
Alcon Supplement
8
Supplement February 2015 ALCON CENTURION ® VISION SYSTEM COUNCIL MEETING 2014 Sunday 12th October Milan, Italy
description
ALCON CENTURION® VISION SYSTEM COUNCIL MEETING 2014
Transcript of Alcon Supplement

Supplement February 2015
ALCON CENTURION® VISION SYSTEM COUNCIL MEETING 2014
Sunday 12th OctoberMilan, Italy

ALCON CENTURION® VISION SYSTEM COUNCIL MEETING 20141
Introduction by the Chairman(K. Tjia, Zwolle, The Netherlands)
ALCON CENTURION® VISION SYSTEM COUNCIL MEETING PROCEEDING 2014(Milan, 12th October, 2014)Alcon-sponsored event and proceeding
The CENTURION® Vision System Council Meeting was held in Milan on 12th October, 2014 and gathered 14 key opinion leaders in cataract surgery from Europe and the Middle East. They participated in the development of the CENTURION®
Vision System phaco-emulsification machine, or have been users of CENTURION® Vision System since its launch in October 2013 or before. Dr. Johansson started the session by reviewing the settings involved in active fluidics (intra-ocular pressure [IOP], vacuum and pump speed) and the safety boundaries within which surgeons should perform surgery, while Prof. Scharioth presented how to target physiological IOP during the whole duration of the phaco-emulsification. Dr. Aslan talked about reduction of post-occlusion surge. These presentations generated lively discussions around the optimization of settings in Active Fluidics™ technology. This session was followed by some tips given by Prof. Tognetto on how to optimize phacoemulsification efficiency with the INTREPID® Balanced Tip. Dr. Lorente provided an overview of results from clinical studies comparing INFINITI® Vision System and CENTURION® Vision System highlighting the differences between the two systems and improvements brought by CENTURION® Vision System. Applied Integration™ of different technologies with CENTURION® Vision System were also discussed: Dr. Moraru and Dr. Crozafon described the VERION™ Image Guided System and reported their experience using the VERION™ Image Guided System link to CENTURION® Vision System, especially when implanting toric lenses. AutoSert® IOL Injector, the automated lens delivery, which can be controlled via CENTURION® Vision System was also presented by Dr. Mencucci and Dr. Allen, with an emphasis on the potentially reduced wound stretch during the intra-ocular lens (IOL) implantation. Then Dr. Moraru, Dr. Prieto, and Dr. Khalifa showed some videos of interesting, complicated cases, in order to illustrate the CENTURION® Vision System settings can be adjusted to each case. Note that these will not be summarized in this supplement. Finally, Dr. Tjia reported experience gained with the INTREPID® bimanual polymer disposable I/A 23G. This article provides a summary of selected topics and data discussed during the meeting.
Table of ContentsIntroduction By The Chairman 1(K. Tjia, Zwolle, The Netherlands)
Active Fluidics™ Technology 21) Targeting Physiological IOP During Phaco-emulsification 2
(G. Scharioth, Germany/Hungary)
2) Safe Setting With New Fluidics 2(C. Johansson, Kalmar, Sweden)
3) Occlusion Break Surge 2(B. Sıtkı Aslan, Turkey)
Balanced Energy™ Technology 31) Improving Phaco Efficiency Using the INTREPID® Balanced Tip 3
(D. Tognetto, Trieste, Italy)
VERION™ Image Guided System 41) VERION™ Image Guided System Link for the CENTURION®
Vision System 4(O. Moraru, Bucharest, Romania)
2) Femto Laser-Assisted Cataract Surgery with the LenSx® 4 Laser, the VERION™ Image Guided System Digital Markers and the CENTURION® Vision System Phaco Machine – An Outside View (P. Crozafon, Nice, France)
AutoSert® IOL Injector 51) Were the Benefits for the Patients and Surgeons Worth It? 5
(R. Mencucci, Florence, Italy)
Clinical Study Results 61) Prospective Clinical Study Using a New Phaco System 6
with Intraocular System Target Pressure Control (R. Lorente, Orense, Spain)
2) Quantification of Occlusion Break Surge in 6 Peristaltic-Based Phacoemulsification Systems (R. Lorente, Orense, Spain)
References 7
Please refer to the Directions for Use (DFU) for the Alcon products described in this supplement for approved indications.
K. Tjia
P. Crozafon
C. Johansson
R. Mencucci
G. Scharioth
D. Allen
B. Sıtkı Aslan
I. Prieto
D. Tognetto
H. Khalifa
R. Lorente
W. Omulecki
O. Moraru
G. Vogt

ALCON CENTURION® VISION SYSTEM COUNCIL MEETING 2014 2
Active Fluidics™ Technology1) Targeting Physiological IOP During Phaco-emulsification
(G. Scharioth, Recklinghausen/Szeged, Germany/Hungary)
Prof. Scharioth reported his first case handled with the help of CENTURION® Vision System in late summer 2012. Since then, more than 3’000 cases were treated at the Aurelios Eye Centre in Recklinghausen, Germany. The presenter started his presentation
by highlighting the characteristics of the traditional gravity system. The fundamental principle of a gravity system is that the higher the surgeon positions the bottle, the greater the IOP. For the height of 100 cm, the IOP is 74 mmHg. Some risks are however associated with high intra-operative IOP, notably, damage to endothelial cells and optic nerve leading to glaucoma, impairment of retinal/choroidal perfusion, iris prolapse, pain, and increased risk of complications in general.1,2,3
• The characteristics4,5 of Active Fluidics™ technology are 1) preservation of the stability of the anterior chamber at surgeon selected target IOP, 2) reduction of surges (Fig. 1), 3) reduction of stress to ocular tissues, 4) reduction of intra-cameral turbulences, 5) reduction of complications, 6) increased efficacy.
