
Allan Gibofsky, MD, JD, FACP, FCLM Joseph A. … · Allan Gibofsky, MD, JD, FACP, FCLM, ... Pfizer...
145
Allan Gibofsky, MD, JD, FACP, FCLM Allan Gibofsky, MD, JD, FACP, FCLM Professor of Medicine and Public Health Weill Medical College of Cornell University Attending Physician Hospital for Special Surgery Adjunct Professor of Law Fordham University School of Law New York, New York Joseph A. Markenson, MD Professor of Clinical Medicine Weill Medical College of Cornell University Hospital for Special Surgery New York, New York Supported by an educational grant from Amgen Inc and Wyeth Pharmaceuticals This educational activity has been facilitated by Gullapalli & Associates, LLC.
Transcript of Allan Gibofsky, MD, JD, FACP, FCLM Joseph A. … · Allan Gibofsky, MD, JD, FACP, FCLM, ... Pfizer...

Allan Gibofsky, MD, JD, FACP, FCLMAllan Gibofsky, MD, JD, FACP, FCLMProfessor of Medicine and Public HealthWeill Medical College of Cornell University Attending PhysicianHospital for Special SurgeryAdjunct Professor of Law Fordham University School of Law New York, New York
Joseph A. Markenson, MDProfessor of Clinical MedicineWeill Medical College of Cornell UniversityHospital for Special SurgeryNew York, New York
Supported by an educational grant from Amgen Inc and Wyeth PharmaceuticalsThis educational activity has been facilitated by Gullapalli & Associates, LLC.

Sponsorship and Support
This educational activity is jointly sponsored by
Gullapalli & Associates, LLC and the University of Kentucky.
Support is provided by an educational grant from Amgen Inc and Wyeth Pharmaceuticals, Inc.
Accreditation and Credit Designation
• This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME).
• The University of Kentucky College of Medicine is accredited by the ACCME to provide continuing medical education for by the ACCME to provide continuing medical education for physicians.
• The University of Kentucky College of Medicine designates this educational activity for a maximum of 4 AMA PRA Category 1 Credit (s)™. Physicians should only claim credit commensurate with the extent of their participation in the activity.

Disclaimer
The University of Kentucky College of Medicine presents this activity for educational purposes only.
Participants are expected to utilize their own expertise and judgment while engaged in the practice of medicine.
The content of the presentations is provided solely by presenters who have been selected because of their recognized expertise in this field.
The University of Kentucky is an Equal Opportunity University.

Course Directors
Marc D. Cohen, MDProfessor of Medicine, Chief of RheumatologyNational Jewish Medical and
Research Center Denver, Colorado
Philip J. Mease, MDSeattle Rheumatology Associates Chief of Rheumatology Research, Swedish Medical Center Clinical Professor of Medicine, University of Washington Seattle, Washington
FacultyAllan Gibofsky, MD, JD, FACP, FCLMProfessor of Medicine and Public HealthWeill Medical College of Cornell University Attending PhysicianHospital for Special SurgeryAdjunct Professor of Law Fordham University School of Law New York, New York
Joseph A. Markenson, MDProfessor of Clinical MedicineWeill Medical College of Cornell UniversityHospital for Special SurgeryNew York, New York

DisclosuresMarc D. Cohen, MD, reports serving as a consultant for Abbott Laboratories, Amgen Inc, Genentech, Inc, and Wyeth Pharmaceuticals. Dr Cohen reports his spouse/significant other serving as a consultant for Abbott Laboratories, Amgen Inc, Genentech, Inc, UCB Pharma, and Wyeth Pharmaceuticals.
Philip J. Mease, MD, reports receiving grants/research support from and serving on the speakers' bureau for Abbott Laboratories, Amgen Inc, Biogen Idec, Bristol Myers-Squibb Company, Centocor, Inc, Genentech, Inc, and Wyeth Pharmaceuticals; and serving as a consultant for Abbott Laboratories, Amgen Inc, Biogen Idec, Bristol Myers-Squibb Company, Centocor, Inc, Genentech, Inc, Roche Pharmaceuticals, Wyeth Pharmaceuticals, and UCB Pharma.
Allan Gibofsky, MD, JD, FACP, FCLM, reports serving as a consultant for Abbott Laboratories, Allan Gibofsky, MD, JD, FACP, FCLM, reports serving as a consultant for Abbott Laboratories, Bristol-Myers Squibb Company, and Pfizer Inc; serving on the speakers bureau for Abbott Laboratories, Amgen Inc, Bristol-Myers Squibb Company, Pfizer Inc, and Wyeth Pharmaceuticals; and holding stock in Abbott Laboratories, Amgen Inc, Johnson & Johnson, and Pfizer Inc.
Joseph A. Markenson, MD, reports receiving grants/research support from Abbott Laboratories, Amgen Inc, and Bristol-Myers Squibb Company; serving as a consultant for Abbott Laboratories, Vertex, and UCB, Inc.; and serving on the speakers' bureau for Abbott Laboratories, Amgen Inc, Bristol-Myers Squibb Company, and Wyeth Pharmaceuticals.
Rheumatoid ArthritisEducational Challenge
Overview

Rheumatoid Arthritis Educational Challenge(RAEC)
RAEC consists of an integrated series of CME-accredited educational activities.
These multi-interventional series are developed to optimize outcomes of patients with rheumatoid arthritis (RA).
Educational activities:
- Regional meetings/workshops
- Live broadcasts of today’s meeting (VHATV)
- PDA-based activity (Epocrates)
- Self-study course on CE Central
- Website and toolkit
Goal of Today’s Meeting
This continuing education initiative seeks to advance
the management of RA and improve collaboration among health care professionals.
Today’s session will include case studies, followed by workshop discussions.workshop discussions.
The remaining 2 workshops will be fine-tuned based on your feedback.

Learning Objectives
IDENTIFY the benefits of an aggressive treatment strategy in the early management of RA.
APPLY appropriate integrated referral and care pathways for multidisciplinary management of patients with RA and comorbid conditions.
UTILIZE the risk/benefit profiles to understand appropriate use of biologic/tumor necrosis factor (TNF-α) antagonist therapies in the management of patients with RA.
DEMONSTRATE patient-physician communication skills appropriate for discussing the rationale, benefits, and risks of biologic/TNF-α antagonist therapies in RA.

Today’s Agenda 8:30 – 9:00 AM Breakfast
9:00 – 9:15 AM Welcome and Introduction
9:15 – 9:30 AM Workshop 1
9:30 – 9:45 AM RA Overview
9:45 – 10:00 AM Break
10:00 – 10:30 AM Current Management of RA
10:30 – 11:00 AM Case Study 1 and Discussion 10:30 – 11:00 AM Case Study 1 and Discussion
11:00 – 11:30 AM Case Study 2 and Discussion
11:30 – 11:45 AM Case Study 3 and Discussion
11:45 – 12:00 PM Case Study 4 and Discussion
12:00 – 12:45 PM Lunch
12:45 – 1:00 PM Workshop 2
1:00 – 1:30 PM Case Study 5 and Discussion
1:30 – 2:00 PM Workshop 3

Workshop 1: New Diagnosed RA

Workshop 1: Newly Diagnosed RA
Please review the clinical scenario summarized on the next slide
You are encouraged to interact with your colleagues to determine the optimal response to the scenario
Flipcharts are provided to capture the findings from each group
Faculty will review and facilitate discussion through ARS based on your responses
Workshop 1: Newly Diagnosed RA
RM is a 37-year-old woman who presents to your clinic saying that she has “pain in her hands and she can no longer work in her garden.”
Her primary care doctor had suggested that she take ibuprofen when she visited his office 6
She has smoked 1 pack of cigarettes daily for 10 years but denies alcohol or any drug use.
Yearly tuberculosis skin tests, required as a result of her occupation as a health care worker, have been negative.suggested that she take ibuprofen
when she visited his office 6 weeks ago.
Initially her symptoms improved but then she developed more pain, morning stiffness lasting at least 1 hour, and swelling of her hands as well as her knees.
Rheumatoid factor and CCP antibody are negative and CRP is 15 (NR ≤10).
Family history and the remainder of the review of systems are unremarkable except for occasional dyspepsia, relieved by chewable antacids, since she used naproxen 2 years ago for dysmenorrhea.

Workshop 1: ARS
How confident, if at all, would you feel treating the patient described in the above scenario? (Select ONE answer)
Not at all confident Very confidentNot at all confident Very confident
1 2 3 4 5 6
Workshop 1: ARS
Please indicate how often, if at all, you initiate biological therapy in patients demonstrating structural damage in the absence of laboratory findings when evaluating patients with possible rheumatoid disease. (Select ONE answer)rheumatoid disease. (Select ONE answer)
Never incorporate this behavior Always incorporate this behavior
1 2 3 4 5 6
Workshop 1: ARS
Which of the following tools do you use routinely when evaluating patients with rheumatoid disease? (Select ONE answer)
A. ACR 20/50/70 criteria
B. DAS (disease activity scale)
C. Simplified Disease Activity Index (SDAI)
D. The Clinical Disease Activity Index (CDAI)
E. None of the above

ARS Based Group Discussion

Workshop 1: Group Discussion Point
Based on the history, the following factors suggest a
diagnosis of RA except:
a. Swelling of the wrist, metacarpophalangeal (MCP), or proximal interphalangeal (PIP) joints for at least six proximal interphalangeal (PIP) joints for at least six weeks
b. History of smoking
c. Swelling of the same joints on both sides of the body
d. Morning stiffness lasting at least one hour

Workshop 1: 6 months later
She is taking MTX 15 mg/week and ibuprofen and has developed two nontender subcutaneous nodules near the left elbow.
C-reactive protein (CRP) level (27mg/L) (NR <10)
Normal hemoglobin and white-cell count.
A latex test for rheumatoid (-) Both wrists and the MCP joints
of both hands were swollen and tender but not deformed.
Vasculitic lesions were absent.
A latex test for rheumatoid (-) and antinuclear antibodies were not detected.
X-rays of her hands reveal peri-articular osteopenia but no clear-cut erosions.
Workshop 1: ARS
How would you classify the severity of her arthritis?
1. Mild rheumatoid arthritis
2. Moderate rheumatoid arthritis
3. Severe rheumatoid arthritis3. Severe rheumatoid arthritis
4. End-stage rheumatoid arthritis

Workshop 1: Group Discussion Point
RM is no longer responding to prior treatment with ibuprofen. The following are reasonable approaches to her continued management except:
a. Prescribe oral glucocorticoids
b. Initiate treatment with an oral disease-modifying b. Initiate treatment with an oral disease-modifying agents
c. Initiate treatment with methotrexate in combination with at least 2 biologic-disease modifying agents
d. Consider early initiation of biologic response modifier if an oral disease-modifying agent is inadequate or not tolerated
Workshop 1: Group Discussion Point
At this point, which option would you not likely pursue?
a. Increase MTX to 20 mg per week
b. Add sulfasalzine
c. Add hydroxychloroquinec. Add hydroxychloroquine
d. Add a biologic agent
e. Refer to a specialist (if PCP)
f. Decrease MTX dose because of concern about toxicity

Rheumatoid Arthritis
Overview
Epidemiology Incidence rate: approximately 3 cases per 10,000
Peak incidence: 30 to 40 years of age
Prevalence rate: 1% of population
Age prevalence:
- 55 to 75 years: 4.5%
- 75 years: 7%- 75 years: 7%
Female predominance 3:1
Daily living activities limited: >33%
Substantial functional disability: 29%
Significant comorbidity
Increased mortality rates
Am J Med. 1985;78(suppl 1A):1-5; J Rheumatol.1989;16:867-884; Semin Arthritis Rheum. 1991;21(suppl1):4-12.

Clinical Features
Systemic inflammatory disease
Constitutional symptoms (fever, weight loss, fatigue)
Morning stiffness
Symmetrical, erosive polyarthritis
Extra-articular manifestations (nodules, pulmonary fibrosis, serositis, vasculitis, eye inflammation)fibrosis, serositis, vasculitis, eye inflammation)
Serologic correlates– Rheumatoid factor (RF)
– Cyclic Citrullinated Proteins (CCP)
– Anemia
– Elevated acute-phase reactants (ESR, CRP)
– Antinuclear antibodies (ANA)
ESR = erythrocyte sedimentation rate; CRP – C-reactive protein
RF and Anti-CCP Antibodies and Disease Progression
RF positivity may be associated with1-4:– More active disease
– Development of bone erosions
– Disability
Anti-CCP positivity at baseline may predict3,5,6: Anti-CCP positivity at baseline may predict3,5,6:– Development of erosions and radiologic progression
– Response to treatment
– Changes in anti-CCP levels are not predictive of changes in disease activity
1. Emery P, et al. Rheumatology. 2008;47:392-398; 2. Nell VP, et al. Ann Rheum Dis. 2005;64:1731-1736; 3. Symmons DPM. Rheumatology. 2007;46:725-726; 4. Visser H. Best Pract Res Clin Rheumatol. 2005;19:55–72; 5. Rönnelid J, et al. Ann Rheum Dis. 2005;64:1744–1749; 6. Schellekens GA, et al. Arthritis Rheum. 2000;43:155–163.

