn’
tha
ve$2
0,00
0.S
ud
den
lth
epr
ice
beca
me
513,
800.
This
was
st:ll
anun
imag
nabl
esu
m,
but
Ifoe
ndit
inco
ncei
vabl
eto
beba
rgai
ning
for
my
life.
Was
Iin
apa
ralle
ln
,vrs
e
I dis
soci
ated
:fr
omth
ein
side
Iwas
tern
fied
and
mis
erab
le;
from
she
outs
ide
Icou
ldn’
tfa
thom
she
absu
rdity
.C
anyo
uim
agin
eba
rgai
ning
for
your
life
the
way
you
hagg
lefo
ra
used
car’
I was
inca
psta
nsitc
hing
agon
yan
dco
uldn
’tfa
thom
how
$15K
coul
dbe
com
e52
0Kco
uld
beco
me
5135
K.
As
Itur
ned
yello
wer
and
yello
wer
over
the
wee
ks,
the
pric
efi
naty
drop
ped
to5
8,0
00
—rd
r.eg
osia
sed
the
pnce
ofm
yow
nlif
edo
wn
65%
.lv
this
free
-mar
ket
heal
shca
re?
Isth
isbe
ing
asa
ny
heal
thca
reco
nsum
er?
Iwas
n’t
tryi
ngto
bea
good
capi
talis
t,m
uch
less
akn
owle
dgea
ble
cons
umer
Isim
ply
wan
ted
tosa
vem
ylif
e,bu
tIF
elt d
emea
ned.
This
isw
hyI s
uppo
rtN
YH
ealth
—Im
prov
edM
edic
are
for
All
New
Yor
kers
,
Onl
yin
the
U.S
.do
heal
thca
reco
sts
lead
tofi
nanc
ial
turn
,ba
nkru
ptcy
,or
deat
h.Ev
ery
othe
rde
velo
ped
coun
try
has
univ
ersa
lhe
alth
care
;ev
eryo
neis
cove
red:
lack
ofw
ealth
does
n’s
prev
ent
care
Abo
ut45
.000
Am
eric
ans
die
each
year
beca
use
cost
prev
ents
life-
savi
ngm
edic
alca
re
Iwas
n’t
tryi
ngto
bea
good
capi
tali
stIs
impl
yw
ante
dto
save
my
life
Even
with
insu
ranc
e,h:
gh.d
olta
rde
duct
ible
ske
eppe
ople
from
early
,ea
sily
trea
tabl
edi
aqno
ses
kMie
not
hers
,al
soin
sure
d,ge
tse
riou
sly
ill,
pre’
auth
onza
tion
dela
ysan
dbe
nefi
tde
nial
sfo
rce
them
tofa
ceru
inou
sou
t-of
-poc
ket
cost
s,M
any,
like
me
with
out
muc
hsa
ving
s,no
tw
antin
gto
impo
veri
shou
rfa
mili
es,
fore
got,
eatm
ent
—an
ddi
e.
NYH
ealth
will
rem
ove
knan
cial
obst
acfe
sro
care
,If
you
lose
your
job
beca
use
ofill
ness
,yo
u’ll
still
beab
leto
see
ado
ctor
and
get
trea
lmen
t.
Man
y...
not
wan
ting
toim
pove
rish
our
fam
ilie
s,fo
reg
otr
eatm
ent
—an
ddi
e
You
won
’tev
erhe
arth
atyo
une
edto
find
$20,
000
—
or$1
3600
,or
$8,0
00or
even
$1500—
for
aro
usin
epr
oced
ure
that
prev
ents
deat
h.W
hen
you
have
ajo
b,yo
u’ll
pay
apr
ogre
ssrv
esa
x.If
you
lose
shas
oh,
you
won
’tlo
sehn
alth
cam
You
rch
ildre
nw
on’t
lose
met
heal
thca
re;
they
’ll
beco
vere
dbe
caus
eth
eyre
child
ren.
ram
iles
will
wor
ryab
out
love
don
esge
ttin
gbe
ner,
not
abou
tgo
ing
brok
e.
Waf
ter
carp
ente
rco
cks
e,th
eto
uris
t ind
ustry
and
now
advoca
tes
ever
yda
yle
t sin
gle’
paye
’N
a’H
A
This
stor
ym
ayno
tha
vea
happ
yen
ding
beca
use
my
insu
ranc
eco
mpa
nyis
deny
ing
prio
rau
thor
izat
ion
for
am
edic
ar:o
nm
yd
oct
or
wan
tsm
eto
hav
e.M
ydoct
or
isar
guin
gas
sidu
ousl
yon
my
beha
lf—
but
turn
out
succ
ess.
Bus
let
me
begi
nat
the
begi
nnin
g.
I am
very
activ
e-Ir
un,
wal
k,bi
ke,
doY
oga,
eat
heal
thily
and,
until
Pass
over
of20
10,
cons
ider
edm
ysel
fen
tirel
yhe
alth
y.A
sm
yfr
iend
san
dco
llea
gues
can
test
ify,
noth
ing
ssop
sm
e.B
utdu
ring
she
holid
ay,
Isud
denl
ybe
cam
eill
.Ih
adun
cont
roll
edre
ctaf
blee
ding
,di
arrh
ea,
bad
cram
ping
and
sore
mus
cles
,no
sto
men
tion
seri
ous
head
ache
and
chill
s,Ir
emem
ber
suff
erin
grh
roug
hsh
efir
stpa
rtof
the
eigh
t.da
yev
ent
with
anun
cont
roll
able
blad
der,
emba
rras
smen
tan
dpa
in.
At
the
time,
my
fam
ilyha
dbe
enat
tend
ing
Cha
bad
ofR
iver
dale
.
The
Rab
bi’s
fath
er.in
.law
was
ave
ryki
ndan
dse
ason
edph
ysic
ian.
He
diag
nose
dm
eaf
ter
serv
ices
one
day
and
was
conc
eine
d.H
esa
idIn
eede
dIn
get
test
ed.
His
revi
ewof
my
sym
ptom
san
ddi
etsu
gges
ted
som
eki
ndof
low
erin
test
inal
mal
ady.
Ihad
neve
rbe
enre
ally
wck
befo
rear
dso
this
all
cam
eas
ash
ock.
The
appoin
tmen
tsto
okfo
reve
r,th
eco
sts
sky-
rock
eted
,an
dth
em
eds
wer
ein
effe
ctiv
e
Aft
ersh
eho
liday
Ibeg
anse
aich
ing
for
aG
l.I r
ecei
ved
man
yre
ferr
als.
Ala
rge
loca
lpr
actic
edi
agno
sed
me
with
ulce
rativ
eco
litis
fOCI
,an
inlla
mm
ator
ybo
wel
dise
ase
that
mai
nly
affe
cts
the
linin
gof
the
larg
ein
test
ine
(col
on).
This
auto
imm
une
dise
ase
has
are
laps
ing-
rem
itti
ngco
urse
,w
hich
mea
nsth
atpe
riod
sof
flar
e’up
sar
efo
llow
edby
peri
ods
ofre
mis
sion
.
Nea
rly
one
mill
ion
peop
lesu
ffer
from
this
dise
ase.
At
the
mom
ent,
ther
e’s
nom
edic
alcu
refo
ruc
.R
adic
alsu
rger
yca
uses
othe
rpr
oble
ms.
From
day
one,
the
illne
ssw
asdi
ffic
ult
for
me
The
appo
intm
ents
look
fore
ver,
the
cost
ssk
yroc
kete
d,an
dth
em
eds
wer
ein
effe
ctiv
e.T
hedo
ctor
sne
ver
real
lyli
sten
edto
my
com
plai
nts
orha
den
ough
time
real
lyto
help
me
get
sow
here
Icou
ldbe
.
Aft
ertw
oye
ars,
six
(rat
es,
and
thre
eco
lono
scop
ies,
Iwas
tota
llym
iser
ab’e
,M
yen
t,re
body
beca
me
infl
amed
:an
kle
swel
ls,
back
pain
and
ches
tm
uscl
efl
ares
and
pain
.Ie
ndur
edw
eigh
tsw
ings
,lo
sing
ISpo
unds
,th
enbl
oati
ngan
dbi
gw
eigh
tga
ins.
Mos
tim
port
ant,
my
GH
Iin
sura
nce
does
rot
cove
rth
ebe
stm
edic
ines
,w
h,ch
are
very
expe
nsiv
e.
On
my
sala
ryan
dw
ithfa
m’ly
obli
gati
ons,
Ican
not
affo
rdm
ed,c
atio
nsth
aIm
ight
help
me
mor
eth
anth
eon
esIa
mon
.L
eso
man
yot
hers
with
Iong
-las
:ino
cond
itio
ns,
Iam
slnc
ken
both
byth
eill
ness
and
byits
incr
easi
ngfi
nanc
ial
buid
en:
avi
ciou
sci
rcle
beca
use
ansi
esy
incr
ease
ssh
esy
mpt
oms.
Our
heal
thsy
stem
mak
esch
roni
che
alth
diso
rder
sdi
ffic
ult
totr
eat
—bec
ause
insu
ranc
edo
esn’
tco
ver
the
opti
mal
trea
tmen
t
Iam
also
unha
ppy
atth
eim
pact
the
UC
has
onm
yin
depe
nden
cean
dm
obili
ty.
Dur
ing
flar
es,
fhav
eto
know
the
loca
tion
ofev
ery
rest
room
inth
eC
ity.
Iam
tem
fied
ifIg
eta
cram
pan
dm
ust
use
faci
litie
sin
neig
hbor
fsoo
dsw
ithno
publ
icto
ilet.
As
aco
mm
unity
soci
alw
orke
rw
hotr
avel
sa
grea
tde
al,
Ierp
esie
nce
the
toll
ofa
d:se
ase
whi
chaf
fect
sm
yen
ergy
leve
l.
Our
heai
thsy
stem
mak
esch
roni
che
alth
diso
rder
sd,
H:c
ult
totr
eat
—be
caus
ein
sura
nce
does
n’t
cove
rth
eop
timal
trea
tmen
tT
hose
w,t
hch
roni
cd,
seas
esan
dw
ithou
tin
funi
tefi
nanc
ial
reso
urce
sm
ust
cont
inue
tosu
ffer
unex
pect
edfi
are.
ups.
One
wat
ches
adve
rtis
emen
tsfo
rm
irac
lecu
res.
like
the
one
for
Hep
atiti
sC.
whe
reth
eco
urse
oftr
eatm
ent
is$9
4,00
0,an
don
ew
onde
rs,
even
ifth
ere
isa
cure
for
UC
,w
illI
beab
leso
affo
rdis’
“Lit
tle
mor
eth
an1
per
cent
ofG
DP
assi
gned
tohe
alth
coul
dco
ver
ital
l,”-U
we
Rei
nhar
dt
we
need
big
phar
ma
tow
ork
for
us,t
osto
psp
endi
ngon
esh
irdof
itsbu
dget
onad
vert
isin
g,an
dto
beab
leto
nego
tiat
efa
iran
deq
uita
ble
pric
esso
that
all
Am
eric
ans
can
have
the
righ
tto
good
heal
th.
We
need
ahe
alth
syst
emth
atw
illke
epus
heal
thy
ata
pric
ew
eca
nal
laf
ford
.
As
heal
thca
wec
onom
ist
Um
eR
einh
ardt
argu
ed:
“The
issu
eof
unis
ersa
lco
vera
geis
not
am
asiw
ofec
onom
ics,
bole
mor
eth
an1
perc
ent
ofG
OP
ass’
gned
tohe
alth
coul
dco
’,’er
itall
-It
isa
mat
ter
ofso
sif:
Dav
idK
napp
dire
cts
apr
ogra
m(u
nder
the
ausp
:ces
ofth
eN
YC
Dep
anrn
ent
ofA
ging
)to
assi
stol
der
adul
tsto
tsr
aide
pend
enrf
y
You
’llne
ver
hagg
lefo
r you
rlif
e,lik
eyo
uha
ggle
for
aca
r.12
Dru
gpr
ices
will
nolo
nger
extr
act
exto
rtio
nate
prof
its.

