

AGENDA - South Eastern Hampshire CCG... · AGENDA 1 Chair's Welcome 3.00 Owner: Chair 2 Apologies...
237
Top South Eastern Hampshire CCG and Fareham & Gosport CCG SEH Governing Body South Eastern Hampshire CCG Governing Body 19 March 2014 - 15:00 the Council Chamber, East Hants District Council, Penns Place, Petersfield, GU31 4EX AGENDA 1 3.00 Chair's Welcome Owner: Chair 2 3.02 Apologies Owner: Chair 3 3.04 Register of Interests and Declarations of Interest Owner: Chair 3 Register of Interests 5 4 3.05 Minutes of the Previous Meeting Owner: Chair 4 Minutes of the Previous Meeting 9 5 3.07 Matters arising from the Minutes Owner: Chair 6 3.10 CCG Chair's Report Owner: Chair 7 3.15 Five Year Strategy and Two Year Operating Plan Update Owner: Dr Barbara Rushton / Sara Tiller 7 Five Year Strategy and Two Year Operating Plan U 16
Transcript of AGENDA - South Eastern Hampshire CCG... · AGENDA 1 Chair's Welcome 3.00 Owner: Chair 2 Apologies...

Top
South�Eastern�Hampshire�CCG�and�Fareham�&�Gosport�CCG
SEH�Governing�Body
South�Eastern�Hampshire�CCG�Governing�Body
19�March�2014�-�15:00
the�Council�Chamber,�East�Hants�District�Council,�Penns�Place,�Petersfield,GU31�4EX
AGENDA
1 3.00Chair's�WelcomeOwner:�Chair
2 3.02ApologiesOwner:�Chair
3 3.04Register�of�Interests�and�Declarations�of�InterestOwner:�Chair
3�Register�of�Interests 5
4 3.05Minutes�of�the�Previous�MeetingOwner:�Chair
4�Minutes�of�the�Previous�Meeting 9
5 3.07Matters�arising�from�the�MinutesOwner:�Chair
6 3.10CCG�Chair's�ReportOwner:�Chair
7 3.15Five�Year�Strategy�and�Two�Year�Operating�Plan�UpdateOwner:�Dr�Barbara�Rushton�/�Sara�Tiller
7�Five�Year�Strategy�and�Two�Year�Operating�Plan�U 16

Top
8 3.25Draft�Financial�Plans�2014/15�-�2018/19Owner:�Andrew�Wood
8�Draft�Financial�Plans 92
9 3.35Better�Care�FundOwner:�Alex�Berry
9�Better�Care�Fund 103
10 3.40Finance�ReportOwner:�Andrew�Wood
10�Finance�Report 112
11 3.50Performance�ReportOwner:�Andrew�Wood
11�Performance�Report 120
12 4.00Joint�CCG�Quality�ReportOwner:�Dr�Roddy�Bowerman�/�Julia�Barton
12�Joint�CCG�Quality�Report 142
13 4.10Commissioning�UpdateOwner:�Alex�Berry
13�Commissioning�Update 157
14 4.20Chase�Project�UpdateOwner:�Andrew�Wood
14�Chase�Project�Update 160
15 4.30Board�Assurance�FrameworkOwner:�Sara�Tiller
15�Board�Assurance�Framework 166
16 4.40Engagement�UpdateOwner:�Tracey�Faraday-Drake
16�Engagement�Report 181
17 4.50Public�Health�UpdateOwner:�Dr�Ruth�Milton
17�Public�Health�Update 184

Top
18 4.55Minutes/Notes�from�other�MeetingsOwner:�Chair
18�Minutes�Notes�of�Other�Meetings 186
19 5.00Date�of�next�Scheduled�MeetingOwner:�Chair
Date:��Wednesday�21�May�2014�Time:��9.00�am�Venue:��Education�Room,�Chase�Hospital,�CondeWay,�Bordon,�Hants,�GU35�0YZ
Attendees

Top
Index3�Register�of�Interests.pdf.........................................................................................................5
4�Minutes�of�the�Previous�Meeting.pdf......................................................................................9
7�Five�Year�Strategy�and�Two�Year�Operating�Plan�Update.pdf............................................ 16
8�Draft�Financial�Plans.pdf......................................................................................................92
9�Better�Care�Fund.pdf......................................................................................................... 103
10�Finance�Report.pdf.......................................................................................................... 112
11�Performance�Report.pdf.................................................................................................. 120
12�Joint�CCG�Quality�Report.pdf.......................................................................................... 142
13�Commissioning�Update.pdf..............................................................................................157
14�Chase�Project�Update.pdf................................................................................................160
15�Board�Assurance�Framework.pdf.................................................................................... 166
16�Engagement�Report.pdf...................................................................................................181
17�Public�Health�Update.pdf................................................................................................. 184
18�Minutes�Notes�of�Other�Meetings.pdf.............................................................................. 186

GOVERNING BODY Date of Meeting 19 March 2014
Agenda Item No
3 Title
Register of Interests and Declarations of Interest
Purpose of Paper
This paper sets out the relevant and material interests of the members of the CCG Governing Body. This paper supports the CCG Governing Body in fulfilling its duties in accordance with the NHS Code of Accountability.
Recommendations/ Actions requested
The Governing Body is asked to: • Receive and note the Register of Interests of Members • Receive any oral updates on the interests of Members • Declare any interests relating to any item on the agenda
Author
Sandra Jenkinson Committee Support Officer
Sponsoring member
Dr Barbara Rushton CCG Chair
Date
12 March 2014
3�Register�of�Interests.pdf
Top
Overall�Page�5�of�237Page�1�of�4

Governing Body
Register of Interests Name Role Declarations
VOTING MEMBERS Dr Jenny Allinson
CCG Unscheduled Care and Mental Health Lead
Carrying out consultancy work for United Health Group
Julia Barton Chief Quality Officer (Registered Nurse)
Governor, Portsmouth Hospitals NHS Trust
Dr Alastair Bateman
CCG Prescribing Lead GPwSI Cardiology working for Grange Surgery Community Cardiology Clinic
Hospital Practitioner in Cardiology at St Richards Hospital, Chichester
GP Principal at Stakes Lodge Surgery
Stakes Lodge Surgery is a member of South East Hampshire GP Alliance
GP Trainer
Works in Out of Hours service for Care UK
Dr Roddy Bowerman
CCG Quality and Governance Lead
Partner in practice that provides GOS 18 Services Works in Out of Hours service
Dr Andrew Douglas CCG Planned Care Lead
Partner in a practice that has an SPMS contract with NHS Hants for the Community Cardiology Clinic
Tracey Faraday-Drake
Lay Member (Chair of Community Engagement Committee)
Owner of Drakes Consulting, a company that provides mediation, management consultancy and executive coaching
Susanne Hasselmann
Lay Member (Joint Chair of Audit Committee)
Director and shareholder of IP Events Ltd.
Director and owner of Scirum Ltd.
Works as a management consultant in brand protection. Is a non-voting member of the ACG Council and Chair of ACG’s Brand Protection Group.
Parish Councillor in Wherwell Parish.
Ambassador for Diversity in Public
Last update: 8 January 2014
3�Register�of�Interests.pdf
Top
Overall�Page�6�of�237Page�2�of�4

Name Role Declarations Appointments.
Husband is Director System Delivery NHS Southampton City Clinical Commissioning Group
Dr Andrew Holden CCG Practice Performance Lead
GP principal at Swan Surgery, Petersfield
Local Medical Committee – Representative for Hants and IOW LMC
Supporter of Friends of Petersfield Hospital
Swan Surgery is a member of South East Hampshire GP Alliance (providing cover to the Chase Community Hospital)
Adel Resouly Secondary Care Doctor Representative
Sits on War Pensions Tribunals and Industrial Injuries Board
Dr Barbara Rushton
Chair and CCG Strategic Development Lead
PCT appointed Governor RSCH
Practice is a member of the East Hants Alliance (providing cover to the Chase Community Hospital)
Practice is in Circle Partnership
Husband is Finance Director for KPMG
Richard Samuel
Chief Officer (Accountable Officer)
Wife works as an accountant for the Royal Bournemouth and Christchurch Hospitals NHS Trust
Trustee of an HIV/AIDs charity in Bournemouth
Father-in-law is a NED at Poole Hospitals NHS Trust
Step father elected as Hampshire County Councillor for South Waterside ward, Eastleigh
Andrew Wood Chief Finance Officer No interests to be declared
NON-VOTING MEMBERS
Alex Berry Chief Commissioning Officer
No interests to be declared
Ruth Dixon
Deputy Director, Adult Services, Hampshire County Council
No interests to be declared
Jo Hockley Chair, Practice Managers Commissioning Advisory Group
No interests to be declared
Dr Ruth Milton Director of Public Health, Hampshire County Council
No interests to be declared
Last update: 8 January 2014
3�Register�of�Interests.pdf
Top
Overall�Page�7�of�237Page�3�of�4

Name Role Declarations Andrew Mostyn LMC Representative No interests to be declared
Sara Tiller Chief Development Officer
No interests to be declared
CO-OPTED MEMBERS
Cllr Jackie Branson Havant Borough Council Representative
No interests to be declared
Cllr Robert Saunders
East Hampshire District Council representative
No interests to be declared
To note: Richard Samuel, Andrew Wood, Julia Barton and Sara Tiller work across Fareham and Gosport CCG and South Eastern Hampshire CCG. Alex Berry’s role covers Portsmouth CCG, Fareham and Gosport CCG and South Eastern Hampshire CCG.
Last update: 8 January 2014
3�Register�of�Interests.pdf
Top
Overall�Page�8�of�237Page�4�of�4
GOVERNING BODY Date of Meeting 19 March 2014
Agenda Item No
4 Title
Minutes of the Previous Meeting Purpose of Paper
The Minutes of the meeting held on 22 January 2014 are presented for consideration by the Governing Body.
Recommendations/ Actions requested
The Governing Body is asked to: • Approve the Minutes of the meeting held on 22 January 2014,
subject to any amendments which will be recorded in the Minutes of this meeting.
Author
Nikki Roberts Governance and Committee Officer
Sponsoring member
Barbara Rushton CCG Chair
Date
12 March 2014
4�Minutes�of�the�Previous�Meet
Top
Overall�Page�9�of�237Page�1�of�7

Minutes of the meeting of the South Eastern Hampshire Clinical Commissioning Group (SEH CCG) Governing Body held on Wednesday 22nd January 2014 at 3.00pm
in the Hurstwood Room, Havant Civic Centre, Public Service Plaza, Civic Centre Road, Havant, PO9 2AX.
Present: Dr Barbara Rushton Dr Roddy Bowerman Dr Alastair Bateman Dr Andrew Holden Dr Andrew Douglas Susanne Hasselmann Julia Barton Adel Resouly Richard Samuel Andrew Wood
Chair & Strategic Development Lead Quality and Safety Lead Prescribing Lead Practice Performance Lead Planned Care Lead Lay Member Registered Nurse Practitioner & Chief Quality Officer Secondary Care Doctor Chief Officer Chief Finance Officer
In Attendance: Alex Berry Ruth Dixon Jo Hockley Dr Ruth Milton Cllr Jackie Branson Cllr Robert Saunders Nikki Roberts
Chief Commissioning Officer Deputy Director, Adult Services, Hampshire County Council Chair, Practice Managers Commissioning Advisory Group Director of Public Health, Hampshire County Counc Havant Borough Council East Hampshire District Council Governance and Committee Officer
Pippa Cook Service Manager for Paediatric Therapies at Solent NHS Trust
84/12 Chair’s Welcome
The Chair welcomed everyone to the meeting, including Cllr Jackie Branson and Cllr
Roberts Saunders, and reminded all present that this was a meeting held in public, and not a public meeting.
85/12 Apologies
Apologies were received from Sara Tiller, Dr Jenny Allinson and Tracey Faraday-Drake.
86/12 Register of Interests and Declarations of Interest
The register of interests was presented. Dr Andrew Holden declared a declaration of interest for item 14 – Locally Commissioned Services - Recommendations. The Governing Body agreed:
1
4�Minutes�of�the�Previous�Meet
Top
Overall�Page�10�of�237Page�2�of�7

a. To note the Register of Interests b. To note that there were no amendments to the Register of Interests
87/12 Minutes of the previous meeting
The Governing Body agreed to approve the minutes of the previous meeting held on 20th November 2013. There were no amendments.
88/12 Matters arising from the Minutes
There were no Matters Arising.
89/12 CCG Chair’s Report
Dr Barbara Rushton presented the Chair’s Report, reporting on the outcomes of the recent Governing Body away day, the forthcoming submission of the CCG’s strategic plans, the concerns regarding the performance of Portsmouth Hospitals NHS Trust, and the leaflet regarding the sharing of patient information between providers. The Governing Body agreed to accept the Chair’s Report.
90/12 Paediatric Therapies Presentation
Pippa Cook, Service Manager for Paediatric Therapies at Solent NHS Trust gave a presentation regarding the new Paediatric Therapies Service that has been commissioned by the CCG. The presentation covered the tendering process and the new service provisions. The aim of the new service will be to provide a more streamlined service that will enable the three therapy areas, (speech and language therapy, occupational therapy and physiotherapy), to work jointly with one administrative team coordinating nine locality teams. The locality teams do not mirror the CCG or council geographical areas. The administrative team, which will be the point of access for the service, will be at Moorgreen Hospital Site, Botley Road, West End, Southampton. The service will be provided to any child aged 0-19 and will work closely with Social Services, particularly when transferring children to Adult Services. The service will be accessed subject to a set of guidelines, rather than strict criteria as the threshold. Waiting times are to be reduced, and the team are considering ways to achieve this reduction, including a revision to the size of the reports that are to be produced. The Governing Body agreed to accept the Paediatric Therapies Presentation.
91/12 Finance Report
The Finance Report for month nine was presented by Andrew Wood. It was reported that the CCG is currently on plan to meet its target surplus of £0.6m with a year to date surplus of £0.5m. The financial position of Portsmouth Hospitals NHS Trust was produced using extrapolation of month eight activity data, which has shown a considerable increase in elective inpatients and outpatients. A full year outturn of £84.3m is the current understanding of the likely year end position. Prescribing charges attributable to the Local Area Team and Local Authority public health services have increased significantly, which is in line with expectations of the service provisional. Income is due from both organisations to offset these costs,
2
4�Minutes�of�the�Previous�Meet
Top
Overall�Page�11�of�237Page�3�of�7

following the new commissioning responsibilities, however final agreement on the total income due is still to be reached. The QIPP target of £9m still presents a significant challenge to the CCG achieving its surplus target. It is anticipated that any shortfall in QIPP would be covered by the contingency. It was noted that the contingency covers the forecasted shortfall and the QIPP shortfall. The Governing Body members also noted that the QIPP had generated a large volume of positive work, however, any benefits had been offset by the overperformance of Portsmouth Hospital NHS Trust. It is believed that problems may lie in coding, therefore an audit on coding at Portsmouth Hospitals NHS Trust is being taken forward. The Governing Body accepted the Finance Report for month nine.
92/12 Performance Report
The performance report was presented by Michael Drake. Key achievements included that 95.3% of RTT non-admitted patients were seen within 18 weeks, achieving the target of 95%, and the target of 92% for RTT incomplete patients was achieved with 94.7% seen within 18 weeks. However, 79.1% of RTT admitted patients were seen within 18 weeks against the target of 90%. An RTT contract query notice was issued on 23rd December 2013 which requested the projected RTT targets. Additional key achievements included that there were no referred patients waiting over 52 weeks for treatment, and diagnostic waits within six weeks achieved the target of 99% with 99.4% of patients seen within the timescale. There were no patients treated in mixed sex accommodation and there were no reported cases of MRSA and two reported cases of C.Difficile against a monthly trajectory of three. Key areas of underperformance are that the percentage of cancer patients seen more than 14 days after urgent GP referrals is at 92% against a target of 93%. The percentage of cancer patients receiving subsequent surgery within 31 days was at 80%, and 75% of cancer patients were treated after screening referral within 62 days against the target of 90%. The variance in the figures for contracting against Fareham and Gosport, South Eastern Hampshire and Portsmouth CCG was discussed, and it was noted that the differential existed due to a higher number of elective referrals and lower number of non-elective procedures for Fareham and Gosport and South Eastern Hampshire CCG. This was being monitored. The Governing Body accepted the contents of the Performance Report.
93/12 Planning Update
Michael Drake presented a verbal update on the CCG planning processes and progress made. It was reported that the first deadline for submission was the 14th February 2014 for the first draft of the two year operating plan. Michael Drake requested that due to the short timescales the first draft submission of the two year operating plan be approved by Chair’s Action as, although it was a concern, the Governing Body will be unable to meet and approve the plan prior to the submission date. It was noted that the operating plan is a technical framework that allows for little autonomy, and it is the strategy which will allow the opportunity to shape and frame the Governing Body’s intentions.
3
4�Minutes�of�the�Previous�Meet
Top
Overall�Page�12�of�237Page�4�of�7

The Governing Body approved that the two year strategic plan be approved by Chair’s action prior to submission to NHS England on 14th February 2014.
94/12 Quality Report
Julia Barton presented the Quality Report, noting the proceedings of the CCG Joint
Quality and Safety Committee and exception reports from Portsmouth Hospitals NHS Trust, South Central Ambulance Service NHS Foundation Trust, Solent NHS Trust, Sussex Partnerships child and Adolescent Mental Health Services, Royal Surrey County Hospital NHS Foundation Trust, CCG enquiries, concerns and complaints and serious incidents requiring investigation. It was noted that one SIRI and never event had occurred on 21st January 2014. The work and distinction of business between the Quality Operational Forum and the Quality Assurance Committee was discussed. Also, that the issues currently experienced by Portsmouth Hospitals NHS Trust were beginning to have an effect on the quality of services, and the CCG will be meeting with Portsmouth Hospitals NHS Trust and the Trust Development Agency to discuss the problems that exist. The report was fully discussed by Governing Body members. It was noted that a new risk had been identified which was the low scoring on the Friends and Family Test at Portsmouth Hospitals NHS Trust. This was being addressed and any actions are being monitored by the CCG Quality Team. The Governing Body agreed to note the Joint Quality and Safety Report.
95/12 Hampshire Safeguarding Children Board Annual Report
Julia Barton presented the Hampshire Safeguarding Children Board Annual Report. It was noted that CCGs have a key role in scrutinising the governance and planning of safeguarding children across a range of organisations and are to ensure that services are commissioned for the most vulnerable children. The Governing Body noted the Hampshire Safeguarding Children Annual Report.
96/12 Commissioning Summary
Alex Berry presented the Commissioning Summary. Highlights included an update on the re-tendering of the Wheelchair Service, and an update on the tendering process of the specialist musculoskeletal and persistent pain procurement service. Also discussed was the referral to treatments times regarding cancer and details of the remedial action plan that was in place, the Urgent Care Centre, the impact it was having on the Emergency Department at Queen Alexandra’s Hospital, and ambulatory care. The issue of which committee or board has the authority to take commissioning decisions was discussed and it was noted that this was being addressed in a governance review which includes an update to the scheme of delegation. The principle currently in place is that when a new service is designed, the Clinical Cabinet is the arbiter of patient’s views and advice from lay members. The Clinical Cabinet will then take the decision to approve the strategy or to forward it to the Governing Body where any decision would be contentious.
4
4�Minutes�of�the�Previous�Meet
Top
Overall�Page�13�of�237Page�5�of�7

The Governing Body agreed to note the Commissioning Update.
97/12 Locally Commissioned Services - Recommendations
Keeley Ormsby and Dr Andrew Holden presented the Enhanced Services Recommendations paper. For this item, a declaration of interest was declared by Dr Andrew Holden. Each area was discussed and Governing Body members had an opportunity to comment on each decision. It was noted that the contracts would be for one year, therefore the contracts would be reconsidered and presented for approval at the Governing Body in one year’s time. Dr Andrew Holden presented the detail of each individual contract. The impact on member practices was discussed, and the details of the phlebotomy contract was also considered. It was also noted that the LMC are supportive of the revisions made to Locally Commissioned Services. Governing Body members commented that more work was required to further define the Nursing Homes LCS. The Governing Body agreed to:
a. Approve the recommendations for each scheme, b. Defer scrutiny of finances regarding the Nursing Home LCS c. Note the use of the NHS Standard Contract for all locally commissioned
services in 2014/15. d. Approve the delegated authority to the Governing Body Lay Members to
do a more detailed scrutiny of each scheme if required. e. Approve that a quarterly update be brought to the join Clinical Cabinet to
report the progress and outcomes. f. Meet with each practice affected to discuss the removal of finance`s for
locally commissioned services.
98/12 Chase Update
Andrew Wood presented an update regarding the Chase Community Hospital Redevelopment project, which had been provided by Sara Tiller. It was noted that the CCG was working closely with NHS Business Services to enable the business case to be brought before the Governing Body in due course. The Governing Body agreed to note the progress.
99/12 Board Assurance Framework
Richard Samuel presented the top five risks, of which a number had already been discussed during the meeting. In sum, 15 risks were updated, one risk had a reduction in risk score and there was one new risk which related to the low scores of the Friends and Family test at Portsmouth Hospitals NHS Trust. The Governing Body agreed to approve the recommendations contained within the update to the Board Assurance Framework.
100/12 Corporate Diary 2014/15
The diary dates for the governing body meetings during 2014/15 were presented by Richard Samuel on behalf of Sara Tiller. It was noted that dates for May, July and October fell during the school half term holidays, therefore the meetings for May and October will be moved to the week before and held in the mornings.
5
4�Minutes�of�the�Previous�Meet
Top
Overall�Page�14�of�237Page�6�of�7

The Governing Body approved the Corporate Diary dates for 2014/15.
101/12 Governance Committee Establishment
Richard Samuel presented the paper requesting the establishment of a Corporate Governance Committee on behalf of Sara Tiller. It was noted that Lay Members would not be required to attend this committee as the focus was operational rather than assurance based, however, Lay Members may be invited on occasions where an independent overview was required. The minutes and summary of actions of the Governance Committee will be presented at the Audit Committee. The Governing Body agreed to note the report and recommendations.
102/12 Engagement Update
Richard Samuel presented the Engagement Update on behalf of Sara Tiller. The Governing Body agreed to note the Engagement Update.
103/12 Minutes from other meetings
The Governing Body agreed to note the minutes of other meetings • Hampshire Commissioning Group – 16 October 2013 • Clinical Cabinet – 23 October 2013 • Community Engagement Committee – 4 December 2013
104/12 Date of next scheduled meeting
Wednesday 19th March 2014 at 3.00 pm.
Venue – Council Chamber, East Hampshire District Council, Penns Place, Petersfield, GU31 4EX.
6
4�Minutes�of�the�Previous�Meet
Top
Overall�Page�15�of�237Page�7�of�7

GOVERNING BODY Date of Meeting 19th March 2014
Agenda Item No
7 Title
Five year strategy and Two year operating plan update
Purpose of Paper
To provide members of the Governing Body with an update on the development of the CCG’s Five Year Strategy and two Year Operating Plan.
Recommendations/ Actions requested
The Governing Body is asked to:
• note the progress to date • agree to review and comment on the draft documents
between March 21 and March 26. • agree for Chair’s action to sign off final submissions by
April 4
Author
Sara Tiller Chief Development Officer
Sponsoring member
Richard Samuel Accountable Officer
Date
19th March 2014
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�16�of�237Page�1�of�76

Five year strategy and two year operating plan update
1. BACKGROUND 1.1 On December 20th 2013 NHS England published Everyone Counts, Planning for Patients
2014/15 to 2018/19. This document set out the planning requirements and timetable for development of CCGs’ Five Year Strategic Plans and Two year operating Plans.
1.2 Everyone Counts is designed to ensure that NHS organisations work to deliver the five outcomes described in the NHS Outcomes Framework: • prevent people from dying prematurely, with an increase in life expectancy for all
sections of society. • ensure that those people with long-term conditions including those with mental illnesses
get the best possible quality of life. • ensure patients are able to recover quickly and successfully from episodes of ill-health or
following an injury. • ensure patients have a great experience of all their care. • ensure that patients in our care are kept safe and protected from all avoidable harm.
1.3 It defines seven specific ambitions which CCG Strategies and plans must contain: • Securing additional years of life for people with treatable physical and mental health
conditions • Improving the quality of life for people with long-term conditions • Reducing the amount of time people spend avoidably in hospital through better and
more integrated care in the community, outside of hospital • Increasing the proportion of older people living independently at home following
discharge from hospital • Increasing the number of people with mental and physical health conditions who have a
positive experience of hospital care • Increasing the number of people with mental and physical health conditions who have a
positive experience of care outside of hospital • Making progress towards eliminating avoidable deaths in our hospitals
1.4 Additionally there are three more measures which must be covered:
• improving health, which must have just as much focus as treating illness • reducing health inequalities. We need to ensure that the most vulnerable in our society
get better care and better services • committing to move towards parity of esteem, making sure that we are just as focused
on improving mental as physical health.
1.5 The Guidance is also clear that any high quality, sustainable health and care system in England will have the following six characteristics in five years: • a new approach to ensuring that citizens are fully included in all aspects of service
design • wider primary care • a modern model of integrated care • access to the highest quality urgent and emergency care • a step change in the productivity of elective care
1
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�17�of�237Page�2�of�76

• specialised services concentrated in centres of excellence
1.5 The timetable for Strategy and Operating Plans to NHS England is as follows: 14 February 2014 First submission of draft Plans and Strategies to NHS England 31 March 2014 Plans approved by Governing Body 4 April 2014 Final Operating Plan and Draft Strategy submitted to NHS England 20 June 2014 Final 5 Year Strategy submitted to NHS England
2. DEVELOPMENT OF STRATEGY AND PLANS
2.1 The CCGs were required to inform NHS England if they intended to aggregate their plans into wider ‘units of planning’ to ensure alignment across health systems and maximise the use of resources. Fareham and Gosport CCG agreed to submit a joint Strategy and Operating Plan with South Eastern Hampshire CCG.
2.2 During December, January and February both CCGs conducted a series of engagement events to test the views of local people, stakeholders and member practices regarding the priorities for the years ahead. This included a dedicated session for Governing Body members on December 18, 2013. See Appendix A for the full programme of activities.
2.3 Feedback from these events is summarised at Appendix B.
2.4 In the development the Operating Plan the CCGs have undertaken a detailed analysis of all the data available from a number of national toolkits and local sources: • CCGs Outcomes tool which provided detailed analysis of NHS outcomes and other
relevant indicators at a CCG level • Level of Ambitions Atlas to identify opportunities for improvement when benchmarked
against other CCGs and to support the development of our own levels of ambition. • Commissioning for Value packs and atlas to identify where to look as a first stage to
identify real opportunities to improve outcomes and increase value for the local populations.
• Programme budgeting benchmarking tool to identify spending opportunities • Spend and Outcome Tools to compare spend and outcomes against each other to
identify opportunities • Health outcome framework to identify outcomes that can potentially be improved • Joint Strategic Needs Assessment • Public Health outcomes framework to identify outcomes that can potentially be
improved
2.5 In addition to utilizing these tools a detailed analysis and deep dive review of the elective and non-elective opportunities identified in the Commissioning for Value packs has been undertaken. The analysis included using the most recent data available to identify if the opportunities indicated in the national commissioning for value packs still existed and/or if new opportunities could be identified. The level of analysis was undertaken at HRG and HRG subchapter level.
2.6 The first cut planning submission was made on February 14 as required. This submission consisted of: • Operational Plan templates • Financial Plan templates • Activity Plan templates • Plan on a Page
2
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�18�of�237Page�3�of�76

• Strategy Key Lines of Enquiry • Draft strategy narrative • Self-certification checklist • Better Care Fund
2.7 The operating plan templates consisted of three main areas. Each of these incorporated a significant level of detail as set out below.
2.8 The draft Strategy and Operating Plan were circulated to Governing Body members on February 12, 2014 for comment prior to submission on February 14, 2014.Subsequently Governing Body members have reviewed and commented in detail on the drafts (attached on Boardpacks) at an informal meeting of the Governing Body on February 19, 2014.
3. NEXT STEPS
3.1 Work is now underway to refine both the Strategy document and the Operating Plan ready for the next submission on April 4. This includes incorporating feedback on both drafts from NHS England’s Area Team received on February 25, 2014.
3.2 The key areas of work will incorporate the following: • Ensure ongoing alignment between strategy and operating plan • Ensure that all local and national planning requirements are captured in programme
level strategies and underpinning project plans • Need to have main focus on the ‘how’ between now and final submission dates • Imperative that we have bottom-up plans that clearly articulate ‘how’ we are going to
deliver the transformational change required to deliver the CCG’s strategic vision and objectives
• Further work on outcome trajectories to ensure they are challenging enough to drive us to where we need to get to and that they align with the wider planning agenda eg. BCF
• Update of activity and finance templates will be required following the agreement of contracts to take into account agreed levels of elective activity, QIPP, RRM etc
3
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�19�of�237Page�4�of�76

• Further triangulation across activity, finance submissions re: alignment – including checking with main provider submissions and BCF
3.3 An outline timetable for this work is as follows:
NHS England feedback received by 28 Feb Execs to review existing sections and provide comments back by
28 Feb
Existing comments from GB members/Gov Body seminar and public health to be included by
28 Feb
Strategic alignment event with all local providers/commissioners
28 Feb
Phase 2 engagement programme to commence (see separate engagement plan)
31 March to 18 April
Strategy discussion at F&G Community Engagement Committee
4 March
Strategy update at F&G Governing Body 12 March All new copy to be returned by 14 March Editing and developing final draft 17 March to 21
March Strategy update at SEH Governing Body 19 March Exec meeting to review final draft 21 March Document circulated to GBs for comment 21 March GB members to comment by 26 March Comments incorporated and final edits undertaken 27 March to
April 2 Strategy discussion at SEH Community Engagement Committee
April 2
Submission to Area Team April 4
4 DECISION REQUIRED
4.1The Governing Body is asked to: • note the progress to date; • agree to review and comment on the draft documents between March 21 and
March 26; and • agree for Chair’s action to sign off final submissions by April 4.
4
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�20�of�237Page�5�of�76

Key themes from Call to Action engagement The CCGs ran a three month programme of engagement on Call to Action and the CCGs Five Year Strategy from November 2013 to February 2014. This programme sought the views from local residents, the CCGs Governing Bodies, our member GP practices and key stakeholders. Overarching themes The overarching themes from the feedback received during the programme are:
• Preventing ill health and long term conditions through screening, education and raising awareness, including working with local schools
• Involving local people, including young people and children, and those that represent them, in the development of services through continued and improved engagement and communication
• Empowering and encouraging individuals to take control of their own health through healthy community programmes, education and raising awareness
• Working with GP practices to improve access, including providing alternatives such as telephone consultations and seven day working, whilst ensuring they maintain quality
• Improving access to secondary care services including introducing 24 hour, seven day working
• Developing integrated services with partners in social care, the voluntary sector, education, housing and employment
• Developing close working relationships with the voluntary sector to both seek their views when developing services and to support them as providers
• Focusing on quality to raise and then maintain standards • Working with the acute hospital to reduce waiting times and ensure services understand
and meet the needs of individual patients • Reducing the number of inappropriate attendances at the Emergency Department and
inappropriate admissions, including improving the Out of Hours Service • Developing more specialist services in the local community, such as cardiology and
rheumatology • Providing more support for those with long term conditions, such as dementia,
rheumatology, pain management and mental health conditions • Improving communication and partnership between the different services who are caring
for the same patient so they provide care as a package rather than isolated interventions • Improving the administration support and its efficiency • Providing signposting of local services to GPs and local people so they don’t go to the
acute hospital when there is a local alternative • Improve the consistency of who treats an individual so they see the same person each
time • Developing more services that are closer to home • Developing an effective management structure with the right professionals taking
accountability, working efficiently and effectively, and developing open policies • Developing and increasing the use of IT and communications solutions to support
integration and communication between departments and organisations • Involving and listening to the views of healthcare professionals when developing services • Improving the quality and analysis of data available • Tackling the difficulties of recruiting GPs to current vacancies • Ensuring NHS England’s area teams work effectively with CCGs to commission the right
primary care services
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�21�of�237Page�6�of�76

Themes by group Themes from local residents We asked local residents for their views on Call to Action and the CCGs five year strategy by:
• Holding a public seminar before two of the Governing Body meetings (one for each CCG) and handing out the survey
• Having dedicated Call to Action pages on each CCGs website including an online survey • Promoting the online survey through press releases, CCG stakeholder newsletters,
partner newsletters and a Twitter schedule • Attending public events and groups we were invited to such as Fareham Community
Hospital Open day and handing out the survey • Sharing the information with our Community Engagement Committees so they could
share it with their networks (such as Patient Participation Groups and voluntary groups) Themes from the feedback received from events The themes from the discussions held at the events are:
• Developing closer working relationships with the voluntary sector in both involving them in the development of services and supporting them as providers, for example helping with funding applications where possible
• Developing prevention programmes • Continuing to develop and enhance how local people, including young people and
children, are engaged and communicated with so their views as used in the decision making process
• Improving public transport to Queen Alexandra Hospital at the weekends • Reducing waiting times for routine follow up appointments at the Ophthalmology
Department • Providing Saturday appointments at both hospitals and GP surgeries • Ensuring individual patient needs are met when staying at the hospital • Telephone consultations at GP surgeries are a good alternative but could be improved • Decreasing the number of people who go to the Emergency Department inappropriately
and increase public awareness of NHS 111 • Supporting the development of services being available 24/7, including Primary Care
services • Closer working with key stakeholders including local politicians • Prioritising cardiology and early detection of hypertension
Themes from the survey results 71 local residents completed the survey and were asked five questions and the themes for each of these are (the numbers in brackets show how many people made a comment relating to that theme): 1. What is most important to you and your family in terms of healthcare and why?
68 respondents answered this question with the following themes:
• Quick access to a range of local services (49) • Caring and considerate health professionals who communicate with each other (7) • Patient and carer education to promote and support self-care (6) • The quality of services (5) • Health prevention (3) • Continuity of care by health professionals (2)
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�22�of�237Page�7�of�76

• Access to local services seven days a week (2) • Access to rheumatology services for treatment and support (2) • Increasing the support available to those with dementia and their families (2) • Reducing the delays and improving access at the Emergency Department and Out of
Hours Service (2) • Clean and efficient hospitals (1) • Accessible long term support (1) • Support to help older people stay healthy (1) • Clear signposting of where to go when (1) • Support that helps avoid hospital admissions (1) • Access to a second opinion (1) • Access to family counselling (1)
2. Do you think our priorities are right?
64 respondents answered this questions with 45% saying are current priorities are right; 27% saying they are not and 28% saying they did not know. Themes from the additional comments are:
• Prevention, such as reducing obesity and smoking should be a key priority (4) • Increase the support for those with long term conditions such as dementia and
rheumatology (3) • Increasing partnership working with local authorities and the voluntary sector (2) • Access to local GPs needs to be improved (2) • They are too broad in terms of what they cover and the segments of the population
they are aimed at (2) • More care and understanding of older people is needed (1) • The investment in hospitals should be increased (1) • Allow enough time to implement the changes needed to meet the priorities should be
allowed so these can then be monitored and reviewed (1) • Local facilities need to be utilised as efficiently as possible (1) • Increasing healthcare in local areas with deprivation (1) • Increase the support available for those with mental health conditions (1) • Lack of funding makes it difficult to prioritise (1)
3. What do you think we could change or do differently?
64 respondents answered this question with the following themes:
• Improve access to GPs, including being open seven days a week (12) • Provide more prevention services (such as screening), education and self-care
information (7) • Improve communication and partnership working between the different services who
are caring for a patient and different NHS organisations (5) • Improve partnership working with councils on social care, housing and education (4) • Improve the administration support and its efficiency to free up healthcare
professionals (3) • Listen to the feedback given to you and involve service users in developing service
specifications (3) • Provide access to services and treatment as quickly as possible so conditions don’t
get worse (3) • Improve the Out of Hours Service (3) • Focus on quality and raising standards (2)
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�23�of�237Page�8�of�76

• Promote the local services available to GPs so they don’t send you to the acute hospital when there is an alternative closer to home (2)
• Improve the consistency of who treats you (2) • Provide quicker test results (2) • Provide more local services (2) • Provide wider access to Pain Management services (2) • Have more local hospitals with A&E / Walk In facilities (2) • Increase the number of nurses on hospital wards (1) • Have patient participation groups and provide training so members can contribute
effectively (1) • Increase innovation (1) • Re-negotiate the PFI contract (1) • Reduce the layers of management (1) • Local services are very good (1) • Provide greater clarity on the cost of different services to help develop pathways so
patients are seen at the most appropriate place (1) • Improve access to specialist services (1) • Improve the road signage to Fareham Community Hospital (1) • Improve access to rheumatology services (1) • Charge those who go to the Emergency Department in appropriately (1) • Only allow GP or paramedic referrals to be seen at the Emergency Department (1) • Focus on local issues (1) • Improve how older patients are spoken to (1) • Given the limited budget and availability of services be open to help manage public
expectation (1) • Provide consultant based services in community settings (1) • Provide free prescriptions for everyone (1) • Have a database of vulnerable patients and regularly check they are alright (1) • Plan for the inevitable aging population now (1)
4. What do you think we could do now that would help us make changes more quickly?
63 respondents answered this question with the following themes:
• Involve and listen to the views of patients and the voluntary sector by having clear plans they can comment on / be involved with (11)
• Increase GP accessibility including Out of Hours and seven day working (11) • Have a management structure with the right professionals taking accountability,
working efficiently and effectively, and developing open policies (6) • Increase the use of IT and communications solutions to support integration and
communication between departments and organisations (5) • Increase the number of nurses and hospital staff (4) • Involve and fund voluntary organisations and evaluate their effectiveness (3) • Publicising full information to patients about the services available so they can choose
appropriately (3) • Listen to the views of healthcare professionals, including those in other health
systems (2) • Motivate staff to make decisions and implement changes as quickly as possible (2) • Have Red Cross at Fareham Community Hospital (2) • Improve the efficiency of the administration support (2) • Charge those who use the Emergency Department inappropriately (2) • Procure additional necessary buildings / reopen units you have closed (2) • Help local communities have realistic expectations of the NHS (2)
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�24�of�237Page�9�of�76

• Increase health education to support people self-care (2) • Design strong referral routes based on the needs of the population (1) • Compare Queen Alexandra Hospitals performance against the best among similar
hospitals in the country (1) • Triage patients so they are seen at the right place (1) • Increase partnership working with social care (1) • Spend more money on the NHS and employ more staff (1) • Provide a rheumatology service at Fareham Community Hospital (1) • The CCGs seem to be heading in the right direction but it is early days (1) • Charge those who have not paid into the system for at least the last five years (1) • Reduce the long waits at the Emergency Department (1) • Open Minor Injuries Clinics to relieve the pressure on the Emergency Department (1) • Understand individual patient’s needs, both mental and physical (1) • Improve access to services (1) • Put PCs with access to NHS Direct in the Emergency Department and ask people to
use them to see if they could be treated elsewhere (1) • Improve the NHS 111 service (1) • Develop consistency and quality across all GP practices (1) • Stop the in-fighting between Portsmouth and Southampton (1)
5. What do you think are the main difficulties and opportunities for the NHS over the next five
years? 64 respondents answered this question with the following themes: Difficulties:
• Limited finances available to spend on the NHS (27) • Increasing population both in numbers and proportion of older people (18) • Expensive advances in medical technology and treatments (5) • Shortage of GPs, hospital doctors and qualified staff (5) • The political agenda can distract local areas from making the changes needed and
set unrealistic expectations from the general public (3) • People using services inappropriately (2) • Lack of nursing care in hospitals (2) • Lack of communication (2) • Rise in obesity (2) • Increasing demand (1) • Low staff morale (1) • Cleanliness in hospitals (1) • Increasing workload of community carers (1) • Persuading people that the NHS is value for money (1) • The expense of the PFI (1) • Lack of transport means people call an ambulance out of hours (1) • The amount of organisational changes made to the NHS nationally (1) • Privatisation (1) • Wasting resources on national IT projects, initiatives and too many managers (1)
Opportunities:
• Increase the number of specialists, hospital doctors and nurses (3) • Setting clear priorities and expectations for local residents (2) • Educating and empowering patients and local residents to take responsibility for their
health (2) • Increasing patient, public and community involvement in shaping healthcare (2)
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�25�of�237Page�10�of�76

• Developing more community services (2) • Charge patients who have never contributed towards the NHS (2) • Partnership working with social care, including private providers (2) • Developing IT solutions (1) • Adopting modern workflow practices and lean thinking (1) • Increasing the scope of Fareham Community Hospital (1) • Increasing health education (1) • Promoting services and what they do so local residents choose the right one (1) • Increase transparency (1) • Hold managers to account so changes are made (1) • Sponsorship for wards, services or pieces of equipment by private companies (1) • Treat patients as individuals and involve them in their healthcare (1) • Using latest research findings on conditions to help determine how to treat them (1) • Implementing new ideas in the simplest way possible to avoid over complication (1) • Introducing seven day working (1) • Using new technology to communicate with patients (1) • Plan for growth in communities now (1) • Getting the basics of healthcare right (1)
Themes from the CCGs Governing Bodies A joint Governing Body Development session was held for both CCGs and a significant section of the day was dedicated to Call to Action and the CCG five year strategy. The themes from this session are:
• Developing integrated services with our partners in social care, voluntary sector, education, housing and employment
• Taking a holistic approach to the personal as an individual • Providing clear signposting and navigation through the system • Providing care as a package rather than isolated interventions • Increasing admission avoidance by developing early intervention and increasing self help
and care • Breaking down barriers between organisations to increase joint working and integration • Developing locally based solutions • Providing outcome based solutions • Improving the quality and analysis of the information available so we can monitor the
impact services are having on patient outcomes • Improving patient experience and outcomes • Ensuring we use our budget effectively • Increasing the amount we spend on services closer to home and decreasing how much
we spend on acute services
Themes from our member GP practices Workshops on Call to Action and the CCGs five year strategy were held at both CCGs TARGETS (educational days for our GPs), both Practice Managers Forums and both Clinical Assemblies. The themes from these sessions are:
• Decreasing the number of frail, elderly patients being admitted to hospital
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�26�of�237Page�11�of�76

• Improving the quality and analysis of the information available • Developing more integrated services with social care, especially for End of Life patients • Ensuring the Directory of Services needs to do what it says it does • Exploring the concept of federated practices to see if there is support for it • Defining the weekend service model for GP practices • Reducing the number of inappropriate attendances to the Emergency Department and
exploring how GPs may be able to support this • Reviewing GPs workload as this is increasing yet their incentives are reducing • Stopping the duplication of work • Developing ways of having specialists working in services closer to home • Looking at how services can be provided across an area, eg a diabetes nurse based at
one practice but caring for the patients in several practices • Considering federating across primary and secondary care • Developing ways to manage patient expectation • Empowering patients • Ensuring you deal with the patient and not the condition to provide a more effective
service • Developing IT solutions such as aligning systems to allow data sharing • Developing a seamless service between primary and secondary care • Developing the use of the primary care record • Reviewing administration process so it is only undertaken if necessary, for example why
does the acute hospital send letters to GPs when there are alternatives • Ensuring we commission for patient outcomes • Increasing the support available for this with mental health conditions • Reviewing how we triage so it is consultant rather than nurse led • Reviewing the direct access radiology service so consultants review the patients • Tackling the difficulties of recruiting GPs to the local area, particularly in Gosport • Starting succession planning for GP practices as the number due to retire is large and
imminent • Providing career planning for new GPs so they are interested in becoming a practice
partner • Considering charging patients for some services • Setting and managing clear expectations with the public about the NHS can and cannot
afford to provide The groups were asked if the CCGs current priorities were right and which should be the focus for the organisation. It was felt that the Improving the Quality of care priority was the same as the Helping all communities access high quality care priority and they could be combined. They felt that the focus for the CCGs should be:
1. Improving the experience and outcomes for the frail elderly and people with long term conditions
2. Managing change in the health and social care system whilst ensuring continuity and improving quality
3. Enabling people with mental health condition and learning disabilities to receive care closer to home
4. Improving the quality of care and outcomes for patients 5. Care that is planned is delivered in the best way at the best time in the best place 6. Improving maternity and children services to better meet changing needs
Themes from our stakeholder workshops
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�27�of�237Page�12�of�76

We held two stakeholder workshops, one for each CCG, which were attended by key stakeholders including Councillors, Council officers, voluntary organisations, provider organisations and neighbouring CCGs. The content of the workshops covered both CCGs as some stakeholders covered both areas. A total number of 61 stakeholders attended. The numbers in brackets show how many comments were made relating to that theme. In groups, stakeholders were asked what do we want local healthcare to look like in 2020. To help their discussions they are asked three questions:
1. What should the priorities be for the CCGs over the next five years? 2. What do we need to change to achieve these? 3. How do we involve patients, service users and local residents in making these changes?
These themes from the discussions are (the numbers in brackets show how many comments were made relating to that theme):
1. What should the priorities be for the CCGs over the next five years? • Integrating seamless quality care between the NHS, social care and the voluntary
sector, including out of hours services (15) • Developing community resilience through prevention and education (including at
schools) (12) • Developing and improving communication and signposting so patients know what
is available including groups knowing about other groups and GPs knowing what is available (8)
• Increasing patient and public education and support to encourage self-care (7) • Improving mental health care both in and out of hours (4) • Developing primary care services and consistency in how GP practices operate
(4) • Working with voluntary groups to help people stay in their own home (3) • Developing outcome led commissioning that encompasses health and social care
priorities (3) • Putting the patient first and empowering them to be involved in making decisions
about their care (3) • Clarifying who is responsible for what when caring for each patient (2) • Improving the opportunities available for the frail elderly and those with long term
conditions (2) • Improving the quality of care and outcomes for all patients but focussing on the
most deprived communities (2) • Tackling health inequalities (2) • Developing IT solutions to share data and improve communication (2) • Preserving and developing local services (2) • Increasing patient and public involvement in developing services (2) • Taking the needs and views of carers into consideration (1) • Concentrating funding on / where you will get the maximum proven benefit (1) • Streamlining approaches to treatment and the patient journey (1) • Developing care models that meets customer needs (1) • Evaluating services more effectively (1) • Decreasing the independence on using virtual technology for involving and
communicating with patients and local residents (1) • Improving transport access to local services (1) • Investing more funding into the front end of care (1) • Involving supporting palliative care earlier and ensuring advance care planning (1) • Developing maternity and children’s services to provide care after birth (1)
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�28�of�237Page�13�of�76