Clinical Presentation
Early RA Intermediate RA Severe RA
Images courtesy of Dr Mease

Involvement of Joints
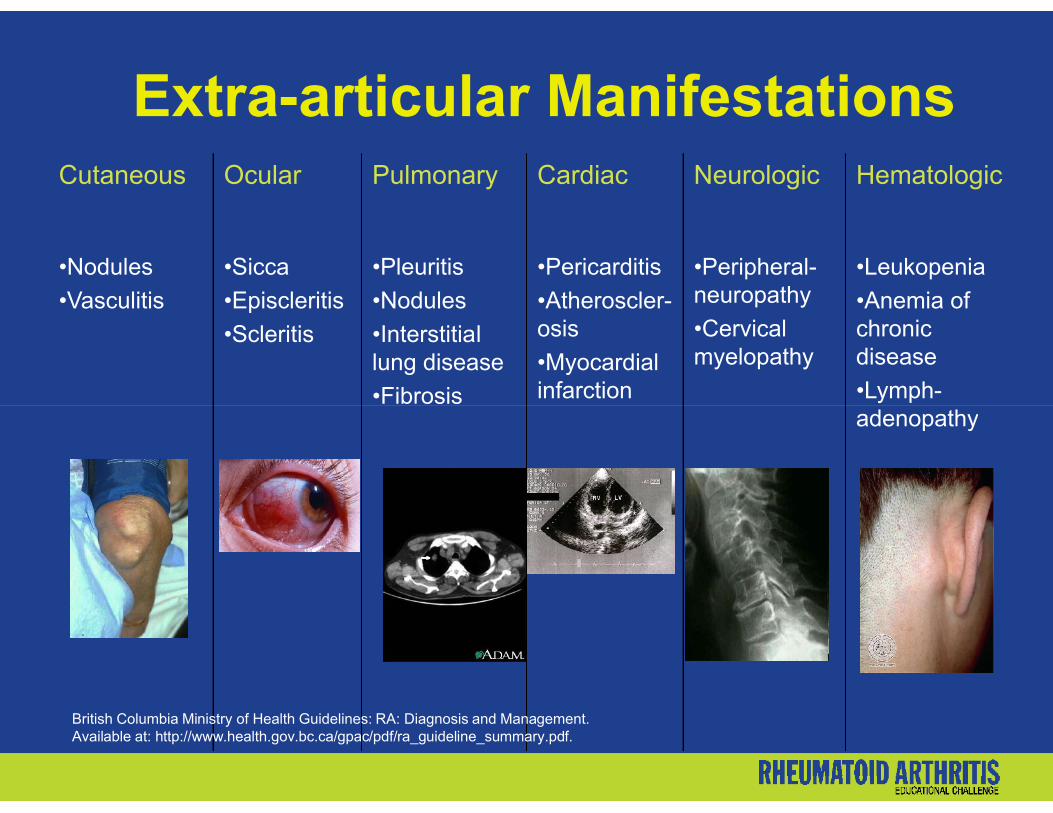
Cutaneous Ocular Pulmonary Cardiac Neurologic Hematologic
•Nodules
•Vasculitis
•Sicca
•Episcleritis
•Scleritis
•Pleuritis
•Nodules
•Interstitial lung disease
•Fibrosis
•Pericarditis
•Atheroscler-osis
•Myocardial infarction
•Peripheral-neuropathy
•Cervical myelopathy
•Leukopenia
•Anemia of chronic disease
•Lymph-adenopathy
Extra-articular Manifestations
•Fibrosisadenopathy
British Columbia Ministry of Health Guidelines: RA: Diagnosis and Management. Available at: http://www.health.gov.bc.ca/gpac/pdf/ra_guideline_summary.pdf.

Baseline Evaluation
Subjective
Degree and location of joint pain
Duration of morning stiffness
Fatigue
Limitation of function Limitation of function
Physical examination
Documentation of inflamed joints (swelling and tenderness)
Loss of joint motion, crepitus, instability, deformity

Baseline Evaluation (cont’d)
Laboratory studies
ESR, CRP
Rheumatoid factor
CCP
CBC CBC
Creatinine
Hepatic panel
Imaging studies
Radiography of selected involved jointsArthritis Rheum. 1996;39:713-722.

ACR’s Criteria for Classification
1. Morning stiffness lasting for at least 1 hour
2. Simultaneous arthritis of 3 or more joint areas
3. Arthritis of hand joints
4. Symmetric arthritis
5. Rheumatoid nodules5. Rheumatoid nodules
6. Abnormal serum rheumatoid factor
7. Radiographic changes typical of RA on posteroanterior hand and wrist radiographs
A patient can be classified as having RA if:• 4 out of 7 criteria are present• Criteria 1 through 4 must be continuous for at least 6 weeks
Arthritis Rheum. 1988;31:315-324. Arthritis Rheum. 1996;36:713-722.

The Pathogenesis of RANORMAL
RHEUMATOID ARTHRITIS
Synovial Membrane
Inflamed Synovial
Membrane
Pannus
Major cell types:T lymphocytesMacrophages
Cartilage
CapsuleSynovialFluid
Pannus
Minor cell types:FibroblastsPlasma cellsEndotheliumDendritic cells
Major cell type:Neutrophils
Adapted from Feldmann M, et al. Annu Rev Immunol. 1996;14:397-440.
Cartilage Thinning

Disease Progression
HyperplasticSynovialMembrane
Neutrophils
Early Rheumatoid Arthritis
Capsule
Bone
Synovial Membrane
Synoviocytes
Normal Joint
Cartilage
Adapted with permission from:Choy EHS, Panayi GS. N Engl J Med. 2001;344:907-916.© 2001 Massachusetts Medical Society. All rights reserved.
Capillary Formation
HypertrophicSynoviocyte T Cells B Cells
Established Rheumatoid Arthritis
Synovial Villi
ExtensiveAngiogenesis
Plasma Cell
PannusEroded Bone
Neutrophils
Synoviocytes

Correlation Between Joint Inflammation, Disability, and Radiographic Findings
Sev
erit
y (A
rbit
rary
U
nit
s)Inflammation
Disability
Radiographs
Adapted from Kirwan JR. J Rheumatol. 2001;28:881–886.
Sev
erit
y (A
rbit
rary
U
nit
s)
0
Duration of Disease (years)
5 10
15
20
25
30

Imaging Studies
Clinically Detectable Damage Occurs Early
Disease progression is more rapid during the first year than during the second and third years3
Most patients (up to 93%) with RA of <2 years’ duration show radiographic damage2
MRI-detectable erosions are present within 4 months of disease onset1
1. McQueen FM, et al. Ann Rheum Dis. 1998;57:350–356.2. Fuchs HA, et al. J Rheumatol. 1989;16:585–591.3. van der Heijde D, et al. J Rheumatol. 1995;22:1792–1796.
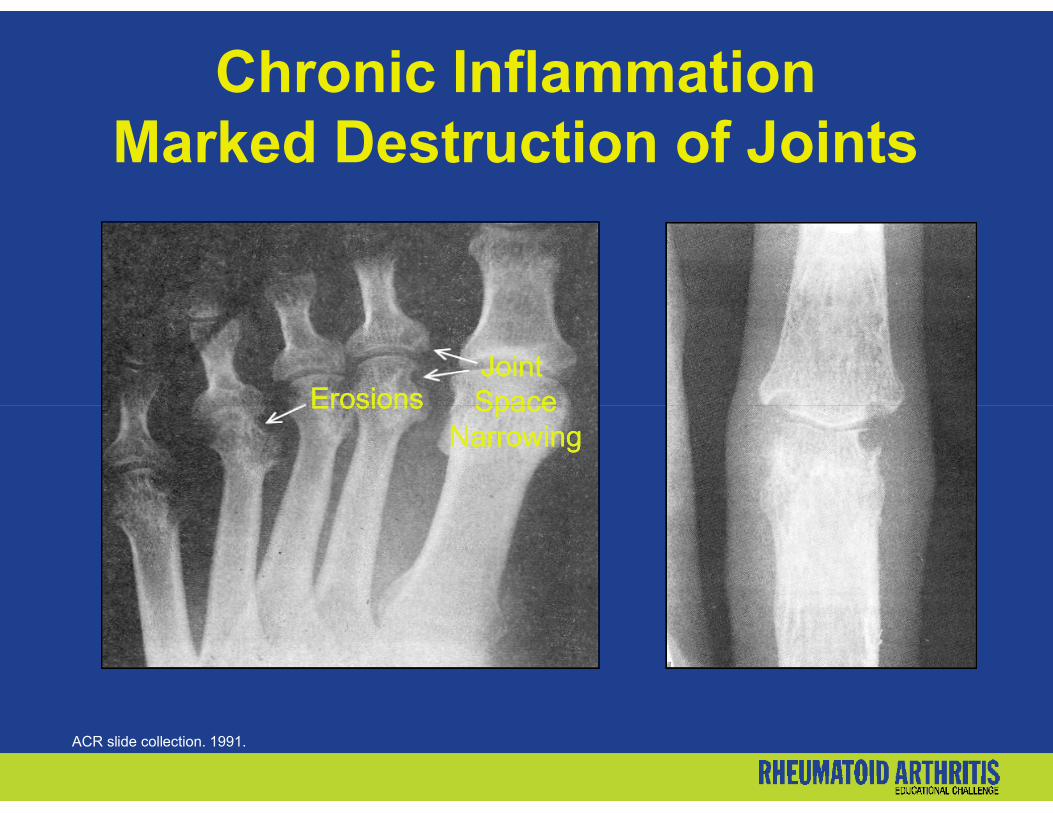
ErosionsErosionsJoint Joint SpaceSpace
Chronic InflammationMarked Destruction of Joints
ACR slide collection. 1991.
ErosionsErosions SpaceSpaceNarrowingNarrowing
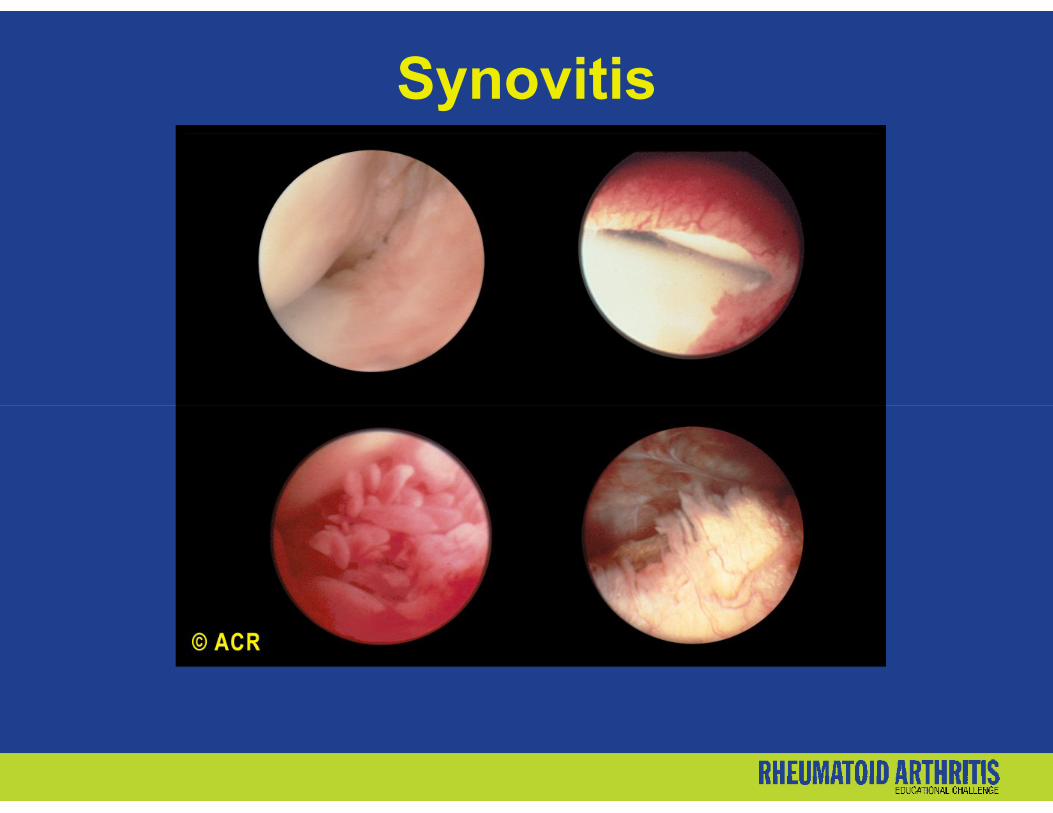
Synovitis
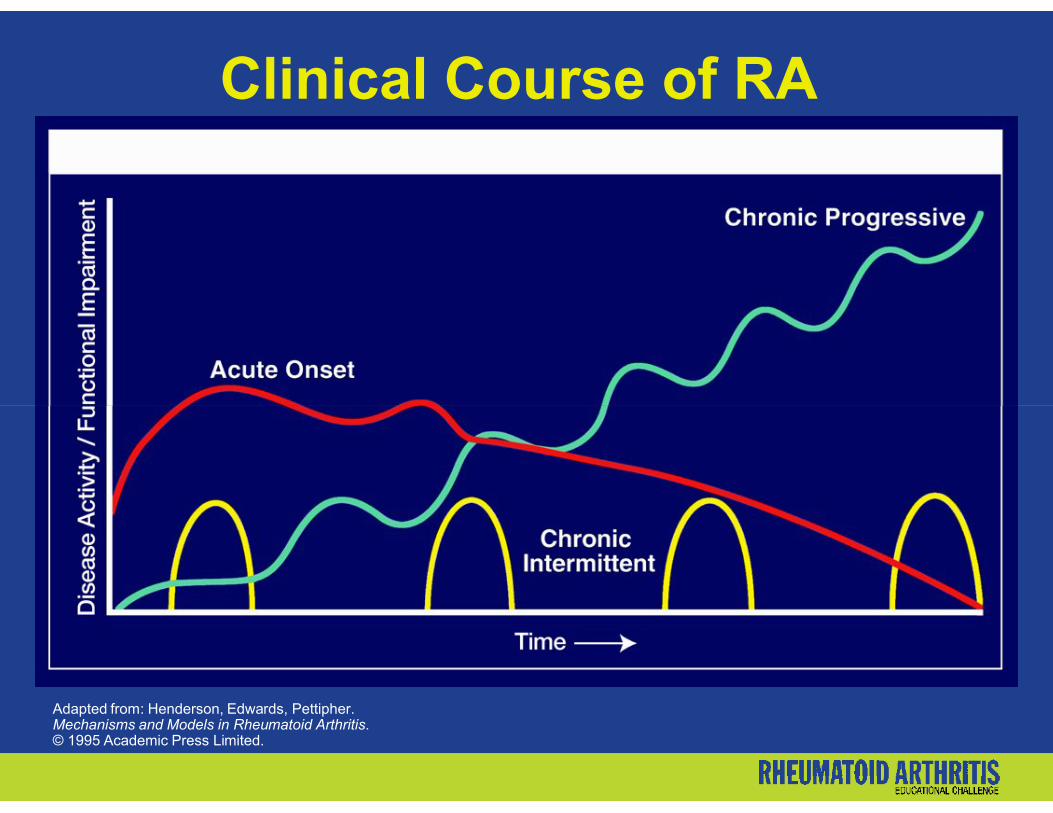
Clinical Course of RA
Adapted from: Henderson, Edwards, Pettipher. Mechanisms and Models in Rheumatoid Arthritis.© 1995 Academic Press Limited.
Indicators of Poor Prognosis
Advanced age at onset
Extra-articular features (subcutaneous rheumatoid nodules, vasculitis, neuropathy, scleritis)1
Involvement of multiple joints2
Early erosive changes on radiographs2 Early erosive changes on radiographs2
High RF and/or CCP levels2
Increased ESR2
Poor functional status2
Comorbid cardiovascular disease1
1. Young A, et al. Best Pract Res Clin Rheumatol. 2007;21(5):907-27; 2. Saag KG, et al. Arthritis Rheum. 2008;59:762-84.

