
Albany Medical Revie Medical Review A QUARTERLY ONLINE PUBLICATION FROM ALBANY MEDICAL COLLEGE;...
6
Albany Medical Review A QUARTERLY ONLINE PUBLICATION FROM ALBANY MEDICAL COLLEGE; INTERNAL MEDICINE RESIDENCY Editors-In-Chief: Anupam Batra, MD Aakash Modi, MD Consulting: Raymond P. Smith, MD Program Director Albany Medical College Ki Tae Mok, MD Stratton VA Medical Center Technical Editor: Michelle Snavely Albany Medical Center 43 New Scotland Avenue Albany, New York 12208 518.262.5377 www.amc.edu Contact: @mail.amc.edu February 2014 Introduction: Pulmonary carcinoma with giant cells and spindle cells (sarcomatoid) is rare, accounting for 0.1-0.4% of all lung carcinomas. Common presenting symptoms include chest pain (14%), hemoptysis (49%), cough (46%) and dyspnea (3%). We present a unique case of a young man with sarcoma- toid carcinoma (SCa) presenting with shoulder pain and pro- gressive upper extremity weakness. Case: A 36 year old male man with no medical history present- ed with a 6 months of right shoulder pain with associated right upper extremity weakness. He also reported a 30 pound weight loss and night sweats. He had a 20-pack year smoking history. There was no family history of cancer. Chest x-ray showed a right upper lobe lesion with erosion into the 2 nd and 3 rd posteri- or ribs. Head CT demonstrated multiple hyperdense lesions with vasogenic edema. Chest CT identified a right apical lung mass with extension into the paraspinal musculature and spinal canal at T3 and T4. CT–guided biopsy of the lung mass was performed and histopathological analysis revealed poorly differ- entiated carcinoma with giant cells and spindle cells (example Fig 1). The tumor had immunohistochemical staining positive for AE1:AE3 and CK7; negative for p40, TTF-1, NapsinA, calretinin, and p63. MRI of the brachial plexus and spine demonstrated invasion of the lower brachial plexus as well as multiple metastatic lesions of the cervical and thoracic spine with hemorrhagic features. Levetiracetam for seizure prophylax- is and dexamethasone for vasogenic edema were started fol- lowed by palliative whole brain and lung radiation therapy. Unfortunately, due to significant disease burden, the patient died 3 weeks later. Discussion: SCa of the lung typically occurs in males in their 5 th decade who are heavy smokers. Immunochemistry often demonstrates co-expression of cytokeratin and vimentin in tumor cells (1,2). Although SCa is rare, common sites of disease include the skin, thyroid, bone, and urinary tract, whereas pulmonary involvement is uncommon, accounting for less than 1% of all lung tumors. The majority of SCa present with local- ized symptoms in older patients (3). The case patient presented with right upper extremity parasthesiae and shoulder pain with- out respiratory symptoms, which is in stark contrast to the majority of SCa cases. The diagnosis was only made after chest x-ray showed a right upper lobe lesion with subsequent staging CT scans demonstrating the metastatic nature of his disease. Rarely, SCa can lead to paraneoplastic syndromes with neuro- logic sequelae, however the case patient’s neurologic symptoms resulted from extensive brain and spinal cord disease. In early stages, chemotherapy and surgical resection are treatment options but overall, the prognosis remains dismal with high recurrence rates post-operatively (2). Conclusion: In summary, this case exemplifies a rare and atypical manifestation of SCa and highlights the diagnostic chal- lenges associated with this type of malignancy. Pooja Kadam, MBBS, PGY-1 Resident, Brian Hirsh, MD, PGY-1 Resident, Internal Medicine, Albany Medical College I NSIDE THIS ISSUE : CASE REPORT: Sarcomatoid carcinoma of the lung presenting as shoulder pain and upper extremity weakness in a young man Pooja Kadam, MBBS, Brian Hirsh, MD 1-2 CASE REPORT: Human babesiosis: A tick-borne illness emerges from the swarm Neeraj Singh, MD, Justine Kang, MD 2-3 CASE REPORT: Chronic lymphocytic lymphoma/small lymphocytic lymphoma meets melanoma Rashmi Haria, MBBS 3-4 CASE REPORT: Varicella zoster virus meningoencephalitis and myelitis Enrico Bravo, MD 4-5 CASE REPORT: Seizures: An unusual initial presentation of metastatic prostate cancer Anupam Batra, MD 5-6 CASE REPORT: Prolonged Survival in Advanced Malignancy Aakash Modi, MD 6 SARCOMATOID CARCINOMA OF THE LUNG PRESENTING AS SHOULDER PAIN AND UPPER EXTREMITY WEAKNESS IN A YOUNG MAN Letter from the Editors Dear Readers: It is our distinct pleasure to continue the long tradition of the Albany Medical Review (AMR) with the release of the Winter 2014 edition. Since its inception, the Medicine House Staff has contributed case reports of significant interest and high educational value. As the newest editors of the AMR, we would like to express our gratitude to Dr. Ki Tae Mok, Dr. Raymond Smith and Michelle Snavely for their efforts in co-editing the presented case reports. In addition, we are thankful for the contributions made by the authors of the current edition of the AMR. We hope that you find this issue both enjoyable and educational. Thank you.”
