
Alfred - nfpa.org · PDF fileBurton R. Klein, Secretary, NFPA ... (Alternate to J. Riess)...
39
SUPPLEMENTARY Report of the Committee on Health Care Facilities Marvin J. Fischer, Chairman Brookdale Hospital Medical Ctr, NY Burton R. Klein, Secretary, NFPA (Nonvoting) Saul Aronow, Tehnology in Medicine Branton B. Blount, Presbyterian Healthcare Services, NM Rep. American Hospital Association Constance Bobik, B&E Fire Safety Equipment, Inc. J. Armand Burgun, Rogers Burgun Shahine & Deschler Inc. Architects Rep. T/C on Safety to Life Bruce M.'Burnett, FDA/Center for Device & Radiology Heal th Suzanne W. Conner, Children's Hospital Medical Center, OH W. II. L. Dornette, Kensington, MD Leo G. Foxwell, Hartford Insurance Group Rep. American Insurance Assn. Martin Grossman, DHHS/US Public Health Services William T~ Guy, 3r.,'The Elizabeth General Medical Ctr., Na ' Rep. NFPAHealth Care Section Stanley'D. Kahn, Forest Elec. Corp. Rep. Nat'l. Elec. Contractors Assn. Ode Richard Keil, Joint Comm. on Accred. of Health Care Qrganizations James W. Kerr, Winter Park, FL William E. Koffel, Jr., Koffel Associates Inc. W..M. Lampe, Post-Glover,'Inc. Rep. Nat'l. Electrical Mfrs. Assn. Ralph Loeb, Sherlock Smith & Adams Inc. Thomas D. Mattern, UCLANeuropsychiatric Hospital" Rep. Nat'"l. Assn. of Priv. Psych. HoOp. David A. McWhinnie, Jr., Mechanical Dynamics Inc. Ray'3. Nichols, Jr., Univ. of TX Medical Branch Rep. American Society of Anesthesiologists Bryan Parker, Montefiore Hospital & Medical Ctr., NY Jack Riess, KemperGroup Rep. A11iance of American Ins. John P. Swope, George Washington University Medical Ctr., WDC Jack L. Taylor, The United Methodist Homes of N3 Rep. American Assn. of IIomes for Aging 3. Michael Thompson, Gage.-Babcock & Assoc. Inc. Rep. American Health Care Assn. Steven Werner, M&M Protection'Consultants Mayer D.Zimmerman, DHHS/Health Care Finan. Admin. A]ternates Douglas S. Erickson, American Hospital Assn. (Alternate to B. B. Blount) Harlan C. Ihlenfeldt, KemperGroup (Alternate to J. Riess) Joseph E. Johnson, Hilton Head Island, SC (Alternate to J. A. "Burgun) SUBCOMMITTEE ON ANESTHESIA SERVICES Dr. John P. Swope, Chairman George Washington Univ. Med. Ctr, Washington, DC Michael J. Albano, AIG Consultants, Inc. James J. Claffey, McPherson CommunityHealth Center, MI Rep. Americah Assn. of Nurse Anesthetists David O. E11iot, Dept; of Mental Retardation, CT Rep. American Hospital Assn. Martin Grossman, DHHS US Public Health Services, NY Dr. George Babe Hart, Memorial Hosp. Med Ctr of Long Beach, CA Rep. American College of Surgeons W.M. Lampe, Post-Glover Inc.' Rep. Nat'l Elec. Manuf. Assn. Norman Menken, American Analgesia Society i: i M.T. Merrigan, Underwriters Laboratories Inc. Dr. James A. Meyer, Pettis Memorial VA Hospita! CA Rep. Amer. Soc. of Anesthesiology Dr. Ray J. Nichols, Jr., Univ. of TX Medical Branch Rep. American Society of Anesthesiology Gerald M. Olderman, Am Pharmaseal, Rep. Health Indus. Manuf. Assn. Michael"R. $hoys, Wisconsin Hospital Assn. Rep. NFPA Health Care Section Clevis T. Svetik,. Johnson & Higgins Gregory L. Welyczko, Ohmeda Rep. CompressedGas Assn. Alternates Dr. John M. Bruner, Groton, MA (Alternate to R.3. Nichols) William F. Doran, Square D Co. (Alternate to W.M. Campe) Douglas S. Erickson, American Hospital Assn. • (Alternate to D.D. Elliot) Hartley C. Ericson, Puritan-Bennett Corp. (Alternate to G.L. Welyczko) Dr. Paul F.Leonard, Mayo Medical School, MN (Alternate to J.A. Meyer) Dr. S.E. Longo, Dr Salvador E Longo & Assoc., Inc. (Alternate to M.R. Sh6~s) Earl 3. Schlosser, Underwriters Laboratories Inc. (Alternate to M.T. Merrigan) SUBCOMMITTEE ON DISASTER PLANNING James W. Kerr, Ph.D., Chairman Winter Park, FL John H. Brenner, Peninsula General Hospital Medical Center, MD Rep. NFPAHealth Care Section C. Roger Camplin, Camplin, Barrels and Assoc.. Inc. John P. 3arrett, New Paltz Nursing Home, NY Rep. American Health Care Assn. James L. Mauney, Volusia County Department of Fire Service, FL a. Benjamin Roy, Jr., Office of the State Fire Marshal, DE Rep. NFPA Fire Marshal Assn. of No. America Clevis T.Svetlik Johnson & Higgins David'Edwa~d Wacher, Princeton Insurance Co. Alternates Douglas S. Erickson, American Hospital Assn. (Alternate to AHA Rep) Peter J. O'Hagan, Jr., Morristown Memorial Hospital, M3 (Alt'ernate to 3. Brenner) SUBCOMMITTEE ON ELECTRICAL EQUIPMEN T Bryan Parker, Chairman Montefiore Hospital & Medical Center Saul Aronow, Ph.D., Waban, MA Jack Berger, J.B. Thomas Hospital, MA Re . New England Hospital Engl.neers Society Hy A~e Bershad, Cost Control Enterprises, Inc. Rep. American Hospital Assn. Yadln David, Texas Childrens Hospital "" Rep. Institute of Electrical and Electrical Engineers Floyd J. DeVore, General Electric Medical Sys. Group Rep. Health Indus. Manuf. Assn. Alfred M. Dolan, Canadian Medical Engr Consultants Rep. Canadian Standards AssnL Kenneth J.Dragmen, P~ckerCorp. Rep. Nat'l Electrical Manuf. Assn. (Vote Limited to radiographic equip.) Dr. George Babe Hart, Memorial Hosp. Medical Center of • Long Beach, CA. Rep. America 9 College of Suregons Alan Lipschultz, The Medical'Center of Delaware Rep. Assn. for Advancementof Med. Instn 89
-
Upload
truongnhan -
Category
Documents
-
view
220 -
download
3
Transcript of Alfred - nfpa.org · PDF fileBurton R. Klein, Secretary, NFPA ... (Alternate to J. Riess)...

SUPPLEMENTARY
Report of the Committee on Health Care Faci l i t ies
Marvin J. Fischer, Chairman Brookdale Hospital Medical Ctr, NY
Burton R. Klein, Secretary, NFPA (Nonvoting)
Saul Aronow, Tehnology in Medicine Branton B. Blount, Presbyterian Healthcare Services, NM
Rep. American Hospital Association Constance Bobik, B&E Fire Safety Equipment, Inc. J. Armand Burgun, Rogers Burgun Shahine & Deschler Inc.
Architects Rep. T/C on Safety to Life
Bruce M.'Burnett, FDA/Center for Device & Radiology Heal th
Suzanne W. Conner, Children's Hospital Medical Center, OH
W. II. L. Dornette, Kensington, MD Leo G. Foxwell, Hartford Insurance Group
Rep. American Insurance Assn. Martin Grossman, DHHS/US Public Health Services William T~ Guy, 3r.,'The Elizabeth General Medical
Ctr., Na ' Rep. NFPA Health Care Section
Stanley'D. Kahn, Forest Elec. Corp. Rep. Nat ' l . Elec. Contractors Assn.
Ode Richard Keil, Joint Comm. on Accred. of Health Care Qrganizations
James W. Kerr, Winter Park, FL William E. Koffel, Jr. , Koffel Associates Inc. W..M. Lampe, Post-Glover,'Inc.
Rep. Nat ' l . Electrical Mfrs. Assn. Ralph Loeb, Sherlock Smith & Adams Inc. Thomas D. Mattern, UCLA Neuropsychiatric Hospital"
Rep. Nat'"l. Assn. of Priv. Psych. HoOp. David A. McWhinnie, Jr. , Mechanical Dynamics Inc. Ray'3. Nichols, Jr. , Univ. of TX Medical Branch
Rep. American Society of Anesthesiologists Bryan Parker, Montefiore Hospital & Medical Ctr., NY Jack Riess, Kemper Group
Rep. A11iance of American Ins. John P. Swope, George Washington University Medical
Ctr., WDC Jack L. Taylor, The United Methodist Homes of N3
Rep. American Assn. of IIomes for Aging 3. Michael Thompson, Gage.-Babcock & Assoc. Inc.
Rep. American Health Care Assn. Steven Werner, M&M Protection'Consultants Mayer D.Zimmerman, DHHS/Health Care Finan. Admin.
A]ternates
Douglas S. Erickson, American Hospital Assn. (Alternate to B. B. Blount)
Harlan C. Ihlenfeldt, Kemper Group (Alternate to J. Riess)
Joseph E. Johnson, Hilton Head Island, SC (Alternate to J. A. "Burgun)
SUBCOMMITTEE ON ANESTHESIA SERVICES
Dr. John P. Swope, Chairman George Washington Univ. Med. Ctr, Washington, DC
Michael J. Albano, AIG Consultants, Inc. James J. Claffey, McPherson Community Health Center, MI
Rep. Americah Assn. of Nurse Anesthetists David O. E11iot, Dept; of Mental Retardation, CT
Rep. American Hospital Assn. Martin Grossman, DHHS US Public Health Services, NY Dr. George Babe Hart, Memorial Hosp. Med Ctr of Long
Beach, CA Rep. American College of Surgeons
W.M. Lampe, Post-Glover Inc. ' Rep. Nat'l Elec. Manuf. Assn.
Norman Menken, American Analgesia Society
i:
i
M.T. Merrigan, Underwriters Laboratories Inc. Dr. James A. Meyer, Pettis Memorial VA Hospita! CA
Rep. Amer. Soc. of Anesthesiology Dr. Ray J. Nichols, Jr. , Univ. of TX Medical Branch
Rep. American Society of Anesthesiology Gerald M. Olderman, Am Pharmaseal,
Rep. Health Indus. Manuf. Assn. Michael"R. $hoys, Wisconsin Hospital Assn.
Rep. NFPA Health Care Section Clevis T. Svetik,. Johnson & Higgins Gregory L. Welyczko, Ohmeda
Rep. Compressed Gas Assn.
Alternates
Dr. John M. Bruner, Groton, MA (Alternate to R.3. Nichols)
William F. Doran, Square D Co. (Alternate to W.M. Campe)
Douglas S. Erickson, American Hospital Assn. • (Alternate to D. D. E l l io t )
Hartley C. Ericson, Puritan-Bennett Corp. (Alternate to G.L. Welyczko)
Dr. Paul F.Leonard, Mayo Medical School, MN (Alternate to J.A. Meyer)
Dr. S.E. Longo, Dr Salvador E Longo & Assoc., Inc. (Alternate to M.R. Sh6~s)
Earl 3. Schlosser, Underwriters Laboratories Inc. (Alternate to M.T. Merrigan)
SUBCOMMITTEE ON DISASTER PLANNING
James W. Kerr, Ph.D., Chairman Winter Park, FL
John H. Brenner, Peninsula General Hospital Medical Center, MD Rep. NFPA Health Care Section
C. Roger Camplin, Camplin, Barrels and Assoc.. Inc. John P. 3arrett, New Paltz Nursing Home, NY
Rep. American Health Care Assn. James L. Mauney, Volusia County Department of Fire
Service, FL a. Benjamin Roy, Jr. , Office of the State Fire Marshal,
DE Rep. NFPA Fire Marshal Assn. of No. America
Clevis T .Svet l i k Johnson & Higgins David'Edwa~d Wacher, Princeton Insurance Co.
Alternates
Douglas S. Erickson, American Hospital Assn. (Alternate to AHA Rep)
Peter J. O'Hagan, Jr., Morristown Memorial Hospital, M3 (Alt'ernate to 3. Brenner)
SUBCOMMITTEE ON ELECTRICAL EQUIPMEN T
Bryan Parker, Chairman Montefiore Hospital & Medical Center
Saul Aronow, Ph.D., Waban, MA Jack Berger, J.B. Thomas Hospital, MA
Re . New England Hospital Engl.neers Society Hy A~e Bershad, Cost Control Enterprises, Inc.
Rep. American Hospital Assn. Yadln David, Texas Childrens Hospital ""
Rep. Inst i tute of Electrical and Electrical Engineers Floyd J. DeVore, General Electric Medical Sys. Group
Rep. Health Indus. Manuf. Assn. Alfred M. Dolan, Canadian Medical Engr Consultants
Rep. Canadian Standards AssnL Kenneth J.Dragmen, P~ckerCorp.
Rep. Nat'l Electrical Manuf. Assn. (Vote Limited to radiographic equip.)
Dr. George Babe Hart, Memorial Hosp. Medical Center of • Long Beach, CA. Rep. America 9 College of Suregons
Alan Lipschultz, The Medical'Center of Delaware Rep. Assn. for Advancement of Med. Instn
89

Alfred 3. Longhitano, Gage-Babcock & Assoc., Inc. Rep. American Health Care Assn.
M.T. Merrigan, Underwriters Laboratories Inc. Dr. James A. Meyer, Pettis Memorial VA Hospital, CA
Rep. American Society of Anesthesiology Richard W. Nalbert, Square D Co.
Rep. Nat'l Electrical Manuf. Assn. (Vote Limited other than radiographic equip.)
Lawrence S. Sandler, VA Central Office
Alternates
Douglas S. Erickson, American Hospital Assn. (Alternate to H,A. Bershad)
Dr. Paul F. Leonard, Mayo Medical School, MN (Alternate to J.A. Meyer)
Robert D. Miller, Hospital Systems Inc. (Alternate to R.W. Nalbert)
SUBCOMMITTEE ON ELECTRICAL SYSTEMS
Ralph Loeb, Chairman Sherlock Smith & Adams Inc.
James L. Crawford, U.S. Dept. of Health & Human Service Dr. George Babe Hart, Memorial Hospital Medical Center
of Long Beach, CA Rep. American College of Surgeons
Lawrence F. Hogrebe, Automatic Switch Co. Eugene A. Lakos, The Methodist Hospital, NY
Rep. Greater New York Hospital Assn. Edward A. Lobnitz, Tilden Lobnitz & Cooper, Inc. Alfred J. Longhitano, Gage-Babcock & Assoc., Inc.
Rep. American Health Care Assn. M.T. Merrigan, Underwriters Laboratories Inc Dr. James A. Meyer, Pettis Memorial VA Hospital, CA
Rep. American Society of Anesthesiology Richard W. Nalbert, Square D Co.
Rep. Nat'l Electrical Manufac. Assn. Hugh O. Nash, Jr., Smith Seckman Reid, Inc.
Rep. Institute of Electric and Electrical Engineers Thomas J. O'Dea, University of MN Hospital & Clinic Donald E. Orner, M-E Engineers, Inc. John M. Owen, Owen & Mayes, Inc.
Rep. Nat'l Society of Professional Engineers Paul 3. Savoie, General Electric Co. Frank 3. Schmid, U.S. Army Corp. of Engineers Georg Stromme, Roseville, MN
Rep. Onan Corp. David L. Vosloh, Naval Medical Command Herbert V. Whittall, Caterpillar, Inc.
Rep. Engine Gen. Sys. Assn. Frank Young, Presbyterian Hospital, MN
Rep. American Hospital Assn.
Alternates
Douglas S. Erickson, American Hospital Assn. (Alternate to F.D. Young)
[)avid K. Norton, VA Office of Facil i t ies (Alternate to VA Rep.)
SUBCOMMITTEE ON GAS EQUIPMENT
Dr. Ray J. Nichols, Jr., Chairman University of Texas Medical Branch
Rep. American Society of Anesthesiology
M. Lee Bancroft, Beth Israel Hospital, MA Rep. Harvard Medical School
Gary Fowler, Jefferson Reg Medical Center, AR Rep. American Hospital Assn.
Leo G. Foxwell, Hartford Insurance Group Rep. NFPA T/C Indust. & Med. Gases
Dr. George Babe Hart, Memorial Hospital Medical Center of Long Beach, CA Rep. American College of Surgeons
Alan Lipschultz, The Medical Center of Delaware Rep. Assn. for Adv. of Med. Instn.
Dr. T.K. Raman, Baystate Medical Center, MA Rep. American College of Chief Physicians
Earl a. Schlosser, Underwriters Laboratories Inc. Joseph G. Weiss, St. Luke's/Roosevelt Hospital, NY
Rep. Greater New York Hospital Assn.
Alternate
Douglas S. Erickson, American Hospital Assn. (Alternate to G. Fowler)
Michael A. Kargyl, Underwriters Laboratories (Alternate to E.J. Schlosser)
Nonvoting
Delila A. Hughes, American Assoc. of Nurse Anesthetists
SUBCOMMITTEE ON USE OF HIGH FREQUENCY ELECTRICITY
Saul Aronow, Ph.D., Chairman Technology in Medicine
Dr. John M. Bruner, Groton, MA Rep. American Society of Anesthesiology
Dr. George Babe Hart, Memorial Hospital Medical Center of Long Beach, CA Rep. American College of Surgeons
Dr. Paul F. Leonard, Mayo Medical School. MN John W. Martin, Ph.D., Cameron-Miller, Inc. M.T. Merrigan, Underwriters Laboratories Inc. Kenneth I. Tobacman, Grant Hospital of Chicago, IL
Rep. American Hospital Assn. Joseph G. Weiss, St. Luke's/Roosevelt Hospital Center,
NY Rep. Greater New York Hospital Assn.
Alternate
Gerard Bashein, University of Washington (Alternate to J.M. Bruner)
Douglas S. Erickson, American Hospital Assn. (Alternate to K. Tobacman)
SUBCOMMITTEE ON HYPERBARIC AND HYPOBARIC FACILITIES
Dr. W.H.L. Dornette, Chairman Kensington, MD
James H. Chappee, Boeing Aerospace Operations Frederick S. Cramer, Oxygen Research Foundation Michael Gerken, Baptist Memorial Hospital
Rep. American Hospital Assn. G.T. Greak, Keyes Offshore, Inc. W.T. Gurnee, Hyperbaric Oxygen Terapy Systems Inc. Dr. George Babe Hart, Memorial Hospital Medical Center
of Long Beach, CA Rep. American College of Surgeons
John Howard Kimzey, Eagle Engineering Clark H. Long, Presbyterian University Hospital, PA M.T. Merrigan, Underwriters Laboratories Inc. Dr. James A. Meyer, Pettis Memorial VA Hospital, CA
Rep. American Society of Anesthesiology Stephen D. Reimers, Reimers Engineering Inc. J. Ronald Sechrist, Sechrist Industries Paul J. Sheffield Ph.D. Office of Surgeon General, USAF
Rep. USAF/Off of Surg General Clevis T. Svetlik, Johnson & Higgins of Ohio, Inc.
Rep. NFPA Health Care Section Joseph G. Weiss, St. Luke's/Roosevelt Hospital Center
Rep. Greater New York Hospital Assn. Wilber T. Workman, U.S. Air Force School of Aerospace
Medicine
Alternates
Douglas S. Erickson, American Hospital Assn. (Alternate to M.A. Gerken)
Earl J. Schlosser, Underwriters Laboratories Inc. (Alternate to M.T. Merrigan)
90

SUBCOMMITTEE ON LABDRATORIES
Suzanne W. Conner, Chairman Childrens Hospital Medical Center, OH
Dr. Spencer Burney, Wellesley, MA Rep. American Society of Clinical Pathologists
C. Roger Camplin, Camplin, Bartels and Assoc., Inc. George D. Harlow, Tufts New England Medical Center, MA
Rep. American Hospital Assn. Dr. Gerald A. Hoeltge, Cleveland Clinic Foundation, OH
Rep. College of American Pathologists Clifford Houser, Joint Committee on Accred. of Health
Care Organizations Robert F. Hughes, Earl Walls Assoc. Harlan C. Ihlenfeldt, Kemper Group
Rep. Alliance of American Insurance M. Carlisle McGarity, WMP Architects, Inc. Kay N. Olson, University of Minnesota Hospital
Rep. American Society of Medical Technology Will ie L. Ruff Ph.D., Howard University Hospital,
Washington, D.C. Rep. American Assn. of C1in. Chem.
Earl 3. Schlosser, Underwriters Laboratories Inc. Norman V. Steere, Norman V. Steere Assoc.
Rep. T/C Chemistry Labs James O. Wear, Veterans Administration Medical Center
Rep. NFPA Health Care Section
Alternates
Douglas S. Erickson, American Hospital Assn. (Alternate to G.D. Harlow)
Arden W. Forrey, University of Washington (Alternate to W. L. Ruff)
M.T. Merrigan, Underwriters Laboratories Inc. (Alternate to E J Schlosser)
SUBCOMMITTEE ON NONFLAMMABLE MEDICAL PIPED GAS SYSTEMS
Leo G. Foxwell, Chairman Hartford Insurance Group
Rep. American' Insurance Assn.
Mark Allen, Ohmeda Medical Eng. Rep. Compressed Gas Assn.)
M. Lee Bancroft, Beth Israel Hospital, MA Rep. Harvard Medical School)
Elizabeth M. Bunn, Dept. of Veterans Affairs Craig B. Doerksen, Doerksen Medical Gas Systems/US Ltd. Danielle S. Earhart, U.S. Depart. of Health & Human
Services, WA Peter Esherick, Patient Instrumentation Corp. Salvatore J. Farruggia, Syska & Hennessy, Inc.
Rep. American Society of Sanitary Engineers Lee W. Gibbs, Underwriters Laboratories Inc. Meryl W. Holmwood, L i t t e l l s Oxygen, [nc. Wayne C. Karcher, Al l ied Healthcare Products, Inc. Antonio A. Mesa, Nash Engineering Co. Dr. James A. Meyer, Pettis Memorial VA Hospital, CA
Rep. American Society of Anesthesiology David B. Mohile, Medical Engineering Services, Inc. Reginald Nease, Medical Gas Services, Inc. J. Richard Wagner, Poole & Kent Co.
Rep. Mechanical Contractors Assn. of America F. David Wyrick, Sr., Cambiare Marketing
Rep. I n t ' l Analgesia Society
Alternates
Kyle Adriance, Puritan-Bennett Corp. (Alternate to M. Allen)
Douglas S. Erickson, American Hospital Assn. (Alternate to AHA Rep)
David Eric Lees, New York Medical College (Alternate to J. Meyer)
Michael 3.'Pastore, Nash Engineering Co. (Alternate to A.A. Mesa)
SUBCOMMITTEE ON VACUUM SYSTEMS AND EQU~IPMENT
David A. McWhinnie, Jr. , Chairman = Hickory Hi l ls , IL
Mark Allen, Ohmeda Medical Eng. Rep. Compressed Gas Assn.
M. Lee Bancroft, Beth Israel Hospital Rep. Harvard Medical School
David L. Br i t ta ln, Busch, Inc. Clyde M. Douglass, St. Marys Hospital of Rochester, MN
Rep. NFPA Health Care Section Dr. George Babe'Hart, Memorial Hospital Medical Center
of Long Beach, CA Rep. AmericanlCollege of Surgeons
Henry R. Kaht, Squlre-Cogswell Co. Wayne C. Karcher, Al l ied Healthcare Products, Inc. Antonio A. Mesa, Nash Engineering Co. R.J. Rei l ly, Jaros Baum & Bolles
Rep. American. Society of Plumbing Engineers
Alternates I'
Kyle Adriance, Puritan-Bennett Corp. (Alternate to M. Allen)
Douglas S. Erickson, American Hospital Assn. (Alternate to American Society of Anesthesiologists Rep)
Dr. Ray J. Nichols, Jr. , Univ. of Texas Medical Branch (Alternate to American Society of Anesthesiologists Rep)
Michael J. Pastore, Nash Engineering Co. (Alternate to A. A. Mesa)
Technical Committee on Industrial and Medical Gases ,
(Concurrent bal lot ing on Gas Systems requirements)
i I
F~ed K. Kitson, Chairman F. K~ Kitson Safety Associates
Theodore Lemoff, Secretary National Fire Protection Association
(Nonvoting)
Francis X. Bender~; Safety Engineering Consultants Carl A. Caves, US,Dept. of Energy = Lee W. Gibbs, Underwriters Laboratories Inc. Charles B. Henrici, Elk Grove Village Fire Dept. IL
Rep. Int l Assn. of Fire Chiefs Edward J. Kilper, Monsanto Co.
Rep. Chemical Manufacturers Assn. Douglas F. Nelson Industrial Risk Insurers David Simon, Liquid Air Corp.
Rep. Compressed Gas Assn./Safety and Health Lionel WoIpert, Ai;rco Industrial Gases Div.
Rep. Compressed Gas Assn./Transportation
Alternates
John M. Cece, US Dept. of Energy (Alternate to C.'A. Caves)
Tommy E. England, Industrial Risk Insurers (Alternate to D. F. Nelson)
Nonvotinb
L. G. Matthews, Las Cruces, NM (Member Emeritus)
Staff Liaison: Burton R. Klein
The Supplementary Report o f the Committee on Health Care F a c i l i t i e s is presented f o r adopt ion.
This Supplementary Report was prepared by the Technical Committee on Heal th Care F a c i l i t l e s and proposes f o r adopt ion a Supplementary Report which documents i t s ac t ion on the pub l i c comments received on
91
i'

the proposed revision to NFPA 99-1987, Standard on Health Care Faci l i t ies, published in the Technical Committee Reports for the 1989 Fall Meeting:
This Supplementary Report has been submitted to le t ter ballot of the Technical Committee on Health Care Faci l i t ies which consists of 27 voting members; of whom at least 2/3 voted affirmatively on each of the Committee proposed actions on the 76 public comments as calculated in accordance with NFPA "Regulations Governing Committee Projects;" I ballot was not returned (Mr. Taylor). Members who voted negatively or abstained on specific comments and their reasons follow:
Comment 99-I (Negative) Mr. McWhlnnie: Recompresslon (in the t ransf i l l ing
context) is not the same as what most users understand as compressed gas/compression. When the primary gas source is above I arm, i t is "compression" (compressed already). The adiabatic heat of "recompression" (in a closed circuit) - - is different, and is a real hazard that has resulted in tragedy. This is a greater hazard than those of the wrong cylinder, or mixing the wrong gases (under present codes/standards).
Most users think they are only releasing a "compressed" gas l ike every time a t i re is f i l led , and don't know of, or even understand, that the act is "recompressing" (what was an i n i t i a l l y compressed gas) can be very hazardous. Explosions, ruptured regulators/gauges, connecting tubing, receiving containers - have caused fires - and injuries and deaths have resulted.
This issue was a major factor over the many years of d i f f icu l ty in NFPA with the matter of t ransf i l l ing.
Comment 99-2 (Negative) Dr. Aronow: The definit ion of "Line Isolation
Monitor" in the NEC (and in Proposal 99-26) is not correct, neither technically nor in function. A LIM may or may not check the impedance from each llne to ground, but whether i t does or does not is immaterial to i ts function. What i t does is predict the Total Hazard Current. Mow i t does this is up to the designer.
Also the fact that i t may include a test circuit is a performance requirement that does not belong in a definition.
The definit ion in the NEC dates back many, many years when a quite primitive technology was in use. As the problem became better understood, NFPA 99 revised the definition to i ts present form. Unfortunately for many years no one noticed the discrepancy between the two documents. I t seems rather s i l l y now to discard a correct definit ion in favor of an obsolete one, particularly when Section 517 may be deleted from the NEC and correlation would not be a question.
Comment 99-12 (Negative) Mr. Lampe: As was concluded by the Subcommittee on
Electrical Systems, in readily evident wet locations, Exception No. 2 would not provide a safe environment for patients or staff.
Comment 99-14 (Negative) Dr. Aronow: I do not concur with the Committee
Action on this comment and i ts related proposal. In both cases I think the proposer and commenter present valid arguments about a significant problem. There is no magic about an emergency system that makes its ~ less l iable to failure than the normal system circuitry. I f anything i t is more subject to overload or failure because i t is inherently limited in capacity and includes the transfer mechanisms.
I t seems to me that ~ some normal system outlets in an anesthetizing location does not create any hazard, does not impose any great economic burden, but does provide some improvement in continuity of power. For these reasons the comment should be accepted.
Comment 99-17 (Negative) Mr. McWhinnie: [In May, 1986, the Vacuum
Subcommlttee voted heavily for this (99-17) proposal and 99-18, 99-19 and 99-20.]
[In May, 1989, the Vacuum Subcommittee again voted heavily (only one negative ballot) for this 99-I? proposal, as well as 9g-18, 99-19 and 99-20.]
Answers to specific issues on Comments 99-17, 18, 19 and 20 have been held in abeyance by the Standards Council and the Board, and as suggested by NFPA Associate General Counsel "due to the (this) revision cycl e."
The Technical Committee actions on Comments 99-17 through 99-20 do violate NFPA Regulations lO-lO(c), 10-11 and [by reference from lO-lO(c)] also I I- I0, all of which are clear, the framers' intent obvious and in the opinion of the Standards Council Secretary "are interpreted l i t e r a l l y . " Other applicable Regulations are l isted under "B" below.
The Technical Committee actions on these four comments are also contradictory to the let ter, and obvious intent, of Standards Council actions 87-46(b), 88-2 and 88-38, among others.
Neither the Technical Committee nor i ts member proponent of combining disparate technologies have responded to the repeatedly asked questions (required by NFPA Regulations) as to "problem", "purpose", "substantiation" - including when asked by the NFPA Fall Meeting Chairman, Denver, November, 1986 (transcript p~. 40 line 2, and pg. 38 line 11). When the same cruclal questions were asked by an involved professional (re separate chapters) at the Technical Committee ad hoc meeting May I I , 1987 the answer was that separate chapters were "possible".
The Technical Committee Chairman assured Mr. Osborne, and the Association, of "stand alone chapters" (underscore added) in 1986 TCR, Log 7. See item "( I ) " under "B" below.
In reference to the two opening "NOTES" above (Vacuum Subcommittee voting) the June 19/20, 1989 Technical Committee meeting was opened with the Chairman's "reminder" (stated repeatedly throughout this project in committees and in writing) that ". • . the Subcommittees are s t i l l the experts for the Committee."
Comments on Committee Statement for Comment 99-17: I. This statement is based upon the 5-11-87 action
of the Technical Committee review ad hoc which did E~ "review," or even address (nor did the Technical Committee) the many technical objections based upon technical changes detailed in the July, 1986 "Perspective/Scenario" (over two dozen listed in "B" below). Nor did either body discuss the universally accepted meaning, and formal definition/intent/meaning of "text" and "technical" which have been made a part of this issue, and, therefore, are in the Subcommittees, Technical Committee and Standards Council f i les. Below, and a part of this negative ballot on the Technical Committee actions 99-17, 18, 19 and 20 is a photo copy of that submittal (Malek, Malcom, Random House, Oxford English Language) at the end of this Section [copy available from NFPA Headquarters].
Having neither discussed these hinge terms within committees, nor rejecting the authoritative sources (Malek et al), and not responding to repeated requests for comment this substantiation is accurate, pertinent and essential to the desision process.
No intel l igent conclusion can result from deliberations on a v i ta l issue without clear definit ion of terms -- and especially unspoken ones.
However, the Technical Committee and i ts ad hoc have, in fact, accepted these definitions, and also the fundamental differences betwen these two dist inct ly diverse technologies - "different technologies", "different requirements", "different hazards" (Technical Committee quotes in the record, including the NFPA Fall Meeting transcript of November, 1986.)
This Technical Committee statement (99-17,1.) indicates (as do the 5/11/87 ad hoc minutes) no "review" or "further study" promised to, and r ightful ly expected by, the "affected" [Reg. 11-9(c)] committees and the entire Association. The promised "review" and "further study" requires compliance with Regs. 10-3, I0-I0(c), 10-11, 11-9(b) ( i f a document "is affected") and 11-9(e) especially. The only "considerable research" was done by the Vacuum Subcommittee which, twice, voted heavily against this Technical Committee action - - See "NFPA Regulations, Part Vl, contravened" in "B" below.
The "review" and " fu l l study" on 5-11-87 met for two hours, and i ts total result was the addition of a one word quali f ier.
92

