
Electro-Mechanical Acoustical Airway Clearance™ Comprehensive ...
Airway Clearance Therapy: Finding the Evidence
Teresa A Volsko MHHS RRT FAARC
IntroductionAirway Clearance Therapy: What Is It and Why Is It Needed?
Impairment of Secretion Clearance and Pulmonary DiseaseNeurorespiratory Dysfunction and Secretion Clearance Problems
Indications for Airway ClearanceWhere to Look for Current Evidence
StudiesSynthesisSystematic ReviewsEvidenced-Based Clinical Practice Guidelines
Putting Evidence Into PracticeSummary
Disease processes can impair ciliary function, alter secretion production and mucus rheology, andinterfere with the cough reflex. Airway clearance therapy has been a cornerstone of therapy aimedat minimizing the devastating effects of airway obstruction, infection, and inflammation due tomucus stasis on the conducting airways and lung parenchyma. Although challenges to performingclinical studies evaluating the effectiveness of airway clearance therapeutic modalities exist, re-sources are available in the literature. In addition to device evaluations and original clinical re-search, the expert opinion, systematic reviews, and evidence-based practice guidelines can be found.These tools can be used to develop protocols and pathways to guide our practice. Monitoring andreporting patient, process, and financial outcomes are essential steps germane to the implementa-tion of evidence-based care. Key words: airway clearance devices; cough; mucociliary transport;postural drainage; active cycle of breathing; positive expiratory pressure; oscillatory positive expiratorypressure; HFCWO; secretion clearance. [Respir Care 2013;58(10):1669–1678. © 2013 Daedalus En-terprises]
Introduction
The mucociliary escalator and cough reflex maintainoptimal function of the respiratory system by removing
secretions and preventing airways obstruction. In health,10–100 mL1 of airway secretions are continuously pro-duced and cleared by the centripetal movement of themucociliary escalator, and with the aid of transient in-creases in expiratory air flow.2 There are a variety of fac-tors that can interfere with the body’s natural defense mech-
Ms Volsko is affiliated with the Department of Respiratory Care, AkronChildren’s Hospital, Akron, Ohio.
Ms Volsko presented a version of this paper at the 28th New Horizonsin Respiratory Care Symposium, “The Scientific Basis for RespiratoryCare,” at the AARC Congress 2012, held November 10–13, 2012, inNew Orleans, Louisiana.
The author has disclosed no conflicts of interest.
Correspondence: Teresa A Volsko MHHS RRT FAARC, Department ofRespiratory Care, Akron Children’s Hospital, One Perkins Square, AkronOH 44308. E-mail: [email protected].
DOI: 10.4187/respcare.02590
RESPIRATORY CARE • OCTOBER 2013 VOL 58 NO 10 1669

anism, making it difficult to mobilize and evacuatesecretions from the airways. The aging process, tobaccouse, and environmental exposures reduce the efficacy ofciliary structure and function.3-6 Disease processes such asprogressive neurodegenerative conditions inhibit the nor-mal cough reflex.7,8 Pulmonary disorders such as cysticfibrosis (CF), COPD, and bronchiectasis alter the produc-tion and composition of mucus, and mucociliary clearancedisorders, such as primary ciliary dyskinesia, reduce theefficacy of ciliary structure and function.9-11
Airway obstruction and structural damage to the air-ways and lung parenchyma result from recurring secretionretention, infection, and inflammatory changes. As a re-sult, airway clearance techniques (ACTs) and devices areused to aid in mucus mobilization and expectoration. The
objectives of this paper are to describe and review the needfor ACTs, discuss methodological challenges and limita-tions to study design, and to describe methods for applyingevidence to clinical practice.
Airway Clearance Therapy: What Is Itand Why Is It Needed?
ACT utilizes physical or mechanical means to manipu-late air flow, aid in the mobilization of tracheal bronchialphlegm cephalad, and facilitate evacuation by coughing.12
Breathing maneuvers,13 gravity assisted drainage,14 man-ual techniques,15 and/or mechanical devices16-18 can beused to alter air flow and/or produce a cough or cough-likeeffect (Table 1). Patient age, disease severity, ease of use,
Table 1. Types of Airway Clearance Modalities Available to Facilitate Secretion Removal
Technique/Device Description
Breathing techniques
Active cycle of breathing A breathing technique that uses alternating cycles of breathing control or relaxed breathing,thoracic expansion exercises to mobilize secretions, and the forced expiration techniqueto facilitate secretion removal.13
Autogenic drainage A technique that uses breathing at the low volumes to loosen secretions, a normal tidalvolume to collect secretions, and large lung volumes to maximize expiratory flow andmove secretions from the central airways where they can be cleared by a cough.13
Manual techniques
Postural drainage The use of patient positioning to assist gravity in facilitating the movement of secretionsfrom peripheral airways to the larger bronchi where they can be cleared.14
Clapping, percussion, and vibration Clapping or percussion is the manual external striking of the chest wall with a cuppedhand, or mechanical device in a rhythmic fashion to loosen secretions from the bronchialwalls. Vibrations are applied to the external chest wall by placing both hands (one overthe other) over the area of the patient’s chest wall to be vibrated, then tensing andcontracting the shoulder and arm muscles while the patient exhales to mobilizesecretions cephalad.15
Mechanical devices
Positive expiratory pressure (PEP) The PEP device consists of a user interface (face mask or mouthpiece) and a one-wayvalve attached to an expiratory resistor. A manometer may be used to monitor pressuresduring the maneuver. Tidal breathing, with a slightly active expiration through theexpiratory resistor will produce expiratory pressures of 10–20 cm H2O at mid-expirationto stent airways open, or increase intrathoracic pressure distal to retained secretions byincreasing functional residual capacity or collateral ventilation.16
Oscillatory positive expiratory pressure (OPEP) OPEP therapy devices use a mechanical means to interrupt flow, and an expiratory resistorto create air flow oscillations during active exhalation of a tidal volume breath throughthe device. Air flow oscillations reportedly decrease the viscoelastic properties of mucus,making it easier to mobilize.16
High frequency chest wall compression An inflatable vest is used to apply high-frequency, small-volume expiratory pulses to theexternal chest wall. Negative transrespiratory pressure is generated by the short, rapidexpiratory flow pulses at 2–25 Hz, to loosen, collect, and mobilize airway secretions.17
Intrapulmonary percussive ventilation Intrapulmonary percussive ventilation creates a positive transrespiratory pressure byinjecting short, rapid inspiratory flow pulses into the airway opening, and relies on chestwall elastic recoil for passive exhalation.