Em
ployer-Based
InsuranceT
hreatensM
ySon’s
LifeM
Y’SM
ost
At-R
iskP
op
ulatio
n:
Un
derserv
ed
My
nine’year-o!dson
despeiaselyneeds
NTh
topass
sheN
ewY
orkH
ealthA
ct
Sevenyea’s
ago,m
yperfectly
healthyand
typraity
developingalm
ost’three’year.oldson
woke
uphaving
aseizure.
He
was
admitted
toLair
neighborhoodhospital
where
overthe
nextsteak
anda
halfw
ew
atchedhim
losehis
abilityto
walk,
talk,sw
allow,
focushis
eyes,and
reliablybreathe,
He
was
eventuallydiagnosed
with
anti’NM
DA
receptorencephalitis.
When
my
husbandw
aschanging
lobs,
moving
ourson
toth
enew
policyw
ould
haveth
reatened
hislife
Ab
ou
ttw
om
on
ths
into
hishosp
italization,
the
hosp
itat
billingoffice
beganasktng
why
I s’saschoosing
oer.of.netw
orkproviders:
ourinsurance
hadcontracts
wish
thehospital,
notthe
doctors.B
utI never
hadany
choiceof
anyn-pahent
providerm
yson
was
seenby
whoever
nappenedto
heon
service.
Bits
hadbeen
sentto
collecl:onsfor
nonpayment
thanI
didn’teven
knowab
out
Form
onths,I had
heldbedside
tigilfor
my
sonas
heteetered
between
lifeand
death.I w
astold
hew
asetig
iefor
nsttut;onslM
edicaid,bun
enmlling
himm
qired
my
go:ngto
them
idtown
offices.I refused
toleave
my
son’sbedw
dew
h.lehe
was
insuch
acritical
stateT
hatinitial
hosp.talizatontasted
IScontinuous
months,
between
threedifferent
tsospitalseach
with
differentinsurance
contracts,causing
more
billingand
payment
complications.
Eventually,w
ebegan
givinghospital’level
careat
home.
eachch
ange
createspoten
tialfor
—nnd
has
caused
—m
istakes
end
disru
ptio
ns,
puttin
ghim
thro
ugh
unnecessary
sufferin
g
The
fightto
geteverything
we
needto
keepour
sonalive,
endto
avoidbankruptcy,
isdaily
anddraining.
We
canonly
usethe
preleeedproviders
who
havecontracts
with
ourinsurance
company,
aneverevolving
listthat
changesw
ithcontract
negotiations.
Each
time
ourinsurer
d,scontnuescontracts
rashproviders,
we
scramble
tofind
newones
endto
restartcom
plcatedprocesses
ofdoctors’
orders,prior
authorizations,and,nsurae
ceapprovals.
en
my
husbandw
aschanging
jobs,m
ovingour
sonto
thenew
policyw
ouldhave
threatenedhe
tile.
We
endedup
usingC
OB
RA
benetitto
keepour
sonon
thepo’icy
we
hadw
henhe
firstgot
sick,and
hiseligib;liry
(orthat
expiresin
thecom
ingyear.
We
stilldo
notknow
howso
ensureour
son’ssafely,
indeedhis
eiabiity,during
thetransit.on
toa
newem
ployment’
basedprim
arypolicy
,itestill
100%dependent
foralt
artivinesof
dailylife,
inthe
sevenyears
sincethe
onsetof
hisillness,
my
sonhas
re!earnedno
walk
with
assistance,he
hasdeveloped
acom
munication
systemusing
vocalizations,eye
gaze,and
hisright
hand,and,
tom
yjoy,
hecan
nowear
bym
outh.H
egoes
toan
amazing
NY
Cpublic
neighborhoodschool
andthrives
inan
inclusiondats.
He
isdeterm
inedand
funny,courageous
andfrustrated,
andoutsm
artseveryone
who
underestimates
himor
hitintelligence
basedon
htsm
edicalcondition
andesutting
limited
motor
control.
My
sonhas
anupcom
ingsutgery.
The
daybefore
Thanksgiving,
Iwas
informed
hem
ightnot
havethe
same
surgicalteam
tnathas
performed
threepnor
sergeneson
h,mat
thehospital
Thathas
managed
hisconsplet
casefor
thetast
sevenyears.
dueso
contractnegotiations
between
shehosptat
andthe
insurancecom
pany.Iw
asterrified
my
son’scare
would
sufferbecause
ofthis.
Itis
gru
eling
.It
issen
seless,It
isd
esign
edto
enhan
ceth
epro
fitsof
insu
rance
com
pan
ies
The
contractnegotiations
ultimately
endedin
anagreem
entand
thisspecific
cnsisw
asaverted,
busw
hatIam
describinghere
5m
addening.ts
isgrueling.
Itis
senseless.It
isdesigned
toenhance
theprofits
ofinsurance
companies
andother
money.m
otieatedm
edicalcoss.inflators.
There
itabsotusely
nosense
inm
yson’s
changingdoctors,
nurses,suppliers,
andhospitals
dueto
contractnegotiations
between
profit’m
otivatedentities,
orchanges
ininsurance
policiesonce
hisC
OB
RA
eligibilityexpires.
Each
changecreales
potentialfor—
.and
hasactually
caused—
mistakes
anddisw
pto
ns
tohis
care,putting
himthrough
unnecessarysuffering
anduitim
ateiynak:ng
hiscare
more
enpensiveto
thesystem
asa
whole.
Likem
anydiseases,
ourson’s
unpredictableillness
couldhappen
toanyone,
atany
time.
SandraJoy
Steinisaw
nrer
andeducarronat consuitant.
Part
I:Workplace
Accidents
Aperfect
stormted
soa
moisplace
injurythat
shouldnew
erhave
hap
pen
edI w
asan
arherrustrativederk
fora
kitchenserving
1Sm
eatsa
day.O
ctober15.
1990the
bakerand
teen
eatinventory
clertcatted
insick.
Assigned
thebaker
duties,Im
itedbread
puddingfor
theday’s
dessert.To
put‘tin
theoven,
I squeezedbetw
eenshe
ovenand
atall
doubtetsathof
boxes,leftthere
byJohn,
thegrudging
meat
cleikreplacem
ent.I nw
:stedto
openthe
ovenand
slidein
thetrays;
thensqueezed
backbetw
eenthe
ovenand
theboxes
ofmeat.
At
1.30pm
,the
freshm
eathad
beensitting
besidethe
hotoven
forthree
hours.E
nvision:bones
ofm
easthat
hadn’tbeen
interlockedto
stabilizethe;,
weight,
boneshaphazardly
side-by-sidein
two
six.footstacks.
Vklsen
Iwent
soopen
theoven,
pullout
thetrays,
tw.st
around,and
headto
thecooling
tables.the
meat
boxesto
pp
led,
bombarding
my
ic%.ier
bathand
leg..
Imust
havesateam
edbloody
murder,
asIw
asknocked
tothe
tEoorDy
600pounds
olm
eatn
SO’to.100.pound
boxes.I rem
ember
searingpain,
notnoticing
breaksto
my
foot,leg,
andankle,
becausethe
traumat;c
hitto
my
lower
backobliterated
allrational
thought.Ilost
conscioutnessfrom
painas
my
tciaticnotch
broke.
Iawoke
unattendedon
ourhealth
clinicfloor
—no
ambulance
was
called,no
onestayed
with
me.
You
see,this
particularw
orkplacediffers
fromthe
comm
ercialkitchen
youvelikely
imagined.
No
onesaid
uN
oso
my
Boss:
shecould
pusyou
insolitary
confinement
fordisobedience.
Pan
2:H
ealthcare:W
eA
llN
eedIs
The
kitchenis
inB
edfordH
illsC
orrectionalFacility,
partof
theN
YS
penalsystem
.thad
alife
sentencefposaible
paroleafter
25yearsl,
forfighting
backin
tetf.protecsionw
irhina
domessc
vio’ence(D
IIrelationship.
Isufferedbeatings
form
oreyears
thanis
easilyim
agnable.
Inor,know
that90%
ofB
edfctd’s
female
inmates
havebeen
physicallyor
tex-jatlyabused
priorto
incarceration;that
prisonreform
advocatesreoor,
wom
enw
hokill
theirabusers
have25%
higherconviction
rates—
andthey
get
farharsher
sentences—
thanm
enw
hokilt
theirfem
alepartners
orm
enw
hokilt
inself.defense.
Inthe
U.S.,
white
females
who
killa
whtte
personcan
expecta
sentenceof
10.30years
Iwith
earlierparote)—
white
female
DV
vicsims
who
killin
setf.defenseare
predictablysentenced,
likem
e,for
[fe
thosebadly
stackedboxes
ofbeef,
andalt
them
:seryshat
fol!owed.
Mo
ther
difference:healthca,e
inprison
‘snotlike
healfhcareon
theoutside
Wnat
was
calledour
prison“hospilal
was
onlya
simple
clinicw
ithnurses
andm
inimat
supplies.C
altngam
bulancesdidn’t
happenbecause
itm
ean,an
unnecessayexpense,
adew
ofadditional
reports,and
possiblyan
investigationinto
mishandling
inmates.
Iwas
lefton
theclinic
floorfor
thenexs
shiftso
dealw
ithbecause
theprison
didn’tw
antto
incurovertim
echarges.
andshe
guardsdidn’t
want
sow
astefam
ilytim
eby
wnsing
overtime
repont.
conrieuedon
page9
“Continuity
of
Care”
willbe
the
norm,
notth
edream
.6
Am
bulancecosts
won
‘tleavea
brokenback
ona
clinicfloor.
Today,a
NY
courtthat
follows
currentsentencing
guidelines(not
alldo)
couldcharge
me
with
second’degree
self.defensem
anslaughterand
my
sciaticnotch
broke.Iaw
okeperhaps
sentenceme
to1.5
years,given
theunattended
onour
healthclinic
floorfo
ctsin
myra
se.tf
that
—no
ambulance
I
‘Tocut costs,
we’re
ddngaw
arw
thheatlh
ewarIcu
irsfavorof
apffea
day.’