• Encouraging the number of home births (1) • Increasing specialisation at the acute trust (1) • Better awareness by GPs on diagnosis and simple self-management for arthritis
(1) • Developing individual, personalised care plans for those with long term conditions
and embed this approach in services (1) • Integrating the planning and delivery of services for children (1) • Reviewing the use of terminology (ie what is a stakeholder?) (1) • Working with partners such as housing (1) • Developing End of Life services, including out of hours palliative services (1) • Increasing early intervention and getting patients onto the correct treatment (1) • Improving pregnancy and ante-natal care (1) • Streamlining learning disabilities services (1) • Improving stroke services (1)
2. What do we need to change to achieve these?
• Increasing partnership working with the voluntary sector and others (including schools) to provide education and awareness raising (5)
• Using signposting to information and advice service (4) • Increasing community services and out of hospital care (3) • Commissioning services from the voluntary sector (3) • Investing once in IT solutions that will help save resources (2) • Changing the NHS culture to focus on making changes where you get the most
benefit (2) • Integrating funding and services for health and social care (2) • Reducing the spend on acute services (2) • Developing communication skills with vulnerable groups (2) • Fostering innovation and efficiencies (2) • Commissioning services creatively using flexible contracts, incentives, etc (2) • Improving the Directory of Services (2) • Managing patient and public expectation (2) • Investing in the future by having more GPs and practice nurses (2) • Changing people’s attitudes so they take control and responsibility of their own
health (1) • Increasing accountability for professional decisions (ie empowering paramedics so
they don’t have to bring people to hospital if unnecessary) (1) • Extending the use of telemedicine and support to patients from consultants over
the phone (1) • Providing disability awareness training for all front line staff (1) • Providing greater diversity of provision (1) • Adopting the Troubled Families model of having lead agencies (1) • Driving quality (1) • Building capacity (1) • Developing GP surgeries into health and wellbeing centres (1) • Improving mental health outcomes (1) • Commissioning stable services (1) • Rewriting the service specifications and ITTs so they reflect the local need (1) • Making decisions in an informed way (1) • Using pharmacies more effectively (1) • Revising DESMOND so it includes patients who have had diabetes for a while
rather than just newly diagnosed patients (1) • Building voluntary sector support into patient education programmes (1)
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�29�of�237Page�14�of�76
• Increasing funding to the CCGs (1)
3. How do we involve patients, service users and local residents in making these changes? • Using existing community communications channels such as voluntary groups,
newsletters, council meetings, group websites and youth services newsletters (4) • Working with the voluntary sector to reach local residents to ask for their views
and feedback (2) • Engaging early with patients and local people in their own communities so they
can be involved in big strategic changes (2) • Changing our language so it is easier to understand (2) • Providing more education and awareness raising opportunities and events on a
wide range of topics that involve GPs and consultants (2) • Providing more opportunities for people and groups to get involved (2) • Linking with existing participation groups (2) • Tackling ageism in the NHS (1) • Understanding peoples motivators (1) • Ensuring the requirement for GP practices to have Practice Patient groups
continues after 2014 (1) • Providing support to carers (1) • Encouraging people to get involved by explaining how a change may affect them
(1) • Make it more attractive to get involved (1) • Investing in developing engagement methods that allow people to have the
conversation (1) • Making sure people are told how their feedback has been used (1) • Going to groups and meetings attended by minority groups (1)
The groups were asked if the CCGs current priorities were right and which should be the focus for the organisations. The priorities are listed below in order of which stakeholders felt should be the focus for the organisations (the numbers in brackets are the number of votes received):
1. Prevention and education – this was added as a priority by the groups (56) 2. Improving the experience and outcomes for the frails elderly and people with long term
conditions (54) 3. Care that is planned is delivered in the best way at the best time in the best place (52) 4. Managing change in the health and social care system while ensuring continuity and
improving quality (40) 5. Improving the quality of care and outcomes for patients (35) 6. Enabling people with mental health conditions and learning disabilities to receive care
closer to home (33) 7. Helping all communities access high quality care (25) 8. Improving maternity services and services for children to better meet changing needs
(15)
The groups were also asked which of the CCGs current priorities should receive the most financial investment. The priorities are listed below in order of which stakeholders felt should receive the most financial investment (the numbers in brackets are the number of votes received):
1. Improving the experience and outcomes for the frails elderly and people with long term conditions (61)
2. Enabling people with mental health conditions and learning disabilities to receive care closer to home (45)
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�30�of�237Page�15�of�76

3. Prevention – this was added as a priority by the groups (42) 4. Care that is planned is delivered in the best way at the best time in the best place (41) 5. Managing change in the health and social care system while ensuring continuity and
improving quality (36) 6. Improving the quality of care and outcomes for patients (29) 7. Helping all communities access high quality care (26) 8. Improving maternity services and services for children to better meet changing needs
(20)
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�31�of�237Page�16�of�76

Communications and Engagement Plan
1. Objectives A combined period of engagement will be undertaken across South Eastern Hampshire and Fareham and Gosport CCG. The objectives of this work are to:
• Raise stakeholders awareness of what the CCGs are and what they stand for • Raise stakeholders awareness of ‘Call to Action’ • Use existing mechanisms for external and internal engagement to gain stakeholders views for use in the development of the CCGs
strategies and ‘Call to Action’ • Seek the views of provider organisations for use in the development of the CCGs strategies and ‘Call to Action’ • Ensure how the views gained during the engagement period have influenced the CCGs strategy are communicated effectively with
stakeholders • Ensure the views gained during the engagement period are shared with NHS England for ‘Call to Action’ • Ensure stakeholders are informed about how their views have been shared with NHS England for ‘Call to Action’.
2. Stakeholders/Audiences For the purpose of this strategy, stakeholders are defined as: Any individual, group, or institution who has a vested interest in the project and/or who potentially will be affected by project activities and have something to gain or lose if conditions change or stay the same. Stakeholders have been identified and plotted onto a stakeholder matrix in Appendix A. The stakeholders identified can be grouped into the following three broad audiences:
• CCG Governing Body members and constituent GP practice members • Patients, members of the public and their representatives (such as MPs and the Hampshire Health Overview and Scrutiny
Committee) CCG Project Plan Version 2 1 Updated on 14/03/2014
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�32�of�237Page�17�of�76

• Partner organisations including neighbouring CCGs, provider Trusts and representative bodies (such as the Local Medical Council). Both South Eastern Hampshire and Fareham and Gosport CCGs are committed to furthering equality, diversity and human rights and reducing inequalities in health. It is acknowledged that we need to communicate and engage with people who are separated by geography, interests and levels of knowledge and ability/disability. We also need to recognise and be sensitive to cultural and language barriers and to adapt methods accordingly.
3. Communications and engagement phases The communications and engagement activity will be carried out in following two key phases:
• Phase one – Information gathering and seeking views from key internal stakeholders including Governing Body members, chief officers and senior managers
• Phase two – Seeking the views of external stakeholders including patients, local residents, the voluntary sector, MPs, Councillors and provider organisations.
4. Communications and engagement methods and routes Primarily views will be gathered using a survey. The survey will ask for views on:
• The NHS in its widest sense • What people value in terms of healthcare • If the priorities for the CCGs are right • What we could change or do differently • What we could now to make changes more quickly • What people think the main difficulties and opportunities for the NHS over the next five years.
In addition a range of communications and engagement routes will be used including:
• Stakeholder workshops (one in each CCG area) • Existing groups and events such as Community Engagement Committees • Briefings • Face-to-face meetings/emails • Press releases
CCG Project Plan Version 2 2 Updated on 14/03/2014
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�33�of�237Page�18�of�76

• CCG stakeholder newsletters • Voluntary sector online newsletters • CCG websites and Twitter account • Partner NHS organisation websites • South Eastern Hampshire and Fareham and Gosport CCGs PIP sites (Primary Information Portals – extranet sites for GP practices).
5. Key messages The success of the plan will depend on consistently using the following agreed messages:
• Our strategy is being developed by local GPs who really know what patients need • Your views are invaluable in helping local GPs decide what our priorities should be and how we can achieve them • Maintaining high quality care for patients is our top priority • The NHS is facing increasing financial pressures so needs to change how it does things.
These messages will be regularly reviewed, and revised if required, as ‘Call to Action’ recommendations and materials become available.
6. Strategy development actions A table detailing the actions required to be taken as part of the strategy development is available in Appendix B. This includes the planned communications and engagement activity.
7. Use of feedback received All of the feedback received will be collated and analysed for trends. This analysed data will be used by the CCGs in the development of their strategy. The data will also be shared with the Wessex Area Team and NHS England as part of our response for ‘Call to Action’.
8. Evaluation process The effectiveness of this Communications and Engagement Strategy will be ongoing throughout the plan. This process needs to be included in the ongoing evaluation of the strategy development.
CCG Project Plan Version 2 3 Updated on 14/03/2014
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�34�of�237Page�19�of�76

Appendix A The following stakeholders have been identified and plotted onto the stakeholder matrix below. Each stakeholder group is identified on the matrix by its corresponding number. The critical stakeholders/audiences groups for this Strategy are: External 1. Patients/service users 2. MPs 3. Hampshire County Councillors 4. Fareham Borough Councillors 5. Gosport Borough Councillors 6. Havant Borough Councillors 7. East Hants District Councillors 8. Council Leaders 9. Council Chief Executives 10. Council Health Leads 11. Director of Public Health 12. Hampshire Health and Overview Scrutiny Committee (Committee members and supporting officers) 13. Hampshire County Council Adult Services Department Senior Management Team 14. Hampshire County Council Childrens Services Department Senior Management Team 15. Hampshire County Council Local Strategic Partnerships 16. South Central Ambulance Service 17. Wessex Local Medical Committee 18. Hampshire Health and Wellbeing Board 19. Healthwatch 20. Fareham and Gosport and South Eastern Hampshire residents 21. Seldom heard groups 22. Local media 23. Voluntary sector organisations 24. Patient Participation Groups Internal 25. South East Hampshire CCG Governing Body
CCG Project Plan Version 2 4 Updated on 14/03/2014
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�35�of�237Page�20�of�76

26. Fareham and Gosport CCG Governing Body 27 Fareham and Gosport and South Eastern Hampshire GP practices members 28. Portsmouth CCG Governing Body 29. Portsmouth Hospitals NHS Trust 30. Southern Health NHS Foundation 31. Solent NHS Trust 32. South Central Ambulance Service NHS Foundation Trust 33. Care UK (GP Out of Hours) 34. Hampshire Hospitals NHS Foundation Trust 35. Royal Surrey County Hospital NHS Foundation Trust 36. Western Sussex Hospitals NHS Foundation Trust 37. University Hospital Southampton NHS Foundation Trust 38. Pharmacies 39. Local Pharmaceutical Committee 40. Dentists 41. Local Dental Committee 42. Opticians 43. Local Optical Committee
CCG Project Plan Version 2 5 Updated on 14/03/2014
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�36�of�237Page�21�of�76

2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37
1, 20, 21, 22, 23, 24
38, 39, 40, 41, 42, 43
CCG Project Plan Version 2 6 Updated on 14/03/2014
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�37�of�237Page�22�of�76

Appendix B – Action plan Please note the actions/activity and dates in the table below are subject to change.
Action/Activity Details Date Lead Additional notes F&G GB public seminar Presentation given and handouts
given out. Copies of Call to Action document and survey available.
Complete (13/11/13)
ST/EK 20 members of the public attended
SEH GB public seminar Presentation given and handouts given out. Copies of Call to Action document and survey available.
Complete (20/11/13)
ST/EK 10 members of the public attended
Planning Workshop for CCG staff
Organised by Mike Drake Complete (25/11/13)
MD
Fareham Area Active Blind group
Presentation given and handouts given out. Copies of Call to Action document and survey available.
Complete (28/11/13)
BW Group invited us to attend and give the presentation following seeing it at Governing Body
Fareham Community Hospital Open Day
Presentation given and handouts given out. Copies of Call to Action document and survey available.
Complete (30/11/13)
BW Invited to attend and give the presentation following seeing it at Governing Body 170 people attended the event
Develop online survey and dedicated web page on each CCG website
Single survey using survey monkey with dedicated pages on both CCG websites with link to survey, presentation, JSNA info and national site
Complete (02/12/13)
EK/SR ST to approve survey questions and web copy
Media work Promote survey Ongoing MW/SM Social media work Promote survey Ongoing SR Twitter schedule SEH CCG CEC Presentation given and handouts
given out. Copies of Call to Action document and survey available.
Complete (04/12/13)
ST/JP
Havant Health and Wellbeing Seminar
Presentation given and handouts given out. Copies of Call to Action document and survey available.
Complete (05/12/13)
ST/JP
East Hampshire District Council meeting
Presentation handouts and survey given out
Complete (09/12/13)
JP
Article in Radian e-magazine Article about Call to Action / Complete EK E-magazine sent out 10/12/13 CCG Project Plan Version 2 7 Updated on 14/03/2014
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�38�of�237Page�23�of�76

Strategy development and links to website
(09/12/13)
Article in Badgerswood and Forest Surgeries newsletter
Article about Call to Action / Strategy development and links to website
Complete (16/12/13)
MW Newsletter due out bgn Jan
Joint GB Development Session
Complete (18/12/13)
ST/JP External facilitator leading
Articles in stakeholder newsletters
Short articles in both newsletters directing people to web page and survey and offering to attend meetings
Complete (20/12/13)
MW/SM
F&G CEC Introduction to Call to Action and Strategy work
Complete (07/01/14)
EK Members told about the stakeholder workshop and checked they had received an invite
Article in Top Tips Article about Call to Action / Strategy development and links to website
Complete (07/01/14)
EK/LHT Article aimed at practice staff
Article in Commissioning Times
Article about Call to Action / Strategy development and links to website
Complete (09/01/14)
EK
SEH CCG PM Forum Presentation including details of survey given
Complete (21/01/14)
EK/KO
F&G CCG Extraordinary PM Forum
Presentation including details of survey given
Complete (21/01/14)
EK/KO
SEH CCG TARGET Presentation and workshop session
Complete (23/01/14)
EK/PH
SEH engagement event Presentation and workshop session
Complete (27/01/14)
EK/PH
SEH CCG Clinical Assembly Presentation and group discussions
Complete (28/01/14)
ST
F&G CCG TARGET Presentation and workshop session
30/01/14 EK/PH
F&G engagement event Presentation and workshop session
05/02/14 EK/PH
Joint GB Development Session
To see first draft of the strategy 19/02/14
CCG Project Plan Version 2 8 Updated on 14/03/2014
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�39�of�237Page�24�of�76

F&G CCG Clinical Assembly Presentation and group discussions
25/02/14 EK/PH
CCG Project Plan Version 2 9 Updated on 14/03/2014
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�40�of�237Page�25�of�76

1
A five-year strategy for local health services
About: 1/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�41�of�237Page�26�of�76

1
Contents
________________________________________________________________
About this strategy 3
Vision 9
Quality and outcomes 20
Sustainability 29
Interventions 30
Governance 45
Values 49
________________________________________________________________
About: 2/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�42�of�237Page�27�of�76

1
About this strategy _______________________________________________________________
A radical transformation of the health care environment to secure high quality, integrated and sustainable health care driven by the needs and expectations of the people we serve. _______________________________________________________________
Fareham & Gosport and South Eastern Hampshire clinical commissioning groups share one deceptively simple purpose: to ensure that NHS funds are used to bring about improved health outcomes and services for the people of the area. We were established, as part of the NHS reforms, to ensure that family doctors and other clinicians lead decisions on how to direct NHS resources. We sit at the heart of NHS and are set up to listen to and act on the wishes of patients, and to work closely with local authorities and other health partners. This document sets out our five-year strategy for the development of improved health across the area served by the CCGs. It reflects both national objectives and important local priorities. These come together to form a new, ambitious and challenging agenda for the local NHS, one designed to safeguard services and maximise resources, place the patient at the centre of the decision-making process, and improve the quality and range of services available. The contents of this strategy reflect the demands of the NHS Mandate, Constitution, Outcomes Framework and Better Care Fund. However, they respond specifically to the requirements of ‘Everyone Counts: Planning for Patients 2014/15 to 2018/19’ produced in December 2013 by NHS England. The purpose of this strategy is to deliver high quality care and to achieve excellent outcomes for patients. These outcomes include: preventing people from dying prematurely, helping people with long-term conditions get the best possible quality of life, enabling people to recover quickly and successfully, ensuring people’s experience of care is excellent, and keeping patients safe. NHS England has converted these outcomes into seven measurable ambitions:
• Securing additional years of life • Improving the quality of life for people with long-term conditions • Reducing the amount of time people spend in hospital • Increasing the proportion of older people living independently at home
following discharge from hospital • Increasing the number of people with mental and physical health
conditions who have a positive experience of hospital care • Increasing the number of people with mental and physical health
conditions who have a positive experience of care outside of hospital • Making progress towards eliminating avoidable deaths in our hospitals
About: 3/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�43�of�237Page�28�of�76

1
The strategy is consistent with these objectives and, in addition, seeks to focus on: improving health, reducing health inequalities, and moving towards equality of service between mental and physical health. To understand and gauge progress towards these outcomes and ambitions, NHS England has identified the six characteristics that a high quality, sustainable, health and care system will be able to demonstrate in five years’ time. These are:
• a new approach, to ensure that citizens are fully included in all aspects of service design and change
• wider primary care, provided at scale • a model of integrated care • access to the highest quality urgent and emergency care • a step change in the productivity of elective care • specialised services concentrated in centres of excellence
In order to harmonise its efforts with NHS colleagues and to demonstrate common links with health and social care partners, we have organised our vision to focus on and reflect these characteristics. ________________________________________________________________ How this strategy is organised This strategy has six main sections: Vision. This brings together the ambitions of all those responsible for health services in the two CCG areas. It sets out how we have worked with our partners to agree key priorities for the local NHS and how each has been developed following extensive consultation with the people we serve. Quality and outcomes. This sets out where we are now and the main health challenges we face. It shows how the local health economy plans to meet both national and local ambitions for the NHS and the level of improvement expected. Sustainability. The NHS will be required to achieve its aims within a limited budget. This section describes how we will achieve our goals, maintain financial stability, and manage our financial and other resources in ways that are both effective and sustainable. Interventions. Here, we describe in detail the plans and programmes we will put in place to achieve our aims within the resources available to us. Governance. This section looks at how we will oversee this programme of improvement, account for what we do and ensure the very highest levels of probity and safety. Values. We believe that it is only possible to achieve our plans by acting in an honest and principled manner. Here, we set out our values, beliefs and principles. In essence, this strategy shows how Fareham & Gosport and South Eastern Hampshire clinical commissioning groups will secure high quality care for all, both About: 4/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�44�of�237Page�29�of�76

1
now and in the future. Its success will be determined by how well it is able to unify the efforts of all those responsible for improved health, listen to and act on the views of local people, drive further improvements in the quality and safety of services, and deliver both economy and value from the resources available. ________________________________________________________________ Our areas The areas served by Fareham & Gosport and South Eastern Hampshire CCGs South Eastern Hampshire Clinical Commissioning Group covers 150 square miles, including Havant, Waterlooville, Petersfield, Bordon and part of the South Downs National Park.
Fareham and Gosport Clinical Commissioning Group covers 38 square miles, including Fareham, Portchester, Crofton, Titchfield, the Western Wards, Gosport, Bridgemary, Elson and Lee-on-the-Solent.
________________________________________________________________ Our communities South Eastern Hampshire CCG a population of around 209,000 people. This includes:
• A higher than average number of people aged 45 to 60 years
• Lower than average numbers of young people
• 6,000 people who are over the age of 85 years
• Around 2,500 new births every year.
Fareham and Gosport CCG covers a population of around 200,000 people. This includes:
About: 5/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�45�of�237Page�30�of�76

1
• A large younger population with more people aged under 20 than over 65 years
• More people aged over 45 years than the national average
• The birth rate in Gosport is higher than the national average.
Tables showing the make-up of our populations and the forecast changes up to 2018 can be found below:
About: 6/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�46�of�237Page�31�of�76

1
As you might expect within a diverse area, the health picture for our population varies. Economic and lifestyle factors can be a big influence on health and we know that there are areas of significant deprivation in the local area, particularly in parts of Gosport and Havant, and this can have a big impact on people's health and wellbeing.
We know that:
• People in the more affluent areas of South East Hampshire are likely, on average, to live around 2.7 years longer than those in more deprived areas
• The proportion of people living with cancer is greater than the national average
• A higher proportion of people have chronic heart disease, stroke and hypertension than compared to other parts of the country
About: 7/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�47�of�237Page�32�of�76

1
• The proportion of people with mental illness or dementia in our area is similar to figures nationally; however estimates suggest that dementia rates will increase significantly over the next 20 years.
• Levels of smoking and obesity in Fareham and Gosport are slightly higher than the local and national average.
________________________________________________________________
About: 8/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�48�of�237Page�33�of�76

2
Our vision ________________________________________________________________
Our mission is to improve the health and wellbeing of the 410,000 people living and working in Fareham, Gosport and south eastern Hampshire and to make sure health services continue to be affordable and accessible to everyone. We shall do this by working together with our partners, patients and the public to transform the way health care is delivered and to commission excellent integrated patient centred care. ________________________________________________________________ Our five-year vision We have used feedback from a programme of engagement with local people in the autumn of 2013 and the ‘Think Local Act Personal: Making it Real’ approach to set five core objectives for the next five years. Our objectives are our response to the Making It Real ‘I’ statements which highlight the issues most important to the quality of people's lives and what people want to see and experience from personalised care services. In five years’ time we want all local people to have: • easily available information and advice to remain as independent as
possible; • access to a range of support that helps them to live the life they want
and remain a contributing member of the community; • flexible, responsive integrated care and support that is directed by patients
and their carers; • considerate, consistently high quality care delivered by competent
people; • support systems in place so that they can get help at an early stage to
avoid a crisis; • the right support in a place of their choosing should they need urgent or
emergency care. ________________________________________________________________ Five core objectives In order to do this we believe we must: 1. Integrate primary care, community care, social care and voluntary services to
Vision: 9/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�49�of�237Page�34�of�76

2
deliver a range of services, close to home for people with mental health conditions, learning disabilities and those who are elderly and frail.
2. Commission services that deliver services close to home to support each
individual with long term conditions, including mental health conditions and learning disabilities to stay healthy and feel in control of their condition.
3. Work with local people and their communities to prevent the causes of ill
health, support healthy lifestyles, reduce health inequalities and to give children the best start in life.
4. Eliminate variable standards and ensure consistency in the quality of
services across all care providers. 5. Ensure a range of easily accessed and responsive urgent and emergency
care to support people in a crisis. ________________________________________________________________ Building our vision This vision is not one constructed by the CCGs alone. It has grown from a concerted effort to listen to local people, our patients, and our colleagues working in other parts of the health and social care system, nationally and locally. It also responds to the strategic direction for health care set by the Hampshire Health & Wellbeing Board. Working with the NHS This strategy responds to the requirements of ‘Everyone Counts: Planning for Patients 2014/15 to 2018/19’ produced in December 2013 by NHS England. It builds on national expectations for improved outcomes and sets out approaches consistent with the six characteristics of a high quality, sustainable health and care system. Working with our communities We conducted a programme of engagement to test the views and wishes of our local communities. This work supported the NHS England ‘Call to Action’ exercise, helped us raise awareness of CCGs and what they do, and allowed us to seek and clarify the opinions and priorities of local people. It also brought together the perspectives of provider organisations. Working with our partners
The vision embraces the four key objectives set by the Joint Health and Well Being Strategy. Starting Well: so every child can achieve its potential and will thrive through transition to adulthood. Living well: empowering people of all ages to live healthier lives. Ageing well: supporting people to remain independent, in Vision: 10/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�50�of�237Page�35�of�76

2 control with timely access to high quality services. Healthier communities: helping communities to be resilient, strong and support those who may need extra help. Members of the Health and Well Being Board attended our stakeholder workshops and will continue to work with us to further develop and implement this strategy. Further information on the work we will do advance the Health and Wellbeing Strategy is set out in section 3 (Quality and Outcomes) on page 20 and section 5 (Interventions) on page 30. ________________________________________________________________ Turning our vision into reality Progress towards our vision will be judged against our ability to achieve six characteristics of a high quality sustainable health system. These are: 1. Citizens fully included in all aspects of service design and change, and patients fully empowered in their own care.
We are committed to working with local communities and services, and to supporting patients and carers to take control of their own care and wellbeing.
Our aim is to ensure that our commissioning decisions flow from the perspectives of local communities and the involvement of people that use services. This will bring a better understanding between all parties of the assets available within local communities and foster a desire to identify and solve problems together.
This approach is fundamental to our ambitions to transform out of hospital care, so that it is both integrated with other services and person-centred, and to redesign our hospital and urgent care services on the basis of insights provided by patients.
We shall work to set and meet objective and measurable targets to improve individual and community participation. All engagement models will include a feedback process to keep citizens informed of the progress of projects and to describe how their input has been used in the process.
We will develop our range of opportunities for participation with diverse communities and will also continue to develop our Community Engagement Committees.
2. Wider primary care provided at scale
We believe that the current model of general practice and primary care will need to change in the next five years. Satisfaction is high but pressures remain, caused by a growing elderly population, a growth in the numbers with long term health problems and difficulties in recruiting staff.
Vision: 11/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�51�of�237Page�36�of�76

2 GPs are telling us that there is an increasing demand for primary care from an ageing population and increasing levels of need from people with long-term conditions. This coupled with problems in the recruitment of staff creates significant pressures on general practice. When these challenges are added to an expected growth in those people with complex or multiple health problems, we know that we cannot continue to do more of the same. Therefore, a new and developing range of solutions and services will be pursued.
We will support GPs to provide care that can be integrated more effectively with other services, particularly those for the elderly or with long-term conditions. Larger groupings of practices will support the deployment of more sophisticated ways of working with patients to improve the quality of services. However, simply increasing the quantity of face-to-face GP consultations alone will not be a cost-effective or sustainable. The GP of the future will need to be skilled in using a suite of new and flexible tools for communicating with patients, including telephone, email and various online forms of consultation.
We are committed to ensuring that shared information and communication systems support and enable this transformation. Securing the GP workforce of the future will remain a major challenge. We will support a broader range of entry solutions to the profession and develop more effective recruitment and working practices. We also want to see a larger role for CCGs in the commissioning of primary care. This will encourage the formation and extension of primary care federations and networks, and support practices to provide enhanced services.
3. A modern model of integrated care
We will adopt approaches to commissioning that will bring about a radical transformation in the way the health and care system organises itself. Working with Hampshire County Council will use the Better Care Fund to drive forward this new way of commissioning and providing health and social care.
This five year strategy aligns with the Better Care Fund vision for a simple, “joined-up” health and care journey through the system for people and communities.
This approach aims to address three key challenges:
• Avoiding unnecessary cost in the system, moving to lower cost solutions
• Preventing dependency and demand for longer term publically funded services
• Delaying people’s dependency on long term health and social care interventions
The current provider landscape is too complex and fragmented to meet the challenge of improving outcomes for local people. We anticipate that, ultimately, we will be commissioning health and care from ‘accountable care organisations’. Currently, payments to providers are too rigidly related to outputs such as the
Vision: 12/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�52�of�237Page�37�of�76

2 number of people seen. An ‘accountable care organisation’ (ACO) is characterised by a payment and care delivery model that reimburses providers for achieving outcomes, quality metrics and reductions in the total cost of care for an assigned population of patients. A group of coordinated care providers forms an ACO, which then provides care to a group of patients. The ACO would be accountable to both local people and the CCGs for the quality, appropriateness and efficiency of the care provided.
The footprint for ACO working will be developed. It is envisaged that it will be organised to serve smaller populations of between 30,000 and 50,000 and be led by both clinical and professional staff who will create the culture and assure standards of care.
4. Access to the highest quality urgent and emergency care
Urgent and emergency care remains an important point of access to the NHS for many patients and one that has a profound and complex relationship in terms of effectiveness with other parts of the health system. We wish to see further and significant improvements in how these services work in partnership with emergency, primary and social care colleagues and in the quality of and access to care.
With colleagues and led by GP commissioners, we will work to review and redesign services and develop project plans to ensure delivery of high quality urgent and emergency care. These will further test new models of provision.
We will continue to improve the responsiveness and effectiveness of the urgent care services (including the Emergency Departments and Minor Injuries Units) that we currently commission. In addition, however, we will enable 15% more people to be safely and appropriately cared for in their own home rather than having to be admitted to hospital. We will achieve this by ensuring that everyone working with the individual and their carer understand the individual’s care plan and wishes and by ensuring that we have commissioned sufficient services in the community to ensure that the individual receives the right support and importantly feels confident in these services.
We will extend the use of both telehealth and telecare solutions to improve the way in which we can support and monitor individuals’ health and wellbeing and develop greater managed care capacity that will allow providers to proactively communicate with and support individuals who would benefit from such an approach.
5. A step change in elective care
The populations we serve benefit, on the whole, from excellent access to planned or elective care. General Practice is of excellent quality and well regarded by patients and provides a good conduit into consultant-led advice and treatment. Thereafter, local people are able to make choices from a number of quality
Vision: 13/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�53�of�237Page�38�of�76

2 provider organisations with good outcomes and relatively short waiting times. There are, however, two significant challenges facing the current service model which need to be addressed:
For some people, and particularly those from our most deprived population, the use of planned care and access to specialised secondary care services is unacceptably low. Too often people from our most deprived communities such as Leigh Park, Wecock Farm and Rowner use emergency services rather than accessing planned care in a timely way and consequently will see an unnecessary deterioration in their condition and poorer outcomes. Supporting these communities to engage with health and care at an earlier stage is a key priority.
The second challenge is that the demand for planned care is rising at an unsustainable rate. With referrals for planned care increasing at around 5.5% year on year, and with this growth in a number of specialties being for suspected cancers under the two-week wait rule, Hospitals are increasingly facing capacity challenges. We know, however, that a proportion of these referrals (varying by specialty) will not add any value for the individual.
To address these challenges, we will take forward the following strategies:
Building on the considerable success of the redesign of the Portsmouth and South East Hampshire diabetes service, we will expand the community-facing delivery model in a number of associated specialties, including Repeat Pain Procedures, BNP Testing, Ophthalmology, Dermatology, Orthopaedics/MSK and Hepatology. We anticipate that the consultants and specialised nurses currently operating in these specialties will provide a stronger advisory and population management role advising and educating the integrated care teams and supporting GPs in the local management of people’s conditions.
We have commissioned new service models in both ophthalmology and orthopaedics but intend to explore with provider partners the evolution of the current contractual arrangements from a system of payment by results to an outcome based approach where, for example, we are commissioning for improved patient reported outcomes rather than simply activity.
We will also review the role and use of diagnostics in the way in which we deliver care. We will explore greater primary care access to diagnostics, accelerating diagnosis and hence treatment. We will also explore developing the current model of diagnostic delivery, encouraging greater partnerships between existing provider organisations to strengthen quality access and reduce costs.
6. Specialised services concentrated in centres of excellence
Specialised services which treat either rare conditions or those that need a specialised team working together at a centre are commissioned by NHS England.
Vision: 14/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�54�of�237Page�39�of�76

2 Fareham and Gosport and South Eastern Hampshire Clinical Commissioning Groups will work in partnership with NHS England’s Wessex Area Team to ensure the whole patient pathway for these specialised services is as locally responsive as possible in meeting patients’ needs. The CCGs are committed to working with NHS England’s Local Area Team to support the delivery of the clinical strategies set out within five National Programmes of Care and will contribute to the development of the five year strategy for specialised services through the five service planning events for internal medicine, cancer and blood, women and children, trauma and mental health. Work to achieve our vision is described in more detail in section 5 (Interventions) on page 30. ________________________________________________________________ New approaches to commissioning and delivery Central to our vision are new approaches to the commissioning and delivery of services that develop and rely on integrated approaches to care. These will build on work already completed over the last 18 months but will require further ambitious change in the way the CCG operates. ________________________________________________________________
Commissioning Integrated commissioning. The Clinical Commissioning Groups consider the integration of commissioning with Hampshire County Council and our District and Borough Council partners (namely Fareham Borough Council, Gosport Borough Council, Havant Borough Council and East Hampshire District Council) as a central tenant of this commissioning vision. For too long, health and care services provided to local people have been unnecessarily fragmented resulting in higher cost and poorer outcomes. For care to be truly person-centred, health commissioning has to radically change its approach and realise the opportunities presented by planning and procuring services in partnership with Local Authorities. The drive for integration will build on the foundation brought about by the Better Care Fund. Integration and scale. Since their creation in April 2013, Fareham and Gosport and South Eastern Hampshire CCGs have embraced the concept of operating at scale to deliver greater efficiency. This has included a shared management team and increasing levels of co-operation and skill sharing among clinical leaders. We also work in a ‘compact’ with neighbouring Portsmouth CCG to realise economies of scale and to act as a single commissioning entity when dealing with local providers. In the coming years, we intend to expand these collaborative relationships to our local authority partners, both at county and district/borough
Vision: 15/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�55�of�237Page�40�of�76

2 level to maximise opportunities to commission collaboratively for the maximum benefit of local people. We expect to continue to develop our clinical leaders so they are equipped to lead both collaborative commissioning and also new models of service provision with general practitioners working alongside community services, adult social care and voluntary sector colleagues for integrated care provision. Common purpose and common infrastructure. In order to strengthen joint commissioning arrangements, both CCGs will work with local authority partners to co-locate commissioning teams. This will enable the creation of Locality Commissioning Hubs including Health commissioners The CCG will also review its make / share / buy model to strengthen the shared infrastructure (e.g. finance, information, business intelligence, etc) with co-commissioners in the Local Authority. Building strong partnerships. The CCGs will be developing locality specific strategies where these are relevant, necessary and add value. For example, the CCG will be working with Hampshire County Council, Havant Borough Council, the Police and Crime Commissioner and other partner agencies to develop an ambitious strategy to combine resources and physical assets across Leigh Park to benefit this more deprived population. A similar approach will be developed for Rowner in Gosport Considerable work has been undertaken to develop health services for the population of Whitehill and Bordon, an area of relatively poor access and communication routes and with some specific health and care needs. Central to our five-year strategy will be the further development of this plan, broadening the vision to develop more health and wellbeing services and using new technologies to overcome any geographic barriers. Commissioning for better outcomes. In parallel to the drive to integrate commissioning with local authority partners, is the intention of the CCGs to depart from current approaches to contracting, specifically: block contracts for community based services, including mental health; and activity-based or day rate payments for much of secondary, residential and domiciliary care. Whilst the CCGs do not currently contract for primary care services, it is the intention of both organisations to work with NHS England Area Team to explore the potential of either delegated or joint commissioning of primary care to ensure an absolute alignment of primary care with integrated health and care services. The CCGs are working in partnership with the Local Authorities and Portsmouth CCG, drawing on the expertise of COBIC and Optum Health, to develop a new outcomes-based approach to commissioning. This approach will shift the focus of providers from delivering isolated components of care for people with long term conditions or the elderly, to one where all health and care delivery outside of an acute hospital setting is planned and delivered to meet the needs of the wider needs of the individual. In practical terms, this will ultimately mean a single contract with a delivery vehicle encompassing community nursing and therapy, adult and older persons mental health, social care provision, elements of Vision: 16/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�56�of�237Page�41�of�76

2 secondary care, elements of primary care (including out of hours and 111) and relevant voluntary sector provision. The benefits of integrating health and care are well established across UK and international health care systems. For the local health and care system, the CCGs are planning on releasing costs from both the current out-of-hospital delivery system and the acute hospital as the non-elective bed stock is reduced in response to a reduced number of non-elective acute admissions and a reduced length of stay for those patients requiring admission. The relationship with the provider in this new approach will need to be longer than the traditional three-year contract. The scale of transformation required in terms of workforce, estates, information and infrastructure would necessitate a contractual relationship of between six to nine years to allow for the necessary investment and return on this investment. The contract will also be judged not on the activity that this undertaken or the costs incurred, but on the outcomes that are secured for the defined population. In this respect, we anticipate a flow of resource from treatment to prevention and promotion. We also believe that this approach to commissioning will enable us to tackle the very clear inequalities that some of our population currently experience. Whilst we still see a fundamental role for the market and choice in many elective specialties, we will also be moving towards outcome based contracts for the provision of elective musculo-skeletal care; ophthalmology and ENT. Information for better outcomes. Central to developing a new outcomes-orientated approach to commissioning will be the development of the integrated information sources that will enable both commissioners and providers to understand efficiency and quality improvement opportunities. It will also allow for greater confidence for commissioners when negotiating contracts with provider partners. The CCGs have engaged Millimans, global health actuaries, to firstly integrate primary, community, secondary, prescribing and social care data and secondly to help us develop an actuarial perspective of our communities’ needs. This is a critical foundation if we are to successfully develop and operate outcomes based commissioning. ________________________________________________________________ Delivery Harnessing third-sector expertise. Whilst the CCGs will not seek to be prescriptive about the design and delivery systems of an accountable care organisation, it will be clear about the importance of the voluntary sector being central to any care planning and delivery. In many respects the greatest impact derived from the integration of care providers is the harnessing of the innovation enthusiasm and expertise of the voluntary sector. Estates and infrastructure. The CCGs are liable for all void space in properties now owned by NHS Property services so we are keen to ensure the full utilisation of these sites. More generally, we want to encourage the further rationalisation of Vision: 17/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�57�of�237Page�42�of�76

2 the estates within the Portsmouth and S E Hants health system. However, we recognise that patients will wish to continue to have access to locally provided services where possible. The CCGs will also support the full and efficient utilisation of our local PFI funded general hospital. The ongoing development of primary care (commissioned by NHS England) will also have a potentially significant impact on the use of the health estate locally and we will review how we can support the transition required in primary care in terms of ways of working and the use of the estate. ________________________________________________________________ Building on firm foundations In our first year, South Eastern Hampshire CCG and Fareham and Gosport CCG have delivered a number of important service improvements that will act as the foundation for taking forward this strategy.
Integrated care team are being piloted in several areas across the CCGs and this will provide the basis from which these services will be rolled out across the two CCGs. In the next eighteen months we will rapidly expand this model of care by developing the local community workforce across agencies into fully integrated care providers. A number of new pathways for elective care have been commissioned including a new musculo-skeletal and persistent pain service. On-going review and refinement of pathways will be central to our work to increase the efficiency and efficacy of the elective care system and ensure that patients are referred to an appropriate service avoiding unnecessary hospital visits. We have expanded the services available out of hospital by commissioning new models of delivery. This has included commissioning a new community ophthalmology service and the redesign of the Portsmouth and South East Hampshire diabetes service. We intend to build on this success to expand the community-facing delivery model in a number of associated specialties. We have worked extensively to improve urgent care services in our area, this has included the roll out of the NHS 111 service and the commissioning of an urgent care centre in the ED at Queen Alexandra Hospital staffed by GPs. The next phase of this work will see us review the current models of Minor Injuries Units and Walk-in Centres to ensure these are aligned with and complement the services offered and re-commission services provided at the ‘front door’ of acute hospitals. This will involve the use of a primary care led integrated team linked to wider primary care services provided at scale and specialist outreach services. These arrangements will promote a ‘pull’ model of care and reduce admission. We have a proven track record in non-elective admissions, with a growth of just 3% at Portsmouth Hospitals NHS Trust (PHT) between 2007 and 2012. The admission rate for assessed patients with a high-risk condition (e.g. heart failure, respiratory disease, and dementia) is 20% compared to a national rate of around
Vision: 18/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�58�of�237Page�43�of�76
2 30%. We will build on this success through the use of seven-days-a-week rapid response teams, greater risk management and stratification in primary care, access to step-down and step-up beds, in-reach teams to support timely admission and discharge, and integrated community care teams. We shall provide active support to help people better manage long-term conditions tailored to individual circumstances. In addition, we wish to increase the use of ‘telehealth’, and ‘hear-and-treat’ services by 111 and SCAS. We have developed close working relationships with local stakeholders and communities and have active Community Engagement Committees running in both CCGs. In the next 18 months, we intend to step up our work with communities to co-produce local services with patients at the centre. For example in Whitehill and Bordon we will use this approach to take forward the redevelopment of Chase Community Hospital to ensure it meets the community’s needs. We also intend to use more sophisticated technologies to capture and act upon real time patient feedback. We will be developing a Quality Surveillance Hub to collate data from local quality monitoring, complaints, comments, surveys, patient stories, website feedback, and social media into a comprehensive, real time, database of information and evidence that will enable us to commission the services people want. ________________________________________________________________
Vision: 19/51:
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�59�of�237Page�44�of�76

3
Quality and outcomes We have developed a series of health ambitions that meet the expectations of our partners, both nationally and locally, and the demands of our communities. ________________________________________________________________
This section sets out where we are now and the main health challenges we face. It shows how the local health economy plans to meet both national and local ambitions for the NHS and the level of improvement expected. ________________________________________________________________
National imperatives The quality and outcome objectives of this strategy derive first from the demands of the NHS Mandate and the direction of travel set out in ‘Everyone Counts: Planning for Patients 2014/15 to 2018/19. They seek to secure locally a range of national health imperatives that have been summarised as seven health outcomes:
1. Securing additional years of life for the people of England with treatable mental and physical health conditions.
2. Improving the health related quality of life of the 15 million-plus people with one or more long-term condition, including mental health conditions.
3. Reducing the amount of time people spend avoidably in hospital through better and more integrated care in the community, outside of hospital.
4. Increasing the proportion of older people living independently at home following discharge from hospital.
5. Increasing the number of people having a positive experience of hospital care.
6. Increasing the number of people with mental and physical health conditions having a positive experience of care outside hospital, in general practice and in the community.
7. Making significant progress towards eliminating avoidable deaths in our hospitals caused by problems in care.
National guidance is also expecting to see significant focus and rapid improvement in three key areas:
1. improving health: working with all partners to address and manage everything that affects the broader determinants of health;
2. reducing health inequalities: ensuring that the most vulnerable in our society get better care and better services and an acceleration in improvement in their health outcomes; and
3. parity of esteem: focused on improving mental as well as physical health and eradicating disparity in such divisions of care.
Quality and outcomes: 20/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�60�of�237Page�45�of�76
3 We have been guided by these national requirements, informed them further with local intelligence and close partnership working, and developed strong, clinically driven and local derived solutions to the challenges they set. ________________________________________________________________
Local causes of ill health and death Wider determinants Whist many risks to health flow from the choices we make as individuals, many others are determined by social conditions and the effect they have on us. These include relative poverty, educational attainment and housing conditions. There are two areas of notable relative deprivation in the areas we serve, at Gosport and Havant. Geographical inequalities are reflected in the difference life expectancy between the least and most deprived 20% of the population in both CCG areas. South-East Hampshire CCG has the highest rates of childhood poverty in Hampshire, with 16.8% of 0-15 year olds living in relative poverty. This figure is 19.8% in Gosport and 9.1% in Fareham respectively. Low educational attainment can affect employment and other life opportunities and is associated with deprivation and high rates of teenage conception, which can be evidenced strongly in Havant and Gosport. Fourteen percent of households in South-East Hampshire and 12.9% in Fareham and Gosport were defined as one-person households, with the occupant being over 65 years-old. Income deprivation also affects a significant minority of other households. Individual risk factors Some risk factors affect people differently. These can be caused by lifestyle choices but some result from social conditions. Both CCGs have some of the lowest rates of breastfeeding take-up in the county but rates are particularly low in Havant. Gosport has the highest rates of childhood obesity in the county. However, rates are also higher in Havant than the Hampshire average. It is estimated that 38% of the adult population in Hampshire is overweight and 24% of the population is obese. The proportion of adults estimated to be smoking in Fareham, Gosport and Havant is higher than the Hampshire average. Around one-third of routine and manual workers smoke. Over 25% of people who drink alcohol consume more than the government recommended safe limits. Quality and outcomes: 21/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�61�of�237Page�46�of�76

3 Research has shown that risk factors tend to ‘cluster’ in the same populations, making some parts of the area particularly at risk of ill-health. Whilst there are significant numbers of people on chronic disease registers, it is estimated that many people remain undiagnosed. The main causes of premature death are: coronary heart disease (in 2012, there 120 deaths in Fareham & Gosport and 131 deaths in South-East Hants), respiratory disease (there were 54 deaths in Fareham and Gosport and 39 in South-East Hants during the same period) and cancer (where the figures were 54 deaths in Fareham & Gosport and 263 in South-East Hants). ________________________________________________________________
Working with colleagues to commission for prevention Priorities and common goals We have worked with the Health & Wellbeing Board to agree a series of priorities to tackle ill health and early death. These have helped shape the ambitions of this strategy and have set a series of required outcomes in health. They can be summarised as follows. HWB priority Suggested local priority How? Best start in life
Increase proportion of children breastfeeding.
Joint or joined up commissioning of services. Commissioning good quality maternity services and evidence based interventions in partnership with other agencies.
Decrease the proportion of children who are overweight and obese.
Fully engage primary care; e.g. provision of brief interventions. Work with partners to integrate prevention and treatment pathways for children.
Living well Tackle obesity and the causes of obesity.
Fully engaged primary care. Joined up prevention and treatment pathways. Interventions designed for the needs of the population. Provide leadership with other partners to tackle the wider determinants that cause obesity.
Reduce rates of smoking, especially in areas of deprivation.
Embed ‘stop before the op’ and other ‘teachable moments’ into acute contracting. Provide leadership with other partners to tackle the wider determinants that cause obesity.
Ageing well Embed self-help and prevention initiatives into primary care long-term conditions management.
Provide the opportunity for self-help management to all people with long-term conditions (LTCs). Ensure all people with LTCs
Quality and outcomes: 22/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�62�of�237Page�47�of�76

3
receive evidence-based advice/interventions to modify risk factors such as smoking and obesity. Ensure falls assessment and prevention is available to all who require it.
Improve the quality of LTC detection management, including dementia in primary care.
Commission and incentivise for case finding and quality across the pathway with a particular focus on Diabetes, COPD, CHD and cancer care.
Provide integrated assessment and support for people at higher risk of deterioration and hospital admission.
Develop Integrated Care Teams so people are identified, have a single assessment and receive joined up interventions.
Healthier communities
Develop coordinated action for provision of joined up health and other support in areas of greatest need for the antenatal and 0-5 period.
Provision of additional health resources in areas of greatest need with other health, statutory and voluntary sector providers.
Work with other agencies to tackle the causes of ill health and ensure health providers recognise and tackle these in individuals.
Active leadership in local multi-agency health and wellbeing partnerships, positively encourage links with voluntary and other providers of support such as education and training.
________________________________________________________________ Reducing inequalities We have also been guided by the five most cost effective interventions, as determined by the National Audit Office: • increased prescribing of drugs to control blood pressure; • increased prescribing of drugs to reduce cholesterol; • increase smoking cessation services; • increased anticoagulant therapy in atrial fibrillation, and • improved blood sugar control in diabetes. ________________________________________________________________ Improving health: a joint agenda The Health & Wellbeing strategy and the Joint Strategic Needs Assessment have helped us to determine, and are therefore closely aligned to, our ambitions for improved quality and health outcomes. We have also sought the views of our community and our clinical leaders during a three-month engagement programme.
Quality and outcomes: 23/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�63�of�237Page�48�of�76
3 These ambitions are: • People with conditions amenable to health care will have 14% more years of
life. • More than 75% of people with more than one long term condition will be
reporting that their quality of life has improved. • Emergency admissions will be reduced by 15% so that people spend less time
in hospital through better and integrated care in the community, outside hospital.
• More people will live independently at home following discharge from hospital. • Over 90% of people will have a positive experience of inpatient care. • Over 95% of people will be reporting a positive experience of care outside
hospital, in general practice and the community. • Avoidable deaths due to problems in hospital care will have reduced
________________________________________________________________ Parity of esteem Poor mental health is one of the biggest social issues in the UK today. The CCGs are part of the Hampshire joint commissioning mental health strategy which sets out priorities for mental health services in the county.
The vision is that good mental health and wellbeing will be supported by commissioning personalised services that meet the needs of all communities in Hampshire.
It is based on the four values of being in control of our lives:
• Reaching full potential • Equality • Justice and human rights • Valuing relationships
This will be achieved through:
• Personalisation • Recovery based services • Support for families and carers • Prevention and early intervention • Tackling stigma and discrimination • Developing a skilled workforce
Quality and outcomes: 24/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�64�of�237Page�49�of�76