Mechanical cough assist Positive pressure is provided during inspiration to provide a slightly larger than tidalbreath, followed by negative pressure to expel secretions from the airways. Typically 5cycles of positive (inspiration) and negative (expiration) pressure breaths are followed bya period of normal breathing or ventilator use for 20–30 seconds, to avoidhyperventilation. The sequence is repeated until no further secretions are expulsed.
AIRWAY CLEARANCE THERAPY: FINDING THE EVIDENCE
1670 RESPIRATORY CARE • OCTOBER 2013 VOL 58 NO 10

comfort, and cost affect device selection, adherence toprescribed plan, and the efficacy with which secretions areremoved.
There are a number of disease processes that impairciliary function, alter secretion production and mucusrheology, and interfere with the cough reflex. Secretionsthat accumulate or are stagnant obstruct conducting air-ways, are conduits for bacterial colonization and infection,evoke inflammatory response, and contribute to airwayand parenchymal damage (Fig. 1).
Impairment of Secretion Clearance andPulmonary Disease
Rare genetic disorders such as primary ciliary dyskine-sia and Kartagener syndrome impair cilia structure andfunction.19,20 Although manifestations of these disordersalso include chronic sinusitis, sinus hypoplasia, and secre-tory otitis media, repeated lower-respiratory-tract infec-tions contribute to the development of bronchiectasis.21
Ciliary function is also altered with chronic pulmonarydisease such as asthma, COPD, and CF. The literaturereports impaired ciliary function, and changes in the flowor surface properties of mucus contribute to impairedmucociliary transport during exacerbations of asthma, aswell as with chronic bronchitis. Thomas et al evaluated theepithelial ultrastructure and ciliary function of patients withvarying degrees of asthma severity and healthy controls.Subjects with severe asthma had a significantly lower num-ber of ciliated cells and higher dyskinesia and cilia immo-tility indices, compared to healthy controls or those withmild or moderate asthma.22 Ciliary disorientation and areduction in mean cilia beat frequency were found in sub-jects with moderate and severe asthma.22 Mucus hyper-secretion and airways inflammation limit air flow during
exacerbations of asthma. Typically, as bronchodilator andanti-inflammatory agents reverse the air-flow limitations,secretion clearance functions are restored.
An increased number of abnormal cilia are found withchronic bronchitis as well. Ciliary dysfunction is exacer-bated by continued cigarette use. Compared to non-smokers and ex-smokers with chronic bronchitis, thosewho continued to smoke had the highest percentage ofciliary abnormalities, as well as the presence of ciliaryparalysis, features comparable to that found in bronchi-ectasis.23 Unlike asthma, mucociliary transport does notfully recover in chronic bronchitis. Recurrent infectionsand inflammation further reduce the number of ciliatedepithelium. Hypersecretion of mucus with similar rheo-logical characteristics to the mucus of those with CFlimit air flow and affect the ability to generate effectivecough flows.24 The increased propensity for mucus re-tention, recurrent inflammation, and infection damageconducting airways and inhibit restoration of mucociliaryfunction.
Ciliary dysfunction in patients with CF is attributed toan abnormality of the gene that encodes for CF transmem-brane conductance regulator.25 Dysregulation of the saltand water content may reduce airway surface liquid, in-hibit ciliary function, and create an environment that isconducive to bacterial colonization and infection.26 As aresult, an exaggerated inflammatory response occurs. Theperipheral airways containing mucus filled bacteria arealso host to inflammatory cells, and cellular breakdownproducts such as neutrophil-derived deoxyribonucleic acidand filamentous actin.27 Airways secretions are more vis-cous and adhesive, and therefore difficult to clear. Thisvicious circle of chronic infection, inflammation, and mu-cus stasis limits air flow in the larger airways and leads tothe complete obstruction of the small peripheral airways
Fig. 1. Physiological factors that reduce the efficacy of mucociliary escalator function.
