ALCOHOL WITHDRAWAL – ASSESSMENT & MANAGEMENT ON...
2
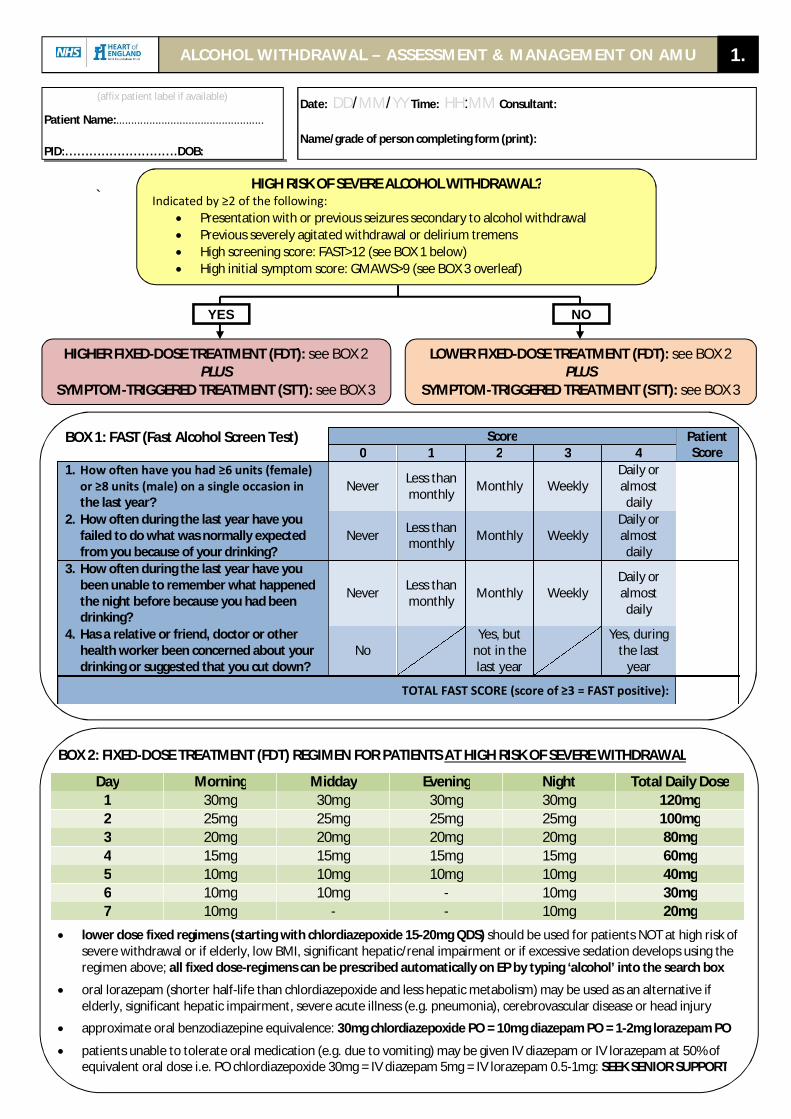
` ALCOHOL WITHDRAWAL – ASSESSMENT & MANAGEMENT ON AMU 1. (affix patient label if available) Patient Name:................................................. PID:............................DOB: Date: DD/MM/YY Time: HH:MM Consultant: Name/grade of person completing form (print): HIGH RISK OF SEVERE ALCOHOL WITHDRAWAL? Indicated by ≥2 of the following: Presentation with or previous seizures secondary to alcohol withdrawal Previous severely agitated withdrawal or delirium tremens High screening score: FAST>12 (see BOX 1 below) High initial symptom score: GMAWS>9 (see BOX 3 overleaf) HIGHER FIXED-DOSE TREATMENT (FDT): see BOX 2 PLUS SYMPTOM-TRIGGERED TREATMENT (STT): see BOX 3 LOWER FIXED-DOSE TREATMENT (FDT): see BOX 2 PLUS SYMPTOM-TRIGGERED TREATMENT (STT): see BOX 3 BOX 1: FAST (Fast Alcohol Screen Test) Score Patient Score 0 1 2 3 4 1. How often have you had ≥6 units (female) or ≥8 units (male) on a single occasion in the last year? Never Less than monthly Monthly Weekly Daily or almost daily 2. How often during the last year have you failed to do what was normally expected from you because of your drinking? Never Less than monthly Monthly Weekly Daily or almost daily 3. How often during the last year have you been unable to remember what happened the night before because you had been drinking? Never Less than monthly Monthly Weekly Daily or almost daily 4. Has a relative or friend, doctor or other health worker been concerned about your drinking or suggested that you cut down? No Yes, but not in the last year Yes, during the last year TOTAL FAST SCORE (score of ≥3 = FAST positive): BOX 2: FIXED-DOSE TREATMENT (FDT) REGIMEN FOR PATIENTS AT HIGH RISK OF SEVERE WITHDRAWAL Day Morning Midday Evening Night Total Daily Dose 1 30mg 30mg 30mg 30mg 120mg 2 25mg 25mg 25mg 25mg 100mg 3 20mg 20mg 20mg 20mg 80mg 4 15mg 15mg 15mg 15mg 60mg 5 10mg 10mg 10mg 10mg 40mg 6 10mg 10mg - 10mg 30mg 7 10mg - - 10mg 20mg lower dose fixed regimens (starting with chlordiazepoxide 15-20mg QDS) should be used for patients NOT at high risk of severe withdrawal or if elderly, low BMI, significant hepatic/renal impairment or if excessive sedation develops using the