2. The only "s im i la r i t y , " as stated in the record by an involved professional designer, is that they are in the same building. "The fundamentals of construction" (Technical Committee) are t o ta l l y di f ferent for "design, censtructien . . . testing . . ." (NFPA 99, I-3), use dif ferent materials, di f ferent materials' preparation, di f ferent insta l lat ion methods, di f ferent source equipment/components/accessories, dif ferent valving, di f ferent alarm requirements, di f ferent "operating" dynamics, widely di f ferent hazards, di f ferent required insta l la t ion tests, di f ferent sizing c r i te r ia , di f ferent terminal performance requirements (none are required for gases)," and dif ferent mediums - - a system for definable elements, commodities, combustion supporting preperties, or mixtures ef such - - at a (nominally) constant 3.5 atmospheres posit ive pressure can, by no logic, be equated with one for "a condition of an undefinable f lu id" at subatmospheric pressures which, by design, are constantly changing over broad ranges.
This statement is inconsistant with the Technical Committees often stated acknowledgement ef basic/fundamental differences (cited in Technical Committee Statement I above).
This Technical Committee action does not help, but handicaps, the systems designers and instal lers - especially "those less famil iar" (stated by a Subcommittee member early in this process). Very many (seme say most) designers and insta l lers have done no such project before, or only l or 2. The AIA discontinued i ts section on Health Care Fac i l i t ies design• The record (NFPAs) shows that a gas or vacuum system is sometimes and instal led singly. Many designers do vacuum systems separate from gas systems - par t icu lar ly in preliminary plans, schematics, r iser diagrams, and often by di f ferent designers - before f inal plans, in preliminary planning, schematics, r iser diagrams, etc., and often by di f ferent designers - - before f inal plans (can be documented).
Vacuum systems designers and instal lers (par t icu lar ly those less informed) who read NFPA 99 contents wi l l miss ent i re ly essential text for MSVS which is completely separated from i ts proper location by 20 pages and over 300 paragraphs of material which pertains only to gases. This would be to ta l l y corrected by acceptance of 99-17, 18 and 19 which the Vacuum Subcommittee voted heavily for (only one negative vote) and which the Technical Committee rejected without the required technical reason•
3. Contrary to this statement the references are absolutely and undeniably appropriate.
As former Vice Chairman of the Medical Equipment Division of CGA and Chairman of the f i r s t edit ion of the f i r s t nationally recognized consensus document on Medical Surgical Vacuum Systems (MSVS) I can assure anyone interested that the CGA Board approved that separate vacuum document, not only because of i ts great need, but because A/Es were not following industry pamphlets and guidelines but, rather, were designing MSVS per, and requiring complianc,~ with, NFPA 565, and subsequently 56F. Knowledgeable and prudent professionals who were involved knew that this practice resulted in poor design, excessive cost, inappropriate materials and components, dangerously ineffective performance, especially in c r i t i ca l care areas - - and fer the HCFs myriads of problems in emergencies and maintenance. These i l l advised practices persist (see following paragraph), and have been exacerbated by the combining of these opposites ( i n t h l s context) in the same chapter-category - - which sends the wrong message to "those less fami l iar . " I t is precisely fer these reasons that NFPA (instigated and proposed by CGA) authorized the 56K project, and also why the NFPA Standards Council took and/or app'reved the steps in items "(a)" through "(e)" in "B" below.
During the era of this issue of combining disparate technelegies, without "a statement of the problem and substantiation for proposal . . ." [Reg. I0- I0(c) ] , the Technical Committee and the "affected" [Reg. I I -9(b) ] Subcommittees have been provided ~vith several (of many known) actual, and current (since 99'84), project(s) specifications which improperly combine these epposite systems, mandating by project Contract Documents the same requirements for gases and vacuum systems - - and, yes, usually by "those less fami l iar . " The Technical
Committee chairman and the Vacuum Subcommittee "survey" ad hoc chairman have copies of another such project specification which is less than one year old. These examples are exactly what NFPA 56K and 99-1984, Chapter 6 were intended to prevent, and why the Technical Committee assured Mr. Osborne, and the Association, of "stBnd aIQne chaeters" (underscore added), 1986 TCR, Log 7 [ " (e)" under "B" below].
4. This Technical Committee statement overlooks "those . . . involved in the design, construction, inspection (cer t i f icat ion) . . .". [99'87, I-3] of these l i fe-support systems who are al l too often "less fami l iar . " These are most frequently the ones involved in Code deviations and, regretably, in patient inquiry/death incidents (based upon long l i t i ga t i on exper ience).
These professions and trades need the "clearly deliniated" dist inct ions f i r s t - - l i t e r a l l y and f igurat ive ly - - any mistakes of those "less famil iar" are most often uncovered after the fact.
This statement acknowledges that these are two types ("beth"), and that "differences exist" between them, and acknowledges what has been the essence ef the issue - - that they should be "clearly del iniated." They could be more "clear ly del iniated" and were, have been, and should s t i l l be. The clearest possible dist inct ion ha~ existed, most successfully, by ~ the separation unt i l twe opposites were combined under one heading because of a feeling (the proposer " fe l t " • . .), which has actually clouded the dist inct ion that existed in NFPA 99'84, Ch. 6. "Combining" diverse concepts in or under one heading can lead to "combining in the mind" - (Webster's NWD and others)• I t seems inconceivable that a matter of this magnitude ceuld have progressed to thfs point without addressing the questions of problem, purpose, substantiation (rat ionale).
"Operation and maintenance" of these "di f ferent technologies" (Technical Committee quote) are net the same, and they are routine factors, but only after the fact of design,: construction, cer t i f icat ion. The document is almost ent i re ly for these phases and the utmest clarity1~in these phases for those prefessiens and trades (which are "less famil iar" than Healti~ Care Fac i l i t ies professionals) can only enhance the safety, operation, and maintenance of these v i ta l systems.
For just some operation and maintenance~differences consider posit ive vs. negative pressure systems' leak detection, terminal valve differences, terminal performance differences (not required for gases), the differences between bulk/ l iquid gases, high pressure gases, a i r qual i ty, oxidizer hazards, etc. and vacuum pumps and accessories•
5. This Technical Committee Statement is covered in I. above. I t does not address any ef the technical substantiations of the proposal, or the 28+ changes of text under "Examples - part ia l l i s t " under substantiations l is ted in Proposals. F
The Technical Committee ad hoc meeting (5-11-87), from which this Technical Committee Statement emanated, did not perform the Technical Committee responsibi l i ty of the promised "review" and " fu l l study" (Fall Meeting, November, '86).
I t simply added a single word modifier. That action among others, simply circumvented the promised "stand alone chapters" (1986 TCR, Log 7).
6. The Technical Committee posit ive statement that NFPA Regulations "have not been violated" doesn't make i t se. The Regulations cited herein are clear in their language and obvious intent. Nowhere in NFPA Regulations is' there a proviso for the arbi trary insertion of an unspoken qual i f ier .
Per the Standards Council Secretary's opinion certain of the cited Regulations are (have been) "interpreted l i ' t e ra l l y . " As the framers ef the Regulations have so interpreted at least three cited herein, those have been violated.
I f any qua l i f ie r to broaden er l im i t a Regulation is intended or permitted (a change in the l i t e ra l meaning) i t would have been announced in advance, including effective date, and inserted in the last (1989) Technical Committee Directory.
The reference to " text" ignores Malek et al. [copy is available from NFPA Headquarters].
7. The Technical Committee Statement is accurate as to 56A and 56G, and is reasonable as both are in the exact same technology, and both t i t l e s are "Inhalation Anesthetics."
93
The same is true of 76A and 76B which are both are in the same technology - - "E lec t r ica l " / "E lec t r lc l ty . "
This example is immaterial and irrelevant. Would the combining of 56A and 76A be reasonable? or even permitted? By no logic can these actions be compared with the fundamental, basic differences between IO (or more) specific gases - - and a subatmospheric condition of a f lu id.
This Statement, as in other Technical Committee Statements, mentions "text" - - and, as in those others, disregards " text , " the universal and authorative meaning of which has been accepted by the Technical Committee (Supporting material available for review at NFPA Headquarters.)
The Technical Committee has provided proof of the va l id i ty these four comments by i ts removal of "vacuum" from 99, Chapter 4, Note 2.
8. This Technical Committee Statement is accurate, obvious, and perfectly i l lus t ra tes just one of the many problems. See last paragraph of "2." above.
This is glaringly inconsistent with the Technical Committee June 19, 1989 opening statement as to the Subcommittees being "the experts for the (T/C) Committee."
This specific point was proposed in 1986 and now in Comment 99-18. The Vacuum Subcommittee has voted twice for this proposal, this second time with only one negative bal lot .
9. This contradicts the Technical Committee opening statement on 6-19-89; and is inconsistent with Malek et al (supporting material available for review at NFPA Headquarters) with which the Technical Committee has concurred.
This Technical Committee statement also triggers some very cr i t ica l points, questions or doubts; concern about which is not unreasonable:
(a) Considering that the Technical Committee has not responded to questions asked re " text" and "technical", and has thereby accepted the only authoratlve def in i t ion in the record, this Technical Committee Statement can only be in error.
(b) How does this Technical Committee Statement correlate with the Technical Committee Chairman's opening statement 6-19-89?
(c) Is a Technical Committee bal lot that states the Technical Committee "should not be influenced" by two heavily aff irmative Subcommittee ballots (3 years apart) an NFPA Regulation or o f f i c i a l policy?
(d) Are these Technical Committee Statements (99-17, 9) and "c" ( last above) not an abuse of the most widely spoken language in the world - - which is NFPAs most important tool? (e) Do these Technical Committee Statements
discount al l Subcommittee ballots, and recommendations? Or just selected ones? Which ones? ( f ) As the issues of "text" and "technical" have
been in the record for three years, and authoritat ive sources are also of record, and have been made the hinge point of extremely important issues why haven't they been addressed? Will they be? When?
(g) Shouldn't the technical responsibi l i t ies of the Subcommittees be more clearly delineated? (h) I f there is a d i f ferent def in i t ion, or a
qua l i f ie r on the presently accepted one(s), what are they? When do they become effective? 10. With respect, this Technical Committee
Statement contradicts the record. I t overlooks, no doubt inadvertently, the information, on record and in f i l e , and referenced in the second and third paragraphs of "3." above (examples provided to the Technical Committee and the affected Subcommittees, and another to the Technical Committee Chairman, and the Chairman of the Vacuum Subcommittee "survey" ad hoc). I t also overlooks the review report of Project 746A which is in the f i l es of the Subcommittees and the Technical Committee.
11. Examples of deletions include 6-5 and 6-5.3 which were removed ent i re ly from 99'87. Numerous deletions of text from their proper location, and changes of intent are l is ted under "Examples - part ial l i s t " and "The following additional changes . . ." [both are detailed in Substantiation of Proposals].
12. This Technlcal Committee Statement ( inc lud ing i t s parenthet ica l second paragraph) is simply a l i s t i n g of meetings and, there fore , redundant. I t is i r r e l e v a n t as i t is t o t a l l y s i l e n t on the numerous technical subs tan t ia t ions in the parent proposals and subsequent comments. I t s claims of "ser ious cons iderat ion" and "ex tens i ve l y discussed" are open to conjecture and beg subs tan t ia t ion , as no where in the records, minutes, or in the memory of th i s commentator, is there i nd i ca t i on that the fo l low lng cruc ia l issues have been discussed:
(a) The "problem" [10-10(c) ] wi th Chapter 6 of 99'84, "purpose" (form fo r proposals) and " subs tan t i a t i on " fo r combining two d isparate technologies in to the same chapter.
( a ) l . "Deta i led . . . statement p re ferab ly technlcal . . . to convey the Committee's ra t lona le
. . . to the Associat ion (Reg. 11-10). (b) Object ions to the Technical Committees
f a i l u r e to adhere to i t s mandate to incorporate documents into 99 "as is" and "without change." (b)l. Failure to adhere to the Technical
Committees promise to the Subcommittees, and to the entire Association, to maintain separate "stand alone chapters" (or even to explain that failure). The then existing separate documents had been eminently successful for years without any complaint. (c) The arbitrary use of an unstated (in the
Regulations) qualifier to rationalizes Technical Committee action. (d) Consensus on terms crucial to the project
(Malek at al). (e) Perspective/scenarlo, July '86, illustrating
the damaging effect of combining opposite (in this context) technologies/concepts in the same chapter. (f) "Research data" and "engineering
fundamentals." The vacuum Subcommittee did the only fundamental (lab) engineering studies, and lab and field research. (g) Separation of connected text by 20 pages and
300+ paragraphs of text for an entirely different technology/concept.
(h) Many a l t e r a t i o n s of t ex t (28 l i s t e d in Proposal) "a f fec ted" t e x t , "would change t e x t , " or "o ther a f fected parts of the document."
( i ) Wording: Delet ions, add i t ions , rev is ions "added, rev ised, how revised, de le ted . " NWD "choice and arrangement." The Vacuum Subcommittee voted heav i l y fo r these
same proposals in May, 1986. The Vacuum Subcommittee has voted, again heav i l y (wi th only one negat ive vote) , fo r the parent proposals of Comments 19-17, 18, 19 and 20, and recommended that the Technical Committee accept Proposals 99-103, and 104.
Hr. Parker: [Changed vote and concurred with Mr. McWhlnnle on c l r c u l a t l o n of negat ive ba l l o t s g iv ing the fo l low ing reasons.] The Technlcal Committee should not over r ide the Vacuum Subcommittees almost unanimous vote. What is the po in t of technical subcommittees i f they are to be t reated in cava l i e r manner? The essentially edi tor ia l decision to merge 56F and 56K into one chapter was a technical error from the start. I t is time for the Technical Committee to admit i ts error and put things right. No great e f fo r t is required. The Subcommittee has done the work; i t merely has to be adopted.
Comment 99-18 (Negative) Mr. McWhinnie: Same reasons as given for Comment
99-17.
Hr. Parker: Changed vote and concurred with Mr. McWhlnnie on circulation of negative ballots.
Comment 99-I~ (Negative) Mr. McWhinnle: Same reasons as given for Comment
99-17.
Mr. Parker: Changed vote and concurred with Mr. McWhlnnle on circulation of negative ballots.
Comment 99-20 (Negative) Mr. McWhinnie: Same reasons as given for Comment
99-17.
94

Mr. Parker: Concurred with Mir. McWhinnle on circulation of negative ballots.
Comment 99-22 (Negative) Mr. Grossman: I agree with n~commendation of
submltter. The alternate methods of (b) and (c) do not" meet the requirements of NFPA lOl, Life Safety Code, Exit Corridor. NFPA lO] reference: 12-3.6.2.2 and 12-3.6.4. Further, storage room does not compare to a to i l e t room, bathroom, shower room, sink closet, or similar auxi l iary space, as nonhazardous to exi t corridor.
Comment 99-22 (Affi.rmative but with comments) Mr. Zimmerman: I t makes sense to of fer several
options for venting a room for the storage of less than 2,000 cubic feet of oxygen. I have no problem with venting to the outside or with mechanical venti lat ion•
I recognize that NFPA lOl requires the integr i ty of an exi t access corridor be maintained. But i t does not make much sense to require a dampest i f the option to provide a louvered opening of 72 inches is selected. By the time the fusible l ink is melted and the damper is activated, the f i r e wi l l already have done i ts damage - and the existance of the damper won't make any difference.
The requirement should be the same for storage areas of less than 2,000 c u f t and for areas of more than 2,000 cu f t i f we are indeed concerned with the 72 inch opening threatening the intecfrity of an exi t access corridor. That is, ALL rooms used for the storage of oxygen should be either mechanically vented, or vented to the outside•
Comment 99-25 (Negative) Mr. McWhinnie: Reference Comlittee Statements for
Comment 99-25. 1. That is a restatement of the problem, and the
essence of the proposal. 2. The problems associated with this issue are
clearly stated in the proposal and supported by the following copy of an actual work-sheet [copy available for review at NFPA Headquarters]; and project 746A actual work-sheet (both already in the Technical Committee and Subcommittees f i l es ) . Also in those f i l es are pertinent data from Plumbing Engineer, September, '83.
NOTE D.P.: Being "unaware of hazards" cannot be a basis to reject. I f so then 99-48, and 99-28, 99-35 must be accepted as (in addition to the Technical Committee and Vacuum Subcommittee) there are 20 Associations and 60+/- involved professionals in unanimous agreement as to hazard (no minority report is known), and 4 possible traumas to patients documented in a professional publication.
Further, 99-43 and 99-74 must be rejected as no dew point l imits should be in required text as no dew point "hazard" has "been reported and proven" (quote from Committee Statement 99-8), and "has not been fu l l y demonstrated" (quote from Committee Statement 99-54)• No one has demonstrated, or even claimed, that, with the presently required aftercoolers and/or a i r dryers, there is a patient hazard.
3. The attached [available for review at NFPA Headquarters] which is in committee f i l es was a "specific recommendation." A similar method for Vacuum has been highly successful. Project 746A work-sheet "observations" item 2 indicates the problem (only one of many) which the following work-sheet (copy) addresses. [Available for review from NFPA Headquarters]•
(See my negative vote on comment 99-28 which is a part of this comment.)
Comment 99-28 (Negative) Mr. McWhinnle: [Reference Complttee Statements on
Comment 99-28.] I. Those informed know, but users are confused
(understatement), especially those "less fami l iar ." I t is often misinterpreted, and many ,users never find i t . Being hidden in a chart is bound to raise doubts when the user has already read 4-3.1.9.7. A "requirement" of this extent/expense i f real ly r,~quired, belongs in and deserves clearly worded text.
At i t s face t h i s " requ i rement" serves no purpose - - • • I .
as no c r i t e r i a i s prov ided to determine "when a i r q u a l i t y cannot be main ta ined" ; no th ina e lse is requi red f o r MCA(b); and to requ i re alarms f o r MCA(b)s, w i thout l imi ts ' c r i te r ia , and without the required "supporting data" [substantiation Reg. lO-lO(c)], and " fu l ly demonstrated need" (quote from 99-25) is beyond NFPA Regulations and!!Style Manual and intent• (See'"Note D.P." in [my reason for negative vote on comment] 99-25, a part of this comment.)
2. 3. Having provided NFPA and i ts Health Care
Faci l i t ies Technical Committee with no data, and not " fu l l y demonstrating" hazards as to patients, f i re , environment, or any other risk related to de~ point i t is contrary to the intent and le t te r of Regulation 10-I0(c) and NFPA Style Manual intent. This topic cannot be a requirement, and must remain in i ts present location - - the Appendix. To do otherwise requires the substantiation of I0-3; "statement of the problem," 10-I0; "considerable research and discussion, 11-9; and a "statement . . . su f f ic ient ly detailed so as to convey . . . to the Association . . . ("the rationale for i ts action so that rebuttal may, i f desired, be offered)", l l - l O .
The claim (99-74) of "a dist inct hazard to l l f e " is not stated, as claimed, in 4-3.1.9.8 and lacks any "data" on "demonstrated need." I t is. a much too strong statement to appear in the required text of the stature of NFPA 99, and is even too alarming to appear in the Appendix - even, i f i t had rationale.
What has happened between the publication of NFPA 99'87 and now, that makes an a rb i t ra r i l y selected level (because of "the lack of a firm number" TCR 99-132 - and because the Subcommittee could not achieve "consensus") a required alarm point?
What new, and patient threatening, medical "research data" (I0-I0) has "been reported and proven" (Committee Statement 99-8) and " fu l l y demonstrated" (Committee Statement 99-54) to jus t i f y making a nation-wide reqvirement out of what is presently an Appendix topic???
This action is completely contradictory to actions 99-18, 99-48, 99-54, 99-74 specif ical ly (among others).
4. 5. Vacuum pumps and systems are outside of the
text of any other Subcommittee, although reference is permitted by way of "Note" or Appendix• [See also my Substantiation in Comment 99-28.]
Comment 99-33 (Negative) Mr. McWhinnie: Vacuum pumps, alarms (and the
entire vacuum project) are out of the Scope ~ and required text - ' o f MGS Subcommittee (but could be referenced in MGS "Notes" or Appendix). (NFPA Regulations, policy, Style Manual intent(s) apply•)
I t is improper for any Subcommittee to include in i ts ~ text, a requirement for a component or function which is assigned to, within the scope, of, and the responsibi l i ty of a di f ferent Subcommittee.
The proposal (table) is clearly for gases, obviously intended for gases and cannot introduce a requirement that is not within i ts responsibil i ty.
Out of the 34 functions proposed, the only one proposed for vacuum, is not only improper, but also wronq ip at least three respects: ,~
I. The "Vacuum Systems" referenced in t~is gases Subcommittee proposal [4-4.1.I .2(e)] has nothing to do with vacuum, is in the gases document, and applies pn_o]Jll to "a l l medical gas piping systems . . . . " The Subcommittee's technically substantiated position that specific gases (any) are to ta l ly di f ferent than a condition of a f lu id, at subatmospheric pressure (vacuum), has been conceded by the Technical Committee. The'Vacuum Systems document is clear on the requirements for these functions.
2. This proposal adds 12 references for i :c lar i ty. All (and properly) refer to only gas systemsi~text requirements. None refers to vacuum.
3. The proposed column heading "Low Pressure" may be proper, as intended for "a l l gases" [ in 4-4.1.I.2(e)] at constant, nominal, operating pressure. I t is not proper for vacuums•
Combining "High" or "Low" - "Pressure" - i s proper for gases conditions above l atm. in psig, but improper and confusing with conditions under l atm. expressed in
95