AIRWAY CLEARANCE THERAPY: FINDING THE EVIDENCE
RESPIRATORY CARE • OCTOBER 2013 VOL 58 NO 10 1671

and the development of diffuse, irreversible bronchiecta-sis.28,29
Neurorespiratory Dysfunction andSecretion Clearance Problems
Cough is a defense mechanism, initiated either volun-tarily or by the stimulation of cough receptors locatedprimarily in the central airways, which aids in the evacu-ation of secretions, and foreign substances from the respi-ratory tract.30 Spinal cord pathology and/or diseases of theneurorespiratory system can impact the control of motornerves, and, depending on the level of insult, interrupt orweaken respiratory muscle function. Cervical spinal cordinjuries, especially those occurring between C3 and C5,affect diaphragmatic function, and contribute to respira-tory insufficiency. Patients with high cervical injuries of-ten require long-term mechanical ventilatory support. In-juries to the thoracic and lumbar spine interrupt abdominaland intercostal muscle function and impair cough func-tion.31 Lack of an adequate cough contributes to the de-velopment of recurrent respiratory-tract infections and at-electasis and remains a major cause of death in this patientpopulation.32
Chronic muscle disease, such as muscular dystrophies,and motor neuron diseases cause muscle fatigue and wast-ing. Respiratory muscle weakness can impair a cough mech-anism by reducing expiratory flow, and the expulsion phaseof a cough, which hinders secretion removal and the abil-ity to maintain adequate lung function.33,34 Flow-volumeloops may be performed and evaluated for the presence ofcough spikes to determine cough effectiveness. Coughspikes are large increases in expiratory flow generatedfrom the presence of enough intrathoracic pressure to causedynamic compression of air within the large airways as theglottis is opened during a cough maneuver.35 In a study of53 patients with motor neuron disease, Chaudri et al re-ported that subjects unable to generate cough spikes wereat increased risk for pulmonary infection and death (79%mortality rate), compared to those with the ability to gen-erate cough spikes (50% mortality rate).36
Indications for Airway Clearance
ACT is indicated for individuals whose function of themucociliary escalator and/or cough mechanics are alteredand whose ability to mobilize and expectorate airwayssecretions is compromised. Early diagnosis and implemen-tation of ACT, coupled with medical management of in-fections and airways inflammation, can reduce morbidityand mortality associated with chronic pulmonary37,38 andneurorespiratory disease.39 Today a variety of interven-tions may be used to enhance airway clearance, with thegoal of improving lung mechanics and gas exchange and
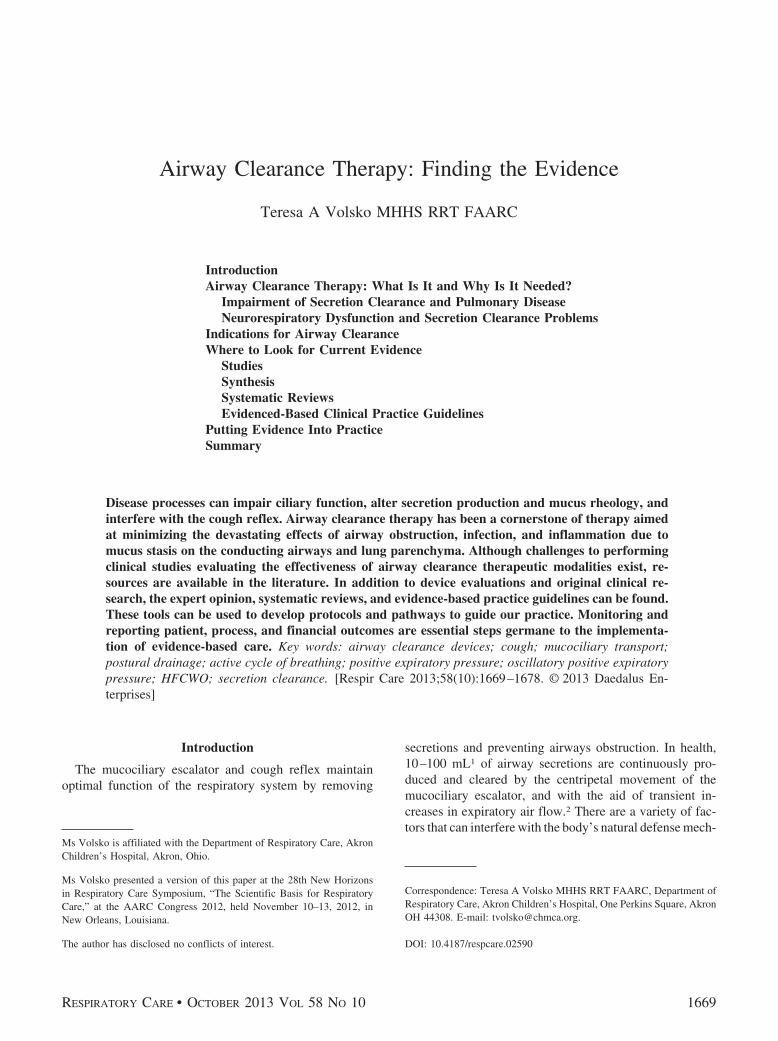
preventing atelectasis and infection. Choosing the mostappropriate airway-clearance device or technique for anindividual patient requires integral knowledge of devicefunction and limitations, as well as an assessment of thepatient’s cognitive ability and the severity of pulmonaryimpairment (Table 2).
Where to Look for Current Evidence
There is a lack of empirical evidence to support thesuperiority of any particular airway-clearance device ortechnique. There is much interest in developing evidence-based airway clearance protocols to guide device/techniqueselection. Searching through the literature to find the ev-idence may be a time-consuming venture. Therefore, it isimportant to become familiar with resources that are avail-able to synthesize information, and the barriers that existwith respect to airway clearance research.