3 In the development of our approach to commissioning personalised mental health services Fareham and Gosport CCG and South Eastern Hampshire CCG are particularly cognisant of the needs of:
Carers and families
Carers and families play an invaluable role in helping peoples recover and that they should be acknowledged, valued and supported. We recognise that they are central to the delivery of mental health care and many carers have developed high levels of expertise gained from years of experience.
Criminal justice
People in contact with criminal justice agencies, which may be caused by or lead to their mental health problems are likely to suffer extra discrimination. In particular for our area we will be identifying and meeting the needs of people with less acute mental health problems, learning difficulties and personality disorders in detention at the Immigration Removal Centre at Haslar.
Armed forces
We have a number of military bases within and close to our CCG areas and we want to ensure that armed forces personnel, families and veterans should not be disadvantaged because of their service. We recognise that early discharge personnel, those physically injured, personnel suffering post-traumatic stress, reservists and those being made redundant are more vulnerable to mental health conditions and are committed to ensuring that these individuals receive the right support.
Delivery
Over the next five years Fareham and Gosport CCG and South Eastern Hampshire CCG will commission improved services to better reflect the aspirations of people with mental health conditions and their carers.
In line with our overall approach to commission a truly integrated out of hospital services we expect mental health professionals and support services to be available within integrated community services, working alongside community services, general practitioners and voluntary sector partners with personlised care for individuals at the centre.
Our aim is that this approach will result in:
• a tiered model of delivery for adult mental health services in which all services understand their role within agreed pathways, have clear access criteria, provide evidence based models of care and can be accessed by a single point of contact for Hampshire residents;
Quality and outcomes: 25/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�65�of�237Page�50�of�76

3
• preventative services that are promoted through the diverse communities, improving access for all and enable people to remain resilient and as independent as possible in the community;
• improving psychological therapy services making sure all residents have access;
• a consistent approach to promoting recovery, tackle the stigma associated with mental health and supporting independence;
• mental health service users accessing main stream services that other members of the community access;
• only those whose needs cannot be met by the expanded community based support services progressing to highly specialised mental health services.
Some early programmes of work include:
• continuing to work with acute providers to evaluate and develop hospital liaison;
• undertaking a review of services for those experiencing a crisis; • developing improved rehabilitation services; • working with Hampshire County Council to improve diagnosis of, and
support for people with autism spectrum disorders; • evaluate and develop pathways for adults with ADHD.
We see the positive benefits of employment, housing and supportive relationships as equally significant for individuals with mental health support needs as for the general population and intend to use our new approach to integrated commissioning with partner agencies to ensure that support services are commissioned to support this approach.
All services that we commission will understand the requirements to safeguard children and adults and know how to take action when safeguarding issues arise.
________________________________________________________________ Compassion and the patient experience Central to this strategy is the desire to improve the patient experience and to minimise variation of this experience across different services. More integration of services will foster improved continuity of care, with team members delivering consistent messages, and we shall introduce quality of life measures across different care pathways. However, we shall continue to build on our reporting, survey and complaints systems to monitor change and identify improvements. We shall also look to develop greater public involvement and feedback in initiatives designed to improve the quality of care.
Quality and outcomes: 26/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�66�of�237Page�51�of�76

3 We will aim to increase the number of people who die in their place of choice and shall review and improve arrangements to ensure people receive not just the clinical help they need but also the compassion and dignity they deserve. Compassion in practice We will be seeking evidence of improvement and sustained change from commissioned services that demonstrate: care, compassion, competence, communication, courage and commitment. This will address: • leadership for compassion in care; • ensuring staffing levels and skill mix reflect caseloads and therefore ensure
levels are driven by safety needs; • staff engagement: ensuring staff are trained appropriately, motivated,
appraised, feel valued and able to contribute to improving care and provided with outcomes on the patient experience; and
• robust procedures for staff to raise concerns. ________________________________________________________________ Quality & safety We will aim to develop an approach to quality and safety that removes organisational barriers and puts the patient at centre of our decision-making. We shall foster a culture that is open, transparent and trusting, identifies the potential for failure before it occurs, embeds quality within our commissioning processes and prioritises efforts to improve quality and its assurance. We shall seek a partnership for quality with our providers and align our quality and safety priorities with them and our commissioning colleagues. This will promote the use of common data and intelligence as well as the introduction of good practice and shared initiatives. Contracts will contain new ways to gain effective assurance and payments will be linked to processes that support this new contracting approach. Clinical leadership will be strengthened and a clinical visits programme initiated. ________________________________________________________________ Staff satisfaction
We will be seeking evidence of improvement and sustained change from commissioned services as required by the National Care Strategy. This will cover the 6 Cs: care, compassion, competence, communication, courage and commitment. This will deliver improvements in leadership to bring compassion in care, safer staffing levels to ensure the skill mix reflects caseloads and is driven by safety needs, better staff engagement to ensure staff are trained and motivated to improve the patient experience and to feel valued, and more robust procedures for staff to raise concerns.
Quality and outcomes: 27/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�67�of�237Page�52�of�76
3 ______________________________________________________ Safeguarding Local standards in safety and safeguarding are high but we shall not take this for granted. Over the period of this strategy, we shall increase the reporting of risk and try to minimize any harm that may stem from a mismatch between the resources we have and the demands we face. We will try to reduce the capacity for any harm to be caused to any patient but will focus specifically on the frail elderly, other vulnerable adults and children.
Quality and outcomes: 28/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�68�of�237Page�53�of�76

4
Sustainability The CCGs have developed detailed financial plans to support the delivery of this strategy. These are based on national planning guidance (amended for local affordability) and allow for non-recurring investment to support the changes required for financial sustainability. More work will be required over the duration of the Strategy to cost particular initiatives and prioritise funding towards achieving the target outcomes. The plans are consistent with national planning guidance and contain broad assumptions about activity growth. Both CCGs have received a greater than average growth in allocations for 2014/15 and 2015/16. Our plans for improving quality, innovation, productivity and prevention for 2014 to 2016 are built using national and local benchmarking information and will focus on changing pathways to deliver both quality and the most effective use of resources. However because of their distance from the funding target, both CCGs will face unrealistically high QIPP challenges if they undertake their planning in line with the national requirement to deliver a surplus of 1% (compared to a 0.3% target in 2013/14) and if 2.5% of funding is set aside as headroom. Our Plans are, therefore, based on a 0.3% surplus and 1.5% headroom, giving rise to a more achievable QIPP challenge of about 3% for each organisation. It is assumed that the demographic challenges out lined in ‘A Call to Action’ will be addressed via the large-scale system change brought about by the Better Care Fund. South Eastern Hampshire
2014/15 £m
2015/16 £m
2016/17 £m
2017/18 £m
2018/19 £m
Allocation 220.4 230.2 238 242.2 246.5 Increase to allocation
6.7 6.2 4.2 4.2 4.3
Expenditure (232.7) (242.0) (247.3) (251.1) (254.8) QIPP 6.3 8.0 7.5 7.0 6.5 Surplus 0.7 2.4 2.4 2.4 2.5 Fareham and Gosport
2014/15 £m
2015/16 £m
2016/17 £m
2017/18 £m
2018/19 £m
Allocation 206.8 2.16.6 224.8 228.7 232.7 Increase to allocation
6.9 6.6 3.9 4.0 4.1
Expenditure (219.6) (230.0) (234.5) (237.6) (241.3) QIPP 6.5 9.0 8.1 7.4 7.0 Surplus 0.6 2.2 2.3 2.5 2.5 Sustainability: 29/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�69�of�237Page�54�of�76

4 Delivering this financial plan and strategy is dependent on large scale transformation in the health and social care system. We expect this to be delivered through new ways of contracting for the delivery of outcomes, quality metrics and reductions in the total cost of care for an assigned population of patients rather than block contracts for community based services, including mental health; and activity-based or day rate payments for much of secondary, residential and domiciliary care. The CCGs are working in partnership with the Local Authorities and Portsmouth CCG, drawing on the expertise of COBIC and Optum Health, to develop this new outcomes-based approach to commissioning. Central to developing a new outcomes-orientated approach to commissioning will be the development of the integrated information sources to create greater confidence for commissioners when negotiating contracts with provider partners. The CCGs have engaged Millimans, global health actuaries, to firstly integrate primary, community, secondary, prescribing and social care data and secondly to help us develop an actuarial perspective of our community’s needs. This is a critical foundation for outcomes based commissioning and our financial challenge. In addition to this new approach to contracting we intend to deliver our financial plan by maximising the economies of scale and efficiency that come from pooling our resources with other agencies commissioning health and care services for local people. Central to this is the creation of Locality Commissioning Hubs including health and social care commissioners. The CCG will also review its make / share / buy model to strengthen the shared infrastructure (e.g. finance, information, business intelligence, etc) with co-commissioners in the Local Authority. ________________________________________________________________
Sustainability: 30/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�70�of�237Page�55�of�76

5
Interventions We will act to secure our ambitions. This will involve a new partnership with the people we serve and a radical transformation of the health landscape.
________________________________________________________________
Sustainable, high quality, outcomes
This section describes the main interventions we will take or maintain to achieve the vision, objectives and quality outcomes we have set, within the financial resources available to us. This will involve a new partnership with the people we serve, a wider approach to primary care, more integrated services, quality improvements to urgent and emergency care, a step change in the productivity of elective care and improvements to specialised services. These will be supported by work to improve access, strengthen our commitment to the NHS constitution and generate improvements through research and innovation. ________________________________________________________________
A new approach to citizen involvement Health services that people want Our aim is to commission services that give people more choice and control over their health care so they can live full and independent lives. We have, therefore, signed up to ‘Think Local: Act Personal. Making it Real’ as this programme sets out what people who use services and carers expect to see and experience if support services are truly personalised. We will be tracking our progress in this area against "progress markers". These have been written by real people and families and will help us check how we transform care for local people. These markers focus on information and advice, active and supportive communities, flexible integrated care and support, feeling in control and safe, the support team, personal budgets, and self-funding. Putting the patient voice at the heart of decision-making Our ambition for the local NHS is to deliver treatment and care that always meets the needs and preferences of patients and service users. This means being flexible, responsive and efficient but, above all else, it means always listening to what our patients and service users tell us. We intend to supplement the insight gained from national surveys and the national Patient Insight Dashboard with a locally developed Quality Surveillance Hub. This tool will collate data from local quality monitoring, complaints, comments, surveys, patient stories, website feedback, and social media into a comprehensive, real time, database of information and evidence that will enable us to commission the services people want.
Interventions: 31/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�71�of�237Page�56�of�76

5 Insight from this Hub will enable us to understand how to improve the patient experience and drive better outcomes, enhanced patient safety and improved clinical effectiveness. Citizens fully involved
Fareham and Gosport and South Eastern Hampshire CCGs are committed to working with local communities to develop local services; and support patients and carers to take control of their own care and wellbeing.
Our five year strategy is to transform the way that local people participate in their own care and well-being and to involve local communities at every stage of commissioning services to improve outcomes.
This approach is fundamental to our ambitions to transform out of hospital care to be integrated and person-centred, to redesign our hospital and urgent care services based on patient insights.
Individual participation.
In 2012/13 63.5% patients in Fareham and Gosport and South Eastern Hampshire who have long term conditions reported they had enough support to manage their own condition. It is our ambition to increase this by 2019 by working with patients and their advocate groups to better understand what is needed to ensure that patients and carers are involved in decisions about their healthcare. We intend to work with fellow commissioners ensure accountable care organisations use a range of mechanisms to develop integrated personal care planning for patients with long term conditions, and, where appropriate, the option of a personal health budget.
Authentic citizen participation We have held a series of events and conversations with local people, GPs and stakeholders in the development of our five-year plan. We have also used an online survey to ask local people for their views. They have helped shape the priorities and ambitions set out in this document. In the next few months, we will refresh our Communications and Engagement strategy to articulate exactly how we will develop our approach to participation and embed this in our organisations’ business processes. Our aim is to ensure that our commissioning decisions are based on working with local communities and the people that use services to understanding the assets within local communities and collaborate to identify and solve problems together.
In order to do this we must work with other commissioning agencies as co-commissioners to involve the community at the earliest opportunity and maximise
Interventions: 32/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�72�of�237Page�57�of�76

5 opportunities and resources to engage people in a co-ordinated and joined up way, avoiding duplication.
In essence, this will include ongoing development of mechanisms already in place such as:
• the Community Engagement Committees, our Locality Participation Groups and each individual practice’s Patient Participation Group;
• website and social media; • online surveys; • community events; • attendance at a range of stakeholder groups; • patient surveys, interviews and feedback; • closer working with local authorities to tap into existing participation
mechanisms.
In addition, we intend to introduce new methodologies and approaches including:
• developing our Quality Surveillance Hub; • actively tracking our progress using the ‘Making It Real’ approach; • working to engage with groups and individuals across all nine protected
characteristics ( race, age, religion, sex, sexual orientation, marital status, pregnancy, gender reassignment and disability) in line with our duty under the Equality Act;
• introducing of new processes, to ensure participation of citizens and member practices occurs at the earliest opportunity;
• working with local authority colleagues to develop an asset based approach to participation in our most deprived communities.
Openness and transparency We will continue to develop our website as a portal for all information relating to participation in local service development and planning. Reports from our Quality Surveillance Hub will be available on the website, at the Community Engagement Community and at public Governing Body meetings. The minutes of the CEC are available at the public Governing Body and on the CCGs websites. We have a lay member for PPI (patient and public engagement) on both CCG Governing Bodies and co-opted members from all local councils. We actively participate in and report to the district and borough Health and Well Being Boards and are members of the Hampshire Health and Well Being Board. ________________________________________________________________ Interventions: 33/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�73�of�237Page�58�of�76

5 Wider primary care Providing care at scale We believe that the current model of primary care will need to change in the next five years. We know that most people still report high levels of satisfaction with their GP but too many remain dissatisfied with access to appointments and continuity of care. There are other, mounting, problems facing primary care too. We will see an increased demand for care from an ageing population and from those with long term conditions and, at the same time, we will continue to face problems recruiting general practice and primary care staff. We know that nationally there is likely to be an increase in the numbers of people needing help with complex health problems. The number of people with more than one long-term condition is estimated rise nationally by 3 million to 18 million patients by 2025. Nationally, the number of people with a long-term condition is expected to rise to 18 million by 2025. This will account for at least half of all GP appointments. We also know that we have an ageing population and expect to see a rise of 10%in the number of people aged over 75 in our area by 2019. We cannot therefore meet current and future demand for primary care services if we continue to do more of the same. Integrated wrap around services We’ve begun discussions with local primary care practitioners about how general practice teams of the future can work together with other practices and in a more integrated way with other primary, community and social care providers as federated or networked organisations. These organisations permit smaller teams and practices to retain their identity (through the association of localism, personal care, accessibility and familiarity) but combine ‘back-office’ functions, share organisational learning and co-develop integrated services that meet the needs of individual patients. It is our aim to work with NHS England to create an environment where practices in our area have a ‘wrap-around’ of dedicated community services, particularly for people with long-term conditions and for the frail elderly. This way of working would put the GP at the heart of a team of professionals with a range of skills such as community nursing, social care, physiotherapy, specialist nursing, occupational therapy and domiciliary care. It is our belief that the improved communication and partnership working in these teams would relieve some of the burden on primary care to ‘do it all’ by using a range of clinicians and optimising how professionals use their skills. In the next two years, we will be working with practices to help introduce this way of working across population groups of approximately 40,000, either by federating or merging. It is our ambition that federated or networked practices will work in partnership with other providers of community and adult social care to act as an NHS ‘provider’ for local communities. These groups or organisations will work together to provide extended services (such as those currently defined Interventions: 34/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�74�of�237Page�59�of�76

5 as ‘enhanced services’), as well as providing community nursing services and GPs with extended clinical roles. In 2014, we will begin the NHS Improving Quality programme to support practices and GPs in their development of this model. We will also use continuous development of Locally Commissioned Services between 2014 and 2019 to incentivise this way of working. We also expect to commission services from community providers that allow different providers to work in partnership or to develop ‘accountable care organisations’. Working with patients to improve quality We know that while most people still report high levels of satisfaction with the care they receive from their GP, 89% of SEH patients and 88% of F&G patients rate their overall experience with their GP surgery as good compared to 87% nationally, people report issues with access to appointments and continuity of care. GPs across our area are telling us that there is an increasing demand for primary care from an ageing population with increasing levels of long term conditions and this coupled with problems recruiting staff creates significant pressure on general practice. It is our aim that these larger groups of primary and community care providers will deploy more sophisticated methods of profiling their populations to ascertain their needs to gain better insight into their preferences. We want to ensure that these groups then use this information to work with patients and the community to co-produce services that allow local people to gain the support they need. By having a better understanding of the local population’s needs, primary care will be able to offer more effective ways of delivering services in line with demand, resulting in increased patient satisfaction. The Friends and Family Test will be a contractual obligation for primary care from 1st April 2014 and the CCG will expect patient satisfaction to increase by 2019. A different approach to appointments Simply increasing the quantity of face-to-face GP consultations alone will not be a cost-effective or sustainable strategy for achieving increased capacity and meeting growing demand, especially given the need to provide longer consultations to patients with more complex needs. The GP of the future will need to be skilled in using a suite of new and flexible tools for communicating with patients, including telephone, email and various online forms of consultation. This will include online group discussions, where appropriate (for example, for patients with long-term conditions) where peer-to-peer support and shared experience can be particularly valuable. Among younger people, the use of social media for interpersonal communication is almost ubiquitous. In 2012, around 95% of 16–20 year-olds and 74% of 20–25
Interventions: 35/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�75�of�237Page�60�of�76

5 year-olds used Facebook each month. To this generation, the traditional face-to-face consultation will no longer be accepted as the ‘default’ way to access care. Access to primary care services must, therefore, be redesigned to provide capacity in line with patients’ individual preferences for consultations and GP support. Our aim is to ensure that, within the next five years, local people have a range of different access points for primary and community health and care services that meet a variety of different needs and individual preferences. These might include a centre for continuity of care where the same GP is important to the patient, an access point for urgent care services available to a population of 40,000 or so, and different methods of access such as video conferencing, and online facilities. Alongside improved access to primary and community care provision, particularly for urgent care, we will review the current models of Minor Injuries Units and Walk-in Centres to ensure these are aligned with and complement the services offered in the new model of wider primary care available at scale. Shared information In line with our vision to truly integrate primary, community and social care, we are committed to ensuring that shared information and communication systems support and enable this transformation. IT and communications systems across a network of providers must have interoperability in order to share patient records and provide the best care for patients. We are already working towards this by encouraging practices to move to hosted systems. These support further encourage interoperability and increase resilience, security and reliability. These systems will need to offer benefit and advantage if they are to remain compatible with the notion of ‘GP systems of choice (GPSoC)’. Over the next five years, it is our aim to move towards one clinical system across primary care that is ‘interoperating’ with community provider systems. This doesn’t necessarily mean the same system but it will explore the ‘Medical Interoperability Gateway (MIG)’ as an option for interoperability. The workforce of the future The number of trainee GPs is well below the government’s target with a gap of nearly 3,000 GP trainee vacancies in 2013 according to the centre of workforce intelligence. There was a significant rise in the number of female and salaried GPs from 2001 to 2011 resulting in an increase in part time working and a reduction in partnership opportunities. Practices in South Eastern Hampshire and Fareham and Gosport CCGs are reporting difficulty in recruiting new partners and salaried GPs. We will, therefore, support and develop processes that support flexible and more attractive working arrangements, widen the entry gate into general practice and recruit and retain staff more effectively. Interventions: 36/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�76�of�237Page�61�of�76

5 A role for CCGs in commissioning primary care An alternative or intermediate approach to a new contract for primary care is for CCGs to be given a mandate to commission additional services from general practice (over and above core general and primary medical services) and other care providers. This would be another way of encouraging the formation and extension of primary care federations and networks, with groups of practices bidding to provide services in accordance with the design principles proposed here. We are well placed to work closely with patients and the public to design new forms of service provision that can assure accessible and high quality primary care and advice. There is a need for further clarification by NHS England as to the precise nature of our involvement in developing, commissioning and assuring the quality of primary care, but we expect to act as co-commissioners for many primary care services. ________________________________________________________________ A model of integrated care A partnership to reduce illness and improve quality Together with our colleague commissioners across health, public health and social care, we continue to learn and develop a stronger understanding of how to support people to maximise their independence. We recognise that many factors influence mortality and morbidity but believe our plans for integration can make a crucial contribution to improving health. For 2014/15 to 2015/16, we would expect integration to contribute, in the longer term, to reducing premature and total mortality from the major causes of death and the difference in life expectancy between people living in the least and most deprived areas. We expect integration too to have a direct impact on improving health related quality of life for people with long-term conditions. Focused interventions We will develop interventions that maintain a constant focus on the long-term quality of care and the achievement of outcomes for users. We shall ensure that fairness and equality in the broader context underpins every decision that we make and give service users and their family’s choice and control over their outcomes. An increase in self-sufficiency and independence lies at the heat of our endeavours and we will aim to reduce unnecessary reliance on services where possible whilst protecting the sustainability of services to meet current and future demographic, financial and statutory constraints,
Interventions: 37/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�77�of�237Page�62�of�76

5 System wide change We have already aligned our priorities with colleague commissioners to support system wide changes. This is helping us to implement the Hampshire Dementia Strategy, enable the development of integrated care, develop enhanced clinical skills and new roles within community services, and begin to make the workforce changes needed to bring about the transformation at scale that is needed across all sectors. This will support work to commission arrangements that focus on primary prevention and early intervention, supported self-care, predictive monitoring, improved ambulatory managing, care co-ordination and case management, admission avoidance, rapid response and effective discharge planning, specialist mental health input and end of life care, and better intermediate care, rehabilitation recovery and re-ablement support. ________________________________________________________________ Urgent and emergency care of high quality Realigning urgent care Currently, our ambition to deliver services that support early intervention and maximise independence does not align with existing arrangements for the provision of urgent and emergency care. We believe we need to see a fundamental shift in the way urgent care is provided. This means services will need to change both what they do and from where they are available. This will support interventions that are coordinated around individual need and delivered as close as possible to people’s homes. At the same time, we must continue to ensure that people with more serious or life-threatening emergency needs are treated in centres with the very best expertise and facilities to maximise their chance of survival and good recovery. To be successful, we will need to invest in primary, community and social care services, and shift some acute hospital based planned activities to safe, alternative community based services. This will require a transformation in the way urgent care is delivered and the creation of highly integrated approaches to service delivery. We will re-commission services provided at the ‘front door’ of acute hospitals. This will involve the use of a primary care led integrated team linked to wider primary care services provided at scale and specialist outreach services. These arrangements will promote a ‘pull’ model of care and reduce admission, a step change in the productivity of elective care and the shifting of some services, such as chemotherapy, to community settings. Interventions: 38/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�78�of�237Page�63�of�76

5 An integrated approach Delivering an integrated approach to urgent and emergency care, and particularly medical admissions, requires joint working between hospitals, community, primary and ambulance services. Urgent care services are often highly fragmented with different entry points, and this generates confusion among patients about how and where to access care. Patients are frequently admitted to hospital or attend ED when its not necessarily clinically justified, often because of a lack of alternative options. Managing increasing demand Demand for urgent and emergency keeps increasing despite the growth in new forms of urgent care, such as walk in and urgent care centres. ED attendances across England grew by 30% between 2003/4 and 2011/12 (department of health 2011a). New forms of urgent care have also failed to reduce emergency admissions, which have continued to grow and rose by 5% between 2008/9 and 2011/12 (Department of Health 2011d;2012). We believe that addressing poor practice, improving continuity of care and reducing the numbers admitted to hospital are likely to have a significant impact on health outcomes. It would also improve the patient experience by making the urgent care system easier to navigate. It is also our view that the integration of urgent and emergency care services will help manage demand more effectively and be more cost effective than existing arrangements. Providers in the South of England experienced a growth in emergency admissions between June 2008 and June 2012 of up to 9%. As has been the case for a number of years, this is significantly in excess of the rate that can be explained by population changes alone (Kings Fund). Between September 2011 and August 2012, there was an average of 250,000 A&E attendances and 100,000 emergency admissions. However, there are significant variations in performance between providers (September 2011 an August 2012:
• Emergency length of stay - 4.8 days average • Readmission: average 13.8% • A&E conversion rate: average 22%, range: 14-46% • A&E patients arriving by ambulance: average 28%, range: 11-39% • 95% in four hours: average: 93.5%, 67 to 97%, and • Discharge to nursing homes and other important variable show similarly
wide variation. Areas where we are strong Locally, we are performing well on a number of indicators. Non-elective
Interventions: 39/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�79�of�237Page�64�of�76

5 admissions at Portsmouth Hospitals NHS Trust (PHT) grew by just 3% between 2007 and 2012. In addition, for 2013/14 they are currently 3.8% lower than last year (against growth nationally 0.5%).
The average emergency length of stay for 2011/12 was 4.4 days. Half went home in one day and around 15% stayed longer than seven days. The ED conversion rate was just 18%, with 30.2% arriving by ambulance. Some 8.8% of emergency patients were discharged to a nursing home compared with the south of England average of 1.6%The admission rate for assessed patients with a high risk condition (e.g. heart failure, respiratory disease, and dementia) is 20% compared to a national rate of around 30%. Our service outcomes and challenges Whilst we are performing well in a number of areas, we face the following challenges: • poor performance in meeting the Emergency Department four hour waiting
target • public remain unclear about what services to best access and when • the urgent care pathway is fragmented, with differing performance and
response times • we do not have a seven days a week service for all services out of hospital.
Overall strategic aim The overall strategic aim of the urgent and emergency care strategy is to deliver care in the right place at the right time, first time and to manage and meet demand as required. To achieve this, we want to ensure that we have a robust: urgent care pathway with greater emphasis on self-management and case management in primary and community care, and emergency pathway The outcomes of the changes will see a reduction in ED attendances and inappropriate emergency admissions Our ambitions We want to ensure that there is rapid assessment and treatment of emergency patients in ED and timely inpatient care. Level 4. Emergency care: We want to review the urgent care model and look to develop a more integrated model of delivery. As a first step, we will introduce an urgent care centre located in ED to ensure patients are triaged to the most appropriate place of care for their needs and only those who require an accident and emergency service will be treated within ED.
Interventions: 40/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�80�of�237Page�65�of�76

5 Level 3. Urgent care: There will be a single ‘front door’ at PHT for all walk-in patients requiring urgent care. These patients will be part of a single integrated administration and triage process and will be signposted to the most appropriate service for them. For many, this may be treatment with the GP within the urgent care center. In other cases this mean a redirection towards their local GP or community services or advice on self-care. Level 2. Out of hospital care: We shall support an increase in the non-conveyance of patients to ED by the ambulance service. This will involve the use of seven-days-a-week rapid response teams, greater risk management and stratification in primary care, access to step-down and step-up beds, in-reach teams to support timely admission and discharge, and integrated community care teams. Level 1. Self-care: We shall provide active support to help people better manage long-term conditions tailored to individual conditions. In addition, we wish to increase the use of ‘telehealth’, and ‘hear-and-treat’ services by 111 and SCAS. Our priorities In delivering high quality urgent and emergency care, the Urgent and Emergency Care Board has agreed an action plan to improve our service challenges, meet the needs of our population and deliver the service model set out above. Our key themes for recovery and improvement are:
Interventions: 41/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�81�of�237Page�66�of�76

5
________________________________________________________________ Improving elective care Our services offer good access to planned or elective care and general practice is of excellent quality and well regarded. Patients are able to choose from a range of good provider organisations, with each offering short waiting times and good outcomes. We still need to make further improvements. The use of emergency care remains high, particularly in areas of relative deprivation, and reliance on planned care services is too low. We want more people to access planned care in a timely way and to support these communities to engage with health and care at an earlier stage. The demand for planned care is rising, unsustainably. Hospitals are increasingly facing capacity challenges even though, in some instances, a proportion of these referrals will not add any value to the patient. To tackle these problems we will build on the successful redesign of the Portsmouth and South East Hampshire diabetes service to expand the community-facing delivery model in a number of associated specialties, including:
• Repeat Pain Procedures • BNP Testing • Ophthalmology
Urgent and emergency
activity
Improving care and
patient flow in ED/hospital
Improving system
access and response for patients in a
crisis
Approprate flow for patient
leaving the hospital
Alternatives to emergency
admissionm - management
of ACS condition
Improving mangement of end of life
management of Integrated urgent care provision across all providers
Interventions: 42/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�82�of�237Page�67�of�76

5
• Dermatology • Orthopaedics/MSK • Hepatology
We want to help clinicians currently operating in these specialties to have a stronger advisory and population management role, work with integrated care teams and support GPs in the local management of patients. We have commissioned new service arrangements for ophthalmology and orthopaedics and intend to explore with provider colleagues how best to move arrangements from a system that pays by results to one where other results are better acknowledged. This will mean we are commissioning for improved patient reported outcomes rather than simply activity. We will also review the role and use of diagnostics in the way in which we deliver care. We will explore greater primary care access to diagnostics, accelerating diagnosis and hence treatment. We will also explore developing the current model of diagnostic delivery, encouraging greater partnerships between existing provider organisations to strengthen quality access and reduce costs. ________________________________________________________________ Better specialised services Fareham and Gosport and South Eastern Hampshire CCGs are committed to ensuring that all local services, whether they be ‘regular’ or specialised, meet the highest standards and deliver the best outcomes for patients. We welcome the development of unified or converged single national service specifications for specialised services and are committed to working alongside NHS England’s Wessex Area Team to provide local knowledge and expertise on services and providers that will ensure that these standards are met. We believe our local intelligence will be crucial to ensuring integration across the patient pathway at a local level and to ensuring local people can access specialized services in the most appropriate setting. ________________________________________________________________ Improvement through innovation and research The vision is for Portsmouth, Fareham & Gosport and South Eastern Hampshire CCGs (PSEH CCGs) to work together to put innovation at the heart of all our activities so that innovation drives continuous improvement and ensures that patients receive the highest standard of care.
Interventions: 43/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�83�of�237Page�68�of�76

5 Aim
To champion innovation, evidence-based practice and the adoption of research and innovative approaches to improve the quality of health services across PSEH CCGs.
Objectives
1. Continue to implement a process to support innovation: we will establish a process that enables innovation to be at the heart of all our commissioning activities. The process will outline clear mechanisms to support the generation, assessment, approval and delivery of innovation to ensure resources are used in the most efficient and effective manner.
2. Support and encourage innovation within all our commissioned services by:
• Applying the right incentives to encourage the systematic development of innovative behaviours and activity, and by directing investment, to help spread new ideas (such as the application of CQUIN incentives).
• Encourage participation in NHS Innovation Challenge Prize and other initiatives that support and reward innovation.
• Work closely with providers to support the development of innovative ideas, products, services and clinical practice.
3. Build and maintain links with research and innovation networks: vital to the innovation agenda is networking to share ideas, best practice, expertise, research, knowledge and skills. The three CCGs will actively participate, build and maintain links with the following networks:
• The Wessex Academic Health Science Network (AHSN) to support the identification, adoption and spread of innovative healthcare across the network.
• The National Institute for Health Research (NIHR) • NHS Benchmarking Network • NHS Improving Quality (NHSIQ) • Other networks as appropriate
4. Ensure innovations supports the delivery of Quality, Innovation,
Productivity and Prevention (QIPP) within financial resources by promoting innovation and sharing best practice in commissioning, clinical practice and models of service delivery:
• Encourage local development and innovation through pathways and work stream developments
Interventions: 44/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�84�of�237Page�69�of�76

5
• Publishing local development and innovation through pathways and work stream developments
• Publishing and sharing of examples of local best practice • Provide inclusive access to evidence and best practice to support
development of innovative healthcare services across the CCGs
5. Develop a culture of innovation throughout the three CCGs: • Evidence suggests that organisations which are able to innovate
successfully have developed a culture of innovation throughout their organisation, and at all levels.
• provide space, time and resources for individuals to generate and pursue innovative ideas they are passionate about;
• actively support and facilitate the generation of new ideas and the uptake of ideas, practices and processes that have been generated externally or elsewhere in the system
• establish mechanisms to quickly form small, flexible teams with the necessary skill sets to refine and drive innovative ideas from conception to implementation
• utilise partnerships and collaboration to encourage and support ‘radical innovation’ while simultaneously assessing and managing associated inherent risk
• Nominate a clinical lead and governing body member to champion the innovation agenda
6. Continue the local adoption of NHS high impact innovations: through the
national CQUIN mechanisms.
7. Ensure all NICE Technology Appraisal recommendations are incorporated into relevant local NHS formularies in a planned way that supports safe and clinically appropriate practice.
________________________________________________________________
Interventions: 45/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�85�of�237Page�70�of�76

6
Governance Excellent and accountable decision-making, led by GPs and driven by patients and the community. ________________________________________________________________ This section describes the work already in place to ensure the highest standards of probity and decision-making and the efforts that will be made in the coming years to improve accountability and clinical leadership. ________________________________________________________________ Building on firm foundations Each CCG has established distinct and independent arrangements to secure the participation locally of GPs and other health professionals in the management of NHS commissioning business. These provide the CCGs with expert clinical leadership that not only understands the needs of local patients but which is also sensitive to the demands of the area as a whole. Each governing body is made up of six local GPs, five officers, two lay members and a secondary care consultant. However, the CCGs have also set up shared administrative and support services to allow each to reduce costs and introduce significant economies of scale. The CCGs share an Executive Director and management team, have joint support staff and, where appropriate, have common administrative processes. These are helping to contain costs, share expertise, maintain standards and implement good practice more widely. The arrangements are designed to ensure the maximum possible scrutiny and probity of management processes. They also place the patient at the heart of the CCGs’ business. ________________________________________________________________ Governance structures A governance structure has been put in place that secures local clinical leadership and accountability whilst maximising opportunities for efficiency and joint working. Each CCG board responds to its membership via separate clinical assembly and clinical discussion forum arrangements. However, each is served by joint quality assurance, governance, audit and remuneration committees and a joint Clinical Cabinet The arrangements allow for effective joint working with the Hampshire Health & Wellbeing Board, and with NHS colleagues via the Hampshire Commissioning Group and the Portsmouth and south east Hampshire Commissioning Collaborative.
Governance: 46/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�86�of�237Page�71�of�76

6
________________________________________________________________ Accountability to our communities The Clinical Commissioning Groups (CCGs) have two community engagement committees (CECs), which are sub-committees of the governing body. The committee’s comprise a range of local stakeholders, together with representatives from local patient participation groups. The committees also have wider networks into community and voluntary groups throughout our area. These Committees and their wider networks are one of the main mechanisms used to ensure that future plans are developed with key stakeholders and the local community. In addition, all future plans are measured against a standard template at the Planning Executive Group, (PEG), a sub-committee of the clinical cabinet. One of the key criteria in the standard template is to ensure that key stakeholders have been engaged and are collaborating with commissioners to assist with the design of the commissioning plan. Once the standard template’s key criteria have been considered and approved at the PEG, the plan is then forwarded to the clinical cabinet for clinical discussion and approval prior to ratification at the governing body. Our on-going organisational development programme includes further strengthening of the role and function of the CECs to ensure that they are involved in, and shape, all commissioning activity and service development work and that each committee is provided with adequate assurance that patient and public participation has taken place. This work will also include on-going development of a range of mechanisms to capture and consider patient and public insight and ensure that commissioners put the patient and public voice at the heart of their plans. This will involve strengthening the process by which our commissioning plans are Governance: 47/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�87�of�237Page�72�of�76

6 scrutinised by the PEG and CECs for evidence of patient and public input to the proposals. Public seminars on subjects associated with future plans are held before each public governing body meeting. These seminars offer another opportunity for commissioners to engage members of the public and other public interest groups and to garner their views and interact with governing body members. ________________________________________________________________ You said, we did. We are already gathering feedback from a range of sources and using this to shape decisions and plans. Feedback comes from: • Website – specific page dedicated to ‘You said we did’ • Practice Information Portal (for clinical staff) • GP and practice engagement events • Public Governing Body seminars • Community Engagement Committees • Regular stakeholder events • On-line surveys • Twitter • Regular engagement activity and attendance at community groups • Practice Patient Participation Groups and locality Patient Participation
Groups • Comments on NHS Choices and other websites • Complaints, comments and compliments • Provider trust surveys, including the Friends and Family Test • Primary care surveys
The challenge of the next five years is to strengthen arrangements to foster local and accountable decision-making whilst securing further and emerging opportunities for joint working, efficient management, and the pooling of resources. A detailed log of all engagement activity undertaken and the key themes given in feedback received is considered by the Community Engagement Committees regularly and used to inform commissioning plans. The public Governing Body meetings receive regular reports on complaints, provider feedback and engagement activity and feedback and any actions taken in response to feedback. In the next two years the CCGs are planning to commission a new tool to enable the systematic collection and analysis of a range of feedback to inform future commissioning and to enable closer monitoring, and early warning of quality issues in provider organisations. Over the next five years we expect this tool to be a key enabler in developing a
Governance: 48/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�88�of�237Page�73�of�76

6 more sophisticated and real time methodology to monitor feedback and act upon it. We will be using our website and Twitter to feedback to our communities as well as other more traditional methods such as public reports and attendance at stakeholder meetings. ________________________________________________________________ Strengthening joint working We have pursued initiatives designed to help us operate at scale and to deliver greater efficiency. The two CCGs share a management team, which brings increased co-operation and sharing of good practice among clinical leaders. We also have a ‘compact’ with neighbouring Portsmouth CCG to realise economies of scale and to act as a single commissioning entity when dealing with local providers. For the future, we plan to develop these relationships with local authority partners in order to maximise opportunities for collaboration. Our clinical leaders will be further developed too to help them work effectively with arrangements that bring collaborative commissioning and also new models of service provision. Common purpose and common infrastructure. In order to strengthen joint commissioning arrangements, both CCGs will work with local authority partners to co-locate commissioning teams. This will enable the creation of Locality Commissioning Hubs including Health commissioners The CCG will also review its make / share / buy model to strengthen the shared infrastructure (e.g. finance, information, business intelligence, etc) with co-commissioners in the Local Authority. Building strong partnerships. The CCGs will be developing locality specific strategies where these are relevant, necessary and add value. For example, the CCG will be working with Hampshire County Council, Havant Borough Council, the Police and Crime Commissioner and other partner agencies to develop an ambitious strategy to combine resources and physical assets across Leigh Park to benefit this more deprived population. A similar approach will be developed for Rowner in Gosport.
Governance: 49/51
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�89�of�237Page�74�of�76

7
Values We will be judged by how we do business, as we believe the ambitions and aspirations of this strategy are a reflection of our values and principles. ________________________________________________________________
What we believe We believe that trust is hard earned and easily lost, that nothing we do which affects others should be decided with their involvement and that by working together we can bring about improvements in health. This means that we will seek to be an organisation that acts with integrity, trust, respect, and honesty. These behaviours will be guided by rationalism and objectivity and by openness and transparency. Our belief in partnerships will drive us to be inclusive and to seek out and value the opinions and wishes of our patients, communities and colleagues. ________________________________________________________________ Our commissioning principles We will follow a series of key principles during the period of this strategy to guide the way we do business. These principles affect everything we do and reflect our determination to seek the right values and behaviours not just in our own endeavours but also throughout the commissioning process as a whole. ________________________________________________________________ How we will do business We will be guided by our partnerships with fellow commissioners and NHS colleagues, constituent practices and our local communities. This will enable us to retain our focus on the delivery of high quality care to our local population while introducing new ways to ensure continuity of care and improved patient experience. We will commission services with patient outcomes and quality of service as our primary concern. In particular we believe people should have access to care on the basis of need without discrimination. We will seek to make decisions that promote the health of the entire community and which support the public health agenda. Some patients and communities may be given priority over others in order to address health inequalities We believe that patients will receive higher quality care with better outcomes and an improved overall experience if we can provide integrated care closer to people’s homes.
Values: 50/51: 14/03/2014
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�90�of�237Page�75�of�76

7 We want to innovate and look for new ways to deliver better care at a reduced cost. We will commission services in a way that represents the best value for money without compromising quality or patient outcomes. We will obtain evidence to assess clinical and cost effectiveness to support our commissioning or inform changes in the way we do this. We will seek to reduce costs where possible to remain a sustainable organisation.
Values: 51/51: 14/03/2014
7�Five�Year�Strategy�and�Two�Y
Top
Overall�Page�91�of�237Page�76�of�76

GOVERNING BODY Date of Meeting 19th March 2014
Agenda Item No
8 Title
Draft Financial Plans 2014/15 – 2018/19 Purpose of Paper
To inform the Governing Body of the current financial modelling for the short (2014/15 to 2015/16 – two year) and medium term (through to 2018/19 (5 Years)) plans;
Recommendations/ Actions requested
The Governing Body is asked to: • Agree the draft Financial Plans • Agree the level of investment, reserves and contingency • Agree the QIPP challenge of £7.4m (14/15) & £8.5m (15/16) • Note that the plan is dependent on contract discussions and
any further national guidance • Note the Risks and mitigating actions • Agree these high level financial programmes which will be
used to set budgets in 2014/15
Author
David Bailey Deputy Chief Finance Officer
Sponsoring member
Andy Wood Chief Finance Officer
Date
12th March 2014
8�Draft�Financial�Plans.pdf
Top
Overall�Page�92�of�237Page�1�of�11

Draft Financial Plans
2014/15 to 2018/19
8�Draft�Financial�Plans.pdf
Top
Overall�Page�93�of�237Page�2�of�11

Contents
1. Introduction 2. Context
3. Key Principles
4. Summary Financial Model 5. Detailed Assumptions
6. Investments and Contingency
7. Key Risks and Mitigation
8. Recommendations
8�Draft�Financial�Plans.pdf
Top
Overall�Page�94�of�237Page�3�of�11

Introduction
• This presents the Draft Financial Plans for 2014/15 & 2015/16
• Covers short and medium term plans
• CCG Allocations (2 years) announced December 2013
• Based on “Everyone Counts” Planning for Patients 2014/15 to 2018/19 guidance
8�Draft�Financial�Plans.pdf
Top
Overall�Page�95�of�237Page�4�of�11

Context
• Local Health System – financially challenged (S E H CCG has the 16th biggest distance from fair shares in funding of all 211 CCG’s)
• Encouraging integrated working across all partner organisations
• COMPACT agreement with Portsmouth and Fareham & Gosport CCGs and risk sharing where appropriate
• Running costs well within threshold but challenge of 10% reduction in 15/16
• Impact of Better Care Fund • Looking at new ways of contracting to incentivise system change
8�Draft�Financial�Plans.pdf
Top
Overall�Page�96�of�237Page�5�of�11

Key Principles
• Allocation published nationally (covers 2 financial years and signals above
average increases beyond 2015/16) • Existing recurring expenditure continues • Surplus returned (non recurring) each year • Target is the achievement of a 1% surplus per year – we only achieved 0.3% in
13/14 and are planning the same in 14/15 • Set aside 0.5% contingency • Set aside non recurrent expenditure (supposed to be 2.5% 14/15 and 1%
thereafter) – we can only afford 1.5% locally in 14/15 • Includes expected tariff efficiency to be delivered by providers • Sets aside inflation costs • Very little investment funding for national priorities and in support of QIPP – May
need more than the available headroom if we are to pump prime real change • Addresses running cost requirements (including 10% reduction in 2015/16) • CQUIN at 2.5% - some of which may form part of the ‘Risk & Reward
Mechanism’ • Population 209,845, which gives a running cost per head of £22
8�Draft�Financial�Plans.pdf
Top
Overall�Page�97�of�237Page�6�of�11

Summary Financial Model Summary Financial Model 2014/15 2015/16 2016/17 2017/18 2018/19
£m £m £m £m £m Resources: Recurrent baseline allocation 210.3 221.5 231.2 235.4 239.6 Growth 6.7 6.2 4.2 4.2 4.3 Running Costs allocation 5.0 4.5 4.5 4.5 4.5 Changes to Baseline Allocations 4.5 0.0 0.0 0.0 0.0 BCF 0.0 3.5 0.0 0.0 0.0 Surplus repayment 0.6 0.7 2.4 2.4 2.5
Total Resources 227.1 236.4 242.2 246.5 250.8
Expenditure: Opening recurrent baseline expenditure 224.6 222.8 227.0 230.5 234.0 Investments 0.0 0.0 0.0 0.0 0.0 Inflationary pressures 7.7 8.1 8.9 9.2 9.5 Population & demand 2.9 2.9 3.0 3.0 3.0 CQUINS - - - - - QIPP Investments 0.6 - - - - Headroom 3.3 2.3 2.4 2.4 2.4 Transformation - - - - - BCF - 11.6 11.6 11.6 11.6 Contingency 1.1 1.2 1.2 1.2 1.2
Total Expenditure 240.3 248.8 254.1 257.9 261.8
Challenge (Resources less Expenditure) -13.2 -12.5 -11.9 -11.4 -10.9 Savings: Efficiency (passed onto providers) 6.5 6.3 6.4 6.4 6.4 QIPP Target, of which; 7.4 8.5 7.9 7.5 7.0 QIPP Prescribing 1.7 1.6 1.6 1.6 1.6 QIPP Savings Identified 3.8 0.0 0.0 0.0 0.0 QIPP Savings Unidentified 1.9 6.9 6.3 5.9 5.4 Total Savings 13.9 14.8 14.3 13.8 13.4
Surplus 0.7 2.4 2.4 2.4 2.58�Draft�Financial�Plans.pdf
Top
Overall�Page�98�of�237Page�7�of�11

Detailed Assumptions CCG Allocation
2014-15 2014-15 2015-16 2016-17 2017-18 2018-19
Programme Allocations Growth 3.1% 2.8% 1.8% 1.7% 1.7%
Admin Allocations Growth 0.0% -10.0% 0.0% 0.0% 0.0%
Provider Portfolio & tariff 2014-15 2015-16 2016-17 2017-18 2018-19 Inflation Efficiency Inflation Efficiency Inflation Efficiency Inflation Efficiency Inflation Efficiency Acute 2.5% -4.0% 2.8% -4.0% 3.0% -4.0% 3.4% -4.0% 3.4% -4.0% Prescribing 9.0% -5.0% 9.0% -5.0% 9.0% -5.0% 9.0% -5.0% 9.0% -5.0% Continuing Health Care 5.5% -3.0% 5.5% -3.0% 5.5% -3.0% 5.5% -3.0% 5.5% -3.0% Community & Mental Health 2.2% -4.0% 2.2% -4.0% 3.0% -4.0% 3.4% -4.0% 3.4% -4.0% Commissioning Support Unit 2.0% -4.0% 2.0% -4.0% 2.0% -3.1% 2.0% -3.1% 2.0% -3.1%
Healthcare Area2014/15
Total
Acute Care 120,182,262 Community 21,625,337 Continuing Care 14,316,520 Corporate 4,542,700 Mental Health 20,217,372 Other 1,073,184 Primary Care 36,187,944 Reserves 8,323,165
Total Resources 226,468,484
8�Draft�Financial�Plans.pdf
Top
Overall�Page�99�of�237Page�8�of�11