Con
tinue
dfr
ompa
ge8
The
next
shif
th
ois
ted
me
into
apr
ison
van
and
seal
edm
e,sh
ackl
ed,
upri
ght
onm
ysc
iatic
brea
kw
ithou
ta
teat
belt
The
15-m
inut
esof
boun
ctng
and
sIdi
ngon
my
spin
alin
juri
es,
enro
seto
apu
blic
hosp
ital
,m
eant
wra
ckin
gne
rve
pain
that
was
beyc
ndex
cwci
alin
gFo
rye
ars.
care
was
hit
orm
iss
Aft
erre
turn
ing
born
one
ofse
ven
surg
erie
sfo
llow
ing
Ibis
acci
dent
,m
ybl
oodi
edho
spita
lba
ndag
esne
eded
chan
ging
.T
hepr
ison
hosp
ital
staf
fig
nore
dth
em-
My
fiie
ndco
nspi
red
sogi
veus
am
omen
tal
one
—te
lling
the
guar
dsIw
asre
turn
ing
toth
ece
llbl
ock
and
telli
ngth
enu
rses
that
she
guar
dsha
dca
lled
sosa
yth
ece
llbl
ock
was
prep
ared
for
me.
Cal
ling
ambu
lanc
esdi
dn’t
happ
enbe
caus
eit
mea
nta
slew
ofad
diti
onal
rep
ort
s,an
dpo
ssib
lyan
inve
stig
atio
n
As
she
push
edm
yw
heel
chai
rou
tof
the
pris
oncl
inic
,sh
egr
abbe
dw
hate
ver
band
ages
,ga
u2e,
and
clea
ns’n
gso
lutio
nw
eco
uld
reac
t.st
uffe
dth
emin
my
lap,
and
cove
red
me
w,th
abl
anke
t,A
noth
ertim
e,w
era
nou
tof
band
ages
and
open
edsa
nita
ryna
pkin
sto
serv
eas
repl
acem
ents
.O
nele
arns
sosu
rviv
eto
heal
.
Hea
lthc
are
cost
saf
fect
me
ever
yda
y:fir
st,
asth
eow
ner
ofa
smal
lbu
sine
ssin
NY
C,an
d,se
cond
,as
one
ofth
eth
ousa
nds
who
defe
ned
heal
thca
retr
ealm
ent
br
fear
ofba
nkm
ptcy
Inm
ysm
all
busi
ness
,I s
eeho
wem
ploy
er’b
ased
heal
thin
sura
nce
crea
tes
job.
lock
for
firs
t-cl
ass
cand
idat
es.
Tho
sew
ithth
ebe
stqu
alif
icat
ions
are
ofte
nst
uck
inde
ad.e
ndob
s:th
eyca
nnot
affo
rdto
lose
thei
rex
pens
ive
bene
fits
pack
age
byju
mpi
ngsh
ipto
me.
emplo
yer
’bas
edh
ealt
hin
sura
nce
crea
tes
job
-lo
ckfo
rfi
rst’
clas
sca
ndid
ates
Iam
alw
ays
jugg
ling
the
cost
sof
grow
ing
my
busi
ness
with
the
cost
sof
prov
idin
gco
mpe
sitv
ein
sura
nce.
Rec
ensl
y,If
ound
asu
perb
cand
idat
efr
omA
ustr
ias-
hodo
esno
tre
quir
ein
sura
nce
—so
lam
relie
ved
ofh:
gh.c
osl
dedu
chb!
esan
dot
her
adm
inis
trat
ive
payr
nIex
pens
es.
Par
tIll
:M
yP
ast
Fre
es(a
ndF
ocus
et)
My
Pre
sent
Iwas
rele
ased
and
paro
led
aye
arag
o,ha
ving
wor
ked
hard
for
othe
rsdu
ring
my
year
sin
side
:se
rvin
gas
the
Eps
scnp
aiR
ecto
r’s
assi
stan
t;te
ach:
ngES
Lcl
asse
s,be
ginn
erm
ath,
and
Eng
lish
toin
mat
esin
the
pris
onsc
hool
;se
rvin
gas
apr
ison
para
tega
t.
Iwas
luck
y,an
dth
ose
eHon
she
lped
me
land
ajo
bon
the
ouss
ide,
wor
king
with
ac,
imin
alde
fens
ear
torn
ey.
Iam
grat
eful
toha
veM
edic
aid,
and
toha
vefr
eedo
mIf
ear
noth
ng.
Hea
ring
aju
dge
ripm
efr
omm
ylif
ew
itha
sent
ence
of25
’to-li
fe,
mea
ning
noch
ance
ofpa
role
or25
year
s.fo
rced
me
into
faci
ngev
ery
day
with
out
fear
.W
hat
mor
eco
uld
I los
e,ev
er?
Med
icai
dgi
ves
usa
chan
ceto
begi
nag
ain
aseq
uals
Isup
port
NY
Hea
lth.
Pers
onal
lyit
veil
give
me
dent
alca
reno
rco
vere
dby
Med
icai
d.M
ainl
ybe
caus
eM
edic
aid
give
sus
all
ach
ance
tobe
gin
agai
nas
equa
ls,
even
thos
eof
usw
hose
rved
mor
eth
anth
ert
ime.
Kar
enTh
omas
sax
asd
iocf
teac
her,
ossv
ied
adet
care
asen
.ad
‘sac
impr
ison
edf0
’OV
hom
icid
eei
5982
asag
e335
5hew
asre
leas
edah
er34
.5ye
a’s.
“Med
ical
cost
sar
eth
eta
pew
orm
ofA
mer
ican
econ
omic
com
petit
iven
ess.
”‘W
arre
nB
uffe
t
Cas
hw
asre
ally
scar
cew
hen
I sta
rted
my
com
pany
,so
Idid
not
have
insu
ranc
efo
rtw
oye
aiw
Fort
unat
ely,
Ifa
ced
nolif
e’th
reas
enin
gco
nditi
ons-
Rut
emer
genc
ytr
eatm
ent
and
12st
itch
esfo
ra
cut
tom
yfo
rehe
adca
used
me
toch
oose
betw
een
the
high
cost
sof
seei
nga
plas
ticsu
rgeo
n—
and
poss
ible
bank
rupt
cy—
orliv
ing
wis
ha
perm
anen
tsc
ar.
That
’sa
pret
tydi
reco
nseq
uenc
efo
r12
.sti
tche
s.
Whe
neve
rIl
ook
inth
em
inor
ora
cust
o”ne
rlo
oks
atm
e,Ir
emem
ber
the
drea
dof
not
ha’s
;ng
heal
thca
re.
Iagi
eew
ithW
arre
nB
uffe
tw
hosa
id.
-M
edca
lco
ats
amth
eta
pew
orm
ofA
mex
ican
econ
omic
com
peti
tive
ness
,’
Jotu
sR
odne
y,is
asu
cces
sful
entre
pren
eur,
grow
ing
hi,
seco
ndst
artu
p.
Iam
livin
gpr
oof
that
even
the
hard
est’
wor
king
.m
ost
educ
ated
oenp
leca
nlo
seit
all
ina
mat
ter
ofm
Ont
hs.
Iwen
tfr
omea
rnin
g$2
25K
aye
arto
less
than
S2
1,
now
,A
fter
losr
egm
y60
.hou
r.a’w
ee’e
, hgh
.pre
ssur
eco
rpor
ate
com
mun
icat
ions
ohin
NY
Can
dha
ving
CO
BR
Aes
pire
Isig
ned
upon
the
Aff
orda
ble
Car
eE
xcha
nge,
payi
ngfo
rm
ydi
sabl
edhu
sban
dsan
dm
yco
vera
gew
ithsa
ving
s.
Sadl
y.ne
ithe
rth
eps
ychi
atri
stno
rth
eps
ycho
logi
stI s
awre
gula
dyfo
rch
roni
cde
pses
sion
was
cove
red
unde
ran
yof
the
Exc
hang
epl
ans,
sow
epa
idou
tof
pock
et.
Inm
yea
rly
SOs,
Iwas
havi
nglit
tlesu
cces
sfi
ndin
gan
othe
rjo
b,w
hich
exac
erba
ted
my
depr
essi
on.
The
nm
yhu
sban
dw
asdi
agno
sed
with
PTSO
afte
rbe
ing
viol
ently
assa
ulte
d.so
heto
obe
gan
seei
nga
psyc
holo
gist
ona
wee
kly
basi
s.
In20
16.
our
heal
thca
rebi
llsex
ceed
ed4O
,OO
O,
quic
kly
drai
ning
our
savi
ngs
toth
atw
eha
dto
sell
our
NY
Cho
me
and
wlo
cate
toe
chea
per
loca
tion
inth
eH
udso
nV
alle
yiIs
iste
niiy
ing
tok”
o:,
that
losi
ngyo
urjo
ban
dne
edin
gcr
itica
lhe
alth
serv
ices
can
rapi
dly
depl
ete
all
the
fina
ncia
lre
sour
ces
you’
vew
orke
dye
ars
soac
crue
.H
avin
ghe
alth
insu
ranc
eti
edto
emp’
oym
ent
mak
eslo
sing
aob
not
only
scar
y,bu
tpo
tent
ially
life
.thre
aten
ing.
As
our
curr
ent
inco
me
isso
low
(I’ve
still
yet
tofin
da
new
fulI
.tim
epo
sitio
n,so
amno
ww
oric
ing
asa
free
lanc
eco
nten
tde
velo
per
and
ghos
twri
ter)
,w
ere
cent
lyqu
afif
ied
for
Med
icai
d.It
has
been
aIm
elif
esav
ergi
ven
my
husb
ands
illne
ssan
dm
yow
nch
roni
cco
ndit
ion.
We
are
mos
tgr
atef
ulto
have
Med
icai
dco
vera
geth
mug
hth
eex
pand
edpr
ogra
mun
der
Oba
mac
are,
but
ther
ear
ega
psth
atm
ean
we
dont
gas
the
esse
ntia
lca
rew
ene
ed.
Firs
t,M
edic
aid
do
esn
spr
ovid
ech
irop
ract
icco
vera
ge.
Iwas
born
with
are
vers
ecu
rvat
ure
ofth
ere
ck,
aco
ndsi
onm
ade
mor
epa
infu
lby
spen
dng
hour
son
aco
mpu
ter
ever
yda
yw
ilin
g.M
yhu
sban
dsu
stai
ned
ase
riou
ssp
inal
inju
ry15
year
sag
ow
hich
left
him
part
ially
disa
bled
,in
pain
,an
dun
able
tow
ork.
Bec
ause
my
sala
ryw
ason
ceso
high
and
Ihad
heal
thco
vera
geth
roug
hw
ork,
hene
ver
qual
ifie
d
for
disa
biit
yco
vera
gaN
oww
eca
n’t
affo
rdto
pay
for
chir
opra
ctic
care
onou
row
n—
sow
eju
stde
alw
ithbe
ing
inpa
inall
the
time-
Toad
din
sult
toin
jury
;pr
oude
rne
twor
kske
epch
angi
ng,
sow
efe
dou
rsel
ves
forc
edto
chan
gedo
ctor
sal
lto
oof
ten
—ev
enif
the
ones
we
orig
inal
lyha
dw
ere
mos
squ
alif
ied
totr
eat
us.
Itsal
sopr
oble
mat
:cth
atco
vera
gefo
rm
enta
lhe
alth
prof
essi
onal
sof
ten
does
n’t
exte
ndbe
yond
just
com
mun
ityor
hosp
ital
clin
ics,
soth
ebe
atth
erap
ists
for
apa
rtic
ular
diag
nosi
sar
eof
ten
out
ofre
ach.
Hav
ing
hea
lth
insu
ran
ceti
edto
emp
loy
men
tm
akes
losi
ng
ajo
bpote
nti
ally
life
-thre
aten
ing
And
then
ther
ear
eth
em
any
gaps
inw
omen
’she
alth
issu
es:
Isuf
fer
from
ara
regy
neco
logi
cal
cond
itio
nth
atre
quir
edm
yco
nsul
ting
with
asp
ecia
list
who
waw
s’t
cove
red
bym
yes
uran
re.
Wne
nIh
ada
job.
Inev
erco
rned
abou
tm
yhe
alth
care
orm
yhu
sban
d’w
Now
Iwor
ryco
nsta
ntly
abou
tou
rw
orse
ning
heal
than
dou
rw
oise
ning
fina
nces
.N
YH
ealth
wou
ldm
ake
such
adl
fere
nce
toou
rliv
es
Sony
aH
aifa
span
s2
5ye
ars
asa
PRan
dC
orpo
rate
Coo
vnun
icar
cns
prof
essi
onal
Her
i.cr.
21an
dae
arm
nonf
ictio
nha
veap
pea
red
inm
ore
than
30lit
erar
y
Top
tale
ntw
on’t
bejo
b-lo
cked
—yo
uca
nre
crui
tth
em.
10H
ard-
wor
king
NY
ers
who
get
sick
won
’tfa
cepe
nury
.
Dua
l-In
com
e.L
ost
Job
s,L
ost
Eve
ryth
ing
I
Smal
lB
usin
ess
Ow
ner:
Nee
ds
NY
HA
toA
ttra
ctT
opT
alen
tIn
2016
,ou
rh
ealt
hca
rebi
llsex
ceed
edS
40,0
00,
quic
kly
drai
ning
our
savi
ngs