Transcript of Albany Medical Revie Medical Review A QUARTERLY ONLINE PUBLICATION FROM ALBANY MEDICAL COLLEGE;...

Albany Medical Review A QUARTERLY ONLINE PUBLICATION FROM ALBANY MEDICAL COLLEGE; INTERNAL MEDICINE RESIDENCY
Editors-In-Chief: Anupam Batra, MD Aakash Modi, MD Consulting: Raymond P. Smith, MD Program Director Albany Medical College Ki Tae Mok, MD Stratton VA Medical Center
Technical Editor: Michelle Snavely
Albany Medical Center 43 New Scotland Avenue Albany, New York 12208 518.262.5377 www.amc.edu Contact: @mail.amc.edu
February 2014
Introduction: Pulmonary carcinoma with giant cells and spindle cells (sarcomatoid) is rare, accounting for 0.1-0.4% of all lung carcinomas. Common presenting symptoms include chest pain (14%), hemoptysis (49%), cough (46%) and dyspnea (3%). We present a unique case of a young man with sarcoma-toid carcinoma (SCa) presenting with shoulder pain and pro-gressive upper extremity weakness.
Case: A 36 year old male man with no medical history present-ed with a 6 months of right shoulder pain with associated right upper extremity weakness. He also reported a 30 pound weight loss and night sweats. He had a 20-pack year smoking history. There was no family history of cancer. Chest x-ray showed a right upper lobe lesion with erosion into the 2nd and 3rd posteri-or ribs. Head CT demonstrated multiple hyperdense lesions with vasogenic edema. Chest CT identified a right apical lung mass with extension into the paraspinal musculature and spinal canal at T3 and T4. CT–guided biopsy of the lung mass was performed and histopathological analysis revealed poorly differ-entiated carcinoma with giant cells and spindle cells (example Fig 1). The tumor had immunohistochemical staining positive for AE1:AE3 and CK7; negative for p40, TTF-1, NapsinA, calretinin, and p63. MRI of the brachial plexus and spine demonstrated invasion of the lower brachial plexus as well as multiple metastatic lesions of the cervical and thoracic spine with hemorrhagic features. Levetiracetam for seizure prophylax-is and dexamethasone for vasogenic edema were started fol-lowed by palliative whole brain and lung radiation therapy. Unfortunately, due to significant disease burden, the patient died 3 weeks later.
Discussion: SCa of the lung typically occurs in males in their 5th decade who are heavy smokers. Immunochemistry often demonstrates co-expression of cytokeratin and vimentin in tumor cells (1,2). Although SCa is rare, common sites of disease include the skin, thyroid, bone, and urinary tract, whereas pulmonary involvement is uncommon, accounting for less than 1% of all lung tumors. The majority of SCa present with local-ized symptoms in older patients (3). The case patient presented with right upper extremity parasthesiae and shoulder pain with-out respiratory symptoms, which is in stark contrast to the majority of SCa cases. The diagnosis was only made after chest
x-ray showed a right upper lobe lesion with subsequent staging CT scans demonstrating the metastatic nature of his disease. Rarely, SCa can lead to paraneoplastic syndromes with neuro-logic sequelae, however the case patient’s neurologic symptoms resulted from extensive brain and spinal cord disease. In early stages, chemotherapy and surgical resection are treatment options but overall, the prognosis remains dismal with high recurrence rates post-operatively (2).
Conclusion: In summary, this case exemplifies a rare and atypical manifestation of SCa and highlights the diagnostic chal-lenges associated with this type of malignancy.
Pooja Kadam, MBBS, PGY-1 Resident, Brian Hirsh, MD, PGY-1 Resident, Internal Medicine, Albany Medical College
INSIDE THIS ISSUE :
CASE REPORT: Sarcomatoid carcinoma of the lung presenting as shoulder pain and upper extremity weakness in a young man Pooja Kadam, MBBS, Brian Hirsh, MD
1-2
CASE REPORT: Human babesiosis: A tick-borne illness emerges
from the swarm
Neeraj Singh, MD, Justine Kang, MD
2-3
CASE REPORT: Chronic lymphocytic lymphoma/small lymphocytic lymphoma meets melanoma Rashmi Haria, MBBS
3-4
CASE REPORT: Varicella zoster virus meningoencephalitis and myelitis Enrico Bravo, MD
4-5
CASE REPORT: Seizures: An unusual initial presentation of metastatic prostate cancer Anupam Batra, MD
5-6
CASE REPORT: Prolonged Survival in Advanced Malignancy Aakash Modi, MD
6
SARCOMATOID CARCINOMA OF THE LUNG PRESENTING AS SHOULDER PAIN AND UPPER EXTREMITY WEAKNESS IN A YOUNG MAN
Letter from the Editors
Dear Readers: It is our distinct pleasure to continue the long tradition of the Albany Medical Review (AMR) with the release of the Winter 2014 edition. Since its inception, the Medicine House Staff has contributed case reports of significant interest and high educational value. As the newest editors of the AMR, we would like to express our gratitude to Dr. Ki Tae Mok, Dr. Raymond Smith and Michelle Snavely for their efforts in co-editing the presented case reports. In addition, we are thankful for the contributions made by the authors of the current edition of the AMR. We hope that you find this issue both enjoyable and educational. Thank you.”

