Alloimmune hemolytic anemia
53
TABLE OF CONTENTS: ALLOIMMUNE HEMOLYTIC ANEMIA.............................2 INTRODUCTION:........................................... 2 CLASSIFICATION OF IMMUNE HEMOLYTIC ANEMIA...............3 ALLOIMMUNIZATION FROM TRANSFUSION.......................4 PATHOPHYSIOLOGY:........................................6 CLINICAL PRESENTATION:....................................8 LABORATORY STUDIES:.......................................9 MANAGEMENT:........................................... 10 ALLOIMMUNIZATION DURING PREGNANCY (RhD ALLOIMMUNIZATION12 BACKGROUND............................................ 13 PATHOPHYSIOLOGY:.......................................13 CAUSES OF MATERNAL ALLOIMMUNIZATION:.....................14 HEMOLYTIC DISEASE OF INFANTS & NEWBORNS (HDFN).........16 PATHOPHYSIOLOGY:.......................................17 CLINICAL PRESENTATION:...................................18 LABORATORY STUDIES:......................................19 MANAGEMENT:........................................... 22 DRUG INDUCED ALLOIMMUNIZATION..........................29 PATHOGENESIS:...........................................30 SEROLOGICAL DIAGNOSIS:...................................32 1
-
Upload
drkhadija-habib -
Category
Health & Medicine
-
view
5.566 -
download
3
description
Transcript of Alloimmune hemolytic anemia

TABLE OF CONTENTS:
ALLOIMMUNE HEMOLYTIC ANEMIA................................................................2
INTRODUCTION:........................................................................................................2
CLASSIFICATION OF IMMUNE HEMOLYTIC ANEMIA.................................3
ALLOIMMUNIZATION FROM TRANSFUSION..................................................4
PATHOPHYSIOLOGY:................................................................................................6
CLINICAL PRESENTATION:.....................................................................................8
LABORATORY STUDIES:...........................................................................................9
MANAGEMENT:........................................................................................................10
ALLOIMMUNIZATION DURING PREGNANCY (RhD
ALLOIMMUNIZATION12
BACKGROUND..........................................................................................................13
PATHOPHYSIOLOGY:..............................................................................................13
CAUSES OF MATERNAL ALLOIMMUNIZATION:..............................................14
HEMOLYTIC DISEASE OF INFANTS & NEWBORNS (HDFN)......................16
PATHOPHYSIOLOGY:..............................................................................................17
CLINICAL PRESENTATION:...................................................................................18
LABORATORY STUDIES:.........................................................................................19
MANAGEMENT:........................................................................................................22
DRUG INDUCED ALLOIMMUNIZATION..........................................................29
PATHOGENESIS:......................................................................................................30
SEROLOGICAL DIAGNOSIS:..................................................................................32
REFERENCES:..........................................................................................................33
1

ALLOIMMUNE HEMOLYTIC ANEMIA
INTRODUCTION:
Alloimmunization is defined as, “an immune response generated in an individual by
an alloantigen from a different individual.”
In alloimmune hemolytic anemia, antibodies are produced against the red blood cells
a person receives in a blood transfusion. If the blood type used for the transfusion is
different than the recipient's blood type, the recipient's immune system can develop
antibodies that attack and destroy the transfused blood cells.
Alloimmune antibodies also can develop as a result of the mixing of blood between a
pregnant woman and her baby at delivery. If the mother's blood type is Rh-negative
and the baby's is Rh-positive, the mother can produce antibodies against the baby's
blood type. If a mother develops anti-Rh antibodies as a result of one pregnancy, they
can cross the placenta during the next pregnancy and harm the fetus. To prevent this, a
medicine called RhoGam can be given at the time of delivery to block the mother's
body from developing antibodies against the baby's blood type.
Certain drugs can cause a reaction that develops into hemolytic anemia. These drugs
include high doses of penicillin and related drugs, acetaminophen, quinine and other
drugs to treat malaria, anti-inflammatory drugs, and levodopa.
Thus Alloimmunization can be broadly divided into three main categories:
1. Alloimmunization after transfusion
2. Maternal Alloimmunization or iso-immunization
2

3. Drug induced alloimmunization
CLASSIFICATION OF IMMUNE HEMOLYTIC
ANEMIA
Antigen Antibody Disease Association
Autoimmune Warm antibody Primary Secondary
Idiopathic Autoimmune disease(SLE)Lymphoproliferative disorders(EBV)Ovarian cystsSome cancersDrugs
Cold antibody Cold haemagglutinin diseaseCold antibody syndromes
Infections, lymphoproliferative disorders
Donath– Landsteiner
Paroxysmal cold hemoglobinuria
Post viral & syphilis
Alloimmune Induced by red cell antigens
Hemolytic transfusion reactionsHDNPost-stem cell allograft
Drug dependent Antibody/macrophage mediatedAntibody/complement mediatedMembrane modification
3

ALLOIMMUNIZATION FROM TRANSFUSION
Allogeneic blood transfusion is a form of temporary transplantation. This procedure
introduces a multitude of foreign antigens and living cells into the recipient that
persist for a variable time. A recipient who is immuno-competent often mounts an
immune response to the donor antigens, resulting in various clinical consequences,
depending on the blood cells and specific antigens involved. The antigens most
commonly involved are classified in the following categories:
Human leukocyte antigens (HLAs)
class I shared by platelets and leukocytes
class II present on some leukocytes
Granulocyte-specific antigens
Platelet-specific antigens (human platelet antigen [HPA])
RBC-specific antigens.
CONSEQUENCES OF ALLOIMMUNIZATION TO BLOOD:
The consequences of alloimmunization to blood include the following clinical
manifestations:
Alloimmunization against RBCs
Acute intravascular hemolytic transfusion reactions (rarely a
consequence of alloimmunization and almost always caused by ABO
antibodies)
Delayed hemolytic transfusion reactions (DHTRs) (hemolysis caused
by RBC all antibodies at least 24 hours post transfusion)
4