Impact of RA Mortality rate significantly higher than in general
population1
43% to 85% of RA patients will be unable to work within 8 to 11 years of disease onset2
– ~50% of employed RA patients are disabled for – ~50% of employed RA patients are disabled for >14 work days annually3
– Change in disability level in the first 2 years of disease predicts subsequent development of functional impairment4
1. Myllykangas-Luosujarvi et al. J Rheumatol. 1995;22:1065-1067.2. Mau et al. Br J Rheumatol. 1996;35:652-659.3. Official Disability GuidelinesTM, 1998. Work-Loss Data Institute LLC, Corpus Christi, Tex.4. Singh G. Arthritis Rheum. 1996.

Increased Mortality RateS
tan
dar
diz
ed M
ort
alit
y R
atio
2.362.26
2.14
1.5
2.0
2.5
Sta
nd
ard
ized
Mo
rtal
ity
Rat
io
0
0.5
1.0
Men Women Overall
Gabriel SE, et al. Arthritis Rheum. 2003;48:54-58.
Patients Within Each Individual Study

Current Management of RA Patients

Control of signs and symptoms
Restoration of function and improvement of daily life quality
Inhibition/slowing of structural joint damage
Beneficial effect on comorbidities and reduction of mortality
Goals of RA Therapy
– Cardiovascular (MI and CVA)– Osteoporosis– Neoplasms– Infection
Impact on society– Cost-benefit of therapies– Return to work
Early intervention, including during undifferentiated state, to change the natural history of RA?
Knell ME. In: Schumock GT, ed. Pharmacotherapy Self-Assessment Program. 2005: 41-88.

ACR Treatment AlgorithmDiagnosis and Initial Evaluation of RA
• Establish Diagnosis of RA Early• Document Baseline Disease Activity and
Damage• Estimate Prognosis
Initiate Therapy• Patient Education• Start DMARD(s) Within 3 Months • Consider NSAID• Consider Local or Low-Dose Systemic
Steroids• Physical Therapy/Occupational TherapyPeriodically Assess
Disease Activity/Progression Inadequate Response
(active disease after 3 months max therapy)
Adapted from: Arthritis Rheum. 2002;46:328-346.
Change/Add DMARDs
MTX Naïve Suboptimal MTX Response
MTX Other Mono
Rx
Combo Rx
Combo Rx
OtherMono Rx
Biologics
Mono Rx Combo Rx
Adequate Response to Therapy
(active disease after 3 months max therapy)
DMARD = Disease-modifying antirheumatic drug; NSAID = nonsteroidal anti-inflammatory drug; MTX = methotrexate

Importance of Early AggressiveTreatment of RA
70% of patients have evidence of radiographic damage within the first
3 years
Critical window of opportunity
Dis
ease
O
nse
t
EarlyEarly EstablishedEstablished End StageEnd Stage

Traditional DMARDs(disease-modifying anti-rheumatic drugs)
Hydroxychloroquine
Sulfasalazine
Methotrexate
Leflunomide
Cyclosporin A
Gold
Azathioprine
D-penicillamine Leflunomide
*Not approved by FDA for treatment of patients with RA.ACR Subcommittee on RA Guidelines. Arthritis Rheum. 2002;46:328–346.
D-penicillamine
Minocycline*
Modes of ActionMethotrexate (MTX) and Leflunomide
Methotrexate competitively and reversibly inhibits dihydrofolate reductase (DHFR), an enzyme that participates in the tetrahydrofolate synthesis.1
Leflunomide immunomodulates by inhibiting Leflunomide immunomodulates by inhibiting dihydroorotate dehydrogenase (an enzyme involved in de novo pyrimidine synthesis) (abbreviation DHODH).2
1. Rheumatrex (methotrexate sodium tablets). Prescribing information. October 2003. 2. Arava tablets (leflunomide). [Prescribing information]. July 2007.

DMARDs Retention Rates(since 1999)
Survival of Treatment Effectiveness (matched analysis)
Leflunomide (n=168)
Sulfasalazine (n=159)
Methotrexate (n=168)
*3-year moving averages.Aletaha D, et al. Ann Rheum Dis. 2003;62:944-951.

Corticosteroids in Clinical Practice Intra-articular injection if a single inflamed joint contributes
significantly to disability1
Systemic therapy as “bridging therapy” when DMARDs have been initiated but have not taken effect1
When DMARDs have been maximized, attempts should be made to discontinue the corticosteroid2discontinue the corticosteroid2
RA disease activity flares may occur with abrupt discontinuation or rapid tapering2
-Taper slowly over 1 to 2 months
Some patients may require chronic therapy1,2
-Use the lowest effective dose1. Rindfleisch JA, et al. Am Fam Physician. 2005;72:1037-1047, 1049-1050.2. Knell ME. In: Schumock GT, ed. Pharmacotherapy Self-Assessment Program. 2005:41-88;
CorticosteroidsRisk/Benefit and Safety
Acceptable risk of adverse effects (AEs) during moderate- and long-term use in RA1
AEs include2-4:– Weight gain– Hypertension (HTN)– Diabetes– Cataracts – Cataracts – Osteoporosis– Cardiovascular events
Baseline: evaluate for HTN, hyperglycemia, osteoporosis4
Evaluate for AEs each visit4
Frequent intra-articular injections may cause systemic effects4
1. Gotzsche PC, et al. Cochrane Database Syst Rev .2004:CD000189; 2. Combe B. Best Pract Res Clin Rheum. 2007;21:17-42; 3. Davis JM III, et al. Arthritis Rheum. 2007;56:820–830;4. Knell ME. In: Schumock GT, ed. Pharmacotherapy Self-Assessment Program. 2005:41-88.

Current Biologic Therapies
Agent Subclass Dosage and Administration
Etanercept TNF-α inhibitor 50 mg: SC every week
Infliximab TNF-α inhibitor 3 mg/kg: IV on Day 1; 2 weeks; 6 weeks; then every8 weeks thereafter
Adalimumab TNF-α inhibitor 40 mg: SC every other week
Anakinra IL-1 inhibitor 100 mg: SC dailyAnakinra(not widely used in US)
Rituximab B-cell ablator Initial dose 1000 mg IV infusions week one and two with 100 mg IV methylprednisone
Repeat same regimen every 6 weeks if needed
Abatacept Costimulatory T-cell inhibitor
250 mg single dose vial
Induction weeks 0,2,4;maintenance every 4 weeks
Body Weight of Patient Dose Number of vials
<60 kg 500 mg 2
60 to 100 kg 750 mg 3
> 100kg 1000 mg` 4

CASE STUDY and DISCUSSION ONE
Aggressive Treatment Strategy in Early Management
of Rheumatoid Arthritis
Supported by an educational grant from Amgen Inc and Wyeth PharmaceuticalsThis educational activity has been facilitated by Gullapalli & Associates, LLC.

Importance of Early RA Diagnosis
• SC waited to see her primary care physician until the pain and stiffness were so bad she could not grip the tennis racket
• Referred to a rheumatologistCase study 1
• RF and CCP +
• CRP elevated
• Started on combination DMARD treatment with MTX + SSZ
• SC, a 45-year-old woman, took up tennis 3 times per week with friends after her child started school
• Almost 1 year ago, she noticed pain and swelling in her hands, which she attributed to tennis and aging

ARS Question
What are the implications of this delay in treatment?
A. More likely to have progressive radiologic damage
B. Higher risk for functional disability
C. Less likely to achieve remissionC. Less likely to achieve remission
D. A and B
E. B and C
F. A, B, and C

Difficulty in Diagnosis of Early RA
>100 types of arthritis1
Early inflammatory arthritis may2:
– Develop into established RA or another definite
Most early UA is self-limiting3
28% with UA develop RA4
No diagnostic tests and – Develop into established RA or another definite arthropathy
– Stay undifferentiated
– Go in to remission
No diagnostic tests and criteria to clearly define early RA2,4
1. Di Martino SJ, et al. HSS Journal. 2005;1:107-109; 2. Combe B. Best Pract Res Clin Rheumatol. 2007;21:17-42;3. Visser H. Best Pract Res Clin Rheumatol. 2005;19:55-72; 4. Mochan E, et al. Am Fam Physician. 2008;77:1451-1453.
UA = Undifferentiated arthritis

Improving the Outcome andDiagnosis of Early RA
First, identify inflammatory arthritis
Consider differential diagnosis of other forms of arthritis (eg, lupus, psoriatic arthritis, seronegative spondylarthropathies)spondylarthropathies)
Finally, estimate the risk of developing persistent and/or erosive irreversible arthritis and develop an optimal therapeutic strategy
Combe B. Best Pract Res Clin Rheumatol. 2007;21:17-42.
Consider Alternative DiagnosisIf…
Mucosal ulcers Photosensitivity Psoriasis Skin rashes Raynaud’s Ocular inflammation Ocular inflammation Urethritis Inflammatory bowel disease (IBD) Infectious diarrhea Nephritis Isolated distal interphalangeal (DIP) joints
British Columbia Ministry of Health Guidelines: RA: Diagnosis and Management. Available at: http://www.health.gov.bc.ca/gpac/pdf/ra_guideline_summary.pdf.

Early Diagnosis and Treatment of RA:The Window of Opportunity
Damage occurs within weeks of symptom onset1
90% have radiologic damage at 2 years2
Evidence of damage before intervention can no longer be justified2
Early aggressive therapy improves disease outcomes
1. McGonagle D, et al. Arthritis Rheum. 1999;42:1706–1711; 2. Quinn MA, et al. Rheum Dis Clin North Am. 2005;31:763–772.

RA May Be PreventedWith PROMPT Treatment
The PRObable rheumatoid arthritis: Methotrexate versus Placebo Treatment (PROMPT) study was a double-blind, placebo-controlled, randomized, multicenter trial involving 110 patients with undifferentiated arthritis (UA) who fulfilled the ACR 1987 criteria for probable RA.who fulfilled the ACR 1987 criteria for probable RA.
Results: Anti-CCP-positive UA patients, who have the highest risk of developing RA, benefit from early MTX treatment.
PROMPT: PRObable rheumatoid arthritis: Methotrexate versus Placebo Treatment studyMethotrexate (MTX) group is indicated by the broken line, the placebo group is indicated by the solid line, and dropouts areindicated by circles.
van Dongen H, et al. Presented at: ACR 70th Annual Meeting; November 12, 2006; Washington, DC. Abstract 657..

RA May Be PreventedWith PROMPT Treatment (cont’d)
van Dongen H, et al. Presented at: ACR 70th Annual Meeting; November 12, 2006; Washington, DC. Abstract 657..
PROMPT: PRObable rheumatoid arthritis: Methotrexate versus Placebo Treatment studyMethotrexate (MTX) group is indicated by the broken line, the placebo group is indicated by the solid line, and dropouts areindicated by circles.

ASPIRE TrialInfliximab + MTX in Early RA
The percentages of patients achieving remission of their disease according to the DAS28 at week 54 are shown for the 3 treatment groups.
St. Clair EW, et al. Arthritis Rheum. 2004;50:3432-3443.
ASPIRE: Active-Controlled Study of Patients Receiving Infliximab for the Treatment of RA of Early Onset; DAS28 = Disease activity score using 28 joint counts
for the 3 treatment groups.
In early stages of active RA combination therapy with Infliximab and MTX provides greater clinical, radiographic and functional benefits than treatment with MTX alone

PREMIER TrialAdalimumab + MTX in Early RA
49% of patients in combination therapy group had remission based on DAS28 <2.6 at 2 years
In early, aggressive RA, combination therapy with adalimumab + MTX was
Radiographic progression (Sharp units)
adalimumab + MTX was significantly superior to either MTX alone or adalimumab alone in improving signs and symptoms of disease, inhibiting radiographic progression, and effecting clinical remission
Breedveld FC, et al. Arthritis Rheum. 2006;54:26-37.

COMET TrialMTX vs Combined MTX + Etanercept
274 participants randomized to double-blind combined parallel treatment and 268 MTX alone
Clinical remission and radiographic progression are achievable in early severe RA achievable in early severe RA within 1 year of combined treatment with etanercept + MTX
COMET : Comparison of methotrexate monotherapy with a combination of methotrexate and etanercept in active, early, moderate to severe rheumatoid arthritis
Emery P, et al. Lancet. 2008 Aug 2;372(9636):375-378.
DAS28 remission (< 2.6) over 52 weeks of treatment

Importance of Early Referral
Disease duration is the most important factor predicting response to treatment4 , best response if treated within 1yr2
33% less long-term radiographic progression with early treatment4,5
Patients presenting with arthritis of >1 joint should be seen by a rheumatologist within 6 weeks3rheumatologist within 6 weeks3
DMARDs should be started within 12 weeks6
Only 17% of patients are seen in this timeframe1
Normal inflammatory markers, negative serology, and normal X-rays are not reasons for delaying referral
1. Aletaha D, et al. Ann Rheum Dis. 2004;63:1269-1275; 2. Anderson JJ, et al. Arthritis Rheum. 2000;43:22-29; 3. Combe B, et al. Ann Rheum Dis. 2007;66:34-45; 4. Finckh A, et al. Arthritis Rheum. 2006;55:864-872; 5. Hyrich KL. BMJ. 2008;336:215-216; 6. Luqmani R, et al. Rheumatology . 2006;45:1167-1169.