• A study designed to compare phaco-emulsification in three groups (n=50 eyes each) with three different pre-set target IOPs=20, 30 and 40 mmHg showed that the outcomes did not differ significantly between the three groups (presenter’s own data, unpublished). Apart from a few cases of anterior chamber instability (two eyes in the 20-mmHg group, none in the 30-mmHg and one eye in the 40-mmHg), no other complications occurred.
• In conclusion, Prof. Scharioth stated that phaco-emulsification at a lower IOP is well tolerated and efficacious with CENTURION® Vision System and the new Active Fluidics™ technology
Figure 1. Reduced occlusion breaks with the Active FluidicsTM system as compared with gravity systems4
for physiological reasons. The conclusion drawn by the presenter was that Active Fluidics™ technology with CENTURION® Vision System is very permissive, and virtually any setting is appropriate with regard to stability of the anterior chamber.
• Then, IOP fluctuations with occlusion breaks were investigated. In such conditions, it is possible to work at very high vacuum settings. According to the model, a vacuum of 700 mmHg with a flow rate of 60 cc, and a target IOP of 60 mmHg would induce a transient pressure drop from 60 mmHg to 24 mmHg, prior to returning to 60 mmHg.
These data suggest that the CENTURION® Vision System fluidics characteristics are extremely flexible and offer many new options to cataract surgeons. Overall, it is not necessary to set a high target IOP; a stable chamber can be easily maintained for settings under 60mmHg. Setting a low target IOP is possible with CENTURION® Vision System, however a target lower than 35 mmHg requires strong surgical skills.
I n his presentation, Dr. Johansson gave an overview of optimal settings with new fluidics. An essential feature of CENTURION® Vision System is the possibility to set a target IOP and to maintain it throughout the whole procedure. As an additional safety measure, the use of small
bore aspiration tubing with low compliance protects against sharp IOP fluctuations which could otherwise occur upon occlusion breaks. The question what ranges or intervals within which parameters can be adjusted are adequate? To answer this question, Dr. Johansson used a fluidics model, based on measurements in a test chamber without leakage. Raw data were then transformed into a mathematical model of the system. • First of all, the results obtained in a steady state without occlusion
showed that the IOP is the same as the target IOP up to 70 mmHg, independently of other settings. At a very high target IOP, in combination with very high pump settings (700 mmHg and an aspiration rate of 60 cc), IOP can be lower than the target IOP. However, such high target IOP and settings are not recommended
2) Safe Setting with New Fluidics (C. Johansson, Kalmar, Sweden)
3) Occlusion Break Surge (B. Sıtkı Aslan, Ankara, Turkey)
Dr. Aslan shared his experience in managing occlusion break surges. He cited data sources indicating that the incidence of vitrectomy was 0.62% (n=17 patients) of a cohort of 2,758 cases treated with INFINITI® Vision System. Posterior capsular tear occurred
during phaco-emulsification in 0.82% of cases (n=14). Surge caused 64% of the reported capsular tears. In contrast, none of the patients included in a group (n=393) due to undergo surgery using CENTURION® Vision System necessitated vitrectomy. In this context, the goal to reach is the reduction of surge incidence (unpublished data – author’s own experience). • The amplitude of occlusion break surges is reduced with the Active
Fluidics™ technology system as compared with procedures using gravity. The surges can be controlled by setting up parameters in the machine itself (vacuum, aspiration flow and irrigation pressure). The surgeon can also have an impact on the occurrence of surges,
by decreasing the effective flow rate (use of a smaller aspiration port, e.g. Microflow tip), increasing the infusion rate and proper wound construction. A too large (thus leaky) wound or a too tight wound can increase the surge.
• Dr. Aslan communicated on results obtained from a study comparing 25 cases using Active Fluidics™ technology and 25 cases receiving passive infusion by gravity (presenter’s own data, unpublished).
• The average number of surges was lower with Active Fluidics™ technology than with passive (gravity) infusion: 0.12±0.33 vs. 0.44±0.58 (p=0.021).