Hemolytic disease in newborns (mother's alloimmunization against
fetal antigens, most often resulting from previous pregnancies)
Alloimmunization against platelets (platelet-specific or HLA class I antigens)
Refractoriness to platelet transfusion (an increase in the platelet count
after platelet transfusion that is significantly lower than expected e.g
< 30% of predicted after 10-60 min or < 20% at 18-24h post
transfusion)
Post transfusion purpura (thrombocytopenia after transfusion of red
cells or other platelet-containing products, associated with presence of
platelet allo-antibodies)
Neonatal alloimmune thrombocytopenia (mother's alloimmunization
against fetal antigens, most often resulting from previous pregnancies)
Alloimmunization against granulocytes
(granulocyte-specific or HLA antigens)
Refractoriness to granulocyte transfusion
Febrile non-hemolytic transfusion reactions
Transfusion-related acute lung injury (i-e a transfusion reaction in
which donor HLA antibodies react against recipient antigens)
Transplant rejection
Alloimmunization against HLA antigens
5

Alloimmunization against blood cell antigens (in bone marrow
transplantation)
DHTR and refractoriness to platelet transfusions are most important. Refractoriness to
granulocyte transfusions involves either anti-HLA or granulocyte-specific antibodies
and is similar to platelet refractoriness, except that refractoriness to granulocyte
transfusions results in the patient failing to respond to the granulocyte transfusions.
Granulocyte transfusions are rarely used.
PATHOPHYSIOLOGY:
The main mechanism for alloimmunization to antigens present in transfused cells may
involve presentation of the donor antigens by donor antigen–presenting cells (APCs),
i-e monocytes, macrophages, dendritic cells, B cells, to recipient T cells. Recognition
of the MHC class I alloantigens by CD4+ recipient T cells and their subsequent
activation requires a co-stimulatory signal from either the donor or recipient APCs.
Alloimmunization by non–leukoreduced platelets involves shared donor HLA
antigens (HLA-restricted) and live functional donor APCs. The TH 2 subset of CD4+ T
helper cells secretes interleukin (IL)–4, IL-5, IL-6, and IL-10; activates B cells; and
initiates the antibody response.
Refractoriness to platelet transfusions:
The presence of HLA antibodies on the platelet surface is the most common cause of
platelet refractoriness. Other non-HLA antigens present on the platelet surface (eg,
platelet-specific antigens, HPA) are also involved in a number of cases. Patients not
previously sensitized develop antiplatelet antibodies approximately 3-4 weeks after
the transfusion. Patients previously immunized by transfusion, pregnancy, or organ
6

transplantation develop antiplatelet antibodies as early as 4 days after transfusion.
Macrophages in the liver, spleen, and other tissues of the mononuclear phagocyte
system phagocytize and destroy antibody-coated platelets. Risk factors for developing
antiplatelet antibodies include:
presence > 1 million donor leukocytes in transfused products
transfusing ABO-mismatched platelets
the presence of an intact immune system (i-e, absence of cytotoxic or
immunosuppressive therapy),
Female sex (approximately 75% of cases)
History of multiple transfusions (>20).
Delayed hemolytic transfusion reactions:
DHTRs occur between 24 hours and 3 months (frequently 2 wk) after transfusion and
usually represent a secondary immune response in patients previously immunized by
transfusion or pregnancy. In very rare cases, brisk primary immune response can
result in DHTR after an initial transfusion. Anti-RBC antibody titers frequently (about
50% of the patients with alloimmunization) drop below detectable levels, allowing
incompatible units to be transfused. Transfusion with incompatible RBCs results in
re-stimulation of memory cells and an increase in antibody titer. Antibodies bind to
the surface of RBCs and, depending on the number of antigen-antibody interactions,
activate complement with deposition of C3b usually more than 105 antigenic sites per
cell are required for potent complement activation.
Rarely, binding of immunoglobulin M antibodies to RBCs activates the classic
complement pathway and leads to intravascular hemolysis. RBCs coated with
immunoglobulin G antibodies and/or complement bind to C3b and immunoglobulin
7

Fc receptors present on mononuclear phagocytes and are destroyed by phagocytosis
(i-e extravascular hemolysis). Immunoglobulin G antibodies that efficiently activate
complement (eg, those in Kidd and Duffy systems) tend to cause more intense
extravascular hemolysis compared with antibodies that do not efficiently activate
complement (eg, Rh and Kell).
CLINICAL PRESENTATION:
Delayed hemolytic transfusion reactions:
Hemolysis is usually extravascular, but in some cases, a component of
intravascular hemolysis is present.
Most cases manifest during the second week after transfusion, but the reaction
can occur from 24 hours to 3 months after the transfusion.
Many patients are asymptomatic, and the condition is detected only by
laboratory methods.1
In some patients, fever and/or chills (50%), jaundice (10%), pain (3%), and
dyspnea (1%) can occur.
Rarely, cases may be complicated with renal failure (6%) or disseminated
intravascular coagulation (1%).
In patients with sickle cell disease, a DHTR can precipitate sickle crisis.
Refractoriness to platelet transfusions:
Frequently, patients with refractoriness to platelet transfusion are
asymptomatic and diagnosed by laboratory methods; however, failure to
achieve haemostatic levels of platelets may preclude these patients from
important procedures, including bone marrow transplantation. 8