NEW YoRKHEALTH ACT
Savings and Spending Under the New York Health Act FAQ
Introduction: The New York Health Act (NXHA) will generate enormous savings by
replacing the marketing, bureaucracy, and profits of insurance companies with a single
publicly-accountable plan, as well as by negotiating fair prices with drug companies. Data
from the RAND study shows that NYHA, while covering everyone, including long-term care,
and eliminating all deductibles and copays, will save more than $11 billion in 2022 and even
more in ffiture years. By distributing the tax burden fairly based on ability to pay and having
capital gains and other taxable investment income contribute to its cost, 90% of New Yorkers
will see substantial savings in their spending for health care.
How Much Will the Average Person Save and Pay under the NY Health Act?
New Yorkers will save billions of dollars by not paying rising premiums, deductibles,
copays,outtofnehvortchargesrandJong=term2aracosts
(homecarenursinghomecare).
We’ll save tens of billions by cuffing out insurance company bureaucracy and profit,
lowering doctor and hospital administrative costs, and negotiating lower drug prices.
The lower cost of the single payer system will be funded by existing Medicare and
Medicaid and other public funds, along with a progressively graduated tax on payroll and
taxable non-payroll (investment) income. The employer will pay at least 80% of the payroll
tax; the employee no more than 20%. A self-employed person would pay the full payroll tax.
MI New Yorkers, including children, will be covered, whether they are working or not.
The NYHA provides that the first $25,000 of a person’s annual income will not be
taxed. The bill does not specify other income brackets and rates, which would be set shortly
before the plan is ready to be implemented.
We can, with reasonably high accuracy, estimate what the average working New
Yorker will spend under the New York Health Act single payer legislation. Over 80% of
New Yorkers earn less than $100,000 per year. For that significant majority of New Yorkers,
here is what they will pay in New York Health taxes, based on the results of the RAND
report and a Summary’ and Evaluation of that report (see below):
Employee Employer Self-employed__1
Annual Tax Effective Tax Effective Tax Effective
Income rate rate rate
$25,000 $0 0% 50 0% $oj 0%
$50,000 $900 1.8% $3,600 7.2% $4,500 9%
$75,000 $1,800 2.4% $7,200 9.6% $9,000 12%
$100,000 $2,700 2.7% $10,800 10.8% $13,500 13.5%
For any income below $100,000, the maximum tax can be calculated as follows:
1. Subtract $25,000 from the income.
2. For employees/employers/self-employed, multiply the result by 0.036/0.144/0.18.

Higher-income persons will pay proportionately more, as tax rates rise in accord with a
progressively-graduated tax schedule, These taxes will raise the funds described below.
Note: The New York Health tax is a tax on individuals, not households or families.
As an example. the median household income in New York State is $65,000; if that income
is earned by two employed people making $32,500 each, their total New York Health tax
will be less than $540.
Compare all these numbers with what people spend today: The average family health
insurance coverage in New York State costs £21,000, and the average deductible is £3,200.
What Will Overall Savings and Spending be under the New York Health Act?
Getting rid of insurance company bureaucracy and profits will save New Yorkers
over $20 billion. We will save over $16 billion we now pay to doctors, hospitals and other
providers for the adminisfrative costs of fighting with insurance companies. Under NY
Health, we could cut drug prices over $18 billion with the bargaining power of 20 million
consumers. That’s over $55 billion a year. The New York Health Act would use the savings
tQpAyj,pflcalth carej pujjjgp,çyt jkers’ pQclcets.
NY Health would pay health care providers more than Medicare and Medicaid now
pay, because the rates would be required to be related to the cost of delivering the service and
sufficient to assure an adequate supply of the service, and unpaid care would now be paid.
For patients, NY Health would also cover what we now spend on deductibles, co
pays, out-of-network charges, and out-of-pocket spending for long-term care.
Table 1. Savings & Additional spending — in S billions
SavingsReduced insurance company bureaucracy and proflt 20.4
Reduced health care provider adnthilsfrative costs 16.3
Reduced prices for prescription drugs 18.6
TOTAL SAVINGS 55.3
• Additional spendingCovering the uninsured & eliminating deductibles,
17 1copays,_out-of-network_charges
I Improved provider payments 8.8
I Long-tenn care — shifting unpaid care to paid 18.0
TOTAL ADDED SPENDING 1 43.9NET SAVINGS
See also Figure 1. See the RAND study and a Summary and Evaluation
for further details on this table and what follows.’of the RAND Report
wwwnnd.orw’content’darn/rand/oubs/research reports/RR2400/RR2424IRAND RR2424.odf:
www.infoshare.org/main/Summary and Evaluation of the RAND reoort - LRodbern.pdf