Investment and Contingency
Summary Investment & Contingency 2014/15 2015/16 2016/17 2017/18 2018/19 £m £m £m £m £m
Population & demand 2.9 2.9 3.0 3.0 3.0 Non Recurrent Expenditure 3.3 2.3 2.4 2.4 2.4 QIPP Investment 0.6 Contingency 1.1 1.2 1.2 1.2 1.2
• Investment funding and contingency set aside to cover all known developments and ‘Everyone Counts’ guidance, including the £5 per head of Practice Population stipulated in the planning guidance
• £500k increase in investment in locally commissioned schemes with Primary Care
• Will develop a Risk & Reward Mechanism (utilising headroom, CQUIN etc.) to pump prime some change
• Quality premium to invest non-recurringly
8�Draft�Financial�Plans.pdf
Top
Overall�Page�100�of�237Page�9�of�11

Key Risks and Mitigation Risks Mitigating Action RAG
rating May need to enter deficit so we have enough to invest in pump priming real service change and sustainability
Agree 5 year financial programme with return to surplus over a 2 -3 year period
Size of QIPP challenge & pace of change Robust monitoring to ensure QIPP on target. Use of 1.5% non recurring fund to support system reconfiguration. Contingency will provide further risk mitigation if necessary.
Costs of meeting NHS Constitution obligations higher than estimates: significant gap in acute contracts
Review through planning governance framework and consider use of contingency and other non recurrent resources. Work with PHT to agree elective plan, especially regarding RTT requirements.
Better Care Fund is used to plug gaps in Social Care funding rather than drive service change
Engagement in the Health & Wellbeing Board and drive development of integrated teams locally
Growth and Cost Pressures – increase beyond existing assumptions
Close scrutiny of contract monitoring and regular contract reviews will highlight areas of concern and address any issues that emerge.
Changes to contracts to move toward outcome based (rather than block or PbR style contracts)
CCG will work closely with providers and contracts team to review likely impact and address any issues as they arise.
CCG allocation published but some legacy risks e.g. a potential Continuing Health Care (CHC) provision required of £250m nationally for all CCG’s to share
CCG will work closely with NHS England and the Wessex Area Team to understand any future guidance and highlight specific issues for the CCG.
Legacy Financial Position of the South East Hampshire system remains challenging
Continue to work with neighbouring CCGs and local providers to ensure health system continues to recover any underlying issues. COMPACT with Fareham & Gosport and Portsmouth CCG’s. Change in contracting approaches to incentivise change.
Quality Premium milestones not achieved Milestones to be monitored and actions taken to rectify as necessary. Investment against allocation to be non recurring.
8�Draft�Financial�Plans.pdf
Top
Overall�Page�101�of�237Page�10�of�11

Recommendations
• Governing Body is requested to: – Agree the draft Financial Plans noting that it follows Everyone
Counts guidance except for: • Only 1.5% held for non recurrent spend in 14/15 rather than the suggested
business rule of 2.5% • Only 0.3% surplus planned in 14/15 rather than the suggested business rule of
1%
– Agree the level of investment and contingency – Note very few reserves available – Agree the QIPP challenge of £7.4m (14/15) & £8.5m (15/16) – Note the above is dependent on contract discussions and any
further national guidance – Note the Risks and mitigating actions
8�Draft�Financial�Plans.pdf
Top
Overall�Page�102�of�237Page�11�of�11

GOVERNING BODY Date of Meeting 19th March 2014
Agenda Item No
9 Title
Better Care Fund Purpose of Paper
To update the Governing Body on the progress of the implementation of the Better Care Fund.
Recommendations/ Actions requested
The Governing Body is asked to:
• note the progress to date • note the draft plan submitted in February 2014
Author
Gill Duncan Director of Adult Services Hampshire County Council
Sponsoring member
Alex Berry Chief Commissioning Officer
Date
10 March 2014
9�Better�Care�Fund.pdf
Top
Overall�Page�103�of�237Page�1�of�9

Agenda item: 5
HAMPSHIRE COUNTY COUNCIL
Decision Report
Decision Maker: Hampshire Health and Wellbeing Board
Date: 11 February 2014
Title: Better Care Fund
Reference: 5620
Report From: Chair NHS North Hampshire CCG Director Adult Services, Hampshire County Council
Contact name: Karen Ashton – Strategic Commissioning Director
Tel: 01962 847226 Email: [email protected]
1. Summary 1.1. The Better Care Fund (BCF) (previously referred to as the Integration
Transformation Fund) provides an opportunity to transform local services pace so that people are provided with better integrated care and support in a way that manages pressures and improves long term sustainability of the health and social care system.
1.2. The Hampshire Health and Wellbeing Board chaired by a Council Cabinet Member and Deputy Chair being the Clinical Chair of North Hampshire CCG, which includes our Districts and Boroughs, will provide strategic leadership and political oversight. Reviewing the Terms of Reference of our current Health and Wellbeing Board and ensuring it is positioned to robustly govern our joint approach will be a priority for the final submission in April.
1.3. In parallel we will establish a joint leadership model with the Local Authority and CCGs and ensure robust governance and legal arrangements support our joint working and have clear and shared arrangements for the joint fund.
1.4. This paper provides an overview of the key actions carried out to produce the plan. A copy of the draft Better Care Plan can be found in appendix C.
1.5. The Health and Wellbeing Board has a key role to play in signing off the initial plan for submission on 14 February 2014. This will then be subject to national evaluation by NHS England and the Local Government Association (LGA).
1.6. The plan does not come into effect until 2015/16, giving partners time to work at scale and pace to transform the system.
2. Contextual information 2.1. Over the last few months significant work has been undertaken to determine the
shape and detail of the joint plan. This has included the development of a BCF Steering Group as well as a Health and Wellbeing Board (HWBB) seminars in September and December 2013.
1. 9�Better�Care�Fund.pdf
Top
Overall�Page�104�of�237Page�2�of�9

Agenda item: 5
2.2. The plan has been informed by the Joint Strategic Needs Assessment and Joint Health and Wellbeing Strategy. The work carried out amongst commissioners with provider with organisations and local people has directly influenced the plan such as CCG public engagement events and Hampshire County Council service user involvement work. The plan therefore reflects the aim of commissioning and providing a “joined up” health and care journey through the system for people and communities i.e. the right care, in the right place at the right time including the strengthening of care in community settings. The approach will address the three key challenges of:
• Avoiding unnecessary cost in the system, moving to lower cost solutions (whilst maintaining or improving outcomes)
• Preventing dependency and demand for longer term publically funded services
• Delaying people’s dependency on long term health and social care interventions
2.3. There is an expectation that the plan will align with the strategy process set out by NHS England supported by the LGA and others in The NHS Belongs to the people: a call to action1 Therefore the final plan submission the Better Care Plan should be submitted to NHS England, as an integral part of CCG Operational and strategic plans by 14 February 2014.
3. How the Better Care Fund (BCF) is being financed 3.1. Nationally the BCF provides £3.8 billion in 2015/16. In 2014/15, in addition to
the already planned £900 million national transfer from the NHS to adult social care, a further £200 million will transfer to help localities prepare for the implementation of the Fund.
3.2. The Fund is being created from a variety of sources and more detail can be gained from http://www.england.nhs.uk/wp-content/uploads/2013/12/bm-item6.pdf. A brief summary is provided below. Current Source of Funding NHS or LA New £ Allocation
Carer breaks NHS No £130m
Reablement NHS No £ 300m
Disabled Facilities Grant LA No £ 220m
Adult Social Care Capital Grants LA No £ 134m
Additional NHS Transfer to LAs LA No £ 200m
NHS Transfer LA No £ 900m
Transfer of additional NHS funding, currently deployed in CCG budgets
NHS No £1.9bn
Total £ 3.784bn
1 http://www.england.nhs.uk/2013/07/11/call-to-action/
2.
9�Better�Care�Fund.pdf
Top
Overall�Page�105�of�237Page�3�of�9

Agenda item: 5
3.3. The statutory framework for the BCF will be a Section 75 joint governance
arrangement (pooled budget) between CCGs and the Local Authority. Legislation is needed to ring fence NHS contributions at national and local levels and to ensure local authorities not party to the Fund can be paid from it, through additional conditions in Section 31 of the Local Government Act 2003. This will ensure the Disabled Facilities Grant (DFG) can be included in the Fund.
3.4. For the five CCGs in Hampshire the 2015/16 allocations have been confirmed as follows: Clinical Commissioning Group 2015/16 allocation2 Hampshire County Council £ 7,942,000 Fareham and Gosport £10,876,000 South Eastern Hampshire £11,617,000 North East Hampshire and Farnham £ 9,086,000 North Hampshire £11,391,000 West Hampshire £29,845,000 Total £80,757,000
3.5. Local partners could commit additional resources to the Pooled Fund from existing allocations if this was desirable. However the decision to formerly expand the Pooled Funds would need to bear in mind that payment of £1bn of the BCF will be dependent on performance achievement against a combination of national and locally determined measures.
4. Performance – National and Local Metrics 4.1. In 2014/15 there are no new requirements for pooling of budgets. The
requirements remain consistent with guidance issued in 2012 3 in line with this: 4.2. National measures underpinning the Fund will be:
• Admissions to residential and care homes
• Effectiveness of reablement
• Delayed transfer of care
• Avoidable emergency admissions; and
• Patient / service user experience 4.3. There is a nationally prescribed performance related payment arrangement
linked to the national measures and a locally determined measure selected from a prescribed list drawn from the NHS, Social Care and Public Health Outcomes
2 http://www.england.nhs.uk/wp-content/uploads/2013/12/allocation-summary.pdf 3 https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/213223/Funding-transfer-from-the-NHS-to-social-care-in-2013-14.pdf
3.
9�Better�Care�Fund.pdf
Top
Overall�Page�106�of�237Page�4�of�9
Agenda item: 5
Frameworks. The local measure is still being finalised for the final submission in April.
4.4. The HWBB is responsible for overseeing performance achievement through the joint governance arrangements.
5. Conditions of Funding 5.1. The statutory framework for the Fund will be through a Section 75 joint
governance arrangements between CCGs and the Local Authority. Funding will be routed through NHS England to protect the overall level of health spending. Legislation is needed to ring fence NHS contributions at national and local levels and to ensure local authorities not party to the Fund can be paid from it, through additional conditions in Section 31 of the Local Government Act 2003. This will ensure the DFG can be included in the Fund.
5.2. Measures will be introduced to ensure the DH Adult Social Care capital grants will reach local areas as part of the fund.
5.3. There are national conditions which will govern access to the BCF including that the plans should be jointly agreed. They are as follows:
• Protection for social care services (not spending)
• 7 day services in health and social care to support patients being discharged
• Better data sharing between health and social care based on the NHS number
• A joint approach to assessments and care planning and that where funding is used for integrated packages of care there will be an accountable professional
• Agreement on the consequential impact of changes in the acute sector
6. Assurance 6.1. Prior to being presented at the Board the draft plan has been shared and
approved at each of the CCG Governing Body meetings in January 2013. 6.2. The format of the plan is based on a national template of two parts.
Part 1:
• Names of commissioning organisations associated with the plan
• Boundary differences
• Authorisation and sign off
• Service provider engagement
• Patient, service user and public engagement
• Related documentation
• Vision and schemes Vision for health and care services Aims and objectives Description of planned changes
4. 9�Better�Care�Fund.pdf
Top
Overall�Page�107�of�237Page�5�of�9

Agenda item: 5
Implications for the acute sector Governance
• National Conditions
• Risks Part 2
• Outcomes and finances 6.3. NHS England’s process for assuring CCG strategic and operational plans will
include a specific focus relating to the BCF, allowing NHS England to rate and aggregate all plans against criteria agreed with government departments and the LGA. The revised Better Care Plan will then be submitted to NHS England by 4 April 2014.
7. Local Implications and Risks 7.1. An Equality Impact Assessment is being developed as part of the final
submission due in April 2014 7.2. As part of the plan development, it has been necessary for CCGs to identify
where existing funding to be invested in the Pooled arrangement is currently being invested, in the context of a small real terms increase in budget. This will have implications for current services as the scale of funding shift is unlikely to be achieved without significant service transformation. The impact on service providers within the health and social care economy is also currently being discussed.
7.3. Similarly, the historic s256 transfers included in the £900m sum and built into budgets to fund key services e.g. placements and personal care will be incorporated into the overall Pooled budget arrangements and therefore could present risks to the Local Authority financial position.
7.4. Our delivery of the plan will be dependent upon the quality of communication, engagement and involvement to enable us to secure the necessary buy in and confidence to support the changes.
7.5. There are also future risks associated with both the inclusion of the impact of
the proposed Care Bill implementation and significantly failure of the system to deliver the improvements. Central Government have determined that in future year’s performance related funds would be withdrawn to be reallocated elsewhere. This would result in the system bearing the cost of failing services.
8. Conclusion 8.1. Better Care Fund provides an opportunity to improve the lives of some of the
most vulnerable people in our society, giving them control, placing them at the centre of their own care and support, and, in doing so, providing them with a better service and better quality of life.
8.2. The Joint Health and Wellbeing Strategy development provided a clear mandate for increased joined up working and improving the service experience and outcomes fro local people. The focus of the Fund will support the aspiration of local people.
5. 9�Better�Care�Fund.pdf
Top
Overall�Page�108�of�237Page�6�of�9

Agenda item: 5
9. Recommendations 9.1. The Board is requested to:
• Note the progress to date to develop the draft plan
• Agree the draft plan for submission by 14 February 2014
6. 9�Better�Care�Fund.pdf
Top
Overall�Page�109�of�237Page�7�of�9

Integral Appendix A
CORPORATE OR LEGAL INFORMATION:
Links to the Corporate Strategy Hampshire safer and more secure for all: no
Maximising well-being: yes
• Promote and support healthy choices for all, reducing the difference between those with the best and worst health
• Help people to manage their health conditions, giving them choice and maintaining their independence
Enhancing our quality of place: yes
• Work with local communities to improve services Section 100 D - Local Government Act 1972 - background documents The following documents discuss facts or matters on which this report, or an important part of it, is based and have been relied upon to a material extent in the preparation of this report. (NB: the list excludes published works and any documents which disclose exempt or confidential information as defined in the Act.) Document Location None
7. 9�Better�Care�Fund.pdf
Top
Overall�Page�110�of�237Page�8�of�9

Integral Appendix B
IMPACT ASSESSMENTS: 1. Equalities Impact Assessment: The final Equalities Impact Assessment is under development.
2. Impact on Crime and Disorder: Not applicable.
3. Climate Change: a) How does what is being proposed impact on our carbon footprint / energy
consumption? b) How does what is being proposed consider the need to adapt to climate
change, and be resilient to its longer term impacts? Not applicable.
8. 9�Better�Care�Fund.pdf
Top
Overall�Page�111�of�237Page�9�of�9

GOVERNING BODY Date of Meeting 19th March 2014
Agenda Item No
10 Title
Finance Report Purpose of Paper
To inform the Governing Body of the financial position for Month 11 2013/14.
Recommendations/ Actions requested
The Governing Body is asked to: • to accept the contents of this report
Author
Mel Froggatt Finance Manager David Bailey Deputy Chief Finance Officer
Sponsoring member
Andrew Wood Chief Finance Officer
Date
14th March 2014
10�Finance�Report.pdf
Top
Overall�Page�112�of�237Page�1�of�8

South Eastern Hampshire CCG
Finance Report Month 11 2013/14
10�Finance�Report.pdf
Top
Overall�Page�113�of�237Page�2�of�8

Finance Summary
Risks Mitigating Actions
The CCG is currently on plan to meet its target surplus of £0.6m with a YTD surplus of £0.6m
The financial position of Portsmouth Hospitals NHS Trust has been produced using extrapolation of M8 activity data, which has shown a considerable increase in elective inpatients and outpatients. A full year outturn of £84.3m is the current understanding of the likely year end position.
In depth data analysis is underway to ensure activity is being coded correctly between CCG and NHS England. Discussions to agree a common understanding of the expected year end outturn position between PHT and the CCG are on going (RTT being a significant concern).
The QIPP target of £9m will not be achieved but the shortfall has been covered out of contingency funding.
QIPP schemes continue to be strengthened in order to get them to a stage that they can be incorporated into provider contracts; contingency funds are being used to cover shortfall.
New national directive that all NHS Property Services and Community Health Partnership estates charges will revert to original CCG allocations for 2013/14 only to ensure financial stability across the health system.
The previous allocation reduction will be reversed and charges will match budget received, therefore no cost pressure for this year. Discussions are to take place to agree next steps moving forward to 2014/15 and onwards.
FP10 expenditure has increased significantly above plan for December activity. Prescribing charges attributable to the Local Area Team and Local Authority public health services have increased significantly, which is in line with expectations of the service provision. Income is due from both organisations to offset these costs, following new the commissioning responsibilities, however final agreement on the total income due is still to be reached.
Working alongside neighbouring CCGs to reach mutual resolution with other commissioners.
10�Finance�Report.pdf
Top
Overall�Page�114�of�237Page�3�of�8

Financial Performance 2013/14 Summary: • Year to date spend on the CCG budgets is in line with the target surplus of £0.6m • Acute Commissioning is over plan, due mainly to over performance at Portsmouth Hospitals. • System wide there has been an increase in levels of activity, mainly EL and NEL in several acute contracts
Forecast Outturn: • The CCG is expecting to meet its surplus target of £0.6m, although the increasing over performance at Portsmouth Hospitals is a cause for concern. This is only possible by using contingency funding to cover unmet QIPP savings targets.
Month 11 - February 2014 Annual Budget to Actual to Variance to Forecast Forecast Budget Date Date Date Outturn Variance £'m £'m £'m £'m £'m £'m Acute Commissioning: 121.4 111.4 115.0 3.7 125.3 4.0 Mental Health Commissioning 19.8 18.1 18.3 0.2 19.9 0.2 Community Services Commissioning 20.2 18.6 19.0 0.5 20.8 0.5 Primary Care Commissioning 34.6 31.6 32.2 0.6 35.2 0.6 Continuing Care 15.0 13.7 13.0 (0.7) 14.2 (0.8) Other Commissioning 1.6 1.5 0.8 (0.7) 1.0 (0.6) Running Costs 4.2 3.9 3.9 0.1 4.4 0.2 Reserves & Contingencies 5.4 4.1 0.0 (4.1) 0.7 (4.7) Total NHS South Eastern Hampshire CCG 222.2 202.9 202.3 (0.6) 221.6 (0.6)
10�Finance�Report.pdf
Top
Overall�Page�115�of�237Page�4�of�8

Financial Performance 2013/14
Month 11 - February 2014 Annual Budget to Actual to Variance to Forecast ForecastBudget Date Date Date Outturn Variance
£'m £'m £'m £'m £'m £'mPortsmouth Hospitals NHS Trust 80.7 74.0 77.2 3.2 84.3 3.5University Hospital Southampton FT 1.8 1.6 2.1 0.5 2.3 0.5Western Sussex Hospitals 7.2 6.6 6.0 (0.6) 6.6 (0.6)Hampshire Hospitals Foundation Trust 5.0 4.5 4.8 0.3 5.2 0.3London Providers 2.0 1.9 1.8 (0.1) 1.8 (0.3)Royal Surrey County Hospital 9.1 8.3 8.5 0.1 9.3 0.2Frimley Park Hospital NHS FT 1.6 1.5 1.5 0.0 1.6 0.0Spire HealthCare 1.4 1.3 1.5 0.2 1.6 0.2South Central Ambulance 6.5 12.5 11.9 5.8 6.4 (0.1)Clinical Assessment and Treatment Centres 2.6 5.0 4.9 2.6 2.7 0.1NCAs / OATs 0.0 0.0 0.0 0.0 0.0 0.0Other Acute Contracts 3.5 (5.9) (5.1) (8.3) 3.6 0.1
Solent NHS Trust (MH) 0.0 0.0 0.0 0.0 0.0 0.0Southern Healthcare FT 0.8 0.7 0.7 0.0 0.8 0.0Sussex Partnership NHS FT 16.3 14.9 14.8 (0.1) 16.1 (0.2)IAPT 0.0 0.0 0.0 0.0 0.0 0.0Child Trust Pooled Budget (CAMHS) 0.0 0.0 0.2 0.2 0.2 0.2Other Mental Health Contracts 2.7 2.5 2.6 0.1 2.8 0.1
Solent NHS Trust (Community) 3.7 3.4 3.5 0.1 3.9 0.2Southern Healthcare FT 14.0 12.9 13.0 0.2 14.2 0.1NHS West Hampshire CCG 0.4 0.4 0.6 0.2 0.4 (0.1)Other Community Contracts 2.1 1.9 1.9 (0.0) 2.3 0.3
Prescribing Costs 31.6 28.8 29.8 0.9 32.7 1.1Local Enhanced Services 1.1 1.0 0.8 (0.2) 0.7 (0.5)111 Service 0.5 0.4 0.4 (0.0) 0.5 0.0OOH (Care UK) 1.5 1.3 1.3 (0.1) 1.4 (0.0)
Adult Continuing Care 11.4 10.5 9.9 (0.6) 10.8 (0.7)CHC Children 0.2 0.2 0.2 0.0 0.2 0.0Funded Nursing Care 3.3 3.0 2.9 (0.1) 3.2 (0.1)
Recharges NHS Property Services Ltd 0.7 0.6 0.6 0.0 0.7 0.0IFRs 0.3 0.3 0.1 (0.2) 0.3 (0.1)Other Commissioning 0.6 0.6 0.1 (0.5) 0.1 (0.6)
Headquarters/ Directorates, Agency and Assurance S 2.8 2.6 3.9 (1.2) 3.1 0.3CSU Charges 1.4 1.3 0.0 1.2 1.3 (0.1)
General Reserve 0.8 0.4 0.0 (0.4) 0.0 (0.8)Commisioning Reserve 4.0 3.1 0.0 (3.1) 0.7 (3.2)Surplus Reserve 0.6 0.6 0.0 (0.6) 0.0 (0.6)Total NHS South Eastern Hampshire CCG 222.2 202.9 202.3 (0.5) 221.6 (0.6)
Other Commissioning
Running Costs
Centrally Managed Programmes
Primary Care Commissioning
Acute Commissioning
Mental Health Commissioning
Community Health Commissioning
Continuing Care
10�Finance�Report.pdf
Top
Overall�Page�116�of�237Page�5�of�8

Portsmouth Hospitals Trust
Based on M10 actual activity
Reported Position £000's
Headline Position 3,801
Payment Adjustments * -638
Agreed Position for Month 10 3,164
Extrapolated to Month 111 3,233
Payment Adjustments * £000's
NEL Threshold -358 Maternity cap adjustment 107 Ambulance Handover estimate -168 Challenges & Other levers 265 Other adjustments -499 Other penalties -113 Trust proposals unagreed 303 CQUIN withheld - agreed -16 CQUIN withheld - unagreed -159 Total -638
Headline Finance Position Activity
Variance %
Finance Variance
% Run Rate Commentary
Elective & Daycase £1978k Over Plan 47.90% 50.00% The combined elective position (inpatients and daycases) has moved out from £1.6m (12.8%) to £1.96m (13.9%), £160k ahead of trend. The main areas of increase are Ophthalmology, Gastro, Breast and Gynae.
Non Elective £190k Over Plan -3.00% 2.80%
The emergency position is up on trend in activity moving from -2.7% to -2.4% under. However the cost variance has dropped from 2.7% to 2.5%: £524k over to £539k over (£40k below trend). There is upward cost and activity pressure in Gynae due to coding movements between CCGs and there is also pressure this month in Thoracic (£44k over largely pneumonia and COPD) . However, Orthopaedic Trauma (£40k under trend) and Paediatrics (£10k under trend) are among a range of subchapters which are below trend.
Outpatients £962k Over Plan 47.30% 42.10% The headline consultant led first outpatient variance has increased very slightly from 9.3% to 9.5% with increases in Colo-rectal, Gen medicine and Gastro. The main year to date variances are in Orthopaedics (£58k, 10%), Rheumatology (£53k, 51%), Breast Surgery (£39k, 28%) and Dermatology (£37k, 15%). Ambulatory Care including follow ups is £101k over plan, and appears to have jumped sharply from 20% over in December to 25% in January.
A&E £74k Under Plan 2.50% 2.40%
Critical Care £387k Over Plan 22.00% 25.30% Increased capacity within the trust continues to create over performance against plan. Multiple organ support continues to be a pressure.
Other £210k Over plan -7.60% 5.00% New robot charges being challenged by commissioners. ICDs causing a pressure to the CCG also.
10�Finance�Report.pdf
Top
Overall�Page�117�of�237Page�6�of�8

Contractual Performance
Forecast Outturn Run Rate Commentary
Acute Commissioning £3,980K Over Plan Growth in activity across many providers; PHT, UHS, Treatment Centres and Ambulances indicating an issue across the whole system. Trauma orthopaedics being a pressure within most contracts.
Mental Health Commissioning £185K Over Plan
The majority of Mental Health commissioning is included in the block contract with Southern Health NHS Trust. The projected overspend in the main relates to the counselling service which will not continue past December when the new IAPT contract is underway. Budgets have been realigned between the Hampshire 5 CCGs to account for the contract envelope at a CCG level. Increased usage of high cost/low volume MH inpatient units impacting CCGs financial position.
Community Services Commissioning £530K Over Plan
Expected activity levels being seen under the AQP contracts has increased, however certain contracts are now known not to be a financial cost to the CCG and are offsetting the pressure seen under the community contracts. TOPS are continually performing above plan (pressure of £99k FOT).
Primary Care Commissioning £599K Over Plan Trends for prescribing are showing a financial risk to the CCG of approx £600k, £400k being derived by FP10s and dispensing items and £200k drug costs met centrally (which the CCG have no control over).
Continuing Care £782K Under Plan Activity levels continue to rise for SE CCG, however the risk share agreement between the Hampshire 5 CCGs smooths this across all its members. Onoging work to understand patient flows in this service is currently underway.
Other Commissioning £614K Under Plan Financial contribution form neighbouring CCGs has improved reserves position.
Running Costs £182K Over Plan Running costs are under target for the CCG, which is enabled from the shared working with Fareham & Gosport CCG and Portsmouth CCG. Vacant posts are starting to be recruited to, hence planned underspend has reduced.
10�Finance�Report.pdf
Top
Overall�Page�118�of�237Page�7�of�8

Financial Risk Risk Mitigation RAG rating
Size of QIPP/Savings and pace of change Robust in year monitoring to ensure schemes are on target to deliver expected savings. Use of 2% non recurring fund to support system reconfiguration. Contingency funds are being used to cover shortfall.
Red Pressure on acute contracts; cost of meeting NHS Constitution and growth in activity levels above plan will carry financial implications
On-going discussions with Portsmouth Hospital and other providers to use Elective Referral data within Primary care in order to manage the activity and identify potential pressure areas.
Prescribing Public Health Drugs circa £500k, unrecovered cost Liaising with Local Authority and NHS England to reach a resolution on Public Health drugs to be included in the recharge.
Amber
Continuing Healthcare; increases in spend. Risk share across Hampshire 5 of a budget that is underspent overall; need to review budget allocation
Excessive growth under AQP contracts, CCG allocations are exclusive of any funding for AQP due to timing of new contracts being after PCT baseline exercise.
Enforcing contract levers to agree activity flows and usage. Communications with providers are on-going to ensure all are adhering to the agreed referral process.
Cost pressures within Ambulance Services due to both activity over performance and fines as a result of handover delays
Ongoing work with Portsmouth Hospital to work on Handover delays and Ambulance Services to ensure that the level of financial risk is minimum for CCG.
Indicative budgets as per fair share suggest significant underfunding for CCGS The CCG will continue to work with neighbouring CCG’s and NHS England to ensure the health system is appropriately funded.
Quality Premium milestones not being met throughout 2013/14, potential loss of 2014/15 income to the CCG of £1m
Milestones continue to be monitored in year to understand current performance
Information Governance rules restrict the ability to verify the authenticity of Non-Contracted Activity and Individual Funding Request charges.
National Guidance has been issued, the CCG is working with the CSU to implement interim solutions
NHS Property Services Ltd (PropCo), allocation charges for property transfers and ‘vacant’ space
NHS Property Services and CCGs are working together to understand the allocation changes and confirm transactions required
Green Potential further anomalies from original expenditure mapping exercise; CCG Allocations are held with the correct commissioner
Hampshire 5 baseline group has reformed to review budget allocations; there have been successful agreements to move funding between commissioners, however there are still areas which could result in the CCG reducing its allocation. Wessex Area Team to ensure potential anomalies from the original mapping exercise are understood.
10�Finance�Report.pdf
Top
Overall�Page�119�of�237Page�8�of�8

GOVERNING BODY Date of Meeting 19th March 2014
Agenda Item No
11 Title
Performance Report Purpose of Paper
To inform the Governing Body of the latest performance position for the CCG
Recommendations/ Actions requested
The Governing Body is asked to: • Note the key achievements of the CCG for the reported
period
• Review areas of concern
Author
Damien Ward Performance Manager Mike Drake Director of Planning and Performance
Sponsoring member
Andrew Wood Chief Finance Officer
Date
6 March 2014
11�Performance�Report.pdf
Top
Overall�Page�120�of�237Page�1�of�22

NHS South Eastern Hampshire CCG Governing Body Meeting
Performance Report 19th March 2014
11�Performance�Report.pdf
Top
Overall�Page�121�of�237Page�2�of�22

Table of Contents
South Eastern Hampshire (SEH) CCG
Executive Summary 3
Dashboard 4
Key Achievements and Underperformance 5
Key Risks and Mitigating Actions 6
Rights & Pledges and Other Key Priorities 7
Estimated Assurance Framework Delivery Dashboard 11
Estimated Quality Premium 12
Primary Care 13
Contracts Summary 14
Quality, Innovation, Productivity and Prevention 15
Portsmouth Hospitals NHS Trust 16
Key Performance Indicators 17
Royal Surrey County Hospital and Western Sussex Hospitals 18
Southern Health NHS Foundation Trust 19
South Central Ambulance Service 20
NHS 111 and Out of Hours 21
11�Performance�Report.pdf
Top
Overall�Page�122�of�237Page�3�of�22

SEH CCG Executive Summary
3
South Eastern Hampshire CCG aims to commission good quality care, promote the Rights and Pledges under the NHS Constitution and secure improvement in health outcomes of the local population, and do all of these within our financial plan. The CCG continues to make significant progress towards this aim in December and achieved 16 out of 23 indicators.
The CCG has now exceeded the annual trajectory for Clostridium Difficile (C.diff) cases and will not achieve the Healthcare Associated Infections (HCAI) element of the Quality Premium as a result. The majority of cases have been apportioned to the community and the Quality team is working with GP practices and nursing homes to reduce the risk of further cases.
The CCG remains concerned regarding Referral to Treatment (RTT), A&E 4 hour waits and Cancer performance at Portsmouth Hospitals NHS Trust (PHT). All three RTT targets were achieved at aggregate level in December, however, there continues to be specialty fails at PHT. A&E performance is below target and was not achieved in December or January. Cancer performance has improved in December, although the sustainability of performance remains a risk. The CCG has issued Contract Query Notices and requested a Remedial Action Plan for each area to provide assurance that performance will improve.
There has been a significant increase in GP referrals from South Eastern Hampshire practices into PHT. The Primary Care team is investigating the increase to identify any potential risk areas and ensure all referrals are appropriate.
Activity at PHT remains above the CCG contract plan in most areas, although there has been a reduction compared to November; the annual forecast for PHT remains above plan. Annual forecasts for Royal Surrey County Hospital, South Central Ambulance Service (SCAS) and Solent NHS Trust remain above plan.
The CCG is on track to meet the target surplus of £0.6m, however, Quality, Innovation, Productivity and Prevention (QIPP) delivery is under target. The Quality Premium payment for 2014/15 is currently estimated at £588,639.
NHS England have produced the final CCG Assurance Framework which ensures CCGs are continuing to meet their ongoing responsibilities to patients and the public. The Balanced Scorecard (which was previously reported) has been renamed the Delivery Dashboard and is assessed quarterly.
As part of the management of risks, the following issues were escalated by the Performance Improvement Action Group (PIAG) to the Portsmouth and South East Hampshire Commissioning Collaborative (PSEHCC) in February: Cancer and RTT waiting times, A&E 4 hour waits, planning requirements for 2014/15-2015/16, Stroke performance at SCAS, Child and Adolescent Mental Health Services (CAMHS) (Sussex partnership) and the Friends and Family Test.
11�Performance�Report.pdf
Top
Overall�Page�123�of�237Page�4�of�22

SEH CCG Dashboard
The dashboard below provides the latest position in relation to quality, performance, contracts and finance. The report is in the main informed by December data and where more up-to-date data is available it has been used.
4
CCG December Year to Dec Ref Planned care Target December Year to Dec RefMRSA 0 G 1 R RTT admitted patients <18weeks 90% 91.8% G 89.6% A Pg 8C.Difficile 3 R 36 R Pg 10 RTT non-admitted patients <18weeks 95% 96.2% G 96.7% G Mixed Sex Accommodation breaches 0 G 0 G RTT incomplete <18weeks 92% 93.6% G 93.6% G
Diagnostic test <6weeks 99% 98.6% A 99.1% G Pg 10PHT Number of cancer measures achieving target 9 7 8 Pg 8Hospital Standardised Mortality Ratio 89.0 G 89.0 G Summary Hospital Level Mortality Indicator 103.0 A 103.0 A Unscheduled careVenous Thrombo-embolus screening 95.1% G 95.5% G A&E 4 hr waits 95% 91.4% A 92.8% A Pg 9Friends and Family Test response rate 26.0% G 17.8% G A&E 4 hr waits (January) 95% 90.7% A 92.6% A Pg 9
48 54 Ambulance handover delays: >30 minutes (PHT) 151 A 1170 R Pg 9Ambulance handover delays: > 60 minutes (PHT) 92 A 710 R
Commentary: Commentary:•RTT targets were not achieved at specialty level.
•Healthcare Associated Infections •RTT and Cancer waiting times•A&E 4 hour waits
Year to January* Annual Year to January AnnualTarget Actual Var. Target Forecast Var. Plan Actual Var. Plan Forecast Var.
£m £m £m £m £m £m £m £m £m £m £m £mSpend:Portsmouth Hospitals Trust 60.5 63.1 2.6 R 80.7 85.0 4.3 R Spend 184.4 183.9 -0.5 G 222.2 221.6 -0.6 GSouthern Health - Mental Health 13.6 13.6 0 G 16.3 16.3 0 GSouthern Health - Community 11.7 11.7 0 G 14.0 14.0 0 G QIPP 7.7 4.3 -3.4 R 9.5 4.9 -4.6 RUniversity Hospital Southapmton 1.5 1.9 0.4 R 1.8 2.3 0.5 RSolent Trust 3.7 3.9 0.2 R 4.4 4.7 0.3 R Year to DecemberCare UK St Marys 1.4 1.4 0 G 1.8 1.8 0 G Quality Premium (estimate) 1.0 0.6 -0.4 RSouth Central Ambulance 5.1 5.3 0.2 R 6.2 6.4 0.2 R
Commentary: Commentary:
Friends and Family Test net promoter score (Q3)
95%
100100
15%<Q1 (63)
Target0
2 (Dec) / 24 (YTD)0
•Costs of additional activity to achieve RTT standards exceed current assumptions.•Commissioning for Quality and Innovation (CQUIN) payments and contract penalties may be renegotiated. •Pressure on acute contracts; activity levels above plan will carry financial implications
*Projected position based on December activity
•The CCG has now exceeded the annual C diff threshold of 32 cases.
Risks (current and future): Risks (current and future):•Costs of meeting NHS Constitution and growth is higher than estimated
•Negative patient experience (PHT)
Risks (current and future): Risks (current and future):
Quality Performance
Finance Contracts
•In line with plan, contract activity levels declined for December. Pressure is still being seen across many providers, mainly in T&O specialities.
•It is expected that the CCG will meet its annual surplus target of £0.6m, although the pressure seen at Portsmouth Hospitals is a cause for concern.
11�Performance�Report.pdf
Top
Overall�Page�124�of�237Page�5�of�22

SEH CCG Key Achievements and Underperformance
5
The key achievements for the month of December are listed below: •All three RTT targets were achieved: Admitted 91.8% (target 90%), Non-admitted 96.2% (95%) and Incomplete 93.6% (92%).
•There were no patients waiting over 52 weeks for treatment.
•There were no reported cases of Methicillin-resistant Staphylococcus Aureus (MRSA). •There were no Mixed Sex Accommodation breaches. •Seven out of the nine Cancer standards were achieved.
•The CCG is currently on plan to meet its target surplus of £0.6m with a year to January surplus of £0.5m.
The key areas where the CCG is underperforming during December are listed below: • A&E 4 hour waits did not achieve the target of 95% with 91.4% of patients seen within the timescale. • There were seven reported cases of Clostridium Difficile against a target of two.
• The diagnostic target of 99% was not achieved with 98.6% of patients seen within six weeks. • ‘Cancer patients receiving subsequent surgery within 31 days’ did not achieve the 94% target with 93.3%.
• ‘Cancer patients receiving subsequent radiotherapy within 31 days’ did not achieve the 94% target with 93.3%.
• Quality, Innovation, Productivity and Prevention (QIPP) delivery under target.
11�Performance�Report.pdf
Top
Overall�Page�125�of�237Page�6�of�22

6
SEH CCG Key Risks and Mitigating Actions
Key Risks Mitigating Actions Referral to Treatment (RTT) • The three RTT targets were achieved in December at aggregate
level, however, the targets were not achieved at specialty level primarily due to underperformance at PHT.
A&E 4 hour waits • The CCG continues to fail to achieve the A&E target due to the
underperformance at PHT. Cancer • Concerns remain regarding PHT’s ability to consistently achieve
targets. Healthcare Associated Infections (HCAI) • The CCG has now exceeded the C Difficile annual trajectory. The
majority of cases have been attributed to the community. PHT Friends and Family Test • Whilst response rates are increasing, the inpatient net promoter
score continues to decline and may have an adverse impact on the achievement of the related Quality Premium.
Stroke performance at South Central Ambulance Service (SCAS) • SCAS are failing to meet targets for conveying stroke patients to
the centre within 60 minutes.
• A Remedial Action Plan has been submitted by PHT in response
to the Contract Query Notice issued in December 2013, which provides the Trust’s plans to achieve targets at specialty level. This has not yet been agreed by commissioners.
• A Contract Query Notice was issued to PHT on 30th January
2014 requesting a Remedial Action Plan which provides the Trust’s plans to achieve the target.
• A Remedial Action Plan has been submitted by PHT in response
to the Contract Query Notice issued in December 2013, which provides the Trust’s plans to achieve Cancer targets consistently for each standard. This has not yet been agreed by commissioners.
• The Quality team has developed a recovery plan to improve
processes and raise awareness in the community, involving GP practices and nursing/residential homes.
• The Trust has been working closely with the Wessex Area Team
to review best practice regionally and nationally. A number of initiatives have been put in place to ensure methods of capturing data are comparable with similar organisations.
• This has been escalated to a Contract Query Notice for review.
There are a number of actions in place by SCAS including benchmarking with two neighbouring trusts to ascertain best practice and improvement initiatives.
11�Performance�Report.pdf
Top
Overall�Page�126�of�237Page�7�of�22

7
SEH CCG Rights & Pledges and Other Key Priorities (1/4)
Indicator Target Period Prev Curr Perf Dir Q1 Q2 Q3 YTD
2013/14
Referral To Treatment waiting times for non-urgent consultant-led treatmentRTT:% of admitted patients who waited 18 weeks or less 90% Dec-13 92.3% 91.8% 91.7% 89.2% 88.1% 89.6%RTT:% of non-admitted patients who waited 18 weeks or less 95% Dec-13 96.1% 96.2% 97.5% 96.8% 95.8% 96.7%RTT:% of incomplete patients waiting 18 weeks or less 92% Dec-13 94.5% 93.6% 94.5% 93.8% 93.6% 93.6%RTT: Number of admitted patients who waited >52 weeks 0 Dec-13 0 0 0 0 0 0RTT: Number of non-admitted patients who waited >52 weeks 0 Dec-13 0 0 0 0 0 0RTT: Number of incomplete patients waiting >52 weeks 0 Dec-13 0 0 0 0 0 0Diagnostic test waiting times% Patients waiting <6 weeks for a diagnostic test 99% Dec-13 99.4% 98.6% 99.1% 99.2% 99.1% 99.1%A&E waitsA&E <=4hrs (QTD) 95% Jan-14 91.4% 90.7% 91.6% 92.7% 94.1% 92.5%Cancer waits – 2 week waitCancer patients seen <14 days after urgent GP referral 93% Dec-13 94.4% 95.6% 94.8% 93.6% 94.1% 94.1%Breast Cancer Referrals Seen <2 weeks 93% Dec-13 92.2% 98.9% 95.1% 94.8% 95.3% 95.1%Cancer waits – 31 daysCancer diagnosis to treatment <31 days 96% Dec-13 98.8% 99.0% 98.0% 97.5% 98.8% 98.1%Cancer Patients receiving subsequent surgery <31 days 94% Dec-13 100% 93.3% 92.7% 95.8% 96.2% 95.1%Cancer Patients receiving subsequent Chemo/Drug <31 days 98% Dec-13 100% 100% 100% 100% 100% 100%Cancer Patients receiving subsequent radiotherapy <31 days 94% Dec-13 97.2% 93.3% 95.4% 99.2% 93.9% 96.2%Cancer waits – 62 daysCancer urgent referral to treatment <62 days 85% Dec-13 88.4% 94.3% 90.1% 88.6% 92.4% 90.3%Cancer Patients treated after screening referral <62 days 90% Dec-13 100% 100% 77.3% 85.0% 100% 87.9%Cancer Patients treated after consultant upgrade <62 days (local threshold) 86% Dec-13 100% 100% 100% 100% 100%Category A ambulance callsCat A calls within 8 minutes - Red 1 75% Jan-14 72.2% 69.7% 75.6% 64.2% 74.3% 71.2%Cat A calls within 8 minutes - Red 2 75% Jan-14 71.1% 79.1% 74.9% 74.3% 72.7% 74.4%Cat A calls within 19 minutes 95% Jan-14 92.9% 93.0% 94.6% 94.3% 94.1% 94.2%Mixed Sex Accommodation BreachesMixed Sex Accommodation Breaches 0 Dec-13 0 0 0 0 0 0Healthcare Associated InfectionsHCAI: Clostridium Diffici le (C. Diff.) Infection rates 32 Dec-13 4 7 9 14 17 40HCAI: Incidence of MRSA 0 Dec-13 0 0 1 0 0 1Mental health
Care Programme Approach (CPA): The proportion of people under adult mental i l lness specialties on CPA who were followed up within 7 days of discharge from psychiatric in-patient care during the period.
95% Q3 100% 98.4% 100% 100% 98.4% 99.4%
11�Performance�Report.pdf
Top
Overall�Page�127�of�237Page�8�of�22

8
SEH CCG Rights & Pledges and Other Key Priorities (2/4)
Referral to Treatment • The three national RTT targets were achieved at aggregate level for the CCG, however, the targets were not achieved at specialty level due
to underperformance at PHT. The specialties which remain the main concern at PHT are Urology, General Surgery, Ear Nose and Throat (ENT) and Trauma & Orthopaedics (T&O).
• Commissioners sent a letter to inform PHT of their intention to issue a Contract Query Notice in order to gain traction surrounding the
delivery of RTT targets. Commissioners met with PHT on 7th January 2014 to discuss the options open to both parties to resolve the performance issues.
• It was agreed to implement a Remedial Action Plan that would seek to address any issues that prevented the Trust from achieving
sustainable specialty level performance. The plan will enable commissioners to gain assurance that the Trust has a comprehensive plan to achieve complete RTT performance. The Trust has now submitted a Remedial Action Plan which has not yet been jointly agreed and the action resides with commissioners to escalate to governing bodies.
• The CCG has achieved the three RTT targets at aggregate level in January, although there have been specialty fails at PHT in Urology,
Cardiology, General Surgery, Gastroenterology and T&O. The Trust anticipate failing ENT in February, T&O in March and General Surgery in April.
Cancer • Seven of the nine Cancer standards were achieved in December. ‘Cancer patients receiving subsequent surgery within 31 days’ did not
achieve target due to one patient breach at Royal Surrey County Hospital (RSCH). ‘Cancer patients receiving subsequent radiotherapy within 31 days’ did not achieve target due to one breach at RSCH and one breach at PHT.
• Cancer performance at PHT improved in December with the Trust achieving all nine standards, however, this was partly due to patients choosing to be seen outside of the holiday period which has affected performance in January.
• The Trust has failed ‘Cancer patients receiving subsequent surgery within 31 days’ in January due to capacity issues in Urology, and ‘Cancer patients receiving subsequent radiotherapy within 31 days’ due to patient choice.
• The CCG has taken a number of actions including the use of contractual levers due to inconsistent performance at PHT. A Remedial Action
Plan has been submitted by PHT in response to the Contract Query Notice issued in December 2013. This provides the Trust’s plans to achieve Cancer targets consistently for each standard, although this has not yet been agreed by commissioners.
11�Performance�Report.pdf
Top
Overall�Page�128�of�237Page�9�of�22

9
SEH CCG Rights & Pledges and Other Key Priorities (3/4)
A&E • The CCG has failed to achieve A&E targets in December (91.4%) and January (90.7%); the graph below shows the CCG weekly A&E
performance.
• The majority of activity is at PHT which continues to have challenges achieving the 95% target. The Trust is also failing in the following
Clinical Quality Indicators (CQIs): unplanned re-attendance rates within seven days, the total time spent in A&E, the arrival to assessment within 15 minutes and arrival to treatment within 60 minutes.
• The performance is regularly discussed at the monthly Contractual Performance Sub Group Meeting at which both PHT and CCG colleagues attend. Any issues are then escalated through to PHT’s monthly Executive Contractual Review Meeting.
• Following PHT’s return to poor performance, coupled with the additional investment made into the system in the form of winter pressure
money, the decision was taken to issue PHT a Contract Query Notice. This was sent to PHT on the 30th January 2014. PHT and the CCG are required to agree that either the Contract Query Notice is withdrawn, or to conduct a joint investigation, or to implement an appropriate Remedial Action Plan.
• The CCG has liaised with NHS 111 and Out of Hours to ensure alternative locations are provided to patients requiring urgent assessment. NHS 111 are promoting the Minor Injuries Unit (MIU) and the Guildhall Walk in Centre (WIC) where appropriate. Out of Hours are providing Bordon and Gosport War Memorial Hospital Primary Care Centres as alternatives to A&E to stem patient flow.
• There was a significant increase in ambulance handover delays in December. Plans by PHT to reduce handover delays include establishing a contract with UKSAS (private paramedic provider) to support A&E with managing patients, and a revised pathway for urgent GP referred patients to go directly to the Medical Assessment Unit (MAU).
11�Performance�Report.pdf
Top
Overall�Page�129�of�237Page�10�of�22