Alloimmunization should be avoided at all costs in candidates for bone
marrow transplantation.
Preexisting bleeding resulting from thrombocytopenia may persist after
transfusion of an appropriate therapeutic dose of platelets.2 Rarely,
spontaneous bleeding may occur after prophylactic transfusion of platelets.
LABORATORY STUDIES:
Delayed hemolytic transfusion reactions:
The most reliable laboratory sign is a failure to observe the expected post
transfusion increase in blood hemoglobin levels (approximately 1 g/dl/U) in
the absence of bleeding.
Laboratory signs of hemolysis include elevated lactate dehydrogenase, indirect
bilirubin, and reticulocyte levels and decreased hematocrit and haptoglobin
levels.
Intravascular hemolysis is characterized by the presence of free plasma
hemoglobin and possibly hemosiderinuria.
The results of direct and indirect Coombs test are often positive.
Alloantibodies can be eluted from RBCs, and their specificity can be
determined. Often (about 15-20%), patients with DHTR have multiple
antibodies and some may be detectable only by elution.
Refractoriness to platelet transfusions:
Refractoriness to platelet transfusions is defined as repeated failure to achieve
the expected increment in platelet count after 2 or more platelet transfusions.
9

The expected increment can be calculated based on the number of platelets
transfused and the patient's blood volume
In general, alloimmunization results in the rapid removal of platelets and in
lower counts at 10 minutes to 1 hour post transfusion, whereas non-immune
causes mostly affect the 4- to 24-hour post transfusion count. Mild
alloimmunization, however, can be present with 1-hour increments within the
reference range.
The percentage of cells to which the patient's serum reacts is referred to as the
panel-reactive antibody (PRA) level. PRA values greater than 20% indicate
significant alloimmunization to HLA antigens and correlate with an increased
risk for platelet refractoriness.
The presence of antiplatelet antibodies can be demonstrated by flow cytometry
or by immunoassays such as the modified antigen capture enzyme-linked
assay, the solid-phase RBC adherence assay, and the monoclonal antibody
immobilization of platelet antigens assay. Most of these assays permit
screening for HLA and HPA antibodies as well as specific identification of the
most commonly involved HPA antigens.
A negative result from platelet antibody screening indicates non-immune
causes of refractoriness.
MANAGEMENT:
Delayed hemolytic transfusion reactions:
Most patients tolerate DHTR well and only require observation and supportive
care.
10

Transfusion support with antigen-negative RBCs. If these RBCs are not
available, weigh the risk of further hemolysis against the indications for
transfusion.
If the load of antigen-positive packed RBCs is large (>5 U), consider
exchange transfusion.
Administer intravenous human immunoglobulin (IVIG) to block further
hemolysis in cases in which antigen-positive blood is transfused.
Refractoriness to platelet transfusions:
Avoiding the use of platelet transfusions as much as possible is important in
allo-immunized patients. Preventive transfusions are not recommended.
Measures to minimize the likelihood and extent of bleeding (eg, rapid
treatment of infection; avoidance of invasive procedures; correction of
coagulation deficiencies, anemia, and renal insufficiency; use of
antifibrinolytic agents) should be used extensively.
After diagnosing alloimmune platelet refractoriness, use the sequence of
measures that follows, initiating each subsequent intervention if the previous
one fails.
o Rule out non-immune, autoimmune, and drug-related causes of platelet
refractoriness, or treat accordingly.
o Consider alternatives to platelet transfusion to control bleeding,
including the use of antifibrinolytic agents such as alpha-aminocaproic
acid, or activated recombinant factor VIIa3
o Transfuse ABO-compatible fresh (aged < 48 h) platelet concentrates.
o Transfuse with platelets from blood relatives.
11

o Select HLA-matched platelets. Perform HLA typing of patients who
receive multiple transfusions before they become pancytopenic.
o Select cross-matched platelets.
o The use of HPA1a/5b-negative platelets has been successful in cases of
post-transfusion purpura and neonatal platelet alloimmunization.
o Pre-treat with IVIG before transfusion. IVIG pretreatment can result in
successful recovery after platelet transfusion in patients who are
alloimmunized.
o Use high-dose platelet transfusion. Empirical use of high doses of
random platelet units may result in titration of the antibody,
overwhelming of the mononuclear-phagocyte system, and increased
survival of transfused platelets.
o Attempt large-volume plasmapheresis.
o Consider administering immunosuppressive drugs. While steroids are
not effective the use of vincristine and cyclosporin A has been
successful but requires 2-3 weeks to take effect.
ALLOIMMUNIZATION DURING PREGNANCY
(RhD ALLOIMMUNIZATION)
Maternal alloimmunization, also known as isoimmunization, occurs when a woman's
immune system is sensitized to foreign erythrocyte surface antigens, stimulating the
production of immunoglobulin G (IgG) antibodies. The most common routes of
maternal sensitization are via blood transfusion or fetomaternal hemorrhage (i-e
12