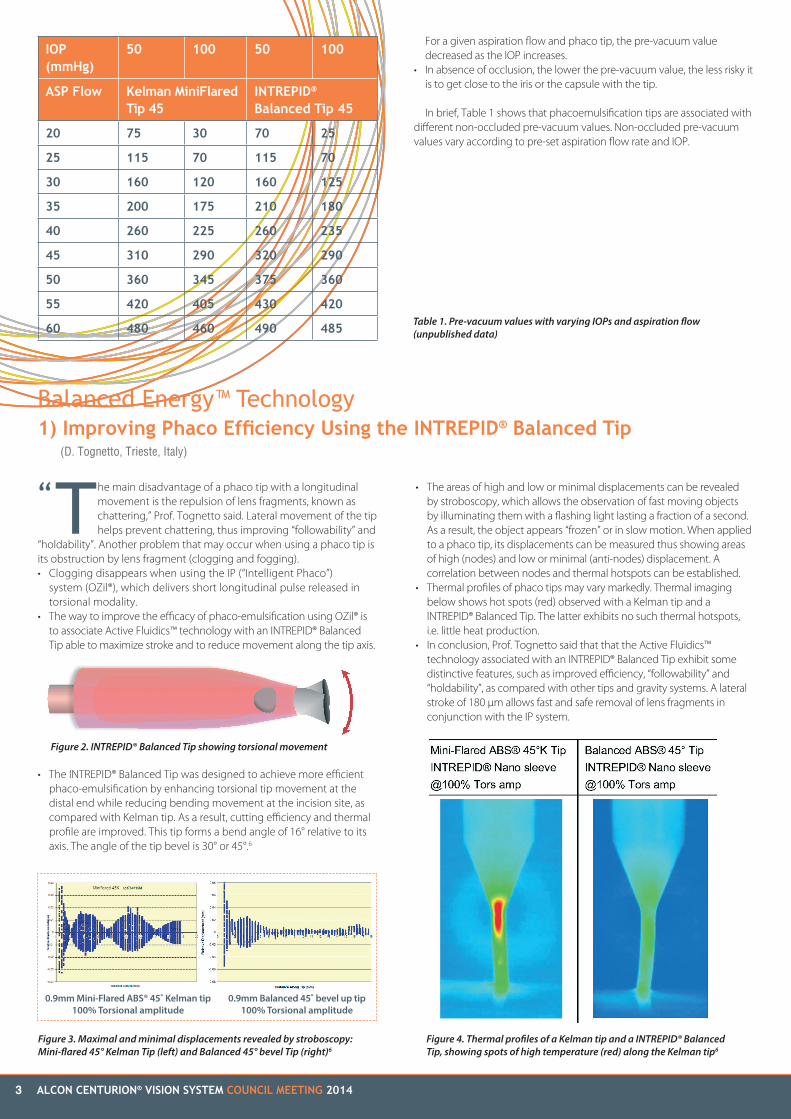
• Different pre-vacuum values are associated with the various phaco tips available. When no occlusion occurs, pre-vacuum values vary according to pre-set aspiration flow and IOP. For a given IOP and phaco tip, the greater the aspiration flow, the higher the pre-vacuum values.
ALCON CENTURION® VISION SYSTEM COUNCIL MEETING 20143
T he main disadvantage of a phaco tip with a longitudinal movement is the repulsion of lens fragments, known as chattering,” Prof. Tognetto said. Lateral movement of the tip helps prevent chattering, thus improving “followability” and
“holdability”. Another problem that may occur when using a phaco tip is its obstruction by lens fragment (clogging and fogging).• Clogging disappears when using the IP (“Intelligent Phaco”)
system (OZil®), which delivers short longitudinal pulse released in torsional modality.
• The way to improve the efficacy of phaco-emulsification using OZil® is to associate Active Fluidics™ technology with an INTREPID® Balanced Tip able to maximize stroke and to reduce movement along the tip axis.
• The INTREPID® Balanced Tip was designed to achieve more efficient phaco-emulsification by enhancing torsional tip movement at the distal end while reducing bending movement at the incision site, as compared with Kelman tip. As a result, cutting efficiency and thermal profile are improved. This tip forms a bend angle of 16° relative to its axis. The angle of the tip bevel is 30° or 45°.6