Importance of AggressiveManagement in Early RA
Case study 1 (cont’d) • At a follow-up visit 6 months later, SC reports some improvement in symptoms, and there are mild radiographic changes since her baseline X-rays; however, she reports that her activity is still reports that her activity is still significantly limited
• What are the next steps?
ARS Question
How often should SC have follow-up visits until she achieves disease remission?
A. Every 1 to 3 months
B. Every 6 monthsB. Every 6 months
C. Once a year
ARS Question
Which of the following are recommended for monitoring RA disease activity?
A. Antinuclear antibody (ANA)
B. Rheumatoid factor (RF)B. Rheumatoid factor (RF)
C. C-reactive protein (CRP)
D. A and B
E. B and C
F. A, B, and C

Disease Activity MonitoringEULAR Recommendations
Monitoring of disease activity should include: – Tender and swollen joint count– Patient’s and physician’s global assessments– ESR and CRP
Arthritis activity should be assessed q 1 to 3 months as long as remission not achieved
Arthritis activity should be assessed q 1 to 3 months as long as remission not achieved
Structural damage assessed using radiographs of the hands and feet every 6 to 12 months during the first few years
Functional assessment (HAQ) can be used to complement the
disease activity and structural damage monitoring
Combe B, et al. Ann Rheum Dis. 2007;66:34–45.
HAQ = Health Assessment Questionnaire
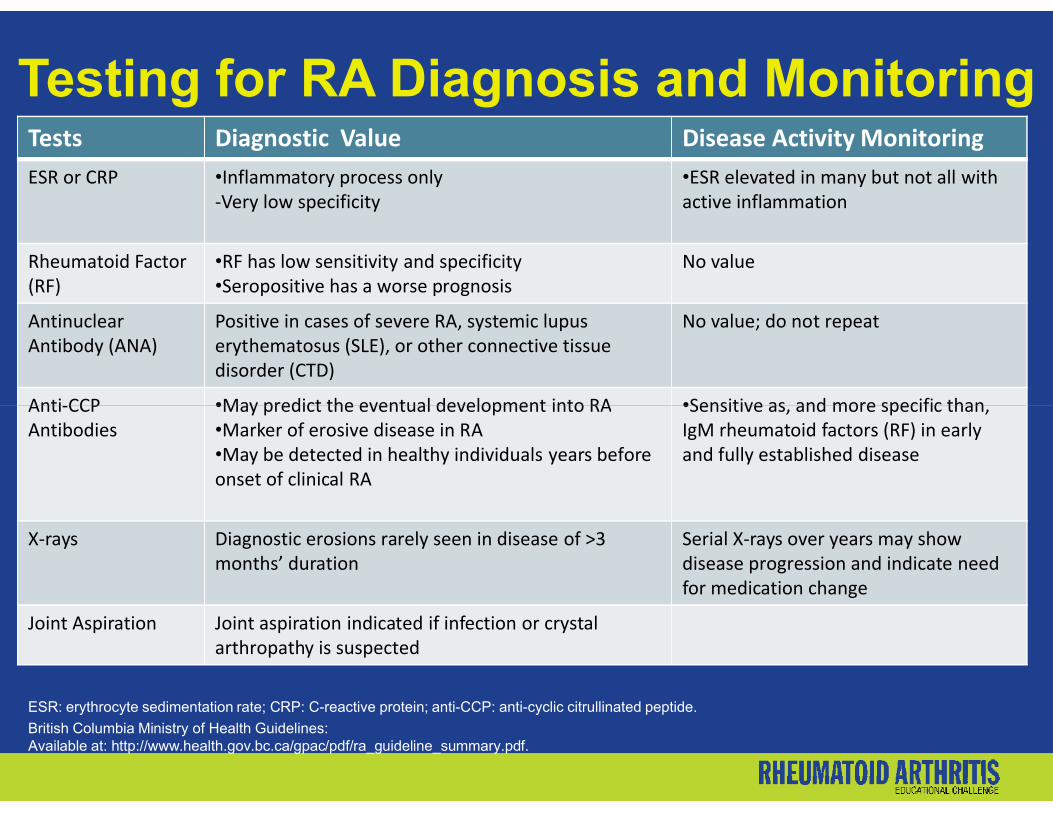
Testing for RA Diagnosis and MonitoringTests Diagnostic Value Disease Activity MonitoringESR or CRP •Inflammatory process only
-Very low specificity•ESR elevated in many but not all with active inflammation
Rheumatoid Factor (RF)
•RF has low sensitivity and specificity•Seropositive has a worse prognosis
No value
Antinuclear Antibody (ANA)
Positive in cases of severe RA, systemic lupus erythematosus (SLE), or other connective tissue disorder (CTD)
No value; do not repeat
Anti-CCP •May predict the eventual development into RA •Sensitive as, and more specific than, Anti-CCP Antibodies
•May predict the eventual development into RA•Marker of erosive disease in RA •May be detected in healthy individuals years before onset of clinical RA
•Sensitive as, and more specific than, IgM rheumatoid factors (RF) in early and fully established disease
X-rays Diagnostic erosions rarely seen in disease of >3 months’ duration
Serial X-rays over years may show disease progression and indicate need for medication change
Joint Aspiration Joint aspiration indicated if infection or crystal arthropathy is suspected
ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; anti-CCP: anti-cyclic citrullinated peptide.
British Columbia Ministry of Health Guidelines: Available at: http://www.health.gov.bc.ca/gpac/pdf/ra_guideline_summary.pdf.

Implications of Chronic DiseaseTreatment Goals for RA
Reduce pain and inflammation
Reduce disability
Prevent radiological damage and progression Prevent radiological damage and progression
Reduce the development of comorbidities
Achieve disease remission
Knell ME. In: Schumock GT, ed. Pharmacotherapy Self-Assessment Program. 2005:41-88.
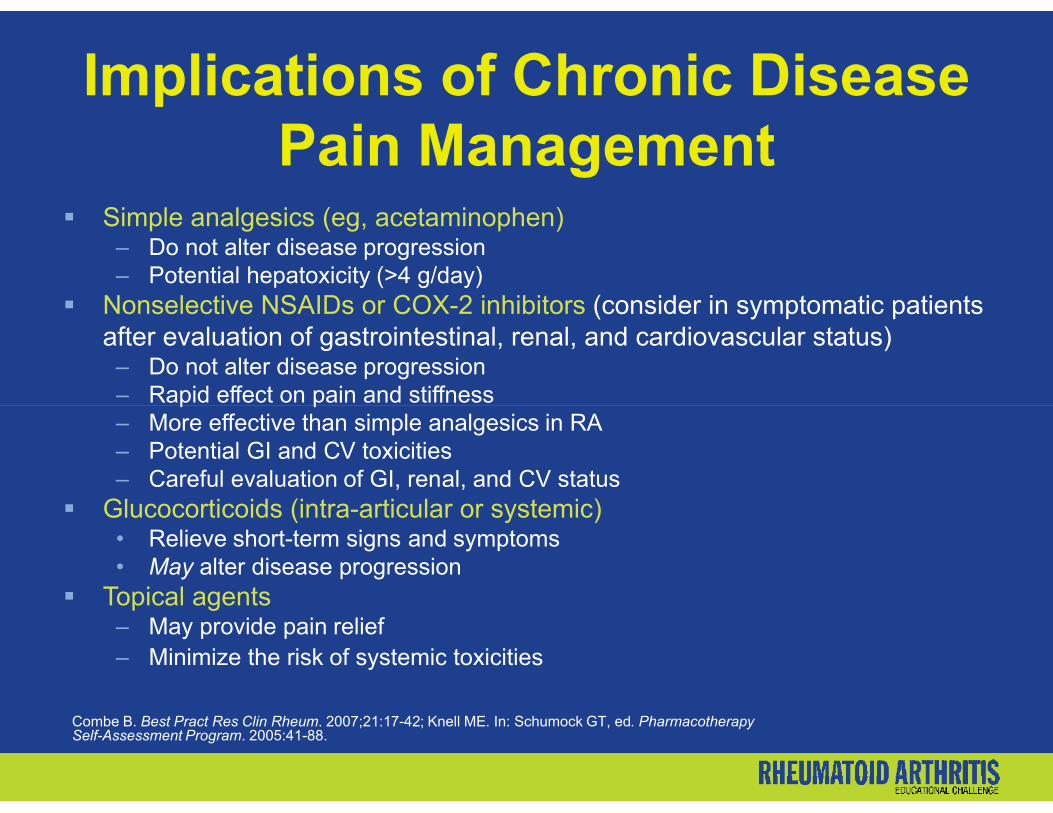
Implications of Chronic DiseasePain Management
Simple analgesics (eg, acetaminophen)– Do not alter disease progression– Potential hepatoxicity (>4 g/day)
Nonselective NSAIDs or COX-2 inhibitors (consider in symptomatic patients after evaluation of gastrointestinal, renal, and cardiovascular status)
– Do not alter disease progression– Rapid effect on pain and stiffness– Rapid effect on pain and stiffness– More effective than simple analgesics in RA– Potential GI and CV toxicities– Careful evaluation of GI, renal, and CV status
Glucocorticoids (intra-articular or systemic)• Relieve short-term signs and symptoms • May alter disease progression
Topical agents – May provide pain relief– Minimize the risk of systemic toxicities
Combe B. Best Pract Res Clin Rheum. 2007;21:17-42; Knell ME. In: Schumock GT, ed. Pharmacotherapy Self-Assessment Program. 2005:41-88.

Important Times forPsychosocial Interventions
A significant medical diagnosis like RA may lead to a psychosocial crisis
Patients living with chronic illness require sensitive psychosocial carepsychosocial care
When compliance or lifestyle issues impinge on health, interventions that focus on biologic mechanisms alone are likely to be ineffective
Ahmed SM, et al. In: Rakel RE, ed. Textbook of Family Medicine. 2007:35-41.
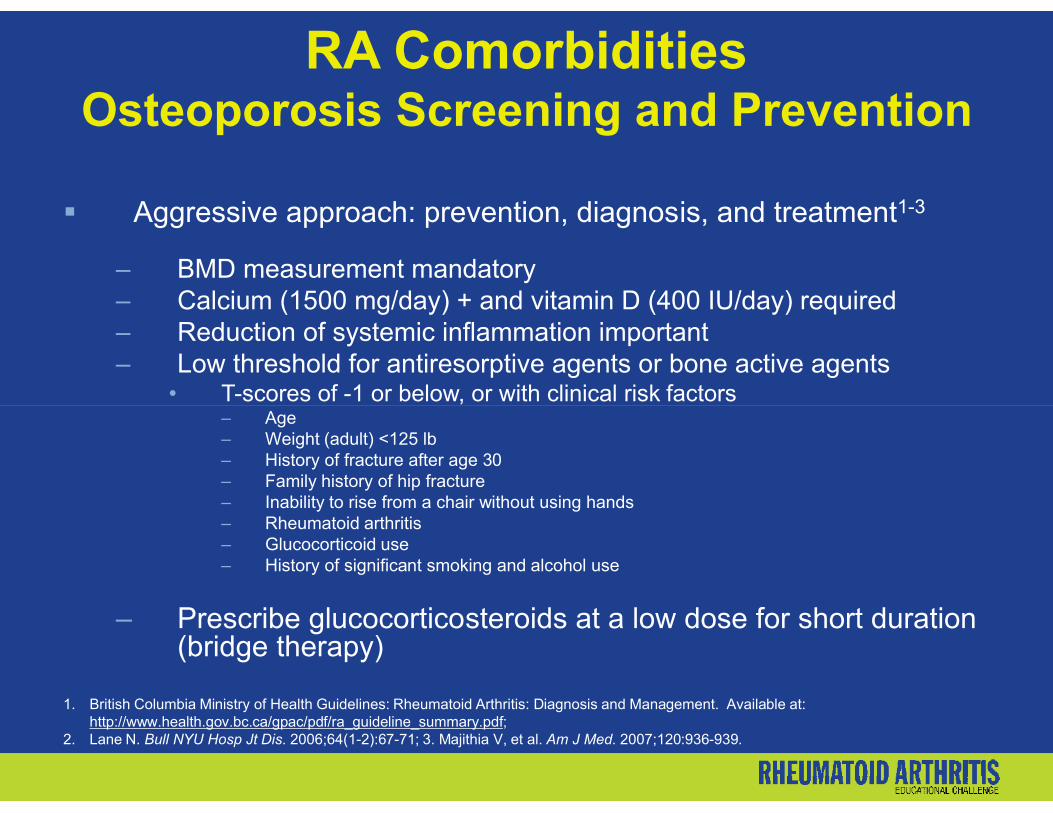
RA ComorbiditiesOsteoporosis Screening and Prevention
Aggressive approach: prevention, diagnosis, and treatment1-3
– BMD measurement mandatory– Calcium (1500 mg/day) + and vitamin D (400 IU/day) required – Reduction of systemic inflammation important – Low threshold for antiresorptive agents or bone active agents
• T-scores of -1 or below, or with clinical risk factors• T-scores of -1 or below, or with clinical risk factors– Age– Weight (adult) <125 lb– History of fracture after age 30– Family history of hip fracture– Inability to rise from a chair without using hands– Rheumatoid arthritis– Glucocorticoid use– History of significant smoking and alcohol use
– Prescribe glucocorticosteroids at a low dose for short duration (bridge therapy)
1. British Columbia Ministry of Health Guidelines: Rheumatoid Arthritis: Diagnosis and Management. Available at: http://www.health.gov.bc.ca/gpac/pdf/ra_guideline_summary.pdf;
2. Lane N. Bull NYU Hosp Jt Dis. 2006;64(1-2):67-71; 3. Majithia V, et al. Am J Med. 2007;120:936-939.