Studies
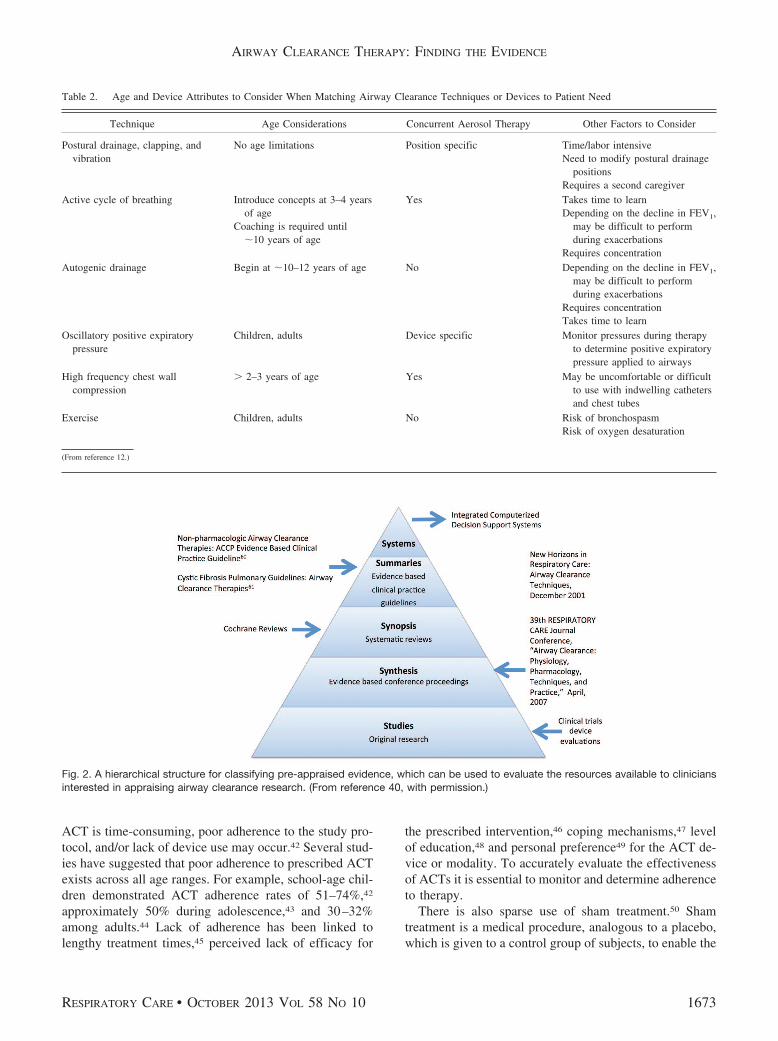
Evidence available in the literature can be categorizedinto pre-appraised levels40 (Fig. 2). Device evaluation andclinical studies lie at the base of this hierarchical structure.It is time and effort intensive to sift through the plethoraof studies evaluating airway clearance techniques and de-vices. Moreover, there is a dearth of high level airwayclearance research. High-level studies are prospective, ran-domized, blinded, placebo-controlled, and assess patient-important outcomes. As a result, several methodologicalchallenges to ACT research exist. Many clinical studieshave very small sample sizes and are not adequately pow-ered. It is often difficult for a single center, especially withdisease conditions that are rare, to obtain a sufficient num-ber of subjects, and therefore report results with smallsamples of subjects.41 Other challenges to designing andconducting valid clinical trials exist. Due to the size anddesign of ACT modalities, it is difficult to mask the treat-ment assignment to the subject and/or the research team,making blinding nearly impossible. Knowledge of the typeand/or sequence of ACT provided may influence the sub-ject’s decision to enroll in or to continue with study par-ticipation. There is also the risk that the subject’s personalpreferences or the researcher’s knowledge of the devicebeing used may bias study outcomes. It is also difficult tocontrol for variations in practice and use of ACTs.
Alterations in device use and adherence to protocol canunintentionally influence outcomes. For example, if per-cussion, postural drainage, and vibration were to be pro-vided for a 30 min period to10 consecutive patients by thesame clinician, how could the researchers guarantee thatthe clapping and vibration were provided with the sameintensity for each of those subjects? The length of thetreatment of intervention may also have an impact. Since
AIRWAY CLEARANCE THERAPY: FINDING THE EVIDENCE
1672 RESPIRATORY CARE • OCTOBER 2013 VOL 58 NO 10
ACT is time-consuming, poor adherence to the study pro-tocol, and/or lack of device use may occur.42 Several stud-ies have suggested that poor adherence to prescribed ACTexists across all age ranges. For example, school-age chil-dren demonstrated ACT adherence rates of 51–74%,42
approximately 50% during adolescence,43 and 30–32%among adults.44 Lack of adherence has been linked tolengthy treatment times,45 perceived lack of efficacy for
the prescribed intervention,46 coping mechanisms,47 levelof education,48 and personal preference49 for the ACT de-vice or modality. To accurately evaluate the effectivenessof ACTs it is essential to monitor and determine adherenceto therapy.
There is also sparse use of sham treatment.50 Shamtreatment is a medical procedure, analogous to a placebo,which is given to a control group of subjects, to enable the
Table 2. Age and Device Attributes to Consider When Matching Airway Clearance Techniques or Devices to Patient Need
Technique Age Considerations Concurrent Aerosol Therapy Other Factors to Consider
Postural drainage, clapping, andvibration
No age limitations Position specific Time/labor intensiveNeed to modify postural drainage
positionsRequires a second caregiver
Active cycle of breathing Introduce concepts at 3–4 yearsof age
Coaching is required until�10 years of age
Yes Takes time to learnDepending on the decline in FEV1,
may be difficult to performduring exacerbations
Requires concentrationAutogenic drainage Begin at �10–12 years of age No Depending on the decline in FEV1,
may be difficult to performduring exacerbations
Requires concentrationTakes time to learn
Oscillatory positive expiratorypressure
Children, adults Device specific Monitor pressures during therapyto determine positive expiratorypressure applied to airways
High frequency chest wallcompression
� 2–3 years of age Yes May be uncomfortable or difficultto use with indwelling cathetersand chest tubes
Exercise Children, adults No Risk of bronchospasmRisk of oxygen desaturation
(From reference 12.)
Fig. 2. A hierarchical structure for classifying pre-appraised evidence, which can be used to evaluate the resources available to cliniciansinterested in appraising airway clearance research. (From reference 40, with permission.)
AIRWAY CLEARANCE THERAPY: FINDING THE EVIDENCE
RESPIRATORY CARE • OCTOBER 2013 VOL 58 NO 10 1673

effects of the supposedly “active” treatment to be assessedobjectively. A sham treatment is not necessarily expectedto be ineffective. Rather, the purpose of a sham treatmentgroup is to identify any specific benefit of one element ofa medical treatment above and beyond all benefits thatmight be attributed to everything else about that treatment.Since ineffective mucociliary clearance leads to increasedmorbidity and mortality, ethical considerations deter theuse of sham treatment in ACT research.