References: Pelosi G, Sonzogni A, De Pas T, et al: pulmonary sarcomatoid carcinomas: a practical overview. International Journal of Surgical Pathology. 2010; 18(2): 103–120.
Franks T, Galvin J: Sarcomatoid Carcinoma of the Lung: Histologic Criteria and Com-mon Lesions in the Differential Diagnosis. Archives of Pathology & Laboratory Medi-cine: January 2010, Vol. 134, No. 1, pp. 49-54.
Travis W: Sarcomatoid Neoplasms of the Lung and Pleura. Archives of Pathology & Laboratory Medicine: November 2010, Vol. 134, No. 11, pp. 1645-1658.
Acknowledgments: Gurpreet Singh, MD, Department of Medicine, Albany Medical Center Hospital, Alba-ny, New York.
SARCOMATOID CARCINOMA OF THE LUNG PRESENTING AS SHOULDER PAIN AND UPPER EXTREMITY WEAKNESS IN A YOUNG MAN (continued)
PAGE 2 ALBANY MEDICAL REVIEW
Fig. 1. Histologic subtypes of sarcomatoid carcinoma. Pleomorphic carcinoma comprising squamous cell carcinoma associated with spindle cell carcinoma (A) but may be composed only of spindle and giant cells (B). Pure lesions of spindle cell carcinoma (C) and giant cell carcinoma (D) are rare. Carci-nosarcoma (E) contains adenocarcinoma on the right, which is intimately associated with chondrosar-coma on the left. Pulmonary blastoma (F) is characterized by malignant glands resembling fetal adenocarcinoma and malignant stroma (asterisk). A small squamoid nest (arrowhead), typical of this lesion, is also present. In the absence of malignant stroma, this lesion would be designated a well-differentiated, fetal adenocarcinoma (hematoxylin-eosin, original magnifications 40x [A and B] and 20x [C through F]) (Franks et al, 2010).
HUMAN BABESIOSIS: A TICK-BORNE ILLNESS EMERGES FROM THE SWARM
Neeraj Singh, MD,PGY-1 Resident, Justine Kang, MD, PGY-1 Resident, Internal Medicine, Albany Medical College
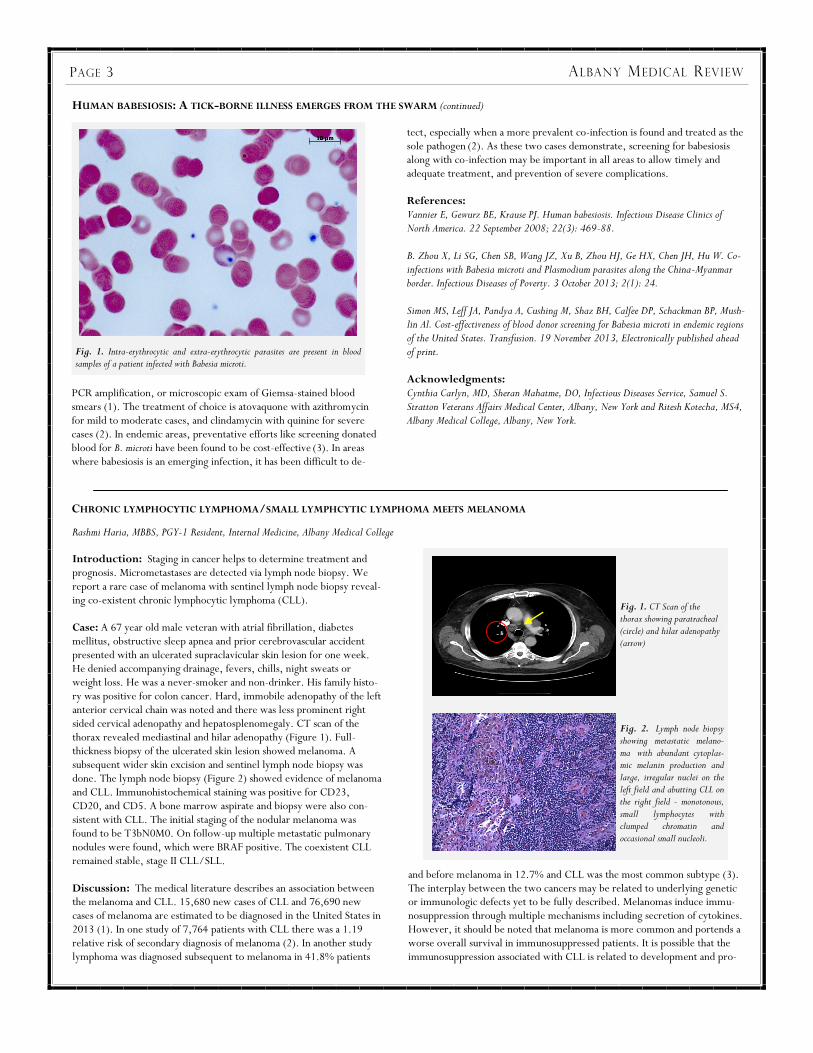
Introduction: Babesiosis, a tick-borne illness caused by intra-erythrocytic parasites, has variable clinical presentation, from mild to fatal. These two cases with distinct severities highlight differences in clinical approach and management. Case 1: A 71 year-old male presented to his clinic with fever, chills, dizziness, malaise, and left upper quadrant abdominal pain for two weeks after removing an engorged tick from his back. Examination revealed an afebrile patient with splenomegaly but no rash. Admission labs revealed hemolytic anemia with Hg 10.6 and MCV 89.9. A periph-eral blood smear showed intra-erythrocytic ring forms and Maltese cross formations consistent with Babesia microti, and parasitemia of 4%. After initiation of atovaquone and azithromycin, the patient’s clinical status rapidly improved and parasitemia declined to <1%. After four weeks, he remained well with no detectable parasites. Case 2: A 62 year-old male presented to the emergency department with dyspnea, shaking chills, sweats, and malaise for three weeks. Examination revealed sinus tachycardia at 110 bpm, yet EKG and echo-cardiogram were unremarkable. Splenomegaly was difficult to assess due to body habitus. Admission labs revealed thrombocytopenia (71k platelets) and transaminitis (AST 54, ALT 58). A CT chest revealed nonspecific lymphadenopathy and splenomegaly. Peripheral smear