transplacental passage of fetal erythrocytes) associated with delivery, trauma,
spontaneous or induced abortion, ectopic pregnancy, or invasive obstetric procedures.
These antibodies can cross the placenta during pregnancies in alloimmunized women
and, if the fetus is positive for these specific erythrocyte surface antigens, result in
hemolysis of fetal erythrocytes and anemia. This, in turn, can lead to potentially
disastrous consequences for the fetus, such as hydrops fetalis, a high-output cardiac
failure syndrome.
BACKGROUND:
Among the more than 50 different antigens capable of causing maternal
alloimmunization and fetal hemolytic disease, the Rhesus (Rh) blood group system is
the most common. The Rh blood system is comprised of the c, C, D, e, and E
antigens. The D antigen of the Rh blood group system (Rh D) causes most cases of
severe hemolytic disease. The incidence of fetuses at risk for anemia due to maternal
alloimmunization to red cell antigens has decreased dramatically since the institution
of routine anti-D immune globulin (RhoGAM) prophylaxis for Rh-negative women in
the 1960s. A review of birth certificate data in 2003 reported the incidence of Rh
sensitization to be approximately 6.8 per 1000 live births.4
EPIDEMIOLOGY:
The prevalence of the Rh D–negative blood type is dependent on ethnicity with
whites having the highest prevalence and Asians and American Indians having the
lowest.
Rates of Rh D negativity among ethnic and racial groups are as follows:
13

White - 15-16%
African American - 8%
African - 4%
Basque (region of Spain/France) - 30-35%
Asian - Less than 1%
Asian American - 1%
American Indian/Inuit - 1-2%
Eurasian - 2-4%
PATHOPHYSIOLOGY:
The risk of alloimmunization in a susceptible Rh D–negative woman is significantly
affected by several factors. These factors include the volume of fetomaternal
hemorrhage, the degree of maternal immune response, concurrent ABO
incompatibility, and fetal homozygosity versus heterozygosity for the D antigen.
Fetomaternal hemorrhages have been demonstrated to occur in as many as 75% of
pregnancies, with the frequency increasing as gestation advances and with most cases
occurring during delivery. If transplacental passage of fetal erythrocytes is suspected,
the rosette screening test is used to determine the presence of a fetomaternal
hemorrhage. When a large hemorrhage is suspected, the Kleihauer-Betke test is used
to quantify the volume of hemorrhage so that an appropriate dose of anti-D IgG can
be administered. Hemorrhage volumes sufficient to cause alloimmunization are
produced in 15-50% of births. This volume of fetal blood, which, in more than 50% of
intrapartum cases can be as small as 0.1mL and in rare cases can exceed 30mL, varies
depending on the degree of maternal immune response.
14

ABO blood group status also affects the risk of alloimmunization. With an ABO-
compatible fetus, the overall risk of alloimmunization if not treated with anti-D IgG is
approximately 16%. However, in an ABO-incompatible fetus, the risk is only 1.5-2%.
The protective effect conferred by ABO incompatibility is believed to be due to
maternal destruction and subsequent clearance of the ABO-incompatible fetal
erythrocytes before Rh sensitization can occur.
Approximately 17% of Rh D–negative women who deliver an Rh D–positive fetus
become alloimmunized if anti-D IgG is not administered appropriately. Of note,
because anti-D IgG prophylaxis has reduced the risk of sensitization to less than 1%
of susceptible pregnancies, other alloantibodies have increased in relative importance.
These include antibodies to other antigens of the Rh blood group system (i-e c, C, e,
E) and other atypical antibodies known to cause severe anemia, such as anti-Kell (i-e
K, k), anti-Duffy (i-e Fya), and anti-Kidd (i-e Jka, Jkb).
Despite the dramatic success of anti-D IgG prophylaxis protocols, prevention is not
universal and 0.27% of susceptible women still become Rh D alloimmunized. One
reason for this is failure to follow recommended protocols. Furthermore, a 0.1-0.2%
rate of spontaneous immunization occurs despite prophylaxis. These cases have
been observed in pregnancies in which no prior overt sensitizing events have
occurred. Finally, alloimmunization involving atypical blood groups (eg, Kell and
c blood groups) is not yet preventable. Therefore, understanding and using available
predictive measures and treatment modalities for hemolytic disease of the fetus and
newborn is essential, as is ensuring that the Rh-alloimmunized pregnancy is properly
managed.
15

CAUSES OF MATERNAL ALLOIMMUNIZATION:
Blood transfusion
Fetomaternal hemorrhage
Antepartum
Intrapartum
Abortion
Therapeutic
Spontaneous
Molar pregnancy
Ectopic pregnancy
Placental abruption
Abdominal trauma
Obstetric procedures
Amniocentesis
Chorionic villus sampling (CVS)
Percutaneous umbilical blood sampling
External cephalic version
Manual removal of the placenta
HEMOLYTIC DISEASE OF INFANTS &
NEWBORNS (HDFN)
The perinatal effects of maternal Rh alloimmunization are now referred to as
hemolytic disease of the fetus and newborn and fetal manifestations of the disease are
16