Synthesis
Conference proceedings review the clinical evidence andscientific basis for diagnosis and treatment of diseases orthe use of therapeutic modalities. For respiratory therapiststhe New Horizons Symposiums and RESPIRATORY CARE
Journal Conferences provide a venue for clinical expertsand scientists to review and present evidence specific toour practice. Conference proceedings are then published inRESPIRATORY CARE. Two conference proceedings were ded-icated to airway clearance: the New Horizons Symposium,presented at the 47th AARC Congress in December, 2001,and the 39th RESPIRATORY CARE Journal Conference, con-ducted in April, 2007. The scientific evidence with respectto the physiology of mucus production and cough, phar-macologic management, and non-pharmacologic ap-proaches to airway clearance were presented and discussed,and findings summarized. The aforementioned narrativereviews also provide recommendations for new directionsand opportunities for future research and clinical care.
Systematic Reviews
A systematic review is a summary of the literature thatuses an organized method to thoroughly search, criticallyappraise, and statistically combine data from valid studiesin the literature.51 This evaluation is performed systemat-ically and rigorously, the results of which are based on thestrength of the evidence found in the literature. SystematicACT reviews are available and include reviews of specifictechniques, such as active cycle of breathing,52 positiveexpiratory pressure devices,53 and oscillatory positive ex-piratory pressure devices,54 as well as sequencing pharma-cologic agents,55,56 and comparing therapeutic modalitiesfor specific diseases such as CF57 or COPD.58
Evidenced-Based Clinical Practice Guidelines
In the last decade, 2 airway clearance clinical practiceguidelines have been published. Guided by systematic re-view of the literature from multiple databases and handsearches, authors constructed recommendations for thenon-pharmacologic management of secretion clearance inpulmonary disease59 and the use of airway clearance forthe treatment of CF lung disease.60 The authors acknowl-edged methodological limitations of airway clearance re-search, and reported recommendations made throughthese guidelines were derived from a “fair” level of evi-dence, or data that were valid enough to make plausibleconclusions in the absence of rigorously conducted scien-tific studies. Recommendations were provided with re-
Table 3. A Summary of Clinical Practice Guideline Recommendations
Cystic Fibrosis Pulmonary Guidelines: Airway Clearance Therapies60 Nonpharmacologic Airway Clearance Therapies: American Collegeof Chest Physicians Evidence-Based Clinical Practice Guidelines59
Airway-clearance therapy is recommended for all patients with cysticfibrosis, for clearance of sputum, maintenance of lung function,and improved quality of life.
Postural drainage, clapping, and vibration has relatively modesteffectiveness, with unproven long-term benefits.
No airway-clearance therapy has been demonstrated to be superior toany other.
Manually assisted cough and cough assist should be considered forpatients with expiratory muscle weakness and impaired cough,to reduce the incidence of respiratory complications.
For the individual, one form of airway-clearance therapy may besuperior to the others. The prescription of airway-clearancetherapy should be individualized, based on factors such as age,patient preference, and adverse events, among others.
Manually assisted cough may be detrimental and should not beused in patients with air-flow obstruction, such as COPD.
Aerobic exercise is recommended for patients with cystic fibrosis, asan adjunctive therapy for airway clearance and its additionalbenefits to overall health.
Huffing and autogenic drainage should be taught as an adjunct toother methods of sputum clearance in patients with COPD andcystic fibrosis.
Oscillatory positive expiratory pressure, high frequency chest wallcompression, and positive expiratory pressure are effectivealternatives to postural drainage, clapping and vibration.
Expiratory muscle training is recommended for patients withneuromuscular weakness and impaired cough to improve peakexpiratory pressure.
Long term outcomes of airway clearance therapy are unknown.
AIRWAY CLEARANCE THERAPY: FINDING THE EVIDENCE
1674 RESPIRATORY CARE • OCTOBER 2013 VOL 58 NO 10

spect to the general needs for airway clearance, as well asfor treatment of individual patients. A summary of thepertinent findings from these guidelines can be found inTable 3.
Putting Evidence Into Practice
The lack of empirical evidence to determine superiorityof any airway-clearance device or technique supports theneed for protocols to guide device/technique selection. Theliterature supports the use of respiratory therapist-drivenprotocols. Studies demonstrate that protocol use improvesappropriate allocation of respiratory services, by reducingover-ordering and under-ordering of respiratory therapies,and the cost of care.61-64 A few studies report that match-ing ACT to clinical need improves patient adherence andreduces missed therapy, especially when the patients areeducated consumers of care and actively engaged in theACT selection process.65-68
An algorithm for guiding ACT was proposed17 but didnot account for an assessment of the patient’s ability toperform therapy, determination of cough characteristics,or frequency of re-evaluation. This algorithm recom-mends to “continue effective therapy” if the patient is a“known responder.”17 However, decline in pulmonaryand/or muscle function can occur during exacerbations orwith time, as a function of the natural progression of thedisease. The rate of decline in muscle and/or pulmonaryfunction can affect treatment efficacy and patient out-comes. Evaluation of the need for ACT and use of a par-ticular device or technique must include initial and on-going assessment of the patient’s lung function, musclestrength, and cognitive ability to perform the therapy.Figure 3 integrates expert opinion,12,17 evidence frompublished systematic reviews,52-54,57,58 and clinical prac-tice guidelines59,60 to construct an algorithm to guide theuse of ACT. The establishment and evaluation of patient,process, and financial outcomes are crucial elements in
Fig. 3. Respiratory therapist driven algorithm to guide airway clearance use. OPEP � oscillatory positive expiratory pressure.