Balanced Energy™ Technology1) Improving Phaco Efficiency Using the INTREPID® Balanced Tip
(D. Tognetto, Trieste, Italy)
Table 1. Pre-vacuum values with varying IOPs and aspiration flow (unpublished data)
“
Figure 2. INTREPID® Balanced Tip showing torsional movement
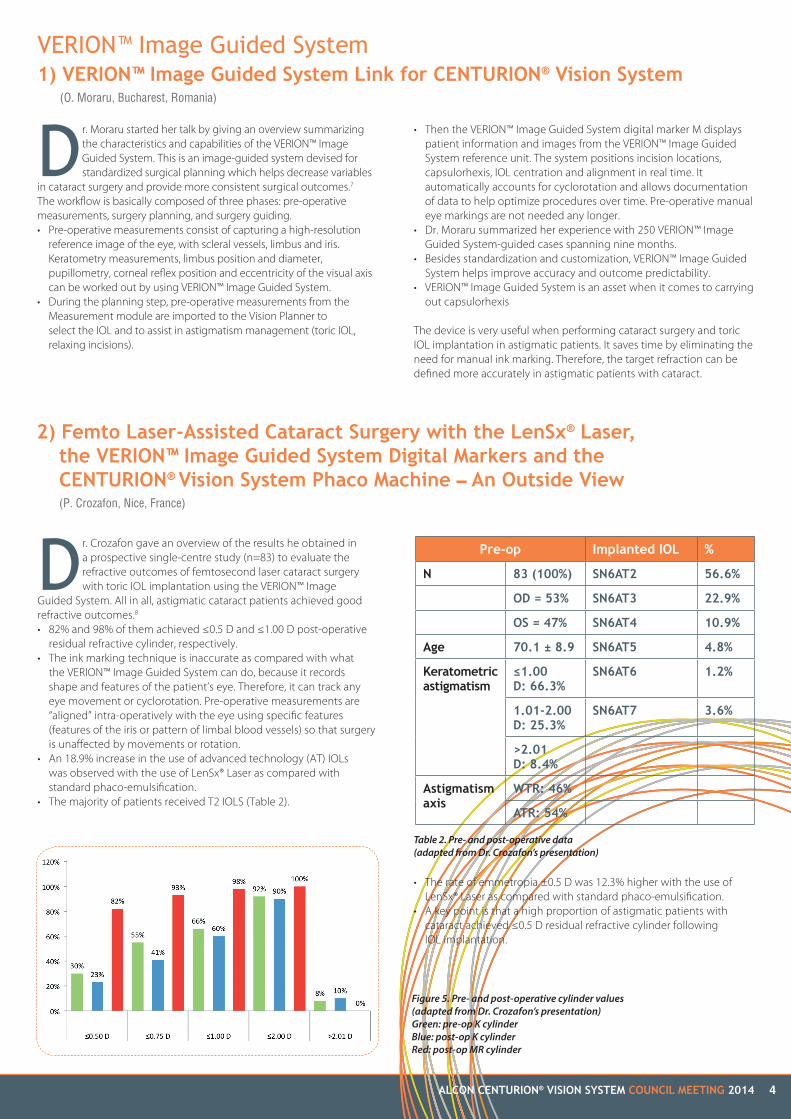
Figure 3. Maximal and minimal displacements revealed by stroboscopy: Mini-flared 45° Kelman Tip (left) and Balanced 45° bevel Tip (right)6
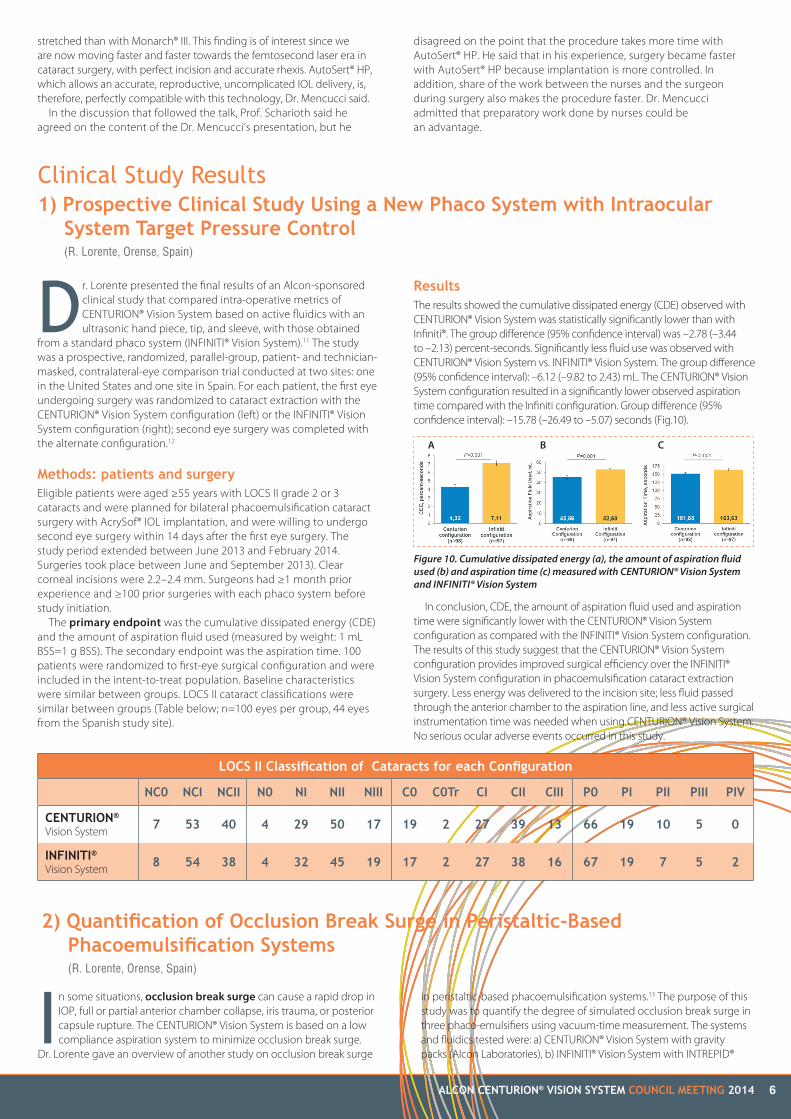
Figure 4. Thermal profiles of a Kelman tip and a INTREPID® Balanced Tip, showing spots of high temperature (red) along the Kelman tip6
• The areas of high and low or minimal displacements can be revealed by stroboscopy, which allows the observation of fast moving objects by illuminating them with a flashing light lasting a fraction of a second. As a result, the object appears “frozen” or in slow motion. When applied to a phaco tip, its displacements can be measured thus showing areas of high (nodes) and low or minimal (anti-nodes) displacement. A correlation between nodes and thermal hotspots can be established.