analysis revealed many ring-formed intracellular parasites consistent with Babesia microti, with 8% parasitemia. Repeat labs revealed declining hemoglo-bin and platelet count to 66k, with relatively stable transaminitis (AST 64, ALT 53) and hyperbilirubinemia (2.6). Serology also returned positive for Borrelia burgdorferi. The patient was admitted to the ICU and started on quinine, clindamycin and doxycycline. Due to persistently elevated parasitemia (11%) and ongoing hemolysis, he underwent red cell exchange transfusion. Due to a quinine adverse effect, tinnitus, therapy was changed to azithromycin and atovaquone. After two weeks, the patient was disease-free with resolved parasitemia on follow-up blood smears. Discussion: Babesiosis is an emerging infectious disease endemic to the Northeastern and Midwestern United States1, with most recorded cases in New York State. There are also sporadic European cases, while other Babesia species affect Asia, Africa, and South America. Mild infections usually feature fever, fatigue, malaise, chills, sweats, headaches, myalgias, and arthralgias1. However, immunocompromised individuals, such as those with asplenia, malignancy, or HIV/AIDS, may suffer from complications such as hemolytic anemia or renal, liver, or respiratory failure, potentially causing death1. Those with parasitemia >10% or co-infection with other tick-borne diseases can suffer similar consequences. Diagnosis can be made by serology, babesia DNA
A B
C D
E F
PAGE 3 ALBANY MEDICAL REVIEW
HUMAN BABESIOSIS: A TICK-BORNE ILLNESS EMERGES FROM THE SWARM (continued)
PCR amplification, or microscopic exam of Giemsa-stained blood smears (1). The treatment of choice is atovaquone with azithromycin for mild to moderate cases, and clindamycin with quinine for severe cases (2). In endemic areas, preventative efforts like screening donated blood for B. microti have been found to be cost-effective (3). In areas where babesiosis is an emerging infection, it has been difficult to de-
tect, especially when a more prevalent co-infection is found and treated as the sole pathogen (2). As these two cases demonstrate, screening for babesiosis along with co-infection may be important in all areas to allow timely and adequate treatment, and prevention of severe complications. References: Vannier E, Gewurz BE, Krause PJ. Human babesiosis. Infectious Disease Clinics of North America. 22 September 2008; 22(3): 469-88. B. Zhou X, Li SG, Chen SB, Wang JZ, Xu B, Zhou HJ, Ge HX, Chen JH, Hu W. Co-infections with Babesia microti and Plasmodium parasites along the China-Myanmar border. Infectious Diseases of Poverty. 3 October 2013; 2(1): 24. Simon MS, Leff JA, Pandya A, Cushing M, Shaz BH, Calfee DP, Schackman BP, Mush-lin Al. Cost-effectiveness of blood donor screening for Babesia microti in endemic regions of the United States. Transfusion. 19 November 2013, Electronically published ahead of print. Acknowledgments: Cynthia Carlyn, MD, Sheran Mahatme, DO, Infectious Diseases Service, Samuel S. Stratton Veterans Affairs Medical Center, Albany, New York and Ritesh Kotecha, MS4, Albany Medical College, Albany, New York.