the Vacuum Systems document as "high" or "low" "vacuum." "Highs" and "lows" above I atm actually move in opposite directions from those below 1 atm; expressed in "hg - a" term, d i f ferent measurement, used throughout the vacuum document, and not at a l l in the gases document. Dif ferent term and opposite movement of highs and low from a common base are confusing. [See Proposal C#024 substantiation.]
4. Gases Subcommittee members including submltter of this proposal, who are also members of the Vacuum Subcommittee, voted on this gases document requirement in both Subcommittees.
Comment 99-34 (Negative) Mr. McWhlnnie: Same reasons as given for Comment
99-33.
Comment 99-33 (Negative) Mr. McWhinnie: The action is not in accord
Regulation I0-I0(c) as to the required substantiation; the proposal provided no "data" or "research" information (10-3); there is no "statement . . . suf f ic ient ly detailed for rebuttal . . . (or presentation) . . . to the Association . . ." (11-I0); and the Technical Committee has not been provided with "reports" of hazard of which the Subcommittee is "aware."
Technical reasons (required) are in 99-28, A.3. and in 99-25, A.2. Note DP.
Those technical reasons ( last above) also apply to 99-43 and 99-74.
Comment 99-36 (Negative) Hr. McWhinnie: A. This proposal was based upon
tile same premises which I believed were the objectives of Saul Aronow, PhD., P.E. in his current proposal for a TIA on another matter."
In the supporting statement for that proposal he stated more eloquently potential problems this proposal envisioned. Dr. Aronow gave permission to quote from his statement.
This proposal (99-156, 180) addresses the problems of "digi ta l components that are much more sensitive to power supply problems . . ." (than other older devices), and "reports" of e lectr ical "~quipment . . . that f a i l s during power transfer . . ,.
This proposal takes into account the fact of Health Care Faci l i t ies emergency power systems and thei r periodic switch-over tests w/timed interruption - - and the "reports of fa i lure during power t ransfer."
Such problems cannot occur with the pneumatically powered continuous/continulty reading, fu l l range indicating, gauges intended in the existing text that have been used safely for many years w/o complaint.
B. The Subcommittee statement of "monitoring" is inconsistent with the intent of the developers of both the gases and vacuum documents - - which intended [4-4.1.1.4(a) and (b), 4-4.2.10, and 4-8.1.1.7(a) and (b)] "pressure gauges" or "vacuum gauges" of the dial type with active needle, and "an indicBted ranqe of 0 in. to 30 in. Hg (vacuum)" (4-10.4.'1.5).
The 18 references in Chapter 4 to "continuous . . . noncancellable . . . responsible observation . . . shall be seen . . . responsible surveillance . . ." were intended, and interpreted, to provide instant information on al l l i fe-support systems, and simultaneous readings of a l l systems - part icular ly for the mixing of gases such as 02/air, 02/C02, 02/N20, etc. where primary (system) pressure(s) differences, depending upon degree, w i l l a l ter the ratios of the resulting multl-component mix. Preciseness of mixtures where required, some as low as .25 l i t e r - or +/- 2% (or lower), at low flows can be seriously affected by s igni f icant ly d i f ferent primary pressures. Primary pressure(s) differences are not uncommon and have been found at 10/12 psig, 20+/-%, (example in Committee f i l e ) .
"continuous . . . noncancellable . . . shall be seen . . ." etc. , throughout both documents, are defined: perpetual, everlasting, constant, incessant, unlimited, uninterrupted. "observation . . . shall be seen . . . surveillance . . ." mean close watch which is, as was or ig ina l ly , thei r intent.
To lose the presently required automatic information of any v i ta l system; simultaneous information of interdependent systems, transient
changes (common), subtle-overtime-decreases or increases (regulator creep or rest r ic t ion - seats, springs, seals, etc.) - without technical substantiation, or addressing the above technical substantiations, this action is not in compliance with the requirement of "technical reason(s) (BRK, 5-9-89), and is c r i t i c a l l y regressive.
Automatic continuous readings are required for v i ta l systems in land, sea, a i r and space vehicles and support equipment, in hazardous equipment and operations, in v i ta l sc ient i f i c equipment and experiments and, yes, for many v i ta l medical devi~es and systems. Medical-Surgical Vacuum Systems' degree of negative
pressure, unlike gases, constantly changes, and at varying rates. Blockages, even at minimum (not uncommon), of any portion of a vacuum system, as well as both normal or abnormal cycling of source equipment, can/"shall be . . . seen . . . " /a t a glance ("close watch"), which is "responsible . . . observation . . . surveillance" as intended.
This proposal would assure that a deteriorating/progressive condition would be detected long before actuation of emergency alarms, and enhance the maintaining of optimum operating conditions.
Comment 99-37 (Negative) Mr. McWhinnie: A. [Reference Committee Statements
on Comment 99-37.] 1. Lab studies were performed for vacuum cr i te r ia ,
and are now detailed in the NFPA 1987: Health Care Fac i l i t ies Handbook, Prologue, page 170. In that same publication the f ie ld "Survey" of hospitals is provided in detai l . The methods employed for the lab study and the f ie ld "survey" would be similar for positive pressure systems and terminals.
99-25 includes a copy of a method that has proven successful.
That data was submitted to both Subcommittees. 2. This same proposal was "held for further study"
in 1986. MGS Subcommittee agrees to the need. B. Technical Reasons:
This proposal recognizes the report (Plumbing Engineer, September, 1983) of "2,833" faul ty outlets.
I t would be an important cr i ter ion to assuring Health Care Fac i l i t ies of providing optimum patient therapy.
Combined with diversi ty, i t would be a tremendous aid to A/E designers, hospital engineers, inspection, cer t i f i ca t ion and accrediting agencies.
Also, ~ portion of Substantiation 4 of Proposal 99-153 (4-4.1.2.4) is applicable.
Comment 99-38 (Negative) Mr. McWhinnie: A. [Reference Committee Statements
for Comment 99-38.] I . True, nor can the Health Care Faci l i t ies be
assured of protection i f this agent is used by an outside supplier - as i t is invariably capped or otherwise sealed by suppliers which can seriously increase the hazard.
Manufacturers/suppliers have a responsibil i ty and should not be free to thei r own devices in a matter of this import. Materials ordered "to meet NFPA 4-4.1.4.1" call be obtained from many sources.
"Out of Scope to prohibit"? How about Carbon Tet - presently, and for many, many years prohibited by NFPA.
2. See above. B. Technical Reasons: (Reasons as given in
Proposal 99-155.)
Comment 99-43 (Negative) Mr. McWhinnie: To make dew point c r i te r ia (now in
the Appendix) a requirement is improper and violates at least Regulation I0- I0(c) .
My negative votes on comments 99-28, 99-25 Note DP, 99-35, 99-43, and 99-74, which also apply.
Comment 99-44 (Negative) Mr. McWhinnie: I . Reasons given in negative vote
on Comment 99-45 apply. 2. Substantiation given in Comment 99-44 apply.
Comment 99-45 (Negative) Mr. McWhinnle: [Reference Committee Statements for
Comment 99-45.]
96
I. Without a specif ic denominator the levels of sensor settings vary by 30%. A £equirement that is not speci f ic, but is ambiguous, is also confusing, can be misinterpreted, and has led to dispute in the f i e ld •
2. I f this is a true statement then the present E ~ E U ~ for back-pressure compensated medical flow meters is without va l id substantiat ion, and must be deleted from applicable Codes/Standards.
3. I f any Health Care Fac i l i t i es do, supporting "data" (Regs. I0-I0, 10-3, I I -9 , 11-10) has not been provided to the Technical Committ,~e or Association.
The issues of med-gas(es) flo,~meter accuracy (and primary pressures) cannot be :separated, are serious medical concerns,.and should be speci f ic . The required audio-visual alarms indicate an emergency-operatlon outside of a safe range. That range should be speci f ic . This proposal provides a speci f ic , and removes an ambiguous, requirement. I t corrects by 30% the present vague range - enhancing the effectiveness of patient therapy. See also substantiation given in Comment 99-45.)
Comment 99-48 (Negative) Mr. McWhinnie: [Reference Comment on Committee
Statement for Comment 99-48.] I. WAGD is not within the Subcommittee scope, and
was not addressed by the Committee (substantiat ion below).
(a) I t is not a Med-Surg patient system. (b) I t is an environmental system and, properly
is referred to in Chapter 5 with requ!rements. (c) Two chapters in 99 cannot cover, provide
requirements for , or otherwise address the subject• Chapter 5 Scope covers this environmental issue, and is the only place where i t s requirements, recommendations, permitted use etc. , should be.
(d) Reference to this topic in chapters other than Chapter 5 should be made in 1.he Appendix, of any other chapter.
(e) A "note" within text is one thing, but a large number of " i f used" notes are scattered throughout another chapter i t is, defacto, included, and has been so interpreted.
( f ) This is not in accordance with the intent of Regulations or Style Manual•
(g) Being out of i t s Scope, Vacuum Subcommittee cannot "provide guidance•"
2. (a) The Technical Committee acknowledges the r isk (November '88 minutes), as does the Vacuum Subcommittee (May '89).
(b) The Vacuum Subcommittee voted heavily (only one negative vote) to delete from the vacuum document the WAGD references and recommended that the Technical Committee accept the proposal (99-18).
(c) The references to WAGD in the Vacuum document are c lear ly contrary to the many risks enumerated in NFPA Health Care Fac i l i t i es Handbook, 1981, 4-7.1.2, pages 177-178, and Prologue, Page 170.
(d) The vacuum document references to WAGD are c lear ly inconsistent with the Technical Committee policy (1986 TCR, repeated twice in Code Red) that " i f we are to er r i t should be on the safe side•"
(e) I n the references of the fol lowing substantiat ion see four potent ial traumas when using "wall suction" fo r WAGD.
( f ) Unti l a WAGD project is assigned for "study" (Technical Committee Statement above) i t is improper to mislead by inference where there is documented r isk.
(g) There are numerous author i ta t ive sources/publications which c i te safe references - including ambient d i f f e r e n t i a l , nonreturn vent i la t ion exhaust, single or double damped microvac blower-plenum, etc.
Also, see Substantiation in Comment 99-168, substantiation from "a l l Subcommittee . . . (through) the i r cl'ients accordingly."
Comment 99-51 (Negative) Mr. McWhinnle: [Reference Committee Statements fo r
Con~ent 99-51.] 1. In certain applications the greater the degree
of vacuum the greater the hazard - pulmonary drainage being only one.
WAGD is another. The substantiat ion nor i ts references have not been challenged, nor is 'there anything in the record to refute Sharrok and Leith on the four named possible traumas.
2• Same is true of dew point. 3. 4. Anything, re safety, in NFPA Health Care
Fac i l i t i es projects, e i ther as to patient safety or f i r e hazard, is within scope.
That statement overlooks the alarm requirements for gases•
In addit ion, see substantiat ion from Comment 99-179.
Comment 99-56 (Negative) Mr. Parker: Reasons given in Negative ba l lo t on
Comment 99-57 apply.
Dr. Swope: Relaxation of current standards is not substantiated by submitted data. Congroenc~ of experience under IEC document and US standards may be in doubt. I feel that r isk reduction should be documented. ;
Mr. McWhinnie: Changed vote to negative on c i rcu lat ion of negative votes, giving fol lowing reasons:
A. The Technical Committee actions have not addressed or "extensively discussed" the previously presented ( i n Subcommittee) r ea l i t y of patient r isk, nor has i t countered the claims in these related comments.
I agree with the recommendations of the Subcommittee and the Task Force on Leakage Current•
Having attended the 3une ]9/20, 1989 Technical Committee.meetihg I can state nothing technical was discussed "extensively," nor do I recall any new technical information having been introduced nor any serious discussion of "pat ient r i sk • "
The most "extensively" discussed topic was that of concern in connection with the 1992 schedule:for the European (Common) Community.
B. I consider the Technical Committee Chairman's opening statement 6/19/89 ["the Subcommittees are s t i l l the technical experts for the Technical Committee"] to be and (without refutat ion) must be, and are, the "experts." These Technical Committee actions debase the process as the Technical Committee lacks a preponderance of "expert ise" found in (and properly so) the appropriate Subcommitees, and evidenced by the Technical Committee minutes themselves: "A number of members expressed concern about ' the i r competency to make a decisionZon the matter."
The Technical Committee respons ib i l i ty is to study. the Subcommittee(s) procedures data and rat ionale, which I have done to the best of my l imited a b i l i t y in this area, and I can only agree with the recommendations of the "expert Subcommittee."
When members of the Technical Committee question the i r own "competency to make a decision . . ." (on thls issue), and are slmultaneously "expected . . . to use the i r best technical judgement (admittedly lacking) in deciding l imi ts , c r i t e r i a , etc." the process is c r i t i c a l l y defective•
"In the area of highly technical, and c r i t i c a l , problems logic is a l l too often a stranger to the decisions of mixed committees" (U.S. Ai r Force General "Hap" C. Arnold)." The Technical Committee Statement of November '86,
repeated twice in Code Red (and never withdrawn or refuted) that " i f we are to err i t must be on the side of safety'! is, therefore, a policy far beyond a mere guideline•
Those pol ic ies of "expert ise" and "safety" have been abrogated - and do not enhance the desired "respect" of de l iberat ive individuals for NFPA procedures and, therefore, documents•
This Section B. applies equally to Comments 99-17 through 99-20; and 99-74, 99-28, 99-25 "Note"; as well as to related 99-33, 34, 35, 43 and 48.
C. The Technical Committee action on the subject 6 comments, and the last above 12 comments, usurp the Subcommittees heavy respons ib i l i t ies ; f l y in the face of repeated assurances at the inception of the Health Care Fac i l i t i es 99 project ( that i t would change nothing on the then Technical Committee leve l ) ; that the i r respons ib i l i t ies would remain the same ~ and that
97

the (then proposed) 99 Technical Committee would act essentially as had the Health Care Faci l i ty correlating Committee.
The ballots (then), ref lect ing the concerns and doubts about those assurances, were prophetic.
D. These 18 Technical Committee actions, al l referenced above (among others), beg a clear, open, and dependable statement to resolve these contradictions, and set lucid policy.
Mr. Mattern: Changed vote to negative on circulation of negative votes, giving the following r e a s o n s :
I t is my opinion that i t was inappropriate for the Technical Committee to over rule the Subcommittee, of the Health Care Faci l i t ies, on the above ident i f ied comments.
I t was the charge to the Subcommittee that they review al l of the available documentation and based on this review, along with discussions with proponents of these submittals bring forth a recommendation to the Technical Committee. This Committee f u l f i l l e d this obligation and did in fact bring forth a recommenation.
I t is my opinion that the Technical Committee was inappropriate in their actions, which in fact overturned the Subcommittees recommendations in favor of the submittals of Mr. Devore, by accepting his comments, and amending the Subcommittees report to the Technical Committee.
I have always understood that i t is the excepted practice of Technical Committees, to appoint subcommittees when special expertise is required on a subject by experts in a specific f ie ld , in order to enlighten the Technical Committee so that they can have the ab i l i t y to act in a responsible manner on a subject, and allow them to evaluate al l of technical merits o f a given point, in order to reach an enlightened decision and reasonable standard. I t appears that in this instance this was not done.
I t is further my understanding, that t radi t ion is, that only when a Subcommittee action was inappropriate, as supported by suf f ic ient documentation, or additional testimonial, supported by suf f ic ient "new" documentation is submitted to the Technical Committee, does a Technical Committee overturn, amend, or otherwise change a Subcommittees recommenation.
In the above referenced submittals i t is my opinion that suf f ic ient documentation was not submitted to cause the Technical Committee to change the Subcommittees recommendation, thus I am casting a negative vote on Comments 99-56, 99-57, 99-58, 99-59, 99-60 and 99-61.
Dr. Dornette: Changed vote and concurred with negative votes on circulation of negative ballots.
Comment 99-57 (Negative) Dr. Aronow: I believe the action taken by the
Electrlcal Equipment Subcommittee should be sustained because i t is a reasonable solution to a d i f f i c u l t problem. The problem has both technical and nontechnical aspects, and I think the technical should take precedence.
I. Two kinds of leBkBqe currents. The problem has two parts, intracardiac currents and other body currents. Most of the discussion at the August, 1988 IEC/AAMI meeting and at the Technical Committee meeting had to do with intracardiac currents (the old microshock). This is a red herring. There are not reported problems because NFPA 99 and i ts predecessors imposed t ight l imits which industry met with l i t t l e problem. Equipment is now quite safe. The differences between NFPA 99 and IEC 601-I are minor and they have been resolved.
I I . Hazards. The disagreement is with other currents (chassis leakage in our terminology). No one claims that 500 mlcroamperes (uA) wi l l be lethal, and we agree there are no reports of deaths, but everyone agrees that 500 uA wi l l cause sensation, star t le, and. pain in a percentage of the population. The Canadians have rationalized that this is an acceptable hazard. The actual reports from Europe that were presented at the IEC meeting did not discuss this issue. We have always maintained that although the probabil i ty of such hazard is small, i t should be avoided where the population involved is sick, immobilized, in close proximity to much electr ical equipment, and often not able to react as normal persons would.
The whole world agrees that 500 uA is a reasonable leakage current l imi t for general domestic appliances used by the public. Our committee in the past applied a safety factor of 5 for patient appliances, to I00 uA. The Subcommittee, af ter much debate, reduced the safety factor to 2, a l imi t of 250 uA. I submit that that is reasonable, considering that we have a peculiar population, with a mul t ip l ic i ty of appliances, and an environment that subjects the appliances to much abuse.
I I I . Costs. The argument is made that our t ighter l imits greatly increase the cost of manufacture. The majority of patient appliances are small and for these that is not true~ The leakage problem was resolved years ago. IEC 601-I spends a lo t of discussion on large appliances, mobile X-ray machine, hypothermia units, etc. Everyone agrees these have d i f f i cu l t y meeting lO0 uA, but NFPA 99 provides an exception. I t is not reasonable to d is tor t a general provision to accommodate a few special cases.
There is now a growing class of intermediate sized appliances, l ike ultrasound, computerized analyzers, etc., where i t is d i f f i c u l t to meet a lO0 uA l imit . These are complicated by problems of electromagnetic noise that may require l lne f i l t e r s . Manufacturers claim i t is expensive to design to meet two leakage l imits. However this is not as valid an argument as i t appears. Since power voltage in Europe are roughly twice that of the US (220 versus 120), an appliance that has 500 uA leakage in the US would have about 1000 uA leakage in Eruope. This would be unacceptable, and the circuits would have to be redesigned anyway.
I submit that interms of design, the Subcommittee's decision of 250 uA is about the same as 500 uA in Europe.
IV. Nontechnical. There is no question that harmonization of standards on a worldwide basis is essential and is the wave of the future. The basic physiology and physics is the same al l over the world. However, there are d i f ferent perceptions of degree of hazard and levels of safety. I t is regrettable that there was not adequate discussion of this problem with the IEC Committee before 601-I was f inal ized. However, I do not think these nontechnical aspects warrant upsetting the reasonable solutions achieved by the Subcommittee for our standard.
Mr. Parker: These remarks are addressed specif ical ly to Public Comment 99-57. The other Comments are essential ly corollaries which stand, or f a l l , with Comment 99-57.
I. The Technical Committee on Health Care Faci l i t ies is unwise to override both the recommendations of the Electrical Equipment Subcommittee and those the "Task Force on Leakage Current" chaired by Mr. Jack Berger. The Technical Committee should heed the advice (minutes of June 18/19, 1989 Technical Committee meeting, p3) of i ts Chairman that "the Subcommittees are s t i l l the technical experts for the Committee." The subject comments concern material assigned to the Electrical Equipment Subcommittee and that committee did not recommend a 500 uA ground leakage current.
2. The Technical Committee's Statement: "This subject was extensively discussed by the Subcommittee on Electrical Equipment at i ts April 27, 1989 meeting and by the Technical Committee on Health Care Faci l i t ies at i ts 3une 19/ZO, 1989 meeting" is not a technical substantiation for anything. I t merely implies considerable controversy. The Comment provided no new technical material beyond that submitted to the Technical Committee for consideration in preparing i ts Report. The Comment is essentially a reiterat ion of the proposal submitted for the TCR. In the absence of new technical material i t is unreasonable to revise the TCR. Be that as i t may, by accepting the Public Comment the Technical Committee tac i t ly agrees with the Comment's substantiation which, for reasons stated below, lacks merit.
3. The argument of the Comment is that "The change proposed is consistent with IEC 601-I which has been proven to be acceptable to the European community for more than ten years." That statement is not technical data. I t ref lects economic and pol i t ica l issues which are not within the scope of the Technical Committee. The Technical Committee is concerned with safety. In this case safety has to do with physiology, patient care, and medical practice; on these topics no new data was provided.
98

4. The Commenter's agrument presumes that medical practice in Health Care Fac i l i t i es is the same in Europe and the United States. This is not so. For example an item o f .pa r t l cu la r concern is the.e lec t r ic patient bed which, in the United States, is very widely used in both general and c r i t i ca l care areas. Not only are e lec t r i c beds more common in North America but aggressive bedside therapy is much more extensively used. A comparison of Cr i t i ca l Care techniques between the United States and England, for comparable groups of patients, shows that Swan Ganz procedures, which are almost always done at the bedside ~nd involve the introduction of transcutaneous conductors into the heart, are 200 time as common in the U.S. In my hospital alone 1,500 such procedures are performed annually, often under urgent and stressful conditions. Under these circumstances the probab i l i t ies fo r accident are greatly magnified. Leakage currents from e lec t r ic beds have found the i r way into cardiac conductors with fa ta l results. Patient beds require more str ingent standards than elecl.r ic toasters, which, i f bu i l t to U.S. standards [ANSI C)01.1], would also meet IEC 601-I standards for medical devices.
5. The IEC supporters argue (t.evln, M., Leakage Current - Then and Now, communicated to the Technical Committee at the October 13, 198B meeting) that loss of ground is an event of "low" (.01) p r o b a b i l i t y . . F o r e lec t r i c beds that f igure seems reasonable. I t is prac t ica l ly impossible to ensure re l iab le grounding at a l l times for every device in a large inventory of medical devices (my hospital has over I000 e lec t r ic beds). Beds are moved frequently For housekeeping and sometimes for patient transport, and the i r power cords aresub jec t to unusual wear. Yet, taking my own hospital as an example, with an av()rage of four or f i ve Swan Ganz procedures a day, the probabi l i ty of such a procedure being done in an ungrounded bed would (according to Levin's pobabi l i ty .ca lcu lat ions) be about l in 20. Of course some beds are used more frequently than others for invasive procedure,s, so we are not dealing with stochastic events, and the I in 20 ra t io is probably high. Nevertheless, in an ungrounded bed with hal f a milliamperes of leakage, even one procedure in 500 would be unacceptable.
6. Another cited basis for the proposed 500 uA "safe" current has been the threshold of perception studies of the type made by Dalziel (Dalz iel , C.F. Reevaluation of lethal e lec t r i c currents, IEEE Trans. Indus. General Applications,4(5):467-476,1968) and others. These studies were fo r skin contact with comparatively large electrodes on healthy adults. They do not apply to readi ly accesssible mucous membranes or to patients who are sedated, unconscious or otherwise unable to terminate the experiment. I t is easy to show that 500 uA AC level is in to lerable (Duncalf D. and Parker B., Proc. AAMI 14th Annual Meeting, 1979, p. 65). One merely applies that current via small electrodes to the l ips . The same current applied to a human heart w i l l invar iably cause ventr icular f i b r i l l a t i o n .
7. The e lec t r i c bed is an exa~ple of a more general argument that the proposed chassis leakage of 500 uA can not be safely applied to a l l kinds of e lec t r ica l equipment in a l l patient care areas. Angiographic dye in jectors, electrocardiographs, physiological monitors, cardiac pacemakers, X-ray tables, and e lec t r i c operating tables have also been implicated in cases of inadvertent f i b r i l l a t i o n in hospitals (Parker B. Why not change the leakage current to 60 uA, Biomed Safety & Standards 8:60, 1978, f3) . In some cases the fa ta l , or near f a ta l , current levels were less than 200 uA. At least for these specif ic devices the present Safe Current Limits should be retained.
8. Final ly, the maker of the Comment submitted a l e t t e r to the Technical Committee providing a personal in terpretat ion of a requirement of IEC 601-I which contradicted Dr. Aronow's in terpretat ion that the IEC permitted even higher leakage currents than 500 uA. This points up another problem. How are we to resolve this? I am unaware of any IEC procedure for providing timely o f f i c i a l in terpretat ions of the i r standards. The l e t t e r went on to in fe r that to disagree with the IEC posit ion would cause a loss of "respect" for NFPA standards. What ga l l ! The IEC is a bureaucratic
nightmare operating in a part of the world where
business is not constrained by Anti-Trust laws. In th is whole business of harmonization between NFPA and the IEC we have not heard any hint of compromise by the IEC. The NFPA w i l l maintain i t s respected posit ion only by preserving an e f f i c i e n t , open standards making process, subject. to frequent review, and based on the best technlqal consensus.
9'. My technical thesis has been that theproposed 500 uA leakage is not safe fo r a l l medical devices. I have i l l us t ra ted this by the example of the e lec t r ic patient bed, though a simi lar case might also be made fo r certain other devices. I therefore urge reject ion of the"subject Public Comments. Sooner or la te r a 500 microamp leakage current for a l l Medical Devices would be disastrous fo r patients and for Health Care Fac i l i t i es .
Dr. Swope: [Same reasons as given for negative vote on Comment 99-56.]
Mr. McWhinnie: [Same reasons as given for negative vote on Comment 99-56.]
Mr. Mattern: [Same reasons as given for negative vote on Comment 99-56.]
Dr. Dornette: [Same reason as given for negatlve vote on Comment 99-56.] ,,
'i Comment 99-57 (Abstain) Mr. Fischer: Changed vote to abstain on
c i rculat ion of negative ba l lo ts , giving the following reasons]:
I would appreciate your recording my bal lo t as af f i rmat ive on a l l issues except Comments 99-57 and 99-60. On those, two, please change my vote to an abstention. Af ter reviewing a l l the information and facts ava i lab le , I feel there is s t i l l some confusion and room for discussion. The Technical Comml.ttee unfortunately did not have an opportunity to hear the Chairman of the Subcommittee nor the or ig inal proposer. In the absence of some additional comments at the time of the meeting, I feel that the Technical Committee should have accepted the decision of the Subcommittee. Unfortunately, at this state in the voting, that poss ib i l i t y is not avai lable. I must e i ther vote for or against the Technical Committee's action, which was to change the Subcommittee's action. I feel that I can do neither. Therefore, I am abstaining, with the hope that the Standards Council in the l r review wi l l reinstate the Subcommittee's action. They, and only they have that power now.
I would hope that the Technical Committee and Subcommittee wi l l have fur ther hearings 'and discussions on this very sensit ive subject. I t may require a TIA in the future.
Comment 99-58 (Negative) Mr. Parker: i~ [Reasons given in negative ba l lo t on
Comment 99-57 apply.]
Dr. Swope: [Same reasons as given for negative vote on Comment 99-56.]
Mr. McWhinnie: [Same reasons as given for negative vote on Comment 99-56.]
Mr. Mattern! [Same reasons as given for negative vote on Comment 99-56.]
Dr. Dornette: [Same reasons as given for negative vote on Comment 99-56.]
Comment 99-59 (Negative) Mr. Parker: [Reasons given in negative ba l lo t on
Comment 99-57 apply.]
Dr. Swope: [Same reasons as given for negative vote on Comment 99-56.]
Mr. McWhinnie: [Same reasons as given for negative vote on Comment 99-56.]
Mr. Matternl [Same reasons as given for negative vote on Comment 99-56.]
99 i
. Dr. Dornet te : [Same reasons as given f o r negat ive vote. on Comment 99-56. ]
qomment 9 9 - 6 0 ( N e g a t i v e ) Dr. Aronow: [Same reason as given f o r n e g a t i v e
vote on Comment 99-57. ]
• Mr. Parker: . [Reasons given in negat ive b a l l o t on Comment 99-57 app l y . ]
Dr. Swope: [Same reasons as given f o r negat ive vote on Comment 99-56. ]
Mr. McWhlnnle: [Same reasons as given f o r negat ive vote on comment gg-s6 . ]
Mr. Mat tern: [Same reasons as given f o r negat ive vote on comment 99-56. ]
Dr. Oornet te: [Same reasons as g iven f o r negat ive vote on comment 99-56. ]
Comment 99-60 (Absta in) Mr. F ischer : [Same reasons as given f o r abs ten t ion
on comment g9-57. ]
Comment 99-61 (Negat ive) Mr. Parker: [Reasons given in negat ive b a l l o t o n
Comment 99-57 app l y . ]
Dr. Swope: [Same reasons as given f o r negat ive vote on Comment 99-56. ]
Mr. McWhinnie: [Same reasons as given f o r negat ive vote on Comment 99-56. ]
Mr. Hat te rn : [Same reasons as given f o r negat ive vote on Comment 99-56. ]
Dr. Dornet te : [Same reason as given f o r negat ive vote on Comment 99-56. ]
Coment 99-74 (Negat ive) Mr. McWhinnie: The requ i red "da ta" -
" s u b s t a n t i a t i o n " - has not been prov ided. See a lso my negat ive votes on comments 99-28, 99-25 "Note DP", 99-35 and 99-43.
Public Comments involvin~ Sections 4-3 through 4-6, and their associated definitlons and Appendix material, have also been submitted to letter ballot concurrence of the Technical Committee on Industrial and Medical Gases. This Committee consists of 9 voting members and 1 nonvoting member of whom 5 voted affirmatively, and 4 ballots were not returned (Messrs. Kitson, Cares, Henrici and Wolpert).
100

ii .i
(Log #53) 99 - I - (2-2): Reject ~ : D.A. McWhinnie, Hickory Hi l ls, ILL ~MMENT ON PROPOSAL NO.: 99-3 RECOMMENDATION: [In proposed revised definition of adiabatic heating], add "or recompression". SUBSTANTIATION: Common in transf i l l ing. As higher pressure in the supplying container is released, pressure and temperature drops, and the gas is then recompressed at, or in, the receiving container - - often with high temperature increase. Evidenced by the need for restricting orifice/burner charging coils to reduce velocity impact and minimize "recompression" heat build-up. COMMITTEE ACTION: Reject. CpMMITTEE STATEMENT: Addition of "recompression" is redundant. Recompression is compression. Definition is complete as proposed in TCR.
(Log #14) 99 - 2 - (2-2): Reject SUBMITTER: Saul Aronow, Technology in Medicine, Inc. COMMENT ON PROPOSAL NO.: 99-26 RECOMMENDATION: Reject Proposal 99-26 and retain the wording of 2-2, NFPA 99 (1987), definition of "Line Isolation Monitor". ~UBSTANTIATION: The definition in 99-26 is from NEC, Article 517. That definition dates back to before 1971 and refers to an obsolete form of monitor called a "ground contact indicator". The definition does not make any sense with reference to present technology. The definit ion in NFPA-99 (1987) is technically correct and was arrived at after long deliberations over the years. I t is true that correlation between 99 and 517 is necessary, and therefore the definition in 517 should be changed to that in 99. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: While definition in existing edition of NFPA 99 is technically correct, definition in NFPA 70, National Electrical Code, is also correct. Committee chooses to correlate definitions, and use one from NEC to reduce confusion.
Definition in NEC is s t i l l current with respect to present technology because devices s t i l l continually sample impedances.
(Log #4) 99- 3 - (2-2): Accept in Principle SUBMITTER: Herbert P. Rhees, Champion Pneumatic Machinery Co., Inc. COMMENT ON PROPOSAL NO.: 99-33 RECOMMENDATION: New definit ion of "Oil-Free or Oil-Less Air Compressor".
Oil-Free or Oil-Less Air Compressor. An air compressor designed specifically to compress air without the use of oi l anywhere in the compressor, including, but not limited to, crankcase, cylinder, air end, bearings, etc. SUBSTANTIATION: Reciprocating compressors which have oil in the crankcase or gear box separated only by distance piece and packing. Packing could fa i l and oi l would travel the piston rod into the air cylinder and into the airstream. This has happened in distance piece "oi l free machines". Also in lubricated rotary screw or rotary vane compressors where the air chamber is flooded with oi l and separated out by means of an external separator. Separators have and do fai l causing major quantities (gallons) of ol l to enter the airstream. Downstream f i l t ra t ion wi l l not guarantee stoppage of that oi l flow. Also, oi l may come in contact with oxygen, see page 99-43,, paragraph 4-6.2.1.2 - Special Precautions. COMMITTEE ACTION: Accept in Principle.
See Committee Action on Comment 99-5 (Log #7).
COMMITTEE STATEMENT: Subcommittee on Nonflammable Medical Piped Gas Systems agrees with additions recommended. However, addition of "gear box" is another necessary example of a possible oi l contamination source.
Qualifier on term "bearing" is needed since there is a type of bearing that would be unacceptable.
!Log #5) 99 - 4 - (2-2): iAccept in Principle SUBMITTER: RobeRt W. Shaffer, Powerex-lwata Air Technology, I n c . COMMENT ON PROPOSAL NO.: 99-33 RECOMMENDATION: New definition of "Oil-Free or Oil-Less Air Compressor". An air compressor designed specifically to compress air without the use of oil anywhere in the compressor, including, but not limited to, crankcase, cylinder, air end, bearings, etc. SUBSTANTIATION: Air compressors without the use of oll anywhere are inherently safer in those applications where no oi l in the discharge air is c r i t i ca l . Seals used to keep oil out of the compression chamber wil l wear and eventually leak i f not maintained. The use of this type of compressor wil l not only be safer, but wi l l actually decrease cost in many instances. COMMITTEE ACTION: Accept in Principle.
See Committee Action on Comment 99-5 (Log #7). COMMITTEE STATEMENT: Recommendation is identical to Comment 99-3 (Log #4). Committee Statement for that comment is applicable here.
(Log #7) 99 - 5 - (2-2): Accept in Principle ~ : David L. Brit tain, Busch, Inc. COMMENT ON PROPOSAL NO.: 99-33 RECOMMENDATION: Change proposed definition of "Oil-Free Air Compressor" as follows:
Oil-Free Air Compressor. An air compressor designed specifically to compress air without the use of o i l anywhere in the compressor, including, but not limited to, crank case, gear box, bearings (except permanently sealed, grease lubricated), etc. SUBSTANTIATION: :Current technology of available oi l - free (also called oi l- less) compressors requires the use of permanently sealed, grease lubricated bearings for acceptable l i f e . The definition needs to differentiate between "o i l " and "grease," since some people assume grease to be in the same classification as o i l . COMMITTEE ACTION: Accept in Principle.
Modify definition of "Oil Free Air Compressor" in TCR to read:
"An air compressor designed . . .. including, but not limited to "crank case, aear bQx, cylinder, air end, and bearinqs (except thQse permanently sealed and qrease lubricated)." [Change underlined.] COMMITTEE STATEMENT: "Cylinder" and "air end" are components of air compressor for which i t is necessary to keep oil free.
(Log #8) 99 - 6 - (2-2): Reject SUBMITTER: James Tapkas, Atlas Copco Industrial Compressors, Inc. COMMENT ON PROPOSAL NO.: 99-33 RECOMMENDATION: New definition of "Oil-Free or Oil-Less Reciprocating Air Compressor."
Oil-Free or Oil-Less Reciprocating Air Compressor. reciprocating air compressor designed specifically to compress air without the use of oi l anywhere in the compressor, incIGding, but not limited to, crankcase, cylinder, airend! bearings, etc.
\
101