RA ComorbiditiesCardiovascular Disease
RA increases risk of atherosclerotic CVD1,2,3
– Not explained by traditional CV risk factors
– Associated with increased mortality in RA
– Management of dyslipidemia and minimizing CV risk factors
1. British Columbia Ministry of Health Guidelines: Rheumatoid Arthritis: Diagnosis and Management.2. Available at: http://www.health.gov.bc.ca/gpac/pdf/ra_guideline_summary.pdf; 3. 2. Dixon WG, et al. Ann Rheum Dis. 2007;66(9):1132-6; 3. La Montagna G, et al. Diab Vasc Dis Res. 2007;4(2):130-5.
Cardiovascular morbidity in a community-based RA sample, compared with general population
Turesson et al 2004

Benefit Profiles and
CASE STUDY and DISCUSSION TWO
Benefit Profiles and Appropriate Administration of Biological/TNF-αAntagonist Therapies in the Management of RA Patients
Supported by an educational grant from Amgen Inc and Wyeth PharmaceuticalsThis educational activity has been facilitated by Gullapalli & Associates, LLC.

Choice of Initial DMARD JC: 38-year-old black female
Single mother, works as a construction worker
Past medical history– Moderate RA, recently diagnosed – Experiences pain and stiffness on “bad days” – Experiences pain and stiffness on “bad days” – Peptic ulcer disease, currently active– Type 2 diabetes mellitus– Currently taking prednisone 10 mg/d
Case study 2

Choice of Initial DMARD (cont’d) Current symptoms
– Morning stiffness – 1 hour– Difficulty with handling power tools and climbing ladders at work– Significant fatigue
Physical exam– 15 tender, 12 swollen joints– 15 tender, 12 swollen joints
Laboratory and X-ray– Sedimentation rate 45– CRP 1.9– Hematocrit 33– Glucose 145– Hand and feet films – erosions noted in MCPs and MTPs
MCPs = metacarpophalangeal joints; MTPs = metatarsophalangeal joints

ARS Question
What is the best choice for initial DMARD therapy for JC?
A. MethotrexateB. LeflunomideC. HydroxychloroquineC. HydroxychloroquineD. Sulfasalazine
ARS Question
What baseline monitoring should be performed before starting treatment with MTX?
A. CBCB. CreatinineC. LFTsC. LFTsD. A and BE. B and CF. A, B, and C

Drug Dosage Adverse Events Monitoring
MethotrexateImmunosuppressant
15-25 mg orally,
SC or IM once weekly
GI intolerance (nausea, vomiting, abdominal pain), oral ulcers, alopecia, hepatitis; rare pulmonary toxicity
- Baseline: CBC + diff, LFTs, renal function, chest X-ray
- CBC, Cr, and LFTs monthly x 6, then q 1-2 months
- Adjust dose or dc if elevated LFTs
Traditional DMARDs: Safety
elevated LFTs
LeflunomideImmunosuppressant
20 mg po daily GI intolerance (nausea, vomiting, abdominal pain), skin rash (rare Stevens-Johnson & toxic epidermal necrolysis), alopecia, hepatic toxicity, leukopenia, thrombocytopenia; highly teratogenic
-Hepatitis B and C serology in high-risk patients
-CBC, Cr, and LFTs monthly x 6, then q 1-2 months
-Reduce dose or dc if elevated LFTs
Khurana R, et al. Pathophysiology. 2005;12:153-165; Knell ME. In: Schumock GT, ed. Pharmacotherapy Self-Assessment Program. 2005:41-88; Majithia V, et al. Am J Med. 2007;120:936-939; Leflunomide prescribing information, July 2007; Methotrexate prescribing information, Oct. 2003.

Drug Dosage Adverse Events Monitoring
Hydroxy-chloroquineAntimalarial
200-400 mg po daily
GI intolerance (nausea, vomiting, abdominal pain, diarrhea), retinal toxicity (contraindication), rash, hepatitis, leukopenia, thrombocytopenia
- Baseline and q 3 months ophthalmologic examinations (including visual acuity, expert slit-lamp, funduscopic, and visual field tests)
- Regular knee and ankle reflexes
Traditional DMARDs: Safety (cont’d)
SulfasalazineAnti-inflammatory
2-3 g daily
(start at 500 mg/day & increase by 500 mg/week)
GI intolerance, oral ulcers, cytopenia, rash
- CBC + diff, LFTs at baseline, qow for 1st 3 months, then monthly x 3 months, then q 3 months
- UA with microscopic evaluation, renal function routinely
- Clinical signs of blood dyscrasias
Hydroxychloroquine prescribing information, April 2002; Khurana R, et al. Pathophysiology. 2005:12:153-165; Knell ME. In: Schumock GT, ed. Pharmacotherapy Self-Assessment Program. 2005:41-88; Majithia V, et al. Am J Med. 2007;120:936-939; Sulfasalazine prescribing information, Dec. 2003.
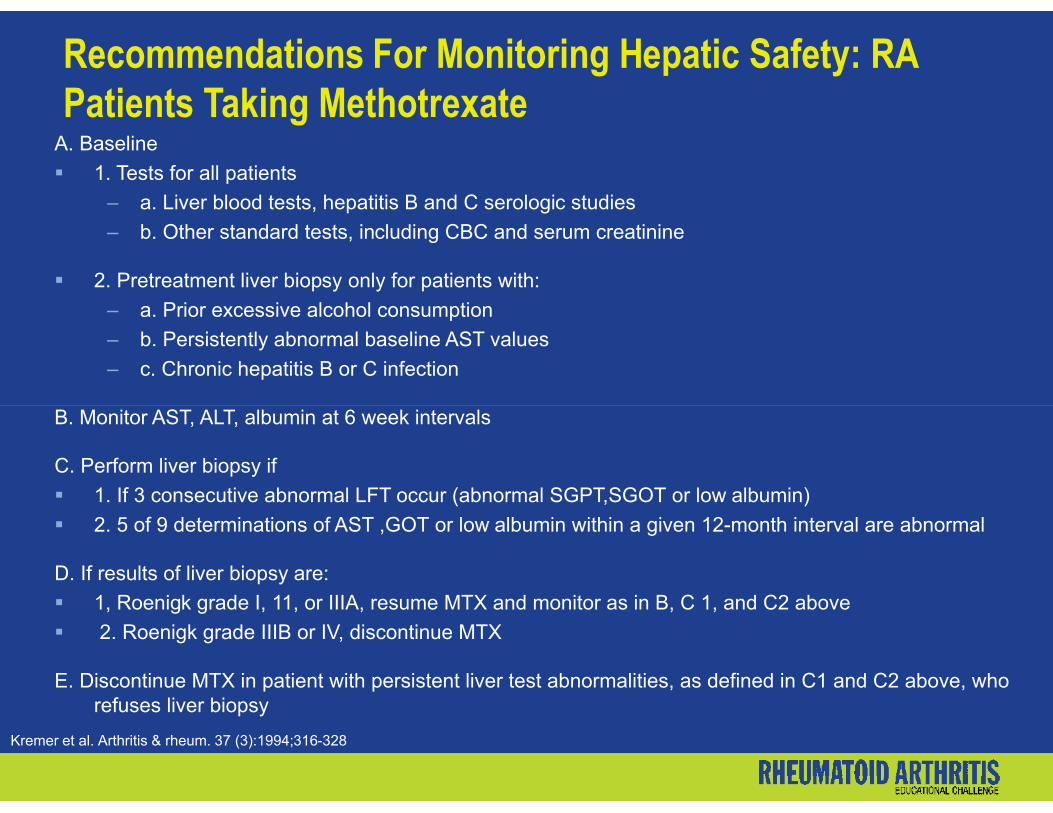
Recommendations For Monitoring Hepatic Safety: RA Patients Taking Methotrexate
A. Baseline
1. Tests for all patients
– a. Liver blood tests, hepatitis B and C serologic studies
– b. Other standard tests, including CBC and serum creatinine
2. Pretreatment liver biopsy only for patients with:
– a. Prior excessive alcohol consumption
– b. Persistently abnormal baseline AST values
– c. Chronic hepatitis B or C infection
Kremer et al. Arthritis & rheum. 37 (3):1994;316-328
B. Monitor AST, ALT, albumin at 6 week intervals
C. Perform liver biopsy if
1. If 3 consecutive abnormal LFT occur (abnormal SGPT,SGOT or low albumin)
2. 5 of 9 determinations of AST ,GOT or low albumin within a given 12-month interval are abnormal
D. If results of liver biopsy are:
1, Roenigk grade I, 11, or IIIA, resume MTX and monitor as in B, C 1, and C2 above
2. Roenigk grade IIIB or IV, discontinue MTX
E. Discontinue MTX in patient with persistent liver test abnormalities, as defined in C1 and C2 above, who refuses liver biopsy

TICORA (Tight Control of RA) Trial
Compared with routine care, patients treated intensively were more likely to be in remission (disease activity score <1.6; 36/55 [65%] vs 9/55 [16%], 9.7 [3.9–23.9], P <.0001).
Patients in the intensive group were more likely to be prescribed combination disease-modifying antirheumatic drug therapy than were those in the routine group (37 [67%] vs 6 [11%]).
Grigor C, et al. Lancet. 2004;364:263–269.
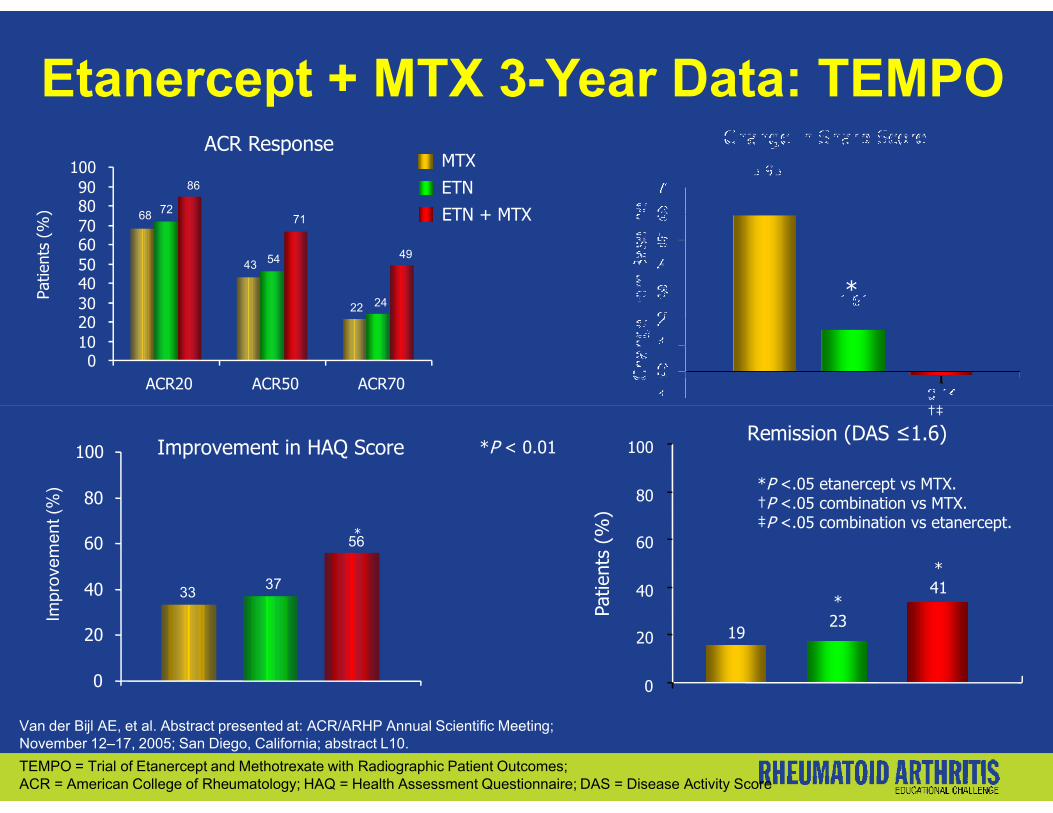
Etanercept + MTX 3-Year Data: TEMPOMTX
ETN
ETN + MTX
*
†‡
ACR Response
22
43
68 72
24
54 49
71
86
0102030405060708090
100
ACR20 ACR50 ACR70
Patie
nts
(%)
*P <.05 etanercept vs MTX.†P <.05 combination vs MTX.‡P <.05 combination vs etanercept.
Remission (DAS ≤1.6)
19
*23
*41
0
20
40
60
80
100
Patie
nts
(%)
†‡
Van der Bijl AE, et al. Abstract presented at: ACR/ARHP Annual Scientific Meeting; November 12–17, 2005; San Diego, California; abstract L10.
*
*P < 0.01Improvement in HAQ Score
3337
56
0
20
40
60
80
100
Impr
ovem
ent (
%)
TEMPO = Trial of Etanercept and Methotrexate with Radiographic Patient Outcomes; ACR = American College of Rheumatology; HAQ = Health Assessment Questionnaire; DAS = Disease Activity Score

Patie
nts
(%)
Adalimumab + MTX (ARMADA):ACR Responses at 24 Weeks
Placebo + MTX (n = 62)Adalimumab 20 mg eow + MTX (n = 69)Adalimumab 40 mg eow + MTX (n = 67)Adalimumab 80 mg eow + MTX (n = 73)
**
**
*
*†
Patie
nts
(%)
*P <.0001; †P = .003; ‡P <.02.
Keystone E, et al. Ann Rheum Dis. 2001;60(suppl 1):67.ACR = American College of Rheumatology
ACR20 ACR50 ACR70
‡
*