CHRONIC LYMPHOCYTIC LYMPHOMA/SMALL LYMPHCYTIC LYMPHOMA MEETS MELANOMA
Rashmi Haria, MBBS, PGY-1 Resident, Internal Medicine, Albany Medical College
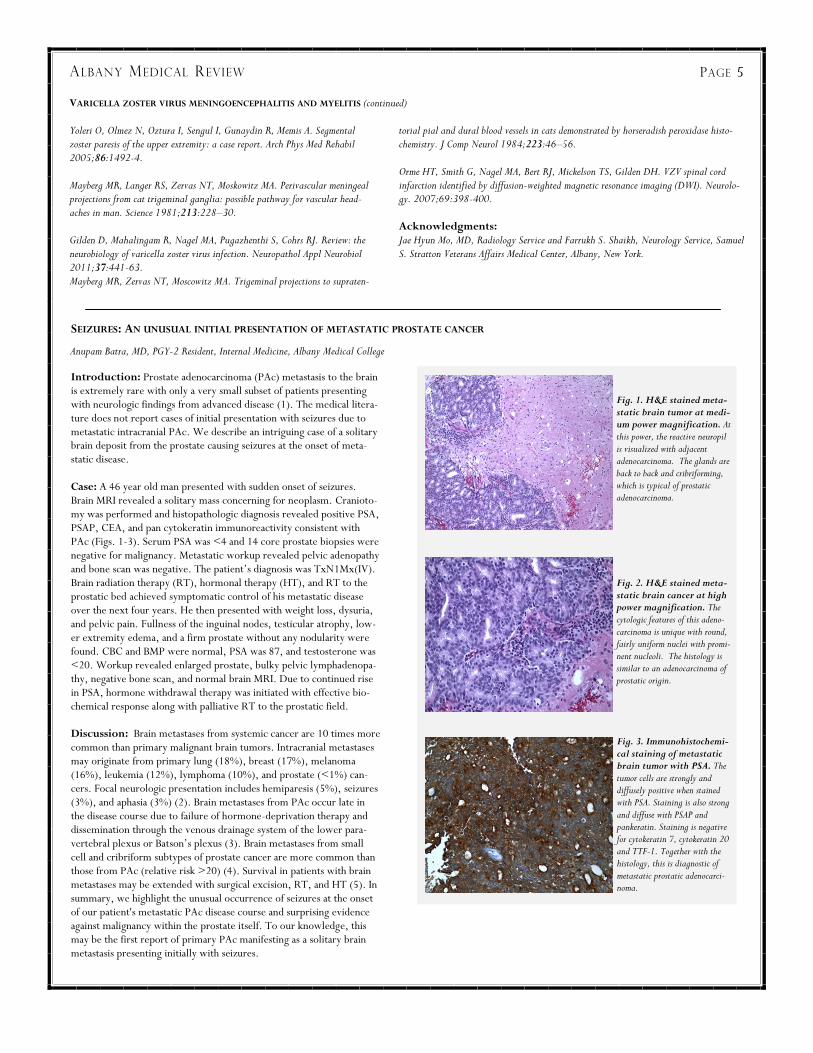
Introduction: Staging in cancer helps to determine treatment and prognosis. Micrometastases are detected via lymph node biopsy. We report a rare case of melanoma with sentinel lymph node biopsy reveal-ing co-existent chronic lymphocytic lymphoma (CLL). Case: A 67 year old male veteran with atrial fibrillation, diabetes mellitus, obstructive sleep apnea and prior cerebrovascular accident presented with an ulcerated supraclavicular skin lesion for one week. He denied accompanying drainage, fevers, chills, night sweats or weight loss. He was a never-smoker and non-drinker. His family histo-ry was positive for colon cancer. Hard, immobile adenopathy of the left anterior cervical chain was noted and there was less prominent right sided cervical adenopathy and hepatosplenomegaly. CT scan of the thorax revealed mediastinal and hilar adenopathy (Figure 1). Full-thickness biopsy of the ulcerated skin lesion showed melanoma. A subsequent wider skin excision and sentinel lymph node biopsy was done. The lymph node biopsy (Figure 2) showed evidence of melanoma and CLL. Immunohistochemical staining was positive for CD23, CD20, and CD5. A bone marrow aspirate and biopsy were also con-sistent with CLL. The initial staging of the nodular melanoma was found to be T3bN0M0. On follow-up multiple metastatic pulmonary nodules were found, which were BRAF positive. The coexistent CLL remained stable, stage II CLL/SLL. Discussion: The medical literature describes an association between the melanoma and CLL. 15,680 new cases of CLL and 76,690 new cases of melanoma are estimated to be diagnosed in the United States in 2013 (1). In one study of 7,764 patients with CLL there was a 1.19 relative risk of secondary diagnosis of melanoma (2). In another study lymphoma was diagnosed subsequent to melanoma in 41.8% patients
and before melanoma in 12.7% and CLL was the most common subtype (3). The interplay between the two cancers may be related to underlying genetic or immunologic defects yet to be fully described. Melanomas induce immu-nosuppression through multiple mechanisms including secretion of cytokines. However, it should be noted that melanoma is more common and portends a worse overall survival in immunosuppressed patients. It is possible that the immunosuppression associated with CLL is related to development and pro-
Fig. 1. Intra-erythrocytic and extra-erythrocytic parasites are present in blood samples of a patient infected with Babesia microti.
Fig. 1. CT Scan of the thorax showing paratracheal (circle) and hilar adenopathy (arrow) Fig. 2. Lymph node biopsy showing metastatic melano-ma with abundant cytoplas-mic melanin production and large, irregular nuclei on the left field and abutting CLL on the right field - monotonous, small lymphocytes with clumped chromatin and occasional small nucleoli.