New definition of "Oil-Free Rotary or Centrifugal Air Compressor."
Oil-Free Rotary or Centrifugal Air Compressor. A rotary or centrifugal a i r compressor designed specifically to compress air without the use of oi l in the compression chamber with a time proven seal system to eliminate the possibi l i ty of oi l contamination from bearings, gears, etc. SUBSTANTIATION: With over twenty (20) years of operating experience with oi l - free rotary screw compressors and centrifugal compressors, i t has been proven oi l- free compressed air can be provided as long as the compressor has been designed to not require oi l in the compression chamber. The design considerations for reciprocating, rotary, and centrifugal compressors are al l very different. I t is therefore necessary to differentiate between these types of compressors. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Compressors are available to deliver medical compressed air within the definit ion per Subcommittee on Nonflammable Medical Piped Gas Systems action on Comment 99-5 (Log #7). I t is not necessary to differentiate between types of compressors because any compressor that met the definit ion referenced would be acceptable.
(Log #1l) 99 - 7 - (2-2): Reject S__UBMITTER: Bruce W. Osborne, T.I. Pneumotive COMMENT ON PROPOSAL NO.: 99-33 RECOMMENDATION: A. Current accepted Recommendation reads:
Oil-Free Air Compressor. An air compressor designed specifically . . . . including, but not limited to, crankcase, ger box, bearings, etc.
B. Should read: Oil-Less Air Compressor. An air compressor designed
with permanently sealed bearings in an open crankcase design specifically to compress air without the use of o i l . SUBSTANTIATION: Definition in "A" above is s t i l l unclear. First, there is a dist inct and industry acceptable difference between lubricated, oi l- free and oi l- less air compressors (supporting material available for review at NFPA Headquarters). Second, an oi l- less air compressor should be the appropriate unit since there is no oi l present in the crankcase, therefore no oi l can migrate into the system. The bearings (in al l compressors) must be at least grease lubricated, therefore permanently sealed bearings ut i l ized in an open crankcase design oi l- less air compressor would be appropriate for medical a i r use. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: I. For purposes of this document, oi l - f ree air compressors, as defined in Committee Action on Comment 99-5 (Log #7), are acceptable for medical a i r purposes.
2. Design of crankcase is not necessary in defining term "Oil-Free Air Compressor" for purposes of this document.
(Log #12) 99 - 8 - (2-2): Reject S_S~_~tIITTER: P.J. Stanaitis, Ingersoll-Rand Company COMMENT ON PROPOSAL NO.: 99-33 RECOMMENDATION: Revise as follows:
"The air compressor and ancillary equipment shall be designed, bui l t and capable of being installed to supply on a continuous basis medical quality breathing air. Both lubricated and nonlubricated roatary and reciprocating compressors with the appropriate accessory equipment are acceptable for this application." SUBSTANTIATION: The quality of the air should be specified by NFPA. The type of compressor and ancillary equipment to support continuous flow of medlcal breathing air is the responsibility of the manufacturer. Quality of a i r is important not the type of compressor to be specified. NFPA should be interested only in tlle final product, that being the purity of the compressed air delivered to the system.
COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Submitter's Recommendation is not suff iciently restr ict ive. Lubricated air compressors (as proposed to be defined by Submitter) have been reported and proven to contaminate air systems to the extent that f i re hazards may be created.
(Log #9) 99 - 9 - (2-2, 12-2.6): Reject B~LU_~_H_!_T_~_~: Marvin J. Fischer, Brookdale Hospital Medical Center COMMENT ON PROPOSAL NO.: 99-47, 245 BECOMMENDATION: Change definit ion of "Wet Locations" in Chapter 2 to a~ree with the wording adopted in these proposals. This is mainly an editorial change. SUBSTANTIATION: Wording in Chapter 2 is different. This would leave two different definitions for the same words in one document, creating an obvious conflict. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Committee Action on Comment 99-10 correlates situation.
(Log #6) 99 - 10 - (2-2): Accept in Principle ~ : Mike Daniel, U.S. Army Health Facil i ty Planning Agency COMMENT ON PROPOSAL NO.: 99-47 RECOMMENDATION: 1. Change the definit ion of "Wet Location" to read as follows: .
Wet Location. Wet locations are those patient care areas that are normally subject to wet conditions while patients are present, including standing fluids on the floor or r_rgJLtj_~ drenching of the work area intimate to the patient or staff. Routine housekeeping procedures and incidental spillage of liquids do not define a wet location. (Changes underlined)
2. This change should also apply to 12-2.6(c). SUBSTANTIATION: The wording accepted by the Committee is essentially what was recommended by the Ad Hoc Subcommittee on isolated power systems. As a member of that Subcommittee, I am concerned that the arbitrary deletion of the word "routine" between "or" and "drenching" (with respect to the previous definition) may send an erroneous signal and lead to widespread misinterpretation of Committee intent. The word "routine" was dropped by the Subcommittee with the general consensus that "normally" used earl ier in the definition would also be considered applicable to "drenching". A later ruling by NFPA staff, however, included the following interpretation:
"For drenching, 'routine' would be more appropriate because there is no such thing as 'normal' drenching (considering the opposite, i ,e . , 'abnormal' drenching). In context of definit ion, issue is 'when' (or how often) drenching occurs, as opposed to 'amount' or 'how much' drenching occurs." ,
The Subcommittee did not have the opportunity to meet after this ruling by NFPA staff. The Subcommittee definition that went forward did not, therefore, address this issue. In order to c lar i fy intent and make the definit ion technically correct, request that the word 'routine' be reinserted in the definition as indicated. This wi l l help to avoid further misinterpretation of an extremely controversial definltion/issue. COMMITTEE ACTION: Accept in Principle.
I. Rephrase wording in Committee Action to Proposal 99-47 to read as follows:
Wet Locations. Those patient care areas that are normally subject to wet conditions while patients are present. Thi~ includes standing fluids on the floor or drenching of the work area, either of which condition is intimate to the patient or staff. Routine housekeeping procedures and incidental spillage of liquids do not define a wet loction. [Changes underlined.]
Replace definit ion of wet location in Chapter 2 with the above.
2. Revise 12-2.6(c) to read: (c) Wet Locations. (See definit ion in Chapter 2.)
102

'. i i
COMMITTEE STATEMENT: I. Rephrasing is considered to c lar i fy the problem of misinterpretation as to when "standing fluids" or "drenching" constitutes a'wet location. Subcommittees on Anesthesia Services and Electrical System believes rephrasing also meets the intent of Submitter on the issue of "how much" vs "when" drenching.
Addition of word "routine" before drenching would create confusion with phrase "routine housekeeping procedures" in sentence 2.
2. Having definit ion only in Chapter 2 eliminates confusion, and conforms to NFPA Style Manual on definitions.
(Log #42) g9 - 11 - (3-4.1.2.6): Reject SUBMITTER: Alan Lipschultz, Medical Center of DE COMMENT ON PROPOSAL NO.: 99-64 RECOMMENDATION: Revise Submitter's proposal to take some of the wording intended for Section 3-4.1.2.6 and instead add i t to the definition of "Wet Locations".
Revise definit ion of "Wet Locations" to add an additional sentence at the end reading:
"Hydrotherapy fac i l i t ies , immersion l i thotr iptors, swimming pools and similar patient care areas in which patients are intentionally immersed in fluids during the cause of treatment are considered wet locations." S__UBSTANTIATION: These areas clearly are wet locations. The Submitter's wording pointed out that the existing definit ion for "Wet Locations" does not include this type of patient care area. I think his wording correctly belongs in the definition rather than the body of the standard, ~_OMMITTEE ACTION: Reject. COMMITTEE STATEMENT: I t is not necessary to have examples for definitions.
(Log #10) 9g - 12 - (3-4.1.2.6(a) Exception No. 2): Accept ~ : Marvin 3. Fischer ~, Brookdale Hospital Medical Center COMMENT ON PROPOSAL NO.: 99-6? R_ECOMMENDATION: Reject this proposal. SUBSTANTIATION: The Substantiation given is that "safety requirements for wet locations have been clarif ied (see Committee Action on Proposal 99-47 (Log #AS-3).)" Proposal 99-47 in fact only changes the definiton for a wet location. I t does not address the safety requirements. While the document is to be used for new construction only, some jurisdictions adopt i t for both new and existing construction. This could be a very costly and unnecessary change for an existing insti tut ion which could have met the requirements for Exception No. 2. This document does not specifically address existing conditions. COMMITTEE ACTION: Accept.
(Log #15) 99 - 13 - (3-4.2.2.2(c)(I)): Reject SUBMITTER: Saul Aronow, Technology in Medicine, Inc. COMMENT ON PROPOSAL NO.: 99-84 R _ E _ C p M ~ : Accept proposal 99-84 as submitted. ~BSTANTIATION: The substantiation (b) in the proposal is quite valid. The Submitter presents a very good case that having a mix of receptacles provides increased safety. The receptacles on the cr i t ical branch should be clearly differentiated from those on the normal system, so that the Committee Statement in 99-83 may be considered a much less significant hazard. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: 1. Risk of failure of normal power and emergency power/circuits is very low.
2. Proposal would create confusion for staff in terms of having normal-power receptacles lose power i f normal power were lost (as noted in Committee Statement on Proposal 99-83 in TCR).
[Issue was extensively discussed at May 8, 1989 meeting of Subcommittee on Electrical Systems.]
(Log #43) 99 - 14 - (3-4.2.2.2(c)(I)): Reject ~UBMITTER: Alan Lipschultz, Medical Center i f DE COMMENT ON PROPOSAL NO.: 99-84 RECOMMENDATION:I I support the Submitter's original proposal. I urge the Committee to reverse i ts previous decision. : SUBSTANTIATION: The whole purpose of the emergency power system is to provide continuity of power. Toward this goal, the standard requires that the emergency power system be run in different conduits, different panels from normal power. The rationale for this requirement is to avoid having crucial power needs total ly vulnerable to failure of any one device or damage to any one location.
When a crucial patient care location is supplied entirely by emergency power, this basic precept is ignored. When IO0 percent of the power in a given area is on emergencypower, 100 percent of their Rower flows through the transfer switch, one conduit andone branch panel. A failure anywhere along this chain wil l leave the area without any power. In an ICU or OR situation, where al l of the rooms have 100 percent emergency power, i t could happen that a fault could entirely knock out power to the whole ICU or OR suite.
Truly crucialpat ient equipment is either battery operated, or alarms when power is cut off (such as ventilators) ori}is constantly attended (such;as heart lung pumps). I t is true that i f one has mixed emergency and non-emergency power in an area~ the users may plug l l f e support equipment into the normal power outlets. However, they wi l l know that power has been interrupted (because the lights wil l go out until emergency power, comes on) and be able to take prompt action to be able to replug crucial devices into emergency power'outlets.
I t may happen~ however, that the emergency,outlets lose power and the normal power outlets keep.lgoing. I f there is not a Mixture of emergency and non-emergency outlets, the users wil l be helpless to take corrective action.
I support this proposal over the similar ones on the same subject because "most" implies a heavy majority of the outlets in these areas, whereas "selected" carries no such implication. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Same Recommendation as in Comment 9g-13 (Log #15). Committee Statement for that comment is applicable here as well.
(Log #16) 99 - 15 - (3-4.2.2.2(c)(8)(i)): Reject SUBMITTER: Saul Aronow, Technology in Medicine, Inc. COMMENT ON PROPOSAL NO,: 99-86 RECOMMENDATION: Delete 3-4.2.2.2(c)(8)(i) entirely and adjust numbering of following clauses. SUBSTANTIATION:: ]. The substantiation (1) of the proposal is correct. The term "acute care b~d" is not defined. By the same token, "general care bed" is not defined either. Both terms were dropped in earl ier editions because of controversies over grounding, isolated power, and other issues not germane to this section. It.should be noted that the concept of acute care beds vs. general care beds is a real i ty of hospital function, and does in fact appear i,n other parts of NFPA-99, for example 4-8.1.1.1 and 3-5.2.2.2. However the terminology is not the issue. II
2. The rationale of 3-4.2.2.2 is to l imi t the load on the Emergency system to only those purposes for which i t is essential to maintain power. The concept is that a smaller system can be made more reliable than a larger system. For this reason i t was very specifically intended that every bed in the hospital need not be provided with receptacles or l ighting from the Emergency system because most patients could tolerate a temporary loss of power, or that other solutions would be found. I t should be noted that 3-4.2.2.2(c)(3)i(iv) and 3-4.2.2.2(c)(4) already make provision for special areas.
103
COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: I. With increase demand fo r e lect r ica l equipment in any patient care area, Subcommittee on Electr ical Systems believes that provisions for at least one duplex receptacle/bedroom to be wired fo r emergency power should be made. This proposed requirement applies only to new construction.
2. With "swing use" of beds now more possible, having at least one duplex receptacle on emergency power c i r cu i t w i l l eliminate need to have such a receptacle insta l led i f a change in room u t i l i z a t i o n would require a receptacle in the room to be on emergency power.
(Log #17) 99 - 16 - (3-4.3.3.6): Hold For Further Study SUBMITTER: Saul Aronow, Technology in Medicine, Inc. COMMENT ON PROPOSAL NO.: 99-95 RECOMMENDATION: In the second sentence of Proposal 99-95, change "corresponding to at least the tota l hazard current at the nominal voltage" to "corresponding to a tota l hazard current of 5.0 milliamperes at the nominal l ine voltage, or to a lesser alarm hazard current i f the l lne iso la t ion monitor is so rated." SUBSTANTIATION: I. The proposal wording misinterprets the meaning of "hazard current", and would allow the test to run at any value of hazard current. The revision makes provision for the usual 5.0 mA LIM or a lesser value rat ing.
2. The proposal was o r i g ina l l y intended for NEC 517, which lacks a corresponding section in the LIM discussion. That is why i t appears redundant in 99. COMMITTEE ACTION: Hold For Further Study. COMMITTEE STATEMENT: I. Paragraph 3-4.3.3.6 applies only to test switch for test purposes. Actual value of alarming is set by 3-4.3.3.2 and 3-4.3.3.4.
2. I t appears that manufacturers set the 5.0 ma test switch t r i p - l eve l at 15 percent below nominal voltage level . Consequently, the t r i p level at higher voltages (nominal 15 percent to 10 percent) w i l l be higher. The Subcommittee on Electr lcal Systems needs to study an acceptable current range for voltages involved.
[This issue was extensively discussed at May 8, 1989 meeting of Subcommittee on Electr ical Systems.]
(Log #49) 99 - 17 - (Chapter 4): Reject SUBMITTER: D.A. McWhinnie, Hickory H i l l s , I l l COMMENT ON PROPOSAL NO.: 99-103, 104 RECOMMENDATION: Delete "Gas and Vacuum Systems".
Add "Chapter xx Vacuum Systems". SUBSTANTIATION: This issue, and that of " tex t " ( in a separate public comment), are now in abeyance by the Board and Standards Council due to the "revis ion cycle," and as suggested by NFPA Associate General Counsel:
(a) In 1971 the Committee on Hospitals rejected proposals to combine gases with vacuum.
(b) At the ANSI Hearing on this issue the Technical Committee, representing the Standards Council, succeeded in defeating a proposal (to ANSI) to combine Vacuum and Gases; and acted to publish a separate document on Vacuum (56K).
(c) In 1982 the Standards Council action maintained Vacuum as a separate document, with the same (as ' current) Substantiation on f i l e .
(d) The NFPA Code 99 project mandated 56 series documents to be incorporated into 99 "as is" ~nd "without change" ( in the record).
(e) Neither of the affected Subcommittees were represented on the Technical Committee "restructur ing" ad hoc.
( f ) The Technical Committee provided no substantiation other than a " fee l ing" fo r combining two fundamentally disparate technologies.
(g) The Vacuum Subcommittee noted against combining gases and vacuum in one chapter.
(h) The Standards Council 's Secretary's in terpretat ion is that two Regulations (10-I0(c) and 10-11) are to be interpreted " l l t e r a l l y . " By reference 11-10 also applies.
( i ) D iscount ing unstated q u a l l f i e r s in NFPA Regulat ions (which woutd devalue them a l l to a pick and choose gamble) o thers ( than (h) above) a lso apply.
( j ) The Regulat ions c i ted throughout t h i s process are c l ea r , concise, understandable and apply " l i t e r a l l y . " Even wi th i n t e r j e c t i o n o f an unstated q u a l i f i e r the f ramer ' s i n t e n t ( requested and awai t ing rep ly ) remains eminent ly c l ea r .
(k) As the unstated q u a l i f i e r has been in the record since '86, and has not been va l i da ted by i nc l us i on in '88 Part VI I Regu la t lons , and the "has been i n t e r p r e t e d " precedent (see (a ) , (b ) , and (c) above) has been invoked, i t can only be assumed tha t a l l c i ted regu la t i ons are to be i n t e r p r e t e d l i t e r a l l y .
( l ) The Technical Committee agreed to "s tand-a lone chapters" (Osborne, '86 TCR, Log 7) .
(m) The Technical Committee "recommended tha t the two systems be separated . . . " (May, '87)
(n) The Technical Committee ad hoc advised that separa t ion by chapter "was p o s s i b l e . "
(o) Other proposals f o r separate chapters inc lude B.R. Keuhn (Pres . , C.G.A.) '86 TCD~Log 30; S.D. Kahn, l e t t e r 2/13/87.
(p) In t h i s 1988 r e v i s i o n cycle the need f o r separa t ion is evidenced by Logs 23, 43, 44, 45 and 46. [Proposals 99-105, 99-106, 99-109, 99-108, and 99-167, r e s p e c t i v e l y in the TCR.]
(q) A separa t ion [ (p ) above] which leaves 20 pages and 300+ paragraphs o f one technology, separa t ing requirements o f an oppos i te ( i n t h i s contex t ) technology, is unacceptable, and s t i l l combines " i n the mind" (Webster 's N.W.D., 1980) o f the user two l i f e - s u p p o r t s p e c i a l t i e s which have t o t a l l y d i f f e r e n t requirements from source to the l a s t p a t i e n t te rmina l . Several examples o f such combining " i n the mind" are evidenced by ac tua l , and cu r ren t , A/E con t rac t s p e c i f i c a t i o n s where the confus ion is ev ident ( a l l in the Technical Committee and Subcommittee f i l e s ) . The ob jec t o f t o t a l separa t ion , by document as ex is ted before NFPA 99-1984, i s to minimize, i f not e l im ina te , t h i s confus ion and poss lb le m i s i n t e r p r e t a t i o n , e s p e c i a l l y f o r " those less f a m i l l a r . " The Heal th Care F a c i l i t y can be the l o s e r , i f not the p a t i e n t (see the annals o f l i t i g a t i o n ) .
Among the app l i cab le NFPA regu la t i ons are the f o l l o w i n g :
NFPA Regula t ions , Part VI, contravened: L is ted below are c e r t a i n app l i cab le NFPA Regulat ions: 1. 10-3 Shal l be based on " . . . research data,
eng ineer ing fundamentals . . . " 2. 10-10(c) "a statement o f the problem and
s u b s t a n t i a t i o n f o r Proposal . . . " 3. 10-11 ( r equ i r es compliance wi th "10-10(b) , (c)
and (d) . . . " ) 4. l l - 9 ( b ) " t h a t . . . ra ises a quest ion on
mater ia l which is e i t h e r new or p_jEp_p_q~_~dd . . . or is a f f e c t e d . . . " (underscores added)
11-9(c) "would chanoe the t e x t . . . Technical Committee . . . would have to restudy the t e x t . . . or o ther " a f f e c t e d " par ts . . . " (underscores added)
The ac t ions on t h i s issue " a f f e c t " two documents. (See 4/28/88 l e t t e r from J.S. Halek, Ph.D., OePaul U n i v e r s i t y , and S. Malcom, AAAS, August 1988, which are a v a i l a b l e f o r review at NFPA Headquarters)
11-g(e) " . . . would requ i re cons iderab le research and d iscuss ion by the Technical Committee . . . "
Ne i the r was done by the Technical Committee nor i t s ad hoc Res t ruc tu r ing group. The only known research was done in the Vacuum Subcommittee, which voted heavily against these actions, and which appears throughout in the correspondence, in the forced (because of the lack of discussion 7/I/86) "perspective" w/coverlng l e t t e r , and the Fall '86 TCR and TCD.
"5. 11-10 " . . . shall include a statement, preferably technical in nature, on the reason for the Technical Committee action. Such statement shall be su f f i c i en t l y detai led so as to convey the Committee's rat ionale for i t s action . . . to the Association for consideration."
Although asked from the f l o o r of the November '86 Association Fall Meeting, answers to purpose ( t ranscr ip t pg. 40, l ine 2 and rat ionale were never provided. (See Section I above, paragraphs I, 8 and 9.) Eight pages of the Fall '86 t ranscr ipt cover purpose, rat ionale, technical questions and
104

i! . !
technical examples: (pg. 35 to 38 line 10, 48 to 50 line 2, and 52 to 53 line 18). None of those points were addressed during the two-year process, nor in response to the Association Chairman (transcript 38-11).
Examples - partial l l s t . (Other:; are detailed in July '86 'Perspective" scenario.)
All of the following changes of text, or which "affect" text (Regulations 11-9(b), and II-9(c) above) are improper, and were never discu:~sed, intended or approved by (at least) one of the responsible technical Subcommittee's - Vacuum. They were made by the Technical Committee Restructuring .~d hoc and wi l l lead to misinterpretation, inadvertent ,grrors, confusion and possible hazardous Code violations by "less familiar users" (Appeal Item I I ) . This includes A/E designers, installers and AJHs (the principal users) - where
misunderstandings and errors can, and have led to tragedy. Very few A/Es and proportionally fewer installers, ever do more than one medical gas or vacuum project in their entire careers (F.W. Dodge Reports).
Chapter 4 contains many more changes of text, and "affect" context, than the twenty-eight +/- l isted below:
,99 '87 ~ 9 _ ~ (4-10.2.].1) removed 6-2.1
(4-9.1.3.3) removed 6-3.1.2
(4 -8 . ] . 1 .2 ) removed 6-3.2
(4-7.1.Z) inserted 6-6.2.3
z)
(4-7.1.2.1) inserted 6-6.2.3. i
4-I0.4.1.I removed 6-3.2.7*
(4-8.1.I.3(e) deleted- altered- removed
From 4-7.1.I where i t is essential for the preplanning phase of any construction project.
Pump cr i ter ia from pump section (Appeal IX, para. 2).
From i ts proper location for A/E designers and, particularly, installers.
Incredible - between pumps and piping? under "Patient Vacuum Source" and "Medical- Surgical"? I t is neither. This is an environmental system no__t_t for "Patient" suction (see NFPA HCF Handbook, '84 and '87), and belongs where placed by the responsible S/C. (Appeal VII I , para.
6-3.3.5*
(4-I0.4.1.3) deleted 6-3.3.6*
In contractor equipment and installation section - from S/C intended location.
From systems' design and instal lat ion section, a requirement essential for A/E designers and, more importantly, installers.
Text and i l lustrat ion, and intended context, c r i t i ca l l y altering the content.
Entirely from design, system components and installation sections - an insipient action.
(4-8.1.I.4(a) deleted- altered 6-3.4.1" removed
(4-10.4.1.5) removed 6-4.3.3*
deleted
- !,
6-5**
deleted 6-5.3 **
(4-8 .1 .1 .8) removed 6-5.1.1 (4 -9 . ] . 2 ,1 ) removed 6-5.1.2" (4-9.1.2.2) removed 6-5.1.3"
Text and i11ustration and context; c r i t i ca l l y altering the intended content.
From Systems' design and installation section, a requirement essential for A/E designers, and, more importantly, installers.
More incredible - a crucial section heading, c r i t i ca l l y essential for designers, system safety and especially installers. ~ A/Es specify, only - installation shall be in s t r ic t accordance with NFPA No. " , and installers'l~]w_B3~ need clear and concise "Installation" guidelines. They are responsible for Code compliance and, unfortunately, make most of the potentially hazardous ~errors. This de le t ion , constant ly denied by the T/C as being a " techn ica l " change, is glaringly inconsistent with 4-4.1.4! Why? (Appeal VII I , para. 3).
Same note. as 6-5 (last above)' applies. A number of different types of tests are required, and the unapproved (by the responsible S/C) deletion of this qua]if ier by the T/C destroys the intended context, and adds "confusion" (persistently denied by the T/C and i ts ad hocs)..
From "Installation . . ." (see 6-5 above), deleted by T/C action, essential requirements for the instal l ing contractor.
(4-9.1.4.1) removed 6-5.3.2 Last note above (4-9.1.2.3) removed 6-5;3.3 applies.
* (Appeal Item IX, paragraph 3.) ** (Appeal Item VIII , paragraph 3.)
The following additional changes made to the Association approved NFPA 99 '84 by the Restructuring ad hoc group are of major dimension, and include the creation, insertion, addition and improper location of v i ta l material. Neither intended, discussed, nor approved by the Subcommittee these changes have resulted in the virtual decimation of the approved context and clar i ty:
105

_9_9_.L_B]_
4-8• 1 . I
4-9
4-9.1.4
4-I0.2.1.I
4-10.4.1.1
4-10•2.1.2 4-10.4.1.3 4-10.4•1.4
Created and added a section heading neither intended nor log ica l , combining f ish with fowl; piping ins ta l la t ion methods and techniques - with - f inished, outside purchased, e lec t r ica l and mechanical devices and systems.
Created and added a major section heading combining two very broad and var iant aspects of the construction procedure, and includes at least three ins ta l la t ion methods and techniques which are t o t a l l y unrelated to the t i t l e .
Created and inserted a heading which is ambiguous, too broad and deletes the intended heading and i ts q u a l i f i e r (99 '84, 6-5.3). I t also deletes four steps required in this section (99 '84, 6-5.3.3, 5, 6 and 9).
Inserted text improperly in a section which is intended for the f a c i l i t y a f te r construction is completed and systems are "on stream" for patient use - as is evident by the context of i t s six fol lowing paragraphs (4-10•2.1.2 through 4-I0.2.1.7) - only pertaining to proper operation and maintenance during i t s useful l i f e .
This is upfront information, intended only fo r the pre-plannlng group, and belongs only where placed by the Vacuum Subcommittee (6-2.1).
A heading and section inserted improperly (as 4-10.2.1.I las t above)• This is a crucial reoulrement intended for A/E designers, and esoecial lv ins ta l le rs , before cei l ings are ins ta l led, or walls, par t i t ions , crawl spaces, pipe shafts and chases are closed, and does NOT belong in a section intended for use only a f te r
• systems are ce r t i f i ed for patient therapy. This misjudgment has already resulted (which can be guaranteed to continue) in oversight (del iberate in some cases). Why should a plumber or p i p e - f l t t e r contractor read 99-87, 4-10??
Inserted, and do not belong in 4-10 (see last two notes above.)
4-I0.4.1•4 Created and added a sentence not in the Association approved 99 '84.
4-I0.4.1.5 Inserted unreasoningly. (See note nn 4-10.4.1.1 above.)
The above changes resul t in a synergist ic negative ef fect on the qual i ty of l i fe -suppor t systems and the optimum of patient care. They overlook the needs for accuracy and c l a r i t y of the most important (and most often inexperienced) users - the i ns ta l l e r who, by A/E contract documents, must "comply s t r i c t l y in accordance with NFPA Code 99."
The very actions of the Standards Council i t s e l f (San Diego, Jan., 1988) are also basic to the substance of this issue, (underscores added):
87-46(b) (To provide) " . . . formal explanations of the me__e_a_D_Ln_q or ~ of anv specif ic
or provisions of any document."
88-2 ~ the complaint " . . . because the Committee did no~ provide statements of su f f i c ien t detai l so as to convej( the Committee's ~ for i ts actions • • . , I
To date neither of the above c r i t e r i a , among others, have been complled with, although asked numerous times in wri t ing and: at the Technical Committee meeting 7/I /86; by the Chairman of the Associations Fall '86 Meeting ( t ranscr ipt pg. 38, l ines 11-13); and by an experienced and qual i f ied guest at the Technical Committee ad hoc meeting on 5/11/87• (At that ad hoc meeting i t was "querried as to problems in separating material into two chapters?") The answer was " e d i t o r i a l l y i t was possible".
Not only was such "separation . . . possible", but as these "d i f fe ren t technologies" (Technical Committees and i t s ad hoc's words) had existed successfully for over 33 years, including at least twice by Standards Council decision, and with no "problem" ever stated over those years, or even now.
The questions of purpose, problem or substantiation not only remain unanswered, but they have not even been acknowledged, including at the Fall '86 Meeting when asked by the Association Chairman.
By anyone's logic, and the l i t e r a l and clear meaning of NFPA's "Form For Proposals . . . item 4" the "Statement of rP_~p_b_]_~ and Sqb~tantiation . • ." are reouirements (underscores added), as they are also reoulrements for negative votes or abstentions in NFPA l e t t e r bal lots•
NFPA Regulations: 1. 10-3 covered at length above. Reference to "The
number and type of documents" was never, and is not now, at issue. The language is clear, concise, and without a single qual i fy ing word. The issue is "technical" per the Technical Committee and i t s ad hoc, repeatedly, in the record of correspondence, minutes and the Association Fall '86 t ranscr ipt• The "affected" (from the Regulations) Documents are "d i f fe ren t " and "separate" - "technologies" and "have d i f fe ren t requirements" per the Technical Committee and i ts ad hoc, and reauirements have been changed (per Comment I-A Examples, and under "cutt ing-up" process above, as well as the July '86 Perspective).
2. I0-I0(c) and 10-11 are " interpreted l i t e r a l l y " and "require" - "must state" the "problem", "substantiat ion" and "why". Without a single qual i fy ing term, they have c lear ly been violated• No "problem" has ever been "stated", no "why" has ever been answered, and i f "format" is claimed as "substant iat ion" i ts facetious and untrue. The arguments proving the hollowness of that contention have never been answered.
11-10 As in I0-3 (item I above) the language is clear, concise and without a single qua l i f i ca t ion leaving only a " l i t e r a l " in terpreta t ion. Further, the
"reason fo r the Technical Committee action • • . su f f i c i en t l y detai led so as to convey the committee's rat ionale for i t s action . . ." is in consummate accord with the Standards Council 's Dockets 87-46(b) and 88-2, January, 1988.
Regulation 11-10 wording, in quotes above, is equivalent to 10-I0(c) - which is also a requirement of 10-11 (by reference). Your l e t t e r states.10-10(c), item 2 above, and 10-11 have been interpreted " l i t e r a l l y " • Because i t is the same requirement as lO-lO(c), the 7th paragraph of 11-I0 is also a requirement to be interpreted l i t e r a l l y .
Therefore, the complaint and Appeal posit ion that Regulations have been violated are, in fact, true - based upon your personal opinion and interpretat ions - as to 10-10(c), I0 - I I and 11-10.
1 0 6