more appreciated with newer technologies such as cordocentesis and fetal
ultrasonography.
PATHOPHYSIOLOGY:
After sensitization, maternal anti-D antibodies cross the placenta into fetal circulation
and attach to Rh antigen on fetal RBCs, which form rosettes on macrophages in the
reticuloendothelial system, especially in the spleen. These antibody-coated RBCs are
lysed by lysosomal enzymes released by macrophages and natural killer lymphocytes
and are independent of the activation of the complement system.
Reticulocytosis is noted when fetal Hb deficit exceeds 2 gm/dl compared with
gestational age norms. Tissue hypoxia develops as fetal anemia becomes severe.
When the hemoglobin (Hb) level drops below 8 g/dl, a rise in umbilical arterial lactate
occurs. When the Hb level drops below 4g/dl, increased venous lactate is noted.
Hydrops fetalis occurs when fetal Hb deficit exceeds 7 g/dl, and starts as fetal ascites
and evolves into pleural effusions and generalized edema. The various mechanisms
responsible for hydrops are hypoalbuminemia secondary to depressed liver function,
increased capillary permeability, iron overload secondary to hemolysis, and increased
venous pressures due to poor cardiac function.5
Hemolysis associated with ABO incompatibility exclusively occurs in type-O mothers
with fetuses who have type A or type B blood. Hemolysis due to anti-A is more
common than hemolysis due to anti-B.
CLINICAL PRESENTATION:
17

An infant born to an alloimmunized mother shows clinical signs based on the severity
of the disease. The typical diagnostic findings are jaundice, pallor,
hepatosplenomegaly, and fetal hydrops in severe cases. The jaundice typically
manifests at birth or in the first 24 hours after birth with rapidly rising unconjugated
bilirubin level. Occasionally, conjugated hyperbilirubinemia is present because of
placental or hepatic dysfunction in those infants with severe hemolytic disease.
Anemia is most often due to destruction of antibody-coated RBCs by the
reticuloendothelial system, and, in some infants, anemia is due to intravascular
destruction. The suppression of erythropoiesis by intravascular transfusion (IVT) of
adult Hb to an anemic fetus can also cause anemia. Extramedullary hematopoiesis can
lead to hepatosplenomegaly, portal hypertension, and ascites.
Anemia is not the only cause of hydrops. Excessive hepatic extramedullary
hematopoiesis causes portal and umbilical venous obstruction and diminished
placental perfusion because of edema. Increased placental weight and edema of
chorionic villi interfere with placental transport. Fetal hydrops results from fetal
hypoxia, anemia, congestive cardiac failure, and hypoproteinemia secondary to
hepatic dysfunction. Commonly, hydrops is not observed until the Hb level drops
below approximately 4 g/dl (Hct < 15%)5 . Clinically significant jaundice occurs in as
many as 20% of ABO-incompatible infants.
CAUSES:
Common causes of hemolytic disease of the newborn
Rh system antibodies
18

ABO system antibodies
Uncommon causes - Kell system antibodies
Rare causes
Duffy system antibodies
MNS and s system antibodies
No occurrence in hemolytic disease of the newborn
Lewis system antibodies
P system antibodies
LABORATORY STUDIES:
CBC COUNT:
Anemia: Measurements are more accurate using central venous or arterial
samples rather than capillary blood.
Increased nucleated RBCs, reticulocytosis, polychromasia, anisocytosis,
spherocytes, and cell fragmentation
The reticulocyte count can be as high as 40% in patients without
intrauterine intervention.
The nucleated RBC count is elevated and falsely elevates the leukocyte
count, reflecting a state of erythropoiesis.
Spherocytes (< 40%) are more commonly observed in cases of ABO
incompatibility. Glucose does not correct the autohemolysis in ABO
incompatibility unlike hereditary spherocytosis.
In severe hemolytic disease, schistocytes and burr cells may be
observed, reflecting ongoing disseminated intravascular coagulation.
19

A low reticulocyte count is observed in fetuses provided with
intravascular transfusion in utero and with Kell alloimmunization.
Neutropenia: This condition seems to be secondary to stimulation of
erythropoiesis in favor of myelopoiesis. However, neutrophilia can be
observed after intrauterine transfusion because of an increase in circulating
cytokines (granulocyte-macrophage colony-stimulating factor).
Thrombocytopenia: This condition is common, especially after intrauterine or
exchange transfusions because of platelet-poor blood product and suppression
of platelet production in favor of erythropoiesis.
HYPOGLYCEMIA:
Hypoglycemia is common and is due to islet cell hyperplasia and hyperinsulinism6
The abnormality is thought to be secondary to release of metabolic byproducts such as
glutathione from lysed RBCs. Hypokalemia, hyperkalemia, and hypocalcemia are
commonly observed during and after exchange transfusion.
SEROLOGIC TEST FINDINGS:
Indirect Coombs test and direct antibody test results are positive in the mother
and affected newborn. Unlike Rh alloimmunization, direct antibody test
results are positive in only 20-40% of infants with ABO incompatibility.7 In a
recent study,8 positive direct antibody test findings have a positive predictive
value of only 23% and a sensitivity of only 86% in predicting significant
hemolysis and need for phototherapy, unless the findings are strongly positive
(4+). This is because fetal RBCs have less surface expression of type-specific
20

antigen compared with adult cells. A prospective study has shown that the
titers of maternal immunoglobulin G (IgG) anti-A or anti-B may be more
helpful in predicting severe hemolysis and hyperbilirubinemia.
Although the indirect Coombs test result (neonate's serum with adult A or B
RBCs) is more commonly positive in neonates with ABO incompatibility, it
also has poor predictive value for hemolysis. This is because of the differences
in binding of IgG subtypes to the Fc receptor of phagocytic cells and, in turn,
in their ability to cause hemolysis.
IgG2 is more commonly found in maternal serum but has weak lytic activity,
which leads to the observation of little or no hemolysis with a positive direct
antibody test result. On the other hand, significant hemolysis is associated
with a negative direct antibody test result when IgG1 and IgG3 are
predominant antibodies, which are in low concentration but have strong lytic
activity, crossing to neonatal circulation.
In newborns with hemolytic disease due to anti-c or anti-C antibodies, direct
antibody test results may be negative, and the diagnosis is established after
indirect Coombs testing.
IMAGING STUDIES:
High-resolution ultrasonography has been a major advance in detection of early
hydrops and has also reduced the fetal trauma and morbidity rate to less than 2%
during percutaneous umbilical blood sampling (PUBS) and placental trauma during
amniocentesis. High-resolution ultrasonography has been extremely helpful in
directing the needle with intraperitoneal transfusion (IPT) and intravascular
transfusion (IVT) in fetal location.21

