
Allogeneic Stem cell transplant in CR1 for AML
42
XIAO JUN HUANG, MD, PHD Beijing, China • Chairman, Peking University Institute of Hematology; Director, Department of Hematology, Peking University People’ s Hospital; Director, Beijing Key Laboratory of Hematopoietic Stem Cell Transplantation • Dr. Xiao Jun Huang, MD, PhD is a pioneer in the field of haploidentical stem cell transplant and leads the transplant program at Peking University. As the Head of the Association of Chinese Hematologists, five years ago, Dr. Huang established a platform of education for professional standardization to junior hematologists in Mainland China. It consists of series of conference that covers around 20 cities each year in China. He serves as APHCON
Transcript of Allogeneic Stem cell transplant in CR1 for AML

XIAO JUN HUANG, MD, PHDBeijing, China
• Chairman, Peking University Institute of Hematology; Director, Department of Hematology, Peking University People’ s Hospital; Director, Beijing Key Laboratory of Hematopoietic Stem Cell Transplantation
• Dr. Xiao Jun Huang, MD, PhD is a pioneer in the field of haploidentical stem cell transplant and leads the transplant program at Peking University. As the Head of the Association of Chinese Hematologists, five years ago, Dr. Huang established a platform of education for professional standardization to junior hematologists in Mainland China. It consists of series of conference that covers around 20 cities each year in China. He serves as APHCON President/Executive Chairman and is committed to uniting practicing hematologists of participating nations and providing educational opportunities to the younger generation. He also serves as the President of the Chinese Society of Hematology.

Hematopoietic stem cell transplantation for the treatment of acute myeloid leukemia in CR1:
who and which type
Xiao-Jun HuangPeking University People’s Hospital
& Institute of HematologyBeijing Key Laboratory of HSCT
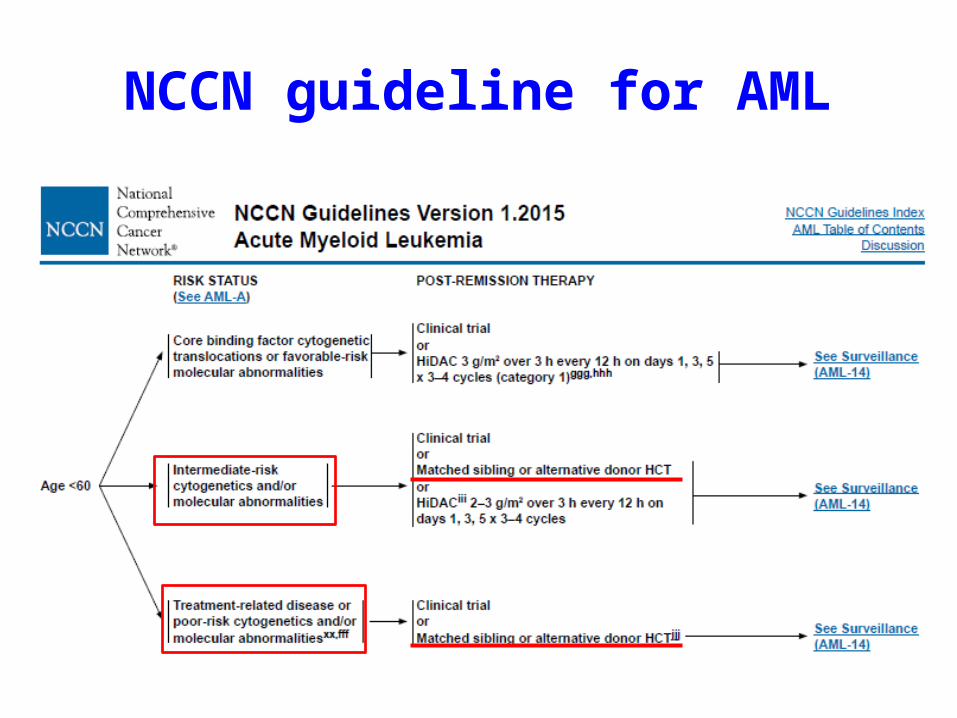
NCCN guideline for AML

1964
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
0500
1000150020002500300035004000
1990
1993
1996
1999
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
0
200
400
600
800
1000
1200
1400
1600
1800
2000
Number of HSCT cases in PUIH

Dose allogeneic hematopoietic stem cell transplantation benefit all patients with AML in CR1 ? Who and wich type?
AML-CR1
≤60 ys
Favorable risk
Unfavorable risk
> 60ysFavorable
risk
Unfavorable risk
Is allo-HSCT benefit for the different age group
Is allo-HSCT benefit for the favorable risk AML in CR1
Which type of HSCT will be chosen?

HSCT for patients aged < 60 years old

HSCT for unfavorable risk AML in CR1
• Does patients with intermediate- or high risk AML in CR1 benefit from allogeneic HSCT?
• Which type of allogeneic HSCT will be chosen?