• Thermal profiles of phaco tips may vary markedly. Thermal imaging below shows hot spots (red) observed with a Kelman tip and a INTREPID® Balanced Tip. The latter exhibits no such thermal hotspots, i.e. little heat production.
• In conclusion, Prof. Tognetto said that that the Active Fluidics™ technology associated with an INTREPID® Balanced Tip exhibit some distinctive features, such as improved efficiency, “followability” and “holdability”, as compared with other tips and gravity systems. A lateral stroke of 180 µm allows fast and safe removal of lens fragments in conjunction with the IP system.
For a given aspiration flow and phaco tip, the pre-vacuum value decreased as the IOP increases.
• In absence of occlusion, the lower the pre-vacuum value, the less risky it is to get close to the iris or the capsule with the tip.
In brief, Table 1 shows that phacoemulsification tips are associated with different non-occluded pre-vacuum values. Non-occluded pre-vacuum values vary according to pre-set aspiration flow rate and IOP.
IOP (mmHg)
50 100 50 100
ASP Flow Kelman MiniFlared Tip 45
INTREPID® Balanced Tip 45
20 75 30 70 25
25 115 70 115 70
30 160 120 160 125
35 200 175 210 180
40 260 225 260 235
45 310 290 320 290
50 360 345 375 360
55 420 405 430 420
60 480 460 490 485
0.9mm Mini-Flared ABS® 45˚ Kelman tip100% Torsional amplitude
0.9mm Balanced 45˚ bevel up tip100% Torsional amplitude
ALCON CENTURION® VISION SYSTEM COUNCIL MEETING 2014 4
Table 2. Pre- and post-operative data (adapted from Dr. Crozafon’s presentation)
• Then the VERION™ Image Guided System digital marker M displays patient information and images from the VERION™ Image Guided System reference unit. The system positions incision locations, capsulorhexis, IOL centration and alignment in real time. It automatically accounts for cyclorotation and allows documentation of data to help optimize procedures over time. Pre-operative manual eye markings are not needed any longer.
• Dr. Moraru summarized her experience with 250 VERION™ Image Guided System-guided cases spanning nine months.
• Besides standardization and customization, VERION™ Image Guided System helps improve accuracy and outcome predictability.
• VERION™ Image Guided System is an asset when it comes to carrying out capsulorhexis
The device is very useful when performing cataract surgery and toric IOL implantation in astigmatic patients. It saves time by eliminating the need for manual ink marking. Therefore, the target refraction can be defined more accurately in astigmatic patients with cataract.
Dr. Moraru started her talk by giving an overview summarizing the characteristics and capabilities of the VERION™ Image Guided System. This is an image-guided system devised for standardized surgical planning which helps decrease variables
in cataract surgery and provide more consistent surgical outcomes.7 The workflow is basically composed of three phases: pre-operative measurements, surgery planning, and surgery guiding.• Pre-operative measurements consist of capturing a high-resolution
reference image of the eye, with scleral vessels, limbus and iris. Keratometry measurements, limbus position and diameter, pupillometry, corneal reflex position and eccentricity of the visual axis can be worked out by using VERION™ Image Guided System.
• During the planning step, pre-operative measurements from the Measurement module are imported to the Vision Planner to select the IOL and to assist in astigmatism management (toric IOL, relaxing incisions).
VERION™ Image Guided System1) VERION™ Image Guided System Link for CENTURION® Vision System
(O. Moraru, Bucharest, Romania)
2) Femto Laser-Assisted Cataract Surgery with the LenSx® Laser, the VERION™ Image Guided System Digital Markers and the CENTURION® Vision System Phaco Machine – An Outside View (P. Crozafon, Nice, France)
Dr. Crozafon gave an overview of the results he obtained in a prospective single-centre study (n=83) to evaluate the refractive outcomes of femtosecond laser cataract surgery with toric IOL implantation using the VERION™ Image
Guided System. All in all, astigmatic cataract patients achieved good refractive outcomes.8 • 82% and 98% of them achieved ≤0.5 D and ≤1.00 D post-operative
residual refractive cylinder, respectively.• The ink marking technique is inaccurate as compared with what
the VERION™ Image Guided System can do, because it records shape and features of the patient’s eye. Therefore, it can track any eye movement or cyclorotation. Pre-operative measurements are “aligned” intra-operatively with the eye using specific features (features of the iris or pattern of limbal blood vessels) so that surgery is unaffected by movements or rotation.
• An 18.9% increase in the use of advanced technology (AT) IOLs was observed with the use of LenSx® Laser as compared with standard phaco-emulsification.
• The majority of patients received T2 IOLS (Table 2).