CHRONIC LYMPHOCYTIC LYMPHOMA/SMALL LYMPHCYTIC LYMPHOMA MEETS MELANOMA (continued)
gression of melanoma. Although there is a reported association between the two cancer the underlying phenomenon is not fully characterized. Further research in this area may provide information new therapy op-tions and prognosis for coexistant melanoma/CLL. Conclusion: Further studies are necessary to explore the increased asso-ciation between melanoma and CLL in order to identify underlying genet-ic or immunologic factors responsible for this phenomenon. References: American Cancer Society.: Cancer Facts and Figures 2013. Atlanta, Ga: American Cancer Society, 2013.
Landgren O, Pfeiffer RM, Stewart L, et al. Risk of second malignant neoplasms among lymphoma patients with a family history of cancer. Int J Cancer. 2007;120(5):1099-102. Verwer N, Murali R, Winstanley J, et al. Lymphoma occurring in patients with cutaneous melanoma. J Clin Pathol. 2010;63(9):777-81. Acknowledgments: Syed Mehdi, MD, Chief of Hematology and Oncology and Lezah McCarthy, MD, Laboratory Service, Samuel S. Stratton Veterans Affairs Medical Center, Albany, New York.
PAGE 4 ALBANY MEDICAL REVIEW
VARICELLA ZOSTER VIRUS MENINGOENCEPHALITIS AND MYELITIS
Enrico Bravo, MD, VA Chief Medical Resident, Internal Medicine, Albany Medical College
Introduction: Viral encephalitis has a predilection for the elderly,
often resulting in serious neurologic manifestations. Varicella zoster
virus (VZV) encephalitis is a well-described but poorly understood
phenomenon. We report a case of varicella zoster encephalitis and
myelitis.
Case: An 88 year old man presented with a sub-acute history of fevers, confusion, hallucinations, unsteady gait, and left leg rash. He denied any neck stiffness, headache, emesis, or photophobia. There was no contact with sick persons and he did not receive a shingles vaccine. His vital signs were stable. He had chronic right corneal opacification with-out scleral ulceration and an old nasal scar. Visual tracking was pre-served and nuchal rigidity was absent. His right lower extremity was spastic, left lower extremity flaccid, and both were myoclonic. The right patella was hyper-reflexive, left patella was hypo-reflexive. Babin-ski sign was present bilaterally. A vesicular rash was noted along the L1-L4 dermatome at the left lower extremity. Lumbar puncture revealed a leukocyte count of 68/mL with 97% lymphocytes, negligable red blood cells, protein of 101 mg/dL, glucose of 46 mg/dL, and no oligo-clonal bands. Cerebrospinal fluid (CSF) was positive for varicella zoster virus DNA by PCR. MRI of the brain was unremarkable. MRI of the lumbar spine showed enhancement of the left ventral aspect of the cauda equina and multi-level foraminal narrowing at L3-L4, L4-L5, and L5-S1 without spinal stenosis (Figs 1 and 2). Intravenous acyclovir was initiated at a dose of 10 mg/kg/day with significant improvement in symptoms. Discussion: VZV is a human neurotropic alpha-herpesvirus affecting approximately 1 million individuals in the United States annually (1). Following primary infection, varicella virus remains latent within crani-al nerve, dorsal root, and autonomic ganglia. Declining cell-mediated immunity with age or immunosuppression leads to viral reactivation. Reactivation may result in herpes zoster, postherpetic neuralgia, vascu-lopathy, retinal necrosis, cerebellitis, and rarely, paresis (2,3). Central nervous system (CNS) infection with VZV may present as meningitis or meningoencephalitis. Patients present with fever, encephalopathy, headaches, focal neurologic deficits along with CSF findings of VZV DNA. In 8% of cases, VZV is the etiology for aseptic meningitis (4). VZV may also present as a self-limiting, post-infectious myelitis, possi-bly consisting of a monophasic spastic paraparesis (4). This has been reported to occur days to weeks after an acute shingles outbreak. CSF findings usually consist of mononuclear pleocytosis and a normal or mildly elevated protein level. Spinal MRI may show multi-level en-hancing lesions. VZV infection may result in vasculopathy or stroke
caused by virus infection of cerebral arteries (5). In one study, VZV was believed to spread transmurally from the adventitia to the intima, presumably after transaxonal spread to the artery ganglionic afferent fibers (4,6). In an-other study, VZV vasculopathy led to spinal cord infarction detected by diffu-sion-weighted MRI with subsequent virologic confirmation (7).
Conclusion: Clinicians should suspect VZV meningoencephalitis and myeli-
tis in patients with shingles, encephalopathy, and motor deficit.
References: Mueller NH, Gilden DH, Cohrs RJ, Mahalingam R, Nagel MA. Varicella zoster infec-tion: clinical features, molecular pathogenesis of disease, and latency. Neurol Clin 2008;26:675-97. Merchet MP, Gruener G. Segmental zoster paresis of limbs. Electromyogr Clin Neuro-physiol 1996;36:369-75.
Fig. 1. MRI Lumbar spine. T2-weighted sagittal view of lumbar signal demonstrating elongated enhancement of some of the ventral cauda equina nerve roots. Fig. 2. MRI Lumbar spine. T2-weighted horizontal view of lumbar spine showing enhance-ment of nerve bundles suggesting breached blood-brain barrier.