AIRWAY CLEARANCE THERAPY: FINDING THE EVIDENCE
RESPIRATORY CARE • OCTOBER 2013 VOL 58 NO 10 1675
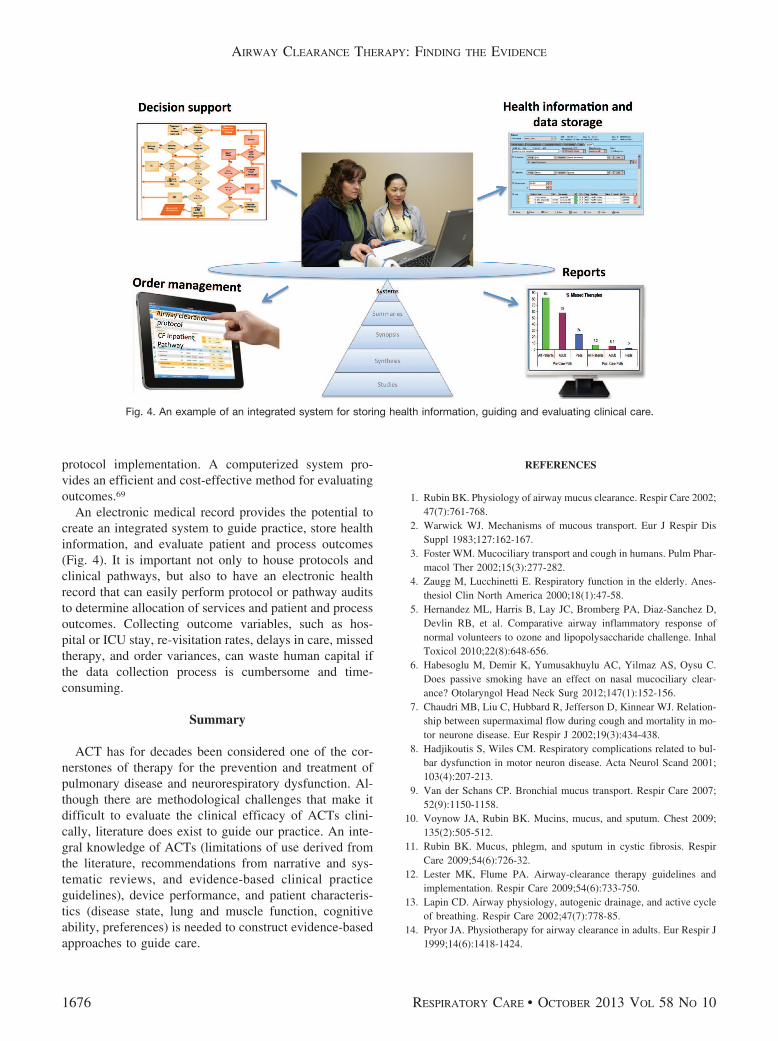
protocol implementation. A computerized system pro-vides an efficient and cost-effective method for evaluatingoutcomes.69
An electronic medical record provides the potential tocreate an integrated system to guide practice, store healthinformation, and evaluate patient and process outcomes(Fig. 4). It is important not only to house protocols andclinical pathways, but also to have an electronic healthrecord that can easily perform protocol or pathway auditsto determine allocation of services and patient and processoutcomes. Collecting outcome variables, such as hos-pital or ICU stay, re-visitation rates, delays in care, missedtherapy, and order variances, can waste human capital ifthe data collection process is cumbersome and time-consuming.
Summary
ACT has for decades been considered one of the cor-nerstones of therapy for the prevention and treatment ofpulmonary disease and neurorespiratory dysfunction. Al-though there are methodological challenges that make itdifficult to evaluate the clinical efficacy of ACTs clini-cally, literature does exist to guide our practice. An inte-gral knowledge of ACTs (limitations of use derived fromthe literature, recommendations from narrative and sys-tematic reviews, and evidence-based clinical practiceguidelines), device performance, and patient characteris-tics (disease state, lung and muscle function, cognitiveability, preferences) is needed to construct evidence-basedapproaches to guide care.
REFERENCES
1. Rubin BK. Physiology of airway mucus clearance. Respir Care 2002;47(7):761-768.
2. Warwick WJ. Mechanisms of mucous transport. Eur J Respir DisSuppl 1983;127:162-167.
3. Foster WM. Mucociliary transport and cough in humans. Pulm Phar-macol Ther 2002;15(3):277-282.
4. Zaugg M, Lucchinetti E. Respiratory function in the elderly. Anes-thesiol Clin North America 2000;18(1):47-58.
5. Hernandez ML, Harris B, Lay JC, Bromberg PA, Diaz-Sanchez D,Devlin RB, et al. Comparative airway inflammatory response ofnormal volunteers to ozone and lipopolysaccharide challenge. InhalToxicol 2010;22(8):648-656.
6. Habesoglu M, Demir K, Yumusakhuylu AC, Yilmaz AS, Oysu C.Does passive smoking have an effect on nasal mucociliary clear-ance? Otolaryngol Head Neck Surg 2012;147(1):152-156.
7. Chaudri MB, Liu C, Hubbard R, Jefferson D, Kinnear WJ. Relation-ship between supermaximal flow during cough and mortality in mo-tor neurone disease. Eur Respir J 2002;19(3):434-438.
8. Hadjikoutis S, Wiles CM. Respiratory complications related to bul-bar dysfunction in motor neuron disease. Acta Neurol Scand 2001;103(4):207-213.
9. Van der Schans CP. Bronchial mucus transport. Respir Care 2007;52(9):1150-1158.
10. Voynow JA, Rubin BK. Mucins, mucus, and sputum. Chest 2009;135(2):505-512.
11. Rubin BK. Mucus, phlegm, and sputum in cystic fibrosis. RespirCare 2009;54(6):726-32.
12. Lester MK, Flume PA. Airway-clearance therapy guidelines andimplementation. Respir Care 2009;54(6):733-750.
13. Lapin CD. Airway physiology, autogenic drainage, and active cycleof breathing. Respir Care 2002;47(7):778-85.
14. Pryor JA. Physiotherapy for airway clearance in adults. Eur Respir J1999;14(6):1418-1424.
Fig. 4. An example of an integrated system for storing health information, guiding and evaluating clinical care.