Table 2: Comparison oh Rh and ABO incompatibility:
CHARACTERISTICS Rh ABO
Clinical Aspects First born 5% 50%
Later pregnancies More severe No increased
severity
Still born/hydrops Frequent Rare
Severe anemia Frequent Rare
Jaundice Moderate to
severe/frequent
Mild
Late anemia Frequent Rare
Laboratory
Findings
Direct antibody test Positive Weakly positive
Indirect Coombs
test
Positive Usually positive
Spherocytosis Rare Frequent
MANAGEMENT:
Management of maternal alloimmunization
As a rule, serial maternal antibody titers are monitored until a critical titer of 1:32,
which indicates that a high risk of fetal hydrops has been reached. At this point, the
fetus requires very intense monitoring for signs of anemia and fetal hydrops. In Kell
22

alloimmunization, hydrops can occur at low maternal titers because of suppressed
erythropoiesis, and, thus, a titer of 1:8 has been suggested as critical.
Maternal titers are not useful in predicting the onset of fetal anemia after the first
affected gestation. Large differences in titer can be seen in the same patient between
different laboratories, and a newer gel technique produces higher titer results than the
older tube method. Therefore, standard tube methodology should be used to determine
critical titer, and a change of more than 1 dilution represents a true increase in
maternal antibody titer. For all the antibodies responsible for hemolytic disease of the
newborn (HDN), a 4-fold increase in any antibody titer is typically considered a
significant change that requires fetal evaluation9.
When indicated, amniocentesis can be performed as early as 15 weeks' gestation
(rarely needed in first affected pregnancy before 24 weeks' gestation) to determine
fetal genotype and to assess the severity. Maternal and paternal blood samples should
be sent to the reference laboratory with amniotic fluid sample to eliminate false-
positive results (from maternal pseudogene or Ccde gene) and false-negative results
(from a rearrangement at the RHD gene locus in the father).
Fetal Rh-genotype determination in maternal plasma has become routine in other
countries and will soon be offered in the United States. Fetal cell free DNA accounts
for 3% of the total circulating maternal plasma DNA. It is subjected to real-time PCR
for the presence of RHD gene-specific sequences and has been found to be accurate in
99.5% of cases. The SRY gene (in the male fetus) and DNA polymorphisms in the
general population (in the female fetus) are used as internal controls to confirm the
fetal origin of the cell-free DNA.10
23

Serial amniocentesis is begun at 10-14 day intervals to monitor the severity of the
disease in the fetus. All attempts should be made to avoid transplacental passage of
needle which can lead to fetomaternal hemorrhage (FMH) and a further rise in
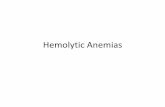
antibody titer. Serial delta-OD 450 values are plotted on the Queenan chart or the
extended Liley chart to evaluate the risk of fetal hydrops.
Traditional management of alloimmunized patients with serial amniocenteses (as
depicted below) was based on which zone the delta OD450 measurement falls into on
the Liley or Queenan curves. Evidence from several studies, including Liley's original
work, indicates that mild or no hemolytic disease occurs in zone 1; intermediate
disease occurs in zone 2 (transitional between mild and severe hemolysis); and severe
disease, including the development of hydrops within the week, occurs in zone 3.
24

Based on this evidence, once serial measurements are started, if a zone 1 reading is
obtained, monitoring the delta OD450 approximately every 3 weeks is reasonable.
However, with a trend into zone 2, the frequency of testing should increase to every 1-
2 weeks depending on the steepness of the slope of the curve and the closeness of the
measurement to zone 3.
Early ultrasonography is performed to establish correct gestational age. Frequent
ultrasonographic monitoring is also performed to assess fetal well-being and to detect
moderate anemia and early signs of hydrops.
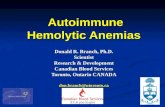
The peak systolic middle cerebral artery (MCA) Doppler velocity has proved to be a
reliable screening tool to detect fetal anemia. The MCA is easily visualized with
color-flow Doppler; pulsed Doppler is then used to measure the peak systolic velocity
just distal to its bifurcation from the internal carotid artery. Because the MCA velocity
increases with advancing gestational age, the result is reported in multiples of median
(MOMs). In recent studies, the sensitivity for detection of moderate and severe fetal
anemia has been proven to be 100%, with a false-positive rate of 10% at 1.5
MOM.11 It has been shown to reduce the need for invasive diagnostic procedures such
as amniocentesis and cordocentesis by more than 70%.12
MCA Doppler studies can be started as early as 18 weeks' gestation but are not
reliable after 35 weeks' gestation13 . It has also been used to time the subsequent fetal
transfusion and to diagnose anemia from multiple causes, such as in twin-twin
transfusion. The MCA slope from 3-weekly readings is now used to predict fetal risk
for severe anemia14
25