Yoleri O, Olmez N, Oztura I, Sengul I, Gunaydin R, Memis A. Segmental zoster paresis of the upper extremity: a case report. Arch Phys Med Rehabil 2005;86:1492-4. Mayberg MR, Langer RS, Zervas NT, Moskowitz MA. Perivascular meningeal projections from cat trigeminal ganglia: possible pathway for vascular head-aches in man. Science 1981;213:228–30. Gilden D, Mahalingam R, Nagel MA, Pugazhenthi S, Cohrs RJ. Review: the neurobiology of varicella zoster virus infection. Neuropathol Appl Neurobiol 2011;37:441-63. Mayberg MR, Zervas NT, Moscowitz MA. Trigeminal projections to supraten-
torial pial and dural blood vessels in cats demonstrated by horseradish peroxidase histo-chemistry. J Comp Neurol 1984;223:46–56. Orme HT, Smith G, Nagel MA, Bert RJ, Mickelson TS, Gilden DH. VZV spinal cord infarction identified by diffusion-weighted magnetic resonance imaging (DWI). Neurolo-gy. 2007;69:398-400. Acknowledgments: Jae Hyun Mo, MD, Radiology Service and Farrukh S. Shaikh, Neurology Service, Samuel S. Stratton Veterans Affairs Medical Center, Albany, New York.
PAGE 5 ALBANY MEDICAL REVIEW
SEIZURES: AN UNUSUAL INITIAL PRESENTATION OF METASTATIC PROSTATE CANCER
Anupam Batra, MD, PGY-2 Resident, Internal Medicine, Albany Medical College
Introduction: Prostate adenocarcinoma (PAc) metastasis to the brain is extremely rare with only a very small subset of patients presenting with neurologic findings from advanced disease (1). The medical litera-ture does not report cases of initial presentation with seizures due to metastatic intracranial PAc. We describe an intriguing case of a solitary brain deposit from the prostate causing seizures at the onset of meta-static disease. Case: A 46 year old man presented with sudden onset of seizures. Brain MRI revealed a solitary mass concerning for neoplasm. Cranioto-my was performed and histopathologic diagnosis revealed positive PSA, PSAP, CEA, and pan cytokeratin immunoreactivity consistent with PAc (Figs. 1-3). Serum PSA was <4 and 14 core prostate biopsies were negative for malignancy. Metastatic workup revealed pelvic adenopathy and bone scan was negative. The patient’s diagnosis was TxN1Mx(IV). Brain radiation therapy (RT), hormonal therapy (HT), and RT to the prostatic bed achieved symptomatic control of his metastatic disease over the next four years. He then presented with weight loss, dysuria, and pelvic pain. Fullness of the inguinal nodes, testicular atrophy, low-er extremity edema, and a firm prostate without any nodularity were found. CBC and BMP were normal, PSA was 87, and testosterone was <20. Workup revealed enlarged prostate, bulky pelvic lymphadenopa-thy, negative bone scan, and normal brain MRI. Due to continued rise in PSA, hormone withdrawal therapy was initiated with effective bio-chemical response along with palliative RT to the prostatic field. Discussion: Brain metastases from systemic cancer are 10 times more common than primary malignant brain tumors. Intracranial metastases may originate from primary lung (18%), breast (17%), melanoma (16%), leukemia (12%), lymphoma (10%), and prostate (<1%) can-cers. Focal neurologic presentation includes hemiparesis (5%), seizures (3%), and aphasia (3%) (2). Brain metastases from PAc occur late in the disease course due to failure of hormone-deprivation therapy and dissemination through the venous drainage system of the lower para-vertebral plexus or Batson’s plexus (3). Brain metastases from small cell and cribriform subtypes of prostate cancer are more common than those from PAc (relative risk >20) (4). Survival in patients with brain metastases may be extended with surgical excision, RT, and HT (5). In summary, we highlight the unusual occurrence of seizures at the onset of our patient's metastatic PAc disease course and surprising evidence against malignancy within the prostate itself. To our knowledge, this may be the first report of primary PAc manifesting as a solitary brain metastasis presenting initially with seizures.
VARICELLA ZOSTER VIRUS MENINGOENCEPHALITIS AND MYELITIS (continued)
Fig. 1. H&E stained meta-static brain tumor at medi-um power magnification. At this power, the reactive neuropil is visualized with adjacent adenocarcinoma. The glands are back to back and cribriforming, which is typical of prostatic adenocarcinoma.
Fig. 2. H&E stained meta-static brain cancer at high power magnification. The cytologic features of this adeno-carcinoma is unique with round, fairly uniform nuclei with promi-nent nucleoli. The histology is similar to an adenocarcinoma of prostatic origin. Fig. 3. Immunohistochemi-cal staining of metastatic brain tumor with PSA. The tumor cells are strongly and diffusely positive when stained with PSA. Staining is also strong and diffuse with PSAP and pankeratin. Staining is negative for cytokeratin 7, cytokeratin 20 and TTF-1. Together with the histology, this is diagnostic of metastatic prostatic adenocarci-noma.