10
SEH CCG Rights & Pledges and Other Key Priorities (4/4)
Diagnostics • The CCG did not achieve the 99% diagnostic target in December with 98.6% of patients seen within six weeks. The majority of breaches
occurred at PHT and have been attributed to increased demand and capacity issues. • Local NHS trusts were contacted by PHT requesting assistance with additional capacity, however, the trusts were experiencing similar
issues and were also needing to outsource activity. Capacity offered by Spire and Nuffield was utilised, although there have been patients booked outside of the six week target by outsourcing providers.
• Pre-operative assessments are being booked earlier to allow patients greater flexibility and choice. Further work will be undertaken with
outsourcing providers to ensure that there are clear booking rules and patients are booked within six weeks. Feedback is provided to educate staff where requests for scans are deemed to be inappropriate.
• Recruitment continues with challenges at sonographer and sub specialty level. PHT report the majority of new staff should be in post by April 2014. A locum has been secured from the end of January who will deliver between three and four additional Endoscopy sessions a week.
• PHT have not achieved the diagnostics target in January.
Healthcare Associated Infections (HCAI) • The CCG has now exceeded the annual C.diff threshold of 32 with a year to January figure of 43 reported cases. The HCAI element of the
Quality Premium (£130,809) will not be achieved as a result. There have been 33 cases which have been apportioned to the community and seven of the remaining cases have been apportioned to PHT.
• The Quality team has developed a recovery plan to improve HCAI performance within the community including: o The analysis and monitoring of cases through coding from GP practices to identify potential links to nursing/residential homes. o The development of a ‘Primary Care Infection Prevention and Control Policy’ for GP practices to review against their own policies. o Ensuring awareness in primary care with regard to appropriate antibiotic prescribing.
• PHT have attributed the rise in C.diff cases to increased acuity and bed occupancy affecting the ability to isolate patients in a timely manner,
as well as the standard of cleaning and disinfection in clinical areas. PHT is taking a number of actions including reinstating deep clean programmes and more education for staff.
11�Performance�Report.pdf
Top
Overall�Page�130�of�237Page�11�of�22

11
SEH CCG Estimated Assurance Framework Delivery Dashboard
NHS England published its final Assurance Framework in November 2013 and has made some amendments to the Draft Assurance Framework published at the beginning of the financial year. The final Assurance Framework has changed what was previously called the Balanced Scorecard to the Delivery Dashboard. All of the underpinning elements of the previous Balanced Scorecard and the new Delivery Dashboard remain the same, however, the overall RAG rating of domains have been removed. The CCG’s estimated performance at the end of December (Quarter 3) using NHS England assessment criteria is shown in the Delivery Dashboard below.
Q1 Q2 Q3 Q3 Indicators failing
•Feedback from the Friends and Family Test indicates causes for concern at PHT
•PHT has reported more C.diff cases than trajectory
•Southern Health have reported unclosed Serious Incidents Requiring Investigation (SIRIs)
•RTT Admitted
•Diagnostics
•A&E 4 hour waits (PHT)
•Cancer patients receiving subsequent radiotherapy <31 days
•An improvement in combined Friends and Family Test scores for acute inpatient care and A&E services
•Number of C.diff cases exceeding trajectory
•Year to date Quality, Innovation, Productivity and Prevention (QIPP) delivery
•Financial plan meets the 2013 surplus planning requirement
South Eastern Hampshire CCG Assurance Framework Delivery Dashboard
Section Titles
Are patients receiving clinically commissioned, high quality services? (Indicators achieved out of 20)Quality 19
Are CCGs delivering services within their financial plans? (Indicators achieved out of 10)
18 17
NHS ConstitutionAre patient rights under the NHS Constitution being promoted? (Indicators achieved out of 20)
15 16 16
Are health outcomes improving for local people? (Indicators achieved out of 8)
6
888Finance
5 6Outcome
11�Performance�Report.pdf
Top
Overall�Page�131�of�237Page�12�of�22

12
SEH CCG Estimated Quality Premium
The Quality Premium is intended to reward the CCGs for improvements in the quality of the services that they commission, and for associated improvements in health outcomes and reducing inequalities. The CCG estimated Quality Premium for the year is £588,639 (as at the end of December). This position assumes that all of the financial gateway conditions have been met. The payment of the 2014/15 premium will be based on the 2013/14 performance on four national measures and three local measures which are detailed in the table below.
National Measures Achieved Value (£)Mortality* 12.50% Y £130,809Avoidable Emergency Admissions* 25% Y £261,618Patient Experience (Friends and Family Test score) 12.50% N £0Preventable Infections 12.50% N £0Local MeasuresOnward referral rate from the COAST service to Portsmouth Hospitals Trust (CAU/A&E, including self-referral) to be no more than 20%
12.50% Y £130,809
50% of patients attending pulmonary rehab in 2013/14 to have an agreed care plan in place.
12.50% Y £130,809
Number of patients reviewed and discussed which have been identified by using the ACG Tool (include those in RUB 3 and 4, High and Medium users)
12.50% Y £130,809
TOTAL 100% £784,853
£130,809£261,618£130,809
£130,809
£130,809
* Assumed position - data not yet available
Measure % of Quality Premium Value for CCG
Dec-13
£130,809
£130,809
£1,046,470
Measure achieved
Quality Premium adj.
Y N -£196,213Y Y
-£196,213£588,639
Category A Red 1 ambulance calls 25%Total adjustmentREVISED TOTAL
NHS Constitution rights and pledges % reduction
for non-achievement
Referral to treatment times (18 weeks) 25%A&E waits 25%Cancer waits – 62 days 25%
11�Performance�Report.pdf
Top
Overall�Page�132�of�237Page�13�of�22

13
SEH CCG Primary Care
GP Referrals – period ending December 2013 • There is a concern with the increasing number of GP referrals into PHT (primarily from Fareham & Gosport and South Eastern
Hampshire CCGs) compared to 2012/13. • There has been a 11.5% increase of referrals into PHT from SEH CCG practices. The graph below shows the April to December
yearly comparison.
• Specialties at PHT which have seen the highest increase from SEH are Trauma & Orthopaedics, Breast Surgery and Cardiology. • Commissioners have requested the conversion rates from PHT for referrals to outpatients and outpatients to inpatients. It is expected
that this information will provide the CCGs with the knowledge to ascertain whether or not the increased levels of referrals are significant, if PHT regularly clinically triage referrals and if GPs are sending appropriate referrals.
• The CCG wish to re-engage GP practices in referral monitoring, understanding data to create intelligence, and share understanding
of the resource implications. Actions to be undertaken by practices include:
– Referrals generated by locum GPs or trainee doctors will be checked and signed off by another GP in the practice. – Clinicians will use systems that assist them to identify the pathway when referring a patient. – The practice manager will identify their three highest referring specialties on a six monthly basis. The practice will peer
review a sample of the referrals and provide evidence that internal discussions have taken place to share best practice, share knowledge and skills, and identify any training needs.
11�Performance�Report.pdf
Top
Overall�Page�133�of�237Page�14�of�22

14
SEH CCG Contracts Summary
Portsmouth Hospitals NHS Trust • Elective inpatient activity is above plan with the main pressures in Breast procedures, Ophthalmology and Vascular.
• Non-elective activity is below plan driven by Gynaecology and Orthopaedic Trauma.
• Outpatient first attendances have reduced in Ophthalmology and Orthopaedics, however, the position remains above plan primarily
due to pressures in Rheumatology, Respiratory, Dermatology and Breast.
• A&E activity is over plan. Southern Health NHS Foundation Trust – Community • The final variances of the baseline review were presented to Chief Finance Officers in December 2013. Southern Health has also
made contact with NHS England and the Local Area Team regarding the variances in the allocations. Chief Finance Officers are awaiting formal responses from all organisations as to the willingness to transfer costs and allocations.
Southern Health NHS Foundation Trust – Mental Health
• Rehabilitation inpatient activity is under plan and Southern Health cite a lack of demand. CCGs are currently undertaking a review of the Rehabilitation pathway.
• Psychiatric Intensive Care Unit activity is under plan and consideration will be given to how best construct plans for services prone to such fluctuation.
• The Hospital at home service activity is over plan. An in depth review of Adult Mental Health community pathways is being
undertaken. Royal Surrey County Hospital • Elective, non-elective and A&E activity is above plan. Trauma & Orthopaedics is the highest performing elective specialty and
Geriatric and Orthopaedics are the highest performing non-elective areas.
11�Performance�Report.pdf
Top
Overall�Page�134�of�237Page�15�of�22
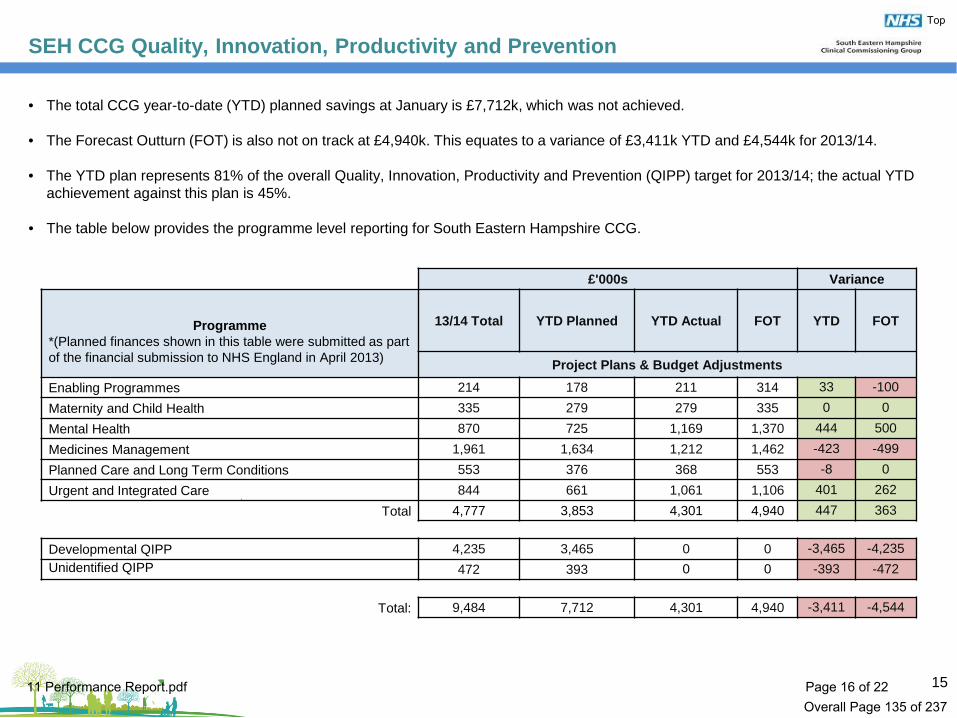
15
SEH CCG Quality, Innovation, Productivity and Prevention
• The total CCG year-to-date (YTD) planned savings at January is £7,712k, which was not achieved.
• The Forecast Outturn (FOT) is also not on track at £4,940k. This equates to a variance of £3,411k YTD and £4,544k for 2013/14. • The YTD plan represents 81% of the overall Quality, Innovation, Productivity and Prevention (QIPP) target for 2013/14; the actual YTD
achievement against this plan is 45%. • The table below provides the programme level reporting for South Eastern Hampshire CCG.
£'000s Variance
Programme
*(Planned finances shown in this table were submitted as part of the financial submission to NHS England in April 2013)
13/14 Total YTD Planned YTD Actual FOT YTD FOT
Project Plans & Budget Adjustments
Enabling Programmes 214 178 211 314 33 -100 Maternity and Child Health 335 279 279 335 0 0 Mental Health 870 725 1,169 1,370 444 500 Medicines Management 1,961 1,634 1,212 1,462 -423 -499 Planned Care and Long Term Conditions 553 376 368 553 -8 0 Urgent and Integrated Care 844 661 1,061 1,106 401 262
Total 4,777 3,853 4,301 4,940 447 363
Developmental QIPP 4,235 3,465 0 0 -3,465 -4,235 Unidentified QIPP 472 393 0 0 -393 -472
Total: 9,484 7,712 4,301 4,940 -3,411 -4,544
11�Performance�Report.pdf
Top
Overall�Page�135�of�237Page�16�of�22

16
Portsmouth Hospitals NHS Trust
This dashboard provides an overview of Portsmouth Hospitals Trust (PHT) performance from the quality, performance, contracts and finance perspectives. The data is sourced from PHT’s Integrated Performance Report (with the exception of contracts).
Target December Year to Dec Target December Year to DecHCAI - MRSA 0 0 G 0 G RTT admitted patients <18weeks 90% 90.7% G 87.3% R HCAI - C.Difficile 7 R 27 R RTT non-admitted patients <18weeks 95% 96.2% G 96.6% G Venous Thrombo-embolus screening 95% 95.1% G 95.5% G RTT incomplete <18weeks 92% 93.6% G 93.6% G Pressure Ulcer Prevalence (grade 2, 3,4) 1.06% 0.79% G 1.53% A Diagnostic waits <6 weeks 99% 98.0% A 99.1% G Hospital Standardised Mortality Ratio (HSMR) 100 89.0 G 89.0 G Admission directly to stroke unit 90% 87.7% A 90.0% G Summary Hospital Level Mortality Indicator (SHMI) 100 103.0 A 103.0 A Number of cancer measures achieving target 9 9 9 Never events 0 0 G 0 G Friends and Family Test (response rate) 15% 26.0% G 17.8% G A&E 4 hr waits 95% 87.5% R 90.7% A Friends and Family Test (net promoter score) n/a 42 - A&E unplanned re-attendance rates < 7 days 5% 5.3% R 5.5% R Number of Serious Incidents Requiring Investigations (SIRIs) n/a 5 68 Ambulance handover delays: >30 minutes 151 A 1170 R Number of complaints received n/a 47 484 Ambulance handover delays: > 60 minutes 92 A 710 R Complaints acknowledged <3 days n/a 100% G 99.6% G
•Healthcare Associated Infections
Year to January* Annual Year to December AnnualTarget Actual Var. Target Forecast Var. Plan Actual Var. Plan Forecast Var.
£m £m £m £m £m £m £m £m £m £m £m £mFinance:
Fareham & Gosport 68.8 71.6 2.8 R 91.3 95.7 4.4 R Surplus / -deficit -3.6 -6.1 -2.5 R -5.0 -5.0 0 GSouth Eastern Hampshire 60.8 63.4 2.6 R 80.7 84.2 3.5 RPortsmouth 77.5 78.4 0.9 R 102.9 105.1 2.2 R Workforce:
Staff turnover 12.0% 9.7% -2.3%Sickness 3.0% 3.4% 0.4%
•Increased referral activity •Achieving planned deficit
•There has been a decline in the stroke/PPCI performance. The CCG has invited the stroke clinical lead to provide a brief and update at the Performance Sub Group Meeting.
Commentary:•December RTT specialty fails: Urology (admitted & incomplete), General Surgery (non-admitted & incomplete) & T&O (non-admitted & incomplete).
•The decrease in pressure ulcer prevalence has been attributed to continued work with the tissue viability team and validation of figures.
Commentary:
Risks (current and future):
•A&E 4 hour waits
•The Trust has implemented a recovery plan with financial work-streams to ensure the year end forecast is achieved.
2 (Dec)/ 21 (YTD)
*Projected position based on December activity
•The primary over-performing elective specialties YTD are T&O, ENT, Rheumatology, Cardiology and General Surgery.
•Turnover has increased across all staff groups, although this remains comparable with other large acute trusts and in line with the acute NHS average of 9.5%.
•Non-elective activity has seen increased pressure in Orthopaedic Trauma, Digestive, Immunology, Renal and Thoracic procedures.•The main over-performing specialties for First Outpatients are T&O, Rheumatology, Audiology, Dermatology and Breast Surgery.
•Sickness absence is above target, however, compares favourably at regional and national level against other acute hospitals.
Risks (current and future): Risks (current and future):
•Negative patient experience
Commentary:
Risks (current and future):
Commentary:
•RTT and Cancer waiting times
Quality Performance
Finance & WorkforceContracts
11�Performance�Report.pdf
Top
Overall�Page�136�of�237Page�17�of�22

17
Portsmouth Hospitals NHS Trust Key Performance Indicators
2013/14 Targets
Previous Month
Dec-13Performance
DirectionQ1 Q2 Q3
Meeting CDIFF Objective < / = 30 5 7 4 10 13 27 RMeeting MRSA Objective 0 0 0 0 0 0 0 GVTE Risk Assessment 95% 95.5% 95.1% 95.2% 95.7% 95.3% 95.4% GA&E 4 hr arrival to admission/transfer/discharge 95% 94.0% 87.5% 88.9% 90.3% 92.8% 90.7% RUnplanned re-attendances rate <7 days < 5% 5.8% 5.3% 5.5% 5.8% 5.4% 5.5% RLeft without being seen < = 5% 1.1% 1.2% 1.8% 1.9% 1.1% 1.7% GTotal time in A&E (95th percentile) < 4hrs 4.54 7.32 6.20 6.04 5.25 6.01 RArrival to assessment (95th percentile) < 15 mins 0.11 0.25 0.29 0.20 0.16 0.21 RMedian time arrival to treatment < 60 mins 0.45 0.50 1.00 0.56 0.49 0.55 GSingle longest wait arrival to treatment Improve 6.03 8.04 9.19 8.41 8.04 9.19 RAmbulance delays > 30 minutes 0 76 151 597 257 316 1170 RAmbulance delays > 60 minutes 0 10 92 488 93 129 710 R% Admitted 90% 90.6% 90.7% 91.8% 86.3% 84.2% 87.3% R% Non-Admitted 95% 95.9% 96.2% 97.3% 96.6% 95.8% 96.6% G% Incomplete Pathways < 18 wks (monthly) 92% 94.3% 93.6% 95.7% 93.6% 84.2% 93.6% G95th percentile for Admitted 23 weeks 23.9 24.4 24.2 31.6 27.0 28.0 R95th percentile for Non-Admitted 18.3 weeks 18.7 18.5 17.8 18.3 18.7 18.3 G95th percentile for Incomplete 28 weeks 19.7 20.8 18.2 20.5 19.8 19.7 GAdmitted backlog target 308 571 739 736 844 574 574 R18-week Non-Admitted backlog (monthly) 2292 916 87 395 620 878 878 GIncomplete patients waiting > 52 wks 0 0 0 0 0 0 0 G
Diagnostics Diagnostic waits 99% < 6 wks 99.2% 98.0% 99.3% 99.3% 98.9% 99.1% GAll 2-week wait referrals 93% 91.7% 94.2% 94.9% 93.8% 92.7% 93.8% GBreast symptomatic 2-week wait referrals 93% 94.4% 97.0% 94.4% 94.8% 95.2% 94.8% G31-day diagnosis to treatment 96% 96.6% 99.2% 97.2% 98.9% 98.3% 98.2% G31-day subsequent cancers to treatment 94% 91.0% 95.7% 96.5% 96.1% 92.1% 95.1% G31-day subsequent anti-cancer drugs 98% 100% 100% 100% 100% 100% 100% G31-day subsequent radiotherapy 94% 96.3% 97.7% 97.1% 95.8% 96.9% 96.6% G62-day referral to treatment 85% 82.2% 85.8% 86.3% 87.4% 85.7% 86.5% G62-day screening to treatment 90% 100% 100% 84.1% 93.1% 99.2% 91.9% G62-day consultant upgrade to treatment 86% 85.2% 100% 91.0% 97.0% 91.0% 93.0% G90% of stay on a stroke unit 80% 77.6% 81.5% 92.0% 94.0% 81.7% 89.0% GAdmission directly to a stoke unit 90% 89.6% 87.7% 89.3% 93.0% 88.3% 90.0% G% of high risk TIA seen and treated within 24 hrs of first contact with health professional
60%85.4% 68.6% 75.8% 86.5% 77.9% 81.4% G
Urgent CT within 60 minutes of arrival 50% 68.7% 74.1% 71.7% 61.2% 70.0% 67.9% GPPCI within 120 mins of call 75% 61.9% 59.3% 77.6% 75.0% 61.2% 71.3% RPPCI within 90 mins of arrival (door to balloon) 80% 87.5% 93.0% 95.0% 91.0% 90.9% 92.0% GPPCI within 60 mins of arrival (door to balloon) 50% 79.2% 78.8% 88.0% 74.2% 76.6% 80.5% GRapid Access Chest Pain Clinic within 2 wks 98% 100% 100% 100% 100% 100% 100% GEmergency Re-Admissions within 30 days 7% 0% 0% - 6.0% 0% - GCancelled Operations - 28 day Guarantee 5% 0% 0% 0% 0% 0.4% 0% GUrgent Operations Cancelled for a 2nd time 0 0 0 0 0 0 0 G
Flow
Cancer
Stroke Care
NSF Coronary Heart Disease
RTT
YTDKey Targets Dashboard
Quality of Care
A&E Patient Impact
A&E Timeliness
11�Performance�Report.pdf
Top
Overall�Page�137�of�237Page�18�of�22

18
Royal Surrey County Hospital & Western Sussex Hospitals
This dashboard provides an overview of Royal Surrey County Hospital (RSCH) and Western Sussex Hospitals Foundation Trust (WSHFT) performance from the quality, performance, contracts and finance perspectives. The data is sourced from Integrated Performance Reports (with the exception of contracts).
RSCH WSHFT RSCH WSHFTDecember December Target December December
HCAI - MRSA 0 G 0 G RTT admitted patients <18weeks 90% 94.0% G 90.1% GHCAI - C.diff. 2 R 2 G RTT non-admitted patients <18weeks 95% 98.0% G 95.2% GVenous Thrombo-embolus screening 96.0% G 96.5% G RTT incomplete <18weeks 92% 95.0% G 92.0% GFriends and Family Test response rate 32.6% G 39.2% G Diagnostics <6weeks 99% 99.8% G 99.8% GFriends and Family Test net promoter score (Q3) 62 75 Number of cancer measures achieving target 8 8 8Mixed Sex Accommodation 0 G 0 GNumber of complaints received 23 37 A&E 4 hr waits 95% 94.1% A 94.9% AComplaints acknowledged <3 days 63.0% R n/a
Risks: Risks:•Healthcare Associated Infections •A&E
Year to January* Annual Year to December AnnualTarget Actual Var. Target Forecast Var. Plan Actual Var. Plan Forecast Var.
£m £m £m £m £m £m Finance:RSCH Surplus / -deficit (RSCH) 2.2 2.9 0.7 G 3.2 3.2 0 GFareham & Gosport 0.02 0.08 0.06 A 0.03 0.10 0.07 A Surplus / -deficit (WSHFT) 4.8 -0.7 -5.5 R 5.2 5.2 0 GSouth Eastern Hampshire 6.8 7.0 0.2 R 9.1 9.3 0.2 R
Workforce (RSCH)Turnover 12.0% 13.2% 1.2%
WSHFT Sickness 2.7% 3.1% 0.4%South Eastern Hampshire 6.0 5.5 -0.5 G 7.2 6.6 -0.6 G Workforce (WSHFT)Portsmouth 0.6 0.5 -0.1 G 0.8 0.7 -0.1 G Turnover 11.0% 7.2% -3.8%
Sickness (November) 3.3% 4.2% 0.9%
Commentary: Commentary:RSCH•The SEH overspend is primarily due to increased Non-elective activity, driven by Geriatric and Orthopaedics. WSHFT•All SEH CCG activity is performing under the contract plan. Risks: Risks:
80%
<Q1 (RSCH 57 / WSHFT 75)
1 (RSCH) / 3 (WSHFT)
•The 95% target was not achieved in January. The operational structure has been changed to merge A&E and the Emergency Assessment Unit to strengthen working between the departments. •WSHFT: The Trust achieved the A&E target in Q3 with 95.4%; the target was achieved in January.
Target0
15%95%
0n/a
Performance
Commentary:
Contracts Finance & Workforce
•RSCH: The A&E Q3 performance was 93.9%. An improved IT tracking system is being developed.
•Increased RSCH activity
Commentary:
•RSCH: Financial performance was a little ahead of plan in Month 9, with above plan commissioned income offset by continued pressure on temporary pay costs.•WSHFT: The existing forecast is dependent upon achieving the Cost Improvement Targets and achieving the patient and quality safety targets.
Quality
*Projected position based on December activity
•WSHFT achieving target surplus
•RSCH: The annual C.diff trajectory of 14 has been exceeded with 20 reported cases YTD; there has been one case involving a SEH patient. An action plan has been submitted to Monitor and they are being regularly updated on progress.•WSHFT: C.diff annual trajectory is 46 with 44 reported cases YTD; there have been no cases involving SEH patients.
11�Performance�Report.pdf
Top
Overall�Page�138�of�237Page�19�of�22

19
Southern Health NHS Foundation Trust
This dashboard provides an overview of Southern Health NHS Foundation Trust’s (SHFT) performance from the quality, performance, contracts and finance perspectives.
Target December Year to Dec Community Hospitals: Target DecemberHCAI - MRSA 0 0 G 0 G Bed occupancy 85% 92.0% GHCAI - C.diff. 6 0 G 3 G Delayed Transfer of Care (DTOC) 7.5% 9.6% ANever events 0 0 G 0 G RTT admitted patients <18weeks 90% 98.1% GMSA breaches 0 0 G 0 G RTT non-admitted patients <18weeks 90% 99.3% G
Community Community Care Teams: F&G SEHPatient satisfaction n/a 96% 97% Response within 2 hours 80% 89.3% G 84.0% GHigh harm falls n/a 0 5 Receiving treatment within 3 weeks 90% 92.0% G 92.0% GNumber of SIRIs n/a 25 221 End of life - dying in preferred location 80% 100% G 75.0% ANumber of complaints received n/a 23 155 < 3 working days 95% 100% n/a Mental Health: F&G SEH
Care Programme Approach 12m review 95% 95.1% G 97.3% GMental Health: CPA 7 day follow up 95% 100% G 100% GPatient satisfaction n/a 90% 86% Seen within 7 weeks 90% 95.3% G 95.4% GHigh harm falls n/a 1 14 DTOC 7.5% 5.1% G 5.1% GNumber of SIRIs n/a 5 71Number of complaints received n/a 10 160p g < 3 working days 95% 80% n/a Commentary:
Commentary:
Risks: Risks:
Year to January Annual Year to Dec* AnnualTarget Actual Var. Target Forecast Var. Plan Actual Var. Plan Forecast Var.
£m £m £m £m £m £m £m £m £m £m £m £mSpend: Finance:Fareham & Gosport - Mental Health 13.0 13.0 0 G 15.5 15.5 0 G 0.4 0.8 0.4 G -1.2 -2.4 -1.2 RFareham & Gosport - Community 6.3 6.3 0 G 7.6 7.6 0 GSouth Eastern Hampshire - Mental Health 12.2 12.2 0 G 16.3 16.3 0 G *Latest figures availableSouth Eastern Hampshire - Community 10.5 10.5 0 G 14.0 14.0 0 G
WorkforceStaff sickness 3.5% 4.8% 1.3%
Commentary: Commentary:
Risks: Risks:
•The mental health high harm fall in December involved an inpatient at Gosport War Memorial Hospital.
•No major risks identified
Contracts Finance & Workforce
Quality
•No major risks identified •Data quality issues
Performance
Surplus / -deficit
•The Trust is embedding a health and well-being strategy which will seek to improve organisational performance in sickness absence.
•DTOCs at Petersfield have reduced again. Days lost were due to social care, with two patients awaiting specialist equipment or adaptations in order to go home.
•No major risks identified
•The reporting for end of life has changed recently. Southern Health is investigating whether the reporting is a data quality issue or if this is correct reporting.
•The Q1 and Q2 payments for the National CQUINs is in the process of being signed off. Until this is finalised it should be assumed that SHFT may earn all of the allocated financial value.
11�Performance�Report.pdf
Top
Overall�Page�139�of�237Page�20�of�22

20
South Central Ambulance Service
SCAS Trust SEH CCG
Response Times Target Dec-13 Q3 YTD Dec-13 Q3 YTD
Category A calls within 8 minutes – Red 1 75% 79.5% 78.6% 78.9% 72.2% 74.3% 71.3%
Category A calls within 8 minutes – Red 2 75% 75.5% 75.1% 75.9% 71.1% 72.7% 73.9%
Category A calls within 19 minutes – Red 19 95% 95.7% 95.5% 95.6% 92.9% 94.1% 94.3%
• The three response time targets were achieved at trust level for SCAS in December, however, the targets were not achieved at CCG level.
• SCAS report that the underperformance in the South Eastern Hampshire area is due to increased activity, ambulance queuing and the availability of crews/vehicles. SCAS has been asked to benchmark activity/performance against other providers and whole system programmes are in place.
• The CCG quarterly Assurance Framework assessment for ambulance response times at trust level was achieved in Quarter 3. The CCG
Quality Premium is assessed on the Red 1 measure at trust level and is currently being achieved.
• The three response times were achieved at trust level in January.
Month Year to Date
Target Dec-13 Target YTD
FAST patients to centre in 60 minutes 53.5% 45.1% 51.5% 45.0%
Hear & Treat (telephone advice) 6.9% 5.0% 5.8% 4.6%
Non-conveyance to A&E 42.6% 40.6% 41.9% 40.3%
See & Treat re-contacts within 24 hours 6.4% 6.5% 6.7% 6.6%
• An audit into Face, Arms, Speech and Time (FAST) patient breaches has identified the SCAS operational areas which need attention and improvement. SCAS are working with two neighbouring trusts to ascertain best practice and improvement initiatives to increase performance.
• Hear & Treat monthly and annual trend continues to show improvement. SCAS report that continued clinical vacancies (recruiting the right calibre of staff), limit any further improvement.
• Conveyances to A&E remain above plan due to the higher levels of acuity in 2013/14 compared to 2012/13.
The tables below show the December performance for South Central Ambulance Service (SCAS). The response times performance is reported at trust level and CCG level for South Eastern Hampshire.
11�Performance�Report.pdf
Top
Overall�Page�140�of�237Page�21�of�22

21
NHS 111 and Out of Hours
Target Nov-13 Dec-13
NHS 111
Calls offered to the service - 35,931 41,250
Abandoned calls <5% 0.9% 2.6%
Call waiting time (60 seconds) 95% 96.3% 90.3%
Transfer to 999 <10% 6.5% 8.3%
Advised to attend A&E <5% 6.5% 6.0%
Target Nov-13 Dec-13
Out of Hours
Urgent response <15 minutes 95% 94.5% 91.3%
Routine response <60 minutes 95% 88.4% 82.9%
Routine response <120 minutes 95% 97.3% 92.5%
Routine response <180 minutes 95% 99.1% 97.3%
Face to Face Consultations Primary Care Centres
Emergency <15 minutes 95% 100% 100%
Urgent <120 minutes 95% 88.5% 92.0%
Routine <360 minutes 95% 98.5% 95.6%
Face to Face Consultations Home Visits
Emergency >60 minutes 95% 100% 50.0%
Urgent <120 minutes 95% 93.2% 90.6%
Routine <360 minutes 95% 97.5% 89.8%
NHS 111
• Additional demand and staff sickness in December affected the call waiting time within 60 seconds standard. Actions to improve performance include:
o A review of the hours the standard was not achieved and ensuring that staffing and call volumes are correct going forward.
o Ensuring best utilisation of staff by offering overtime and asking staff to move shifts to ensure best use of cover.
• Performance has shown improvement in January, however, staff sickness continues to be reported as the primary reason for breaches. SCAS will manage the staff concerned through the sickness and capability policy.
Out of Hours • Factors which have affected response times in December:
o The quality of incoming referrals. A number of cases have been identified by clinical leads and fed back to the NHS 111 provider for further investigation.
o The scale of repeat prescription demand. Options are being considered for the re-direction of repeat prescription requests before they are referred to Out of Hours.
o Mental health cases grew significantly during the holiday period. Commissioner intervention is underway but has yet to change crisis cover to ensure Out of Hours cover is able to sustain the demands.
• Primary Care Centres (PCCs) experienced increased demand. Additional clinic capacity has been opened in Queen Alexandra Hospital (QAH) PCC where demand has been greatest.
• There was an increased number of cases demanding home visits over the holiday period. 11�Performance�Report.pdf
Top
Overall�Page�141�of�237Page�22�of�22

GOVERNING BODY Date of Meeting 19th March 2014
Agenda Item No
12 Title
Joint CCG Governing Body Quality Report Purpose of Paper
To provide the Governing Body Members exception reports regarding quality and safety including: • CCG Joint Quality Assurance Committee proceedings
February 2014 • Portsmouth Hospitals NHS Trust (PHT) • South Central Ambulance Service NHS Foundation Trust
(SCAS) 999 Services • Southern Health NHS Foundation Trust (SHFT) • Sussex Partnerships Child and Adolescent Mental Health
services (CAMHs) • University Hospitals Southampton Foundation Trust (UHSFT) • Royal Surrey County Hospital Foundation Trust (RSCHFT) • SCASFT 111 Service • Care UK Havant Diagnostics/Out of Hours Service • Quality Team Internal Risk Register • Healthcare Associated Infections (HCAI) • CCG Enquiries, Concerns and Complaints • Serious Incidents Requiring Investigation (SIRI)
Recommendations/ Actions requested
The Governing Body is asked to: • note the report
Author
Louise Spencer Deputy Chief Quality Officer
Sponsoring member
Julia Barton Chief Quality Officer
Date
12th March 2014
12�Joint�CCG�Quality�Report.pd
Top
Overall�Page�142�of�237Page�1�of�15

Joint Quality Report
Governing Body Report
March 2014 Reporting Period up to Month 9 (Q3)
Louise Spencer Deputy Chief Quality Officer
1 12�Joint�CCG�Quality�Report.pd
Top
Overall�Page�143�of�237Page�2�of�15

Joint Quality Report Index Page (s) Item
3 CCG Joint Quality Assurance Committee proceedings February 2014
4-5 Provider Exception Report: Portsmouth Hospitals NHS Trust (PHT)
6 Provider Exception Report: South Central Ambulance Service NHS Foundation Trust (SCAS) 999 Services
6-7 Provider Exception Report: Southern Health NHS Foundation Trust (SHFT)
8 Provider Exception Report: Sussex Partnerships Child and Adolescent Mental Health services (CAMHs)
9 Provider Exception Reports: University Hospitals Southampton Foundation Trust (UHSFT) Royal Surrey County Hospital Foundation Trust (RSCHFT)
10 Provider Exception Reports: SCASFT 111 Service Exception Report Care UK Havant Diagnostics/Out of Hours Service Exception Report
11 Quality Team Internal Risk Register Exception Report
12 Healthcare Associated Infections (HCAI) Exception Report
13 CCG Enquiries, Concerns and Complaints Exception Report
14 Serious Incidents Requiring Investigation (SIRI): Exception report
12�Joint�CCG�Quality�Report.pd
Top
Overall�Page�144�of�237Page�3�of�15

The CCG Joint Quality Assurance Committee Proceedings
The Joint Quality Assurance Committee met on 12th February 2013 and accepted the following reports:
A quality strategy, planning and priorities update report The revised Quality Assurance Committee (QAC) and Quality Operational sub-group (QOG) Terms of Reference An integrated quality report including:
CCG non - provider quality risk register (risks 12 and above) An enquiries, concerns and complaints report (Q3) A Healthcare Associated Infection (HCAI) report (Q3) A Serious Incidents Requiring Investigation (SIRI) exception report and revised SIRI panel terms of reference The final version of the revised complaints policy, including an update on the complaints information leaflet
and general guidance sheet A provider report including:
The provider risk register (risks 12 and above) A quality analysis report on Royal Surrey County Hospital Foundation Trust (RSCHFT) An update on progress with the provider quality contract negotiations 14/15
A update on the development of a CCG quality surveillance hub A clinical visits report outlining visits and themes over the year to date Updates from the Community Engagement Committees (CEC) for both Fareham and Gosport and South Eastern
Hampshire CCGs A safeguarding children report A vulnerable persons/safeguarding adults report and update from the Hampshire Safeguarding Adults Board (HSAB) An update from the Wessex Quality Surveillance Group meeting
There were no issues identified from the Joint Quality and Safety Committee to escalate to the Governing Body. Committee minutes and papers are available for Governing Body members to review on request.
3 12�Joint�CCG�Quality�Report.pd
Top
Overall�Page�145�of�237Page�4�of�15

Portsmouth Hospitals NHS Trust (PHT) Exception Report (1)
The CQC Intelligent Monitoring score of 4 is noted for PHT (October 2013). This is based on a set of national quality and safety metrics collected and analysed by the CQC for acute hospitals. Band 1 is the highest concern and band 6 is the least concern. Further information on CQC intelligent monitoring can be accessed at: http://www.cqc.org.uk/public/hospital-intelligent-monitoring
Discharging patients from hospital: Several examples have been raised indicating that the quality of discharge may not be optimum for some patients; a commissioner letter has been sent to the Trust requesting a quality assurance review and report. The analysis of a range of information is being undertaken. Safe and timely discharge from hospital is reviewed monthly at the Clinical Quality Review Meeting (CQRM); this includes the monitoring of contractual requirements for issuing comprehensive discharge summaries in a timely manner, which continue to be challenging for the Trust.
Healthcare Acquired Infection The Trust is experiencing challenges with meeting the individual nationally set reduction target for Clostridium difficile (CDI) infections; to have no more than 30 cases in 2013/14. These challenges have also been identified in the local communities and nationally. For context, since 2007 a radical reduction of CDI cases has occurred nationally; the levels of cases occurring now in the population are very small in comparison. However to ensure continuous review and improvement the hospital is working closely with the CCGs and other local health partners to identify any areas that could be addressed; for example the clinical environment, clinical practice, appropriate prescribing of antibiotic therapy and review of other medications for patients who have higher risk factors. 1 MRSA bacteraemia has been reported in January 2014 and has been subject to a Post Infection Review (national requirement). Early indication would suggest this infection was avoidable and the Trust is working to identify learning and will implement any actions required in relation to this case.
4 12�Joint�CCG�Quality�Report.pd
Top
Overall�Page�146�of�237Page�5�of�15

Portsmouth Hospitals NHS Trust (PHT) Exception Report (2)
Friends & Family Test The CCGS’ Quality Team and the Wessex Area Team of NHS England have undertaken a detailed review and analysis with the Trust to identify why the Trust has scored low nationally. Areas for action were identified and work is in progress; early indicators are showing some improvement in inpatient scores. The January 2014 score has increased to 72.2 which brings the Trust in line with other acute hospitals in Wessex
Ophthalmology waiting list backlog The overall picture is improving, with prioritisation systems and consultant triage in place. A reduction in the backlog has been reported, with increased capacity. The management of demand through the community based screening programme is planned. Monitoring continues monthly through the CCG at CQRM.
Quality of care delivery and staff wellbeing In light of increased challenges of capacity and demand the Trust is reporting and analysing a variety of quality data and working with the CCG on the process of identifying any potential impact on quality and contingency planning. The NHS Staff Survey Results were published the end of February 2014 and these will be analysed.
Emergency Department (ED) The CCGs had requested assurance on the quality and safety for patients attending the ED department as consistent patient queues are occurring. A quality review has been undertaken with agreed actions completed including: Increase staffing in ED An urgent care centre in ED A positive commissioner visit occurred in January 2014, and the Friends and Family Test (FFT) ED score is above national average. A focus on the quality of care for patients in ED will be a feature every other month on the CQRM agenda. The CCG will continue to monitor FFT responses.
Cancer Services The CCG continues to monitor quality in cancer services due to the Trust breaching the 2 week wait target and as a result of the Trust scores in the national cancer patient experience survey. Actions continue internally in the Trust in the areas of recruitment and to improve patient experience. Monitoring continues through the CCG via the commissioning team and at CQRM.
5 12�Joint�CCG�Quality�Report.pd
Top
Overall�Page�147�of�237Page�6�of�15

South Central Ambulance Foundation Trust (SCASFT) 999 Services Exception Report
Long Waits (Across Hampshire and Thames Valley) SCASFT are reporting that patients are experiencing long waits for all categories of calls. A review is planned at the March 2014 CQRM to understand why this is the case and how this can be improved. A review of the protocol for GP Urgent calls and actions to improve GP communication is underway.
Stroke patients The ambulance Trust is experiencing challenges in meeting the target response times for stroke patients. An improvement action plan had been in place during the year, which has not altered outcomes. Therefore further analysis has been undertaken to identify the challenges in reaching specialist stroke centres against the requirements for on scene times. This has executive level input in the Trust. The CCG has reviewed a robust plan with improvement trajectories in February 2014 and is expecting receipt of progress against the plan at the March CQRM. Monthly monitoring continues via the overarching Contract Review Meeting and the Clinical Quality Review Meetings.
Safeguarding Previous concerns had been raised over safeguarding capacity in the Trust. Positive progress has been made including an increase in safeguarding capacity, a peer review has been undertaken with suggested recommendations and monitoring continues at CQRM. Further support is being given for the Serious Case Review reporting requirements.
Southern Health Foundation trust (SHFT) Community Care Team Exception Report
Pressure Ulcers SHFT community services are reporting increased incidences of grade 3 and 4 pressure ulcers in peoples homes. The Trust is on target to achieve the point prevalence reduction target for pressure ulcers this year and analysis shows that the Trust is similar to the national average for pressure ulcers acquired as a result of direct care. Monitoring continues at CQRM. Good practice incudes:. Whole system working through the Stamp out Sores project A good reporting culture, including pressure ulcers which did not necessarily arise from SHFT direct care delivery (initial analysis
shows 65% pressure ulcers occurring in patient own homes ) A Wessex wide pressure ulcer summit is being held on the 14th March focusing on patient experience, prevention, risk
assessment and grading
12�Joint�CCG�Quality�Report.pd
Top
Overall�Page�148�of�237Page�7�of�15

Southern Health Foundation trust (SHFT) Mental Health and Learning Disability Services
Exception Report Access to Mental Health services Quality concerns have arisen, across the whole health system in connection with access to mental health services and Section 136 patients. A number of incidents have been reported in connection with this. A panorama programme was broadcast outlining the difficulty of appropriate assessment if a patient is intoxicated. SHFT are working across the health economy with health and social care partners to address this. Current areas of work are: The Section 136 pathway development is in progress, led by Dr James Hogan in NHS Portsmouth CCG The start of a pilot in January 2014 called “Serenity”. This pilot includes Mental Health Staff undertaking joint shifts with the
Police in a combined service across areas of Hampshire to establish stronger community links Monitoring continues via the Lead Commissioner West Hampshire CCG with local CCG quality and vulnerable adults team input.
Care Quality Commission (CQC) visits The CQC has visited some care provision areas in SHFT outside of the F&GCCG and SEHCCG geographical area in Hampshire. Care areas were Antelope House, Parklands Hospital and Melbury Lodge. The CQC has requested some actions in relation to some aspects of care delivery at these places. As a result of this information, the CCG quality team has made a clinical visit to the local Elmleigh psychiatric intensive care unit in Havant, which includes a 136 suite and Electroconvulsive Therapy (ECT) suite. The “Hospital at home” team is also based at this unit. The clinical visit was positive overall, with the service demonstrating a good governance structure and processes within the unit. The staff were engaged with patient safety, experience and quality improvement. Ongoing monitoring of SHFT includes: Bi-monthly assurance reports from WCCG Locality presence at CQRM A review of the assurance mechanisms for services within the locality Out of Hampshire areas visited by CQC include Learning Disabilities (LD): Slade House and John Sharich House. The Trust has received enforcement notices in relation to these services and NHS England has subsequently held a risk summit which identified key work streams to progress, with a follow up meeting planned for March 2014. The LD service pathway in Oxford is under review and there are plans to implement the Hampshire model. Monitoring continues via the Lead Commissioner (West Hampshire CCG) with local CCG quality and vulnerable adults team input.
12�Joint�CCG�Quality�Report.pd
Top
Overall�Page�149�of�237Page�8�of�15

Sussex Partnerships Child & Adolescent Mental health Services (CAHMS) Exception Report
Quality Monitoring There have been insufficient quality indicators in this contract and the joint CCG quality team, in partnership with the Lead Commissioner (North East and Farnham CCG) have made progress to develop and agree additional key quality indicators. Monitoring continues at monthly CQRM via the Lead Commissioner with local CCG attendance
Staff Feedback The Trust has initiated a listening exercise with staff to look at culture and staff satisfaction. As a result of some concerns raised by staff around the level of staffing and resource to meet a safe and effective service, multidisciplinary work sessions have undertaken to identify more effective and supportive ways of working. This has had positive feedback from clinical staff. A local leadership team has been developed in Basingstoke. The Trust is further recruiting to posts, including Tier 4 (specialist commissioning) services at Leigh House.
Section 136 The Trust acknowledges the national challenge with children and adults being kept in police cells under Section 136 as a “place of safety”. This issue was raised at January CQRM. Although rare, the impact for the person under 18 is extreme. The Trust is working with police to provide information on access to services out of hours and consideration of alternative
options , with risk management plans being shared The Trust is determining the level of risk and numbers of children affected locally This will be a focus item with a review paper in March CQRM
Autism It has been recognised that the provision of care for patients with autism is inconsistent across Hampshire and may lead to lengthy waiting times for assessment and support - autism pathways are being reviewed by the commissioning team.
8 12�Joint�CCG�Quality�Report.pd
Top
Overall�Page�150�of�237Page�9�of�15

University Hospitals NHS Foundation Trust (UHSFT) Exception Report
The CQC Intelligent Monitoring score of 2 is noted for UHS (October 2013). This is based on a set of national quality and safety metrics collected and analysed by the CQC for acute hospitals. Band 1 is the highest concern and band 6 is the least concern. Further information on CQC intelligent monitoring can be accessed at: http://www.cqc.org.uk/public/hospital-intelligent-monitoring
The Foundation Trust (FT) is experiencing challenges in consistently meeting the 4 hour performance targets in the Emergency Department (ED). The quality team has raised this concern with the Lead Commissioner (Southampton City CCG) to enquire about the quality and safety assurances and are awaiting a response.
Royal Surrey County Hospital NHS Foundation Trust (RSCHFT) Exception Report
The CQC Intelligent Monitoring score of 2 is noted for RSCFT (October 2013). This is based on a set of national quality and safety metrics collected and analysed by the CQC for acute hospitals. Band 1 is the highest concern and band 6 is the least concern. Further information on CQC intelligent monitoring can be accessed at: http://www.cqc.org.uk/public/hospital-intelligent-monitoring
An in-depth quality analysis paper was presented to the Quality Assurance Committee in February 2014 The Quality Assurance Committee discussed and accepted the conclusions and recommendations in the paper The committee is assured that governance monitoring processes are in place via the CCGs Quality team and the lead
commissioner (Guilford and Waverly CCG) Improvement plans for the areas of concern have been or are in the process of being agreed with the lead commissioner and
RSCHFT Findings from the latest CQC inspection did not identify any “MUST DO” actions and services were described as “overall the trust
was providing services that were safe, effective, responsive, caring and well – led. However, there were some areas for improvement
9 12�Joint�CCG�Quality�Report.pd
Top
Overall�Page�151�of�237Page�10�of�15

South Central Ambulance Foundation Trust (SCASFT) 111 Service
Exception Report The service is currently undertaking a patient satisfaction survey; the results of which will be published in March 2014.
111 Feedback
Care UK: Out of Hours (OOH) and Havant Diagnostic Centre Exception Report
Havant Diagnostics Did Not Attend (DNA’s) and late/cancellation of appointments In the last two quarters DNA’s and cancellation of appointments has risen in both Havant Diagnostics and St Marys Treatment Centre. Care UK is working with a sample of general practices to ensure up-to-date patient details and has increased the amount and spread of contact calls.
Out of Hours Improved outcomes from the patient satisfaction survey The monthly data is showing improved scores in almost every section. H Docs medical leads will ensure continuous efforts are made to raise awareness and ensure all staff are compliant with high quality standards.
Information supplied by NHS Portsmouth CCG Quality Team (Lead Commissioners for SCASFT 111 service and Care UK) 10 12�Joint�CCG�Quality�Report.pd
Top
Overall�Page�152�of�237Page�11�of�15