26

Management of the sensitized neonate
Mild hemolytic disease accounts for 50% of newborns with positive direct antibody
test results. Most of these newborns are not anemic (cord hemoglobin [Hb] >14 g/dL)
and have minimal hemolysis (cord bilirubin < 4 mg/dL). Apart from early
phototherapy, they require no transfusions. However, these newborns are at risk of
27

developing severe late anemia by 3-6 weeks of life. Therefore, monitoring their Hb
levels after hospital discharge is important.
Moderate hemolytic disease accounts for approximately 25% of affected neonates.
Moderate hemolytic disease of newborn is characterized by moderate anemia and
increased cord bilirubin levels. These infants are not clinically jaundiced at birth but
rapidly develop unconjugated hyperbilirubinemia in the first 24 hours of life.
Peripheral smear shows numerous nucleated RBCs, decreased platelets, and,
occasionally, a large number of immature granulocytes. These newborns often have
hepatosplenomegaly and are at risk of developing bilirubin encephalopathy without
adequate treatment. Early exchange transfusion with type-O Rh-negative fresh RBCs
with intensive phototherapy is usually required. Use of IVIG in doses of 0.5-1 g/kg in
a single or multiple dose regimen have been able to effectively reduce need for
exchange transfusion.15
A prospective randomized controlled study has shown early high-dose IVIG 1 g/kg at
12 hours of age to reduce duration of phototherapy and hospital stay and to prevent
exchange transfusion in neonates with moderate-to-severe Rh
isoimmunization.16 These newborns are also at risk of developing late
hyporegenerative anemia of infancy at 4-6 weeks of life. However, one randomized
double-blind placebo-controlled trial failed to show the benefit of prophylactic IVIG
therapy 0.75 g/kg within 4 hours of age in severely affected neonates who were
treated with intrauterine transfusion for Rh isoimmunization.17
Severe hemolytic disease accounts for the remaining 25% of the alloimmunized
newborns who are either stillborn or hydropic at birth. The fetal hydrops is
predominantly caused by a capillary leak syndrome due to tissue hypoxia,
28

hypoalbuminemia secondary to hepatic dysfunction, and high-output cardiac failure
from anemia. About half of these fetuses become hydropic before 34 weeks' gestation
and need intensive monitoring and management of alloimmunized gestation as
described earlier. Mild hydrops involving ascites reverses with IVTs in only 88% of
cases with improved survival but severe hydrops causing scalp edema and severe
ascites and pleural effusions reverse in 39% of cases and are associated with poor
survival.
Management of ABO incompatibility
Management of hyperbilirubinemia is a major concern in newborns with ABO
incompatibility. The criteria for exchange transfusion and phototherapy are similar to
those used in Rh alloimmunization. IVIG has also been very effective when
administered early in the course. Tin(Sn) porphyrin a potent inhibitor of heme
oxygenase, the enzyme that catalyzes the rate-limiting step in the production of
bilirubin from heme, has been shown to reduce the production of bilirubin and reduce
the need for exchange transfusion and the duration of phototherapy in neonates with
ABO incompatibility.
Tin or zinc protoporphyrin or mesoporphyrins have been studied in newborns. They
must be administered intramuscularly in a dose based on body weight, and their
effectiveness appears to be dose related in all gestations.18 Their possible toxic effects
include skin photosensitization, iron deficiency, and possible inhibition of carbon
monoxide production. Their use in Rh hemolytic disease of newborn has not been
reported. Their routine use cannot be recommended yet because of lack of long-term
safety data.
29

DRUG INDUCED ALLOIMMUNIZATION
It is rare but in some cases may be acute, severe and even life threatening. Four main
mechanisms have been proposed for antibody dependent drug-induced hemolytic
anemia: drug adsorption, immune complex and membrane modifications lead to
antibody reacting with novel epitopes and the true auto-antibody induced hemolytic
anemia. The same dose at different doses and repeated usage may activate different
mechanisms but the main underlying mechanism is membrane modification.
Diagnosis of drug-induced hemolytic anemia is made in three stages (1) diagnosis of
DAT positive hemolytic anemia (2) careful drug history (3) serological examination
of specific antibodies.
PATHOGENESIS:
Drug adsorption mechanism: IgG antibodies and extravascular hemolysis
drugs in this group readily form hapten-carrier complexes with plasma proteins,
which enhance drug specific antibody production. Prototype drug is penicillin
although cephalosporins and other penicillin derivatives have also been implicated.
90% individuals receiving penicillin produce clinically insignificant IgM anti-
penicillin antibodies. When high dose I/V penicillin is given, drug is adsorbed onto
the red cell surface and become non-specifically attached to red cell surface proteins.
A minority of patients on high dose I/V penicillin therapy ( >1million units daily)
develops high titer IgG antibodies which attach to the drug bound to the red cell
surface and result in extravascular hemolysis. If unrecognized and large doses
continued then complement fixation and acute I/V hemolysis may occur.
30