Figure 5. Pre- and post-operative cylinder values (adapted from Dr. Crozafon’s presentation)Green: pre-op K cylinderBlue: post-op K cylinderRed: post-op MR cylinder
Pre-op Implanted IOL %
N 83 (100%) SN6AT2 56.6%
OD = 53% SN6AT3 22.9%
OS = 47% SN6AT4 10.9%
Age 70.1 ± 8.9 SN6AT5 4.8%
Keratometric astigmatism
≤1.00 D: 66.3%
SN6AT6 1.2%
1.01-2.00 D: 25.3%
SN6AT7 3.6%
>2.01 D: 8.4%
Astigmatism axis
WTR: 46%
ATR: 54%
• The rate of emmetropia ±0.5 D was 12.3% higher with the use of LenSx® Laser as compared with standard phaco-emulsification.
• A key point is that a high proportion of astigmatic patients with cataract achieved ≤0.5 D residual refractive cylinder following IOL implantation.

ALCON CENTURION® VISION SYSTEM COUNCIL MEETING 20145
AutoSert® HP. She showed the appearance of the endothelial side of a 2.2-mm incision on electron microscope scans. In this particular case the injection was performed with AutoSert® HP through this incision. We can note how smooth and regular, uniform, and consistent the margins are. It is also important to observe the details of the lateral margins and notice the minimal impact of AutoSert® HP on the surrounding tissue.
With Monarch® III, the appearance, even though well-defined is less smooth and regular in most cases, with a more extended involvement of surrounding tissue. The lateral margins are regular and appear similar to those with AutoSert® HP only in some cases. According to Dr. Mencucci this may not have any clinical importance, but the difference is impressive. Nowadays, there is striking, remarkable evidence supporting the idea that a perfect wound architecture is of paramount importance in preventing endophthalmitis.
According to Dr. Allen’s paper as well as in Dr. Mencucci’s experiments, the size of the inner side of the incision was smaller in AutoSert® HP specimens as compared with manual ones (Monarch® III).
In summary, AutoSert® HP is simple to set up and use, with little-to-no learning curve. It alleviates a potentially significant challenge for the surgeons when it comes to controlling the injection process. The IOL implantation can be carried out smoothly, and the incision is less
Dr. Mencucci started her talk by stating that the success of cataract surgery is based on a perfect surgical technique and standardization of every step of the procedure, i.e. the incisions, the rhexis and IOL implantation. The challenges for the surgeon
are that the current cartridges don’t fit an incision <2.4 mm, and the leading edge of the cartridge tip must be kept in constant close contact with the incision. In addition, the surgeon has to hold the injector with one hand and rotate the screw thread as quickly as possible, keeping the injector aligned with the incision axis.
A few years ago Alcon launched an automated delivery device (AutoSert® IOL Injector handpiece [AutoSert® HP]). One question that may come to mind is whether this is a “gadget” for the smartest and most up-to-date surgeons. Perhaps more serious concerns may arise, notably:• Higher costs are associated with the use of AutoSert® HP as compared
with currently available injectors. • The surgical staff needs just a little more time for setting up the hand
piece, as compared with manual injectors. Loading the IOL in the cartridge and pushing it safely into the eye took approximately only 12-13 more seconds with AutoSert® HP than with currently available injectors.
• The availability of easy to use injectors on the market, for instance Monarch® III. Dr. Mencucci said, “Monarch® III is one of my favourites”. Monarch® III provides a very good control of the insertion procedure, but both hands are needed and thus a “blind” moment may occur during the insertion (i.e. a lapse of time in which the surgeon cannot see very well what he/she is doing). The syringe (pre-loaded delivery system) with a “one-hand” procedure, requires significant force to compress the IOL and move it into the cartridge. Then the force needed to make the IOL exit the cartridge rapidly drops and thus overshooting may occur. With time, the plunger does not always ensure smooth movements.9
• Low acceptance of AutoSert® HP by surgeons, because they consider they don’t need it. Dr. Mencucci showed some videos highlighting examples of issues with IOL injection, even with Monarch® and Acrysof: the stress on the incision, the corneal folds and sometimes the “blind” moment.
So why use AutoSert® IOL Injector HP?1) It helps the surgeon manage forces involved in IOL delivery. 2) It is a motorised system that allows continuous movement (injection)
without disruption, contrary to twist-style injectors.3) There is a lower risk of uncontrolled overshoot, as can happen with
plunger-style inserters (pre-loaded systems). 4) Both hands are available to stabilize the eye. 5) There is the possibility to standardize IOL injection velocity (4.4 mm/
sec is the maximal speed). Indeed, with AutoSert® HP, the speed of IOL injection can be modulated, with the possibility to pause for less than a second to verify if everything is under control, before successfully completing the insertion.
Incision enlargement is an issue with the current cartridge as the trend is to reduce the incision size. A study by Allen et al.10 showed significantly less incision enlargement with AutoSert® used at a fast injection speed (4.4 mm/sec) than with either Monarch® III or AutoSert® HP at 1.5 mm/sec.
It is also known that a more regular incision is of particular importance to reduce the possibility of post-op wound leak and less ingress of fluid and bacteria from the conjunctival sac. Dr. Mencucci showed some OCT pictures comparing injections with Monarch® III and AutoSert® HP. The overall wound architecture was perfectly maintained with AutoSert® HP while a less regular appearance of wound architecture due to less accurate insertion is observed with Monarch® III.