AIRWAY CLEARANCE THERAPY: FINDING THE EVIDENCE
1676 RESPIRATORY CARE • OCTOBER 2013 VOL 58 NO 10
15. Walsh BK, Hood K, Merritt G. Pediatric airway maintenance andclearance in the acute care setting: how to stay out of trouble. RespirCare 2011;56(9):1424-1440.
16. Myers TR. Positive expiratory pressure and oscillatory positive ex-piratory pressure therapies. Respir Care 2007;52(10):1308-1326.
17. Chatburn RL. High-frequency assisted airway clearance. Respir Care2007;52(9):1224-1235.
18. Gauld LM. Airway clearance in neuromuscular weakness. Dev MedChild Neurol 2009;51(5):350-355.
19. Armengot M, Milara J, Mata M, Carda C, Cortijo J. Cilia motilityand structure in primary and secondary ciliary dyskinesia. Am JRhinol Allergy 2010;24(3):175-180.
20. Carlen B, Stenram U. Primary ciliary dyskinesia: a review. Ultra-struct Pathol 2005;29(3-4):217-220.
21. Santamaria F, Montella S, Tiddens HA, Guidi G, Casotti V,Maglione M, de Jong PA. Structural and functional lung disease inprimary ciliary dyskinesia. Chest 2008;134(2):351-357.
22. Thomas B, Rutman A, Hirst RA, Haldar P, Wardlaw AJ, Bankart J,et al. Ciliary dysfunction and ultrastructural abnormalities are fea-tures of severe asthma. J Allergy Clin Immunol 2010;126(4):722-729.
23. Verra F, Escudier E, Lebargy F, Bernaudin JF, De Cremoux H,Bignon J. Ciliary abnormalities in bronchial epithelium of smokers,ex-smokers, and nonsmokers. Am J Respir Crit Care Med 1995;151(3 Pt 1):630-634.
24. Jeffery PK. Comparative morphology of the airways in asthma andchronic obstructive pulmonary disease. Am J Respir Crit Care Med1994;150(5 Pt 2):S6-S13.
25. Boucher RC. Evidence for airway surface dehydration as the initi-ating event in CF airway disease. J Intern Med 2007;261(1):5-16.
26. Boucher RC. Cystic fibrosis: a disease of vulnerability to airwaysurface dehydration. Trends Mol Med 2007;13(6):231-240.
27. Rubin BK. Mucus structure and properties in cystic fibrosis. PaediatrRespir Rev 2007;8(1):4-7.
28. Belessis Y, Dixon B, Hawkins G, Pereira J, Peat J, MacDonald R,et al. Early cystic fibrosis lung disease detected by bronchoalveolarlavage and lung clearance index. Am J Respir Crit Care Med 2012;185(8):862-873.
29. Regamey N, Tsartsali L, Hilliard TN, Fuchs O, Tan HL, Zhu J, QiuYS, Alton EW, Jeffery PK, Bush A, Davies JC. Distinct patterns ofinflammation in the airway lumen and bronchial mucosa of childrenwith cystic fibrosis. Thorax 2012;67(2):164-170.
30. Rubin BK. The role of mucus in cough research. Lung 2010;188(Suppl1):S69-S72.
31. Zimmer MB, Nantwi K, Goshgarian HG. Effect of spinal cord injuryon the respiratory system: basic research and current clinical treat-ment options. J Spinal Cord Med 2007;30(4):319-330.
32. Brown R, DiMarco AF, Hoit JD, Garshick E. Respiratory dysfunc-tion and management in spinal cord injury. Respir Care 2006;51(8):853-868.
33. Fairclough RJ, Bareja A, Davies KE. Progress in therapy for Du-chenne muscular dystrophy. Exp Physiol 2011;96(11):1101-1113.
34. Chandrasoma B, Balfe D, Naik T, Elsayegh A, Lewis M, Moseni-far Z. Pulmonary function in patients with amyotrophic lateralsclerosis at disease onset. Monaldi Arch Chest Dis 2012;77(3-4):129-133.
35. Beardsmore CS, Wimpress SP, Thomson AH, Patel HR, GoodenoughP, Simpson H. Maximum voluntary cough: an indication of airwayfunction. Bull Eur Physiopathol Respir 1987;23(5):465-472.
36. Chaudri MB, Liu C, Hubbard R, Jefferson D, Kinnear WJ. Relation-ship between supramaximal flow during cough and mortality in mo-tor neurone disease. Eur Respir J 2002;19(3):434-438.
37. Davis PB. Cystic fibrosis since 1938. Am J Respir Crit Care Med2006;173(5):475-482.
38. Sivasothy P, Brown L, Smith IE, Shneerson JM. Effect of manuallyassisted cough and mechanical insufflation on cough flow of normalsubjects, patients with chronic obstructive pulmonary disease(COPD), and patients with respiratory muscle weakness. Thorax2001;56(6):438-444.
39. Perrin C, Unterborn JN, Ambrosio CD, Hill NS. Pulmonary com-plications of chronic neuromuscular diseases and their management.Muscle Nerve 2004;29(1):5-27.
40. Hayes RB. Of studies, syntheses, synopses and systems: the “4S”evolution of services for finding the current best evidence. ACP JClub 2001;134(2):A11-A13.