Immune complex mechanism: complement activated acute intravascular
hemolysis
Most common drugs include rifampicin, phenacetin, quinine, quinidine,
hydrochlorothiazide and chlorpropomide. More recently iv cephalosporins and
diclofenac are indicated. Hapten carrier complexes are formed between these drugs
and plasma proteins, leading to the production of drug specific antibodies. Once drug
antibodies are formed reintroduction results in immune complexes to form, which are
adsorbed onto the red cell surface and complement is activated. Classically hemolysis
occurs on the second or subsequent exposure exposure to the drugand may develop
within minutes or hours of drug ingestion.
Membrane modification mechanism:
Cephalosporin in addition to the drug adsorption mechanism, can cause a positive
DAT by modifying red cell membrane components. cisplatin and carboplatin has also
been reported to cause immune hemolytic anemia by this method. As a result, a
variety of plasma proteins including immunoglobulin and complement, may attach via
a non-immune mechanism to the red cell membrane. This may result in finding of a
positive DAT but rarely causes immune hemolytic anemia.
Autoimmune mechanism:
In this case the antibodies show no Rh specificity when tested against Rhnull cells.
some drugs may produce hemolysis by both the immune mechanism and autoimmune
mechanism depending on the circumstances
31

SEROLOGICAL DIAGNOSIS:
Drug adsorption and membrane modification mechanism:
The DAT is usually positive with IgG1 or IgG and C3 on red cell surface.
The red cell elutae or serum donot react against normal or enzyme modified
red cells
Warm reacting drug specific antibody in the eluate or serum is only detected
after preincubation of the test red cells with the appropriate drug.
Immune complex mechanism:
DAT is usually positive but may be negative if performed immediately after
brisk episode of hemolysis.
Red cell eluate is not reactive even in the presence of drug
Drug specific antibody is best detected by preincubating the patient’s serum
with the drug in solution to allow immune complexes to form.
Drug metabolite may be detected by preincubating drug metabolite obtained
from the serum or urine of a volunteer with patient’s serum.
32

REFERENCES:
1. Heddle NM, Soutar RL, O'Hoski PL, Singer J, McBride JA, Ali MA. A
prospective study to determine the frequency and clinical significance of
alloimmunization post-transfusion. Br J Haematol. Dec 1995;91(4):1000-5
2. Kerkhoffs JL, Eikenboom JC, van de Watering LM, van Wordragen-
Vlaswinkel RJ, Wijermans PW, Brand A. The clinical impact of platelet
refractoriness: correlation with bleeding and survival. Transfusion. Sep
2008;48(9):1959-65
3. Poon MC. The evidence for the use of recombinant human activated factor VII
in the treatment of bleeding patients with quantitative and qualitative platelet
disorders. Transfus Med Rev. Jul 2007;21(3):223-36.
4. Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Menacker F, Munson ML.
Births: final data for 2002. Natl Vital Stat Rep. Dec 17 2003;52(10):1-113.
5. Moise KJ. Hemolytic disease of the fetus and newborn. In: Creasy RK, Resnik
R. Maternal-fetal Medicine: Principles and Practice. 6th edition. Philadelphia:
WB Saunders; 2008:477-503
6. Vidnes J, Finne H. Immunoreactive insulin in amniotic fluid from Rh-
immunized women. Biol Neonate. 1977;31(1-2):1-6
7. Romano EL, Hughes-Jones NC, Mollison PL. Direct antiglobulin reaction in
ABO-haemolytic disease of the newborn. Br Med J. Mar 3 1973;1(852):524-6.
8. Murray NA, Roberts IA. Haemolytic disease of the newborn. Arch Dis Child
Fetal Neonatal Ed. Mar 2007;92(2):F83-8
33

9. Bowman J. The management of hemolytic disease in the fetus and
newborn. Semin Perinatol. Feb 1997;21(1):39-44
10. Moise KJ Jr. Red blood cell alloimmunization in Pregnancy. Seminars in
Hematology. 2005;42:169-178
11. Segata M, Mari G. Fetal anemia: new technologies. Curr Opin Obstet
Gynecol. Apr 2004;16(2):153-8
12. Zimmerman R, Carpenter RJ, Durig P, et al. Longitudinal measurement of
peak systolic velocity in the fetal middle cerebral artery for monitoring
pregnancies complicated by red cell alloimmunisation: a prospective
multicentre trial with intention-to-treat. BJOG. Jul 2002;109(7):746-52
13. ACOG Practice Bulletin No. 75: management of alloimmunization. Obstet
Gynecol. Aug 2006;108(2):457-64.
14. Opekes D, seward G, Vandenbussche F, et al. Minimally invasive management
of rh alloimmunization: Can amniotic fluid delta OD 450 be replaced by
Doppler studies? A prospective study multicenter trial. Am J Obstet Gynecol.
2004;191:S3
15. Gottstein R, Cooke RW. Systematic review of intravenous immunoglobulin in
haemolytic disease of the newborn. Arch Dis Child Fetal Neonatal Ed. 2003
Jan;88(1):F6-10. 88(1);2003:F6-10.
16. Elalfy MS, Elbarbary NS, Abaza HW. Early intravenous immunoglobin (two-
dose regimen) in the management of severe Rh hemolytic disease of newborn-
a prospective randomized controlled trial. Eur J Pediatr. Apr
2011;170(4):461-7
34

17. Smits-Wintjens VE, Walther FJ, Rath ME, Lindenburg IT, Te Pas AB, Kramer
CM, et al. Intravenous immunoglobulin in neonates with rhesus hemolytic
disease: a randomized controlled trial. Pediatrics. Apr 2011;127(4):680-6.
18. Kappas A. A method for interdicting the development of severe jaundice in
newborns by inhibiting the production of bilirubin. Pediatrics. Jan 2004;113(1
Pt 1):119-23
35