Joint Quality Team internal Risk Register Exception Report The quality team risk register is updated on a monthly basis. The risk register identifies any areas of concern within the quality team and outlines mitigating actions. The quality risk register is a sub register of the Board Assurance Framework. The risk register was reviewed by the Deputy Chief Quality Officer on the 3rd February 2014. Changes are: Risk 11 (CAMHs) has been transferred to Provider Risk register and risk rating increased to 16 Please see Quality Team Provider Risk register for provider quality risks The top 4 internal quality team risks that remain rated 12 and 16 are:
No Risk and scoring Controls in place Actions planned
04
16 Gaps in designated doctors for safeguarding children and looked after children in Hampshire
• West Hampshire hosting arrangements July 2013 with action plan in place
• January 2014 Section 11 audit completed and SG nurse in post.
National recognition that the model requires revision by PCP and National Leads
Options for a new model have been circulated
March 2014 – unchanged, risk remains 16
05 16 Challenging C. difficile reduction targets for both CCGs, over yearly allocated CCG reduction target
• Successful recruitment to post • Assurance on provider HCAI plans for
2013/14 sought • IPC training for Practice Nurses completed
in January for both CCGs • 4 hours a week IPC specialist nurse cover
(micro surveillance) secured
Recovery plan in place RCA's continue on cases in SEHCCG Ongoing work continues however remains
high risk Microbiology support and review of
hospital cases for F&GCCG GP Link nurse networks to be revived
13 12 Lack of robust assurance of the OOH contract development and monitoring in relation to quality metric development and SIRI performance management through Lead CCG (Portsmouth)
• Close liaison between Quality Teams (QT) • Involvement of the QT in contribution to
metrics • Assurance reports requested monthly on
provider to Portsmouth CCG • Head of Quality attends Clinical
Governance meetings
Combined SIRI panels to support Portsmouth CCG quality team transition
New quality requirements under development
12 12 CCG unable to access Personal Identifiable Information due to Information Governance restrictions on CCGs with a potential impact on quality and safety monitoring e.g. infection control (National Risk)
• NHS.net addresses for SIRI and Safeguarding correspondence
• Secure storage on L drive for any data • IG training completed by all team • Specialist IPC nurse secured from Solent
NHS Trust for 4 hours a week for microbiology surveillance
Further completion of HCAI recovery plan Continued guidance from IG team
12�Joint�CCG�Quality�Report.pd
Top
Overall�Page�153�of�237Page�12�of�15
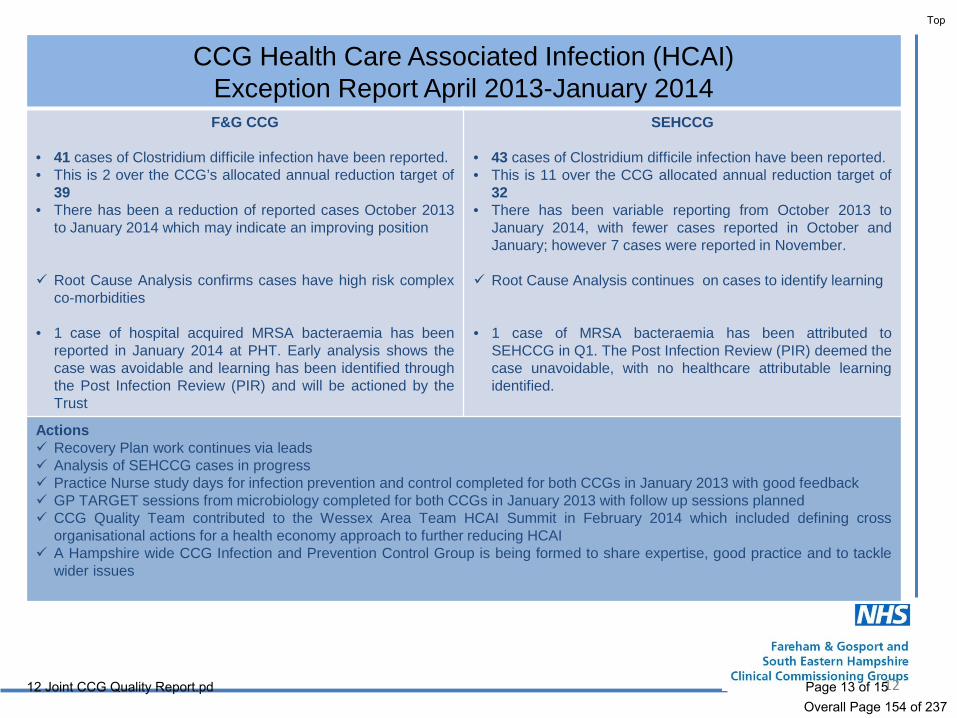
CCG Health Care Associated Infection (HCAI) Exception Report April 2013-January 2014 F&G CCG
• 41 cases of Clostridium difficile infection have been reported. • This is 2 over the CCG’s allocated annual reduction target of
39 • There has been a reduction of reported cases October 2013
to January 2014 which may indicate an improving position Root Cause Analysis confirms cases have high risk complex
co-morbidities • 1 case of hospital acquired MRSA bacteraemia has been
reported in January 2014 at PHT. Early analysis shows the case was avoidable and learning has been identified through the Post Infection Review (PIR) and will be actioned by the Trust
SEHCCG • 43 cases of Clostridium difficile infection have been reported. • This is 11 over the CCG allocated annual reduction target of
32 • There has been variable reporting from October 2013 to
January 2014, with fewer cases reported in October and January; however 7 cases were reported in November.
Root Cause Analysis continues on cases to identify learning • 1 case of MRSA bacteraemia has been attributed to
SEHCCG in Q1. The Post Infection Review (PIR) deemed the case unavoidable, with no healthcare attributable learning identified.
Actions Recovery Plan work continues via leads Analysis of SEHCCG cases in progress Practice Nurse study days for infection prevention and control completed for both CCGs in January 2013 with good feedback GP TARGET sessions from microbiology completed for both CCGs in January 2013 with follow up sessions planned CCG Quality Team contributed to the Wessex Area Team HCAI Summit in February 2014 which included defining cross
organisational actions for a health economy approach to further reducing HCAI A Hampshire wide CCG Infection and Prevention Control Group is being formed to share expertise, good practice and to tackle
wider issues
12 12�Joint�CCG�Quality�Report.pd
Top
Overall�Page�154�of�237Page�13�of�15
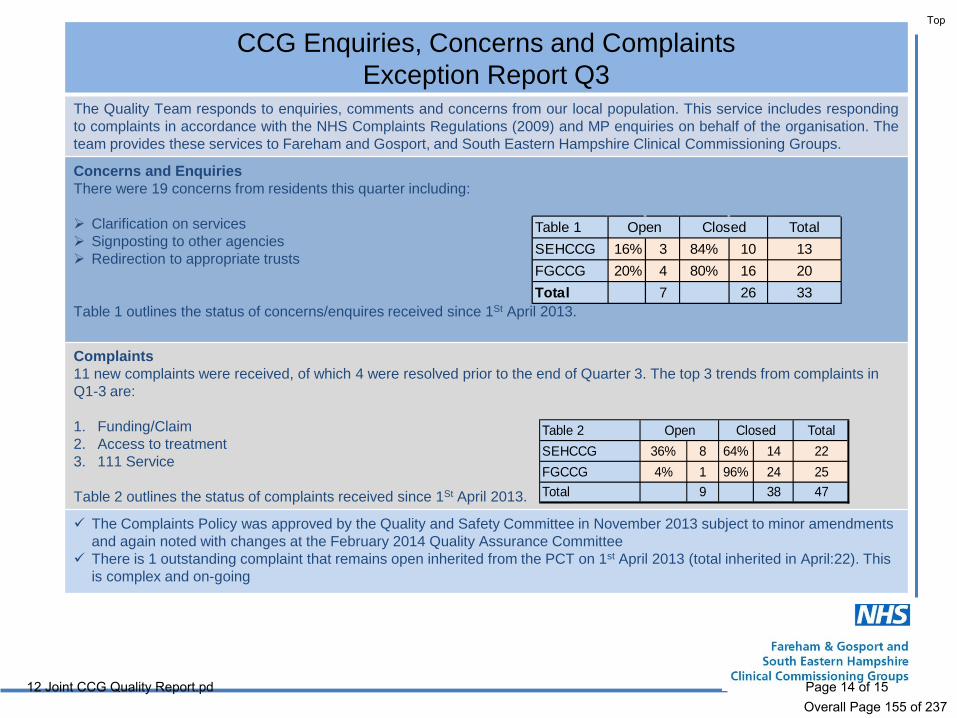
CCG Enquiries, Concerns and Complaints Exception Report Q3
The Quality Team responds to enquiries, comments and concerns from our local population. This service includes responding to complaints in accordance with the NHS Complaints Regulations (2009) and MP enquiries on behalf of the organisation. The team provides these services to Fareham and Gosport, and South Eastern Hampshire Clinical Commissioning Groups.
Concerns and Enquiries There were 19 concerns from residents this quarter including: Clarification on services Signposting to other agencies Redirection to appropriate trusts
Table 1 outlines the status of concerns/enquires received since 1St April 2013.
Complaints 11 new complaints were received, of which 4 were resolved prior to the end of Quarter 3. The top 3 trends from complaints in Q1-3 are: 1. Funding/Claim 2. Access to treatment 3. 111 Service Table 2 outlines the status of complaints received since 1St April 2013.
The Complaints Policy was approved by the Quality and Safety Committee in November 2013 subject to minor amendments and again noted with changes at the February 2014 Quality Assurance Committee
There is 1 outstanding complaint that remains open inherited from the PCT on 1st April 2013 (total inherited in April:22). This is complex and on-going
Table 2 TotalSEHCCG 36% 8 64% 14 22FGCCG 4% 1 96% 24 25Total 9 38 47
Open Closed
Table 1 TotalSEHCCG 16% 3 84% 10 13FGCCG 20% 4 80% 16 20Total 7 26 33
ClosedOpen
12�Joint�CCG�Quality�Report.pd
Top
Overall�Page�155�of�237Page�14�of�15

Serious Incidents Requiring Investigation (SIRI) Exception Report (Q3)
SIRI reported by organisation Quarter 1 to 3
55 SIRI were reported in Quarter 3 53 of the 55 SIRI reported were categorised as Grade 1 (grading information can be accessed through the below hyper link) The top 3 Grade 1 incidents reported were:
• Pressure Ulcers • Slips/Trips/Falls • Venous Thromboembolism (VTE)
2 incidents were Grade 2 both being categorised as ‘Ambulance General’ Key Themes of investigations: Risk assessment – not completed or not timely Stock piling medicines at home leading to overdose/suicide Communication – between providers and around discharge
(NHS England Serious Incident Framework http://www.england.nhs.uk/wp-content/uploads/2013/03/sif-guide.pdf)
The Joint CCG Quality Team is working with Portsmouth CCG Quality Team to develop and provide a CCG review panel across the Compact and has amended the SIRI panel terms of reference to reflect this
The provider contract SIRI and Safeguarding schedules have been refreshed for the 14/15 contract year The CCG Quality Team performance manages SIRI investigations within the national guidance with regard to review and closure
timeframes.
14
SIRI raised per Month/QuarterOrganisation Apr 13 May 13 Jun 13 Jul 13 Aug 13 Sep 13 Oct 13 Nov 13 Dec 13 Grand TotalNHS Fareham And Gosport CCG - Provider 2 2NHS South Eastern Hampshire CCG - Provider 1 1Portsmouth Hospitals NHS Trust 12 17 9 14 10 5 8 8 5 88South Central Ambulance Service NHS FT 2 1 1 2 1 3 2 1 13Southern Health NHS Foundation Trust 4 5 7 7 9 9 8 9 11 69Grand Total 19 23 17 23 22 14 19 19 17 173
Quarter 1 Quarter 2 Quarter 3
12�Joint�CCG�Quality�Report.pd
Top
Overall�Page�156�of�237Page�15�of�15

GOVERNING BODY Date of Meeting 19th March 2014
Agenda Item No
13 Title
Commissioning Update Purpose of Paper
To inform the Governing Body of the Commissioning workstreams.
Recommendations/ Actions requested
The Governing Body is asked to: • Note the report
Author
Alex Berry Chief Commissioning Officer
Sponsoring member
Alex Berry Chief Commissioning Officer
Date
12th March 2014
13�Commissioning�Update.pdf
Top
Overall�Page�157�of�237Page�1�of�3

Commissioning Briefing Paper
1.0 Introduction 1.1 This paper is to brief the Governing Body on key areas of commissioning that are being
undertaken for South Eastern Hampshire CCG. 2. 18 Week Referral to Treatment 2.1 Referral to Treatment performance at Portsmouth Hospitals Trust (PHT) continues to be
below national targets for admitted and non-admitted at speciality level. 2.2 As part of the formal contractual process, a CQN meeting was held on 7th January 2014
with Portsmouth Hospitals NHS Trust to discuss a Remedial Action Plan (RAP) to address the issues that prevent the Trust from achieving sustainable specialty level RTT performance.
2.3 The submitted plan was not felt to contain sufficient assurance at speciality level on the management of the backlog. This was escalated to the Portsmouth and South Eastern Hampshire Commissioning Committee, where performance and actions to date were discussed and it was agreed to continue with the CQN. This is now with the Commissioning Support Unit to progress.
3. Specialist Musculoskeletal and Persistent Pain Procurement 3.1 Solent NHS Trust, as the preferred Bidder for this service, is now at the final stages of
implementing mobilisation plans to provide a persistent pain self-management and Specialist Musculoskeletal service for our local population. This new service development addresses the gaps in service raised by our local clinicians and patients around the need for a community pain service with improved access to specialist physiotherapy and psychology.
4. Cancer 4.1 Sustained achievement of the cancer waiting time targets (CWT) remains an area of
challenge within Portsmouth Hospitals Trust (PHT) predominantly within urology, colorectal and dermatology.
4.2 As part of the formal contractual process, a CQN meeting was held on 7th January 2014 with Portsmouth Hospitals NHS Trust to discuss a Remedial Action Plan (RAP). As the plan was not felt to contain sufficient detail this was escalated to the Portsmouth and South Eastern Hampshire Commissioning Committee, where it was agreed to continue with the CQN. This is now with the Commissioning Support Unit to progress.
5.0 Urgent and emergency Care 5.1 The front door urgent care model is currently a proof of concept model and is staffed seven
days a week from 8.00am – 6pm. The service was originally anticipated to see around 32 patients per day, however average daily performance is currently around 17 patients. Commissioners are working with providers to establish whether the increase in filled nursing slots will improve flow within the Centre.
1
13�Commissioning�Update.pdf
Top
Overall�Page�158�of�237Page�2�of�3

5.2 In February, the GP clinical leads visited the Urgent Care Centre in Basingstoke.
Commissioners hope to use the learning from this visit to identify potential opportunities to improve the service further during the proof of concept stage.
5.3 The Centre is under constant review and as part of the evaluation process commissioners
have worked with providers to gather feedback on their perception of the way the Centre works and this will be viewed in conjunction with performance against the set Key Performance Indicators. These recommendations will be presented at the individual CCG Clinical Cabinets/Committees for consideration
5.4 The Out of Hours service has failed a number of targets around Routine Response <60
minutes and home visits. Care UK is looking to introduce direct booking into the service so that the NHS 111 service, which is commissioned separately, would automatically transfer the call to either a Primary Care Centre or Home Visit as appropriate. This could improve the 60 minute call response target which has not been achieved during the duration of the contract; however this will need to be discussed with commissioners once the provider has submitted a detailed plan around the potential impact of any changes.
5.5 The delivery of the 4hour ED target within Portsmouth Hospitals Trust remains
unacceptably poor despite good work across the system that has seen an improvement in a number of other metrics such as a reduction in non-elective admissions, reduction in delayed transfers of care. The system met with the TDA and NHSE to review performance and actions being taken. As a consequence, a revised system wide plan is being developed supported by a clear diagnosis of the issues. Governance arrangements are also being strengthened.
6.0 Recommendations 6.1 The South Eastern Hampshire Clinical Commissioning Group Governing Body is
requested to note the commissioning update.
2
13�Commissioning�Update.pdf
Top
Overall�Page�159�of�237Page�3�of�3

GOVERNING BODY Date of Meeting 19th March 2014
Agenda Item No
14 Title
Chase Project Update Purpose of Paper
To update the Governing Body on the current position related to the Chase Hospital redevelopment and the development of enhanced models of care for the population of Whitehill and Bordon and the surrounding area.
Recommendations/ Actions requested
The Governing Body is asked to: • note progress of the project to redevelop the Chase Hospital,
Bordon and endorse the additional capital spend of up to £600k, therefore the new project value is £3.5m
• endorse the new project timescales for late completion, now anticipated to be summer 2015
• endorse the vision of creating a community well-being hub with traditional medical services supported by community wellbeing and voluntary sector services.
Author
Lisa Medway Chase Redevelopment Project Manager
Sponsoring member
Sara Tiller Chief Development Officer
Date
13th March 2014
14�Chase�Project�Update.pdf
Top
Overall�Page�160�of�237Page�1�of�6

Chase Community Hospital Redevelopment 1. Introduction
1.1. The purpose of this paper is to update the Governing Body on the progress of the Chase Hospital redevelopment project.
1.2. In addition to a general update on progress, the business case development and
project risks, the paper also describes the emerging thinking for extending the use of the hospital to provide health and well-being services.
2. Background
2.1. Following on-going uncertainty about the future of Chase Community Hospital for a
number of years, in 2011 the NHS held a six week public consultation on how to develop the right services on the hospital site and make sure that people have access to the highest quality care. This enabled a range of options to be considered. The option selected was to create an integrated care team to provide support services to patients in their own homes, and commission four nursing home beds to provide inpatient care if needed. The preferred option also proposed that the hospital would then be redeveloped to provide a vibrant range of services to meet the needs of local people.
2.2. In particular the redevelopment will involve reconfiguration of the disused ward areas to accommodate two GP practices, as well as a dedicated space for Adult and Older Peoples Mental Health services. This then facilitates the closure of the Elizabeth Dibben Centre. The existing outpatient department will be reconfigured and refurbished. The back of house catering facilities will be reduced and reconfigured to enable additional office accommodation to be created for team bases.
2.3. In March 2013 the CCG’s Governing Body approved the Outline Business Case
(OBC) for the redevelopment of the hospital, as did the Board of Hampshire PCT. The Wessex Area Team of NHS England has re-confirmed their commitment to the project on a cost-neutral basis (as of June 2013). Also in March 2013, the meeting of the Hampshire Health Overview and Scrutiny Committee (HOSC) stated its position that the changes to service provision are in the best interest of the local population. Following a number of recommendations made by HOSC the CCG presented the project again in September 2013 where the HOSC reiterated its support for the project and requested a further progress update in March 2014. This has now been rescheduled for the meeting in April 2014.
2.4. On the 2nd September 2013 four nursing home beds providing, step up, step down, and end of life care at Wenham Holt were commissioned. This enabled the inpatient ward at Chase Community Hospital to be decommissioned. At the same time the enhanced model of community based care with an Integrated Community Care Team working extended hours was implemented. On 21st October 2013 the Chief Quality officer visited Wenham Holt and feedback from this visit, and from GPs and
1
14�Chase�Project�Update.pdf
Top
Overall�Page�161�of�237Page�2�of�6

stakeholders was very positive, with patient experience and levels of care reported as good.
Since that time Stakeholder feedback, including reports from Steering group members has remained extremely positive.
3. Progress 3.1. Since the last report in November 2013 there has been a great deal of progress on
the detail of the project and the overall cost plan. Many of the uncertainties since the last Governing Body report are now known and project risks have mitigation plans.
3.2. Planning Application Planning Consent for the new dedicated entrance to the GP Practices and additional car parking spaces (20 standard bays with 3 accessible bays) was given on 23rd December 2013. No other external works are required to the Hospital.
3.3. Project Costs The Outline Business Case (OBC) presented in March 2013 identified capital project costs as being £2.9m. Following the development of detailed designs over the autumn 2013, project costs were estimated at £4.2m by December 2103. This triggered a first round of value engineering sessions. These sessions involved parties from NHS Property Services; the design team; and CCG representatives interrogating the scope of the project plans, with the aim of bringing the project back into scope and the value down closer to that of the original cost plan presented in the OBC of £2.9m. In January 2014 a projected cost of £3.9m for the scheme was tabled to the Project Board and Steering Group. The Steering Group tasked the project team with finding additional savings and efficiencies By the 29th January 2014 after a number of finance meetings, a reduction in the overall cost of £400k had been realised. It was agreed by all parties represented by NHS England, NHS Property Services and the CCG that the current anticipated cost for the tabled scheme is now £3.5m (incl.VAT). The table below sets out the major changes in cost -
Capital Costs original OBC
current forecast Change
^£000 ^£000 ^£000 Department construction costs 1.547 2.126 0.579 Fees 0.273 0.441 0.168 Fees - NHS Direct 0.074 0.074 Non Works ((removals/ data & telecoms etc.) 0.100 0.089 -0.011 Equipment costs 0.090 0.030 -0.060 Contingency / Risk 0.141 0.169 0.028 Optimism bias 0.312 -0.312 Inflation 0.057 -0.057 VAT 0.448 0.597 0.149 VAT Recovery -0.089 0.089 Total 2.879 3.526 0.647
2
14�Chase�Project�Update.pdf
Top
Overall�Page�162�of�237Page�3�of�6

The cost challenges have primarily been due to having a greater understanding of the building fabric; the supporting infrastructure; rises in inflation and material costs; as well as a change in the way the NHS now accounts for VAT. When the OBC costs were prepared PCTs were able to reclaim VAT on professional fees, as well as a percentage of capital refurbishment costs, under the contracted out rules. However this is not available to NHS Property Services which means that the full impact of VAT is now included in the capital costs.
3.4. Business Case NHS England is responsible for allocating capital for developments like the Chase Community Hospital and business cases under £3m can be submitted through a ‘fast track’ process. As the project value is over £3m it now needs to follow the £3m-£10m process, and be taken through the gateways for this capital development workstream. The anticipated delay by following the “non-fast tracked” process is likely to be in the region of six months but this has not been tested in the new approvals environment. The project Business Case was due to be completed in January 2014, however due to the uncertainty around the scope of works and, therefore, the overall project cost, this has not been possible. The timescales for delivery have been highlighted as a red risk on the project risk register, as the targeted completion in April 2015 is now unlikely. As part of the Business Case process designed by NHS England, all tenants have to commit to an agreement to lease to enable the full business case to be approved. At present, neither GP practice nor Southern Health NHS Foundation Trust have been in a position to enter into negotiations on the Agreement to Lease because rental values can only be determined once a project value has been set. It is anticipated that Southern Health will agree to the heads of terms for the Adult Mental Health Services. The length of time that it could take to get all parties to sign up is identified as a red project risk. A surveyor has been appointed to liaise with the GP Practices to agree terms; a briefing for the surveyor is scheduled for April 2014. The two GP Practice model has been added to the project risk register as a red risk, as the design for the area may need to be reassessed and a new tenant(s) found if the GPs do not commit to the scheme.
3.5. Project Board Restructure The CCG has taken the opportunity to refocus and restructure the project board membership, ensuring that the new structure includes decision makers from partner organisations. The first meeting with the new governance structure is due on 20th March 2014.
3.6. Out Patients The mapping of clinics has been completed however further work to ascertain the utilisation of the existing services is to be carried out. Further work with partnering organisations is to be undertaken shortly to promote Chase Community Hospital. A new MSK service is due to begin operating from Chase Community Hospital in April 2014. The tender for Community Ophthalmology is being evaluated and although it has not been possible to stipulate Chase as a specific site for services the tender does specify that a site in North Hampshire be provided as an operating location. The ISTC contract is due to be tendered in July 2014 (for a one year period) and Chase Community Hospital has been specified as a site for that service.
3.7. Community Wellbeing hub Following greater analysis of the clinics at Chase and the utilisation of those clinics, there remains a significant risk that the outpatient department of Chase Community Hospital is unlikely to be fully utilised. Coupled with this is the development of more
3
14�Chase�Project�Update.pdf
Top
Overall�Page�163�of�237Page�4�of�6

integrated, holistic services for patients with complex needs both in the community and at home, which means that a traditional model of community hospitals offering solely medical outpatient clinics is unlikely to be sustainable in the longer term. Following discussion with the Chase Hospital Steering Group it is proposed that the operating model for Chase Community Hospital be changed from a purely medical facility to a more community well-being focused resource offering support and wellbeing services to the residents of Whitehill and Bordon areas. In this model it is envisioned that medical services will be underpinned by wellbeing and voluntary services, which will support the needs of the whole community. This change of emphasis was broached at the Project Board and Steering Group on 14th February and was met with very positive responses. The CCG will now run a series of stakeholder workshops beginning with the Voluntary Sector on 17th March 2014, where the possibility of redesigning part of the space to offer facilities for providers to run health and well-being support services at the Chase Community Hospital is to be tabled and discussed. The CCG will then actively pursue this to maintain the level of support for additional services by the suppliers. The use of technology is also being investigated and the CCG is in talks about how high-tech equipment on the site could provide more ‘virtual’ appointments and services.
4. Risk 4.1. A full risk register with appropriate mitigation has been developed and is reviewed
monthly at redevelopment team meetings, as well as by the Project Board and Steering Group.
4.2. The greatest risks to the project has been the lack of clarity around the scope of works and therefore the project costs; and the more rigorous NHS Business case approvals process and the NHS PS Land Transaction Approvals processes are likely to have an impact on the intended project completion date. This has impacted on the overall business case and project timeframe. The time taken to secure commitment from the incoming tenants is also a risk to the project programme. It should be noted that delivery for April 2015 is not expected to be met.
4.3. Other than the risks identified within the progress report, recent announcements of
NHS organisational changes within NHS Property Services may have an impact on progress but assurances have been provided that ‘business as usual’ is being adopted in this regard.
4.3.
5. Conclusion and Recommendations 5.1. The project is now subject to delay, due to requirement to finalise the scope of works
and obtain best value as the overall project value is higher than anticipated due to design changes and cost inflation. Rigorous financial interrogation of the overall costs, has been undertaken.
5.2. The Governing Body is asked to note progress of the project to redevelop the Chase Hospital, Bordon and endorse the additional capital spend of up to £600k, therefore the new project value is £3.5m. We hope to mitigate these costs further as risks are eliminated and design freeze is achieved.
Formatted: Font: (Default) Arial, Bold
Formatted: Outline numbered +Level: 2 + Numbering Style: 1, 2, 3, …+ Start at: 1 + Alignment: Left +Aligned at: 0.63 cm + Indent at: 1.4cm
4
14�Chase�Project�Update.pdf
Top
Overall�Page�164�of�237Page�5�of�6

5.3. The Governing Body is also asked to endorse the new project timescales for late completion, now anticipated to be summer 2015.
5.4. The Governing Body is requested to endorse the vision of creating a
community well-being hub with traditional medical services supported by community wellbeing and voluntary sector services.
5
14�Chase�Project�Update.pdf
Top
Overall�Page�165�of�237Page�6�of�6

GOVERNING BODY Date of Meeting 19th March 2014
Agenda Item No
15 Title
Board Assurance Framework Purpose of Paper
To present the Board Assurance Framework to the Governing Body for approval.
Recommendations/ Actions requested
The Governing Body is asked to: • Approve the attached recommendations for amendment to the
Board Assurance Framework • Note the top risk scores
Author
Nikki Roberts Governance and Committee Officer
Sponsoring member
Sara Tiller Chief Development Officer
Date
12th March 2014
15�Board�Assurance�Framework.p
Top
Overall�Page�166�of�237Page�1�of�15

Board Assurance Framework Update
March 2014
Top Risk Scores Risk Ref
Description of Risk and Impact Current Risk Score
Strategic Objective: COR 3-4
There is a risk that Portsmouth Hospitals NHS Trust is unable to improve its 4 hour ED wait position this creates quality and safety risks.
16
Strategic Objective 6: Managing change in the health and social care system while ensuring continuity and improving quality COR 6-2a
There is a risk that 2013/14 QIPP schemes do not deliver the required activity changes resulting in inability to reduce system capacity and cause organisational financial pressures. Significant level of unidentified QIPP.
20
COR 6-8a
There is a risk that Portsmouth Hospital Trust will be unable to deliver the planned financial plan in 13/14 which will create a sustainability challenge for the organisation.
16
COR 6-14
There is a risk that growth and costs are beyond existing assumptions with the result that cost pressures meant the CCG is unable to achieve planned surplus and receive the Quality Premium in 14/15.
15
Strategic Objective 7: Improving quality of care and outcomes for patients COR 7-3
Challenging C. difficile national reduction target for the CCG. 16
15�Board�Assurance�Framework.p
Top
Overall�Page�167�of�237Page�2�of�15

Board Assurance Framework Update
March 2014
Update of Progress and Assurances
Risk Ref
Description of Risk and Impact Amendments
Strategic Objective: Improving experience and outcomes for the frail elderly and people requiring long term care including dementia COR 2-1
There is a risk that primary care providers will not be able to establish functional structures that allow them to work seamlessly with other care providers in delivering integrated care solutions for the frail elderly and individuals with long term conditions.
Amendment to Progress and Assurances:
Project manager in place. Alliance now attend Sustainability Board. NHS IQ programme has been commissioned to focus on primary care development. ICT pilots now established. Pilot clinical leads identified. Admin identified. Reviewed structures and programmes. Re-established groups. Developing service specification for delivery of model
Strategic Objective: Care that is planned is delivered in the best way at the best time in the best place COR 3-1
There is a risk that Portsmouth Hospitals NHS Trust is unable to sustain national performance requirements for Referral to Treatment time.
Amendment to Progress and Assurances: - Significant pressure in key speciality areas and this has been escalated
through ECRM and CQN. - planned care QIPP on target - milestone and key deliverables being achieved
1
15�Board�Assurance�Framework.p
Top
Overall�Page�168�of�237Page�3�of�15

Risk Ref
Description of Risk and Impact Amendments
- slippage being reported through performance and planning groups
COR 3-2
There is a risk that provider partners will not remain committed to the planned care QIPP programme and will seek to pursue expansion strategies in an emerging market.
Amendment to Progress and Assurances: Clinical Leaders meeting to discuss planned care and QIPP on 12th March.
COR 3-3
There is a risk that the newly commissioned 111 service and out of hours service does not realise the benefits and outcomes set out within the specification
Amendment to Progress and Assurances: - 111 programme board to address service improvement - investigating direct booking from 111 to ooh. - both contracts on tariff deflator - activity modelling completed to look at demand vs services.
Strategic Objective: Improving maternity services and services for children COR 4-3
Gaps in substantive Designated Doctor Safeguarding children in Hampshire may lead to inadequate strategic medical oversight, damage to reputation
Amendment to Progress and Assurances: March 14 - options for a new model have been circulated.
Strategic Objective: Enabling people with mental health conditions and learning disabilities to secure care closer to home at the right time.
COR 5-1
There is a risk that the transition from Hampshire PCT to five Hampshire CCGs will result in the fragmentation of existing joint-commissioning strategies for adult and older peoples mental health
Amendment to Progress and Assurances: BCF 1st cut submitted 14/2/14
Strategic Objective: Improving Quality of Care and Outcomes for Patients COR 7-1
Significant differences in how the Community Care Teams around the locality are working with primary care could lead to a failure to develop teams according to the integrated care model resulting in the outcomes of the commissioning strategy not being realised.
Amendment to Progress and Assurances: - Review of specifications and outcomes. Contract management meetings
addressing progress. Regular dialogue with Southern Health NHS Trust. Additional project management support introduced.
2
15�Board�Assurance�Framework.p
Top
Overall�Page�169�of�237Page�4�of�15

Risk Ref
Description of Risk and Impact Amendments
COR 7-2
Challenging C. difficile national reduction target for the CCG.
Amendment to Progress and Assurances: - March 2014 – Both CCGs exceed the nationally designated local reduction
target. Awaiting national guidance on plans for 2014/15.
COR 7-4
PHT FFT scoring Friends & Family Test net promoter inpatient score is lowest in England for October 2013. Response rates for ED below average. Patients report a less positive experience in inpatient settings than the national average.
Reduction in risk score: from (4x5) 20 to (4x3) 12 Amendment to Progress and Assurances: - Assurance around impact of change in methodology. Further update from PHT indicates this has improved scores for January.
Recommended for Removal
Risk Ref
Description of Risk and Impact
Strategic Objective: Supporting people to have the healthiest lifestyle they can COR 1-1
There is a risk that the challenging financial position of the CCG could limit the ability of the CCG to target support to areas of deprivation.
Financial position now known.
COR 1-2
There is a risk that the Hampshire-wide Health and Wellbeing Strategy is not sensitive to local deprivation challenges.
Assurance received.
COR 4-1
There is a risk that the programme to deliver an integrated team with the right skill mix to ensure that any child attending QAH as an emergency is seen by the most appropriate health professional in a timely fashion is not delivered because of organisational resistance or cost constraints.
This risk removed as it is out of date and a review of the acute paediatric pathway will be started in due course.
3
15�Board�Assurance�Framework.p
Top
Overall�Page�170�of�237Page�5�of�15

Strategic Objective: Managing change in the health and social care system while ensuring continuity and improving quality COR 6-1
There is a risk that the impact of transition and re-organisation results in loss of focus on key priorities and a failure to deliver specified outcomes.
Transition complete and authorisation conditions cleared
COR 6-10
The CCG allocation has been announced but there are a number of unresolved baseline issues with a result that spend may not be able to be contained within allocated resources.
Allocation has been announced
COR 6-11
There is a risk that the ‘Maximum Take/Group 3 transfers of further services and budgets into the specialised portfolio may remove allocation from the CCG in excess of the saving that will be made on Specialised Commissioning.
Completed Baseline adjustments
COR 6-16
There is a risk that capital funding will be delayed or not forthcoming from NHS England due to organisational change and its impact on the availability of capital funding and recurring revenue. This would impact the granting of Planning Permission and the appointment of a Design Team.
It has been agreed that the over cost of the scheme had increased and planning permission was granted on 23rd December 2014.
New Risk
Strategic Objective: Managing change in the health and social care system while ensuring continuity and improving quality COR 6-18
There is a risk of delay to the overall project completion timescales due to the Full Business Case process. Proposed Risk Score: (4x4) 16
Following the revised project costs the CCH Business case is now required to be taken through the full NHS England (£3m to £10m) approvals route. There will be an impact on the overall project programme. Once the draft business case has been submitted to the PAU, NHS PS will have a better understanding of the timescales involved in obtaining full sign off. In addition, the Business Case will require ‘agreement to lease’ sign-off by Southern and SEH CCG and both GP Practices as key tenants before NHS England and NHS Property Services nationally will approve the Business Case. The impact on the overall programme is currently being assessed.
4
15�Board�Assurance�Framework.p
Top
Overall�Page�171�of�237Page�6�of�15

Appendix A Strategic Risk Register and Assurance Framework South Eastern Hampshire CCG
1 of 8
Risk Ref Theme Date Raised
Original Risk
Score (IxL)
Current Risk Score
(I x L)
Gaps in Control and Actions Required
Deadline for Action Action Owner Progress and
assurancesLevel of
assurance
Risk Owner (Accountable
Person)
Target Risk
Score(I x L)
Date of Last
Review
Identifier used on risk register
Details of any expected controls that are not in place
or controls that are not operating effectively
Details of sources from where positive assurances
can be gained
Level of assurance gained from
arrangements (substantial, limited
etc)
SEH (J)COR1-1 Commissioning Jul-12
There is a risk that the challenging financial position of the CCG could limit the ability of the CCG to target support to areas of higher deprivation
9 (3 x 3) (3x2) 6
- clinical cabinet has a focus on tackling inequality- equality impact assessment framework established as part of the CCG governance system- Community Advisory Committee receives updates on tackling inequalities- DPH on CCG Governing Body
13/14 Final Plans submitted
- The CCG needs a detailed understanding of the implementation and impact of the Integration
Transformation Fund.
05/04/2013 Chief OfficerAuthorisation process. 3rd cut submission of 13/14 plan on Mar 15.
substantial Chief Officer 6 Mar-14
SEH (J)COR1-2 Commissioning Jul-12
There is a risk that the Hampshire-wide Health and Wellbeing Strategy may not be 'sensitive' to local deprivation challenges
8 (4x2) (2x3) 6
- CCG Clinical Chair a member of the Health & Wellbeing Board- CCG is a consultee to the H&WB strategy- DPH and HCC Head of Adult Services members of the CCG Governing Body - Working with Hampshire County Council to ensure the Integration Transformation Fund supports the tackling of inequalities
n/a n/a n/aStrategy published for
consultation and feedback given
n/a Clinical Chair 6 Mar-14
SEH (J) COR 1-3 Commissioning Nov-12
There is a risk that the newly commissioned 111 service and out of hours service does not realise the benefits and outcomes set out within the specification
12 (4X3) (4X2) 8
PCCG currently co-ordinator of 111 contract - group established to review effectiveness of services and report back to CCG Clinical Cabinet/GB - 111 has been achieving its target from June - OOH is under performance measures but has ben beginning to achieve its targets from September
111 live and advertising campaign underway monthly
Chief Commissioning Officer (Debbie
Purdy)
- 111 programme board to address service improvement - investigating direct booking from 111 to ooh. - both contracts on tariff deflator - activity modelling completed to look at demand vs services.
significantChief
Commissioning Officer
3 Mar-14
SEH (J) COR 1-4 Commissioning Jan-13
There is a risk that Portsmouth Hospitals NHS trust is unable to improve its 4 hour ED wait position and this creates quality and safety risks.
(4x4) 16 (4x4) 16
- ECIST action plan in place - monitored through unscheduled delivery board - key actions being progressed eg front door in ED- ED Summit being scheduled for November 2013- CCG now holds weekly reviews with the Chief Executive of the Trust
Delays in implementing more effective working practices in ED; impact of out of hours and 111 arrangements on ED attendances
31/04/2014Chief
Commissioning Officer
Action Plan being developed: "Gold Command" in place - Action Plan being progressed through the unscheduled care delivery board - Service Specification for unscheduled care produced - Daily monitoring of ED activity and performance
Chief Officer 4 Mar-14
Description of the Risk and Impact Key Controls in Place
Clinical Commitment 1: Supporting the access of all communities to high quality care
Strategic Objective 2: Improving experience and outcomes for the frail elderly and people requiring long term care including dementia
15�Board�Assurance�Framework.p
Top
Overall�Page�173�of�237Page�8�of�15

Appendix A Strategic Risk Register and Assurance Framework South Eastern Hampshire CCG
2 of 8
Risk Ref Theme Date Raised
Original Risk
Score (IxL)
Current Risk Score
(I x L)
Gaps in Control and Actions Required
Deadline for Action Action Owner Progress and
assurancesLevel of
assurance
Risk Owner (Accountable
Person)
Target Risk
Score(I x L)
Date of Last
Review
Identifier used on risk register
Details of any expected controls that are not in place
or controls that are not operating effectively
Details of sources from where positive assurances
can be gained
Level of assurance gained from
arrangements (substantial, limited
etc)
Description of the Risk and Impact Key Controls in Place
SEH (J)COR2-1 Commissioning Jul-12
There is a risk that primary care providers will not be able to establish functional structures that allow them to work seamlessly with other care providers in delivering integrated care solutions for the frail elderly and individuals with long term conditions
12 (4X3) (3x3) 9
- invested in interim project management to enable the GP Alliance to develop- Integrated Care Design group and Delivery Board invite members of the Primary Care Alliance provider- Alliance now participating in System Sustainability Board- Alliance now collaborating with Portsmouth Hospital Trust around the Urgent Care Centre
30/04/2014Chief
Commissioning Officer
Project Manager in place. Alliance now attends sustainability Board. NHSiQ programme has been commissioned to focus on primary care development. ICT pilots now established. Pilot clinical leads identified. Admin identified. Reviewed structures and programmes. Re-established groups. Developing service specification for delivery of model.
substantial Chief Officer 6 Mar-14
15�Board�Assurance�Framework.p
Top
Overall�Page�174�of�237Page�9�of�15

Appendix A Strategic Risk Register and Assurance Framework South Eastern Hampshire CCG
3 of 8
Risk Ref Theme Date Raised
Original Risk
Score (IxL)
Current Risk Score
(I x L)
Gaps in Control and Actions Required
Deadline for Action Action Owner Progress and
assurancesLevel of
assurance
Risk Owner (Accountable
Person)
Target Risk
Score(I x L)
Date of Last
Review
Identifier used on risk register
Details of any expected controls that are not in place
or controls that are not operating effectively
Details of sources from where positive assurances
can be gained
Level of assurance gained from
arrangements (substantial, limited
etc)
Description of the Risk and Impact Key Controls in Place
SEH (J)COR3-1 Performance Jul-12
There is a risk that Portsmouth Hospitals NHS Trust is unable to sustain national performance requirements for Referral to Treatment time
9 (3X3) (3X4) 12
-weekly monitoring reported to Clinical Cabinet - Fortnightly performance review with PHT- monthly Governing Body meetings to review performance- monthly SHA/LAT performance assurance - financial risk pool established to ensure our RTT delivery
- Limited Data received on RTT
Deputy Chief Commissioning
Officer
- Significant pressure in key speciality areas and this has been excalated through ECRM and CQN. - planned care QIPP on target - milestone and key deliverables being achieved - alippage being reported through performance and planning groups
Chief Commissioning
Officer3 Mar-14
SEH (J)COR3-2 Commissioning Jul-12
There is a risk that provider partners will not remain committed to the planned care QIPP programme through and will seek to pursue expansion strategies in an emerging market
12 (4X3) (4x3) 12
Continued engagement and communication, underpinning contracting framework to support the delivery of QIPP. Relevant delivery boards hold systems to account. Sign off role for PHT and Solent IBP and LTFM
Robust contract based system for monitoring and
challenging elective activity
monthlyDeputy Chief
Commissioning Officer
Clinical Leaders meeting to discuss planned care and
QIPP on 12th March 14.
n/aChief
Commissioning Officer
4 Mar-14
Strategic Objective 3: Care that is planned is delivered in the best way at the best time in the best place
15�Board�Assurance�Framework.p
Top
Overall�Page�175�of�237Page�10�of�15

Appendix A Strategic Risk Register and Assurance Framework South Eastern Hampshire CCG
4 of 8
Risk Ref Theme Date Raised
Original Risk
Score (IxL)
Current Risk Score
(I x L)
Gaps in Control and Actions Required
Deadline for Action Action Owner Progress and
assurancesLevel of
assurance
Risk Owner (Accountable
Person)
Target Risk
Score(I x L)
Date of Last
Review
Identifier used on risk register
Details of any expected controls that are not in place
or controls that are not operating effectively
Details of sources from where positive assurances
can be gained
Level of assurance gained from
arrangements (substantial, limited
etc)
Description of the Risk and Impact Key Controls in Place
SEH (J)COR4-1 Commissioning Jul-12
There is a risk that the programme to deliver an integrated team with the right skill mix to ensure that any child attending QAH as an emergency is seen by the most appropriate health professional in a timely fashion is not delivered because of organisational resistance or cost constraints
(3x3) 9 (3x3) 9
- CQUIN agreed in contract to incentivise provider - Commissioning leadership arrangements established- P&SEH Commissioning Collaborative Group established to oversee progress - system sustainability Board reviews programme
-agreement in the optimum delivery model- Agreement to be reached between commissioner and provider. - Implementation plan required
May-13 AD Children Comm n/a AD Children
Comm 3 Mar-14
SEH (J)COR4-3 Quality Jul-12
Gaps in Designated Doctor Safeguarding Children in Hampshire may lead to inadequate strategic medical oversight, damage to reputation
15 (5X3) (3x3) 9
-safeguarding children policy agreed by Governing Body- Quality Framework and quality monitoring arrangements approved by Governing Body- GP Quality Leads appointed- authorisation review of arrangements - agreement between PHT and commissioning on future delivery model - SG nurse in post
National recognition that the model requires revision by PCP and National Leads
ongoing Chief Quality Officer
- June 2013 interim arrangements in place- West Hampshire CCG hosting Safeguarding arrangements- Full gap analysis and action plan in place- Reviewed at Quality and Safety Committee 9 October- Vulnerable Persons Committee established and first meeting held 15 October - - January 2014: Section 11 Audit completed with action plan in development. - Mar 14 - options for a new model have been circulated.
significant Chief Quality Officer 6 Mar-14
SEH (J)COR5-1 Commissioning Jul-12
There is a risk that the transition from Hampshire PCT to five Hampshire CCGs will result in the fragmentation of existing joint-commissioning strategies for adult and older peoples mental health
12 (3X4) (3x2) 6
- established Hampshire 5 CCG Commissioning Group to ensure collaborative commissioning arrangements continue- HCC Director of Adult Services on CCG Governing Body- collaboration agreement reached with Hampshire 5
- The CCG needs a detailed understanding of the implementation and impact of the Better Care Fund
Sep-14Chief
Commissioning Officer
BCF 1st cut submitted 14/2/14 n/a Chief Officer 3 Mar-14
Strategic Objective 5: Enabling people with mental health conditions and learning disabilities to secure care closer to home at the right time
Strategic Objective 4: Improving maternity services and services for children
15�Board�Assurance�Framework.p
Top
Overall�Page�176�of�237Page�11�of�15

Appendix A Strategic Risk Register and Assurance Framework South Eastern Hampshire CCG
5 of 8
Risk Ref Theme Date Raised
Original Risk
Score (IxL)
Current Risk Score
(I x L)
Gaps in Control and Actions Required
Deadline for Action Action Owner Progress and
assurancesLevel of
assurance
Risk Owner (Accountable
Person)
Target Risk
Score(I x L)
Date of Last
Review
Identifier used on risk register
Details of any expected controls that are not in place
or controls that are not operating effectively
Details of sources from where positive assurances
can be gained
Level of assurance gained from
arrangements (substantial, limited
etc)
Description of the Risk and Impact Key Controls in Place
SEH (J)COR6-1 Leadership Jul-12
There is a risk that the impact of transition and re-organisation results in loss of focus on key priorities and a failure to deliver specified outcomes
12 (4X3) 6 (3x2)
- SHIP Board of Clinical Commissioners responsible for managing transition and whilst maintaining focus on delivery- CCG performance and assurance processes ensure monthly review of delivery- CCG Governing Body and Clinical Cabinet receive monthly performance reports - CCG legacy and transition group established - authorisation site visit assurance
n/a n/a Chief OfficerTransition complete.
Authorisation conditions cleared.
Chief Officer 3 Mar-14
SEH (J)COR6-2 Performance Jul-12
There is a risk that 2012/13 QIPP schemes do not deliver the required activity changes resulting in inability to reduce system capacity and cause organisational financial pressures. Significant level of unidentified QIPP.
16 (4X4) 20 (4x5)
• Greater system collaboration on the design and delivery of QIPP schemes• CQUIN and contracts used as a driver to ensure greater integration between providers of care (e.g. OPP)• Continued performance management and assurance through system sustainability• Increased ownership of the challenge in Primary Care through CCG leadership• Robust monitoring during 13/14 and beyond to ensure QIPP on target. • Use of 2% non recurring fund to support system reconfiguration. • Contingency will provide further risk mitigation if necessary.
Conitinued existence of unidentified QIPP Mar-14 Chief Finance
Officer
QIPP plans. Reported financial position. Contract
performance.
n/a Chief Finance Officer 6 Mar-14
SEH (J)COR6-7 Partnership Jul-12
There is a risk that QIPP schemes / commissioning intentions result in an under-utilisation of PHT’s fixed cost estate such that efficiencies are not realised by the system
12 (4x3) 9 (3x3)
• Estates rationalisation plan continues to manage capacity transfer to Queen Alexandra Hospital and is under review• Gap in capacity utilisation is to be covered by Portsmouth Hospitals Trust (PHT) through:− Seeking to increase market share for NHS activity outside of Portsmouth & F&G CCGs− Marketing excess capacity to non-NHS market (private patients, retail, pharmaceutical industry, etc)
- Need to reinvigorate estates strand of
sustainability work.Mar-14 Chief Finance
Officer - financial position -
estate savings limited Chief Finance Officer 6 Mar-14
SEH (J)COR6-8 Partnership Jul-12 PHT is not yet an FT and may require
system support to secure such status (4x3) 12 (4x3) 12
• Respective tri-partite agreements in place.• Regular communication on progress and monitoring of QIPP and contract performance
- PHT financial review and performance position prevents progression of FT status at this time.
Jan-15 Chief Finance Officer - PHT FT application limited Chief Finance
Officer 4 Mar-14
Strategic Objective 6: Managing change in the health and social care system while ensuring continuity and improving quality
15�Board�Assurance�Framework.p
Top
Overall�Page�177�of�237Page�12�of�15