41. Pattishall EN. Negative clinical trials in cystic fibrosis research.Pediatrics 1990;85(3):277-281.
42. Modi AC, Cassedy AE, Quittner AL, Accurso F, Sontag M, KoenigJM, Ittenbach RF. Trajectories of adherence to airway clearancetherapy for patients with cystic fibrosis. J Pediatr Psychol 2010;35(9):1028-1037.
43. Modi AC, Lim CS, Yu N, Geller D, Wagner MH, Quittner AL. Amulti-method assessment of treatment adherence for children withcystic fibrosis. J Cyst Fibros 2006;5(3):177-185.
44. Arias Llorente RP, Bousono García C, Díaz Martín JJ. Treatmentcompliance in children and adults with cystic fibrosis. J Cyst Fibros2008;7(5):359-367.
45. Bernard RS, Cohen LL. Increasing adherence to cystic fibrosistreatment: a systematic review of behavioral techniques. PediatrPulmonol 2004;37(1):8-16.
46. Kettler LJ, Sawyer SM, Winefield HR, Grenville HW. Determi-nants of adherence in adults with cystic fibrosis. Thorax 2002;57(5):459-464.
47. Grossoehme DH, Opipari-Arrigan L, VanDyke R, Thurmond S, SeidM. Relationship of adherence determinants and parental spiritualityin cystic fibrosis. Pediatr Pulmonol 2012;47(6):558-566.
48. Flores JS, Teixeira FA, Rovedder PM, Ziegler B, Dalcin Pde T.Adherence to airway clearance therapies by adult cystic fibrosispatients. Respir Care 2013;58(2):279-285.
49. Myers LB, Horn SA. Adherence to chest physiotherapy in adultswith cystic fibrosis. J Health Psychol 2006;11(6):915-926.
50. Hess DR. The evidence for secretion clearance techniques. RespirCare 2001;46(11):1276-1293.
51. Cook DJ. Moving toward evidence-based practice. Respir Care 2003;48(9):859-868.
52. McKoy NA, Saldanha IJ, Odelola OA, Robinson KA. Active cycleof breathing technique for cystic fibrosis. Cochrane Database SystRev 2012;(12):CD007862.
53. Elkins MR, Jones A, van der Schans C. Positive expiratory pressurephysiotherapy for airway clearance in people with cystic fibrosis.Cochrane Database Syst Rev 2006;(2):CD003147.
54. Morrison L, Agnew J. Oscillating devices for airway clearance inpeople with cystic fibrosis. Cochrane Database Syst Rev 2009;(1):CD006842.
55. Elkins M, Dentice R. Timing of hypertonic saline inhalation forcystic fibrosis. Cochrane Database Syst Rev 2012;(2):CD008816.
56. Dentice R, Elkins M. Timing of dornase alfa inhalation for cysticfibrosis. Cochrane Database Syst Rev 2011;(5):CD007923.
57. Main E, Prasad A, Schans C. Conventional chest physiotherapycompared to other airway clearance techniques for cystic fibrosis.Cochrane Database Syst Rev 2005;(1):CD002011.
58. Osadnik CR, McDonald CF, Jones AP, Holland AE. Airway clear-ance techniques for chronic obstructive pulmonary disease. CochraneDatabase Syst Rev 2012;(3):CD008328.
59. Cool FD, Rosen MJ. Nonpharmacologic airway clearance therapies:ACCP evidence-based clinical practice guidelines. Chest 2006;129(1 Suppl):250S–259S.
AIRWAY CLEARANCE THERAPY: FINDING THE EVIDENCE
RESPIRATORY CARE • OCTOBER 2013 VOL 58 NO 10 1677

60. Flume PA, Robinson KA, O’Sullivan BP, Finder JD, Vender RL,Willey-Courand DB, et al; Clinical Practice Guidelines for Pulmo-nary Therapies Committee. Cystic fibrosis pulmonary guidelines:airway clearance therapies. Respir Care 2009;54(4):522-537.
61. Kallam A, Meyerink K, Modrykamien AM. Physician-ordered aero-sol therapy versus respiratory therapist-driven aerosol protocol: theeffect on resource utilization. Respir Care 2013;58(3):431-437.
62. Colice GL, Carnathan B, Sung J, Paramore LC. A respiratorytherapist-directed protocol for managing inpatients with asthmaand COPD incorporating a long-acting bronchodilator. J Asthma2005;42(1):29-34.
63. Drescher GS, Carnathan BJ, Imus S, Colice GL. Incorporating tiotro-pium into a respiratory therapist-directed bronchodilator protocol formanaging in-patients with COPD exacerbations decreases broncho-dilator costs. Respir Care 2008;53(12):1678-1684.
64. Kollef MH, Shapiro SD, Clinkscale D, Cracchiolo L, Clayton D,
Wilner R, Hossin L. The effect of respiratory therapist-initiated treat-ment protocols on patient outcomes and resource utilization. Chest2000;117(2):467-475.
65. Shapiro BA, Cane RD, Peterson J, Weber D. Authoritative medicaldirection can assure cost-beneficial bronchial hygiene therapy. Chest1988;93(5):1038-1042.
66. Alexander E, Weingarten S, Mohsenifar Z. Clinical strategies toreduce utilization of chest physiotherapy without compromising pa-tient care. Chest 1996;110(3):430-432.
67. Homnock DN. Making airway clearance successful. Paediatr RespirRev 2007;8(1):40-45.
68. White D, Stiller K, Haensel N. Adherence of adult cystic fibrosispatients with airway clearance and exercise regimens. J Cyst Fibros2007;6(3):163-170.
69. Christman SL, Volsko TA. Evaluation of an oxygen protocol inlong-term care. Respir Care 2006;51(12):1424-1431.
AIRWAY CLEARANCE THERAPY: FINDING THE EVIDENCE
1678 RESPIRATORY CARE • OCTOBER 2013 VOL 58 NO 10


