American Association for the Advancement of Science, August, 1988.
" text" def in i t ion: Dr. S. Malcom states; "without the r ight subject in
the right sequence . . . technical l i teracy is affected* (and), i f not in sequence the project is poorly organized and essentiallyhandicapped."
*See "affects" in NFPA Regulations (at least twice in 11-9). Also see pertinent documentation in 12/7/86 complaint, 2/14/87 appeal, and 5/I0/88 le t te r and attachments to Mr. Joseph E. Johnson.
Essential to this issue and in the record since 1984, this topic has been consistently.ignored by the Technical Committee, i ts restructuring ad hoc, and review ad hoc.
• Webster's Random House, and Oxford English Language Dictionaries:
"A structure formed by words, phrases, sentences and paragraphs - and their order as written . . ."
"Original language as opposed to a translation or rendering."
"The very words, sentences and sections in their order."
"Connected writ ing in i ts developed form and structure."
That "cutting-up" process: I. has removed NFPA 99-'84, 6-2.1 requirements from
the orientation and advisory section up-front where i t is necessary for planners and A/E designers information hefore construction budgeting and preliminary sketching are begun.
2. has removed A/E designers' requirements (wording designed and clearly intended for them) and made them the responsibi l i ty of the f a c i l i t y administration (99-'87, 4- I0.2.1. I ) . "Administration", contrary to the Vacuum Subcommittee intent, now includes responsibi l i ty intended for systems' designers. However, designers need not, nor should they be expected to, refer to a section at the end of the document which obviously doesn't apply to them - and many wi l l not.
3. has removed essential informa.tion (99-'84, 6-1.1) from Vacuum Systems, and placed i t 19 pages and more than 300 paragraphs away from the Vacuum document - with only gas systems requirements in between. Vacuum systems designers who check 99 contents wi l l miss i t ent i re ly.
This is only one example which disproves the ad hoc 5/17/87 claim that "any ambiguity" (underscore added) has been "eliminated" (minutes item 4-6). There are others - too long to l l s t here.
4. has deleted the only proper, and Subcommittee intended, 99-'84, 6-5 " Instal lat ior l of Piping System." (The best, and most meaningful, caption for design and construction documents, and especi~Llly for the requirements which i t covers); and created and added a to ta l l y inappropriate and misleading substitute heading (99-'8?, 4-9).
The explanation for this deletion was - "necessary because of format" is inane and contradictory, considering that the crucial caption, " . . . Insta l lat ion . . ." (improperly deleted from the Vacuum document), has been inserted in the Gases document - twice!
5. has removed an essential requirement (99-'84, 6-5.1.I) from 99-'84, 6-5*, last above, and placed i t in a section intended for, and l imited to, l ine components (99-'8?, 4-8.1.I) which has nothi~l to do with ins ta l le r methods.
*(The requirement removed belongs; "technical ly" under 99-'84, 6-5 which was deleted by the Technical Committee - per item 4, last above.)
!! ,i i ii i II '
6. has deleted from 99-'84 designer and ins ta l ler Section 6-3: pa~t'of 6-3.3.5, and al l of 6-3.3.6, 6-3.4 and 6-3.4.1, al l requirements for systems designers and instal lers.
7. has, as in 2 above, made what are properly, and intended to be, manufacturer and ins ta l le r requirements, now the responslbi l i ty, of the f a c i l i t y administration (99-'87, 4-I0~4.1.1 through 4- I0 .4.1.5) . .Fur ther , i t would be v i r t ua l l y impossible for the " f a c i l i t y administration" to perform these insta l la t ion requirements in any type of completed construction. (See 4-I0.4.1.I in Part I I I of Comment I-A.
8. has deleted 99 '84, 6-5.3 "Acceptance Testing." and seriously altered the Subcommittees intended "testing" Sections 6-5.3.4 through 6-5.3.9.
See Part I I I of Comment I-A for approximately two dozen more such changes of text , deletions, additions and c r i t i ca l alterations which ser ious ly " ff~_~Le_¢_~" text, per Regulations 11-9(b), 11-9(c) and l l -9 (e) .
"Rearranging" the pieces of a jigsaw puzzle, although the exact same size and shape, grossly "affects" (Regs. l l -9(b) and (c)), changes, the " text " - colori pattern, le t ters, digi ts, ! i l ines - and more importantly i ts meaning, the impression and interpretat ion o f ! i t s viewer, and i ts designer's intent. COMMITTEE ACTION~ Reject. COMMITTEE STATEMENT: I. Steps have been taken to improve usefulness of restructured document with respect to Chapter 4 ( i . e . , Proposals 99-I05, 99-I00, 99-108 in TCR). Each type of.system (gas, vacuum) is now clearly indicated as a result of changes from proposals in TCR.
2. The fundamentals of construction andtest ing of gas and vacuum systems (e.g., .pipes, alarms, purging) are similar. I t . i s thus technically acceptable to place both in one chapter, as long as each type is ident i f ied.
3. Arguments of 1971 are not appropriate today since at that time a l l ,heal th care documents were separate. Combining of individual documents into one document was a new and di f ferent step. Arguments in 1971 related to NFPA 56K and a CGA document on medical-surgical vacuum systems.
4. Operation and maintenance practices consider both systems, as "medical piping systems," and look for testing c r i te r ia for both in one area of document. Where differences exist , they are clearly delineated.
5. Action of Proposal 99-105 in TCR has removed some remaining ambiguities without compromising the . insta l la t ion, maintenance and testing of each system.
6. Reorder of text without changing c r i te r ia or intent is not considered a technical change. Thus, NFPA "Regulations Governing Committee Projects" have not been violated.
7. Restructuring of text has occurred for a number of other formerly separate health care documents.(e.g., NFPA 56A, 56G, 76A, 76B). No allegations of changes in intent have been reported to the Technical Committee.
8. Scopes have been placed at the beginning oF each chapter. Chapter 4 covers al l "medical piping systems".
9. Technical Committees have the r ight to arrange text anyway they deem appropriate. 10. Problems with d i f ferent ia t ing between gas and
vacuum systems have not been reported to the Chairman nor most members of the Committee, nor to NFPA staff .
I I . In restructuring of NFPA 99 for 1987, no text was deleted, and no change of intent was made.
12. Issue of structure of Chapter 4, as well as al l of NFPA 99, has been given serious consideration by Subcommittee on Restructuring, by Technical Committee on Health Care Fac i l i t ies , by public (through review of TCR for 1986 Fall Meeting, TCD for. 1986 Fall Meeting, TCR for 1989 Fall Meeting), by NFPA Association members at 1986 Fall Meeting, by NFPA Standards Council in reviewing complaints, by NFPA Board of Directors in reviewing appeals, and by Subcommittee on Structure of Chapter 4.
[This issue was again extensively discussed by Subcommittee on Nonflammable Medical Piped Gas Systems at i ts Hay 3, 1989 meeting, by Subcommittee on Vacuum Systems at i ts May 4, 1989 meeting, andby Technical Committee on Health Care Fac i l i t ies at i ts June 19/20, 1989 meeting.]
107

(Log #50) 99 - 18 - (Chapter 4): Reject ~ : D.A. McWhinnie, Hickory Hil ls, I l l COMMENT ON PROPOSAL NO.: 99-103, 104 RECOMMENDATION: Create new Chapter for Vacuum, and relocate 4-I.4 and 4-2.2 to proposed new "Chapter xx", and number accordingly.
In 4-1.4, 5th line add (after "apply to")"WAGD or to".
In proposed new Chapter add t i t l e "Vacuum Central Piping Systems", and "Medical Surgical".
Delete present 4-7, 4-7.1, and 4-7.1.1. Insert "Scope" (from present 4-1.4), and "Hazards"
(from present 4-2.2). Insert "General" (from present 4-10.2.1.I). Insert present 4-9.1.3.3. Renumber al l above accordingly. Under 4-10 "Admlnlstrati'on" refer user back to newly
numbered "General", and relocated (new number) "Minimum Vacuum and Oper. Range".
This is a universal, and commonly accepted format, and in accordance with AIA and M.E, practices - giving the user the latitude and ground rules up-front, where they belong for an overview/perspectlve of the details and requirements which follow. SUBSTANTIATION: I t is this Submitter's opinion that several NFPA Regulations have been contravened; and A.E. Cote's~"personal opinion" that several are to be interpreted " l i t e ra l l y " (6-7-88). Other Regulations which should (based upon obvious intent) apply have been couched on the basis of an unspoken qual i f ier, and are now in abeyance due to the "revision cycle". The trouble with an unspoken qual i f ier is that al l Regulations are le f t in doubt - leaving an impossible choice - pick and choose situation. Those upon which my contentions are based are attached to "Comment Chapter 4, Log #49" [Comment 99-17].
The Technical Committee commitment was to maintain the Subcommittee documents "as is" and "without change" (confirmed in writing). The Subcommittee's did not combine their documents, nor make any of the many changes of text.
The Technical Committee also agreed to keep the documents separate in "stand alone chapter(s)" [B.W. Osborne, '86 TCR, Proposal 99-4, Log #7].
The "review" ad hoc members, 75 percent from the restructuring ad hoc, were advised that the "Technical Committee members recommended that the two systems be separated . . ."
Contrary to i ts statement [Denver, Nov., '86 transcript] the Technical Committee did not review [July I, '86] or discuss the issues of text or chapter separation precipitating the July, '86 "Perspectlve/Scenario".
However, without a stated reason as to "Problem" "Purpose", or "Substantiation" the two disparate (acknowledged) chapters were combined; the only Substantiation being a "feeling" in the restructuring ad hoc.
After the fact (Nov. '86 meeting), the Technical Committee contradicted i ts earl ier stand (much too late) and conceded that the affected chapters were "different technologies" and had "different requirements" (in the record).
When the questions of Substantiation (NFPA Regulations) on the floor, and then were asked by the Assn. Chairman (November '86 transcript) there was no response.
Instead, the Assocation was promised a "review" ad hoc would "restudy" the issue. When the same question of separate chapters was put before the review ad hoc the answer " i t was possible". The question was from a guest, and there was no discussion of substantiation, 9~ the matter of the many distortions of text (many in the July, '86 record). The only recommendation of the review ad hoc was the addition of a single word and some spacing.
On the basis of this Submitter's proposal; the Vacuum Subcommittee vote; S.D. Kahn let ter 2/13/87; B.W. Osborne, Proposal 99-4 (Log 7) TCR '86; B.R. Kuehn (CGA), Comment 99-35 (Log 30) TCD '86; and TCR '89, Logs 23, 43, 44, 45 and 46 [Proposals 99-105, 99-106, 99-109, 99-108 and 99-167 respectively in TCR] - - i t is clear that to maintain separate documents (as had existed successfully for over 35 years) were not only proper, but are now the intent (TCR '89) of the Technical Committee - - but not wholeheartedly.
To leave only two small paragraphs of essential Vacuum text (4-1.4 and 4-2.2) 20 pages and over 300 paragraphs away from the Vacuum requirements - - separated by the text of an entirely different technology (opposite in this context) is unthinking can result in vacuum system designers, installers and others missing the basic up-front material - - especially those using the table of contents (being directed past that information), and "those less familiar", of whom there are very many, and for whom these documents must be meticulously clear.
The issue is complex as are the two technologies affected. This proposal for separate chapters, and those listed above, are for nothing more than has proved successful, and eminently effective for many, many years.
Substantiation of this comment includes that of Comment 99-17, (Log #4g). C_~_MMITTEE ACTION: Reject. COMMITTEE STATEMENT: See Committee Statement for Comment 99-17 since i t is applicable for this comment as well.
(Log #51) 99 - 19 - (Chapter 4): Reject SUBMITTER: D.A, McWhinnie, Hickory Hi l ls, I I I qOMMENT ON pROPOSAL NO.: 99-103, 104 RECOMMENDATION: Rearrange text sequence per May 2, '88 Comment I-A, 3, 4 and 5 and Perspective/Scenario, July, '86. SUBSTANTIATION: As the Technical Committee Mandate for NFPA 99 was to restructure, keeping the documents "as is and without change", the Subcommittees had no reason for concern:
(a) The Subcommittees, on that basis, were not represented on the Technical Committee ad hoc, and fel t no need to be.
(b) Objections/negative notes were made on all drafts.
(c) All text changes were made by the Technical Committee ad hoc.
(d) The vacuum Subcommittee voted heavily against approval of the "restructured" text.
(e) The Technical Committee repeatedly denied that the text was changed, and contended throughout the process, including at the November '86 Assn. Meeting, that al l changes of text by the Technical Committee ad hoc were necessary for "format".
(f) The rebuttal of these positions, with valid technical substantiation, is in the record and the Denver, '86 transcript.
(g) Contravention of several NFPA Regulations are cited in the process, two of which the Standards Council Secretary opines are to be interpreted l i t e ra l l y . By reference, at least one other would apply.
(h) Standards Council actions 87-46(b), 88-2 and 88-38, among others, would also apply.
( i) The Perspective/Scenario of July, '86, in the Technical Committee f i le , includes only a partial I s i t of major alterations of text.
( j) None of the objections/technical substantiations have been challenged or even discussed, including at the July '86 Technical Committee meeting forced the July '86 Perspectlve/Scenarlo.
The proper definitions of "text" ("cutting-up") process, and rearrangement of "text" in this proposal, are on f i l e and remain unaddressed.
Substantiation of this Comment includes that of Comment 99-17, (Log #49).
American Association for the Advancement of Science, August, 1988.
"text" definit ion: Dr. S. Malcom states; "without the right subject in
the right sequence . . . technical l i teracy is affected* (and), i f not in sequence the project is poorly organized and essentially handicapped."
*See '~affects" in NFPA Regulations (at least twice in 11-9). Also see pertinent documentation in 12/7/86 complaint, 2/14/87 appeal, and 5/10/88 let ter and attachments to Mr. Joseph E. Johnson.
Essential to this issue and in the record since 1984, this topic has been consistently ignored by the Technical Committee, i ts restructuring ad hoc, and review ad hoc.
108
Webster's Random House, and Oxford English Language Dictionaries:
"A structure formed by words, phrases, sentences and paragraphs - and their order as written . . ."
"Original language as opposed to .~ translation or rendering."
"The very words, sentences and sections in their order."
"Connected writ ing in i ts developed form and structure." COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: See Committee Statement for Comment 99-11 since i t is applicable here as well.
(Log #52) 99 - 20 - (Chapter 4): Reject S B M ~ R : D.A. McWhinnie, Hickory H i l l s , I l l COMMENT ON PROPOSAL NO.: 99-104 RECOMMENDATION: Provide "Separate Form(s) for Each Proposal" (change) made in 99, '87, Chapter 4 (a]though admittedly after the fact). SUBSTANTIATION: NFPA Regulations I0-I0(c) and lO-l l are violated, per this proponent and Standards Council Secretary (6-7-88); as was 11-10 by reference; and which "have been interpreted l i t e r a l l y " by the Standards Council.
"Committee Statement", Log 127 [Proposal 99-I03 in TCR], is pa r t ia l l y correct in that the above is not within the Subcommittee Scope - - or responsibi l i ty - - as the Subcommittee did not make the many changes to "te__e~_~". The changes were made by the Technical Committee ad hoc, usurping the Subcommittees, and assuming their responsibi l i ty; making the "Committee Statement", Log 127, wrong as to "not leaving" the Subcommittees.
"Committee Statement", Log 128 [Proposal 99-I04 in TCR], is wrong also. "Proposal 9g-105 (Log 23)" covered only the integration of Health Care Fac i l i t ies documents into Code 99, and not to combine fundamentally diverse.documents, or to a l ter their " texts". I f so there would be no need for Subcommittees. (See Malek and Malcom below.) This "Committee Statement" ignores the fact that "comment on proposed structure" was made, since 1982 on both structure and " tex t " , and that the Subcommittee did "comment" by voting heavily against that structure (not against the concept of 99, one document). I t also ignores the fact of the '86 Perspective/Scenario (July '86) which had irrefutable technical "Substantiations" (required by NFPA Regulations) opposing the many technical changes of " tex t " none of which was substantiated. This proposal repeats those many technical objections, seeks val id substantiation for the technical changes of " text" and Technical Committee rebuttal of proponent's substantiations.
Action within Vacuum Subcommittee (June '88) is only a small step, indicating the distort ion of " tex t " .
Substantiations ~ on a "Separate Form for Each Proposal"; also r _ _ e ~ for negative and abstain votes on le t te r bal lots; have not been provided on the following (only a part ia l l i s t ) , which includes the effect of the "cutting-up" of " tex t " .
Standards Council Actions (underscores added): I. 87-46(b) (to provide) " . . . formal explanations
of the ~ or intent of ~ specific provision or provisions of n an_£ document."*
2. Upheld the complaint " . . . because the Committee did not provide statements of suf f ic ient detail so as to convey the Committee's rationale for i ts actions
* Of well over two dozen s__pecific changes ("provisions") none had any substantiation ("meaning" - " intent") except "necessary for format" - - the disproof of that statement unanswered. ** The only "rat ionale" in the record for the i n i t i a l action of combining in one chapter disparate technologies (opposite in this context) is "a feel ing", lacking any detail vs. "suf f ic ient detail . . . to convey . . ." ( l . above). Was not that action a "specif ic provision" (No. l above)?
This substantiation includes that of Comment g9-17 (Log #49).
ii
ii
COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: See Committee Statement !'for Comment 99-17 since i t is applicable here as well.
i
(Log #72') 99 - 21 - (4-3.1, 15-3.4.1): Accept ~ : Leo G. Foxwell, The Hartford Insurance Group COMMENT ON PROPOSAL NO.: 99-122 RECOMMENDATION: In Figure 4-3.1.5, 4-3.1.6, 4-3LI.7, 4-3.1.9 and 4-3.1.10.I add "Type I Systems" to end of caption.
In 15-3.4.1 in sentence 1, change "Section 4.3 through 4-6" to read "4-3.2, 4-4.2, 4-5.2, 4-6". SUBSTANTIATION: iEditor ial . Confusion in f ie ld in applying Type I Requirements to f a c i l i t i e s that are Type I I . COMMITTEE ACTION: Accept.
(Log #71) 99 - 22 - (4-3.1.2.3.1 (New)): Accept in Principle SUBMITTER: Leo G. Foxwell, The Hartford Insurance Group COMMENT ON PROPOSAL NO.: 99-118 RECOMMENDATION: Reject present Committee Action on Proposal 99-118 and add new 4-3.1.2.3.1 to read:
4-3.1.2.3.1 Where the location of the supply system door opens into an ex i t corridor, the requirements of paragraph 4-3.1.2.2(c) and 4-3.1.2.2(d) shall be complied with. SUBSTANTIATION: 1. This paragraph is under the jur isd ic t ion of the Subcommittee on Nonflammable Medical Piped Gas Systems and should be acted on by them, not the Anesthesia Subcommittee.
2. The need for vent i la t ion storage systems under 2000 c u f t is needed. The need is in al l applications such as dentistry, medical off ices, nursing homes - not just anesthesia suites. The more appropriate action in complying with the Life Safety Code is to have a l hour rated enclosure and outside venting not no venting. COMMITTEE ACTION: Accept in Principle.
1. Revise 4-3.1.2.3 to read: 4-3.1.2.3 Additional Storage Requirements ~or
Nonflammable Gases ~ Than 2000 c u f t (57 m~). Where the location of the supply system door opens onto an ex i t access corridor, (a) the requirements of 4-3.1.2.2(c) and 4-3.1.2.2(d) shall be complied with; or (b) the door shall have louver opening(s) with a minimum of 72 sq in. in total free area, and with f i re damper(s) of appropriate rating; or (c) the wall of t h e location shall be provided with a ~ouver openlng(s) with a minimum of 72 sq in. (.05 m c) in total free area, and with f i re damper(s) of appropriate rating.
2. Revise A-4-3.2.2.1 by adding the following at the end of the paragraph:
" I f the door to the enclosure opens onto an ex i t access corridor, see 4-3.2.2." COMMITTEE STATEMENT: 1. Mechanical vent i lat ion is not practical in a l l situations. Addition of methods (b) and (c) provide alternat ive methods of vent i lat ion of room while s t i l l meeting requirements of NFPA 101, Life Safety Code.
2. Addition in Appendix is made to indicate that storage locations for Type I I systems also have to comply with NFPA 101 when the door to such storage locations opens onto an ex i t access corridor.
(Log #13) 99 - 23 - (4-3.1,8.5(a)): Reject ~UBMITTER: Jonathan P. Lauch, Lauch Mechanical Engineering COMMENT ON PROPOSAL NO.: 99-162 RECOMMENDATION: Change the maximum re l ie f valve setting from "200 psig" to "300 psig". The last sentence would read:
" . . . shall be set at 58 percent above l ine pressure or 300 psig whichever is lower."
109
SUBSTANTIATION: Recognizing that some gas driven medical tool systems require outlet pressures of 215 psig, and that necessary piping runs and f i t t ings dictate supply pressure requirements well in excess of 200 psig. This recommended change would be consistent with the TCR's decision to accept revision of 4-5.1.3.6, Proposal #99-162 (Log #160). COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: CGA document on DISS connectors s t i l l references 200 pslg max. NFPA 99 cannot unilaterally change value.
(Log #20) 99 - 24 - (4-3.1.9, Figure 4-3.l.9): Accept in Principle SUBMITTER: Antonio A. Mesa, Nash Engineering Co. COMMENT ON PROPOSAL NO.: 99-123 RECOMMENDATION: Revise as follows:
In order to permit service without interuption to medical air:
A) Aftercoolers, where required, shall be duplexed and provided with bypassing or installed local to each compressor and trapped.
B) Medical a i r receiver shall have bypassing and not to be used as an aftercooler trap.
C) One redundant dryer shall be installed and piped in parallel with appropriate valving to allow isolation and servicing of one unit while the other(s) are on-line.
D) Medical a i r f i l te rs shall be . . . (as proposal states).
E) All final l ine regulators shall • • • (as proposal states).
Add note to Figure 4-3.1.9: NOTE: Flow schematics which di f fer may be acceptable as long as they meet intent of Code.
SUBSTANTIATION: I) No compressor installation wi l l deliver 39°F dew point without a functional dryer. Therefore, redundancy is warranted and necessary everywhere in the country.
2) Dryers cannot function at adiabatic discharge temperatures of typical compressors, therefore, redundant aftercoOler requirement.
3) Tank bypassing means condensate wi l l travel downstream to refrigerant or desiccant dryers, therefore, the aftercoolers must be trapped.
4) Various flow schematics can meet intent of Code and flow schematic should not be considered restrict ive. (Same note as in Figure 4-7.].I.1 of Vacuum Systems). COMMITTEE ACTION: Accept in Principle.
1. Modi fy wording in Committee Act ion 1 in Proposal 99-123 to read as f o l l o w s :
"The medical a i r receiver shall be provided with a three valve bypass to permit service to this device without shutting down the medical a i r system." [Changes underlined.]
(New) Aftercoolers, where required, and dryers shall be duplex and valved to permit the isolation of a device and the continued operation of the system in the event of failure of the unit in service. Under normal operation, only one dryer or aftercooler shall be open to air flow, with the second valved off.
(New) Aftercoolers, where provided, shall be provided with a condensate trap, and shall not rely on the receiver drain to remove aftercooler condensate.
(New) When more than two devices are provided, the peak calculated demand shall be met with the largest single unit out of service.
Medical air f i l te rs . . . (rest the same). 2. Delete new subparagraph (b) in Committee Action 2
in Proposal 99-123 in TCR. 3. Modify Figure 4-3.1.9 in TCR proposal 99-123
Committee Action 3 as follows on next page [to reflect items ] and 2 of this Committee Action].
4. Add Note to Figure 4-3.1.9 as recommended by Submitter, except change "Code" to "standard". COMMITTEE STATEMENT: For Actions l to 3: Changes by Subcommittee on Nonflammable Medical Piped Gas Systems are made to correlate with proposed changes in Con~ittee Action on Proposal 99-123 in TCR.
4. NFPA 99 is currently a "standard" not a "Code".
110
(Log #55) 99 - 25 - (4-3.1.9): Reject SUBHITTER: D.A. McWhinnie, Hickory Hi l ls, I l l COMMENT ON PROPOSAL NO.: 99-124 RECOMMENDATION: Add air compressor sizing recommendations. SUBSTANTIATION: Essential for designers and users to provide proper source equipment, which is essential to maintaining the required safe pressure and flow "performance". There are examples of gross undersizlng and oversizing - - many. See Documentation 746A, and Plumbing Engineer, September '83, both in Subcommittee and Technical Committee f i les.
The Subcommittee "choice", Lo~ 135 [Proposal 99-124 in TCR] rhetorically evades an important topic that has been both neglected and abused. I t ignores the fact that source sizing is beinQ done al l the time -- with recommendations ranging from the tenuous to the ridiculous, often by unqualified advisers, and evidenced by the many years of complaints and discussion within Committees. There are many examples of gross undersizing and oversizing.
Subcommittee Statements, Log #135 [Proposal 99-]24 in TCR]:
I. "Performance cr i ter ia is a ( i f not the) primary objective, and responsibility, of Standards/Codes producing groups and "performance" "effectiveness" (check the definit ion), for which safe and effective capacity cr i ter ia is essential. NFPA's stated responsibilities include for "performance"; "proper safeguards", "related safety goals", "including other hazards" - which, in Health Care Facil it ies documents, cover patient life-support systems and equipment.
Z. Without thought, that Subcommittee statement of " f i re, explosion or electrical safety" is reckless, and inconsistent with i ts own actions, in requiring extremely expensive dewpoint monitors and alarms which, lacking any valid documented substantiation and mandating arb i t rar i ly selected levels, is contrary to NFPA policy and should not be in the text.
Designers do not know (is documented) minimum safe "performance" cr i ter ia for the Chapter 4 r_~p,_q_uj_~p_~ "peak calculated demand" - - "maximum flow rate" (repreated throughout Chapter 4 and essential to capacity levels) without a performance minimum (NFPA requirement for patient safety).
"Less familiar" designers are at the mercy of those advisers who don't know (undersizing per Plumbing Engineer, September '83); or who do (or maybe don't) know and greatly oversize, using "cushion" "future expansion", etc. as rationale - a proprietary ploy (documented).
Without valid and authorative consensus guidelines on minimum requirements for the maximum consuming treatment device, and the diversity of use factor, i t is l i t e ra l l y impossible for A/Es to properly design sources, pipe/f i t t ings, valving, pressure rel ief capacities, etc., etc. In this regard the Subcommittee Statement is (I regret to say, but can't apologize) facetious.
These life-support systems require such cr i ter ia at least as much as other pneumatic, hydraulic and electrical "systems for patient application which all commonly and routinely must, and do, have in standard's minimum cr i ter ia for minimum capacity and projected diversity.
3. This Subcommittee Statement (3) is, simply, wrong. No prudent professional* would deny that source and system's capacities of patient systems (any patient life-support systems) are essential to safe-optimum designed "performance".
* (or anyone who had read the above refs.) There is reference material in the Subcommittee and
Technical Committee f i les which the Subcommittee could (should) employ and incorporate into i ts document.
As I feel that Committee rejections require the same quality of substantiation as proposals, ballots (and Committee deliberations should have) - I consider the Subcommittee [Log 135 (Proposal 99-124 in TCR)] Statement a non-response. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: 1. Subcommittee on Nonflammable Medical Piped Gas Systems is unaware of any concensus. data on calculating compressor sizing.
2. Subcommittee is unaware of hazards associated with compressor sizing.
3. Submitter did not provide specific recommendations per 11-7 of NFPA Regulations Governing Committee Projects.
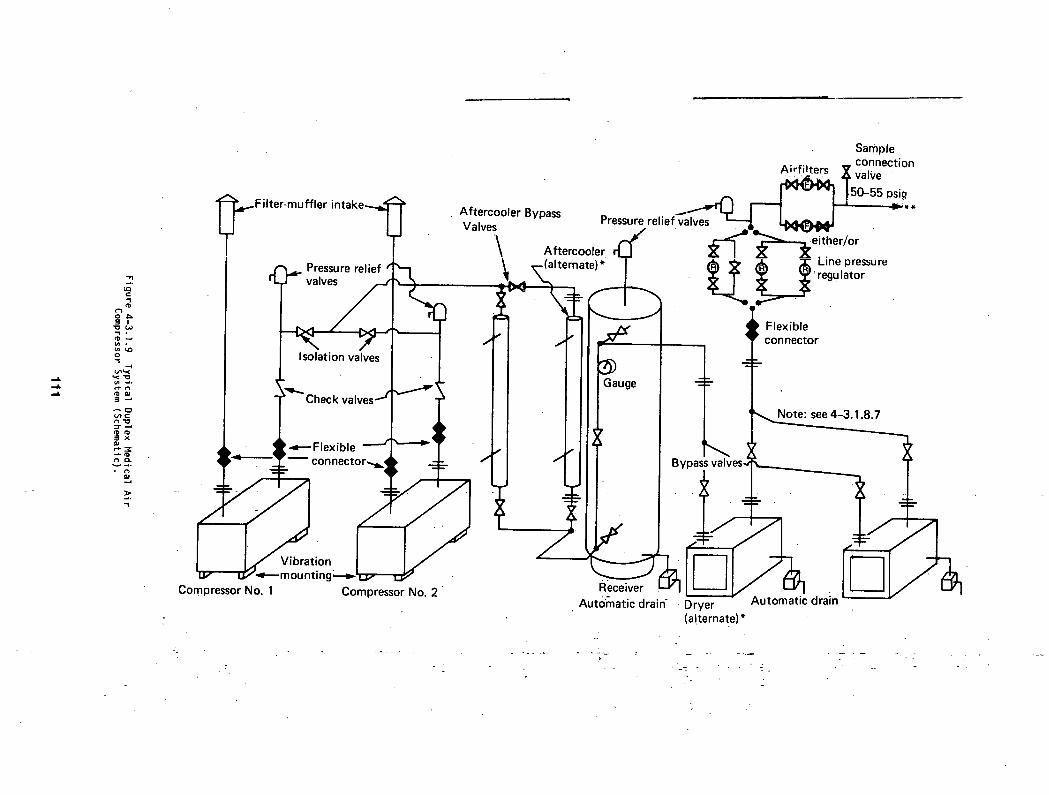
~ .
2==
~ . < ' O
: : 3 " ~
e-~ '-a"
-L
~Filter-muffler i n t a k e ~
Compressor No. 1 Compressor No. 2 "
Sample _ connection • A irfilters v valve
0-55 Dsi . Aftercooler Bypass Pressure relie Valves
\ ~ " . C _ ~ - ~ V e ~ t her/or Aftercooler r[_ I ~ I ~' ~ . .
f
11 , . - (a l ternate) *~ ~ ~ , reguLInelatorPressure . t ~ "3
I
Gauge
I Flexible connector
~ . ~ see 4-3.1.8.7
J
Rieceiver L ~ Automatic drain - Dryer
(a!ternate)*
Bypass valves,
Automatic drain
- - r k - -