ASPIRE + MTX: Results at Week 54
*P <.05 vs MTX alone.†P <.01 vs MTX alone.
ACR20 ACR50 ACR70 INF3 mg/kg+ MTX
INF 6 mg/kg+ MTX
MTXAlone
Patie
nts
(%)
100
75
50
25
0
6576† 76†
Change in HAQ >0.25
50 P <.01 vs MTX alone.‡P <.001 vs MTX alone.
Smolen J, et al. Abstract presented at: ACR/ARHP Annual Scientific Meeting; November 12–17, 2005; San Diego, California; abstract 35. St. Clair EW, et al. Arthritis Rheum. 2004;50:3432-3443; van der Heijde D, et al. Abstract presented at: EULAR Annual Meeting; June 8–11, 2005; Vienna, Austria; abstract SAT0028. 7
Change in DAS28
vdH-S Score> SDC
(SDC = 6.4)
Erosion Score> SDC
(SDC = 5.6)
JSN Score> SDC
(SDC = 2.0)
+ MTX + MTX
-4
0
Med
ian
Chan
ge -1
-2
-3
-2.0
-2.7†
-3.2‡
19 18
108 7
44 3 4
0
10
20
30
40
50
Patie
nts
(%)
ASPIRE = Active-Controlled Study of Patients Receiving Infliximab for the Treatment of Rheumatoid Arthritis of Early Onset; HAQ = Health Assessment Questionnaire; DAS 28 = Disease Activity Score with 28 joint count

Abatacept: AIM Extension StudyACR50 Results at 1, 2, and 3 Years
N = 151 each year
Patie
nts
Achi
evin
g AC
R50
(%
)
P < .001.Westhovens R, et al. Ann Rheum Dis. 2006;65(suppl 2):512 [abstract SAT0203].
Patie
nts
Achi
evin
g AC
R50
(%
)
AIM = Abatacept in Inadequate responders to Methotrexate
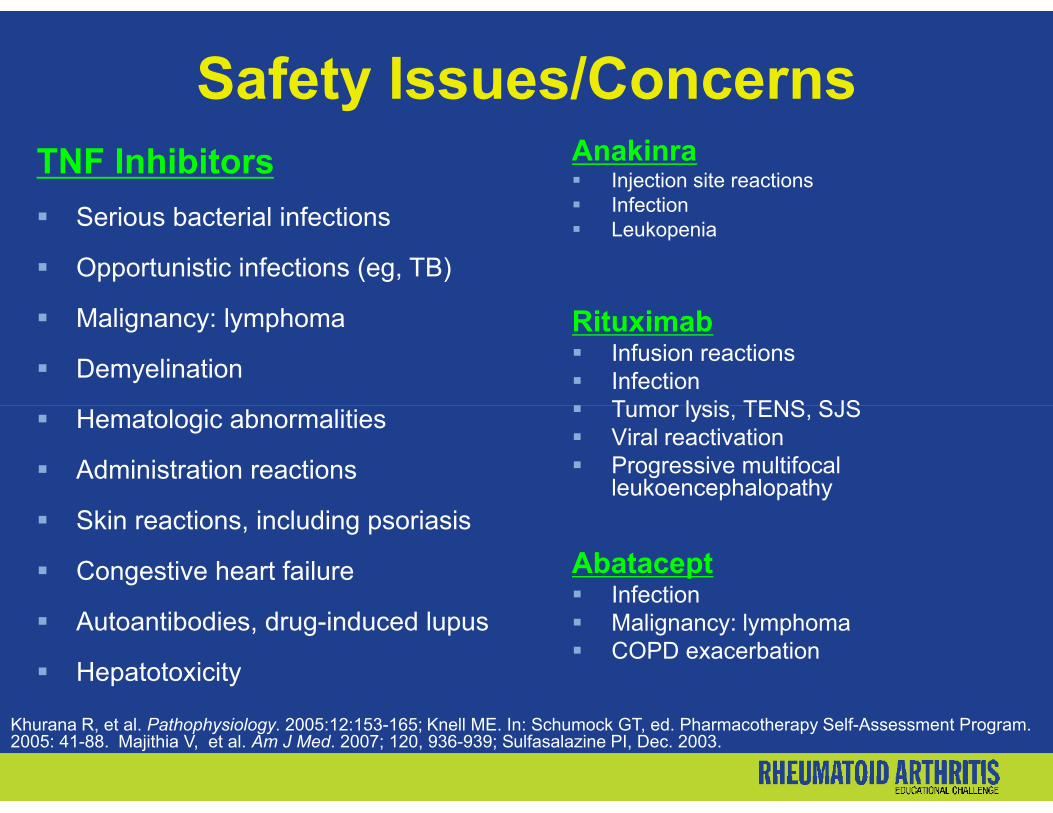
Safety Issues/ConcernsTNF Inhibitors
Serious bacterial infections
Opportunistic infections (eg, TB)
Malignancy: lymphoma
Demyelination
Hematologic abnormalities
Anakinra Injection site reactions Infection Leukopenia
Rituximab Infusion reactions Infection Tumor lysis, TENS, SJS Hematologic abnormalities
Administration reactions
Skin reactions, including psoriasis
Congestive heart failure
Autoantibodies, drug-induced lupus
Hepatotoxicity
Tumor lysis, TENS, SJS Viral reactivation Progressive multifocal
leukoencephalopathy
Abatacept Infection Malignancy: lymphoma COPD exacerbation
Khurana R, et al. Pathophysiology. 2005:12:153-165; Knell ME. In: Schumock GT, ed. Pharmacotherapy Self-Assessment Program. 2005: 41-88. Majithia V, et al. Am J Med. 2007; 120, 936-939; Sulfasalazine PI, Dec. 2003.
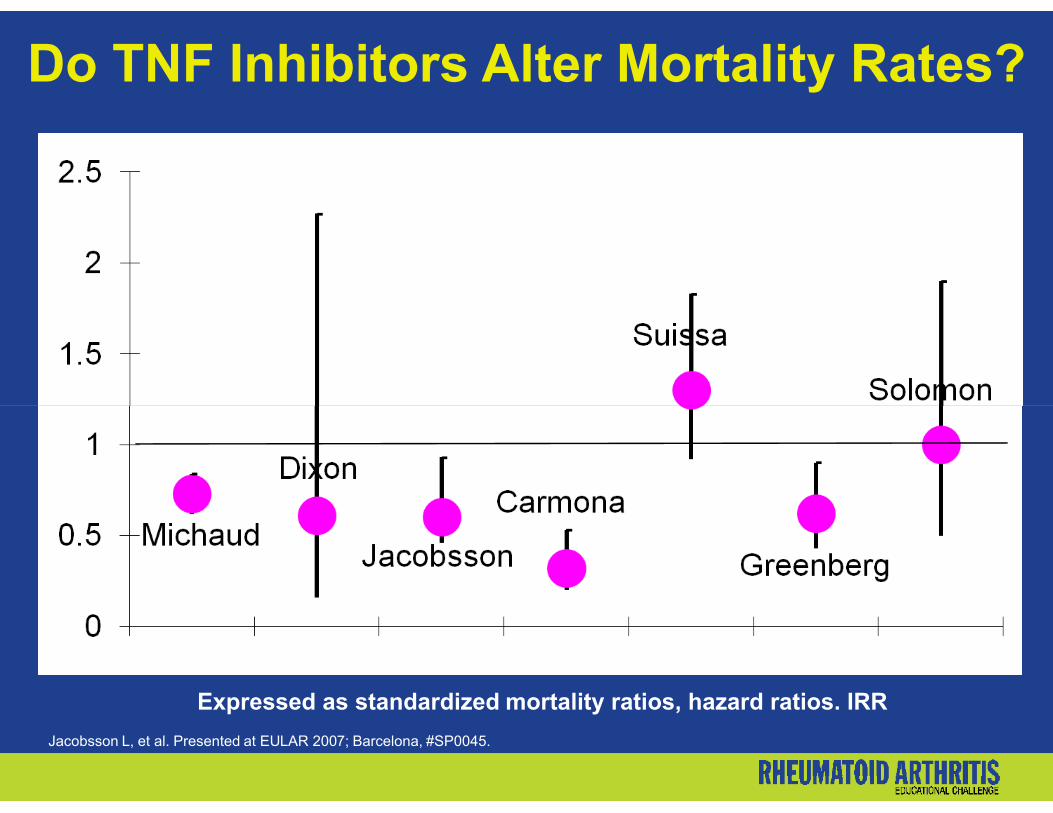
Do TNF Inhibitors Alter Mortality Rates?
Expressed as standardized mortality ratios, hazard ratios. IRR
Jacobsson L, et al. Presented at EULAR 2007; Barcelona, #SP0045.
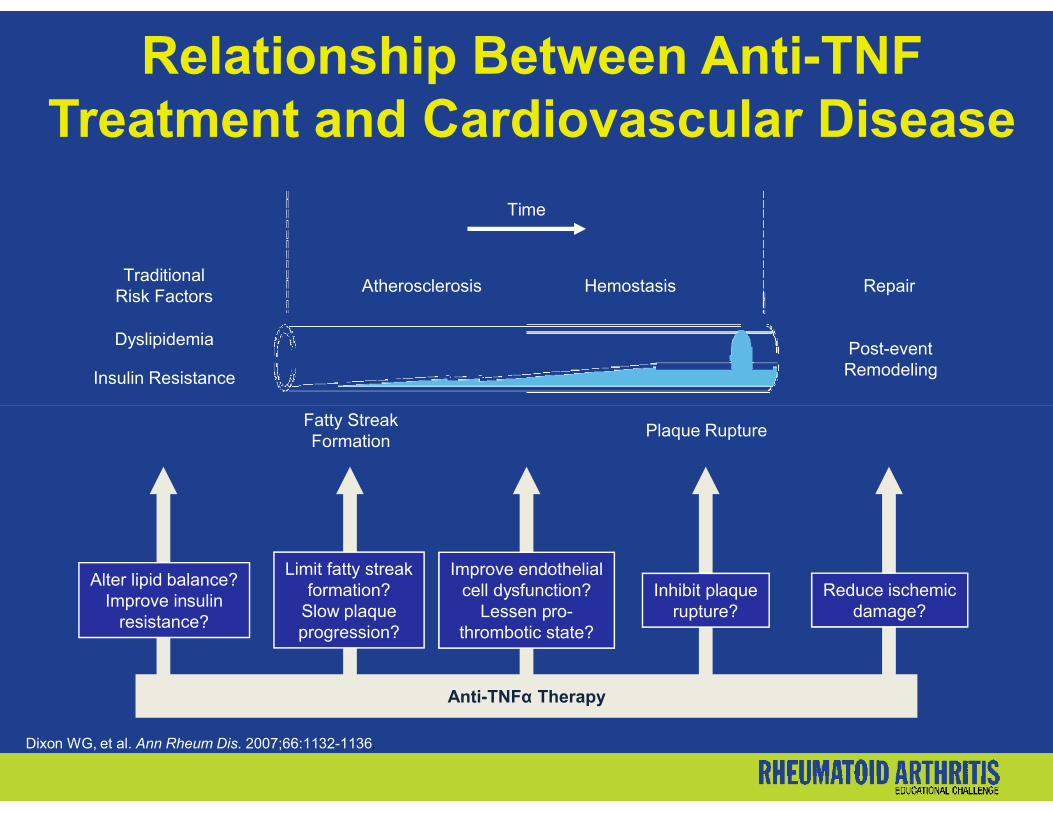
Relationship Between Anti-TNFTreatment and Cardiovascular Disease
Insulin Resistance
Dyslipidemia
TraditionalRisk Factors
Atherosclerosis Hemostasis Repair
Post-eventRemodeling
Time
Dixon WG, et al. Ann Rheum Dis. 2007;66:1132-1136.
Anti-TNFα Therapy
Fatty StreakFormation
Plaque Rupture
Alter lipid balance?Improve insulin
resistance?
Limit fatty streakformation?
Slow plaqueprogression?
Improve endothelialcell dysfunction?
Lessen pro-thrombotic state?
Inhibit plaquerupture?
Reduce ischemicdamage?

Myocardial Infarction and Cerebrovascular Accidents:
Anti-TNF Therapy vs DMARDs
United Kingdom registry prospectively followed previously anti-TNF-naive RA patients (N = 8076) versus subjects who received conventional DMARDs (N = 1351)
Dixon WG, et al. Ann Rheum Dis. 2006;65(suppl II):109.
Differences between groups does support the hypothesis that anti-TNF treatment may reduce cardiovascular risk by reducing inflammatory burden

Benefits on ComorbidityTNF-α Antagonists May Reduce Risk for CV Events
QUEST-RA study: reduced CV morbidity with:
– Methotrexate (HR 0.85; 95% CI 0.81 to 0.89)
– Leflunomide (HR 0.59; 95% CI 0.43 to 0.79)– Leflunomide (HR 0.59; 95% CI 0.43 to 0.79)
– Sulfasalazine (HR 0.92; 95% CI 0.87 to 0.98)
– Glucocorticoids (HR 0.95; 95% CI 0.92 to 0.98)
– Biologic agents (HR 0.42; 95% CI 0.21 to 0.81; P <.05)
Naranjo A, et al. Arthritis Res Ther. 2008;10(2):R30.
Infection Rates Among PatientsWith RA
RA patients have 3.1 to 9.57 serious infections per 100 patient-years (PY) exposure
These rates are higher than in patients without RA
Increased risk of infection in RA patients correlates with:– Degree of disability – Concomitant disease– Concomitant corticosteroids and other immunosuppressive
agents
Doran M, et al. Arthritis Rheum. 2002;46:2143–2151;Singh G, et al. Arthritis Rheum. 1999;42:S242.