regimen above; all fixed dose-regimens can be prescribed automatically on EP by typing ‘alcohol’ into the search box oral lorazepam (shorter half-life than chlordiazepoxide and less hepatic metabolism) may be used as an alternative if elderly, significant hepatic impairment, severe acute illness (e.g. pneumonia), cerebrovascular disease or head injury approximate oral benzodiazepine equivalence: 30mg chlordiazepoxide PO = 10mg diazepam PO = 1-2mg lorazepam PO patients unable to tolerate oral medication (e.g. due to vomiting) may be given IV diazepam or IV lorazepam at 50% of equivalent oral dose i.e. PO chlordiazepoxide 30mg = IV diazepam 5mg = IV lorazepam 0.5-1mg: SEEK SENIOR SUPPORT YES NO
Transcript of ALCOHOL WITHDRAWAL – ASSESSMENT & MANAGEMENT ON...
`
ALCOHOL WITHDRAWAL – ASSESSMENT & MANAGEMENT ON AMU 1.
(affix patient label if available)
Patient Name:.................................................
PID:............................DOB:
Date: DD/MM/YY Time: HH:MM Consultant:
Name/grade of person completing form (print):
HIGH RISK OF SEVERE ALCOHOL WITHDRAWAL? Indicated by ≥2 of the following:
Presentation with or previous seizures secondary to alcohol withdrawal Previous severely agitated withdrawal or delirium tremens High screening score: FAST>12 (see BOX 1 below) High initial symptom score: GMAWS>9 (see BOX 3 overleaf)
HIGHER FIXED-DOSE TREATMENT (FDT): see BOX 2 PLUS
SYMPTOM-TRIGGERED TREATMENT (STT): see BOX 3
LOWER FIXED-DOSE TREATMENT (FDT): see BOX 2 PLUS
SYMPTOM-TRIGGERED TREATMENT (STT): see BOX 3
BOX 1: FAST (Fast Alcohol Screen Test) Score Patient Score 0 1 2 3 4
1. How often have you had ≥6 units (female) or ≥8 units (male) on a single occasion in the last year?
Never Less than monthly Monthly Weekly
Daily or almost daily
2. How often during the last year have you failed to do what was normally expected from you because of your drinking?
Never Less than monthly Monthly Weekly
Daily or almost daily
3. How often during the last year have you been unable to remember what happened the night before because you had been drinking?
Never Less than monthly Monthly Weekly
Daily or almost daily
4. Has a relative or friend, doctor or other health worker been concerned about your drinking or suggested that you cut down?