Apart from these anterior segment OCT images, what’s happening on the endothelial side, the speaker asked. To answer this question, the presenter recently conducted some research on 40 porcine eyes. Twenty of them received an IOL by manual injection with Monarch® III through an incision of 2.2 mm and 20 with received the IOL by
AutoSert® IOL Injector 1) Were the Benefits for the Patients and Surgeons Worth it?
(R. Mencucci, Florence, Italy)
Figure 6. Wound appearance following the use of AutoSert® HP (left) and Monarch® III (right) as seen on OCT
Figure 7. Incision as they look like following injection with AutoSert® HP
Figure 8. Appearance of incision following injection with Monarch® III
Figure 9. Incisions in specimens injected with AutoSert® HP (left) and Monarch® III (right)
ALCON CENTURION® VISION SYSTEM COUNCIL MEETING 2014 6
Dr. Lorente presented the final results of an Alcon-sponsored clinical study that compared intra-operative metrics of CENTURION® Vision System based on active fluidics with an ultrasonic hand piece, tip, and sleeve, with those obtained
from a standard phaco system (INFINITI® Vision System).11 The study was a prospective, randomized, parallel-group, patient- and technician-masked, contralateral-eye comparison trial conducted at two sites: one in the United States and one site in Spain. For each patient, the first eye undergoing surgery was randomized to cataract extraction with the CENTURION® Vision System configuration (left) or the INFINITI® Vision System configuration (right); second eye surgery was completed with the alternate configuration.12
Methods: patients and surgeryEligible patients were aged ≥55 years with LOCS II grade 2 or 3 cataracts and were planned for bilateral phacoemulsification cataract surgery with AcrySof® IOL implantation, and were willing to undergo second eye surgery within 14 days after the first eye surgery. The study period extended between June 2013 and February 2014. Surgeries took place between June and September 2013). Clear corneal incisions were 2.2–2.4 mm. Surgeons had ≥1 month prior experience and ≥100 prior surgeries with each phaco system before study initiation.
The primary endpoint was the cumulative dissipated energy (CDE) and the amount of aspiration fluid used (measured by weight: 1 mL BSS=1 g BSS). The secondary endpoint was the aspiration time. 100 patients were randomized to first-eye surgical configuration and were included in the intent-to-treat population. Baseline characteristics were similar between groups. LOCS II cataract classifications were similar between groups (Table below; n=100 eyes per group, 44 eyes from the Spanish study site).
stretched than with Monarch® III. This finding is of interest since we are now moving faster and faster towards the femtosecond laser era in cataract surgery, with perfect incision and accurate rhexis. AutoSert® HP, which allows an accurate, reproductive, uncomplicated IOL delivery, is, therefore, perfectly compatible with this technology, Dr. Mencucci said.
In the discussion that followed the talk, Prof. Scharioth said he agreed on the content of the Dr. Mencucci’s presentation, but he
In some situations, occlusion break surge can cause a rapid drop in IOP, full or partial anterior chamber collapse, iris trauma, or posterior capsule rupture. The CENTURION® Vision System is based on a low compliance aspiration system to minimize occlusion break surge.
Dr. Lorente gave an overview of another study on occlusion break surge
Clinical Study Results1) Prospective Clinical Study Using a New Phaco System with Intraocular System Target Pressure Control
(R. Lorente, Orense, Spain)
2) Quantification of Occlusion Break Surge in Peristaltic-BasedPhacoemulsification Systems(R. Lorente, Orense, Spain)
ResultsThe results showed the cumulative dissipated energy (CDE) observed with CENTURION® Vision System was statistically significantly lower than with Infiniti®. The group difference (95% confidence interval) was –2.78 (–3.44 to –2.13) percent-seconds. Significantly less fluid use was observed with CENTURION® Vision System vs. INFINITI® Vision System. The group difference (95% confidence interval): –6.12 (–9.82 to 2.43) mL. The CENTURION® Vision System configuration resulted in a significantly lower observed aspiration time compared with the Infiniti configuration. Group difference (95% confidence interval): –15.78 (–26.49 to –5.07) seconds (Fig.10).
In conclusion, CDE, the amount of aspiration fluid used and aspiration time were significantly lower with the CENTURION® Vision System configuration as compared with the INFINITI® Vision System configuration. The results of this study suggest that the CENTURION® Vision System configuration provides improved surgical efficiency over the INFINITI® Vision System configuration in phacoemulsification cataract extraction surgery. Less energy was delivered to the incision site; less fluid passed through the anterior chamber to the aspiration line, and less active surgical instrumentation time was needed when using CENTURION® Vision System. No serious ocular adverse events occurred in this study.
disagreed on the point that the procedure takes more time with AutoSert® HP. He said that in his experience, surgery became faster with AutoSert® HP because implantation is more controlled. In addition, share of the work between the nurses and the surgeon during surgery also makes the procedure faster. Dr. Mencucci admitted that preparatory work done by nurses could be an advantage.