(Log #21) 9 9 - 26 - (4-3.1.9.2): Accept ~ : Antonio A. Mesa, Nash Engineering Co. COMMENT ON PROPOSAL NQ.: 99-125 RECOMMENDATION: Change 2nd sentence to:
"Where this is done, open inlet piping to a compressor removed for service shall be isolated by manual or check valve, blind flange or pipe cap to prevent backflow." SUBSTANTIATION: A) Liquid ring installations ellminate the need for these valves through use of inlet check valves.
B) Inlet connections can be sealed during compressor service by blind flanges or pipe caps.
C) Unnecessary inlet valves may accidently choke and damage compressor. COMMITTEE ACTION: Accept.
(Log #22) 99 - 27 - (4 -3 , l .9 .4 (b ) (New) , 4 -7 .1 .1 .1 ( c ) ) : Accept in P r inc ip le SUBMITTER: Antonio A. Mesa, Nash Engineering Co. COMMENT ON PROPOSAL NO.: 99-139 RECOMMENDATION: Add similar requirement to vacuum section possibly under 4-7.1.1.1(c) or,
Do not add requirement to compressors. SUBSTANTIATION: Consistency with reserve equipment alarm requirements for both services. COMMITTEE ACTION: Accept in Principle•
Add following new paragraph to 4-7.1.1.1(c): "A local audible and visual signal shall be provided
to indicate when the reserve or off-duty vacuum pump is in operation."
Add following new Appendix A-4-7.1.I.1(c): A-4-7.1.1.I(c) One method of indicating the reserved
vacuum pump is in use is to activate'the alarm from the vacuum switch that starts the reserve vacuum pump. COMMITTEE STATEMENT: Subcommittee on Vacuum Systems agrees with recommendation, but i t is necessary to change "pressure" references to "vacuum" references.
(Log #56) 99 - 28"- (4 -3 .1 .9 .8 , Table 4 -3 .1 .9 .8 , Table A-4-3.1.9.8, 4 -3 .1 .9 .9 , and Figure A-4-3 .1 .9 .7 ) : Reject ~ : D.A• HcWhtnnie, Hickory H i l l s , I l l COPPIENT ON PROPOSALS NQ.: 99-132, 140 and 278 RECOMMENDATION: 1. Figure A-4-3.1.9 .7 - Delete "Typical" and insert "Optional" ( i t ' s not typical).
2. Delete 4-3.1.9.8, Table 4-3.1.9.8, Table A-4-3.1.9.8, 4-3.1.9.9 and proposed new 4-5.1.5.
3. Delete "Air Compressors", "Vacuum Pumps" and "Vacuum Systems" from Table4-4.1.1.2. SUBSTANTIATION: I agree with S.3. Farruggia, A.S.S.E. (Proposal 99-30, Log #120) that there is "much confusion in the industry." I t is an understatement as regards some designers, hospital engineering execs and others who must interpret (or try to), for on-site compressors.
(a) Nowhere is i t stated that "a dewpoint monitor is required"• (Same for " " alarm).
(b) Nowhere is "air quality" defined for on-slte compressors.
(c) 2-2 "Medical Compressed Air (b)" is "local outside" a i r [when compressors meet 2-2 MCA(b)]. To L'e_q_~j_~g the designer, instal ler, hospital, authority having jurisdict ion, cer t i f ier , or anyone to "verify" a i r which meets MCA(b) is !! (unreasonable?)
(d) On-site compressors account for probably 98/99 percent, certainly not less than 95 percent, and yet quality of a i r from other sources is defined in 2-2 MCA(a), but not MEA(b)!
Dewpoint monitors and alarms(??) are only ~ , and then under "required tests" - - an afterthought - - after the compressors and system are bought and installed?? (See S. Malek and S. Malcom (in f i le ) re text and sequence.) I f required, this information belongs up front along with al l other compressor component requirements. Both of these never-stated-clearly "requirements" have been missed where reliance was placed upon MCA(b) (can be documented).
Even the Subcommittee agrees [Log 174 (Proposal 99-132 in TCR)] wi th S.J. Farruggla (Proposal 99-30, Log 120) as to confusion. But to reeu i re an a r b i t r a r i l y selected dew po in t leve l because of " the lack of a f i rm number" (3g°F being changed from A-2-2 recommendation to t e x t requirement) is improper, and wi thout medical documentat ion/substant la t ion is contrary to NFPA Regulat ions. I f 39°F+ is a pa t ien t hazard why was i t only a recommendation?? What has happened since promulgatlon of 99-'87?? - Rationale??
What is meant by a i r q u a l i t y that "cannot be maintained"?? What cons iderat ion has been given to hot, cold, dry, high geographic areas?? - A l l with changing condi t ions.
I f a dewpoint alarm is ever required i t should be wi th a l l other required l i ne components, and not in 4-5. I t belongs in 4-4 wi th other l i ne components - as i t s monitor, i f required (LHU), belongs as a par t of source equipment. (Something about Malek's and Malcom's unique " text-sequence" hang-up.) Where should the alarm be located - in the event of • . . (What?? emergency!)? What set point? With a hazardous dew point leve l se t t i ng there could be many fa lse alarms - - due to any, or a combination of , changing condit ions of pressure, temperature, f low among others. With documented subs tan t ia t ion (an NFPA requirement) of a hazard to pa t ien ts a set po in t must be spec i f ied .
I f f i r e and/or explos ion hazards re la ted to dew point - - or pa t ien t hazards confirmed as to dew po in t , they should be put before the Associat ion through appropr ia te Committees, per Regulat ion 10-13 (and, by reference IO(a) through (d ) ) , 11-9 and 11-]0, and 10-3, (assuming l i te ra l interpretation).
Li teral ly many 1000s of on-site MCA(b) compressor sources have been in use for many years. With this history, f i re, explosion or patient hazard, i f any, should be cited. I t would be rash to mandate, at great expense to Health Care Facil i t ies which are already financially over stressed, this proposal without solid Justification, and contrary to AHA cost containment objectives.
Delete Table 4-3.1.9.8: Nowhere is i t stated clearly; "a dew point monitor is required", or a dew point alarm is required or a dew point alarm setting shall be . . .(??)" No substantiation is shown for these requests.
Delete Table A-4-3.1.9.8: "the compressors may be accepted". Implies that without this test the compressors are not acceptable, which is not true. Delete al l "R"s, "NR"s and "Required" wherever they appear, as g_O_t,b_tD_g in this table is required for anv on-slte MCA(b) compressors, (or any others). Users can ignore A-4-3.1.9.8 Table entirely. I t lacks substantiation of any need, and has no value to any one with MCA(b)s. I f 98-99 percent aren't using on-slte compressors, the Subcommittee has not documented anything different. The use of the same designations ["R",, "NR", and "Required"] in Tables with the same numeric designations, one required (although without substantiation), and the other only a recommendation, is (again) confusing.
Log 173 [Proposal 99-280 in TCR]: The Subcommittee Statement "there are compressors for which" (certain testing) "is necessary" is baseless. I f i t is " ~ " for safety i t should be in the text (required portion) per Bylaws Article 2, "Purposes . . • proper safeguards". I f "necessary" i t is also incomplete and (again) confusing -- having l isted some types and not others.
This entire topic is confusing, as i t is fraught with unsubstantiated and unnecessary requirements and recommendations. Virtual ly al l such systems are MCA(b)s, and al l that this is about is the air delivered to the patient - - from only two sources, pre-packaged or on-site, and both are clearly defined. Leave i t at that. For I or 2 percent of prepackaged sources there is already appropriate cr i ter ia. I f that cr i ter ia is inadequate i t is easily upgraded through the normal process or TIAs. A motor-driven cranked bellows is even covered, assuming pressure requirements and calculated load.
Confusion: "Those familiar" may know or understand, but even they must wade through extraneous (unrequired) cr i ter ia; and wade very carefully when some
112

reouirements are only implied, and then wonder about other hidden implications; and when required and not required c r i te r ia have the same numeric designation, and they both contain "requirements" and neither contains "required" levels or rationale!!
What about the inexperienced, "those not fami l iar , " and "problems . . . of design, insta l la t ion . . . poor advice to the designer . . . ignorance . . ." (Plumbing Engineer, September '83)?
Users deserve better. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT! I. Dew point monitoring is required (see 4-3.1.9.8).
2. Air quality is defined per Proposal 99-274 in TCR. 3. Document (NFPA 99) does not require quali ty of
outside, local a i r to meet Grade D a i r . Requirement for dew point is not related to issue of qual i ty of a i r .
4. Subcommittee on Nonflammable Medical Piped Gas Systems can address qual i ty of a i r when compressors are involved, but not when local outside a i r is involved. To define quali ty of local outside a i r is not within scope of Subcommittee on Nonflammable Medical Piped Gas Systems.
5. Table 4-4.1.1.2 is for user convenience only, and are based on requirements in text.
(Log #2) 99 - 29 - (4-3.1.9.9): Reject SUBMITTER: Reginald Nease, Lenexa, KS COMMENT ON PROPOSAL NO.: 99-132 RECOMMENDATION: Add subparagraph 11) that requires a minimum dewpoint of -18°C (O°F) at atmospheric condi t ions. SUBSTANTIATION: Typical d ry ing devices are capable of providing moisture removal to this level. Testing of l i t e r a l l y hundreds of medical a i r systems indicate that dewpoint levels above -15°C provido a clue that molsture removal is not adequate avid the result may be fa i lure of equipment that is considered c r i t i ca l and l i f e support. Failure of this equipment due to excessive moisture constitutes a d is t inct hazard to l l f e .
Table 4-3.1.9.8 of NFPA 99 presently requires continuous monitoring of the medical a i r supply dewhoint~
Table 4-4.1.-1.2 as presented in the TCR has been accepted by the Committee and requires alarm and therefore monitoring of the medical a i r dewpoint. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Issue addres:~ed in Comment 99-43 (Log #26) Committee Action and Statement is applicable for this comment.
(Log #23) 99 - 30 - (4-3.1.9.10): Accept in Principle ~ : Antonio A. Mesa, Nash Engineering Co. COMMENT ON PROPOSAL NO.: 99-133 RECOMMENDATION: Add to paragraph being inserted " i f required by the dynamics of equipment or location relat ive to occupied space." SUBSTANTIATION: CLARIFICATION. Typical rotary equipment type instal lat ions require no ant iv ibrat ion or f lex type instal lat ions.
These have been used at excess cost to industry because of confusion in Code requirement vs. actual need. COMMITTEE ACTION: Accept in Principle.
Revise wording in TCR to read: 4-3.1.9.10 I f required by equipment dynamics Or
location, ant i -v ibrat ion mountings, in . . . (rest the same) [addition underlined.] COMMITTEE STATEMENT: There are location factors other than occupied space that influence whether ant i -v ibrat ion mountings are instal led.
(Log #73) 99 - 31 - (4-3.2.3 (New)): Accept SUBMITTER: Leo G. Foxwell, The Hartford Insurance Group COMMENT ON PROPOSAL NO.: 99-30, 33, 274 RECOMMENDATION: Add new:
4-3.2.3 Dental Air Compressor Supply System. (Reserved) SUBSTANTIATION: Edi tor ia l : Requirements of ~-3.1.9.I are applicable to Type I only systems. Reports received by Committee indicate that these requirements are being mis-applied to Type I I systems. Committee intends to develop requirements for Type I I Dental Air Compressor Supply Systems. COMMITTEE ACTION: Accept.
(Log #29) 99 - 32 - (4-4.1.1.2 and 4-8.1. I .5) : Reject SUBMITTER: Antonio A. Mesa, Nash Engineering Co. COMMENT ON PROPOSAL NO.: 99-138 and 177 RECOMMENDATION: Should secondary alarm requirements be the same for vacuum and air?
Proposal 99-177 allows secondary alarm to building management computer for vacuum.
Proposal 99-138 does not for gases. SUBSTANTIATION: Clar i f icat ion and consistency. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: I. No Recommendation provided.
2. Vacuum systems are not required to have two master alarms.
(Log #24) 99 - 33 - (Table!4-4.1.1.2): Accept in Part ~ : Antonio A. Mesa, Nash Engineering Co. COMMENT ON PROPOSAL NO.: 99-140 RECOMMENDATION: I) Reserve in use should b e "yes" or "no" consistent for vacuum and a i r , pending outcome of meetings.
2) High pressure and low pressure should have "(vacuum)" in paragraph t i t l e .
3) Add reference to table in Vacuum Section, maybe under 4-8.I .1.5(g). SUBSTANTIATION: iC la r i f i ca t lon and consistency.
absolute: technically as "low vacuum" which would be misleading. COMMITTEE ACTION: Accept in Part.
I. Reject Recommendation I. 2. Accept Recommendation 2. In Table 4-4.1.1.2,
change "High Pressure" to "High Pressure/Vacuum", and change "Low Pressure" to "Low Pressure/Vacuum". Change references "4-4.,I.1.2(c)" to "4-4.1. I .2(b)".
3. Accept in Principle Recommendation 3. Add new Note 2 in 4-8.1.1.5(e). Number exi~stihg Note
as Note I. NOTE 2: See Table 4-4.1.1.2 for l i s t of Master Alarm Signals.
COMMITTEE STATEMENT: I. Lead/lag alarm for vacuum is not required to :be connected to master alarm,(per Proposal 99-139 in TCR).
2. Change in reference is edi tor ia l correction. 3. Advisory material can not be added as a paragraph
in text of a standard. Per NFPA Style Manual, either a Note or placement in Appendix is to be used.
(Log #58 ) 99 - 34 - (Table 4-4.1.1.2): Reject SUBMITTER: D.A. McWhinnie, Hickory H i l l s , Ii'l COMMENT ON PROPOSAL NO.: 99-140 RECOMMENDATION: Delete "Vacuum Pumps" and "Vacuum Systems". Add to t i t l e "NMPGS". SUBSTANTIATION: Not within Gases Scope.
Vacuum is to ta l l y separated from gases: Logs 23, 43, 44, 45 and 46 [Proposals 99-105, 99-106, 99-109, 99-108, and 99-167, respectively]. 4=4.1.1.2, and i ts referenced subsections, as well as referenced appendixes, and referenced 4-3.1.9.8 al l apply ~ to gases.
113
ii

Vacuum text states clearly vacuum alarm requirements. Chapter 4 text is clear that the combining of alarms is not required•
33 of 34 functions l isted apply to gases only. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Table is for user convenience only, is based on requirements in document, and just l is ts requirements in text for Master Alarm Signals for gas and vacuum systems in one table.
(Log #59) 99 - 35 - (Table 4-4.1.1.2): Reject SUBMITTER: D.A. McWhinnie, Hickory Hi l ls, I l l COMMENT ON PROPOSAL NO.: 99-140 R__E~OMMENDATIQN: Delete "Dewpoint High" column. SUBSTANTIATION: No "Problem" or "Substantiation" has been provided to any Committee showing f i re, explosion, or patient hazard,* contravening Regulations 10-13, 11-9, 11-10.
*(Medical problem) COMMITTEE ACTION: Reject. CQHMITTEE STATEMENT: Subcommittee on Nonflammable Medical Piped Gas Systems is aware of reports that l i s t hazards associated wlth high dew point.
(Log #54) 99 - 36 - (4-4•I•1.4(a) and (b), 4-4.2•10•I, 4-8.1.1.7(a) and (b)): Reject SUBMITTER: D.A. McWhinnie, Hickory Hi l ls, I l l COMMENT ON PROPOSAL NO.: 99-156, 180 RECOMMENDATION: Add "continuous reading" before "pressure/vacuum gauge". SUBSTANTIATION: Consistency with intent of both Subcommittees; "continuous surveillance", "continuous responsible observation", "noncancelable visual signal • . . shall be seen": 4-4.1.1.2, 4-4.2.9.2, 4-5.1.4.2, 4-8.1.1.5, 4-8.1.1.6(b). Manually actuated (button or switch) devices to get a reading are unacceptable. COMMITTEE ACTION: Reject. C~MITTEE STATEMENT: Intent of Subcommittee on Nonflammable Medical Piped Gas Systems was continuous monitorlno of pressure. Visual display can be of any form, as. iong as i t is readable. Reference to manually activated devices (e.g., 4-4.1.1.2(f)) is not related to the issue of the readout of gauges.
(Log #6]) 99 - 37 - (4-4•l.2.4): Hold For Further Study SUBMITTER: D.A. McWhinnie, Hickory Hi l ls, I l l CO.~MENT ON PROPOSAL NO.: 99-153 RECOMMENDATION: Add outlet minimum flow required for optimum patient treatment using the maximum demand respiratory devices, SUBSTANTIATION: [Refer to Committee Statement of Proposal 99-]53 in TCR.]
I. Simply not so, Maximum quality patient.need is equal to the minimum flow required to properly operate the demands of the highest use respiratory care device.
2. This statement is irresponsible, in that i t ignores, doesn't consider or address, the substantiations in Logs 133, ]34, 10 and II [Proposals 99-153, 99-284, 99-285, and 99-288, respectively in TCR]; nor the pertinent and documented information known throughout the health cere f ield - - of "2,833" faulty outlets (some completely occluded), -- Plumbing Engineer, September, ]983. I t also ignores the documented flew demand(s) data in Subcon~ittee documentation (Log 135, Proposal 99-124), and ProJect 746A on medical compressed air systems. Material to, and a part of, this Substantiation are Log 135 [Proposal 99-124 in TCR], Log 137 [Proposal 99-163], and Log 141 [Proposal 99-164 in TCR].
Many others involved in this unique technology have reported, on the record, station terminal flow problems.
3. This proposal is, for life-support gases delivery components, more "germane" than for 4-9. The Subcommittee fa i ls to address subsantiations paragraph 6, Log 133 [Proposal g9-153], paragraph 4, Log 134 [Proposal 99-284 in TCR], paragraph 5, Log lO [Orioisak 99-284 in TCR]; and has disregarded the objectives and intent of Regulations 10-3 - -wh i le inconsistently cit ing those same objectives in Logs 135 and 174 [Proposals 99-124 and 99-132 respectively in TCR].
4• They have been for years - - and wander over an inconceivably broad range. See Med. Air portions (two) of attachments, Log 135 [Proposal 99-124 in TCR]; Project 746A (Medical Air portion) and Plumbing Engineer, September, 1983.
Many A/E designers have done no Medical Gas or Vacuum systems, and some have done only one or two. They all require reasonable consensus guidelines~ They need better than widely divergent proprietary information. See last references above for both over and under sizing.
What happened to "Hold For Further Study", (Logs lO and l])?
A means to i n i t i a l l y determine medical gases outlet performance, and periodically check for proper flow, is not only appropriate but needed to assure optimum patient care. I t would be hard to find a hospital that doesn't have in i ts normal inventory the few, and adequate, items to easily determine outlet flow performance.
A medical gas outlet is a valve, and no valve is immortal - nor should one be expected to operate consistently throughout i ts useful l i fe .
Field spot checks of outlets have revealed flow restrictions due to torn or broken-off pieces of the elastomeric seals, tensionloss or breakage of springs, as well as costly concealed, undetectable leaks which, under certain conditions, can elevate gas concentrations in concealed and/or confined spaces. (See 8-2.1.1.5).
Hospitals should be encouraged to periodically check medical gases outlet performance (which, experience indicates, is seldom done). Such checks are especially important in ORs and cr i t ical care areas.
Methods to perform outlet flow and leak tests need not be complex or require expensive apparatus, would encourage maintaining peak performance, would assure optimum patient care and would reduce costs and potential hazards due to leaks. Such tests could be accomplished simultaneously• COMMITTEE ACTION: Hold For Further Study (November '86)
COMMITTEE ACTION: Hold For Further Study. COMMITTEE STATEMENT: I. Subcommittee on Nonflammable Medical Piped Gas Systems agrees there is a need for minimum flow characteristics. However, data needs to be acquired and reviewed before setting minimum performance characteristics. No data was submitted with public comment.
2. Proposals Log #10 and #11 in TCR are Proposals 99-285 and 99-288 respectively in TCR. They were submitted as comments for 1987 edition of NFPA, but were held for further study. Comments held for study become proposals for the next edition of a document.
(Log #62) 99 - 38 - 4 - 4 • 1 . 4 . 1 ) : Hold For F u r t h e r Study SUBMITTER: D.A. McWhinnie, Hickory Hil ls, I l l COMMENT ON PROPOSAL NO.: 99-155 RECOMMENDATION: Delete "at the job site". SUBSTANTIATION: The Subcommittee prompts the question -- did anyone read the proposal? "Disposal" of the agent was (is) not the issue; and to so infer requires a high degree of imagination. Disposal of hazardous wastes is not within the scope of this Subcommittee, and, as a non-response to the problem of patient hazard, is in conflict with Regulations I0-13, II-9, and l l - lO.
The hazard exists, especially with capped or sealed system components, no matter where the process is performed.
114

COMMITTEE ACTION: Hold For Further Study. Move new sentence of Committee .Action on Proposal
99-155 in TCR from 4-4.1.4.1(a) tD 4-4.1.4.1(a)(2). COMMITTEE STATEMENT: I. Trichloroethylene can not be properly control led at the job s i te . Residues of i t can not be easi ly removed, and would present a d is t inc t hazard to patients or personnel i ns ta l l i ng piping.
Submitter's Recommendation would prohib i t a l l use of t r ichloroethylene. However, i t is outside the scope of the Subcommittee on Nonflammable Medical Piped Gas Systems as to methods used by manufacturers to clean pipes. Submltter's concern is being forwarded to the Compressed Gas Association on this issue.
2. Movement of sentence is ediLor ial to make i t clear that new sentence applies only at job s i te .
(Log #3) 99 - 39 - (4-4.1.4.2, 4 -8 .1 . I .8 (a ) ) : Hold for Further Study SUBMITTER: Robert M. Henson, J'.W. Harris Co., Inc. COMMENT ON PROPOSAL NO.: 99-182 RECOMMENDATION: Revise 4-4.1.4.2 as fol lows:
" . . . comply with speci f icat ion for Brazing F i l l e r Metal ANSI/AWS A5.B or a suitable a l ternat ive as noted in (a).
(a) Copper to copper j o in t s shall be made using a copper-phosphorous or copper-phosphorous-silver brazing f i l l e r a l loy simi lar to or complying with the requirements of the AWS BCuP series without f lux .
Revise 4-8.1. I .8 Note as fol lows: " . . . medical gas piping. (Refer to 4-4.1.4.2 for
recommended brazing f i l l e r metals.)" SUBSTANTIATION: The reference to brazing should refer the reader to 4-4.1.4.2 to f ind outwhat brazing f i l l e r metals are acceptable. At the same time 4-4.1.4.2 should be expanded because these are copper-phosphorous and copper-phosphorous-silver f i l l e r metals not l i s ted in AWS A5.8 that are commonly used in industry. These f i l l e r metals exhibi t the same j o i n t strength propert ies, melt above 1000°F, and can be used without f lux on copper to copper jo in ts . COMMITTEE ACTION: Hold For Further Study. COMMITTEE STATEMENT: Insu f f i c ien t data was submitted to substantiate proposed wording, and thus for Subcommittee on Nonflammable Medical Piped Gas Systems to act on ( i . e . , AWS document defines a number of physical propert ies; proposedwording does not). Subcommittee is uncertain which physical properties are most relevant.
(Log #76) 99 - 40 - (4-4.2.12.2 and 4-4.2.1}~.3): Accept ~BMITTER: Leo G. Foxwell, The Hartford Insurance Group COMMENT ON PROPOSAL NO.: 99-158 RECOMMENDATION: Revise second sentence from:
" i t is mandatory that emergency shut o f f . . ." To read: " i t is mandatory that cyl inder shut o f f . . ."
SUBSTANTIATION: Ed i to r ia l . The Committee did not intend to use the emergency shut o f f valves as stated. This would be v io la t ion of other parts of text . COMMITTEE ACTION: Accept.
(Log #25) 99 - 41 - (4-5.1.3.6): Hold For f'urther Study SUBMITTER: Antonio A. Mesa, Nash Engineering Co. COMMENT ON PROPOSAL NO.: 99-162 RECOMMENDATION: Add to proposed paragraph:
" I f supplied by the central medical a i r system, i t shall be separately piped upstream of the main l ine regulator and have i t s own iso la t ion valve, regulator, alarms, etc." SUBSTANTIATION: A) Simpl i f lcat ion of piping, regulators, and alarms for nominal 50 Ib medical a i r system.
B) This would keep industry from d is t r ibu t ing unregulated a i r and regulaLing at mult iple 1ocat lons, result ing in less consistent pressure throughout hosp!tals and creating master alarming d i f f i c u l t i e s .
COMMITTEE ACTION: Hold For Further Study. COMMITTEE STATEMENT: Issue raised goes beyond the change contained in Proposal 99-162 in TCR, 'and requires fur ther research in order to address properly.
(Log #70) 99 - 42 - (4-5.11.3.6(a)): Accept in Principle SUBMITTER: D.A. McWhlnnie, Hickory H i l l s , I l l COMMENT ON PROPOSAL NO.: 99-163 RECOMMENDATION: Delete "be capable of del iver ing" and in i ts place add "maintain". SUBSTANTIATION: [Refer to Subcommittee Statement in Proposal 99-163.] I. I t ' s obvious the proposal (99-163) was nolt clear. I ts intent was to c l a r i f y the Subcommittee wording. In this context, pressure is "maintained", and flow is "del ivered" (and also per Webster's N.W.D., and Roget's I I ) .
I f the optimum 50 psig ( fo r which a l l fiowmeters for these systems are cal ibrated) were s tat ic that pressure i sn ' t delivered ~, i t ' s maintained.
I believe the' intent of the Subcommittee is to maintln "50-55 psig".
Anyone understands that to maintain a required pressure, the "maximum flow" (4-5.1.3.6) must be known.
Without "f low" information/guidelines i t is l i t e r a l l y impossible to comply with 4-5.1.3.6(a); and .that results from fa i lu res in 4-3.1.9 and 4-4.1.2.4 and 4-5.2.4.1 [Logs 135, 133 and 141 (Proposals 99-124, 99-153 and 99-164, r espec t i ve l y ) l , as well as Logs 10, 11 and 134 [Proposals 99-285, 99-288, and 99-284, respec t i ve ly ] , a l l re la ted, and on which proposals have been made.
[This comment = is fur ther evidence of the need for not reject ing Proposals 4-3.1.9 and 4-4.1.2.4. (Proposals 99-124 and 99-153)]
2. This statement reveals a d i f f i c u l t y with the word "semantics". There is cer ta in ly no equivalence between maintaining a required pressure, and del iver ing a flow (volume).
The Subcommittee has neither addressed the comment, nor substantiated i t s re ject ion. COMMITTEE ACTION: Accept in Principle.
Change "shall be capable of del iver ing" to "shall be capable of maintaining". COMMMITTEE STATEMENT: l . Submitter's Recommendation is res t r i c t i ve because i t would mandate 50-55 psig. Intent of Subcommittee on Nonflammable MediCal Piped Gas Systems is to set minimum requirements. Other pressure settings than 50-55 pslg may be necessary.
2. Subcommittee on Nonflammable Medical Piped Gas Systems agrees with use of term "maintaining" with reference to flow.
(Log #26) 99 - 43 - (4-5.1.5): Accept in Principle SUBMITTE___R: Antonio A. Mesa, Nash Engineering Co. COMMENT ON PROPOSAL NO.: 99-132, 276. RECOMMENDATION: A) Change proposed wording of 4-5.1 5 to read:
4-5.1.5 Dew point fo r loca l l y compressed a i r shall be monitored and alarmed per 4-3.1.9.8 and 4-4.1.1.2 to protect from a pressure dew point r ise to 50°F from the nominal design of 39°F.
B) Insert alarm requirement as 50°F in 4-3. ] .9.8. SUBSTANTIATION:. I) Alarming at capabi l i ty of dryer w i l l force industry to dry at elevated pressures and consume more power needlessly to create margin from alarms.
2) State design (or nominal) and alarm range as with pressure.
3) Stated problem was confusion with exist ing wording of requirements not actual dew point. 50°F alarm wi l l not result in saturated a i r and is an acceptable minimum. COMMITTEE ACTION: Accept in Principle.
I. In Submltter's Recommendation A, change "from a pressure" to "from a l ine pressure"; change "50°F '' to "39°F'!, and change "39°F '' to "35°F ''.
2. In Submitter's Recommendation B change "50°F '' to "39°F at l ine pressure".
115
COMMITTEE STATEMENT: I. Dew point is lowered because condensation has been shown to occur at 50°F.
2. "Line pressure" is added since i t is desired to maintain 39°F alarm dewpoint, regardless of the operating pressure.
Change in B is for consistency with changes in A.
(Log #27) 99 - 44 - (4-5.2.4.1): Reject SUBMITTER: Antonio A. Mesa, Nash Engineering Co. COMMENT ON PROPOSAL NO.: 99-164 RECOMMENDATION: Per Mr. Dave McWhinnie's original proposal. SUBSTANTIATION: ± 20 percent of which l ine pressure?
As noted in Proposal 99-162, the pro l i ferat ion in pressure requirements for medical a i r , because of tools, etc., w i l l begin to raise questions about "nominal", ult imately compromising the control pressure range for manufacturers of respiratory therapy equipment.
These alarm settings should be clearly stated as was fe l t to be the case for dew point. COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: Same Recommendation as in Public Comment 99-42 (Log #70). Thus, comment is rejected for same reasons as given in Comment 99-42.
COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: I. Intent of Subcommittee on Nonflammable Medical Piped Gas Systems was to reference a percentage around operating pressure of gas, irrespective of actual operating pressure.
2. Accuracy of flow meters is not germaln to the issue of alarm set points.
3. Subcommittee is aware that some f a c i l i t i e s operate their systems at pressure ranges other than 50-55 psig. Section 4-5 of NFPA 99 l i s t s minimum performance c r i te r ia and is not equipment specific. Subcommittee thus believes i t has met the intent of Section 10-13 of NFPA Regulations Governing Committee Projects.
(Log #66) 99 - 46 - (4-7.1.1.1): Accept SUBMITTER: D.A. McWhlnnie, Hickory Hi l ls , I l l COMMENT ON PROPOSAL NO.: 99-173 RECOMMENDATION: Add new (g) and re le t ter present (g)*, (h) and ( i ) accordingly.
Add: "All piping between vacuum pump(s), discharge(s),
receiver(s) and vacuum main l ine value shall be in accordance with 4-8.1. I .2(a) . " SUBSTANTIATION: To c la r i f y Subcommittee intent. COMMITTEE ACTION: Accept.
(Log #60) 99 - 45 - (4-5.2.4.1): Reject SUBMITTER: D.A. McWhinnie, Hickory H i l l s , I l l COMMENT ON PROPOSAL NO.: 99-164 RECOMMENDATION: Delete "drops . . ." (to end of paragraph).
Replace with "drops to 40 psig or increases to 60 psig." SUBSTANTIATION: Subcommittee Statement for Proposal 99-164 confl icts with 4-5.1.3.6(a) which applies to v i r tua l l y a l l medical gas systems, and are clearly the ones intended by the text - - "50-55 psig" being the only (and optimum) range mentioned in the entire document; along with "normal" l ine pressure mentioned at least six times.
All medical oxygen, a i r and nitrous oxide flowmeters are accurate only at 50 psig., as also applies to reconstituted or mixed gases for patient respiration.
The Subcommittee fa i l s to ident i fy any "even higher ''~ systems operating pressure range(s), thereby fa i l ing the obvious intent of Regulation 10-13 as to "preferably technical . . ." and certainly as to "suf f ic ient ly detai led."
Designers, ins ta l le r , authorit ies having jur isd ic t ion, cer t i f ie rs and JCAHO v i r t ua l l y always (always, based on experience) u t i l i ze , and reference Chapter 4 as above. The Sucbommittee has provided no "higher" pressure systems information to the appropriate NFPA Committees.
I f any do exist they should be in the Scope, separate section, Appendix, etc.
Unspecified "higher" (or lower) pressures could (woutd) affect piping materials, sizing, l ine component Capacities and other characteristics.
* I f that statement applies to hyperbaric systems nothing in Chapter 4 is applicable. They are less than I percent of systems and belong in another Subcommittee.
(Log #28) 99 - 47 - ( 4 - 7 . 1 . 1 . 1 ( h ) ) : Accept in P r i n c i p l e SUBMITTER: Antonio A. Mesa, Nash Engineer ing Co. COMMENT ON PROPOSAL NO.: 99-171 RECOMMENDATION: 1. Change second l i n e of o r i g i n a l comment to:
"Where t h i s is done, open d ischarge p ip ing from a vacuum pump removed f o r se rv ice sha l l be i s o l a t e d by a manual or check va lve , b l i nd f l ange , or pipe cap to prevent back f low. "
2. Do not change Figure 4 -7 .1 .1 .1 to imply requirement. ~UBSTANTIATION: Discharge isolat ion valve le f t closed can damage a pump from backpressure. Pumps are rarely removed from l ine for service and isolat ion can be done by other less potent ia l ly hazardous and expensive ways, i f necessary. This is more applicable to routine service of sl iding
vane oi l changes and demister service only, and should be recommended by manufacture for their unit o n l y . COMMITTEE ACTION: Accept in Principle.
I. In the Recommendation in Proposal 99-171, change sentence 2 ("Where exhausts are . . .") to read as follows:
"Discharge of pumps u t i l i z i ng a common exhaust pipe shall be f i t ted with a check valve, a manual valve, or arranged to permit capping of the active pipe when removing or servicing a pump."
2. Modify Figure 4 - 7 . 1 . I . I ( i ) , as shown on next page, by making valves in discharge l lne dotted to indicate they are optional. COMMITTEE STATEMENT: I. To allow al l options for isolat ion.
2. To ref lect that valves are optional.
116