Adalimumab Opportunistic InfectionsPostmarketing US Reports*
Patient-years exposed 55,384
Total number of cases 31
Candidiasis (16 oral and/or localized) 18
Histoplasmosis/Cocci 5
Pneumocystis carinii 2Pneumocystis carinii 2
Nocardiosis 1
Cryptococcal pneumonitis 2
Toxoplasmal eye infection 1
Listeriosis 2
US reporting rate per 100 patient-years 0.06
*Postmarketing spontaneous US reports of opportunistic infections with HUMIRA Dec 31, 2002–Dec 31, 2004.
Opportunistic Infections
Rituximab RA RCT (herpes zoster <5%)
NHL: no increase
– HIV pts: OI and death
Abatacept
No literature reports
RCT: no OI observed
– HIV pts: OI and death
Rare reports of PML
– Most in NHL (23/700,000)
– RA 0 cases
– SLE 2 cases
– RA 1 fatality reportedRCT = Randomized controlled trial; NHL = Non-Hodgkin’s lymphoma; OI = opportunistic infections; HIV = human immunodeficiency virus; RA = rheumatoid arthritis; PML = Progressive multifocal leukoencephalopathyhttp://www.fda.gov/medwatch/safety/2008/Rituxan_PI.pdf; accessed October 2008; http://www.fda.gov/cder/drug/InfoSheets/patient/abataceptPIS.htm; Accessed October 2008

Each visit: Evaluate for infection/obtain travel history
Investigate respiratory or neurologic symptoms, fever, constitutional symptoms
Prevention and Avoidance of InfectiousComplications
Stop biologics if signs of serious illness
High index of suspicion/consider coverage for unusual pathogens
Serious infections may present atypically
Saketoo LA, et al. Infect Dis Clin North Am. 2006;20:931–961.

Influenza vaccine seems to be safe but may not be effective
Pneumococcal vaccine ≥2 weeks before biologic use if not already given
Biologic Therapeutic Agentsand Vaccines
Update vaccinations before initiation of biologic therapy
Avoid live vaccines with all biologics
Saketoo LA, et al. Infect Dis Clin North Am. 2006;20:931–961.
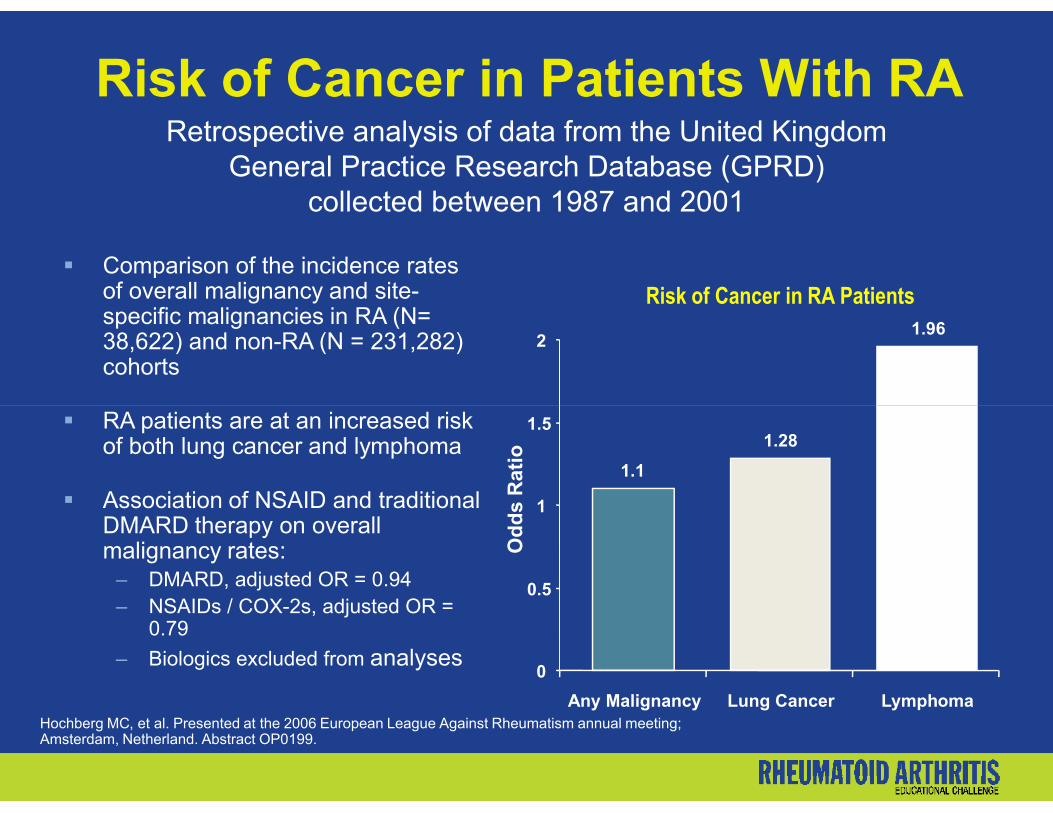
Risk of Cancer in Patients With RA
Comparison of the incidence ratesof overall malignancy and site-specific malignancies in RA (N= 38,622) and non-RA (N = 231,282) cohorts
Retrospective analysis of data from the United Kingdom General Practice Research Database (GPRD)
collected between 1987 and 2001
1.962
Risk of Cancer in RA Patients
RA patients are at an increased riskof both lung cancer and lymphoma
Association of NSAID and traditional DMARD therapy on overall malignancy rates:
– DMARD, adjusted OR = 0.94– NSAIDs / COX-2s, adjusted OR =
0.79
– Biologics excluded from analyses
Hochberg MC, et al. Presented at the 2006 European League Against Rheumatism annual meeting; Amsterdam, Netherland. Abstract OP0199.
1.1
1.28
0
0.5
1
1.5
Any Malignancy Lung Cancer Lymphoma
Od
ds
Rat
io
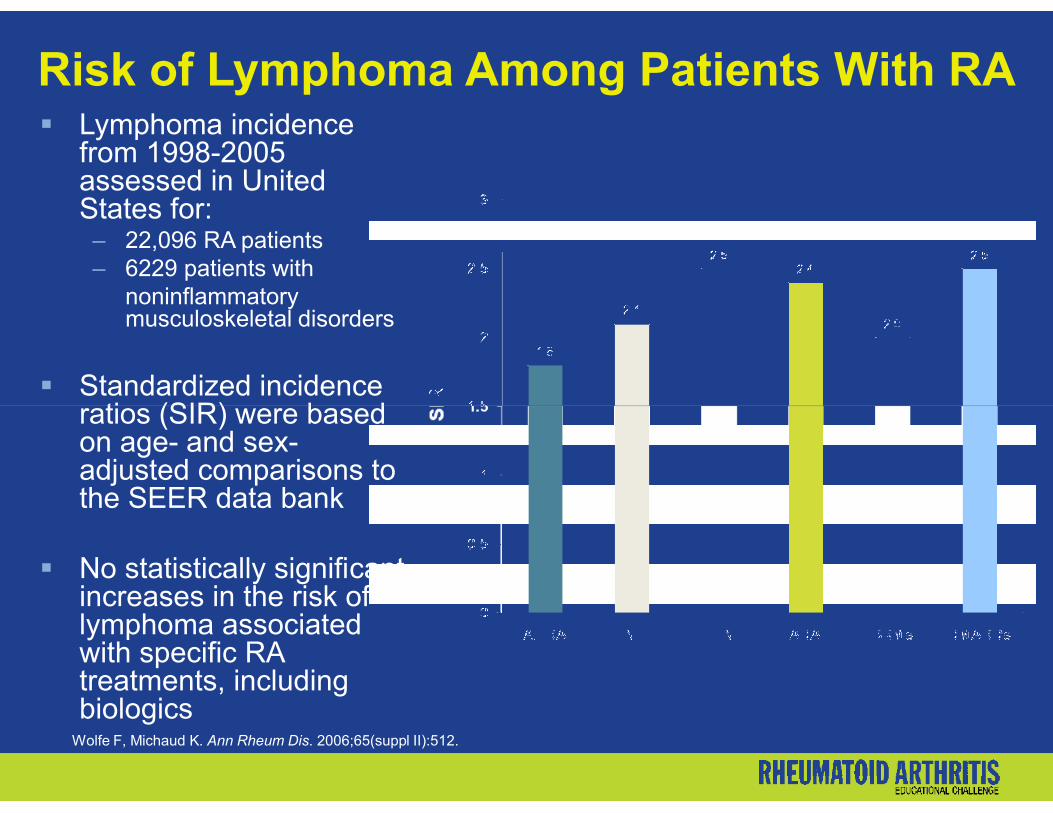
Risk of Lymphoma Among Patients With RA Lymphoma incidence
from 1998-2005 assessed in United States for:
– 22,096 RA patients– 6229 patients with
noninflammatory musculoskeletal disorders
Standardized incidence ratios (SIR) were based ratios (SIR) were based on age- and sex-adjusted comparisons to the SEER data bank
No statistically significant increases in the risk of lymphoma associated with specific RA treatments, including biologics
Wolfe F, Michaud K. Ann Rheum Dis. 2006;65(suppl II):512.

Overall Cancer Rates in RA PatientsTreated With TNF Antagonists
Cancer in RA not treated with anti-TNFtherapy relative risk of cancer in 66,471 Swedish RA patients, 1998 through 2005
All sites, 3742 1.11 (1.08, 1.16)Respiratory tract, 410 1.35 (1.21, 1.51)
Cancer in the General Population
Cumulative Risk by Age 75
Site %
Any cancer 30
Askling J, et al. Presented at the 2007 European League Against Rheumatism annual meeting;Barcelona, Spain. Abstract OP0013.
Respiratory tract, 410
Upper GI, liver, pancreas, 300
Colorectal, 329
Breast, 534
Ovary, Uterus, Cervix, 227Prostate, Testes, 530
Kidney, Bladder, 253
Skin, melanoma, 115
Central nervous system, 72
Skin, nonmelanoma, 306
Other, 279
0 1 2 3 4
1.35 (1.21, 1.51)
1.12 (0.98, 1.27)
0.75 (0.67, 0.85)
0.94 (0.86, 1.03)
0.83 (0.72, 0.96)1.06 (0.96, 1.16)
1.22 (1.06, 1.41)
1.14 (0.93, 1.40)1.76 (1.54, 2.01)
1.09 (0.84, 1.41)
1.29 (1.12, 1.47)
Any cancer 30
Prostate 14
Female breast 10
Colon-rectum 4
Lung 2.5
Lymphoma 1
Leukemia 0.7

Overall Cancer Rates in RA Patients Treated With TNF Antagonists (cont’d)
N Incident Cancers
Anti-TNF-exposedN = 6297
No anti-TNFN = 66,471
Relative risk
All primaries 217 5404 0.99 (0.85–1.14)
Final primaries 169 3746 0.95 (0.80–1.12)
Second primaries 13 444 1.33 (0.66–2.67)
Respiratory tract 37 587 1.29 (0.91–1.83)
GI, not CRC 10 397 0.72 (0.38–1.39)
Askling J, et al. Presented at the 2007 European League Against Rheumatism annual meeting; Barcelona, Spain. Abstract OP0013.
Colorectal (CRC) 17 505 0.84 (0.51–1.40)
Breast 28 729 0.61 (0.41–0.90)
Uterus/cervix/ovary 18 298 1.22 (0.74–2.03)
Prostate/testis 15 651 0.61 (0.36–1.03)
Kidney/bladder 12 389 0.95 (0.52–1.74)
Melanoma 8 184 0.87 (0.41–1.81)
Nonmelanoma skin 26 613 1.55 (1.02–2.37)
CNS 7 92 1.14 (0.50–2.56)
Other solid sites 15 392 0.93 (0.54–1.60)

Demyelination WithTNF Antagonists in RA
Adalimumab2334 in clinical trials
3 cases of demyelinating diseases
1 case of optic neuritis
1 case of paresthesia with
ETN180,000 in clinical trials, extension, and postmarketing studies
18 cases of demyelinating diseases
14 cases of new
INF170,000 in clinical trials, extension, and postmarketing studies
19 cases of demyelinating diseases
3 relapses of existing MS
FDA Arthritis Advisory Meeting, March 4, 2003. Advisory committee briefing document for safety with Remicade. Available at: http://www.fda.gov/ohrms/dockets/ac/01/briefing/3779b2_03_centecor.pdf. Mohan N, et al. Arthritis Rheum. 2001;44(12):2862-2869.
1 case of paresthesia with abnormal MRI
1 case of lower extremity numbness
2 of 3 cases resolved completely
1 has residual leg numbness
definite/probable MS
4 cases of MS relapse
7 cases of optic neuritis
Other cases including myelitis, paresthesias
4 cases resolved completely,4 lost to follow-up
3 relapses of existing MS
3 cases of new MS
5 optic neuritis
8 other

CASE STUDY and DISCUSSION THREE
RA Progression on Combination Therapy With Anti-TNF Agent + MTX
Supported by an educational grant from Amgen Inc and Wyeth PharmaceuticalsThis educational activity has been facilitated by Gullapalli & Associates, LLC.