Appendix A Strategic Risk Register and Assurance Framework South Eastern Hampshire CCG
6 of 8
Risk Ref Theme Date Raised
Original Risk
Score (IxL)
Current Risk Score
(I x L)
Gaps in Control and Actions Required
Deadline for Action Action Owner Progress and
assurancesLevel of
assurance
Risk Owner (Accountable
Person)
Target Risk
Score(I x L)
Date of Last
Review
Identifier used on risk register
Details of any expected controls that are not in place
or controls that are not operating effectively
Details of sources from where positive assurances
can be gained
Level of assurance gained from
arrangements (substantial, limited
etc)
Description of the Risk and Impact Key Controls in Place
SEH (J) COR 6-8a Jun-13
There is a risk that Portsmouth Hospital NHS Trust will be unable to deliver planned finance plan in 13/14 which can create a sustainability challenge for the organisation.
(4x4) 16 (4x4) 16
- key issues meeting held with Trust Executive on a monthly basis- Board to board meeting between 3 CCGs and PHT now in place - monthly contract meetings continuing - joint work programme underway between 2 CCGs , CFOs and PHT's FD to map the impact of further commissioning intentions- discussions and actions agreed with the Trust Development Authority and Area Team- recovery plan established and an assurance process agreed - Meetings held with Trust Development Authority and agreement reached on collaboration between the agencies.
- ill defined understanding of relationship between commissioners and trust development agency. - a framework will need to be developed.
Mar-14 Chief Finance Officer
Disucssions with PHT have agreed a
common view of the Year End position.
Substantial Chief Officer 4 Mar-14
SEH (J)COR6-10 Finance Jul-12
The CCG allocation is currently uncertain with a result that spend may not be able to be contained within allocated resources
16 (4x4) (3x3) 10
CCG will work closely with CSS to ensure new returns are robust. Should the allocation change significantly the CCG would review expenditure programmes and adjust accordingly. Regular update to CCG Board.
- agreeing risk share arrangement with Hampshire 5
Sep-13 Chief Finance Officer
Baseline issues now unilaterally resolved n/a Chief Finance
Officer 6 Mar-14
SEH(J) COR 6-11 Finance Jan-13
There is a risk that the 'Maximum Take'/group 3 transfers of further services and budgets into the specialised portfolio may remove allocation from the CCG in excess of the saving that will be made on Specialised Commissioning
(4x3) 12 (4x2) 8Work closely with other CCGs and LAT to agree risk sharing mechanisms to limit impact in 13/14.
- Lack of understanding of the basis of national allocation adjustments and the true impact of the new rules on providers- Potential inaccuracy of revised provider adjustments and unclear of the true impact of the new rules on providers
Jul-13 Chief Finance Officer
Completed baseline adjustments
Chief Finance Officer 8 Mar-14
SEH (J)COR6-14 Finance Jul-12
There is a risk that growth and costs are beyond existing assumptions with the result that cost pressures meant the CCG is unable to achieve planned surplus and receive the Quality Premium in 14/15.
12 (4x3) 15 (5x3)
- Close scrutiny of contract monitoring and regular contract reviews will highlight areas of concern and address any issues that emerge- Contingency available to manage the position
- lack of control over elective referrals Mar-14 Chief Finance
Officer
- Discussions with PHT and PCCG about
how to limit our respective financial
risk.
substantial Chief Finance Officer 4 Mar-14
SEH (J) COR 6-15 Finance Jun-13
Impact of Health and Social Care Information Centre (HSCIC) Guidance poses a significant risk to financial controls on contracts, and increased financial cost to CCGs from CSUs.
(4x4) 16 (3x4) (12)
- Letter sent to Director Wessex LAT highlighting issue, Jun 13. - Guidance has been received from NHS England - CSU is undertaking investigative actions
- Gap in guidance continues to limit the use of PID for non-direct care
purposes which may result in an inability to validate
invoice payments
Chief Finance Officer
- Further guidance has been provided allowing for PCD to be used for invoice
validation
limited Chief Officer 4 Mar-14
15�Board�Assurance�Framework.p
Top
Overall�Page�178�of�237Page�13�of�15

Appendix A Strategic Risk Register and Assurance Framework South Eastern Hampshire CCG
7 of 8
Risk Ref Theme Date Raised
Original Risk
Score (IxL)
Current Risk Score
(I x L)
Gaps in Control and Actions Required
Deadline for Action Action Owner Progress and
assurancesLevel of
assurance
Risk Owner (Accountable
Person)
Target Risk
Score(I x L)
Date of Last
Review
Identifier used on risk register
Details of any expected controls that are not in place
or controls that are not operating effectively
Details of sources from where positive assurances
can be gained
Level of assurance gained from
arrangements (substantial, limited
etc)
Description of the Risk and Impact Key Controls in Place
SEH(J) COR 6-16 Chase Hospital Jun-13
There is a risk that capital funding will be delayed or not forthcoming from NHS England due to organisational change and its impact on the availability of capital funding and recurring revenue. This would impact the granting of Planning Permission and the appointment of a Design Team.
(4x3) 12 (4x3) 12
- Capital requirement for the redevelopment has been included with the 5 year forecast capital spend for NHS Property Services and is subject to approval of a full business case. - Early consultation with planners to ensure proposed development meets local planning requirements and is supported by key stakeholders. - NHS Property Services working with NHS England and the CCG have identified a solution and a technical design team has now been appointed - Joint work continues to understand and follow the fast track process for Full Business Case development and approval
Lisa Medway
- NHS Property Service working with NHS England and the CCG has identified a solution and a technical design team has now been appointed. - Joint work continues to understand and follow the fast track process for Full Business Case development and approval
Sara Tiller 3 Mar-14
SEH (J) COR 6-17 Partnership Sep-13
There is a risk that poor performance/lack of delivery in functions supplied by NHS South CSU results in an inability of the CCG to monitor performance of provider Trusts and therefore commission effectively.
(4x4) 16 (4x3) (12)
- CSU user group meeting monthly to identify issues. - Weekly meeting with CSU customer relationship lead to monitor performance and raise issues of concern. - Issue log in place and monitored monthly. CSU senior manager attends CCG management meetings. Rectification plans in place for contracting a HR and monitored through CSU User Group.
Service specifications are ill defined and therefore performance is difficult to monitor.
Sep-14
Chief Finance Officer
- Regular reports taken to Clinical Cabinet. Hants-wide review of service specifications under way. SCU/CCG Staff workshop undertaken to improve joint working.
substantial
Chief Development
Officer 4 Mar-14
SEH(J) COR 6-18
Chase Redevelopment Project
Mar-14There is a risk of delay to the overall project completion timescales due to the Full Business Case process
(4x4) 16 (4x4) 16
- NHS PS will produce a draft Business Case for discussion with PAU which will inform discussion regarding the level of detail to be provided. This will then inform the project programme, and timescales for sign-off. - NHS PS have engaged the services of a surveyor. A briefing meeting is being arranged, however due to the unavailability of key personnel this has been moved to 23rd April. - The impact on the overall programme is being assessed and ways in which the construction programme shortened investigated. - Areas will be released as redevelopments/refurbishments are completed.
- Sponsoring organisations to brief the surveyor prior to meeting with GPs or their representatives. Timescales for agreement to lease wil be established once the GP meeting has taken place.
Chase Project Manager
Chief Development
Officer Mar-14
15�Board�Assurance�Framework.p
Top
Overall�Page�179�of�237Page�14�of�15

Appendix A Strategic Risk Register and Assurance Framework South Eastern Hampshire CCG
8 of 8
Risk Ref Theme Date Raised
Original Risk
Score (IxL)
Current Risk Score
(I x L)
Gaps in Control and Actions Required
Deadline for Action Action Owner Progress and
assurancesLevel of
assurance
Risk Owner (Accountable
Person)
Target Risk
Score(I x L)
Date of Last
Review
Identifier used on risk register
Details of any expected controls that are not in place
or controls that are not operating effectively
Details of sources from where positive assurances
can be gained
Level of assurance gained from
arrangements (substantial, limited
etc)
Description of the Risk and Impact Key Controls in Place
SEH (J)COR7-1 Partnership Jul-12
Significant differences in how the Community Care Teams around the locality are working with primary care could lead to a failure to develop teams according to the integrated care model resulting in the outcomes of the commissioning strategy not being realised.
16 (4X4) 12 (4X3)
- programme management arrangements established (in partnership with HCC and Southern Health NHS FT reporting to the Clinical Cabinet - Locality Clinical leads have been appointed supported by an overall GP Clinical lead
Chief Commissioning
Officer
Review of specifications and
outcomes. Contract management meetins addressing progress. Regular dialogue to
Southern Health NHS Trust. Additional
project management support introduced.
substantial Clinical Chair 6 Mar-14
SEH (J) COR7-3 Q05
Quality May-13 Challenging C.difficile national reduction target for the CCG. (4x4) 16 (4x4) 16
- Interim cover via DCQO- HCAI cover via secondment- Recovery plan in progress
- Secondee commences 2/9/13- Interim HCAI expert cover stops 15/8/13- DCQO is covering 2 weeks in August- PID sharing disagreement escalated to Public Health and DoH to seek clarity as a matter of urgency- Limited access to PID required for full Root Cause Analysis (national problem)
Sep-13 Deputy Chief Quality Officer
- Recruit to vacancy - secondee commences 2/9/13- Interim HCAI expert cover- PID Sharing disagreement escalated to Public Health and DoH to seek clarity as a matter of urgency- Recovery plan in progress including work with meds management and -infection control training planned in Primary Care - Jan 14 specialist IPC nurse time secured and post filled. Analysis of cases show some areas in primary care that CCG can refresh re antibiotic prescribing. Jan IPC training for practice nurses and TARGET
Chief Quality Officer 4 Mar-14
SEH(J) COR 7-4 Quality Jan-14
PHT FFT scoring Friends and Family Test net promoter inpatient score is lowest in England for October 2013. Response rates for ED below average. Patients report a less positive experience in inpatient settings than the national average.
(4x5) 20 (4x3) 12
Joint CCG and Wessex Area Team visit. CCG FFT analysis undertaken. FFT report received from PHT. Escalation to ECRM.
Early indications shows improvements. Apr-14 Head of Quality
Assurance around impact of change in methodology. Further update from PHT indicates this has improved scores for January. Improvement in scores brings PHT in line with other acute trusts in Wessex.
good Chief Quality Officer 6 Mar-14
Strategic Objective 7: Improving quality of care and outcomes for patients
15�Board�Assurance�Framework.p
Top
Overall�Page�180�of�237Page�15�of�15

GOVERNING BODY Date of Meeting 19th March 2014
Agenda Item No
16 Title
Engagement Report Purpose of Paper
To provide members of the Governing Body with information on engagement with public and patients that has taken place in the CCG in the last two months.
Recommendations/ Actions requested
The Governing Body is asked to: • Note the Engagement Update
Author
Jo Parkinson Senior Development and Engagement Officer
Sponsoring member
Tracey Faraday-Drake Lay Member (Patient Participation and Involvement)
Date
19th March 2014
16�Engagement�Report.pdf
Top
Overall�Page�181�of�237Page�1�of�3

SOUTH EASTERN HAMPSHIRE CCG – ENGAGEMENT REPORT
1 Purpose 1.1 The purpose of this paper is to provide members of the Governing Body with information on engagement with public and patients that has taken place in the CCG in the last two months.
2 Locality Patient Groups 2.1 The North of Butser Locality Patient Group met for the first time on 16 January 2014 and the South of Butser Group meet on 27 February. The purpose of the group is for representatives of the local patient participation groups to meet together regularly to share good practice and discuss issues that affect the local practices. Representatives from four of the seven practices attended the North of Butser meeting, and 11 of the 18 practices for the South of Buster meeting. It is hoped that the representatives from the other practices will attend future meetings. Once the groups are better acquainted a chair will be chosen for each group and they will be involved in the Community Engagement Committee. 3 CCG Strategy 3.1 The CCG set up a Call to Action strategy session held at Havant Public Plaza on 27 January 2014. Over 40 people representing local groups attended the meeting to help develop the CCG’s five year strategy. Richard Samuel gave a presentation, and then those attending worked together to agree the local objectives and to see how closely these related to the current priorities for the CCG. The feeling of the meeting was that two of the existing objectives could be developed and that prevention and education needed to be included. The work of the group is being fed into the strategy for the CCG. 4 Community Engagement Committee 4.1 The core membership of the Community Engagement Committee met on 5 February 2014 to discuss the first year of the Committee’s work and how to develop the committee going forward. A proposal will be made to the full membership of the Committee in March on having a small group to review strategy with a much larger reference group to support the work of the CCG. 5 Board to Board meeting 5.1 On 5 February 2014 a total of 40 members from the Governing Bodies of South Eastern Hampshire, Fareham & Gosport and Portsmouth CCGS and Portsmouth Hospitals NHS Trust attended a Board to Board meeting. Richard Samuel presented on the Five year strategy for South Eastern Hampshire and Fareham & Gosport CCGs; Innes Richens (Portsmouth CCG) presented on the Better Care Fund and Ursula Ward (Portsmouth Hospitals NHS Trust) spoke about the hospital’s Three year strategy.
1
16�Engagement�Report.pdf
Top
Overall�Page�182�of�237Page�2�of�3

6 Chase Community Hospital 6.1 The Chase Communality Hospital Steering Committee last met on 14 February 2014. A full report on the progress being made on the project is available at item 14, and the Steering Group continues to be fully engaged at every stage to help shape the development of the hospital. 7 Havant Health and Well Being Board 7.1 Sara Tiller attended the first meeting of the Havant Health and Well Being Board on 6 March 2014. The meeting discussed the purpose of the group, which is to bring together a range of agencies to work together on health and well being projects for maximum benefit of local people. An update was given on the bids submitted by Havant Borough Council for public health funding. £46k has been given to support the following projects: Men in Sheds; Being Independent in Later Life (BILL); Couch to 5K; and a Breastfeeding project. A further bid for £42,000 has been submitted and a decision is still awaited.
8 The Governing Body is asked to note this report.
2
16�Engagement�Report.pdf
Top
Overall�Page�183�of�237Page�3�of�3

GOVERNING BODY Date of Meeting 19th March 2014
Agenda Item No
17 Title
Public Health Update Purpose of Paper
To summarise issues pertaining to the delivery of specialist public health advice to the CCGs by Hampshire Public Health.
Recommendations/ Actions requested
The Governing Body is asked to: • Note the update on Public Health
Author
Ruth Milton Director of Public Health Hampshire County Council
Sponsoring member
Ruth Milton Director of Public Health Hampshire County Council
Date
19th March 2014
17�Public�Health�Update.pdf
Top
Overall�Page�184�of�237Page�1�of�2

South East Hampshire CCG Public Health Update Report
February 2014
Public Health advice to NHS commissioners
This report summarises issues pertaining to the delivery of specialist public health advice to the CCGs by Hampshire public health as set out in the Memorandum of Understanding (MOU) between the CCG and the Director of Public Health for Hampshire.
Public health colleagues continue to deliver against the work plan as agreed in the 2013/14 Memorandum of Understanding with the Clinical Commissioning Group.
There has been a welcome improvement in specialist public health capacity since the beginning of February.
During December and January this has focused on supporting the development of the CCG strategic plans for the coming year and the CCGs’ clinical pathway work to inform the proposals regarding the future provision of high quality hospital services for the people of North and Mid Hampshire.
Another strand of specialist public health advice has been the initiation of evaluation and benefits realisation work across the partnership of the CCGs and Hampshire County Council in support of the integration heralded by the Better Care Fund approach.
The public health team continue to support the work of the urgent care board.
Work to review and agree the MOU for 2014/15 has started.
End of Year Report
An end of year report will be submitted to the meeting of the Board in March 2014.
17�Public�Health�Update.pdf
Top
Overall�Page�185�of�237Page�2�of�2

GOVERNING BODY Date of Meeting 19th March 2014
Agenda Item No
18 Title
Minutes/Notes of Other Meetings Purpose of Paper
For information
Recommendations/ Actions requested
The Governing Body is asked to note the minutes of the following meetings: • Hampshire Commissioning Group – 20th November 2013 • Hampshire Commissioning Group – 22nd January 2014 • South Eastern Hampshire CCG Clinical Cabinet – 27th
November 2013 • Joint CCG Clinical Cabinet 27th November 2013 • South Eastern Hampshire CCG Clinical Cabinet – 29th January
2014 • Joint CCG Clinical Cabinet – 29th January 2014 • Community Engagement Committee – 4th December 2013
Author
Nikki Roberts Governance and Committee Officer
Sponsoring member
Dr Barbara Rushton CCG Chair
Date
13th March 2014
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�186�of�237Page�1�of�52

Minutes Minutes of the meeting of the Hampshire Commissioning Group held at 9.00 am on Wednesday 20 November 2013 in the Wykeham Room, Winchester Guildhall, The Broadway, Winchester, SO23 9GH
Summary of Actions Minute Ref
Action Who By
8 Act on response re concerns over CAMHS services, and escalate if appropriate.
RH
9 Examine the figures in the confidential paper on emergent financial pressures in detail
HH/MF/PH Next meeting
Present: Richard Samuel (Chair)
Chief Officer Fareham & Gosport and South Eastern Hampshire CCGs
David Chilvers Chair Fareham & Gosport CCG Hugh Freeman Chair North Hampshire CCG Heather Hauschild Chief Officer West Hampshire CCG Maggie MacIsaac Chief Officer North East Hampshire & Farnham
CCG Sarah Schofield Chair West Hampshire CCG In attendance: Karen Ashton Strategic Commissioning
Director Hampshire County Council
Mike Fulford Chief Finance Officer West Hampshire CCG Ros Hartley North East Hampshire & Farnham
CCG Inger Hebden Director of
Commissioning, Long Term Conditions and Community
West Hampshire CCG
Pam Hobbs Chief Finance Officer North Hampshire CCG Angela Murphy Interim Associate
Director for Children and Maternity
North East Hampshire & Farnham CCG
Roshan Patel Chief Finance Officer North East Hampshire & Farnham CCG
Apologies: Lisa Briggs Chief Operating Officer North Hampshire CCG Debbie Fleming Local Area Director NHS England Wessex Local Area
Team Ruth Milton Director of Public Health Hampshire County Council Barbara Rushton Chair South Eastern Hampshire CCG Andrew Wood Chief Finance Officer Fareham & Gosport and South
Eastern Hampshire CCGs
1
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�187�of�237Page�2�of�52

1 Welcome and Apologies Richard Samuel welcomed everyone to the meeting, which had been preceded
by a meeting between the Chairs and Chief Officers of the CCGs and the Chief Executive and senior officers of Hampshire County Council. As members had been delayed in returning from the meeting, the meeting of the Hampshire Commissioning Group would be shortened.
Apologies had been received from Lisa Briggs, Debbie Fleming, Ruth Milton, Barbara Rushton and Andrew Wood.
2 Declarations of Interest There were no declarations of interest relating to any items on the agenda. 3 Minutes of the previous meeting The minutes of the meeting held on 18 September 2013 were approved,
subject to the following amendments: Item 5.1: amend ‘know’ in the second bullet point to read ‘known’ Item 5.2: amend the third sentence of the fourth paragraph to read “Costs
have been moved …..”. 4 Matters Arising
Date Minute Ref
Action Who Progress
16.10.13 6 Co-ordinate CCG representatives at Strategy Workshop
AB
16.10.13 12 Develop risk sharing agreement on Serious Case Reviews
CFOs
5 Finance Matters There was no update on Finance Matters, due to pressure of time. 6 Southern Health Foundation Trust – Briefing following West Hampshire
CCG Extraordinary Board Seminar of 7 November 2013 Inger Hebden gave a verbal update on the outcome of an Extraordinary
Seminar of West Hampshire CCG Board members held on 7 November 2013. The meeting was attended by members of the West Hampshire CCG (WHCCG) Board and Southern Health NHS Foundation Trust (SHFT) Board. Clinical leads were also present at the meeting. The purpose of the meeting was to look at high profile risk areas and recent media attention. It was noted by the meeting that governance processes, especially Clinical Quality Review Meetings needed some improvement, as did some aspects of clinical leadership. Members recognised that SHFT was a large and complex organisation. It was agreed that both organisations should work together so that the response of the commissioners was seen to be proportionate. It was
2
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�188�of�237Page�3�of�52

agreed that WHCCG should co-ordinate the contracting process for the year 2014/15.
The Hampshire Commissioning Group:
• noted the verbal update on Southern Health Foundation Trust • agreed that West Hampshire CCG should co-ordinate the contracting
process for the year 2014/15 7 Personal Health Budgets The paper on Personal Health Budgets was deferred, due to lack of time. 8 Children’s Risk Log Ros Hartley presented a paper to update members on current risks related to
Children’s Services delivery, excluding safeguarding factors. Richard Samuel raised concern over the Child and Adolescent Mental Health
Services (CAMHS), which had been raised as a new risk on the Children’s Risk Log. A meeting had been held with clinicians, and serious concerns had been raised about capacity within the service to meet demands. Without immediate action, this would potentially lead to unacceptable levels of risk and ultimately an unsafe service. A letter had been written to the provider detailing the concerns, and a formal response was awaited. An issue log had been compiled, which had been reviewed and the actions raised would be followed up. A service review would be undertaken if the response was not sufficient to reassure the commissioners. Ros Hartley agreed to act on the response and escalate if appropriate.
Action: RH
9 Integration Transformation Fund Karen Ashton tabled a paper in confidence relating to emergent financial
pressures within Adult Social Care. In response to the paper and the earlier meeting with the Chief Executive of
Hampshire County Council, members felt that it would be difficult for the CCGs to commit any further resources to Hampshire County Council without more detailed financial contracting information. Members agreed to consider supporting relevant changes that result in tangible health benefits where plans were available in enough detail to make business sense and where CCGs were treated as equal partners. Members also recognised, however, that the financial pressures incurred in domiciliary care could materially impact on health outcomes. Heather Hauschild, Mike Fulford and Pam Hobbs agreed to examine the figures in the paper in detail.
Action: HH/MF/PH 10 Hampshire Health and Wellbeing Board There was no update on the Hampshire Health and Wellbeing Board, due to
pressure of time. 11 Hampshire Health Overview and Scrutiny Committee
3
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�189�of�237Page�4�of�52

There was no update on the Hampshire Health Overview and Scrutiny Committee, due to pressure of time.
12 Future Agenda Items
• Personal Health Budgets – DW – February 2014 • Children’s Contracts S256 – AM – January 2014 • Continuing Healthcare: Phase Two Proposals – DW • Vulnerable Adults Team seminar – IH – January 2014 • Adoption Medical Advisors (Naomi Black) • Feedback on workshop on Strategy for services for people with a physical
disability, long term condition and/or sensory impairment – (Geoff Woollan) – January 2014
• Chronic Fatigue Service – DW 20 Next Meeting Wednesday 22 January 2014
9.00 am – 10.30 am Fair Oak Room, Wells Place, Eastleigh
4
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�190�of�237Page�5�of�52

Minutes Minutes of the meeting of the Hampshire Commissioning Group held at 9.00 am on Wednesday 22 January 2014 in the Fair Oak Room, Wells Place, Eastleigh, SO50 5LJ. Summary of Actions Minute Ref
Action Who By
5 Co-ordinate sharing of QIPP plans with CFOs and Deloitte SJ/ All
Next meeting
5 Arrange dialogue re SHFT IH Next meeting
7 Draft response to letter from Chief Executive of HCC and agree with other Chief Officers
HH Next meeting
Present: Richard Samuel (chair) Chief Officer Fareham & Gosport / South
Eastern Hampshire CCGs Lisa Briggs Chief Operating Officer North Hampshire CCG David Chilvers Chair Fareham & Gosport CCG Heather Hauschild Chief Officer West Hampshire CCG Maggie McIsaac Chief Officer North East Hampshire &
Farnham CCG Barbara Rushton Chair South Eastern Hampshire CCG Sarah Schofield Chair West Hampshire CCG In attendance: Karen Ashton Strategic Commissioning
Director Hampshire County Council
Sallie Bacon Associate Director of Public Health
Hampshire County Council
Alex Berry Chief Commissioning Officer Fareham & Gosport / South Eastern Hampshire CCGs
Gill Duncan Director of Adult Services Hampshire County Council Mike Fulford Chief Finance Officer West Hampshire CCG Ros Hartley North East Hampshire &
Farnham CCG Inger Hebden Director of Commissioning,
Long Term Conditions and Community
West Hampshire CCG
Pam Hobbs Chief Finance Officer North Hampshire CCG Sandra Jenkinson Committee Support Officer Fareham & Gosport / South
Eastern Hampshire CCG Angela Murphy Interim Associate Director for
Children and Maternity North East Hampshire & Farnham CCG
Roshan Patel Chief Finance Officer North East Hampshire & Farnham CCG
Diane Wilson West Hampshire CCG Apologies: Hugh Freeman Chair North Hampshire CCG Ruth Milton Director of Public Health Hampshire County Council
1
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�191�of�237Page�6�of�52

Andy Whitfield Chair North East Hampshire & Farnham CCG
Andrew Wood Chief Finance Officer Fareham & Gosport / South Eastern Hampshire CCG
1 Welcome and Apologies The chair welcomed everyone to the meeting. Apologies were received from Hugh
Freeman, Ruth Milton, Andy Whitfield and Andrew Wood. 2 Declarations of Interest There were no declarations of interest relating to any items on the agenda. 3 Minutes of the previous meeting The minutes of the meeting held on 20 November 2013 were approved as a correct
record. 4 Matters Arising Item 6: Southern Health Foundation Trust. It was reported that a debate was continuing around the contract for Older Persons
Mental Health.
Date Minute Ref
Action Who Progress
20.11.13 8 Act on response re concerns over CAMHS services, and escalate if appropriate
RH Completed
20.11.13 9 Examine the figures in the confidential paper on emergent financial pressures in detail
HH/MF/PH
Completed
5 Finance Matters Mike Fulford gave a verbal update on behalf of West Hampshire CCG. The
CCG expected to achieve a 3.5% QIPP saving during the year 2014/15. A total of 80% of the QIPP savings had been identified, although no account had been taken of the risk arising from the Better Care Fund.
Pam Hobbs gave a verbal update on behalf of North Hampshire CCG. The
CCG had declared a deficit for the current financial year. All headroom had been used. The CCG faced a number of underlying problems, including Hampshire Hospitals NHS Foundation Trust and Southern Health NHS Foundation Trust (SHFT).
Roshan Patel gave a verbal update on behalf of North East Hampshire &
Farnham CCG. QIPP schemes were currently under discussion with provider organisations. The CCG would need to make £7m QIPP savings in the next financial year, of which 95% had been identified. The CCG would lose £2.6m
2
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�192�of�237Page�7�of�52

due to re-basing of the financial allocation. Discussions were currently underway with Frimley Park Hospital NHS Foundation Trust, which was working towards a merger with Heatherwood and Wexham Park NHS Foundation Trust.
Richard Samuel gave a verbal update on behalf of Fareham & Gosport and
South Eastern Hampshire CCGs. Both CCGs planned to make 6% QIPP savings. Some progress had been made, and discussions were ongoing with Portsmouth Hospitals NHS Trust. Paediatric QIPPs were strong, and work was ongoing around other services.
Heather Hauschild reminded the meeting that there was a £12m gap in
community mental health services. An overall discussion was needed regarding the contract with SHFT.
Gill Duncan added that there now needed to be a refocus around community
services generally, it was important to ensure that the right services were in place. Deloitte was undertaking some work for Hampshire County Council, and it might be appropriate for Deloitte to see the QIPP plans of the CCGs. Members noted that benefits could be gained from sharing, and it was agreed that QIPP plans be circulated between CCG commissioning leads and chief finance officers (in confidence). QIPP plans would also be shared with Deloitte.
Action: All Angela Murphy informed the meeting that there had been a recent change of
age limits relating to children and young people, and this should be borne in mine during the planning process.
Members then had a discussion around SHFT. Inger Hebden agreed to
arrange a dialogue between commissioning leads, contracting leads at NHS South Commissioning Support Unit (CSU) and Hampshire County Council regarding SHFT.
Action: IH The Hampshire Commissioning Group noted the verbal update on
Finance Matters. 6 Emerging Financial Pressures – Adult Services A paper from Karen Ashton had previously been circulated. The Hampshire Commissioning Group noted the paper that had
previously been circulated.
3
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�193�of�237Page�8�of�52

7 Partnership with Hampshire County Council Richard Samuel reminded the meeting that a meeting had been arranged with
the Chief Executive and senior officers of Hampshire County Council (HCC) on Wednesday 19 February 2014. The CCGs would be represented by Chief Officers and Chairs. It would be useful to meet sometime before that meeting.
Members agreed that the focus was now on working relationships between the
CCGs and HCC. The Health and Wellbeing Board was based within local government, and the implementation of the Better Care Fund would pose some risks to the CCGs. The relationship with SHFT would need to be borne in mind, as well as acute providers. Members acknowledged that the CCGs had been working constructively with Karen Ashton and Gill Duncan, and believed that it was important to maintain the relationships. Elected members of HCC would bring political issues into the mix.
No transfers of funding were required during the year 2014/15; however this
would change in the year 2015/16. HCC and the CCGs would need to look for opportunities to make changes and there also needed to be mutual benefit sharing.
A letter regarding funding had been received on 21 January 2014 from the
Chief Executive of HCC; it was agreed that a joint response be sent from all CCGs. Heather Hauschild agreed to draft a letter and share with other chief officers for comment.
Action: HH Members discussed the implementation of the Better Care Fund, and agreed
that an infrastructure should be put in place, with a lead officer in place. Deloitte was undertaking work for HCC, and would be able to advise on governance arrangements. The chief finance officers would need to detail any risks to the CCGs. The governance framework was expected to require the Constitutions of each CCG to be amended. Richard Samuel agreed to take a lead on governance arrangements. The chief finance officers would agree who should lead on a benefits appraisal.
The Hampshire Commissioning Group noted the verbal update on
Partnership with Hampshire County Council, and agreed that an infrastructure for the implementation of the Better Care Fund should be put in place.
8 Better Care Fund (BCF)
4
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�194�of�237Page�9�of�52

Gill Duncan was in attendance to discuss approaches to the Better Care Fund. She first commented on the letter that had been sent by the Chief Executive of Hampshire County Council. There was currently a difficult political situation, and the sign off of a two year budgetary strategy was predicated on £20m of BCF funding being released. Heather Hauschild remarked that CCGs had not yet had time to consider the content of the letter. Richard Samuel stressed that the CCGs and HCC were partners in addressing challenges to health and social care. It was important to ensure that the relationship between the organisations was constructive. There were three important points in the letter, which were an enhanced BCF governance structure, a change in capacity and control over the fund.
Gill Duncan informed the meeting the Deloitte had been engaged to carry out
work for HCC, focusing on areas of redesign, and circulated a paper detailing a high level scope of the BCF. A number of changes of focus were under discussion, including Free Nursing Care, the use of CQUINs, the scaling up of primary care and the use of tele-healthcare. New models would aid in the reduction of emergency admissions. This was an opportunity to be bold in planning.
There would need to be a Joint Programme Management and Governance
infrastructure between the CCGs and HCC. Therefore it would be useful for CCGs and HCC to commission Deloitte jointly. Telehealthcare was seen as an important tool.
David Chilvers commented that a visit was planned to the BT Telehealth project
Centre in Cornwall, to explore the advantages of this way of service delivery. It was important to ensure that changes were made in a timely way to avoid additional costs.
Karen Ashton presented a review of existing s256 agreements, which would
now be affected by the implementation of the BCF. It was therefore proposed that the agreements be extended by one year. Some of the agreements related to individual CCGs and others would need to be signed off by all CCGs. Agreements relating to Children’s services were not included in the review. There would be a funding gap between s256 and the BCF: CCG funding of s256 stood at £15m, with some funding from NHS England.
Members commented that funding between CCGs was not equal, with
differential gaps. It was agreed that s256 agreements stand for the current financial year, and roll over to the next financial year.
The Hampshire Commissioning Group:
5
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�195�of�237Page�10�of�52

• Noted the information provided in the review of existing s256 agreements
• Agreed to approve the approach to negotiation for 2014/15 agreements in the context of the Better Care Fund
• Agreed to work towards a Joint Programme Management and Governance infrastructure for the Better Care Fund, with work being carried out by Deloitte
9 Structure for Hampshire Vulnerable Adults Service Team Inger Hebden presented a review of the current structure and working
arrangements of the Hampshire wide Vulnerable Adults Team. The structure was being reviewed in the light of the retirement of the current Associate Director, which was a key role to replace.
It was agreed to defer this item until the next meeting, due to lack of time. The Hampshire Commissioning Group:
• Noted the review of the current structure and working arrangements of the Hampshire wide Vulnerable Adults Team
• Agreed to discuss the matter at its next meeting. 10 Children’s Services – General Update
Angela Murphy presented an update on Children and Maternity Commissioning, on five work programme areas. Paediatric Therapies Tender Solent NHS Trust had been awarded the contract in both the north and south areas of the county, and was working towards mobilisation. Recommendation 1: to note progress and receive future updates on the therapies mobilisation programme. S75 Agreement – CAMHS Strategy, CAMHS service improvement programme Service improvement plans were in place following a deep dive inspection which included quality leads, and progress had been made. It was noted that there had been a significant increase in referrals to the service since the beginning of the contract. The increase had been steady, but with higher complexity of cases and longer treatment times. The CSU had applied a 1.8% reduction in payment to the service provider, Sussex Partnership NHS Foundation Trust (SPFT). Detailed discussions had been held with SPFT; the
6
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�196�of�237Page�11�of�52

organisation had responded to the Action Plan and had submitted evidence of work being undertaken to make improvements to the system. Sarah Schofield noted the increase in the number of referrals, and wondered if any preventative work could be carried out before referral. Mike Fulford confirmed that CAMHS was a priority for NHS England, and believed that financial savings could be made at lower tiers of the service. This was currently under discussion. Members were supportive of the service improvements, which needed further evidence. Members agreed to recommendation five, that an additional joint child health commissioner be appointed. Recommendation 2: There is an uncommitted budget within the s75 agreement for 2013/14. It was recommended that any verified service capacity gaps be addressed through use of this budget and more work is undertaken to ascertain future funding requirements of the service. Recommendation 3: Hampshire Commissioning Group establish whether contract support should be supplied through the CSU for the Child & Adolescent Mental Health Contract as contract variations are required and there is no contract manager allocated to the service currently. Recommendation 4: Extend the current CAMHs contract until September 2015 to enable time for new procurement legislation to move through Parliament; commence the market engagement activity and drafting new specification between January and April 2014. Recommendation 5: Part of the uncommitted s75 budget was in the past used for commissioner posts that have since left and not been replaced. It is recommended by the JCHCB that an additional joint child health commissioner be appointed on a permanent basis to help manage the demands of the joint partnership services and detailed tendering activities that are due to commence this post is currently covered on a fixed term contract. S136 Alternative Place of Safety A full options appraisal and costings was being developed and would be brought to a future meeting. Recommendation 6: To receive the full options appraisal in February 2014, to note that finances will need to be identified.
7
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�197�of�237Page�12�of�52

Children’s Continuing Care It was suggested that Diane Wilson be involved in the proposed changes to the service. Recommendation 7: to receive an end of year report per CCG on continuing care activity. Children and Families Bill The Children and Families Bill was expected to become statute in September 2014, and would ensure a joined up approach to services for children and young people with special educational needs. It was recommended that a joint transition co-ordinator be appointed. The Commissioning Leads of the CCGs would sign this off. Recommendation 8: The Hampshire Commissioning Group may like to consider the following options in terms of this appointment: 1 Appoint to a temporary 12 month full time position (subject to
appropriate job evaluation), likely band 7 or 8a 2 Develop the proposal further with more detail and present to the
following of the Hampshire Commissioning Group Richard Samuel believed that more emphasis should be placed on Children and Maternity Commissioning, and requested that Angela Murphy provide regular updates to the individual CCGs. Barbara Rushton added that Children’s Services at Hampshire County Council should also have an input. The Hampshire Commissioning Group: • Noted the progress described in the paper • Agreed the eight recommendations detailed above.
11 Children’s Risk Log Angela Murphy presented the Children’s Risk Log to bring members up to date
on current risks related to Children’s Services delivery, excluding safeguarding factors.
The Hampshire Commissioning Group noted the Children’s Risk Log. 12 Individual Funding Requests – Processes This item was not discussed due to lack of time.
8
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�198�of�237Page�13�of�52

13 Continuing Healthcare: Phase 2 Proposals This item was deferred due to lack of time. 14 Chronic Fatigue Service This item was not discussed due to lack of time. 15 Hampshire Health and Wellbeing Board Richard Samuel reminded members that the Health and Wellbeing Board
(HWB) had requested a joint presentation on the strategies of the five Hampshire CCGs. Barbara Rushton commented that it was important for the HWB to see the strategies, and agreed to speak to a presentation at the next meeting of the HWB.
16 Hampshire Health Overview and Scrutiny Committee It was noted that the next meeting of the HOSC would take place on 28
January 2014; the papers had recently been published. 17 Future Agenda Items
• Formal Review on Safeguarding • Children’s Contracts S256 – AM – March 2014 • Adoption Medical Advisors (Naomi Black)
18 Next meeting The next meeting would now be held on 9.30 am on Wednesday 19 February
2014 in the Denning Room, Elizabeth II Court, Hampshire County Council, The Castle, Winchester, SO23 8UJ.
9
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�199�of�237Page�14�of�52

Minutes Minutes of the meeting of the South Eastern Hampshire Clinical Commissioning Group Clinical Cabinet held at 3.30 pm on Wednesday 27 November 2013 in the Board Room, Commissioning House, Building 003, Fort Southwick, James Callaghan Drive, Fareham, Hampshire, PO17 6AR
Present Dr Andrew Douglas Dr Jenny Allinson Dr Alastair Bateman Dr Roddy Bowerman Jo Hockley Dr Andrew Holden Richard Samuel Andrew Wood
Chair – Planned Care Lead Unscheduled Care and Mental Health Lead Prescribing Lead Quality and Governance Lead Chair, Practice Managers Commissioning Advisory Group Practice Performance Lead Chief Officer Chief Finance Officer
In attendance
Alex Berry Sian Davies Sandra Jenkinson
Chief Commissioning Officer Public Health Consultant Committee Support Officer
Apologies Julia Barton Dr Barbara Rushton Sara Tiller
Chief Quality Officer CCG Chair & Strategic Development Lead Chief Development Officer
1 Apologies for Absence Apologies for absence were received from Julia Barton, Dr Barbara Rushton
and Sara Tiller. 2 Register and Declarations of Interest Members were asked if they had any interests to declare relating to agenda
items being considered at the meeting. Dr Roddy Bowerman declared an interest in the Community Ophthalmology Service (minute 6.1). His practice currently provided the existing GOS18 service. Dr Bowerman took part in the discussion but did not take part in the final decision.
The Clinical Cabinet:
• received and noted the Register of Interests of Members
3 Minutes of the Previous Meeting The minutes of the meeting held on 23 October 2013 were agreed as a correct
record.
1
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�200�of�237Page�15�of�52

4 Summary of Actions and Matters Arising
Date Minute Ref
Action Who Progress
23.10.13 6.1 Inform NHS England Local Area Team (Wessex) that GP practices had not yet signed formal tenancy agreements re the Chase Community Hospital
ST Completed
23.10.13 6.1 Visit GP Practice to discuss any issues around location within the Chase Community Hospital
RS/AW Completed
A telephone conversation had been held with representatives of a practice that
had been invited to relocate to the Chase Community Hospital. NHS Property Services had become involved, as the practice would face negative equity issues.
5 Local Items for Discussion 5.1 Summary on Obesity It was agreed to defer this item until January 2014 due to time constraints. 5.2 Feedback from Member Practices Dr Andrew Holden had no current feedback from member practices. 6 Any Other Business 6.1 Community Ophthalmology Service A paper on the proposed pilot for a Tier 2 Community Ophthalmology service
had been discussed at the joint meeting of the Fareham & Gosport and South Eastern Hampshire CCG Clinical Cabinets.
Members of the Fareham and Gosport CCG Clinical Cabinet had agreed that
commissioners should undertake a limited tender amongst acute providers of ophthalmology, and the final recommendation should be subject to Chair’s Action due to the short timescale. However, members of South Eastern Hampshire CCG Clinical Cabinet wished to have a further discussion on the proposals. It had been agreed that the discussion should take place at the meeting of the South Eastern Hampshire CCG Clinical Cabinet, following the meeting of the joint Clinical Cabinet.
Members continued the discussion and noted the need to make a decision on
changes to the current service. Members also noted that the proposals had been agreed by both Fareham & Gosport CCG and Portsmouth CCG.
Alex Berry explained the procurement process and informed members that
advice had been sought from the procurement team before the proposal had been put forward. If the requirements were revised then the procurement process could delay the implementation of the service.
2
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�201�of�237Page�16�of�52

Members noted that the services provided through the GOS18 referral forms currently worked well, and wondered if the existing service provider could be included in the process. Members then discussed the possibility of including the existing service provider within the proposed contract, and running the two services in tandem. Alex Berry agreed that the commissioning team would work towards aligning the Tier 2 provider with the existing service. The existing provider would need to have a formal NHS contract.
After discussion, the Clinical Cabinet agreed to support a limited tender
amongst existing acute providers of ophthalmology, and align the service with the existing provider.
The Clinical Cabinet:
• noted that this was predominantly a quality initiative to improve patient access to Ophthalmology services within the local health economy
• noted the draft service specification • agreed that commissioners undertake a limited tender amongst
existing acute providers of Ophthalmology • requested that the existing provider be included within the
procurement process • agreed a change to the 2013/14 QiPP plan to include implementation of
the service pending sign off of the final financial arrangements • agreed that the recommendation be subject to Chair’s Action due to
the pressing nature of the capacity in the local health system 6.2 Dr Jenny Allinson suggested that new work should be highlighted in clinical
portfolios. Date of Next Scheduled Meeting
Wednesday 27 November 2013 4.00 – 4.55 pm Board Room, Commissioning House
3
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�202�of�237Page�17�of�52

Minutes Minutes of the joint meeting of the Fareham & Gosport CCG and South Eastern Hampshire CCG Clinical Cabinet held at 1.30 pm on Wednesday 27 November 2013 in the Board Room, Commissioning House, Fort Southwick, James Callaghan Drive, Fareham, Hampshire PO17 6AR
Summary of Actions
Minute Ref
Action Who By
11.3 Amend the term ‘developmental QIPP’ to ‘planned QIPP’. MD Next meeting
Present: Dr Paul Howden Chair – Clinical Cabinet
Lead – Planned Care & Prescribing Fareham & Gosport CCG
Dr Jenny Allinson Unscheduled Care and Mental Health Lead
South Eastern Hampshire CCG
Dr Alastair Bateman Prescribing Lead South Eastern Hampshire CCG
Dr Ian Bell Clinical Member (Clinical Service & IT) Fareham & Gosport CCG Dr Roddy Bowerman Quality and Governance Lead South Eastern Hampshire
CCG Dr David Chilvers CCG Chair Fareham & Gosport CCG Dr Andrew Douglas Planned Care Lead South Eastern Hampshire
CCG Paul Edwards Practice Manager Representative
(Gosport) Fareham & Gosport CCG
Jo Hockley Chair, Practice Managers Commissioning Advisory Group
South Eastern Hampshire CCG
Dr Andrew Holden Practice Performance Lead South Eastern Hampshire CCG
Dr Simon Larmer Clinical Member (Governance Lead) Fareham & Gosport CCG Dr Alan McFarlane Clinical Lead (Practice Performance
and Development) Fareham & Gosport CCG
Richard Samuel Chief Officer Dr Koyih Tan Clinical Member (Engagement Lead) Fareham & Gosport CCG June Thomson Practice Manager Representative
(Fareham) Fareham & Gosport CCG
In Attendance: Alex Berry Chief Commissioning Officer Sian Davies Public Health Consultant, Hampshire
County Council Fareham & Gosport CCG
Michael Drake Head of Planning & Performance Fareham & Gosport, Portsmouth & South Eastern Hampshire CCGs
Sandra Jenkinson Committee Support Officer Keeley Ormsby (for Primary Care Team
1
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�203�of�237Page�18�of�52

items 7.1 and 7.3) Louise Spencer Deputy Chief Quality Officer Andrew Wood Chief Finance Officer Observer: Catherine Dampney Chief Information Officer NHS South
Commissioning Support Unit
Keith Myhill Head of Procurement for SST NHS South Commissioning Support Unit
Apologies: Julia Barton Chief Quality Officer Dr Sally Robins Children and Maternity Lead Fareham & Gosport CCG Dr Barbara Rushton CCG Chair South Eastern Hampshire
CCG Sara Tiller Chief Development Officer 1 Apologies for Absence Apologies for absence were received from Julia Barton (represented by Louise
Spencer), Dr Sally Robins, Dr Barbara Rushton and Sara Tiller. 2 Declarations of Interest The following declarations of interest were made: Dr Roddy Bowerman declared an interest in item 6.2: Community
Ophthalmology Service. His practice provided the existing GOS18 service. It was noted that all GPs would have an interest in item 7.1: Local Enhanced
Services Review. Dr Ian Bell wished to have it noted that he would be attending a course on anti-
coagulation funded by Roche Pharmaceuticals. 3 Minutes of Previous Meeting The minutes of the meeting held on 27 November 2013 were agreed as an
accurate record. However, Richard Samuel requested that minute 5.3: Portsmouth Hospitals NHS Trust (PHT) Recovery Plan be re-written.
4 Matters Arising and Summary of Actions
Date Minute Ref
Action Who Progress
27.11.13 8.3 Work with Jen Allinson to develop service specification for Chronic Fatigue Service
DC Planned
27.11.13 12.2 Send comments on Ambulatory Care Pathway to Andrew Douglas
All Completed
Minute ref 8.3: Dr Jenny Allinson reported that there was nothing specific to report back on the service specification for the Chronic Fatigue Service and work was ongoing. Dr Alastair Bateman suggested that this be progressed outside of the meeting, as this was now a matter of urgency.
2
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�204�of�237Page�19�of�52