No Yes, but
not in the last year
Yes, during
the last year
TOTAL FAST SCORE (score of ≥3 = FAST positive):
BOX 2: FIXED-DOSE TREATMENT (FDT) REGIMEN FOR PATIENTS AT HIGH RISK OF SEVERE WITHDRAWAL
Day Morning Midday Evening Night Total Daily Dose 1 30mg 30mg 30mg 30mg 120mg 2 25mg 25mg 25mg 25mg 100mg 3 20mg 20mg 20mg 20mg 80mg 4 15mg 15mg 15mg 15mg 60mg 5 10mg 10mg 10mg 10mg 40mg 6 10mg 10mg - 10mg 30mg 7 10mg - - 10mg 20mg
lower dose fixed regimens (starting with chlordiazepoxide 15-20mg QDS) should be used for patients NOT at high risk of severe withdrawal or if elderly, low BMI, significant hepatic/renal impairment or if excessive sedation develops using the regimen above; all fixed dose-regimens can be prescribed automatically on EP by typing ‘alcohol’ into the search box
oral lorazepam (shorter half-life than chlordiazepoxide and less hepatic metabolism) may be used as an alternative if elderly, significant hepatic impairment, severe acute illness (e.g. pneumonia), cerebrovascular disease or head injury
approximate oral benzodiazepine equivalence: 30mg chlordiazepoxide PO = 10mg diazepam PO = 1-2mg lorazepam PO
patients unable to tolerate oral medication (e.g. due to vomiting) may be given IV diazepam or IV lorazepam at 50% of equivalent oral dose i.e. PO chlordiazepoxide 30mg = IV diazepam 5mg = IV lorazepam 0.5-1mg: SEEK SENIOR SUPPORT
YES NO
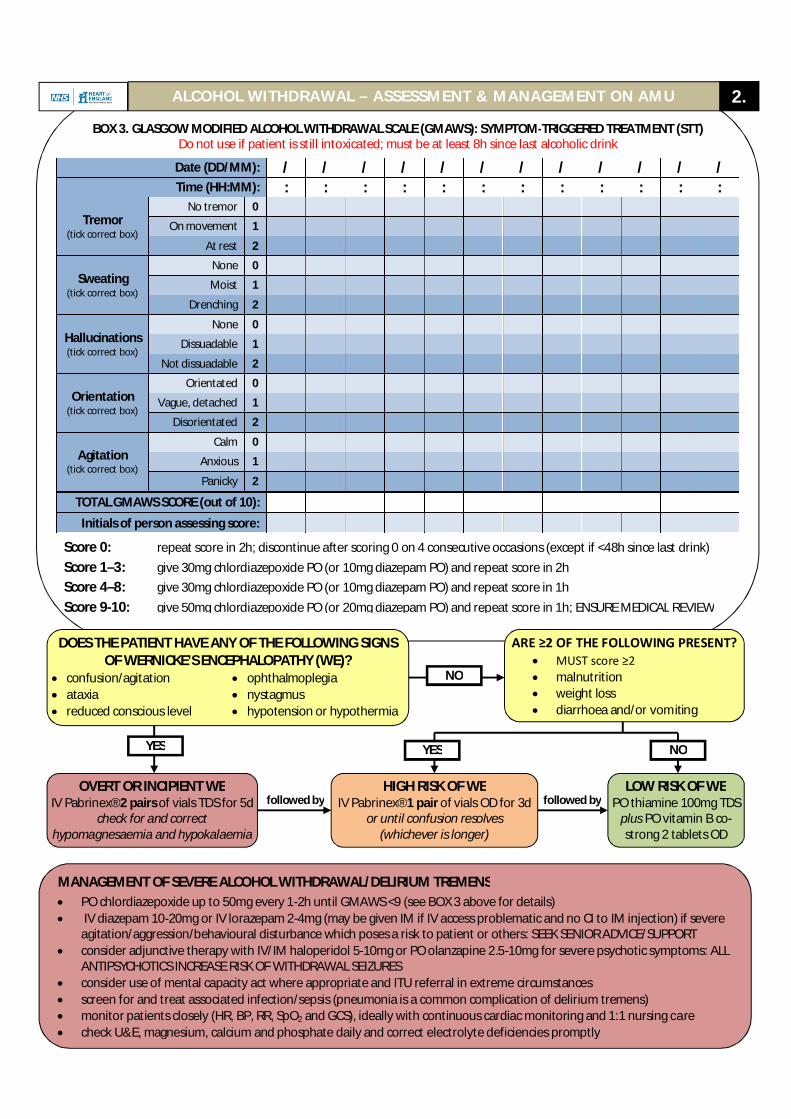
BOX 3. GLASGOW MODIFIED ALCOHOL WITHDRAWAL SCALE (GMAWS): SYMPTOM-TRIGGERED TREATMENT (STT) Do not use if patient is still intoxicated; must be at least 8h since last alcoholic drink
Date (DD/MM): / / / / / / / / / / / / Time (HH:MM): : : : : : : : : : : : :
Tremor (tick correct box)
No tremor 0 On movement 1
At rest 2
Sweating (tick correct box)
None 0 Moist 1
Drenching 2
Hallucinations (tick correct box)
None 0 Dissuadable 1
Not dissuadable 2
Orientation (tick correct box)
Orientated 0 Vague, detached 1
Disorientated 2
Agitation (tick correct box)
Calm 0 Anxious 1 Panicky 2
TOTAL GMAWS SCORE (out of 10): Initials of person assessing score:
Score 0: repeat score in 2h; discontinue after scoring 0 on 4 consecutive occasions (except if <48h since last drink) Score 1–3: give 30mg chlordiazepoxide PO (or 10mg diazepam PO) and repeat score in 2h Score 4–8: give 30mg chlordiazepoxide PO (or 10mg diazepam PO) and repeat score in 1h Score 9-10: give 50mg chlordiazepoxide PO (or 20mg diazepam PO) and repeat score in 1h; ENSURE MEDICAL REVIEW
MANAGEMENT OF SEVERE ALCOHOL WITHDRAWAL/DELIRIUM TREMENS PO chlordiazepoxide up to 50mg every 1-2h until GMAWS <9 (see BOX 3 above for details) IV diazepam 10-20mg or IV lorazepam 2-4mg (may be given IM if IV access problematic and no CI to IM injection) if severe
agitation/aggression/behavioural disturbance which poses a risk to patient or others: SEEK SENIOR ADVICE/SUPPORT consider adjunctive therapy with IV/IM haloperidol 5-10mg or PO olanzapine 2.5-10mg for severe psychotic symptoms: ALL
ANTIPSYCHOTICS INCREASE RISK OF WITHDRAWAL SEIZURES consider use of mental capacity act where appropriate and ITU referral in extreme circumstances screen for and treat associated infection/sepsis (pneumonia is a common complication of delirium tremens) monitor patients closely (HR, BP, RR, SpO2 and GCS), ideally with continuous cardiac monitoring and 1:1 nursing care check U&E, magnesium, calcium and phosphate daily and correct electrolyte deficiencies promptly
followed by followed by
DOES THE PATIENT HAVE ANY OF THE FOLLOWING SIGNS OF WERNICKE’S ENCEPHALOPATHY (WE)?
confusion/agitation ophthalmoplegia ataxia nystagmus reduced conscious level hypotension or hypothermia
ARE ≥2 OF THE FOLLOWING PRESENT? MUST score ≥2 malnutrition weight loss diarrhoea and/or vomiting
OVERT OR INCIPIENT WE IV Pabrinex® 2 pairs of vials TDS for 5d
check for and correct hypomagnesaemia and hypokalaemia
LOW RISK OF WE PO thiamine 100mg TDS
plus PO vitamin B co-strong 2 tablets OD
HIGH RISK OF WE IV Pabrinex® 1 pair of vials OD for 3d
or until confusion resolves (whichever is longer)
YES
NO
YES NO
ALCOHOL WITHDRAWAL – ASSESSMENT & MANAGEMENT ON AMU 2.