By treatment arm for the unfavorable risk group
E3489/S9034
Blood. 2000 Dec 15;96(13):4075-83.
A single phase III intergroup study

J Clin Oncol. 2011 Jul 10;29(20):2758-65.
1996-2005;N=1557;
Southern German Hemoblastosis Group AML96 trial
OS in patients without allogeneic SCT was generally worse than in patients who received an allogeneic SCT

HOVON-SAKK
Leukemia (2014), 1–10

OS was comparable following allo HSCT and auto HSCT in patients with intermediate-risk. Allo HSCT was associated with less relapse (hazard ratio (HR) 0.51, P< 0.001) and better relapse free survival (RFS) (HR 0.74, P = 0.029) as compared with auto HSCT in intermediate-risk AMLs
Leukemia (2014), 1–10
HOVON-SAKK
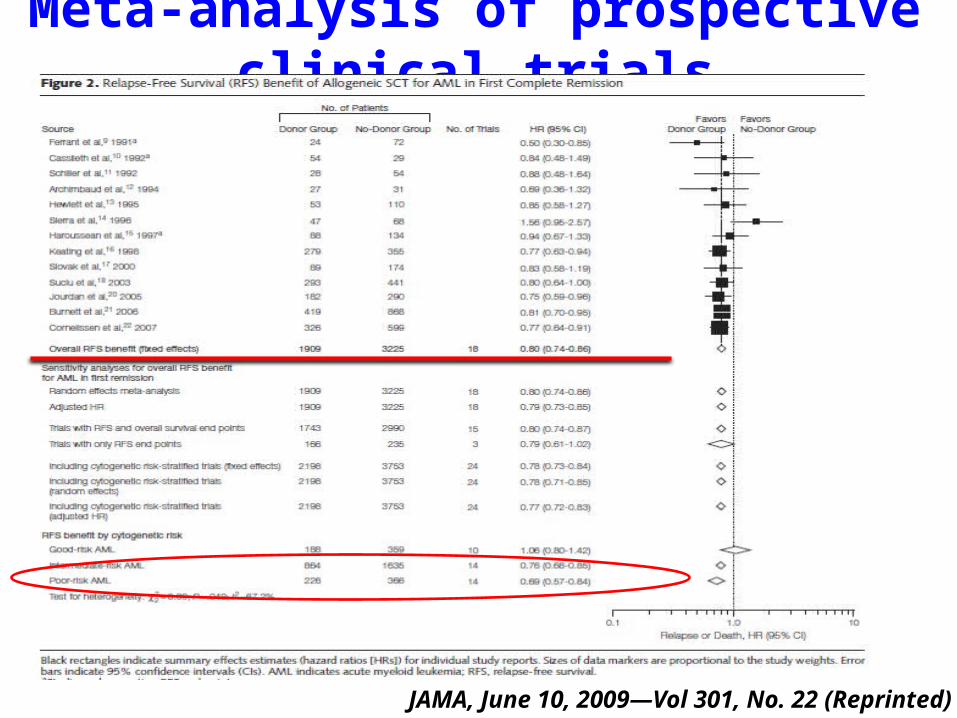
Meta-analysis of prospective clinical trials
JAMA, June 10, 2009—Vol 301, No. 22 (Reprinted)

Meta-analysis of prospective clinical trials
JAMA, June 10, 2009—Vol 301, No. 22 (Reprinted)

Summary 1
• Allogeneic HCT from a matched related donor (MRD) or a matched unrelated donor(MUD) is a preferred therapy for patients with intermediate and high risk AML inCR1.

What about the role of Haplo-HSCT in intermediate and high risk AML in CR1 ?

Lu DP, et al. Blood,2006,107(8):3065-3073
Haplo-HSCT vs. MSD
Unmanipulated HBMT can achieve comparable outcomes with matched related donor transplant

Haplo-HSCT vs. CTData source: PKUHPatients: from 2006.1-2010.5, prospective
Huang XJ, et al. Blood,2012,119(23):5584-5590

Superior survival of HBMT to chemotherapy alone as post-remission therapy for IR and HR AML
Huang XJ, et al. Blood,2012,119(23):5584-5590

Haplo vs. MSD
Transplant Candiate
Matched sibling donor
Yes (n=219)
MSDT
NO
Unrelated donor
YesNO
MUDTHaplo-SCT (n=231)
This study was registered as ChiCTR-OCH-10000940 at www. chictr.org.

Manipulated haplo-SCT is a valid alternative modality
Wang Y, Huang XJ, et al. Unpublished data from a multicenter study
TRM Relapse

Unmanipulated haplo-SCT is a valid alternative modality
Wang Y, Huang XJ, et al. Unpublished data from a multicenter study
OS LFS
Days since transplant Days since transplant
Identical sibling donor Identical sibling donor
Haploidentical donor Haploidentical donor

Summary 2
• Haplo-hematopoietic cell transplantation may benefit patients with intermediate and high risk AML in CR1

Transplant candidate of AML
HLA-identical related donors
Yes
MSDT
No
1.Search 8/8 matched unrelated donor with 8 week?2.Urgent for transplantion?
not urgent
8/8 MUDTHaplo-SCT
urgent
Huang XJ, et al. Blood,2012,119(23):5584-5590 Lu DP, et al. Blood,2006,107(8):3065Chang YJ,et al. Semin Oncol,2012,39:653-663 Mo XD, et al. BMT,2014,Online publication
Recommendation 1

NCCN-2015
No room of allo-HSCT
Is all patients with favorable risk
factor will have a favorable outcome?