LOCS II Classification of Cataracts for each Configuration
NC0 NCI NCII N0 NI NII NIII C0 C0Tr CI CII CIII P0 PI PII PIII PIV
CENTURION®
Vision System7 53 40 4 29 50 17 19 2 27 39 13 66 19 10 5 0
INFINITI®
Vision System8 54 38 4 32 45 19 17 2 27 38 16 67 19 7 5 2
in peristaltic-based phacoemulsification systems.13 The purpose of this study was to quantify the degree of simulated occlusion break surge in three phaco-emulsifiers using vacuum-time measurement. The systems and fluidics tested were: a) CENTURION® Vision System with gravity packs (Alcon Laboratories), b) INFINITI® Vision System with INTREPID®
Figure 10. Cumulative dissipated energy (a), the amount of aspiration fluid used (b) and aspiration time (c) measured with CENTURION® Vision System and INFINITI® Vision System
A B C

7 ALCON CENTURION® VISION SYSTEM COUNCIL MEETING 2014
Balanced Tip and gravity packs (Alcon Laboratories) and c) WhiteStar Signature® System with OPO70 packs (Abbott Medical Optics). Occlusion break testing was designed to enable direct, reproducible comparison of phacoemulsification systems and fluidics without confounding variables. The test set-up was based on a previously published methodology.14 The same hand piece, phacoemulsification tip design, and matching sleeve were used to test all systems. Note that the hand piece (OZil® [Alcon Laboratories]), the phaco tip (30°R, 0.9 mm, non-aspiration bypass system [Alcon Laboratories]) and six fluidics packs were tested in each system.
Occlusion break test setup and simulation The irrigation bottle was placed at 90 cm in height and aspiration flow rate was 30 cc/min. Systems were tested at vacuum limits of 300, 400, 500, and 600 mmHg. Occlusion was simulated by clamping the aspiration line with needle-nosed pliers between the luer fitting and the hand piece to simulate tip occlusion. Vacuum was then allowed to build up to a pre-set limit.
Occlusion break surges were recorded, and the area-under-the-curve was measured by a digital storage oscilloscope. The results showed that CENTURION® Vision System produced significantly less surge than INFINITI® Vision System and Signature® across the tested vacuum limit range (P<0.05, 2-way analysis of variance). Occlusion break surge increased with increasing vacuum in all systems. At both usual (400 mmHg) and demanding (600 mmHg) vacuum limits CENTURION® Vision System produced the lowest surge and Signature® produced the greatest surge (Fig. 11).
In conclusion, the CENTURION® Vision System was associated with a significantly improved occlusion break surge as compared with the other tested peristaltic-based phacoemulsification systems across a range of surgical aspiration vacuum limits. Testing was performed under controlled laboratory conditions and according to clinically relevant settings by using a previously described laboratory set up and a standardized, reproducible simulation method. The decreased surge area obtained with CENTURION® Vision System is likely due to its lower-compliance fluidics as compared
References1. Healey PR, Thomas R. Fast facts: glaucoma. Health Press Limited, Oxford, U.K., 2010.
2. Casson RJ, Chidlow G, Wood JPM, Crowston JG, Goldberg I. Definition of glaucoma: clinical and experimental concepts. Clin Experiment Ophthalmol 2012; 40(4): 341-9.
3. Pillunat KR, Ventzke S, Spoerl E, Furashova O, Stodtmeister R, Pillunat LE. Central retinal venous pulsation pressure in different stages of primary open-angle glaucoma. Br J Ophthalmol 2014; 98: 1374-8.
4. http://www.alconsurgical.co.za/centurion/active-fluidics.aspx
5. Packard R. The surgical control of Active Fluidics. Insert to Cataract and Refractive Surgery Today, 2014.
6. Data on file: INTREPID® Balanced Tip technical file.
7. http://www.alconsurgical.co.za/VERION-Image-Guided-System.aspx
8. Crozafon P. Initial experience with the new image-guided system for standardized surgical planning for refractive cataract surgery. Presented at the XXXII Congress of the ESCRS, London, 2014.
9. Larkin H. Automated IOL injection. Update Cataract & Refractive. EUROTIMES, vol. 17, issue 3, 2012.
10. Allen D, Habib M, Steel D. Final incision size after implantation of a hydrophobic acrylic aspheric intraocular lens: new motorized injector versus standard manual injector. J Cataract Refract Surg 2012; 38: 249-55.
11. CENTURION® Vision System FMS Pack Direction for use, 2012-13.
12. Lorente R, Solomon K, Cionni R, Fanney. Prospective clinical study using a new phaco system with intraocular system targer pressure controlled. Poster shown at the XXXII ESCRS Conference, London, 13-17th September 2014.
13. Sharif-Kashani P, Fanney D, Injev V. Comparison of occlusion break responses and vacuum rise times of phacoemulsification systems. BMC Ophthalmol 2014; 14: 96.
14. Han YK, Miller KM. Comparison of vacuum rise time, vacuum limit accuracy, and occlusion break surge of 3 new phacoemulsification systems. J Cataract Refract Surg 2009; 35(8): 1424-9.
Figure 11. Surge area as a function of aspiration line vacuum at the time of occlusion breakYellow: CENTURION® Vision System; Blue: INFINITI® Vision System; Green: WhiteStar Signature®
Supplement February 2015
with other systems. A lower surge results in more stable and predictable conditions in the anterior chamber of the eye and the surgical experience gained so far appears to confirm this finding.


