,=& ==L
==
f~
A
F r o m
piping ,--~ system
B V = Bypass valving (optional)
Master alarm vacuum switch [~]
Note: dotted lines indicate optional items.
Gauge / ~ I- O'P~n~ 7 . _(Normally ~-ILm---u f--fler- J
, - , . . ~ - - - ~ Vent ~tZp V N a..~.. BV I '*-"-lines
A • V |~ I -~xj .-r, o.
Receiver*
Vacuum pVuaCU;= pump
I = To drain*
L
"~Manual valves
~1 Vent-discharge I line(s) outside ~r of building
~Drip leg(s) required as
(one as close as possible to the pump)
~ C h e c k valves
:~---- Flexible couplings
\
- . . . , . ' .
(Log #63) 99 - 48 - (4-7.1.2, 4-8.1.I.1(a) and (b), 4-8.1.2, C-4.6(3), C-4-3.1(b)): Hold For Further Study SUBMITTER: D.A. McWhinnie, Hickory Hi l ls, I l l COMMENT ON PROPOSAL NO.: 99-168 RECOMMENDATION: Delete 4-7.1.2, 4-8.1.2; C-4-6(3); C-4-3.i(b) double asterisks; 4-8.1.1.1 "but does . . . (through) . . . gases"; parenthetical and "NOTE" under Table 4-8.1.1.I t i t l e ; 4-10.4.1.4 "or, i f used," and WAGD (box); A-4-8.1.1.1(a) second line; and A-4-8.1.1.1(b) "NOTE I". Add: Disclaimer B, Log 129 [Proposal 99-107 in TCR]. SUBSTANTIATION: All Subcommittee Statements (Logs 129, 143) Proposals 99-107 and 99-168 in TCR are uniformed, unsubstantiated, lack basis and completely contradict the authoritative documentation in the Subcommittee (Proposal 99-168, Log 143 in TCR). There are at least 25 references in the hands of the Subcommittee and Technical Committee refuting the Subcommittee and Technical Committee 1988 actions• ( I f the references were reviewed they've not been addressed.)
(a) Subcommittee "Statements" [Logs 129 and 143 (Proposals 99-I07 and 99-168, respectively in TCR)]:
Statement I. WAGD is not in the scope 4-1.4; i t is n_ok for "patient drainage, aspiration and suction(ing)"; i t is not used on patients for any treatment, or other, procedure. The l i terature is clear that exposure of the anesthetized patient to the MSVS degree of vacuum in the breathing circuit could cause various types of trauma (at least four documented in Subcommittee/Technical Committee records). The Subcommittee and Technical Committee f i les contain at least 25 references refuting Subcommittee Statement I.
"ANSI Z79" reference in NFPA 99, A5-4.1 and 2 "Ventilation of Anesthetizing Locations" (the NFPA t i t l e i tse l f states exactly that the issue is environmental) cautions against any "application" of equipment tht could expose "the breathing circuit to
pressure less than atmospheric" (underscores added). Further, that same reference (in NFPA 99, A-5-4.1 and
2) cautions against "the dunking" of any flammable vapors into a central suction system not designed for such operation." (Chapter 4 MSVS is not so designed). Additional hazard: "Flammable anesthetics are s t i l l being used" [Log 52 (Proposal 99-2 in TCR) and EE Subcommittee 8-15-88].
There remain ORs without WAGD, and many with WAGD/scavengers/"evac" not being used - - and performing surgery daily. Its obvious that these are certainly not patient treatment systems, and do not qualify as "patient" or "medical-surgical" (4-7.1) systems.
Statement 2. This statement is without thought, being only a partial one. The Subcommittee has a very serious responsibility as to the intended appliction of i ts assigned project. Vir tual ly every NFPA document limits to some degree its application, depending upon i ts intent, purpose and scope. ~ everyone knows that [NFPA] 99, 4-1.4 l imits i ts application and excludes/prohlblts a specific application. I t should not be necessary to explain "dedicated" systems, or to l l s t the hundreds of exclusions, prohibitions or other application l imits throughout NFPA documents.
Statement 3. This statement reflects a lack of concern about hazards, or knowledge of the facts. NFPA texts should not include, and infer by reference, applications which have voluminous documentation cit ing patient hazards (regardless of degree), and l is ts of potential patient trauma•
Technical Committee 7-I-86: " I f the Technical Committee is to err le t 's do so on the side of safety." I t is at least inconsistent, i f not irrational to include, infer by reference, and "permit" (Subcommittee Statement) an application with documented, by name, at least 4 hazards/traumas (pulmonary barotrauma, ref. in Proj. 746-A in Subcommlttee-Technlcal Committee f i les) - - and simultaneously ~ in the same NFPA 99 chapter the monitoring and alarming of a condition for which there is no documented hazard (dew point), and no Subcommittee Substantiation (per Regulation I0-3, 10-10). To reauire an arb i t rar i ly selected l imi t because of "the lack of a firm number . . ." [Subcommittee Log 174 (Proposal 99-132 in TCR)] is inconceivable.
Statement 4. This is a non-statement as i t ' s i r r e l e v a n t • The Submit ter o f tha t statement has f a i l e d to prov ide the Subcommittee wi th the requested documentation on tha t p r o j e c t . In any event i t is not p e r t i n e n t as "scavenging dev ices" are not w i t h in the Subcommittee Scope. (See Subcommittee Statement 2, Log 129 [Proposal 99-107 in TCR].) *
WAGD i nc l us i on w i thou t s u b s t a n t i a t i o n v i o l a t e s NFPA regulations.
~(a) Although irrelevant, scavenging devices are well known for failure "to function safely when wall suction was applied to the exhaust port." Note: "Wall suction" i_ss relevant to this Subcommittee. (See "Governing Criteria" item I below.) (b) " . . . in normal use, some scavenging apparatus, even when operating properly, can alter the normal characteristics of an anesthetic breathing machine . . . for medical use." (See "Governing Criteria" item 2 below.) Underscores in quotes above have been added.
WAGD is an environmental problem "to minimize pollution of ORs, and occupational exposure of OR personnel" and, therefore, is an OR "ventilation" function as is confirmed by i ts inclusion in [NFPA] 99, A-5-4.1 and 2.
Without the clar i f icat ion of this proposal the patient, medical staff and hospital are at risk.
The Health Care Faci l i t ies Technical Committee has accepted, 1/12/88, the fact of patient hazard in this application.
End of response to Subcommittee "Statements". (b) I t is appropriate to note that ISO and BSI
(British Standards Institute) oppose MSVS use for WAGD because of "very onerous safety problems" which "can seriously affect patients".
The following is based upon Health Care Facil i t ies conferences, seminars, training programs and field experience:
I t has been noted, and is clear, that this function is one of environmental ventilation for "staff protection from pollution by anesthetizing gases" and, therefore, is appropriate to the "Ventilating" section.
NFPA 56K, 1980; Codes 99, 1984 and 1987; and NFPA Health Care Faci l i t ies Handbooks, '84 and '87 al l caution against the use of MSVS for WAGD/"evac" due to the documented and acknowledged hazard to anesthetized patients. WAGD/"evac" is neither a "Medical-Surgical" patient system per 99, '87, 2-2 nor is i t for "patient
' I I drainage, aspiration and suctlon(Ing) per 99, '87, 4-I.4. NFPA "strongly discourages" this use of the MSVS (Health Care Faci l i t ies Handbooks '84 and '87).
In answer to a direct question on this issue at the NFPA Health Care Faci l i t ies Technical Committee meeting less than five months ago the members were advised by John P. Swope, M.D., Chairman of the Anesthesia Services Subcommittee, that the use of the MSVS for WAGD/"evac" is hazardous to the anesthetized patient. The fact of this hazard was accepted without dissent by the NFPA Health Care Faci l i t ies Technical Committee on I0/12/88.
This also is further affirmation of the telephone communication to the May 6, 1980 MSVS Technical Committee by 3ohn H. Lecky, M.D., Chairman of the ANSI Z79.11 Committee on " . . . excess anesthetic gases", and Editor of the ASA 1980 document Waste Anesthetic Gases in Operating Room Air.
The "intent" of ANSI Z79.11 (A-3-3.1.3.3.5) is that the negative/vacuum pressure "approximate ambient pressure" :
• . . in normal use, some scavenging apparatus, even when operating properly, can alter the normal characteristics of an anesthetic breathing machine, extracorporeal oxygenator, or breathing machine for medical use."
Employing the normal barometric pressure differential between the anesthetizing area and i ts surrounding local atmosphere, the non-recirculatin 9 ventilation system "is suitable for waste anesthetic gas disposal." (ASA "Waste Anesthetic Gases in Operating Room Air", 1980) - reconfirmed by Charles Whitcher, M.D., a principal investigator, and many others.
118

i' i;
Or "a dedicated . . . blower system." (ASA[ and others); and maintaining a degree of vacuum not exceeding "0.5 cm H20 during normal operating c o n d i t i o n s . . . , to protect the pat ient" is e f fec t ive without "compromise" of the anesthetized patient (ANSI Z79.11).
"CLINICAL REPORTS" (Anesthesiology 46:152-154, 1977): "Our data confirm the i r (Whitcher et a l . ) fears and extend the i r observations of the possible consequences of venting gases to suction." (N.E. Sharrock, M.D., and D.E. Leith, M.D.)
None of the warnings against the use of MSVS for WAGD/"evac", including the Br i t ish Standards Ins t i tu te and the International Standards Organization, has been refuted, or even challenged.
Without any (to say nothing of substantive) rat ionale i t is f o l l y for Codes, Standards or Regulations which become requirements, to include an admittedly (and documented) hazardous appl icat ion. This action promulgates and provides " j u s t i f i c a t i o n " by implication for unintended use, addit ional danger to patients, and potential l i a b i l i t y . To be unclear about a t o t a l l y unnecessary medical r isk , regardless of degree, is a grave mistake. NFPA text vs. Appendix and Health Care Fac i l i t i es Handbook commentary send contradictory messages.
All of the documentation researched on this subject, and based upon sc ien t i f i c studies and performance test ing, warn against this hazard. Therefore, patient safety and in tegr i t y demand that val id rat ionale for the use of MSVS for WAGD/"evac", i f any, be put before the appropriate assemb]age(s).
Because of the present mixed and contradictory signals, l i fe -suppor t systems' designers, inspectors and c e r t i f i e r s are obligated, in conscience and fo r the i r own legal protection (3CAHO ~andbook: "and for l i t i g a t i o n purposes"), to advise a] l pr incipals involved of the pat ient hazard and attendant l i a b i l i t y .
Participants in the development of documentation containing these warnings include: AANA, AART, ACCP, AORNd, ASA, CGA, UL, USAF, USN, USVA, among many other involved professionals.
The fol lowing includes other references and some applicable excerpts: DESIGN AND Waste Anesthetic Gas Disposal - INSPECTIONS: Vent i la t ion of Anesthetizing Locations.
GOVERNING The applicable, author i ta t ive consensus CRITERIA: documents, a l l of ,~hich c i te the
cautionary rat ionale (of potential hazard.) against the use of Medical-Surglcal Vacuum pumps or systems for WAGD "evac".
1. Potential Pulmonary Barotrauma When Venting Anesthesia Gases To Suction; Sharrock, N.E., and Leith, D.E.; Anesthesiology 46; 152-154; 1977.
2. ANSI Standard Z79.11-1982; American Natioinal Standards Ins t i tu te ; " . . . intended to set minimum performance and safety c r i t e r i a . . ." Scavenging system pressure should "approximate the ambient pressure in normal use." " . . . . rat ionale is provided fo r the requirements in this standard."
3. National Fire Protection Association; Health Care Fac i l i t i es Handbook, 2nd Edit ion, 1987; Rationale and Commentary on NFPA 99: The intent of NFPA Health Care Fac i l i t i es Standard No. 99 (both 1984 and 1987 Editions) is that Medical-Surgical type vacuum pumps, and MSVS systems not be used for WAGD "evac" - and that a separate dedicated ambient d i f f e r e n t i a l , vent i la t ion exhaust, or "micro-vac" blower system be used. (See NFPA Health Care Fac i l i t i es Handbook, '87, 4-7.1.2, pgs. 177-178, and Prologue, Pg. 170. For volumn displacement see pg. 177, l i n e s 13 and 14.
" . . . the maximum safe pressure for the patient shall not exceed (0 negative) -0.5 cm H20 (0.0]446847 " Hg vac. ) . " This is O.OOl2 percent of the MSVS required minimum 12" Hg vac. and "829.3 times the maximum safe degree of negative pressure that should
qbe experienced by the anesthetized patient" and over ]ogo timnes excess degree of vacuum when the MSVS is on stream within i t s normal operating range. Further, no l im i t has been set fo r MSVS maximum degree of vacuum.
4. Hospital Special-Care Fac i l i t ies :(Cl inical Engineering Series); Academic !iPress, 1981 - Chapter 14: / ' . . . preferable (WAGD) disposal method . . . a i r conditioning (vent i la t ion) . . .exhaust . U "Advantages . . . not hazardous to the pat ient . . . is economical . . . negative pressure is low . . . no special machinery is necessay . . . and is safe because the pressures (negative) are inherently l imited . . ."
5. The Br i t ish Standards Ins t i tu te and The International STandards Organization both oppose the user of the MSVS for WAGD-"evac" because of the "very onerous safety problems" which "can seriously a f fect pat ients." (See reference 3 above.)
Ref. ] above: " . . . another potential hazard For the pat ien t and anesthesiologist.." i f " . . , each scavenger valve tested ilfailed to function safely when wall suction was applied to the exhaust po r t . " "Such subatmospher~c 'pressures may induce @ulmonary edema Or at lectas is , J and . . . could result in cardiovascular collapse or trauma to pulmonary parenchyma."
Ref. 2 above: ". . . in normal use some scavenging apparatus, even when operating properly, can a l te r the normal character ist ics of an anesthetic breathing machine . . ."
At i t s October ]2, 1988 meeting the NFPA Health Care Fac i l i t i es Technical Committee members were advised by John P. Swope, M.D., Chairman, Anesthesia Services Subcommittee, that the use of the Medical-Surgical Vacuum System fo r WAGD/"evac" can be hazardous to the anesthetized patient, confirming that hazard reported to NFPA Technical Committee on Medlcal-Surgical Vacuum Systems meeting May 6, 1980 by telephone comn~unication from 3.H. Lecky, I~ M.D., Chairman, ANSI Z79.11 ,Committee.
The fact of tffe hazard was accepted by the NFPA Health Care Faci. l i t ies Technical Committee, Without discent, at i ts meeting on October 12, 1988.
Proper design and appl icat ion of l i fe-suppor t systems in health care f a c i l i t i e s , and the meticulous avoidance of any degree of pat ient hazard, are essential " fo r various agencies, including government and insurance agencies, for l i : t igat ion purposes" (JCAHO Handbook).
For se l f -protect ion and, especial ly, that of the patient, i t is incumbent upon prudent professionals to advise the i r cli.ents accordingly. qOMMITTEE ACTION: Hold For Further Study. COMMITTEE STATEMENT: I t is recognized that there are r isks associated with WAGD being used with Medical/Surgical Vacuum Systems. However, deleting text would not provide any guidance on subject. Subcommittee on Vacuum Systems intends to review subject fo r next edi t ion of NFPA 99.
[Technical Committee believes issue needs study. I f Subcommittee on Vacuum Systems does not want to address issue, Technical Committee wi l l assign task to another Subcommittee.]
119

(Log #68) 99 - 49 - (4-8.1.1.2(a)): Accept SUBMITTER: D.A. McWhinnie, Hickory H i l l s , I l l COMMENT ON PROPOSAL NO.: 99-146 RECOMMENDATION: Delete "Type K". SUBSTANTIATION: The Subcommittee Statement is a non-response - - only a restatement of what is widely known and clearly stated throughout a l l NFPA documents; that materials, components, devices, etc., etc. which meet or exceed NFPA minimum requirements are acceptable.
The reference proposed for deletion is not only redundant (with the above paragraph), but is unnecessry for this application and, therefore, inappropriate in the body of text which should state only minimum safer criteria/performance,
Designers are s t i l l requirin~ Type K for a l l systems (the easy way out) while suppllers furnish hospitals with both pressure and vacuum components which far exceed the requirements and v io late, simultaneously, contract document's requirements. The suppliers save money, the designers are safe, and, as usual, the hospital is the only one involved who pays for what is unnecessary, while a l l others benefit.
Both the Subcommittees have actual, current, project specifications in f i l e (documented) which prove al l the above.
And anv of the materials named in this section for WAGD is ludicrous - - (and i t has happened - - requiring Type K copper). COMMITTEE ACTION: Accept.
(Log #67) 99 - 50 - (4-8.1. I .2(c)) : Accept in Principle SUBMITTER: D.A. McWhinnie, Hickory H i l l s , I l l COMMENT ON PROPOSAL NO.: 99-145
I RECOMMENDATION: After f i r s t word of the second l ine ("piping"), delete the comma and add "or ductwork,", SUBSTANTIATION: For consistency with 4-4.1.2.1(a), Log I13, and for the same reason.
I COMMITTEE ACTION: Accept in Principle. I. Accept Submitter's Recommendation. 2. Add "Vacuum" at beginning of Sentence I.
COMMITTEE STATEMENT: To further correlate with changes of Proposal 99-145.
(Log #69) 99 - 51 - (4-8.1.1.6(e)): Reject SUBMITTER: D.A. McWhinnie, Hickory H i l l s , I l l COMMENT ON PROPOSAL NO. : 99-179 RECOMMENDATION: Add "or rises to 20" ( in. ) Hg". SUBSTANTIATION: (a) Subcommittee Statements are unsupported;
I. Medical-Surgical Vacuum Systems have been operating betwen "an operating range of 15 in. to 19 in. Hg - - . . . at the receiver", and hundreds of such systems have been doing so for over 35 years, and in accordance with present 4-9.1.3.3 Note.
2. Subcommittee Statement is unsubstantiated. "May rest r ic t " is an unexplained conjecture, and doesntt j us t i f y that contention regarding the scope 4-1.4, " for patient drainage, aspiration, and suction(ing)", and the "operating range of 15 in. to 19 in. Hg" presently in 4-9.1.3.3.
3. Is a non-response considering that the Subcommittee has agreed on the topic of "an operating range of 15 in. to 19 in. Hg". There's no rationale for higher than 19 in. Hg.
4. Untrue. Most vacuum regulators for suctioning of patients are calibrated to only 200 mm Hg, or approximately 8 in. Hg, and many have '!hi-vac" lettered above 8 in. Hg - - some with a red pie-shaped area above 8 in. Hg. Why? Because the potential for patient trauma [" to sensitive tissue, such as delicate neonatal, eye, pulmonary, etc., surgery, and collapse of capil laries/venules (Log #142 (Proposal 99-179 in TCR))] increases in proportion to the increase in the degree of vacuum.
(End of comment on Subcommittee "Statements".) (b) To increase any hazard beyond the level of
maximum/optimum performance is not consistent with NFPA prime objectives of safety, nor with AHA cost containment ef for ts.
There is no benefit above 19 in. H~ - - only increased hazard. The "operating range of 15 in. to 19 in. Hg" (4-9.1.3.3) was selected because, at i ts lowest point (15 in. Hg), i t is above the maximum f lu id displacement of patient aspiration/suctionlng equipment in i ts most c r i t i ca l application. Nothing is gained above 12/13 in. Hg as indicated in curve D: (See chart on next page.) COMMITTEE ACTION: Reject. COMMITTEE STATEMENT: I. There have been no demonstrated hazards shown for high vacuum in piped systems.
2. There are hospitals that operate at greater than 20 in. Hg without reports of incidents.
3. Operating level of pumps is not germain to issue of alarming and high vacuum.
4. There is no need to set high l im i t for the vacuum piping system. There are external means to address this issue, but that is not within scope of Subcommittee on Vacuum Systems.
(Log #64) 99 - 52 - (4-8.1.1.8): Accept ~ : D.A. McWhinnie, Hickory H i l l s , I l l COMMENT ON PROPOSAL NO.: 99-181 RECOMMENDATION: Delete 4-8.1.1.8 (Proposal 99-181).
Under (new) 4-8.1.1.8 ( " Ins ta l la t ion of Piping System") leave present "(a) 3oints" (etc'.), and ~_~_:
(b) "Flux" (etc.) (from deleted 4-9.1.2.1). (c) "Cleaning" (etc.) (from deleted 4-9.1.2.2). (d) "Purging" (etc.) (from deleted 4-9.1.2.3). (e) "Threaded Conns." (etc.) (from deleted
4-8.1.1.9). (f) "Pipe Ident i f icat ion" (etc.) (from 4-I0.4.1.1). Delete 4-8.1.1.9 (now 4-8.1.1.8(e)). Add new 4-10.4.1.1 "Piping Distr ibution System.
Shall conform to 4-8.1. I .8." Delete 4-I0.4.1.5; and add new 4-8.I.1.7(c) (from
deleted 4-10.4.1.5). In new 4-8.1.1.7(c) add "continuous reading and"
between "shall be" and "manufactured". new 4-10.4.1.5 "Gauge Ident i f icat ion. Shall
conform to 4-8.1.1.7(c)." lo_R~]_Q_~_t_~ 4-10.4.1.2 and 3 to 4-8.1.I .3; and
4-10.4.1.4 to 4-8.1.1.4. (Renumber accordingly.) SUBSTANTIATION: The Subcommittee Statement [Log 130 (Proposal 99-181 in TCR)] of bel ief and intent is correct. Although poorly worded i t was intended as above [ in second sentence, (Proposal 99-181 in TCR)], but d i f f i c u l t to implement. These are al l designer/suppl ier/ instal ler requirements, and do not belong under "administration". COMMITTEE ACTION: Accept.
120

H.F..~T ~AT.
VAC (Suc
_Dis.?lace_~ent.re!!ul.ts from CGA/NFFA laboratory tests_of
12
! F ~ - ~ - - - L - ~ - - ~ . ~ | o - - - l - - - i ~ r - - - J - - ~ , A l l above measurements i ~ V - J ' ! ~.~'-] .... I ~ _ " ' ~'were reconfirmed 3/2/88
' i..k----~.--'=~------~-~-%L--~-----~----~a-~IA..~.'.---- ~ ~ : ;by a hospital Chief
| 2 3 4 5. 6 7 8 9 10 I I 12 13 I
121
(Log #65) 99 - 53 - (4-9.I .3.3): Accept SUBMITTER: D.A. McWhinnie, Hickory Hi l ls , I l l COMMENT ON PROPOSAL NO.: 99-133 RECOMMENDATION: Delete second and third sentences. (Leave "Note".) SUBSTANTIATION: There are twj d i f ferent vacuum characteristics covered under 4-9.1.3 t i t l e :
4-9.1.3.1 covers minimum vacuum flow (volume) "3 SCFM".
4-9.1.3.3 covers minimum vacuum pressure "12 in. Hg". "Calculated demand" (in SCFM) is mentioned only as
the basis for maintaining the 12 in. Hg minimum degree of vacuum (when displacing the "calculated demand").
That demand is already covered in 4-9.1.3.1 ("3 SCFM"), in 4-I0.2.1.4 [" f ree a i r (SCFM)"] and in C-4-3. I (b) ( "SCFM" and "Adjusted SCFM").
All projects, as last paragraph above, in their design and contract specifications are expressed in "SCFM".
This is because the performance of patient suction equipment results ~ from the movement of local a i r ("SCFM") and i t is the only factor in determining the "calculated demand".
Consistency with 4-9.1.3, 4-9.1.3.1, 4-I0.2.1.4 and C-4-3.1(b).
[This original "Proposal and Substantiation (Log 136) (Proposal 99-183 in TCR)" was badly prepared and poorly stated.]
Above meets the Subcommittee Statement (which was proper). Proposed change leaves Subcommittee intent (Log #136 [Proposal 99-183 in TCR]) intact: "sets minimum vacuum level, and only a recommended operating range. ,i COMMITTEE ACTION: Accept.
(Log #18) 99 - 54 - (5-4.1.1): Accept in Principle SUBMITTER: Saul Aronow, Technology in Medicine, Ind. COMMENT ON PROPOSAL NO.: 99-184 RECOMMENDATION: Do not delete 5-4.1.1.
Retain the present paragraph, but change the l imi t of "50%" to "65%".
Revise the Note to read: "The maintenance of moderate humidity reduces the
hazard of electrostat ic discharge. Such discharges may cause involuntary star t le reaction by s ta f f and are of increasing concern in damaging digi tal electronic equipment. In addition, there are numerous medical hazards associated with the maintenance of low relat ive humidity. These include possible hyperthermia, increased f loat ing particulate matter and increased risk of wound infect ion." ~UBSTANTIATION: I. With reference to the proposal, i t is true that I - I cites the primary hazards, but i t also says "include other hazards associated with the primary hazard."
2. Increasing the upper l imi t of humidity would make control easier to achieve with no essential hazard increase.
3. Revising the note recognizes some direct primary hazards and puts less emphasis on associated hazards. COMMITTEE ACTION: Accept in Principle.
I. Retain subject of humidity control for nonflammable anesthetizing locations.
2. In existing 5-4.1.1, change "within the range of 35 to 50 percent" to read "at a level of 35 percent or greater."
3. In the NOTE to existing 5-4.1.1: a) Delete sentence I. b) Change sentence 2 to read:
"Advantaqes claimed for humidity include avoidance of hypothermia inpatients, especially . . . that the incidence of wound infections may be minimized. [Changes underlined.] COMMITTEE STATEMENT: I. NFPA 99 is a highly referenced document. Deleting subject of humidity control for nonflammable anesthetizing locations wil l send an erroneous signal to other standards organizations. Subcommittee on Anesthesia Services reiterates i ts previous contention that i t can not exclude the possib i l i ty of humidity affecting f i r e susceptibi l i ty in oxygen enriched atmospheres.
2. Setting minimum level is the major concern. Humidity levels can be higher than 35 percent and not create problems.
3. Submitter's proposed NOTE is conjectural. Startle reaction and damage to digi tal electronic equipment, as a result of low humidity in anesthetizing locations, has not been fu l l y demonstrated. Modern design considers the la t te r problem.
Wording in NOTE of existing 5-4.1.I reflects opinions regarding the advantages of humidification. Modification to NOTE is only to more clearly l i s t these advantages.
(Log #19) 99 - 55 - (7-2.2.2): Accept SUBMITTER: Saul Aronow, Technology in Medicine, Ind. COMMENT ON PROPOSAL NO.: 99-195 RECOHMENDATION: In the second sentence of the proposal, change " f lu ids" to "moisture".
In the third sentence, change " f lu ids" to " l iquids". SUBSTANTIATION: Editor ial . Fluids includes gases as well as l iquids, and the intent is not to deal with gasses. COMMITTEE ACTION: Accept.
(Log #36) 99 - 56 - (7-5.1.3.3(c)): Accept SUBMITTER: Floyd a. Devore, HIMA COMMENT ON PROPOSAL NO.: .99-212 RECOMMENDATION: Change the last sentence from " . . . up to a maximum mult ip l ier of 100.", to " . . . up to a maximum of I0 milliamps". SUBSTANTIATION: The req,;rement as written would allow 50 milliamps for equipmet,, covered under paragraph 7-5.1.3.5 Exception No. 2. The l imi t for equipment in patient care areas, as stated in ANSI/AAMI Standard ES-I, is lO milliamps. This would also be consistant with UL544 27.2 Exception, and IEC 601-I. COMMITTEE ACTION: Accept.
• (Log #37) ~ 9 9 - 57 - (7-5.1.3.5): Accept ~SUBMITTER: Floyd 3. Devore, HIMA
,)COMMENT ON PROPOSAL NO.: 99-212 [IRECOMMENDATION: Change the second sentence from "The l ~ l i m i t sha l lbe 100 microamps", to "The l imi t shall be I1100 microamps with the ground intact and 500 microamps I with the ground open." I Delete Exception 1 and Exception 2.
SUBSTANTIATION: The change proposed is consistent with IEC 601-I which has been proven acceptable by the European community for more than ten years.
Exception No. 2 states that the 500 microamps is not a hazard as long as the ground connection is intact; and calls for a periodic check of the ground. However 7-5.1.3 and Figure 7-5.1.3 indicate that the l imits, 100 microamps normal and 500 microamps for the Exception, apply both with the ground open and intact. This would allow the 500 microamps with the ground intact.
The periodic maintenance requirements are called out in 7-6.2.3.6 (proposed 7-5.2.2) and should not be called out here. COMMITTEE ACTION: Accept. COMMITTEE STATEMENT: This subject was extensively discussed by Subcommittee on Electrical Equipment at i ts April 27, 1989 meeting, and by Technical Committee on Health Care Faci l i t ies at i ts June 19/20, 1989 meeting.
(Log #38) 99 - 58 - (7-5.1.3.6): Accept in Part SUBMITTER: Floyd 3. Devore, HIMA COMMENT ON PROPOSAL NO.: 99-212 RECOMMENDATION: I. Change the last sentence of 7-5.1.3.6(b) from " . . . less than lO microamps" to " . . . less than lO microamps with the ground intact, and 50 microamps with the ground open."
122