What does Long-term Care (Long-term Services and Supports) Add to the
Cost of the New York Health Act?
Today in New York, spending on LTSS is $22 billion by government (primarilyMedicaid) and $11 biffion private spending (insurance plus out-of-pocket) -- totaling $33billion. The RAND study estimates that people in New York provide about $3 I billion inunpaid home care (generally provided by a family member, usually a woman), and assumesthat a portion of current unpaid home care will be replaced by paid home care under NYH,costing $18 billion. Therefore, the new public spending on LTS S under NYH would be $11billion plus $18 billion, totaling $29 billion.
Table 2. Long-term care — in S billionsCurrent government spending for LTSS 22.0Spending shifted to NY Health:Current insurance spending for LTSS 4.0Current out-of-pocket spending for LTS S 7.0Unpaid home care shifted to paid care 18.0TOTAL NY HEALTH SPENDING FOR LTSS 5.29.0
____
How Much Revenue Must be Raised by the NY Health tax?
New York Health will replace current spending by New Yorkers: $131 billion wenow spend on premiums (employer and employee share, individual coverage, Medicare PartB premiums, etc.), $29 billion in out-of-pocket costs (deductibles, co-pays, out-of-networkcharges, paying for long-term care, etc.). It would cover the $8.9 billion cost of the localshare of Medicaid. This current spending totals $169.3 billion. Table 1 shows that NYHealth saves $11.4 billion in current spending. Taking account of these savings, the NYHealth tax will need to raise $157.9 billion. See also Figure 2.
Table 3. Revenue needed from NY Health TaxCurrent spending replaced by NY HealthInsurance premiums (employment-based, P S 131.5
individual,_Medicare_Part_B,_etc.)Out-of-pocket spending 28.9 IMedicaid local share 8.9TOTAL 169.3Net savings from Table 1 -11.4Revenue to be raised by NY Health tax 157.9
3

Pigure 1
Sources of Savings, Added Costs and Net Savings
t$43.9B
Covering Everyone WhileSa’ing Money
Total p,oJactn status quo[__ypendiag In 2Dfl:$3116
In,,r,nrp
almr. rotv
Not:—$11.4 B
Rpd,prd Mu
P. -Ir.piThl
4cinFfl nsT
nio: ftzLciem
(.‘E
‘5.5% Net Savings:
-3.6%
Total Savings —17.7% Thtal Additional Costs: t14.1%
1otI__. _____
— ——
scr,t:JcLmrz.s,3n,::’wLzr;/eyrNcclthjc1. Pttçocr_.4cpi;313
Inni T.&c..Sr—’cr ru £‘&: nj’’w&tVDC.nóñ Lxr:n’.f;’w S’,Aw. a.t20:S.
—$55.1 B
Figure 2 Current Sources of Funding
vs. Funding under the New York llealth Act
iThe NY HuaILh Wx rephct>
& co-artt-Mecicaid cosis
Sa \i I g bi 1111) as
private insuauce. oai-of-pc.cket c,sIs. throuhadailiüstrtive simplification and
CURRENT SOURCES OF;:1% HEALTH CAn FUNDING
Fr,vate
redicedriccs of drjgs andinedical devices
HEALTH CARE FUNDING UNDERruE NEW YORK HCALTh ACT
lnsuran
It%irci Po:,.i
34% rdo,
- — I 0% Slob— Gz.
-
3% ovnly ,. -
I 1., jl,crrund:
Health Tar
0% SuosGovu
Ilt Cuhar
Sour:,,: )odi U... et u An A ustsnuenr 0.’ rt rjy Htc,th 4:; 154s:’ corprxrtloh, AIfL.Sb C18);
teonrndbr;. S.mrs..ycndEv:snnti;th4kPtvp,rcr,—rAsnuw:,r.r{5apIe,nbi.r20I2b.

• How the New York Health Act Works
in Tables and Figures
1. Where New Yorkers Currently Get Their Coverage Today
Source of coverage Population (millions)’
Employment-based private insurance 9.4
Individual (non-group) insurance 1.8
Medicaid, Essential Plan & CHIP 4.3
[Medicare&VA 2.4
Dual Medicaid and Medicare 1.0
Uninsured1.2
Total20.1
‘Data from Jodi Liu eta!, et cii, An Assessment of the J’1Y Health Act (RJ4}D Corporation,
August 2018), 2022 projection.

2. How the Cost of Private-sector Employer-based Health Insurancein New York has Grown
Percent2008 2017
Increase
Average premium
Average employee share of premiumSingle coverage $947 $1,568 65.6%
Family coverage $3,376 $5,878 74.1%
DeductiblePercent of employees with deductibles 46.6% 75.2% 6 1.4%
Average single deductible $732 $1,687 130.5%
Average family deductible $1,524 $3,226 111.7%
Note: General inflation between 2008 and 2017 was 15%.
Source: Medical Expenditure Panel Survey, Agency for Healthcare Research and Quality. DFU-{S.
Washington, DC, 2018
Single_coveragçFamily coverage
$4,638 $7, 30R$12,824 $2 1,317
57.6%66.2%
https:!/rneps.ahrg .ov/rnepsweb!data stats/quick tables search.jsp?cornponent=2&subcornponent=2

3. Savings under the New York Health Act:Comparison with Status Quo Spending on Health Care Services
Expenditures ($2022 Billions)
1R9S1 1Q7 11 R°/
Includes increased utilization (per RAE]) report) and improved provider fees
2NYHA could negotiate lower prices (not included in RAE]) report)
Includes universal long-term care
Medical care
Status PercentNYHA Change
Quo ChangeHealth care services
161Prescription drugs & devices 48.1 36.2 -11.9 -24.7%Nondurable medical products2 6.0 6.0 0.0 0.0%Long-term care (paid) 38.0 56.0 18.0 47.4%Long-term care (unpaid) [31.0] [13.0] [-18.0/ [-58.0%!
Total health care services 255.4 280.7 25.3 9.9%Administration
Health plan administration 28.5 8.3 -20.2 -70.9%Provider administration 26.4 10.1 -16.3 -61.7%State fmancial administration 0.6 0.6 0.0 0.0%Employer health benefit admin 0.2 0.0 -0.2 -100.0%
Total administration 55.7 19.0 -36.7 -65.9%Total health care spending 311.2 299.7 41.4 -3.7%

4. How Health Care Is Paid for Today,
and How It Would Be Paid for under the New York Health Act
Expenditures (S2022 Billions)
Source of Health Care SpendingStatus
NYHA Change
EM±cr, MedicaithACAkc.) 120.5 JP±S_ - 0 —
State & local govt (Medicaid, etc.) 34.1 ! 25.22 -8.9Employer-based private insurance 84.8 -84.8
Individual (non-group private insurance) 10.4 -10.4Other miscellaneous premiums2 27.8 -27.8Medicare Part B premiums3 8.5 -8.5NYHApayrolltax4 102.0 102.0
NYHA non-payroll tax4 55.9 55.9Out-of-pocket payments 33.5 4.6 -28.9
j Total health care spending 319.6 308.2 I 11.4
1Local share of Medicaid removed and paid for by NYHA tax
2lncludes Medigap, Essential Plan, CHIP premiums
3Paid to the Federal government and thus not reflected in Table 2 health care sen’ice spending
‘NY Health tax replaces private insurance premiums, out-of-pocket costs, and other premiums. It pays for
improved provider fees, Medicaid local share, Medicare Pan B premiums, and universal long-term care.

5. Savings and Additional Spendingunder the New York Health Act
Savings -— __S2022RReduced health plan admin costs & profit 20.4Reduced provider admin costs 16.3Reduce prices of drugs & devices 18.6
Total savings1 55.3Additional spending
Covering the uninsured & elimination of cost-sharing 17.1Improved provider fees 8.8Long-term care 18.0
Total additional spending 43.9Net savings 11.4
NYHA could achieve additional savings through reduction in fraud and waste. RAt’4D did notprovide an estimate of potential savings; Friedman estimated at least $5B in savings.

a
6. One Proposed Effective Payroll and Non-payroll Tax Ratesunder the New York Health Act’
NYHAIncome
Effective RateS250U00J0$50,000 6.9%$75,000 10.2%$100,000 12.2%$200,000 16.9%$400,000 20.8%
Note: Average health care spending today at all income levels, including premiums paid byindividuals, out-of-pocket payments (including the cost of long-term care), tax payments supportinghealth care programs, and premiums paid by employers (forgone wages), is over 20% of householdincome. See Jodi Liu, eta!, An Assessment of the MY Health Act (RAND Corporation, August 2018),especially Fig. 5.4 and Appendix B.
1Marginal tax rates: <$25,000: 0%; $25,000-$49,999: 13.8%; S50,000-$74,999: 16.9%;$75,000-$99,999: 18.4%; $lOO,000-$199,999: 21.6%; $200,000 or more: 24.6%. See L. Rodberg,Summaiy and Evaluation ofthe RA]TD Corporation’s Assessment of the AT Health Act (September201 8). Section 9.

Sources of Savings, Added Costs, and Net Savings
Covering Everyone Whileoney
Total:
Total projected status quo
spending In 2022: $3118
Net:
—$1i.A B
Total SavinEs: —17.7%
—$55.1 B
Total Additional Costs: +14.1%
÷$43.9 B
Reduced Reduced MDInsurance & Hospital
Admin Costs: Admin Costs:-6.5% -52%
CoveringEveryone &EliminatingCos: Sha:ing:+5.5%
improvedProvider Fees+2.8%
Reduced Pricesof Drugs &Devices: -6%
termCare+5.8%
Net Savings:-3.6%
Sources: mdi Lit. ci a!.. .1nAssrswieni ofrheNYHethth4c:. RAND CoipomtiomAucust 2018
Leonard Rodbera.Siuimca v and Emluarion ofthe RAND Colporarioii;rAsse.rcnienr of the NYHeahiiAc!, September2015.