UK MRC-AML15
Liu Yin JA ,et al . Blood 2012; 120: 2826 MRD analysis in a perspective protocol MRC-AML15
Time : 2002.7 -2009.1Including: 361 CBF-AML 278 suitable for MRD study t(8;21) N=163MRD monitoring: CR、 each consolidation、 follow-up
CR: >3log
Post-consolidation 3:>4log
Follow-up: BM>500copies
t(8;21)( n=59)

• Prospective, multicenter, cohort study
• Time :from 2005.6 to 2011.11
• MRD: RUNX1-RUNX1T1( RQ-PCR )
• KIT mutation: direct sequencing
Huang XJ, et al. Blood 2013; 121 4056
AML05 trial: MRD-directed stratification treatment of t(8;21)-AML

High-risk(MRD): CT vs. HSCT
Huang XJ, et al. Blood 2013; 121 4056

Multivariate analysis
CIR DFS OS
p p pMRD status
high- vs. low-risk 0.003 0.002 0.02
Treatment choice risk- vs. non risk-directed 0.026 0.036 0.037KIT status
mutation vs. wild-type 0.049 ns ns
Huang XJ, et al. Blood 2013; 121 4056

Allo-HSCT can improve outcome of high-risk t(8;21)AML

MRD could predict relapse in AML with inv(16) or t(16;16)
IS allo-HSCT can improve outcome of high-risk inv (16) or t(16;16) AML?

MRD post Consolidation ≤0.2%MRD post Cons 1 ≤0.2%
MRD post Cons 2 ≤0.2%
Unpublished data of PUIH

Allo-HSCT can improve outcome of high-risk inv(16)AML
MRD post Cons 2 >0.2%
MRD post Cons 2 >0.2% or lose ≤0.2% post Cons3-8
Unpublished data of PUIH

Recommendation 2
• Patients with MRD-stratified high risk AML with t(8;21), inv (16) or t(16;16) may benefit from the allogeneic HSCT.
• Prospective studies are need to confirm the conclusion

HSCT for patients aged ≥60 years old

HSCT or CT , which will be
chosen?

Allo HSCT or CT• 1999-2006, retrospective, matched• Allo-HCT patients (n=94) (excluding UCB
and MAC) from CIBMTR aged 60-70 • CT patients (n=96) from two
CALGB( CALGB 9720 and CALGB19902) • All patients included had been in CR1 for
at least 4 months
3-year NRM 36% vs. 4%; P< 0.01
3-year relapse 32% vs. 81%; P<0.01
3-year LFS 32% vs. 15%; P< 0.01 3-year OS 37% vs. 25%; P=0.08
Biol Blood Marrow Transplant 17:1796-1803, 2011

Blood. 2007 Feb 15;109(4):1395-400. Epub 2006 Oct 12.
There is still no study compared RIC with MAC HSCT for elderly patients
RIC-HSCT was superior than CT(P = .004)

Micro transplantation(MST)
Blood. 2011 Jan 20;117(3):936-41
G-PBSC infusion improves the probability of DFS and OS for elderly patients with AML.
2-years DFS (MST vs. control)38.9% vs. 10% P=0.01
2-years OS (MST vs. control)39.3% vs. 10.3% P=0.0006

Micro transplantation(MST)
6-year leukemia-free survival (LFS) 6-year overal survival (OS)Low-risk group 84.4% 89.5%Intermediate-risk group 59.2% 65.2%
P=0.272 P=0.308
No GVHD was observed in any of the patients
Micro transplantation as a post remission therapy may improve outcomes and avoid GVHD in patients with AML-CR1
J Clin Oncol. 2012 Nov 20;30(33):4084-90.

Summary 3
• Some patients aged > 60 years old with intermediate and high risk AML in CR1 could benefit from allogeneic HSCT.
• RIC conditioning regimen is preferred and micro transplantation may be a choice.

Conclusions
AML patients in CR1
Intermediate risk and/or high risk
Favorable risk
ECOG PS 0-1And elects aggressive treatment
CR1
Allo HSCT
MRD stratified high risk group

Thank you for your attention!
Stem cell collection centerHai-Yin ZhengHong XuQing ZhaoSu Wang
Department of bone marrow transplant Xiao-Jun Huang Dai-Hong LiuKai-Yan Liu Xiao-Su ZhaoLan-Ping Xu Xiao-Hui Zhang Huan Chen Wei HanXiang-Yu Zhao Yu-Hong Chen Feng-Rong Wang Yu WangJing-Zhi Wang Chen-Hua Yan Yuan-Yuan Zhang Yu Ji Yu-Qian Sun
Laboratory of PUIHDan LiYa-Zhen QinYan-Rong LiuYue-Yun Lai


