52-year-old male on MTX + infliximab for 2.5 years with increasing doses but with slowly more active RA
Presents with increased swelling/tenderness in ankles, feet, hands, wrists
Previous medical history: – Allergic rhinitis treated with nasal CS– Osteopenia treated with alendronate
Progressive RA on MTX + Infliximab
– Osteopenia treated with alendronate
Current meds: MTX 15 mg/week, 8 mg/kg infliximab q 4 weeks, etodolac 400 mg 3 times/day x 2 months
– MTX increased to 25 mg/week in past, but decreased due to severe oral ulcers
– Inadequate response to monotherapy with HCQ; MTX + minocycline + cyclosporine; MTX + leflunomide
Allergies: TMP/SMX (extensive rash on torso and legs)
Knell ME. In: Schumock GT, ed. Pharmacotherapy Self-Assessment Program. 2005:41-88.
.
ARS Question
Which one of the following is the best therapeutic plan at this time?
A. Stop infliximab and MTX; start SSZ + HCQ + adalimumab; continue the same NSAID
B. Change to another NSAID; add low-dose prednisone; continue MTX and continue infliximab
C. Stop infliximab; start etanercept; continue MTX and continue the same NSAID
D. Change to another NSAID; add anakinra; continue MTX and continue infliximab

Appropriate Use of Biologics in RA(ACR Position Statement 2006)
Rheumatologists have a responsibility to provide what they consider to be the safest and most effective treatment option for the patient's illness on individual basis
Etanercept, infliximab, adalimumab, anakinra, rituximab and abatacept are currently FDA approved for the treatment of RA
Financial considerations are not limited to direct medication cost By slowing disease progression, biologics may reduce costly disease-related complications
Third party payers should not attempt to mandate the use of one agent over another based on cost alone
ACR Position Statement on the Use of Biologic Agents for Rheumatic Diseases. Available at: http://www.rheumatology.org/publications/position/biologics.pdf.
Cost-effectiveness of BiologicsACR Position Statement 2006
Rheumatologists have responsibility to select appropriate treatment
Financial considerations are not limited to direct medication cost
By slowing disease progression, biologics may reduce costly disease-related complications disease-related complications – Long-term disability– Joint replacement surgery– Cardiovascular complications
Medication access restrictions may adversely affect patients and outcomes, as all drugs are not bioequivalent
ACR Position Statement on the Use of Biologic Agents for Rheumatic Diseases. Available at: http://www.rheumatology.org/publications/position/biologics.pdf.
Spectrum of Use of BiologicsACR Position Statement 2006
Etanercept, infliximab, adalimumab, anakinra, rituximab, and abatacept are currently FDA approved for the treatment of RA
Many rheumatic diseases may never have FDA approval but are supported by adequate evidence-based data
Third-party payers should not deny payment for treatments for which there is good evidence
Rheumatologists have a responsibility to provide what they consider to be the safest and most effective treatment option for the patient's illness
ACR Position Statement on the Use of Biologic Agents for Rheumatic Diseases.
Available at: http://www.rheumatology.org/publications/position/biologics.pdf.

CASE STUDY and DISCUSSION FOUR
Switching Among Anti-TNF Agents
Supported by an educational grant from Amgen Inc and Wyeth PharmaceuticalsThis educational activity has been facilitated by Gullapalli & Associates, LLC.
Case Study 4Switching Among Anti-TNF Agents
MK is a 45-year-old Asian male with RA for 3 years
He has been treated with MTX + infliximab for the last year, but has had infliximab for the last year, but has had disease progression based on the CDAI and radiographic progression

ARS Question
Is it appropriate to switch to another biologic agent in MK’s case?
A. Yes
B. No B. No

Switching Among Anti-TNF Agents
• In patients who fail TNF-α antagonist therapy with one agent, switching to a second agent may be beneficial
• Before switching, reasons for lack of efficacy should be addressed– Adherence
– Development of antibodies (infliximab and adalimumab)
Buch MH, et al. Arthritis Rheum. 2007;57:448–453; Furst DE, et al. Ann Rheum Dis. 2007; 66:893–899; Hyrich KL, et al. Arthritis Rheum. 2007; 56:13–20; Van der Kooij SM, et al. Curr Opin Rheumatol. 2008;20:287–294.

Workshop 2: Comorbidity
Workshop 2: Comorbidity
Please review the clinical scenario summarized on the next slide
You are encouraged to interact with your colleagues to determine the optimal response to the scenariodetermine the optimal response to the scenario
Flipcharts are provided to capture the findings from each group
Faculty will review and facilitate discussion based on your responses
Case Vignette 2Comorbidity
John, a 55-year-old carpenter with rheumatoid arthritis, presented with 15 tender and 10 swollen joints 5 years ago.
He has been maintained on MTX 15 mg SC weekly and added hydroxychloroquine 200 mg qd 1 year ago.
He mentions that his father and brother both had myocardial infarctions during their 50s.
At present he has no tender or swollen joints.
Skin test for tuberculosis was
He denies morning stiffness and fatigue.
Cardiopulmonary review of systems is negative.
Your patient mentions that he is unable to manage his weight in spite of attempting regular exercise and dieting.
Skin test for tuberculosis was negative last year.
He has smoked 1 pack of cigarettes daily for the past 30 years and drinks 1 or 2 beers nightly.
Other family history and the remainder of the review of systems are unremarkable other than for a 43-inch waist.

ARS Based Group Discussion

Workshop 2: ARS
How confident, if at all, would you feel treating the patient described in the above scenario? (Select ONE answer)
Not at All Confident Very confident
1 2 3 4 5 6

Workshop 2: Group Discussion Point
Based on patient presentation at this visit what blood tests do you order?
a. A chem screen only since patients on methotrexate need to have LFTs and creatinine checked.
b. A chem screen, CBC, and lipid panel in order to b. A chem screen, CBC, and lipid panel in order to monitor MTX on liver, blood counts, and because of his cardiovascular risk factors.
c. A chem screen is not indicated for this patient
d. A lipid panel only to evaluate for dyslipidemia
Workshop 2: Group Discussion Point
His blood pressure is 150/95 mmhg. Your treatment plan includes all of the following except:
– Aspirin 75-325 mg daily
– Smoking cessation
– Statin therapy if LDL-C is elevated– Statin therapy if LDL-C is elevated
– Exercise plan only
Workshop 2: Group Discussion Point
As you initiate treatment of John’s dyslipidemia which of the following is not something you consider regarding future treatment options for RA and to reduce the likelihood of future cardiovascular events?
A. Anti-tumor necrosis factor α therapy may further reduce CVD in addition to methotrexate.
B. NSAIDS and selective COX-2 inhibitors could contribute to cardiovacular risk.
C. The effect of corticosteroids on systemic inflammation needs to be balanced with potential adverse effects on hypertension.
D. RA treatment choices will have no impact on cardiovascular risk.

Appropriate
CASE STUDY and DISCUSSION FIVE
Appropriate Patient-Physician Communication Skills
Focus on rationale, benefits, and risks of biological/TNF antagonist therapies in RA
Supported by an educational grant from Amgen Inc and Wyeth PharmaceuticalsThis educational activity has been facilitated by Gullapalli & Associates, LLC.

Case Study 5Improving Physician-Patient Communication
JD is a 52-year-old female who presents with early RA
Her son is in medical school
She has a printout of treatment She has a printout of treatment options and potential adverse events

ARS Question
How would you approach a discussion of treatment strategies with JD focused on facilitating effective physician-patient communication?
A. Provide complete education about the rationale, benefits, and risks of treatment optionsand risks of treatment options
B. Agree upon a treatment and monitoring plan based on medical evidence, but considering JD’s wishes and concerns
C. Set mutually agreed-upon treatment goals
D. A and B
E. B and C
F. A, B, and C

Patient Perspectives on SharedDecision Making
Patients never on a biologic agent– 41% preferred rheumatologist decision– 61% of men vs 36% of women – 7% preferred a joint decision – 33% preferred making the decision themselves– 33% preferred making the decision themselves
Patients previously treated with biologic agents described the experience of shared decision making as “positive and beneficial”
Chilton F, et al. Musculoskeletal Care. 2008;6:1-14.

Effective Physician-PatientCommunication
Major component in the process of caring for chronic conditions
“Patient-centered care” is associated with greater patient satisfaction and adherence, enhanced understanding of satisfaction and adherence, enhanced understanding of health issues, more commitment to treatment, and:– Is informative
– Provides more explanations
– Shows more sensitivity to the patient’s concerns
– Offers more reassurance and support
Suarez-Almazor ME. Curr Opin Rheumatol. 2004;16:91–95.
Effective Physician-PatientCommunication (cont’d)
Three essential functions of patient-centered care:– Information gathering
– Relationship building
– Patient education
Patients should be fully educated about the rationale, benefits, and risks of biological therapies, and should be included in the decision-making process
Combe B, et al. Ann Rheum Dis. 2007;66:34–45; Suarez-Almazor ME. Curr Opin Rheumatol. 2004;16:91–95.
Effective Communication Costs
Patient barriers1
– Their own discomfort (19%)– Insufficient time (13%)– Physician did not have a viable solution (11%)– Concerns regarding impact on quality of care (9%)
Physician barriers1 Physician barriers1
• Insufficient time (67%) • Belief that they did not have a solution (19%)
Efforts to promote physician-patient discussions about costs should focus on brief, actionable alternatives that physicians can undertake to advocate maximally on their patients’ behalf2
1. Alexander GC, et al. J Gen Intern Med. 2004;19:856-860. 2. Suarez-Almazor ME. Curr Opin Rheumatol. 2004;16:91–95.
Improving Adherence to TNF-αAntagonists
• Retrospective cohort study – 14,932 patients with RA, new use of DMARDs (12
regimens) – Adjusted HRs (95% CI) for discontinuation:
• SSZ = 1.59, 1.47-1.72• IFX alone = 1.37, 1.09-1.73 • IFX alone = 1.37, 1.09-1.73 • Etanercept = 0.82, 0.73-0.92 • MTX + adalimumab = 0.63, 0.48-0.84
• Adherence higher for leflunomide, IFX, etanercept, and adalimumab vs MTX, lower for SSZ and all combinations
Grijalva CG, et al. Med Care. 2007;45(10, suppl 2):S66-S76.
SSZ = sulfasalazine; IFX = infliximab; MTX = methotrexate

Case Study 5Improving the Process of Care
Dr. Smith recently joined a large practice that sees many patients with RA
The practice recently signed a contract that involves pay-for-performance, with that involves pay-for-performance, with reimbursement for many chronic conditions tied to quality
What initial steps can be taken to improve the process and quality of care for patients with RA?
Workshop 3: Severe RA
Workshop 3: Severe RA
Please review the clinical scenario summarized on the next slide
You are encouraged to interact with your colleagues to determine the optimal response to the scenario
Flipcharts are provided to capture the findings from each Flipcharts are provided to capture the findings from each group
Faculty will review and facilitate discussion based on your responses

Workshop 3: Severe RA
KV, a 55-year-old single librarian, presented 30 months ago with 8 weeks of acute, severe RA, manifested by fatigue, pain and swelling bilaterally in the hands, wrists, shoulders, knee joints, and
Tuberculosis skin testing was negative.
Six months of prednisone with shoulders, knee joints, and feet, and morning stiffness despite naproxen 500 mg bid.
She denied fever, skin rash, chest pain, shortness of breath, dysphagia, dry mouth or eyes, headache, abnormal bleeding, or visual changes.
Six months of prednisone with titration of MTX dosing to 15 mg/week SC resulted in minimal improvement in fatigue, pain, and morning stiffness.

Workshop 3: ARS
How confident, if at all, would you feel treating the patient described in the above scenario? (Select ONE answer)
Not at All Confident Very confident
1 2 3 4 5 6

ARS Based Group Discussion

Workshop 3: Group Discussion Point
What is the next therapeutic option you would consider?
A. Increase MTX to 20 mg/wk
B. Increase prednisone from 10 mg/d to 40 mg/d
C. Add leflunomideC. Add leflunomide
D. Initiate an anti-TNF medicine and anakinra

Workshop 3: Group Discussion Point
Because KV has been on prednisone therapy for longer than 3 months your next steps include:
A. Ordering a DEXA scan
B. Discontinuing her prednisone
C. Increasing the dose of prednisoneC. Increasing the dose of prednisone
D. Initiate local glucocorticoid injections into the joints immediately

Workshop 3: Group Discussion Point
KV returns for her next scheduled visit 2 months later. She complains of an increased number of swollen and tender joints. Physical exam confirms the return of significant RA activity despite maximal MTX, prednisone, and naproxen therapy and suggests the prednisone, and naproxen therapy and suggests the need for aggressive treatment with which of the following?
A. Leflunomide
B. Hydroxychloroquine
C.Anti-TNF agent
D.Stop mtx therapy and add another biologic

Workshop 3: Group Discussion Point
True or False. This patient can be prescribed a biologic response modifier without further testing
A. True, because she has had a negative TB test.
B. True because she has already been prescribed MTXMTX
C. False, she needs to have a recent TB skin test
D. False, she needs to have a CXR , recent TB skin test, and hepatitis status confirmed

RA vs Other Inflammatory Arthritides
RA likely if:
– Morning stiffness lasting >30 minutes
– Painful swelling of 3 or more joints
– Involvement of hands (metacarpophalangeal [MCP] joints and feet (metatarsophalangeal [MTP] joints), joints and feet (metatarsophalangeal [MTP] joints), and/or
– Duration of ≥4 weeks
British Columbia Ministry of Health Guidelines: Rheumatoid Arthritis: Diagnosis and Management. Available at: http://www.health.gov.bc.ca/gpac/pdf/ra_guideline_summary.pdf.
Delay in Rheumatologist ConsultationScope of the Problem
10,001 cases coded as incident RA by nonrheumatologists
Only 27.3% saw a rheumatologist in the next 2.5-3.5 years– Median time from initial visit to rheumatologist consultation: 79
days
The strongest predictors of shorter time to consultation: – Female sex– Younger age– Higher socioeconomic class
Feldman DE, et al. Arthritis Rheum. 2007;57(8):1419-1425.
Referral Rules for Suspected RA Patients with joint pains persisting >6-8 weeks should be
referred, especially with:
– Joint swelling– Morning stiffness ≥30 min– MCP/MTP involvement (pain on compression)– Constitutional complaints– Raised inflammatory markers– Raised inflammatory markers– Positive RF
Normal inflammatory markers, negative serology, and normal X-rays are not reasons for delaying referral
All rheumatologists should make it a priority to see patients with suspected IA urgently
De Coster C, et al. Clin Rheumatol. 2008 Jun 17. [Epub ahead of print]; Suresh E. J R Soc Med. 2004;97:421-424.
Multidisciplinary Care in RA Primary care and orthopedic surgery1
– Identify inflammatory arthritis and refer early– Physicians need to think of early inflammatory arthritis as an
emergency Rheumatologists1
– Experts in RA care– Early arthritis centers – Early arthritis centers
Allied health professional roles2
– Clinical nurse specialists– Physical therapists– Occupational therapists– Psychologists
Communication is critical1,2
1. Di Martino SJ, et al. HSS Journal. 2005;1:107-109; 2. Vliet Vlieland TPM, et al. J Rheumatol. 2006;33:1900–1903.

Questions?Thank you!Supported by an educational grant from Amgen Inc and Wyeth Pharmaceuticals
This educational activity has been facilitated by Gullapalli & Associates, LLC.


