Current Sources of Funding
vs. Funding under the New York Health Act
HEALTH CARE FUNDING UNDERTHE NEW YORK HEALTH ACT
Savings 34% Federd
$IIB‘\Govt.
10% StaleGovt
The NY Health tax replaces Saving billioas
private insurance, out-of-pocket costs.& countyMedicaid costs
31% PrivateInsurance
CURRENT SOURCES OFHEALTH CARE FUNDING
through administrative simplification andreduced prices of drngs and medical devices
34% FederalGovt.
-fr
il%OuL20c Pocket
3% CountyGvt ii Olper
— Funds
41% NYRealth Tax 11 % Other
Funds
Sources: Jodi Uu, a of An Assessment of the WV flea/ti, Act (RAND corporation, August 20181;Leonard Radberg, Sun,maryondEva(ustioti of the RAND CorpororianAssessntetir(September 20181.

Progressively Graduated Taxes
under the New York Health Act
-Paying foTNYHIththroughVayroIL&Non-PatU1iTaW
T 80% paid by empIoye 20% paid by employee
-r--1
4 t_TaxBracket
$I
Wages & Salary & Taxable Investment Income
lncome/ Effective Employee Pays Employer Pays Non-Payroll
year Tax (20%)/year (B0%)/year (investor pays)
A 550K 69% 5690 52,760 53,450
B 5100K 12.3% 52,455 59,820 $12,275
C 5175K 16.3% 55,695 523,475 526,475
0 5225K 17.8% $8,005 $32,020 $40,025
E 5400K 20.8% $16,615 $66,460 $83,075
24%
16%
8%
0Ffe
Sourceriodi Uu, cccl, An Ancssmcnt of the NV HeolthAct (R4ND Corporation, August Zeta).
Leonord Rodbcrg,Summorycnd Ev&uotian of the RAND Corporation’s Assenmcnt of the NVHcolch Act (September 2013).

Data Sources
The principal sources for these tables are the following:
Jodi Liu, et ci, An Assessment ofthe AT Health Act (RAND Corporation, August 2018).
www.rand.ora/oubs!research reports!RR2424.htrnl
Leonard Rodberg, Summaiy and Evaluation of the RAND Corporation ‘s Assessment of the NY Health
Act (September 2018). www.infoshare.org/mainJSurnmary and Evaluation of the RAND report -
LRodbera.pdf. This report includes evidence for greater savings than found in the RAND report as well
as estimates of the cost of improved physician fees, covering the local share of Medicaid. covering
Medicare Part B premiums, and providing universal long-tern care.
Gerald Friedman. Economic Analysis of the New York Health Act (April 2015). www.infoshare.or!
maim/Economic .alysis New York Health Act - OFriedman - April 2015.pdf
Additional data sources on long-term care:
Incorporating Long-tern Care into the New York Health Act, PN}IP NY Mefro Working Group, 2016
www.infoshare.org/main/lncorporating Long-term Care nto the New York Health Act,pdf
Reinhard. 5, Feinberg, L, Choula, R. & Houser, A. (2015). Valuing the invaluable: 2015 update. AARP
Public Policy Institute report. Washington, D.C. Available at
hnp:i/www.aam.orIcontentidamIaarnIDpi/2015/valuinathe-inva1uable-2015uodate-new.odf

NEW YORKHEALTH ACT
Federal Waivers FAQ
Q: In order to efficiently integrate federal funds into the new system, the New York Health
program will seek waivers from the federal government that will bypass ordinary federal
reimbursement rules and enable bulk transfer of funds based on global budget projections.
What options are available should such waivers not be forthcoming?
A: Over half the funds that provide and administer health care services in New York comes from
federal and federal-state public programs. These include Medicare, Medicaid, the Children’s
Health Insurance Program (CHIP), and Affordable Care Act (ACA) tax credits.
The New York Health Act (NY Health) explicitly provides that the Commissioner of Health will
seek federal waivers needed to smoothly and efficiently integrate these funds into the NY
Health trust fund (See the bill Introduction and Section 5109).
Medicaid and CHIP
States manage and partially fund the Medicaid and CHIP programs. Matching funds are
provided by the federal government. Currently, federal funding is conditional upon verifying the
eligibility of each Medicaid and CHIP participant and assuring the validity of each individual
service transition. New York would seek a waiver to allow funds to be received, in bulk, based
upon past receipts and estimates of future eligibility and costs, bypassing the need for case-by-
case, fee-by-fee verification. This would be similar to the global funding waiver currently in
effect for Rhode Island’s Medicaid program.
New York already has a number of approved Medicaid waivers that allow New York to provide
services that are not part of original Medicaid including, among others, long-term care services
in the home and community and certain behavioral health and addiction services. These
waivers would be expected to continue, along with others in effect, or under development, that
allow integrative managed care approaches and capitated payment methods that move away
from the less efficient fee-for-service model.
Medicare
The Medicare program does not have state-based “waivers”, but it does have “demonstration
projects” as defined by the 1967 and 1972 amendments to the Social Security Act which can
potentially serve the same purpose. These are intended to promote research that might assist
Congress and the Department of Health and Human Services (HHS) in designing reforms that
would increase the efficiency and cost-effectiveness of the Medicare program, without
1

compromising health care quality. These reforms could include changes in payment
methodology that would allow for seamless articulation of the Medicare program with NY
Health.
Most projects were expected to be proposed initially by Congress and HHS, and managed and
evaluated by the Center for Medicare and Medicaid Services (CMS). The legislation was not
designed to support state-specific operational program reforms, although the research has led
to some innovative technical improvements and a few state-based operational waivers, such as
one that allows Maryland to establish uniform pricing, and, more recently, global budgeting, for
all hospitals. Maryland is now seeking to extend its Medicare pricing policy to physician
reimbursement.
The Maryland waiver shows that significant changes in payment methods in a state are treated
by CMS as aligning with the intent of the original Medicare legislation.
Medicare Advantage may be used if a Medicare waiver is unavailable
Alternative payment mechanisms such as Medicare Advantage (MA) are available if a waiver
were not to be granted. In 1973, Congress codified federal rules for provider collectives that
offered services on a capitated basis, and Medicare was authorized to develop demonstration
projects that would allow such HMOs to manage services for older adults. This became the
basis for the Medicare Part C (Medicare Choice+) legislation in the Balanced Budget Act of 1997
and the Medicare Advantage legislation in 2003. Although nearly all MA organizations have
been private, usually for-profit, the 1973 law refers to “public or private” entities that could be
authorized by the federal government to be providers for such programs.
Over 38% of Medicare recipients were enrolled in MA programs in New York as of 2017. Such
programs typically offer an expanded set of benefits, usually optical, dental, and hearing, along
with a prescription drug component. The MA organizations typically reduce their expenditures
by offering only a narrow network of providers, by requiring substantial co-pays, and
sometimes by requiring a premium add-on.
A public or quasi-public entity serving as an MA plan could ease the way toward integrating
Medicare into NY Health. Medicare recipients in New York State would be considered to be
part of the state’s MA plan. They would, of course, receive the same comprehensive benefits as
everyone else. The federal government already uses capitated payments for such plans,
replacing inefficient fee-for-service reimbursements. This would help to smoothly integrate
federal funds into the NY Health trust fund, if a waiVer (or demonstration project) could not be
negotiated.
Since this would be a new situation, there are issues that might arise. The original Medicare
Advantage amendments were intended to encourage health marketplace competition to drive
down premiums and allow consumers a broader range of health plan choices. A state MA plan
2

would be part of the single-payer plan that eliminates competition for basic comprehensive
health insurance. NY Health will, of course, reduce health care spending and allow for total
freedom of choice of provider. Comprehensive benefits will cover everything covered by MA
plans, and more, with no cost-sharing.
New York’s dual-eligible plan already incorporates Medicare Advantage
The ACA was designed to help states implement innovative health insurance reforms. One
major goal was to find ways to integrate Medicaid and Medicare for so-called “dual-eligible”
patients, including long-term care. In 2008, dual-eligibles constituted only 20 percent of
Medicare beneficiaries nationally but 31 percent of Medicare spending. They constituted 15
percent of Medicaid beneficiaries but 39 percent of Medicaid spending.
Section 2602 of the ACA set up a Federal Coordinated Health Care Office, reporting to the
administrator of CMS. Among the purposes of the office are to more effectively integrate
benefits under Medicare and Medicaid for dual-eligibles, simplify the processing of claims, and
________—
in effect, becomes the waiver vehicle through which Medicare is integrated with Medicaid into
a single payment stream managed by states.
New York is one of 17 states authorized to carry out such a demonstration project. It is called
Fully-Integrated Duals Advantage (ADA) and is part of the state’s Medicaid Redesign Team
reform effort launched in 2012. Although New York already had two small integrated programs,
including the Program for All-inclusive Care for the Elderly, or PACE, the ADA initiative aimed to
eventually include all dual-eligibles and become part of the ongoing effort of New York to
transition Medicaid recipients into managed care and managed long-term care environments
where, in theory, costs can be managed and quality improved.
The new federal office uses the MA program to carry out its integration efforts. New York’s
FIDA initiative was set up as a set of MA plans using private insurance organizations to manage
the demonstration project. Medicare payments are made according to the MA model.
Medicare wrap-around
As a fallback option, a state could set up a Medigap plan, or other plan, that would “wrap
around” traditional Medicare. Such a plan would run parallel to Medicare as it currently exists
and provide any needed extra payments to providers. While such an approach would limit
administrative savings for the state government, since providers would still have to submit bills
to the Medicare program, an efficient electronic claims processing system could minimize the
additional administrative effort by providers.
There are also provisions under Section 1395kk of the Medicare law that allow the federal
government to hire contractors to maintain data and administer benefits under certain
conditions. A state or state-related entity could qualify as such a contractor and thus could
process Medicare claims as well as claims made directly to NY Health.
3