2. Change the requirement o f 7-5.1.3.6(c) from ". • . less than 20 microamps in each case" to " . . . less than 20 microamps in each case with the ground intact , and 50 microamps with the ground open."
3. Change the requirement of 7-5.1.3.6(e) from ". • . less than lO microamps . . ." to ". , . less than 10 microamps with the ground intact , and 50 microamps wiEh the ground open." ~UBSTANTIATION: The change proposed is consistent~vith IEC 601-I which has been proven acceptable by the European community for more than ten years. COMMITTEE ACTION: Accept in Part.
I. Accept 2. Reject 3. Accept
COMMITTEE STATEMENT: 2. The test with open-ground is not technical ly appropriate. The worst case condition is with ground intact .
Additional Committee Statement:: a. While commentator's substantiation is inadequate,
Committee believes the changes accepted wi l l not s ign i f i can t l y compromise patient safety based on current sc ien t i f i c information.
b. Additional data reviewed by S/C oh Electr ical Equipment included:
I. Report on August 17, 1988 IEC meeting in Boston, MA.
2. Paper included with presentation to T/C on Health Care Fac i l i t i es on October 13, 198B.
3. Ar t ic le by A. Lipschultz on subject in January .1989 issue of JAAMI.
4. Crit ique by S. Aronow on A. Lipschultz's a r t i c l e . [Copies of this material are avai lable for review at
NFPA Headquarters.] c. Subject was extensively discussed at Apri l 27,
1989 meeting of S/C on Electr ical Equipment.
(Log #39) 99 - 59 - (9-2.1.13.3): Accept SUBMITTE_RR: Floyd J. Devore, HIMA COMMENT ON PROPOSAL NO.: 99-212 J RECOMMENDATION: Change the requirement of (2) from ". • • up to a maximum mult ipl ier ' of IO0.", to ". . . up to a maximum of 10 mill iamps." SUBSTANTIATION: The requirement as wri t ten would allow 50 milliamps for equipment covered under paragraph 7-5.1.3.5 Exception No. 2." The l im i t for equipment in patient care areas, as stated in ANSI/AAMI Standard ES-I, is IO milliamps. This would also be consistent with UL544 27.2 Exception, and IEC 601-I. COMMITTEE ACTION: Accept. --L
(Log #40) 99 - 60 - ( 9 - 2 . 1 . 1 3 . 4 ) : Accept SUBMITTER: Floyd J. Devote, HIMA COMMENT ON PROPOSAL NO.: 99-212 RECOMMENDATION: Change the requ i rement from " . . . sha l l not exceed lO0 microamps . . . " to " . . . sha l l not exceed 100 microamps with the ground intact and 500 microamps with the ground open." SUBSTANTIATION: The change proposed is consistent with IEC 601-I which has been proven acceptable by the European community for more than ten years. COMMITTEE ACTION: Accept. COMMITTEE STATEMENT: I. No data submitted disputing recommended 500 microampere l im i t .
2. The 500 microampere l im i t would be in concert with IEC requirements.
[Subject was extensively discussed at Apri l 27, 1989 meeting of Subcommittee on Electr ical Equipment, and at June 19/20, 1989 meeting of Technical Committee on Health Care Fac i l i t i e s . ]
(Log #41) 99 - 61 - (9-2,1.13.5): Accept in Part SUBMITTER: Floyd J. Devote, HIMA COMMENT ON PROPOSAL NO.: 99-212
I ECOMMENDATION: I. Change requ.lrement for (b) from ". . . less than 10 microamps" to ". . . less than lO mlcroamps with the ground intact , and 50 mlcroamps with tile ground open."
2. Change requirement fo r (c) from " . . . less than 20 mlroamps . . . " to " . . . less than 20 m~croamps with the ground intact and 50 microamps with the ground open . . ." and from ". . . less than lO microamps . • ." to ". . . less than lO microamps with the ground intact , and 50 microamps with the ground open . . ."
3. Change requirement for (e) from " . . . less than lO microamps . . ." to " . . . less than lO microamps with the ground intact , and 50 microamps with the ground open . ~ ." SUBSTANTIATION: The change proposed is consistent with IEC 60l-I which has been proven acceptable by the European community for more than ten years. COMMITTEE ACTION: Accept in Part.
I. Accept 2. Reject 3. Accept
COMMITTEE STATEMENT: Proposed changes are essent ia l ly the same as those in Comment 99-58 (Log #38). Committee Statement is applicable to this comment as well. ..
_ _ m
(Log #31) 99 - 62 - ( 1 9 - 2 . 1 . 1 ) : Hold f o r Fur ther Study ~ : Paut J. S h e f f i e l d , O f f i c e of the U.S. A i r Force Surgeon General COMMENT ON PROPOSAL NO.: 99-261 RECOMMENDATION: Request that proposal 99-261 (Log #47) be accepted. SUBSTANTIATION: The purpose of this proposal is to provide fo r equal f i r e safety treatment of Class A and Class B chambers. I f there is a val id requirement for two-hour separation construction, the requirement should apply equally to multiplace Class A chambers and monoplace Class B chambers. We have consulted the Air Force hyperbaric f a c i l i t y experts at USAFSAM, Brooks AFB, TX, and the Navy hyperbaric cer t i f icat ' ion experts at the NAVFAC System Cer t i f i ca t ion Authori ty, Alexandria, VA, and we can f ind no rat ionale to j u s t i f y d i f fe ren t safety standards based on number of chamber occupants. Thus, we take Exception to the Committee statement as fol lows:
(a) The "str ingent Exception" referred to in the Committee statement is not unique to Class B chambers. Class A chambers also comply with the "str ingent Exception." Since both Class A chambers and Class B chambers present the same undo hazard to those in surrounding rooms, Class B chambers should not be exempted i f there is a val id requirement to ' have two-hour separation construction, r
(b) Subsequent to the wr i t ing of this.standard, the application of Class B chambers has changedL Some Class B chambers have been used for more than one occupant (1). Some Class B chambers are now equipped with vent i la tors or oxygen masks that enable patients to be treated at greater pressure (2-8.3 ATA) and on intermit tent a i r breathing (2,3) Hyperbaric oxygen therapy l i t e ra tu re has carried several recent a r t i c les encouraging the treatment of a i r embolism and decompression sickness in Class B chambers (4,5). The current thrust for Class B chambers to t reat a i r embolism and decompression sickness cases prevents the chamber from rapidly ascending to the surface, making the ascent time the same as Class A chambers. Regardless of the type of chamber, rapid ascent of a decompression sickness or a i r embolism patient wi l l have the same negative outcome. Thus, the room in which e i ther a Class A or Class B chamber is located requires the same protection from f i res outside the room. The fol lowing references describe the changes in use of monoplace Class B chambers that make the i r use more l i ke mult~place Class A chambers. I f there is a val id requirement fo r two-hour separation construction, the current expanding use of Class B chambers preclude the i r exemption from the requirement.
1. Martorano, FJ and Hoover, B. The Child Hyperbaric Patient. J. Hyperbaric Medicine:f986: I ( I ) :15-21 i
2. Weaver LK. Air Breaks with the Sechrjst 500A Monoplace Hyperbaric Vent i la tor . J. Hyperbarlc Medicine 1988 3(3):179-186
3. Raleigh, G.W. Air Breaks in the Sechrist Model 2500B Monoplace Hyperbaric Chamber. J. Hyperbaric Medicine 1988 3(I):11-14
123

4. Hart, GB, Strauss, MB, and Lennon, PA. The Treatment of Decompression Sickness and Air Embolism in a Monoplace Chamber. 3. Hyperbaric Medicine 1986, (1 ) :1 -7
5. Kindwall, E.P., Goldmann RW and Thombs PA. Multlplace Chamber in the Treatment of Diving Diseases. J. Hyperbaric Medicine 1988 (3)(I)5-10
[Copies available from Secretary, NFPA Standards Council, NFPA Headquarters.] COMMITTEE ACTION: Hold for Further Study. COMMITTEE STATEMENT: I. Class A and B chambers do not present the same f i re hazards because there is a significant difference in volume of gases within each type.
2. Class B chambers using oxygen can be quickly brought to ambient atmosphere (less than 1 minute) i f a f i re occurs in the fac i l i t y .
3. The Subcommittee on Hyperbaric and Hypobaric Facil i t ies is aware that the current definitions (cr i ter ia) for Class A and B chambers are now oversimplistic in l ight of the way chanmbers are operated today, the type of gases used, the volumes of gases employed, the pressures involved and the number of occupants inside. The Subcommittee intends to review this problem for the next Edition of NFPA 99.
[This subject Was extensively discussed at the May 1, 1989" meeting of the Subcommittee on Hyperbaric and Hypobarlc Faci l i t ies. ]
[Technical Committee on Health Care Facil i t ies recognizes that the state of technology is changing. I t has also been advised that the Undersea Medical Society is studying this issue, and revising a document on subject. Changes wi l l affect NFPA 99, and wi l l be addressed for next edition of NFPA 99.]
(Log #44) 99 - 63 - (19-2.1.I): Hold for Further Study SUBMITTER: Wilbur T. Workman, USAF School of Aerospace Medicine COMMENT ON PROPOSAL NO.: 99-261 RECOMMENDATION: Request that Proposal 99-261 (Log #47) be accepted. SUBSTANTIATION: I t is the intent of this proposal to provlde for the equal treatment of Class A and Class B chambers with regards to f i re safety. Assuming the requirement for a two-hour separation construction is a valid one, there should be no differentiation based on the type of chamber and therefore, Class A and Class B chambers should be treated equally. Historically, this distinction has been based upon the number of occupants the chamber can accommodate. This office cannot understand the basis for this position.
With specific reference to the Committee Statements on this proposal, the following exceptions are noted:
(a) What differentiates Class A and Class B chambers when both chambers routinely comply with the "Stringen,t Exception" cited in paragraph 19-2.1.2 of the Code? Class A chambers comply with the requirements for d~scharge of effluent gases. Therefore, in this re~ard, both chamber types are installed using the same cr l ter ia. As a result, the hazards presented to those in adjacent areas is equivalent. I f there is a valid requirement for the two-hour construction separation, then Class B chambers should not be exempt.
(b) With increasing numbers of Class B chambers being placed into operation throughout the country, i t is a logical progression tht they be used to treat a greater variety of disorders. As more cr i t ica l ptients are being treated in these types of chambers, some treatments actually requiring an inside medical attendant (for example in the treatment of infants and small children in Class B chambers). Many of these chambers are even being retro-f i t ted to allow the chamber to be pressurized with compressed air, with 100 percent oxygen being administered to the patient via an oro-nasal mask. In this configuration, the concept of oxygen delivery to the patient is the same in both chamber classifications. Use of Class B chambers in this manner puts them into the same operational mode as Class A chambers with the same decompression
limitations. In such a case, the amount of time to safely decompress the air embolism or decompression sickness patient is the same for both types of chambers. Time has shown that Class B chambers are being used more l ike Class A chambers and, as such, should not be exempt from the requirement.
(c) This office has conferred with the Office of Device Evaluation of the Food and Drug Administration regarding this issue. I t is the opinion of a reviewer in that office that the standards should not be based on the type of chamber in operation; safety standards should be equally applied. COMMITTEE ACTION: Hold for Further Study. COMMITTEE STATEMENT: See the Committee Statement for Comment 99-62 (Log #31) since i t is applicable here as well.
(Log #33) 99 - 64 - ( 1 9 - 2 . 1 . 1 . 2 ) : Hold f o r Fur ther Study SUBMITTER: Paul O. S h e f f i e l d , O f f i ce o f the U.S. A i r Force Surgeon General COMMENT ON PROPOSAL NO.: 99-262 RECOMMENDATION: Request that Proposal 99-262, (Log #49), be accepted. SUBSTANTIATION: The purpose of this proposal is to provide for equal f i re safety treatment of Class A and Class B chambers. I f there is a valid requirement to reserve a room exclusively for the use of a chamber, we see no difference in the f i re safety requirement for multiple occupancy Class A chambers and single occupancy Class B chambers. Subsequent to the writing of this standard, new chamber designs were introduced that challenge the currently accepted designation of Class A and Class B chambers. For example, some models of Class A chambers for two to three occupants are portable. Conversely, Dr. George B. Hart, former president of the Undersea and Hyperbaric Medical Society, has reported that, on occasion, treatments in Class B chambers have included an infant and an adult, which, under the current definition, would classify i t as a Class A chamber. Art icle by Martotano and Hoover (1986) is available for review from NFPA Headquarters. We feel that the presence of a second chamber occupant has no bearing on the exclusive use of the room. I f there is a valid requirement for exclusive use of the room for hyperbaric chambers, the rule should apply equally to Class A and Class B chambers, whenever the chamber is present. COMMITTEE ACTION: Hold for Further Study. COMMITTEE STATEMENT: I. Traditional Class A chambers (as are s t i l l defined) were of a size that they were not movable. They presented a greater f i re hazard than Class B chambers because of their customarily larger volume (and thus more gas) than B chambers.
2. See also Comment No. 3 under Committee Statement for Comment 99-62 (Log #31) relative to issue of definitions of Class A and B chambers since i t applies here as well.
(Log #45) 99 - 65 - ( 1 9 - 2 . 1 . 1 . 2 ) : Hold f o r Fur ther Study SUBMITTER: Wi lbur T. Workman, USAF School o f Aerospace Medicine COMMENT ON PROPOSAL NO.: 99-262 RECOMMENDATION: Request Proposal 99-262 (Log #46) be accepted. SUBSTANTIATION: The i n t e n t o f t h i s proposal is to prov ide f o r equal f i r e p r o t e c t i o n o f Class A and Class B chambers. The argument tha t Class 8 chambers are po r tab le is not v a l l d . There are inc reas ing numbers of Class A chambers tha t are a lso po r tab le (suppor t ing mater ia l a v a i l a b l e f o r review a t NFPA Headquarters) . I t has been repor ted in the l i t e r a t u r e tha t Class B chambers are being used more l l k e Class A chambers (suppor t ing mate r ia l a v a i l a b l e f o r review at NFPA Headquar ters) . Apply ing the s t r i c t chamber c l a s s i f i c a t i o n c r i t e r i a , when Class B chambers are used
124
in this manner, they become Class A chambers. The number of chamber occupants has no bearing on the exclusive use of .the room, nor does the portabi l i ty of the chamber. I f the requirement for the exclusive use of a room for hyperbaric purposes is valid, then there should be no exception with the Code applying equally to both chamber types. COMMITTEE ACTION: Hold for Further Study. COMMITTEE STATEMENT: Committee agrees that the number of chamber occupants may not be valid for determining exclusivity of use of room. How()ver, Committee also recognizes problem with existing definitions of Class A and B chambers. [See Comment No. 3 under Committee Statement for Comment 99-62 (Log #3]) since i t applies here as well.]
(Log #46) 99 - 66 - (19-2.1.2): Hold for Further Study SUBMITTER: Wilbur T. Workman, USAF School of Aerospace Medicine COMMENT ON PROPOSAL NO.: 99-264 RECOMMENDATION: Request Proposal 99-264 (Log #48) be accepted. SUBSTANTIATION: Given the assumption that the "Exception" cited in paragraph l!)-2.1.2 is valid, i t should apply to both Class A and Class B chambers. The vast majority of Class A chamber:; also comply with this Exception. The Committee statement referred to the fact that Class B chambers have shown to have a reasonable level of safety. This is also true for Class A chambers. This office knows "of no evidence indicating that Class B chambers are any more safe than Class A chambers. The rationale presented for Proposal 99-261 (Log #47) also appl iesto this proposal. COMMITTEE ACTION: Hold for Further Study. COMMITTEE STATEMENT: Intent of Exception, and the traditional definit ion for Class B chambers, recognized a significant difference in the volume of gases within each class of chamber; thus, Exception was intended only for Class B chambers. [See also Comment No. 3 under Commlttee Statement for Colmnent 99-62 (Log #31) on issue of definitions of Class A and B chambers.]
(Log #34) 99 - 67 - ( ]9-2. l .2): Hold for Further Study ~ : Paul J. Sheffield, Office of the U.S. Air Force Surgeon General COMMENT ON PROPOSAL NO.: 99-264 RECOMMENDATION: Request that Proposal 99-264, (Log #48), be accepted. SUBSTANTIATION: The purpose of "this Proposal is to provide for equal f i re safety treatment of Class A and Class B chambers. I f there is a valid just i f icat ion for the "Exception," i t should apply to both Class A and Class B chambers. Like some portable Class B chambers, most Class A chambers also meet the requirements of this Exception. Like Class B chambers, Class A chambers have also been ;hown to provide a reasonable level of safety. In a thorough review of al l hyperbaric chamber fires documented since the f i r s t NFPA hyperbaric fac i l i t y safety code was implemented ]970, we fai l to find any correlation between numbers of chamber occupants and level of safety. We also fa i l to find any evidence that Class L3 chambers provide a level of safety any better than Class A chambers. In the absence of addressing Class ,~ chambers that would qualify under the "Exception," we feel that i t is inappropriate to grant exceptions to Class B chambers, whose level of safety is no better than Class A chambers. Our rationale for recommending acceptance of Proposal 99-26] (Log #47) is also considered applicable to this proposal. COMMITTEE ACTION: Hold for Further Study. COMMITTEE STATEMENT: Committee Statement for Comment 99-62 (Log #46) applies here as well.
(Log #32) 99 - 68 - (19-2.l.2): Mold For Further Study SUBMITTER: Paul J. Sheffield, Office of the U.S. Air Force Surgeon General ~' COMMENT ON PROPOS~Q~.: 99-265 RECOMMENDATION: Request that Proposal 99-265 (Log #6) be accepted. ~_UBSTANTIATION: The purpose of this proposal is to provide for equal f i re safety treatment of Class A and Class B chambers. I f there is a valid requirement for sprinkler protection in rooms housing Class' A chambers, the requirement should also apply to Class B chambers. We fai l to see a correlation between the number of chamber occupants and the need for protection of l i fe and property. We take exception to the Committee Statement in Proposal 99-26] (Log #47): "For'Class A chambers, operation may have to continue for a longer period of timethan Class B chambers. Thus, the room in which Class A chambers are located require greater protection from fires outside the room . . ." Subsequent to the writing of this standard, the cnncept of use for Class B chambers has changed to include the treatment of decompression sickness and air embolism patients; making ascent rates of Class B chambers more l l ke those of Class A chambers. Articles by GB Hart et al (]988) and Ep Kindwall et a] (]988) are available for review at NFPA Headquarters. Thus we feel that the requirement for sprinkler protection in the room should be the same for Class A and Class B chambers. Our rationale for recommending acceptance of Proposal 99-26] (Log #47) is also considered applicable to this proposal. COMMITTEE ACTION: Hold for Further Study. ~.OMMITTEE STATEMENT: Original classification scheme recognized a difference in f i re hazard between Class A and B chambers. Use today has made the original definitions of Class A and B chambers not completely appropriate. [See Comment No. 3 under Committee Statement for Comment 99-62 (Log #3]).]
(Log #47) 99 - 69 - (19-2.l.2): Hold for Further Study ~ : Wilbur. T. Workman, USAF School of Aerospace Medicine ~gMMENT ON PROPOSAL NO.: 99-265 RECOMMENDATION: Request that Proposal 99-265 (Log #6) be accepted, SUBSTANTIATION: As i n i t i a l l y proposed, thi!s suggestion was to provide for the equal f i re protection for both Class A and Class B chambers. With Class B chambers now being used more l ike Class A chambers (e.g., for the treatment of a i r ambolism and decompression sickness with modifications for oxygen admilnistration via a vast delivery system), the same operational limitations apply as they do for Class A chambers. Of specific note here is the decompression requirements incurred by the patient when he/she has been treated in a Class B chamber as conflgured. I f the requirement for sprinkler protection is valid, i t should apply to both types of chambers. The rationale provided for proposal 99~261 (Log #47) also pertains to this comment. COMMITTEE ACTION: Hold for Further Study.. COMMITTEE STATEMENT: The Committee Statement for Comment 99-62 (Log #32) is applicable for this comment as well.
(Logl#35) 99 - 70 - (19-2.1.3) : Hold fo r Further Study SUBMITTER: Paul 3. She f f ie ld , Of f ice of the U.S. A i r Force Surgeon General i COMMENT ON PROPOSAL NO.: 99-266 RECOMMENDATION: Request that Proposal 99-Z66 (Log #7) be accepted. SUBSTANTIATION: The purpose of th i s proposal is to provide fo r equal f i r e safety treatment of Class A and Class B chambers. I f there is a va l i d reason for sp r i nk le r p ro tec t ion of rooms in which Class A chambers are located, then the ru le would seem to also apply to Class B chambers. Like most Class B chambers, most
125

Class A chambers comply with the "one stringent exception" referred to in the Committee Statement. Thus, there exists a double standard for hyperbaric chambers, depending on the number of occupants. Since Class A chambers also comply with the "one stringent exception", the rationale for exempting Class B chambers from sprinkler protection requirements is not clear. Our rationale for acceptance of Proposal 99-261 (Log #47) is also considered applicable to this proposal. COMMITTEE ACTION: Hold for Further Study. COMMITTEE STATEMENT: The same argument as presented in previous comments is applicable for this comment as well, i .e . , the differences in the volume of gases between Class A and B chambers. Subcommittee on Hyperbaric and Hypobaric Faci l i t ies recognizes classification scheme for chambers needs refining due to changes in technology and use. [See Committee Statement under Comment 99-62 (Log #31).]
(Log #48) 99 - 71 - (19-2.1.3): Hold for Further Study SUBMITTER: Wilbur T. Workman, USAF School of Aerospace Medicine COMMENT ON PROPOSAL NO.: 99-266 RECOMMENDATION: Request Proposal 99-266 (Log #7) be accepted. SUBSTANTIATION: Given the fact tht Class A chambers also comply with the "Exception" referenced in the Committee Statement, the val id i ty of requiring sprinkler protection for Class A chambers and not requiring the same level of protection for Class B chambers is not clear. Basing the requirement on the number of chamber occupants is not fe l t to be valid. There appears to be a double standard in this area. The rationale presented for Proposal 99-261 (Log #47) also applies to this comment. COMMITTEE ACTION: Hold for Further Study. COMMITTEE STATEMENT: Committee Statement for Comment 99-62 (Log #35) is applicable here as well.
(Log #74) 99 - 72 - (A-2-2 and Appendix B): Accept SUBMITTER: Leo G. Foxwell, The Hartford Insurance Group COMMENT ON PROPOSAL NO.: 99-274 RECOMMENDATION: I) Item 2 of the Committee Action should also: add at end of Note 2 "See Appendix B".
2) In Appendix B add a new B-I.2.8 US Pharmacopia Standard for Compressed Air and address. SUBSTANTIATION: Editorial. Committee Action was incomplete.
I COMMITTEE ACTION: Accept. Address for USP is 12601Twinbrook Parkway,
Rockville, MD 20852 Document No, is XXII/NFXVII.
(Log #75) 99 - 73 - (A-2-2): Accept SUBMITTER: Leo G. Foxwell, The Hartford Insurance Group ~O_MMENT ON PROPOSAL NO.: 99-274 RECOMMENDATION: The US Pharmacopla Standards for condensed water and hydrocarbons/liquid, CO and CO 2 are referenced. The actual values should be displayed in the text for c lar i ty. SUBSTANTIATION: The Committee accepted these values, but they should also be printed to make the document user friendly. COMMITTEE ACTION: Accept.
Add following to Note under Committee Action 2 for Proposal 99-274 in TCR:
Air characteristics in USP XXII/NF XVII include: Condensed water (see dew point) Carbon Monoxide lO ppm V/V Carbon Dioxide 500 ppm V/V
(Log #I) 99 - 74 - (A-2-2): Accept ~ : Reginald Nease, Lenexa, KS COMMENT ON PROPOSAL NO.: 99-132, 276 RECOMMENDATION: Delete text referencing dewpolnt of medical air. SUBSTANTIATION: Need for measurement and monitoring of dewpoint of a i r system is established as a requirement text of [NFPA] 99. Statement of l imi t belongs in main body of [NFPA] 99, not in appendix. Excessive water vapor in a medical air system can "constitute a dist inct hazard to l i f e " as stated in 4-3.1.9.8. As such, i t i s the r e s p s o n s i b i l i t y o f the Committee to define dewpoint as a requirement, not a suggestion. COMMITTEE ACTION: Accept.
(Log #30) 99 - 75 - (A-2-2): Reject SUBMITTER: Antonio A. Mesa, Nash Engineering Co. COMMENT ON PROPOSAL NO.: 99-276 RECOMMENDATION: Revise as follows:
"Dew point 39°F nominal at 40 PSIG." SUBSTANTIATION: This wil l c lar i fy the design should be for 39°F pressure dew point, but actual alarm settings should be 50°F to prevent nuisance alarms. Alarms cannot be set at normal operating dew points. A 50°F pressure dew point wi l l provide typical indoor installations with more than the 18°F dew point margin presently Code.
EXAMPLE: An air l ine trave111ng through an air conditioned room'at 72°F wi l l s t i l l have 22OF margin from condensate. This air is s t i l l not saturB~ed. Prior substantiation for 39°F dew point should be reviewed.
A 50°F alarm wi l l warn of deterioration in dryer performance prior to forming in-l ine condensate. Lowering dew point pressure requirements wi l l not prevent dryer malfunction.
[Correspondence attached to public comment is available from NFPA Headquarters.] COMMITTEE ACTIOH: Reject. COMMITTEE STATEMENT: I. Committee Action on Comment 99-74 (Log #I) deleted dew point in Appendix A-2-2.
2. Committee Action on Comment 99-43 (Log #26) clari f ied dew point requirement in text.
(Log #57) 99 - 76 - ( C - 4 - 3 . 1 ( b ) ) : Accept in P r i n c i p l e SUBMITTER: D.A. McWhinnie, H ickory H i l l s , I l l COMMENT ON PROPOSAL NO.: 99-286 RECOMMENDATION: Dele te from " the pumps are ra ted" to " . . . 16 in . Hg vacuum," ( i n c l u s i v e ) and "Note" . SUBSTANTIATION: This material is unrelated to the text, and the requirements of 4-9.1,3, 4-9.1.3.1, 4-10.2.1.4 and C-4-3.1(b), and is never used in A/E design specifications or contract documents for hospital Medlcal-Surgical Vacuum Systems.
The text requirements are al l stated in "SCFM" because this is the only constant, and "SCFM" is the rig_clot factor which powers the patient suction equipment. "ACFM" is constantly changing, is created by and occurs inside the pump and belongs in a text book on fluidics physics.
I t is confusing, unnecessary and has been misinterpreted. (Also see Proposal on 4-9.1.3.3.) COMMITTEE ACTION: Accept in Principle.
I. Accept Submitter's Recommendation. 2. In Appendix C-4-4, revise chart (see on next
page) to reflect SCFM, and revise Note for SCFM. COMMITTEE ~TATEMENT: 2. To correlate with change in Item I (deleting reference to SCFM).
126

o o nr Lu
u .
O o} Lu -r o z -r
W . J W
I1.
N ,< _>
0 W u_
0
8
g e r
m
w n
3
2
1
0.7
0.5
0.3
0.2
0.1
0.07
0.05
50 /
/ .75 /
I J
/
#
/
,/
3
/
Valid for copper tube type L (clean and new)
l
/
W J B , i U | R | i | l
IHF4IBB|Bi W A I r I V J R i ~ i W J K N I B I I M I F A I F I I
iKIF4§HI|F41 igHglH|BI i B ~ R B B I / i i B m
5 7 10 20 30 50 70 100 200 300 l
FLOW, ~ F M @ 15 in. Hg. VACUUM
NOTE: Pressure drops at other vacuum levels may be closely
approximated by dividing the pressure drop found from the chart
(four a given SCFM and pipe size) by the ratio:
30 - new vacuum level 15
/
500 700 1000
Edi tor ia l Changes
1. Proposal 99-195 - In sentence 2 of Submitter's Recommendation, change "defectin!)" to "defect ive".
Reason: Correct typographical er ror .
2. Section 9-2.1.13.3/4/5 in NFPA 99-1987: a) In 9-2.1.13.3, delete " (a) " General"; change " ( I )
Techniques . . ." to "(a) Techniques . . ."; change "(2) Frequency . . ." to "(b) Fr~)quency . . ."; and change "(3) Leakage . . ." to "(c) Leakage . . . " .
b) In 9-2.1.13.4(a), change "!)-2.1.13.3(a)(I) and (2)" to "9-2.1.13.3".
c) In 9-2.1.13.5(a), 9-2.1.13.5(b), 9-2.1.13.5(d), and g-2.1.13.5(e), change "g-2.1.13.3(a)" to "9-2. I. 13.3".
d) In A - 9 - 2 . 1 . 1 3 . 3 , add a t end " (see a ls0 A-7-5.1.3.3)".
e) Delete A-g-2.1.13.3(a). R a _ R ~ : Conform to NFPA Style Manual.
3. For Proposal 99-172 in TCR, add the f o l l o w i n g to Committee A c t i o n :
Add in Appendix, under Table A - 4 - 8 . 1 . 1 . 1 : B i r t h i n g Rooms 2/room A Reason: For coordination with Committee'Action on
Proposal 99-172. Appendix A needs this addit ion as a result of change made in Table 4-8.1.1.1. !
4. In Figure A-4-4.2.12.1(b) and (c), add l ines connecting regulator to e lec t r i c solenoid shut-of f valve (essv).
Reason: Line inadvertant ly missing that shows essv connected immediately down stream from regulator.
127


