PAGE 6 ALBANY MEDICAL REVIEW
References: Catane R, Kaufman J, West C, Merrin C, Tsukada Y, Murphy GP. Brain metas-tasis from prostatic carcinoma. Cancer. 1976;38:2583-2537. Saitoh H, Hida M, Shimbo T, Nakamura K, Yamagata J, Satoh T. Metastatic patterns of prostatic cancer. Correlation between sites and number of organs involved. Cancer. 1984;54:3078-3084. Taylor HG, Lefkowitz M, Skoog SJ, Miles BJ, McLeod DG, Coggin JT. Intra-cranial metastases in prostate cancer. Cancer. 1984;53:2728-2730. Demierre B, Berney J. [Intracranial metastases of cancer of the prostate]. Neuro-chirurgie. 1983;29;143-149. Lu-Emerson C, Eichler AF. Brain metastases. Continuum (Minneap Minn). 2012 Apr 18(2):295-311. Posner JB, Chernik NL. Intracranial metastases from systemic cancer. Adv Neu-rol. 1978;(19):579-592.
Lynes WL, Bostwick DG, Freiha FS, Stamey TA. Parenchymal brain metastases from adenocarcinoma of prostate. Urology. 1986;28:280-287. Tremont-Lukats IW, Bobustuc G, Lagos GK, Lolas K, Kyritsis AP, Puduvalli VK. Brain metastasis from prostate carcinoma: The M. D. Anderson Cancer Center experience. Cancer. 2003 Jul 15;98(2):363-8. Batson OV: The function of the vertebral veins and their role in the spread of metasta-ses, Ann Surg 1940;(112):138. Rubin P, Bakemeier RF: Clinical Oncology for Medical Students and Physicians: a Multidisciplinary Approach 5th ed, The University of Rochester School of Medicine and Dentistry, 1978. Achknowledgements: Syed Medhi, MD, Chief of Hematology and Oncology and Lezah McCarthy, MD, Laboratory Service, Samuel S. Stratton Veterans Affairs Medical Center, Albany, New York.
SEIZURES: AN UNUSUAL INITIAL PRESENTATION OF METASTATIC PROSTATE CANCER (continued)
PROLONGED SURVIVAL IN ADVANCED MALIGNANCY
Aakash Modi, MD, PGY-2 Resident, Internal Medicine, Albany Medical College
Introduction: The approximate five-year survival rate for advanced esophageal cancer is 17.3%. Case: In 2005, a 57-year-old male, with no significant past medical history, presented to his primary doctor complaining of worsening epigastric pain of several years for which he was previously prescribed Ranitidine. His symptoms progressively worsened and now he also reported of dysphagia. Endoscopy on March 16, 2005 confirmed a moderately differentiated adenocarcinoma. Staging workup included a CT scan of the chest, abdomen, and pelvis. Scan showed 1.5 cm right distal paraesophageal lymphadenopathy (N1 disease)M0 with final staging TxN1M0. He was treated with neu-adjuvant chemotherapy and radiation followed by esophagectomy. He was followed very closely by Medical Oncology and has had multiple recurrences in the last 8 years: Lung metastasis 2006 Brain metastasis 2007 Liver metastasis 2008 Liver metastasis 2011 Lung metastasis 2013 At each recurrence, he was thoroughly evaluated and very aggressively treated. He underwent resection of the lung metastasis in 2006, fol-lowed by systemic chemotherapy. Then, in 2007, he underwent a resection of the brain metastasis (shown in Figure 1) followed by whole brain radiation and systemic therapy with temozolamide. He also went through a resection of hepatic metastasis, followed by systemic chemo-therapy. The patient has done very well and is currently still being followed off treatment by the Medical Oncology clinic. He has main-tained his weight and performance status. Discussion: Esophageal cancer is the third most common type of cancer of the digestive tract and ranks as the seventh most common cause of cancer-related deaths worldwide. Males over 50 years of age are at the highest risk for this disease. “Brain metastases have been reported in only 1.7-3.6% of all patients with different types of esopha-geal cancer”. The presented case clearly illustrates that aggressive man-agement of advanced malignancies can increase the overall survival, as
well as, quality of life. The case further indicates the importance of a multi-specialty approach involving medical oncology, surgical oncology, radiation oncology, along with, palliative care in complex advanced malignancies. Decisions for comfort care (hospice) should only be taken after consultations with all providers actively involved in the management of such diseases since newer, novel agents are continuously being approved by the FDA. References: Lightdale CJ. Esophageal cancer. American College of Gastroenterology. Am J Gastro-enterol1999. SEER Cancer Statistics Factsheets: Esophageal Cancer. National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/statfacts/html/esoph.html. Jemal A, Bray F, Center MM, et. Al. Global cancer statistics. CA Cancer J Clin 2011; 61;69. Acknowledgements: Syed Mehdi, MD, Chief of Hematology and Oncology, Samuel S. Stratton Veterans Affairs Medical Center, Albany, New York.
Fig. 1. A 2 cm sized ring-enhancing mass (arrow) in the left cerebellum is appreciated with surrounding edema leading to compression of the fourth ventricle.


