ACA Innovation waivers can bypass ACA requirements
The Affordable Care Act Section 1332 offers innovation waivers that allow a state to opt out of
ACA requirements (for instance, the requirement to create a “marketplace” to offer private
insurance plans) in order to introduce new approaches that could address substantive areas of
health insurance policy and/or technical areas such as data collection and claims processing.
The waiver option was included in the ACA on a bi-partisan basis because it could cover
approaches that were of interest to both conservative and liberal membersof congress. The
discussion leading up to the enactment of the law explicitly included single-payer options, and
the state of Vermont submitted a 1332 waiver request for the single-payer legislation it passed
in 2011 (the request was withdrawn when the governor tabled the plan.).
In order for a 1332 waiver to pass muster, the new system must offer benefits at least as
comprehensive and as affordable as would have been the case without the waiver, and it must
cover at least as many residents. In addition, the state must present a ten-year budget that
demonstrates that the system will not add to the federal deficit. The NY prnfioujd
readily meet these “guardrail” provisions.
At a minimum, an innovation waiver will allow a state to receive ACA premium tax credit funds
directly and in bulk form rather than for each individual service fee. A waiver can also allow a
state to develop uniform pricing and innovative claims processing systems. NY Health will likely
use a single “back office” to manage payments to providers to limit administrative expense.
Sources
Legislation
• Medicare demonstration project waivers
Social Security Act Amendment (1967) Section 402a
https://www.ssa.gov/OP Home/comp2/F090-248.html
Social Security Act Amendment (1972) Section 222a
https://www.ssa.gov/OP Horne/como2/E092-603.html
• Medicare Advantage
Health Maintenance Organization Act of 1973
https://www.govtrack.us/congress/bills/93/hr7974/summary
Balanced Budget Act of 1997 (Creates Medicare Part C) https://greenboolc
waysandmeans.house.eov/siteskreenbook.waysandmeanshouse.gov/files/2011/images/l97-
802 gb.odf
Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (Creates Medicare
Advantage). https://www.congress.gov/bill/lOSth-congress/house-bill/1
4

• Medicare-Medicaid Integration: Dual-eligibles
Affordable Care Act (2010) Section 2602 httgs://www.cms,gov/Medicare-Medicaid
Coordinatjon/Medicare-and-Medicaid-Coordination/Medicare-Medicaid-Coordination
Qffice/Downloads/AffordableCareActSection26o2.pdf
• ACA Innovation Waivers
ACA Section 1332 httns://www.cms.gov/CCIIO/Programs-and-lnitiatives/State-lnnovation
Waivers/Section 1332 State Innovation Waivers-.html
Other sources
Medicare waivers. Review by Kip Piper (consultant)
http://piperreport.com/blog/2008/08/12/rnedicare and medicaid demonstration waivers on
_
_
Medicare administrative contracting Section 1395kk
https://www.ssa.ov/OP Home/ssact/titlels/1874A.htm
Maryland Medicare waiver and proposal to add physicians and other providers in 2019.
http://www.baltimoresun.com/business/bs-bz-medicare-waiver-20170824-storv.html
ACA and New York integrated programs for dual-eligibles. Western New York Law Center
http://www.wnylc.com/health/entry/166/
John McDonough on ACA Innovation waivers (Journal of Health Policy, Politics and Law)
httos://read.dukeupress.edu/jhopl/article/39/S/1099/13650/Wvden-s-Waiver-State-
Innovation-on-Steroids
Rhode Island “Global Waiver”.
http //www.oh hs.ri.gov/med icaid/pdf/WaiverPresentation House8-08.odf
Rhode Island “Global Waiver” renewal.
http://www.nilin.state.nius/sfiscal/Dther%2ODocuments/Medicaid%200verview.odf
D

NEW Y*RKHEALTH ACT
The “EPISA Problem” FAQ
Q: The federal Employee Retirement Income Security Act (ERISA) was passed in 1974 to
provide security and uniformity across the nation for pension, health, and other benefits
provided by employers. ERISA declares that the federal government has priority in
governing such plans, and states cannot establish laws or programs that regulate or
otherwise impact such plans. Does the New York Health Act violate the provisions of
ERISA?
A—The-New-Y-ork-HealthAct-1%-Hk-does notsegulateemplover-provided-health- -—-- - -
benefits, nor does it direct employers to provide, or not provide, any particular benefits. MI
employers must pay the state-wide taxes that fund and make possible the NY Health
program, but employers are free to maintain, limit, or eliminate their existing programs.
Insurers that provide coverage for employer-based health insurance plans are regulated by state
insurance laws and regulations. However, what plans are offered by employers, and the extent of
coverage they offer, cannot be regulated by states. That is, federal preemption governs in that
case. (Note: Plans offered by employers that self-insure and take on risk themselves are not
considered insurance plans and are not subject to state regulation of any kind. They may bypass
state health care laws, reaulations, and certain direct taxes.).
The federal ERISA law can potentially preempt any state rule such as NYHA that “impacts”
such plans in any way. This would have a significant effect on the new program, since currently,
millions of workers in New York State get their health insurance benefits through employer-
provided plans.
NY Health will be better than any plan provided by an employer. Such plans usually require
significant cost-sharing, that is, they have large deductibles and co-pays. They also typically
have limited networks and benefits that are less comprehensive than those of NY Health.
Companies must also incur expenses managing such plans or contracting with a management
service to oversee them.
Federal law does not prevent a state from taxing businesses and employees, as long as the taxes
are broadly based and not intended to force actions by such employers. These taxes could include

those aiming to improve health care for all state residents. Under NYHA,, all employers will be
paying such a tax on behalf of their New York employees to help fund the NY Health program.
It would be expected, therefore, that most companies would no longer include their New York
resident employees in their health plans, since these employees will automatically qualify for the
new state health insurance program that will be both superior and less costly. However, NYHA
would not require them to stop offering their own program if they so desired.
The federal ERISA law is vaguely worded, and conflicting legal rulings make it unclear what
might be considered an action by the state that would “impact” an employer plan. Some might
argue that the NY Health tax, while itself iegal, would, in effect, be forcing an employer to
abandon its program in the state. Opponents of NY Health might well launch a law suit claiming
that ERISA preempts the new law because of its “impact” on employers.
Following the advice of legal experts on ERISA, the language of the NY Health Act is explicitly
employers, and their employees, for taxes paid on behalf of employees who live out of state but
work in New York [see Section 4(2)(e)(ii)j. Should a challenge still occur, the bill’s sponsors are
confident that, based upon a clear interpretation of legislative intent and past federal rulings, NY
Health will prevail. Should any part of the bill be ruled in violation of EMSA, an
accommodation that would exempt some employers, while inefficient and costly, would still
leave NY Health as a viable program and in the best interest of the vast majority of New
Yorkers.
Sources
Butler, Patricia A. (2009). Basic short guide to ERISA for health policy makers. National
Academy for State Health Policy. Available at https:/!nashp.or!erisa-preemption-prirner!. For
greater detail, see https:!/nashp.orz/erisa-preempti on-manual-state-health-policy-makers!.
Butler, Patricia A. (2014). What we can lean about Federal ERISA law from Maryland’s court
decision. Wisconsin Family Impact Seminars, University of Wisconsin-Madison. Available at
httv:!!wisfamilvimnacLorAvo-content!upIoads/20l4!l0!s wifis24col.odf
Kaminski, Janet L. (2007). ERISA pre-emption and state health care reform. Office of
Legislative Research Report. Connecticut General Assembly. Available at:
https:!!www.caa.ct.cov/2007!rt!2007-R-0 131 .htm
Hsiao. William, et al. (201 1). Act 128 Health System Reform Design: Achieving affordable
universal health care in Vermont. Report commissioned by the Vermont State Legislature.
Available athtft:ftwww.lea.state.vt.us!ifo.lhealthcare!FINAL%2OREPORT%2oHsiao%2OFinal%2OReport%2
0-%2017%20Februarv%20201 1 3.pdf

NEW YORKHEALTH ACT
Wait Times AQ
Q: Canada, the UK, and other countries are often held up as model single-payer health care
systems, yet we persistently hear of long wait times for appointments and services. Is this
what we can expect from a single-payer system?
A: Numerous careful studies have found that the insurance and financing system is not
responsible for long wait times. Excessive wait times can be found in all systems, single-
payer or multi-payer, public, mixed, or private, and can occur within systems by region, state,
province, county, municipality, or even individual medical facility or practice. The most
impGrta11tfatWrflffttiflWaittiflT€ciflZlUdWphSitiiflh&tage5,
funding constraints, and poor patient flow management.
The “wait time issue” is important. No one should have to suffer pain and anxiety while waiting
for diagnosis or treatment, or be forced to remain away from work or school for unnecessarily
long periods. Nor should they be placed at increased risk of death or disability.
The Organization for Economic Cooperation and Development (OECD), a grouping of the major
industrial countries, has undertaken extensive studies of their health care systems, including
variations in wait times. All of these system but that of the US provide universal coverage with
comprehensive financing and rich data sources. In all of them, government has a major role in
the health system, so waiting times for elective procedures have often become a contentious
political issue. In 2001-04, many of them were concerned about waiting times, and OECD began
reviewing policies for reducing waiting times.
A major study completed in 2013, Waiting Time Politics in the Health Sector: What Works?,
evaluated what progress had been made in that period. Not surprisingly, they found that
countries that spend more on health care, had increased their supply of physicians, and had
greater hospital capacity experienced shorter waiting times. In some cases, they had adopted
waiting time guarantees or targets to place pressure on those working in these systems, and
these incentives were effective when they were enforced.
Most important, these studies found that it was these capacity and budget factors, not the
nature of a country’s health care financing system, that determined the existence and length of
any delay for receiving care.
There has recently been great concern about excessive wait times in Veterans Administration
facilities. An independent assessment conducted for the American Legion found that “waft
I

times at the VA for new patient primary and specialty care are shorter than wait times reported
in focused studies of the private sector.” Overall, the report concluded, “VA wait times do not
seem to be substantially worse than non-VA waits.”
Emergency services
With respect to potentially life-threatening emergencies) all advanced countries use specially
designed and tested triage systems to ensure that high priority emergency room (ER)
admissions are treated immediately upon patient arrival in cases needing resuscitation, and in
less than an hour in cases considered of “emergent” or “urgent” acuity. Under most conditions,
high priority wait time targets are met in the vast majority of cases in all advanced countries.
If target times are not met, there are usually external reasons. In rural hospitals it might be due
to travel time for surgical specialists. In heavily-used urban hospitals, delays are often a
function of temporary or, in extreme cases, chronic ER crowding. Recent cutbacks in National
Health Service funding in England, as another example, have affected ER wait times.
true emergency problems. In a 2013 Commonwealth Fund study involving 11 advanced nations,
the US had the largest percentage of such patients, due primarily to inadequate or no
insurance.
The same study showed that the US and Canada had among the largest percentage of non-
urgent ER admissions due to difficulties getting appointments with primary care physicians. Yet
France, Australia, and the UK, all with universal health care systems, single-payer and multi-
payer, had 40-60% fewer such admissions. Germany and The Netherlands, also with
government-regulated universal systems, reported the overall percentage of ER use at only 25-
35% of that of ER5 in Canada and the US
Wait times for emergency services can vary widely among countries, and among regions and
hospitals within countries. There is no correlation based on national financing system. Single-
payer countries are among the best and the worst with respect to ER wait time. After years of
improvement, the National Health Service in England, for example, has experienced a recent
worsening of ER wait times, while the nearly identical program in Northern Ireland recently
reported that 95% of ER patients get a triage assessment within 8 minutes and are seen by a
medical professional within 29 minutes, both excellent results.
Wait times to see a primary care physician when sick
As noted above, a major reason for crowded ERs is a person’s inability to get an appointment
with a primary care physician to treat an acute condition which is not a true emergency. A
2016, 11-nation Commonwealth Fund survey found the following results for adults “able to get
same-day/next-day appointment when sick.”
2

Percent of adults who made a same-day or next day appointment when needed care,
2010
Netherlands
Austrzfla
Comparable County Average I1,I;i. IIflI
Sweden
United VJngdm
UnftetStates
___
•uiinn -
IIII liii III I I IIIlIllIlIllIll
____
III I II 111111 I_Cenada liii liii Ii • 1—.—-—-
u’te: 2015 ornmonweaah Fund International HealU Poticysuivey’ Get the data • PNC- Petersnti-Rntwr
Health System Tracker
Same-day or next-day access to primary care in Canada and the US is below the 11-nation
average, yet one has a public single-payer health insurance system and the other a private
market-based system. The fully nationalized UK system does better than both. In any case,
there is little difference among these countries having very different financing systems.
Managing patient flow is of critical importance in meeting wait time goals and there are many
aspects to this management Limited physician networks in the private US system are a typical
source of long wait times. Physicians refusing Medicaid patients create long delays in the US
public system as well, affecting wait times for the poor and driving them into emergency rooms.
The single-payer Medicare system in the US, on the other hand, has fewer network restrictions
and better primary care wait time results, on average) than both private and Medicaid patients.
The availability of evening and weekend hours can mitigate wait time problems as can the
availability of urgent care walk-in clinics. Increased use of nurse practitioners and physician
assistants can address wait time problems in areas with physician shortages or long travel
times.
Countries, regions within countries, and individual facilities and practices vary widely in their
ability to manage patient flow. The variation cuts across all modes of health insurance
financing.
3

Wait times for non-urgent care and elective procedures
Many of the complaints involving Canadian, British, and other single-payer or multi-payeruniversal systems relate to care that is not urgent or involves elective procedures. This couldbe first-time visits with a new provider, annual check-ups and screenings, visits to specialists, ornon-urgent or elective surgery such as hip and knee replacement or cataract surgery. Long waittimes in these situations can be a direct product of patient flow management as providers
prioritize care for those with more immediate needs, or can result from physician supplyconstraints due to many of the same factors as described above.
Following years of steadily improving service including reduced wait times, the Canadian
Medicare and English National Health Service systems have experienced substantial increases inwait times for non-urgent services since the recent recession. This has generated publicdiscontent and a barrage of press stories describing some of the worst cases. As a result, publicofficials have prioritized the issue, and both systems have begun using improved patient flow
management systems coupled with penalties or rewards for meeting, or failing to meet, theta?getrMdr im irlytrgaetpewd iwghs1nci’easetiwrEspotrswtopubl itt ternabout the problem.
Here are the data from the 2016 Commonwealth Fund study relating to non-urgent wait times:
Specialists & Surgery
“Waited two months or more for a specialist appointment”
R “Waited four months or more for elective surgery”
h 1k !I Ii h0 I’? f -
pC,
The US fares better in this category than Canada and England and even Norway and Sweden,
and much has been made of this fact, However, the universal social insurance systems ofFrance, Germany, and the Netherlands fare just as well as the US
4

The New York Health Act and wait times
The New York Health Act will remove many of the sources of long wait times in the US. There
will be no limited provider networks, and providers will no longer discriminate against Medicaid
and Medicare patients, since reimbursement rates will be standardized. There will be no
barriers to provider choice, creating a greater range of options, especially in urban areas with
greater concentrations of providers.
With reduced paperwork and administrative burden, providers will have more time to devote
to patient care and the management of patient flow. This will be especially important in the
face of the expected increase in utilization of health care services. Hospitals, too, will be
relieved of an administrative burden and be able to devote more resources to patient services.
In the longer run, NY Health planners will be able to work with the Governor and the
Commissioner of Health to increase the supply of providers in rural areas and to provide the
necessary capital for expanding patient care facilities and diagnostic technology where it is
neededr
- --
—-_____
________
Sources:
“Waiting Time Policies in the Health Sector What Works?,” OECD, Paris. 2013. Available at:
http://dx.doi.orcz/ 10.1787/97892641 79080-en
“Mirror, Mirror, On the Wall: How the Performance of the US Health Care System Compares
Internationally: 2014 Update”, Karen Davis, Kristof Stremikis, David Squires, and Cathy
Schoen, The Commonwealth Fund, June 2014. Available at:
https://www.commonwealthfund.oru/publications/fund-reports!201 4/iun!mirror-rnirror-wail-
201 4-update-how-us-heafth-care-svstem
“Minor. Mirror 2017: International Comparison Rflects Flaws and Opportunities for Better US
Health Care”, Eric C. Schneider, Dana 0. Samak, David Squires,
Amav Shah, and Michelle M. Doty, Commonwealth Fund, Available at:
www.commonwealthfund.org/interactives/2017/july/mirror-rnirror -
“VA Health Care: A System Worth Saving”, Phillip Longman and Suzanne Gordon, prepared for
the American Legion. Available at: https://wwwAegion.org/publications/238801/lonman-
ordon-report-va-hea1thcare-svstem-worth-savinq
Northern Ireland Department of Health. (2017). Emergency care waiting times statistics (Jan
Mar 2017). Available at: https://www.health-ni.gov.uk/news/emergency-care-waitin-time
statistics-january-march-2017
S

Lagasse, Jeffrey. (2017). Hospital wait times longer for Medicaid patients than privately insured,Health Affairs study finds. Heafthcare Finance. Available at:htt://www. healthcarefinancenews,com/news/hospita Is-wa It-times-longer-medicaId-patientsørivately-insured-health-affairs-studv-flnds,
Q’Hara, Mary. (Aug. 25, 2015). Fed up with NHS wait times? It’s even worse in the U.S. TheGuardian. Available at: https://www.theguardian.com/societv/2015/aug/25/go-apoointment-waiting-times-in-us-worse-than-nhs
6

New York Health Act (A 5248, S3577)
Dear Senators and Assembly Members,
The twenty stories collected in this book are typical of the nearly fifty we’ve publishedover the past year for This Is the Bronx.
They tell stories of family members, friends, and neighbors — people representative ofyour constituents who suffer under our current broken healthcare payment system, peoplewho have told pollsters that healthcare continues to be their most urgent election issue.
Most of these stories are about people who thought their job-based insurance would keepthem safe. ft didn’t. It can’t. The current multi-payer private-insurance system has abusiness model that prioritizes profits over patient health, too opaque to manage orimprove. Few New Yorkers have any idea how vulnerable we are.
We are vulnerable because healthcare costs are consuming our economy: about 12% ofGDP 20 years ago; almost 18% today; projected to hit 32% within a decade. In 2000, thecost of family coverage through employment was 13% of the median wage. Today, it is50% of the median wage.
The average family spends more on premium contributions than on food for a year; moreon healthcare premiums plus out-of-pocket health expenses than on housing. Becauseemployers can’t afford it either, they are shifting an increasing share of costs toemployees and reducing the number of covered workers (down 17% since 2000). Bydiscouraging routine medical care, these uncontrolled costs torpedo our public health.
We are volunteers working to pass the New York Health Act, so that all but the wealthiestNew Yorkers will spend less for healthcare and, finally, to control costs by cutting at least17% of wasteful spending that benefits no one’s health, that frustrates physicians, thatreduces their clinical time with patients.
Even more important than monetary savings, however, will be the security of having allfinancial obstacles to care removed — improving public health, increasing productivity,and strengthening families. New Yorkers, like those in these stories, will no longer haveto choose between seeing a doctor and paying rent, filling prescriptions for chronicdisease and buying food, halting an ER doctor’s life-saving treatment for a heart attackand impoverishing their family.
We hope that you — as you read these stories — will hear echoes of people you know.Almost every family has a story similar to these. Enacting NY Health will allow NYS tolead our nation — demonstrating that American exceptionalism doesn’t require poorhealth outcomes at unsustainable prices. Like Tommy Douglas in Saskatchewan, we canlight the way to universal, comprehensive, affordable healthcare.
Thank you for listening to your constituents.- av-bavu
N YHA.Estrin(ö)umail.com NYHA.Estergtiest(1igmail.corn