Alex Berry informed the meeting that discussions would be held with Portsmouth Hospitals NHS Trust (PHT) on the Ambulatory Care Pathway.
5 Chair’s Report The Chair welcomed everyone to the meeting, which had a busy agenda. 6 Commissioning 6.1 End of Life Baseline Review Dr David Chilvers presented a summary of current service provision for End of
Life Care (EoLC) across both Fareham & Gosport and South Eastern Hampshire CCGs. The paper also advised on the opportunity for the CCGs to commission EoLC services moving forward.
It was believed that a unified management option was needed across Fareham
& Gosport, Portsmouth and South Eastern Hampshire CCGs. Provision across the three CCGs was currently diverse, and equity was needed. The strategy for EoLC had been discussed at meetings between the three CCGs.
Advance care plans for dementia patients were currently being developed. Dr Roddy Bowerman reminded the meeting that discussions had been held
nationally following adverse media coverage of the Liverpool Care Pathway (LCP). It was noted that the LCP had originally been developed for palliative care of cancer patients. It was proposed that local care pathways now be designed where appropriate. Alex Berry believed that the redesigned pathway would give an opportunity to achieve savings, although further work was needed on the strategy. The CCGs were part commissioners of services from local hospices. This provision linked to the CCG strategy of provision of care out of the acute sector.
Members discussed the role and status of local hospices. Andrew Wood
agreed to clarify any non contractual flows of funding to hospices providing EoLC to the CCGs.
It was noted that the strategy contained reference to the Liverpool Care
Pathway, and this reference should be removed. The Joint Clinical Cabinet agreed to undertake a systematic redesign of
all South East Hampshire End of Life Care services, with the aim to: • Establish a series of commissioner led workshops with service user
and provider involvement to identify opportunities • Evaluate current financial position and the opportunities within the
financial envelope to redesign the services • Establish a service specification looking at best practice elsewhere
and drawing in the learning from the Portsmouth CCG experience • Return with a progress report in June 2014 with a firm
recommendation on the next steps The Joint Clinical Cabinet also agreed to:
• Allocate a time to discuss the proposal at Clinical Leaders Group
3
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�205�of�237Page�20�of�52

• Receive the Wessex EoL Commissioning Board and PSEH EoL Steering Group response to the LCP Review, note its content and support the interim arrangements proposed in Appendix 1 to the report
• Review the draft PSEH EoL Strategy 6.2 Community Ophthalmology Service Dr Paul Howden presented a brief on the proposed pilot for a Community
Ophthalmology service, with a draft service specification. The pilot was designed to improve patient access to Ophthalmology services
within the local health economy following discussions with local ophthalmologists and the Local Optical Committee.
PHT had notified commissioners of an increased risk relating to a backlog of
Ophthalmology follow-ups. Over 3000 patients were waiting for a follow-up with no capacity at PHT to book these patients. PHT had proposed that no new referrals be made for a period of six weeks from January 2014. CCG Clinical Leads had requested an alternative solution to the proposal.
A solution to the level of demand was therefore a priority. This would also
assist in realising the aims of the 2013/14 QiPP scheme. The Commissioning Team had taken advice on procurement of a service, and
this would take between 12 and 18 months to process. A limited tender amongst existing providers would be subject to a shorter timescale, giving a significant reduction in referrals.
Members then went on to discuss the proposed pilot scheme. The scheme
would be provided on a sessional basis rather than tariff, which would enable financial savings. It was agreed that a solution to the backlog at PHT was needed, and that a proportion of the follow-ups were of low grade and therefore suitable for treatment by community optometrists. Dr Roddy Bowerman expressed concern that there was a reputational risk if parts of the service were removed from Queen Alexandra Hospital.
There was currently no community service within Fareham & Gosport, and
members were supportive of the scheme. Members of South Eastern Hampshire Clinical Cabinet expressed some
reservations around the short notice given to discuss the scheme. It was also noted that an existing GOS18 scheme was provided by the Forest End surgery. A suggestion was made that the pilot scheme run in parallel to the existing GOS18 service, which was accepted to be successful.
Dr David Chilvers reminded the meeting that, as there was not consensus
between both CCGs, two decisions would need to be made. It was therefore agreed that members of South Eastern Hampshire CCG continue the discussion at the following meeting of the South Eastern Hampshire CCG Clinical Cabinet.
The Joint Clinical Cabinet:
4
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�206�of�237Page�21�of�52

• Noted that this was predominantly a quality initiative to improve patient access to Ophthalmology services within the local health economy
• Noted the draft service specification Fareham & Gosport Clinical Cabinet:
• Agreed for commissioners to undertake a limited tender amongst existing acute providers of Ophthalmology
• Agreed a change to the 2013/14 QiPP plan to include implementation of the service pending sign off of the final financial arrangements
• Agreed that this financial recommendation be subject to Chair’s Action due to the pressing nature of the capacity in the local health system
South Eastern Hampshire CCG:
• Agreed to hold a further discussion on the proposal at the meeting of the South Eastern Hampshire CCG
6.3 Individual Funding Requests Andrew Wood presented a paper to advise the Clinical Cabinet on payments to
contractors under the arrangements for specialist services which were not normally commissioned locally.
Individual Funding Requests (IFRs) were administered by NHS South
Commissioning Support Unit (CSU) under policies to inform clinical decisions. The service offered by the CSU was considered to be good.
This was a Hampshire-wide service, and it was noted that both Fareham &
Gosport and South Eastern Hampshire CCGs referred more requests than other Hampshire CCGs. It was suggested that practices should receive information and training on the use of the IFR route; this was a potential subject for Target.
The Joint Clinical Cabinet noted:
• The work carried out by NHS South Commissioning Support Unit to ensure that specialist referrals were approved where such services were not routinely available from existing contracts
• That the CCGs needed to have more direct involvement in the decision making process to ensure that decisions were robust and appropriate
• The need to ensure that processes for validating the quality and outcomes of the providers used by the population of the two CCGs were in place
• The on-going need to review current services provided via Individual Funding Requests for potential opportunities to establish contracts for such services
6.4 Winter Surge and Escalation Plans Alex Berry presented the winter surge and escalation plans for South East
Hampshire, which gave details of each provider organisation’s roles and activities. The plans had been approved by NHS England Local Area Team (Wessex). The process had been updated following a desktop exercise held in October 2013.
5
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�207�of�237Page�22�of�52

NHS England would embed primary care escalation within its Escalation Framework.
The Joint Clinical Cabinet noted the plans, and noted that this was a live
document and subject to change. 6.5 Wheelchair Re-tendering Briefing Update Dr Andrew Douglas presented an update on the progress of the wheelchair
service retendering. Solent NHS Trust, the current provider, had given notice with effect from 31
March 2014. A service specification for the Hampshire-wide retender had been approved at a meeting of the Joint Clinical Cabinet held on Wednesday 25 September 2013.
The Joint Clinical Cabinet agreed to authorise Chair’s Action for the
ratification of the new provider in December 2013. 6.6 Specialist Musculoskeletal and Persistent Pain Self-Management Service
Update The Joint Clinical Cabinet received an update on the progress of the specialist
Musculoskeletal and Persistent Pain Self-Management Service procurement process.
The current provision for specialist musculoskeletal services within Fareham &
Gosport and South Eastern Hampshire CCGs expired in March 2012. The service was extended until April 2014 to allow for the tender of a new service. A procurement process had been undertaken, and a new provider was in the process of being chosen. The new provider would be announced before the next meeting of the Clinical Cabinet.
Dr Andrew Holden requested a further update once the provider had been
appointed. The Joint Clinical Cabinet agreed to authorise Chair’s Action for the
ratification of the new provider in December 2013. 6.7 Integrated Care Pilots Dr Jenny Allinson presented an update on the progress towards developing
integrated community care teams across the Fareham & Gosport and South Eastern Hampshire CCGs. The focus of the paper was largely on key developments to date and forthcoming plans.
A paper had been discussed at the meeting of the South Eastern Hampshire
CCG Clinical Cabinet held on 23 October 2013 on the development of the Bordon integrated care pilot. There were currently two pilot sites within South Eastern Hampshire, supported by community care teams. Patients would be selected to take part in the scheme through a risk stratification tool, the Adjusted Clinical Group tool.
6
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�208�of�237Page�23�of�52

The pilots would be managed by weekly team meetings, and by monthly practice based visits.
It was noted that some teams had currently stepped back from integrated care
while waiting for data from the pilot sites. Work had begun across Fareham & Gosport with one pilot site area identified
in Gosport. Dr David Chilvers noted that the pilot sites were working well. However, there
were issues around staff resources and data. Portsmouth CCG had bought in some GP time. A workshop would be held for Fareham & Gosport GPs.
Louise Spencer asked if there were any information governance issues
associated with the pilot. Dr Jenny Allinson responded that Southern Health NHS Foundation Trust would download data to GP practices. Catherine Dampney added that there had been some disagreement over the use of stratification tools in patient care. NHS England had proposed that the rules on data sharing be changed. Clarification on this was awaited.
The Joint Clinical Cabinet noted progress to develop new models of
integrated care for the local populations of Fareham & Gosport and South Eastern Hampshire.
7 Primary Care 7.1 Local Enhanced Services Review Dr Andrew Holden presented recommendations for local commissioned
services (LCS) for 2014/15, currently commissioned through Local Enhanced Services (LES) agreements.
Members were asked to consider the recommendations, and a further report
would be brought to a future meeting of the Joint Clinical Cabinet. Diabetes The recommendation was to re-commission the service into an NHS Standard
Contract. One component of the LES was to carry out an in-practice audit of one aspect of diabetes care delivered by the practice. Audits would continue to take place, when Quality and Outcomes Framework scores were not being achieved. The LCS would include input from the community diabetes team.
Minor Injuries The recommendation was to de-commission the minor injuries unit in Havant
LES as strategic aims were not being achieved. The suturing LES should be re-commissioned and offered to all practice as this service was well used. A pilot minor injuries service in Emsworth and Bordon would be considered. It was planned to move minor injuries services into primary care.
Richard Samuel suggested that Fareham was an area suitable for a minor
injuries unit. Andrew Holden thought that a hub model of minor injuries provision was good, and had not been achievable through a LES.
Extended Hours Reception Scheme
7
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�209�of�237Page�24�of�52

The recommendation was to de-commission the LES. There was no significant patient access in relation to the payment, and some practices had an extended hours reception without payment. The proposed 8.00 am until 8.00 pm surgery opening hours would negate the need for the LES.
Toxic Drugs and Near Patient Testing This service was mainly used within second line therapies, and there was a
disparity of funding. A joint approach was being considered across three CCGs, and this would give clarity to secondary care consultants. This would allow new drugs to be incorporated as developed. Alastair Bateman said that drugs may not be prescribed if they were not part of a shared care agreement.
No decision had yet been made on a recommendation. Domicillary It was recommended that the domiciliary element be de-commissioned. The
new contract should be for ‘Shared Care’, with a specification to include the three CCGs and offered to all practices with an equal remuneration fee.
Anti-coagulation It was recommended that the anti-coagulation LES be de-commissioned, as
patients on warfarin would be referred to anti-coagulation clinics provided by secondary care. Acute warfarin initiation would be commissioned on an LCS, following guidelines.
BNP and D-Dimer It was recommended that BNP be de-commissioned in Fareham & Gosport
and offered to patients through a service commissioned from PHT. The BNP service was not cost effective. The D-Dimer service was work in progress.
Commissioning LES The commissioning LES was signed up to by all practices in both Fareham &
Gosport and South Eastern Hampshire CCGs. It was recommended that the commissioning LES be recommissioned. Component 2: Effective and Efficient Use of NHS resources should be subject to formal review.
Phlebotomy No final decision had been made about the phlebotomy service, and three
options were listed in the report. It was suggested that a combination of options 1 and 2 be followed, with option 3 to be in place at a later date. Some investment in the phlebotomy service might lead to financial savings.
Nursing Homes It was recommended that the current LES be decommissioned and resources
invested in new services to meet the CCGs’ strategic aims. Ending the contract would not destabilise services. The new LCS would give better and more specific outcomes to patients.
The Chair wished to thank Dr Andrew Holden and Keeley Ormsby for the work
put into reviewing Local Enhanced Services, and noted that firmer proposals would be brought to a future meeting of the Joint Clinical Cabinet.
The Joint clinical Cabinet considered and agreed the recommendations
for the following LESs: • Diabetes
8
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�210�of�237Page�25�of�52

• Minute injuries • Extended hours receptionist • Toxic drugs and near patient testing • Anti-coagulation • BNP and D-Dimer • Commissioning • Phlebotomy • Nursing Homes
7.2 Primary Care Membership Framework
Dr Alan McFarlane presented a paper which set out the principles of a membership framework: this was designed to be a working paper. One of the issues faced was of giving timely feedback to member practices. Practices may not be aware what the GP leads had achieved. A mechanism was needed to show achievements and to share ideas. Currently there was variable knowledge and engagement amongst GPs in member practices. Appendix 1 to the report described proposals to develop the existing Clinical Discussion Fora (CDF). Fareham & Gosport CCG and South Eastern Hampshire CCG managed these meetings as different models. It was agreed that good engagement was needed with member practices, and that feedback should be given in a timely way. Incentives would be given through the Quality and Outcomes Framework (QOF), and this would need to be reviewed. Outcomes of any initiatives should be credited to the lead proponent in any feedback to practices. It was noted that a lot of informal engagement and contacts was taking place, and engagement was being made with practice nurses. The option of a ‘talent register’ was discussed, similar to information held within Portsmouth CCG. One way of obtaining this information would be by the use of an online survey (such as SurveyMonkey). This would also be useful for succession planning for the future.
The Chair thanked Dr Alan McFarlane for the work put into developing the Primary Care Membership Framework, and the proposals for CDF.
The Joint Clinical Cabinet:
• Agreed the principles set out in section 4 of the Primary Care Membership Framework (PCMF)
• Agreed the model detailed in sections 5 and 6 of the PCMF • Noted the progress on engagement set out in section 7 of the PCMF • Agreed the priorities identified for 2014/15 under paragraph 8.2 of the
PCMF • Considered and agreed the proposals for Clinical Discussion Fora in
Appendix 1 of the CDF 7.3 Optometry LES Review Dr Paul Howden presented a paper which set out recommendations for the
three Optometry LES currently commissioned.
9
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�211�of�237Page�26�of�52

Low Vision LES It was recommended that this be recommissioned as a compact with
Portsmouth CCG with a revised specification. This specialised service should be offered to current providers through a single tender action. An uplift to remuneration should be considered.
Stable Glaucoma It was recommended that this be recommissioned as a compact with
Portsmouth CCG with a revised specification. This specialised service should be offered to all providers that could demonstrate compliance through a single tender action with an uplift to remuneration.
The Local Optical Committee was making contact with optometrists; it was
hoped that increased tariffs would give a better response from optometrists, leading to an improvement in the service.
Glaucoma Intra Ocular Pressure It was recommended that the service be decommissioned as there was no
evidence that it had a significant impact on new referrals to secondary care and activity levels were low.
The Joint Clinical Cabinet agreed the recommendations for the following
Optometry LES: • Low vision • Stable glaucoma • Glaucoma intra ocular pressure
8 Portfolio Updates 8.1 Medicines Management There was nothing new to report on medicines management. 9 Governance 9.1 CCG Priorities Committee Dr David Chilvers presented the Terms of Reference, Ethical Framework and
Notes of the Priorities Committee meeting held on 17 September 2013. The Priorities Committee was a committee of representatives of CCGs across
Hampshire, Southampton, Isle of Wight, Portsmouth and Surrey. This large committee had proven to be difficult to get under way.
One item on the agenda of the Priorities Committee meeting was IVF, and
recommendations would be disseminated to all CCGs. Alex Berry noted that the Ethical Framework should align with the Ethical
Framework of both CCGs. The Joint Clinical Cabinet noted:
• The terms of reference of the Priorities Committee • The Ethical Framework of the Priorities Committee • The notes of the meeting held on 17 September 2013
10
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�212�of�237Page�27�of�52

10 Quality 10.1 Joint Quality Report
Dr Roddy Bowerman presented a paper which detailed the quality position against commissioned services at month 6 and Quarter 2 outlining current assurances and actions being taken around issues of concern. The report contained an executive summary covering the following providers: • Portsmouth Hospitals NHS Trust • South Central Ambulance Service NHS Foundation Trust – 999 • South Central Ambulance Service NHS Foundation Trust – 111 • South Health NHS Foundation Trust • Royal Surrey County Hospital NHS Foundation Trust • Sussex Partnerships Child & Adolescent Mental Health Services • University Hospital Southampton NHS Foundation Trust
The issues had been discussed in greater detail at a meeting of the Quality and
Safety Committee. The following items were of particular note. Portsmouth Hospitals NHS Trust PHT had not been able to meet the contractual requirements for the issue of
discharge summaries in the agreed process or the timescale of 24 hours. An interim action plan was in place to improve the processes.
South Central Ambulance Service NHS Foundation Trust - 999 A total of 13 Serious Incidents Requiring Investigation (SIRIs) had been
reported to date, under the key category of ambulance (general). Royal Surrey County Hospital NHS Foundation Trust (RSCH) A significant number of quality and performance areas were identified as being
below expectation. The Care Quality Commission (CQC) had carried out an inspection in October 2013, and RSCH had received a rating of band 2 (1 was the highest risk).
Child & Adolescent Mental Health Service – Sussex Partnership NHS
Foundation Trust This service had a high risk rating, but assurances had been received that
processes were in place to make improvements to the service. Southern Health NHS Foundation Trust A CQC inspection had outlined concerns regarding care for patients within a
residential setting for people with learning disabilities (LD) in Oxford. In addition, a SIRI had been reported in association with LD services, which had raised concerns around governance. A media alert was in place.
Dr Bowerman suggested that the Quality Report be presented to the Joint
Clinical Cabinet in more detail on a quarterly or half yearly basis. Louise Spencer drew the attention of the meeting to the PHT Commissioning
for Quality and Innovation (CQUIN) report, in particular the result for dementia. Feedback was needed on the identification of dementia within PHT. Members had a short discussion on the diagnosis of dementia. Dr Andrew Holden believed that screening could be carried out within an acute setting, but
11
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�213�of�237Page�28�of�52

assessment would be more difficult. It was more appropriate to carry out diagnosis of dementia within primary care.
The Joint Clinical Cabinet noted the information contained within the
Provider Quality Summary Report for month 6 and Quarter 2. 11 Finance and Performance 11.1 Finance Report Andrew Wood presented a report to inform the Joint Clinical Cabinet of the
finance position as at month 7 2013/14 of: • Fareham & Gosport CCG • South Eastern Hampshire CCG
Both CCGs were currently on plan to meet planned target surpluses. Issues of
particular note included the anticipated position of PHT at year end. PHT had requested an increase the value of its contract. Both CCGs faced a significant challenge to meeting QIPP surplus targets. It was expected that the targets for the year 2014/15 were £8-11m for Fareham & Gosport CCG and £9-12m for South Eastern Hampshire CCG.
The Joint Clinical Cabinet accepted the contents of the Finance reports. 11.2 Performance Report Michael Drake presented a report to inform the Governing Body of the
performance position, and highlighted a number of issues of note. Fareham & Gosport CCG There was one case of a patient waiting over 52 weeks for treatment relating to
Fareham & Gosport CCG; however, this was for a complex procedure. A breach of mixed sex accommodation was currently being investigated.
Joint areas of concern There was underperformance in referral to treatment for patients admitted
within 18 weeks. PHT had planned to reduce a backlog, and been successful. However, underperformance was anticipated in the following month.
There had been underachievement in a number of cancer targets relating to
both CCGs. Eight out of nine targets had not been reached in September 2013, and all nine targets had not been achieved in Quarter 2.
There had been an improvement in performance in the Emergency
Department. PHT had achieved 95%, but this had recently dipped to just under 95%.
PHT had provided assurance to the NHS Trust Development Authority that it
would achieve and sustain compliance in three key areas of performance: • 4 hour waits in the Emergency Department by October 2013 • RTT (at aggregate and speciality levels with the exception of Urology) by
November 2013 • Cancer waits by November 2013. PHT was currently on target to meet
these deadlines.
12
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�214�of�237Page�29�of�52

Achievement of the Quality Premium by both CCGs was dependent on monthly figures, but there was an expectation that some of the Quality Premium would be achieved. The Joint Clinical Cabinet noted the contents of the Performance Report.
11.3 Planning Process 2013/14 Update Michael Drake presented an update of progress to date against the planning
process for 2013/14. Both Fareham & Gosport and South Eastern Hampshire CCGs had achieved
savings relating to QIPP schemes. Additional schemes were being looking at, although they were not expected to have a significant impact. A workshop had been held to discuss QIPP schemes for the year 2014/15, and this had been well attended.
The updated Stroke Services Project Plan was attached as Appendix B. Andrew Wood requested that the term ‘Developmental QIPP’ be amended to
read ‘Planned QIPP’. Action: MD
Dr Andrew Douglas commented that the CCGs should focus on large QIPP
projects, as all projects took a lot of resources. Alex Berry added that procurement was a time consuming process.
The Joint Clinical Cabinet:
• Reviewed the update • Agreed the recommendations:
- Note QIPP delivery at Month 7 - Note the update provided in regard to the project plan update and
to approve in principle the proposal - Share any QIPP ideas and/or suggestions with the Planning Team
for review, research and, potentially, work up into project plans to help address the QIPP challenge
- Provide clinical and executive support to the ongoing and continuous planning process (particularly around delivery of 2013/14 expectations and planning for 2014/15 and beyond).
12.1 Minutes/notes from other meetings The Joint Clinical Cabinet noted the minutes/notes of:
• Quality and Safety Committee – 9 October 2013 13 Any Other Business 13.1 Richard Samuel gave members an update on Unit of Planning. NHS England
had issued a letter on 4 November 2013 requiring each CCG to nominate a preferred choice of unit for strategic and operational planning by 12 November 2013. Discussions had been held with partner organisations on suitable Units of Planning (UoP) for the CCG. Following consultation with members, a proposal had been submitted for a combined UoP with Fareham & Gosport
13
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�215�of�237Page�30�of�52

CCG. Further clarifying guidance had since been issued by NHS England, and proposals would be revised in accordance. It was therefore necessary to revise the CCG’s existing proposal to widen the UoP. Members agreed that there was a need to work in partnership across Hampshire due to the impact of the Integration Transformation Fund, and amend the UoP accordingly.
13.2 Dr Ian Bell wished to update members on GP IT systems. Current policy was
to move practices to hosted systems, however decisions would need to be made a practice level. At the present time over two thirds of practices were on hosted networks.
Dr David Chilvers commented that financial savings could be made if all
practices used the same IT system. Members agreed that a radical solution to the connectivity of different IT systems was needed. There was also a need to integrate with provider organisations. Work would be carried on through the IT Enabling Change Board.
13 Future Agenda Items
• Update on Specialist Musculoskeletal and Persistent Pain Self-Management Service - AB
14 Date of Next Scheduled Meeting Wednesday 29 January 2014 1.30 – 3.50 pm Board Room, Commissioning House
14
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�216�of�237Page�31�of�52

Minutes Minutes of the meeting of the South Eastern Hampshire Clinical Commissioning Group Clinical Cabinet held at 4.00 pm on Wednesday 29 January 2014 in the Spindle meeting room, 1000 Lakeside, North Harbour, Western Road, Portsmouth, PO6 3EN
Present Dr Barbara Rushton Dr Jenny Allinson Julia Barton Dr Alastair Bateman Dr Roddy Bowerman Dr Andrew Douglas Jo Hockley Dr Andrew Holden Richard Samuel Sara Tiller
CCG Chair & Strategic Development Lead Unscheduled Care and Mental Health Lead Chief Quality Officer Prescribing Lead Quality and Governance Lead Planned Care Lead Chair, Practice Managers Commissioning Advisory Group Practice Performance Lead Chief Officer Chief Development Officer
In attendance
Lyn Darby Sian Davies Sandra Jenkinson
Deputy Chief Commissioning Officer Public Health Consultant Committee Support Officer
Apologies
Alex Berry Andrew Wood
Chief Commissioning Officer Chief Finance Officer
1 Apologies for Absence Apologies for absence were received from Alex Berry and Andrew Wood. 2 Register and Declarations of Interest Members were asked if they had any interests to declare relating to agenda
items being considered at the meeting. No specific interests were declared. The Clinical Cabinet:
• received and noted the Register of Interests of Members
3 Minutes of the Previous Meeting The minutes of the meeting held on 27 November 2013 were agreed as a
correct record.
1
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�217�of�237Page�32�of�52

4 Summary of Actions and Matters Arising There were no matters arising. 5 Local Items for Discussion 5.1 Summary on Obesity Sian Davies wished to highlight the following to members of the Clinical
Cabinet: • the epidemiology of overweight & obesity locally • the population health implications of overweight and obesity • current measures to prevent and treat obesity • suggestions for further action to prevent and treat overweight and obesity
Obesity was an issue which affected the health of individuals. Childhood obesity would have an impact on the future health of adults. Levels of obesity were considered to be an issue across the country, and would lead to higher levels of diabetes and heart disease within the population. The Public Health team was carrying out health promotion and intervention work across the county. These small pieces of work would have some lasting effect. Public Health had made an input into the development of the CCG’s strategy, and prevention would be considered as a part of the commissioning process. Sara Tiller reported that the issue of obesity had been discussed at the Clinical Assembly, and would be a priority for GPs, the third sector and local authorities. There would be opportunities to work with partners. Jen Allinson would represent the CCG on the Havant Health and Wellbeing Board, and the CCG was represented on other local Health and Wellbeing Boards. Members of the Clinical Cabinet discussed the issue of obesity. It was felt that it would be helpful to have weight charts on the primary care information portal for GPs to access. Sue Crane (Associate Dean, Health Education Wessex) would have a role in the co-ordination of GP training, and would be able to include a focus on obesity. Members agreed that the obesity was an important issue to address, and should remain a priority. The Clinical Cabinet: • acknowledged the paper on obesity • agreed to work with other agencies to promote a strategic approach to
preventing and treating overweight and obesity • considered how services could be commissioned to reduce the
prevalence of obesity in the population and consequent health and economic impact
2
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�218�of�237Page�33�of�52

5.2 Feedback from Member Practices Andrew Holden informed the meeting that the lack of feedback from practices
was being addressed through TARGET. It was noted that the feedback button on the PIP pages was not working.
Sara Tiller added that there was currently not enough resource in the primary
care team to address the issue, but that a new member of staff would be starting on 1 February 2014. The communications team would be moving from NHS South Commissioning Support Unit into the CCGs, and would be a shared service with Portsmouth CCG.
The Clinical Cabinet noted the verbal update on feedback. 6 Any Other Business 6.1 Chase Community Hospital The population served by the hospital was not large enough for some specialist
clinics. It was therefore suggested that some outpatient clinics be carried out by remote consultation. Video-conference equipment could be installed, and the consultation carried out by a consultant, with a nurse accompanying the patient at Chase. BT operated a telehealth hub in Cornwall, and a visit to the facility was planned.
Lyn Darby added that remote consultations could be included in the tender for
the Independent Sector Treatment Centre in the longer term to include St Mary’s Community Hospital, Oak Park and the Chase Community Hospital.
Sara Tiller informed the meeting that the full business case for the Chase
would be brought to a future meeting, and would have to go through the NHS Property Services approval process. It was expected that the model would change.
Andrew Holden expressed concern over the effect on Petersfield Hospital, and
thought that the property resource should be examined. Barbara Rushton believed that the Chase and Petersfield would work together.
The Clinical Cabinet noted the verbal update on the Chase Community
Hospital. 6.2 Barbara Rushton gave a brief update on a recent meeting of the Hampshire
Commissioning Group. 6.3 Barbara Rushton gave an update on the preparation of the CCG Strategy, with
both Jenny Allinson and Andrew Holden involved in the discussions. The strategy was required to align with that of other organisations. The first
draft should be submitted by 14 February 2014, and the final version at the end of March 2014. A period of consultation and refinement would end in June 2014. The strategy was a developmental process, which would drive change.
The draft strategy would be shared with members of the Governing Body, and
be brought to a future meeting.
3
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�219�of�237Page�34�of�52

Date of Next Scheduled Meeting Wednesday 26 February 2014 4.00 – 5.00 pm Rowan meeting room, 1000 Lakeside, Northarbour, Western Road, Portsmouth, PO6 3EN
4
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�220�of�237Page�35�of�52

Minutes Minutes of the joint meeting of the Fareham & Gosport CCG and South Eastern Hampshire CCG Clinical Cabinet held at 1.30 pm on Wednesday 29 January 2014 in the Spindle meeting room, 1000 Lakeside, North Harbour, Western Road, Portsmouth, PO6 3EN
Summary of Actions
Minute Ref
Action Who By
4 Take End of Life Baseline Review to a meeting of the Clinical Leaders Group
LD Next meeting
6.1 Distribute notes of a discussion with the LAT on performance at PHT
JB Next meeting
6.1 Share Action Plan relating to SHFT on request JB On request
7.1 Distribute a paper which defines GMS+ AH Next meeting
7.1 Complete the Care Home LCS and take to a future meeting of the Clinical Cabinet
AH/KO
Present: Dr Barbara Rushton Chair South Eastern Hampshire
CCG Dr Jenny Allinson Unscheduled Care and Mental Health
Lead South Eastern Hampshire CCG
Julia Barton Chief Quality Officer Dr Alastair Bateman Prescribing Lead South Eastern Hampshire
CCG Dr Ian Bell Clinical Member (Clinical Service & IT) Fareham & Gosport CCG Dr Roddy Bowerman Quality and Governance Lead South Eastern Hampshire
CCG Dr David Chilvers CCG Chair Fareham & Gosport CCG Dr Andrew Douglas Planned Care Lead South Eastern Hampshire
CCG Jo Hockley Chair, Practice Managers
Commissioning Advisory Group South Eastern Hampshire CCG
Dr Andrew Holden Practice Performance Lead South Eastern Hampshire CCG
Dr Paul Howden Chair – Clinical Cabinet Lead – Planned Care & Prescribing
Fareham & Gosport CCG
Dr Simon Larmer Clinical Member (Governance Lead) Fareham & Gosport CCG Dr Alan McFarlane Clinical Lead (Practice Performance
and Development) Fareham & Gosport CCG
Richard Samuel Chief Officer Dr Koyih Tan Clinical Member (Engagement Lead) Fareham & Gosport CCG June Thomson Practice Manager Representative Fareham & Gosport CCG
1
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�221�of�237Page�36�of�52

(Fareham) Sara Tiller Chief Development Officer In Attendance: David Bailey Deputy Chief Finance Officer Lyn Darby Deputy Chief Commissioning Officer Sian Davies Public Health Consultant, Hampshire
County Council
Michael Drake Director of Planning & Performance Fareham & Gosport, Portsmouth & South Eastern Hampshire CCGs
Malcolm Heritage-Owen (for item 7.1)
Lay member Fareham & Gosport CCG
Sandra Jenkinson Committee Support Officer Keeley Ormsby (for item 7.1)
Primary Care Team
Apologies: Alex Berry Chief Commissioning Officer Paul Edwards Practice Manager Representative
(Gosport) Fareham & Gosport CCG
Dr Sally Robins Co-opted member – Children and Maternity Lead
Fareham & Gosport CCG
Dr Koyih Tan Engagement Lead Fareham & Gosport CCG Andrew Wood Chief Finance Officer 1 Apologies for Absence Apologies for absence were received from Alex Berry (represented by Lyn
Darby), Paul Edwards, Dr Sally Robins, Dr Koyih Tan and Andrew Wood (represented by David Bailey).
2 Declarations of Interest Members were asked if they had any interests to declare relating to agenda
items being considered at the meeting. Paul Howden reminded the meeting that all GPs would have an interest in item 7.1: Locally Commissioned Services – Recommendations.
3 Minutes of Previous Meeting The minutes of the meeting held on 27 November 2013 were agreed as an
accurate record. 4 Matters Arising and Summary of Actions
Date Minute Ref
Action Who Progress
27.01.13 11.3 Amend the term ‘developmental QIPP’ to ‘planned QIPP’.
MD Completed
Paul Howden referred to item 6.1: End of Life Baseline Review. This would be discussed at the Clinical Leaders Group and Lyn Darby would action this.
Action: LD
2
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�222�of�237Page�37�of�52

5 Chair’s Report Barbara Rushton welcomed everyone to the meeting. 5.1 The three CCGs in south east Hampshire had submitted letters to Portsmouth
Hospitals NHS Trust (PHT) expressing concerns over delivery of services, and a wish to see sustained improvement. A response had been received which did not address all of the issues raised by the letter. A follow-up letter had been submitted to PHT, but so far no further response had been received. Julia Barton was preparing a paper for consideration by the Quality Surveillance Group.
It was noted that on some occasions when it appeared that PHT had not met
targets there had been a problem with software, which therefore gave a false impression.
5.2 A meeting had been held between community providers and two members of
the GP Alliance. Work was being undertaken towards an integrated solution between community and primary care.
6 Quality 6.1 Joint Quality Report Julia Barton, Roddy Bowerman and Simon Larmer gave verbal updates on
aspects of work of the Quality team. Portsmouth Hospitals NHS Trust Roddy Bowerman informed the meeting that it had been planned that PHT
move from paper discharge summaries to electronic discharge summaries (EDS) by 1 January 2014. However this had not been implemented in all main wards. It was noted on a visit to Trauma and Orthopaedics that it was taking between 20-40 minutes to complete each EDS. Penalties would be applied if EDS was not used. However, it was also noted that not all practices were able to accept EDS.
Julia Barton reported that a quarterly assurance programme had been held
with the NHS England Local Area Team (Wessex) (LAT) where the potential impacts of operating performance had been discussed, and challenges on quality had been made. Julia Barton agreed to distribute a summary of the discussion to members of the Clinical Cabinet.
Action: JB A quality review meeting was planned for 2 February 2014 between the Care
Quality Commission, Trust Development Authority, PHT and Portsmouth CCG. There were areas of concern around the Friends and Family (F&F) test, and a meeting had been held between PHT, the LAT and the CCGs to discuss these. It was believed that not enough resources were being put into rolling out the F&F test. It was suggested that a Project Manager be put in place to promote the F&F test throughout the hospital.
It was believed that improvements in operational performance would have a
positive impact on quality.
3
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�223�of�237Page�38�of�52

Southern Health NHS Foundation Trust (SHFT) A risk summit had been held, attended by a significant number of
commissioners. SHFT had taken over the Ridgeway learning disability service where significant problems had been identified. In addition, there were concerns over quality in a number of other facilities. A detailed action plan had been prepared; Julia Barton would share this on request.
Action: JB Contract Negotiations A series of pre-contract provider workshops had been held, and clinical
priorities had been explained. Negotiations had started positively. National CQUINs had been looked at, and local CQUINs were being developed to fit in with planning priorities.
Quality Surveillance Hub A paper on the Quality Surveillance Hub (QSH) proposal would be brought to a
future meeting of the next Clinical Cabinet. Members discussed the possibility of marketing the QSH to other organisations
in future. The Joint Clinical Cabinet noted the verbal update on aspects of the work
of the Quality team. 7 Commissioning 7.1 Locally Commissioned Services – Recommendations Malcolm Heritage-Owen was in attendance for this item, as well as Keeley
Ormsby. Andrew Holden reported that the new Locally Commissioned Services (LCS)
were now complete except for the care home LCS. A strategic aim was to invest in primary care in a targeted way. Another aim
was to facilitate frail elderly people to remain in the community and to avoid inappropriate admissions. There had been a debate around the role of primary care in care homes, whether people should be admitted to such facilities or supported in the community, including the virtual ward. No conclusion had been reached.
Over 3,000 residents were in care homes across both CCGs with both
residential and nursing needs, with more patients in residential care homes than in nursing homes. Some patients received Funded Nursing Care, and others received funding for continuing healthcare. The specification for the care home LCS was subject to a review process, which included the GMS requirements for GPs, and all aspects of care for individuals. It was noted that a number of GP practices had a Locally Enhanced Service in nursing homes, and that should be taken into account in decision making. Staff within residential homes should be supported and educated to avoid inappropriate admissions to secondary care.
4
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�224�of�237Page�39�of�52

It was proposed that funding be targeted at patients with nursing needs, and
remaining funding be used to support Integrated Care Teams. Members agreed that this was a pragmatic solution.
Andrew Holden agreed to distribute a paper which defined GMS+.
Action: AH
Members discussed the practicalities of primary care support to residential homes. There may be inefficiencies due to cross practice working, but practices could have collaborative arrangements. However some practices would lose income, while others would gain. The GP Alliance may be able to fill any gaps in residential home cover.
Members of both CCG Clinical Cabinets agreed to delegate Andrew Holden
and Keeley Ormsby to complete the care home LCS, and bring a report to a future meeting.
Action: AH/KO The Joint Clinical Cabinet agreed to delegate Andrew Holden and Keeley
Ormsby to develop the care home LCS. 7.2 Tier 2 Services – Review Paper Lyn Darby presented a paper to note progress made to date with the service
review for Community Tier Two services. The paper also made recommendations to the Joint Clinical Cabinet for contracting arrangements for 2014/15.
All Tier Two services were required to move to an NHS contract from 1 April
2014. There were 16 Community Tier Two services across both CCGs, and these had been grouped into three types to undergo a review process.
The commissioning team would work with the quality team to prepare a
programme of work for service and quality reviews during the year 2014/15. The Joint Clinical Cabinet agreed the recommendations for each
individual provider based upon the following: 1. Continuation onto an NHS contract for one year with an inbuilt quality
review timetabled for 2014/15 2. Continuation onto an NHS contract for one year with a full service and
quality review timetabled for 2014/15 3. Write a service specification for each service and continue to an NHS
contract with a clear plan for a full detailed service and quality review during 2014/15.
5
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�225�of�237Page�40�of�52

7.3 Evaluation of Rapid Assessment Units
Lyn Darby presented a report to detail the results of the recent review into the rapid assessment units (RAU) across Fareham & Gosport and South Eastern Hampshire CCGs. An audit of referrals to the RAUs had been undertaken where it was found that 39.5% of referrals were inappropriate and 60% were not considered to be urgent. Members discussed the outcomes and objectives of the RAUs, as well as the results of the audit of referrals. It was noted that appropriate use of the RAUs would prevent inappropriate admissions to secondary care. However, it was noted that this appeared to be an expensive way of controlling admission to secondary care, and it was queried whether there was a more cost effective way to do this. One suggestion was that community geriatricians should carry out visits to nursing homes. Sara Tiller wished to ensure that the views of patients and carers were taken into account by undertaking appropriate engagement. There may need to be a separate Task and Finish group linked to MOPRS and to Integrated Care Teams. The Joint Clinical Cabinet: • Noted the contents and findings of the paper • Acknowledged that a full detailed options appraisal should be
completed • Agreed the establishment of a Task and Finish Group to complete a
full options appraisal and conclude with the next steps to be submitted to a future meeting
7.4 Independent Sector Treatment Centre (ISTC) Procurement Lyn Darby presented a paper to brief the Joint Clinical Cabinet on the current
work stream for the ISTC and Havant Diagnostic Centre procurement. An ISTC Retender Group had been established in 2013, and had
recommended an extension to the contract to 30 June 2015. The group had included the Oak Park diagnostic centre in its evaluation.
The retender of both centres coincided with the redesign work being
undertaken around the front door of PHT. In addition, the Local Area Team had informed the CCGs that opportunities for the recommissioning of Diabetic Retinopathy service were being evaluated.
The Joint Clinical Cabinet noted the progress to date with the ISTC
procurement.
6
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�226�of�237Page�41�of�52

7.5 Community Ophthalmology Service Paul Howden reminded the meeting of the discussion over the Community
Ophthalmology Service that had taken place at the meeting held on 27 November 2013. The procurement process would end imminently for the new service scheduled to begin on 1 April 2014.
Lyn Darby informed the meeting that the service specification had been signed,
but Chair’s Action was needed to complete the process. Sara Tiller reported that members of Fareham & Gosport CCG Governing Body had recommended that the Chair’s Action be taken in conjunction with two lay members.
It was expected that the limited tender would improve the quality of the
Ophthalmology service, as reservations had been expressed over waiting times with the current provider. There was no need to carry out an engagement process as there would be no change to the service offered.
The Joint Clinical Cabinet agreed that a Chair’s Action be undertaken to
sign off the Community Ophthalmology ratification report following a limited tender.
8 Portfolio Updates 8.1 Proposal to develop online interactive diagnostic and management
pathways for COPD and Stroke Prevention in AF Ian Bell presented a paper to inform the Joint Clinical Cabinet of the proposal
and to consider approval of the development process. The CCGs were planning to address COPD during the next financial year by an LCS; the proposed online interactive pathways would support the process.
This would give a straightforward way of obtaining information and would be
accessible through the Primary Care Information Portal (PIP). Funding for the software had been secured from Pharma companies. The Medicines Management team would develop the tools for the pathways. Dr Andrew Whittamore, who leads on COPD and the Academic Health Science Network, would support the proposal.
Members of the Clinical Cabinet discussed the proposal. It was reported that
the Clinical Assembly did not believe that PIP was an appropriate location, and the package should be part of a commissioning system. One suggestion was that the package could be integrated with the DXS platform.
Members expressed support for the proposed online interactive diagnostic and
management pathways for COPD and Stroke prevention in AF. However, it was commented that the pathways would remove the skill and wisdom of GPs from the discussion.
7
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�227�of�237Page�42�of�52

The Joint Clinical Cabinet agreed to approve the development of online interactive diagnostic and management pathways for COPD and Stroke prevention in AF.
8.2 Medicines Management Paul Howden commented that Medicines Management was the biggest growth
area faced by the CCGs. It was agreed that the Joint Clinical Cabinet receive a quarterly update on Medicines Management.
9 Finance and Performance 9.1 Non Commissioned Activity (NCA) Payments – Review of Current
Arrangements David Bailey presented a paper to advise on arrangements for payments for
services not routinely commissioned where patients received treatment from mainly NHS providers outside of the Hampshire county area.
This had become an issue because of patient confidential data, as the CCGs
were unable to check invoices in order to validate them. The CSU was contracted to provide a financial service for verifying and processing the invoices. The total of the charges for the current year had reached £1m, with £0.5m processed so far.
This was a country-wide issue across NHS organisations, which was being
addressed. The Joint Clinical Cabinet agreed to:
• Note the work carried out by the CSU to check invoices received for local CCG patients treated at NHS Trusts and others outside the county in terms of validating patient data and pricing
• Noted the pressure on CSU finance and contracting teams as a result of devolvement of the NCA budget to five CCGs since 1 April 2013.
• Note the extent of the backlog in paying invoices promptly due to the resource required to ensure confidentiality of patient data, and the input of the CCG to improve the situation
• Recognise the work being done with the CSU and CCG finance teams to check levels of creditors, effects on cash flow and to improve accruals for accurate financial reporting of NCA spending
• Note the plans to bring CCG budget holders into the invoice approval process.
9.2 Finance Report David Bailey presented a report to inform the Joint Clinical Cabinet of the
finance position as at month 9, 2013/14 for both Fareham & Gosport and South Eastern Hampshire CCGs, and highlighted key headlines from the reports.
8
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�228�of�237Page�43�of�52

Both CCGs had a year to date surplus of around £500k, with a forecast surplus of around £600k.
One of the main issues was over-performance at PHT, which had reached £6m at the end of December 2013, and was expected to reach £8m by the end of the financial year.
Another main issue were QIPP schemes, which had delivered £7m savings, which was £4.5m less than required. There was therefore some concern over QIPP savings for the next financial year.
Most CCGs would expect 2% growth in funding for the next financial year. However, those CCGs that were considered to have been under-funded would receive more. It was expected that Fareham & Gosport CCG would receive 3.5% and South Eastern Hampshire CCG would receive 3.1%.
It was expected that the total transfer to the Better Care Fund would be almost £11m for the year 2015/16.
It was noted that both CCGs had moved closer to the Fair Shares formula, and anticipated that there would be a further move for the year 2015/16. QIPP schemes for the next financial year were expected to deliver savings of £10m.
The Joint Clinical Cabinet agreed to accept the contents of the Finance reports for both Fareham & Gosport and South Eastern Hampshire CCGs.
9.3 Performance Report Michael Drake presented a report to inform the Joint Clinical Cabinet of the
performance position of both CCGs, and highlighted some of the headlines from the report.
All three of the Referral to Treatment standards had been achieved in November 2013. However there were a number of fails within specialities. There were no referred patients waiting over 52 weeks for treatment. The targets for diagnostic waits had been achieved, with 99.5% of patients seen within the timescale.
Fareham & Gosport CCG had achieved five out of nine cancer targets and South Eastern Hampshire CCG had achieved eight out of nine cancer targets in November 2013.
South Eastern Hampshire CCG had achieved a target of 95.6% for four hour waits in the Emergency Department at PHT. There had been under-performance for Fareham & Gosport which was caused by poor performance at University Hospitals Southampton Foundation Trust. However, the situation had not been sustained during December 2013, and targets had not been met in December 2013.
9
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�229�of�237Page�44�of�52

There were a number of areas of under-performance relating to both CCGs. A number of contract query notices had been issued. It was anticipated that the target for diagnostic waits would not be achieved in December 2013.
QIPP projects continued to be a challenge, and a two year plan was being developed.
It was anticipated that there would be a negative effect on the Quality Premium for the current financial year.
Richard Samuel informed the meeting that a consultation had been held on performance in the Emergency Department, with a review of quality indicators. There were potential QIPP savings of 75% during the year 2014/15, but there was less clarity around figures for 2015/16.
The Joint Clinical Cabinet agreed to note the contents of the report.
10 Governance 10.1 Governance Development Sara Tiller presented a paper which proposed that a governance development
programme be undertaken ahead of the next submission of changes to the CCG’s constitution in June 2014.
The report had been written following discussion at a Governing Body Away Day held in December 2013. The meeting had discussed arrangements for meetings and governance processes, and a number of areas had been identified, and work was under way to make improvements.
Clinical Cabinet would involve more facilitated clinical discussion in future around key topic areas. This would maximise the value of clinical time.
The Corporate Governance Committee had been constituted which would oversee all aspects of corporate governance, thus releasing time in the Clinical Cabinet and Governing Bodies.
The Clinical Cabinets would follow the format of running individual and joint meetings.
The Joint Clinical Cabinet agreed to: • Note the progress made to date and the work that had yet to be
conducted • Support the proposals for future Clinical Cabinet meetings to be more
clinically focused around fewer items 11 Other Meetings 11.1 Minutes/Notes from other meetings The Joint Clinical Cabinet noted the minutes/notes of the following
meeting:
10
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�230�of�237Page�45�of�52

• Planning Executive Group – 10 December 2013 11.2 Members were reminded that the next Board to Board meeting with PHT would
be held on Wednesday 5 February from 6.00 – 8.00 pm in the Quad Centre at Queen Alexandra Hospital.
12 Any Other Business There was no other business. 13 Future Agenda Items
• Update on Specialist Musculoskeletal and Persistent Pain Self-Management Service – AB
• Quality Surveillance Hub – JB • Care Home Locally Commissioned Service – AH/KO
14 Date of Next Scheduled Meeting Wednesday 26 February 2014
1.00 – 4.00 pm Spindle meeting room, 1000 Lakeside, North Harbour, Western Road, Portsmouth, PO6 3EN
11
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�231�of�237Page�46�of�52
Community Engagement Committee Meeting
Wednesday 4 December 2013 Havant Borough Council Offices
MINUTES, confirmed by email
Present: Tracey Faraday-Drake Chair Jim Harrison Patient representative
Jo Hockley Practice Manager Representative, SEH CCG
Elizabeth Kerwood Governance and Committee Officer, SEH and F&G CCGs
David Lee Badgerswood/Forest PPG Debbie Purdy
Senior Commissioning Officer, SEH, F&G and Portsmouth CCGs
Jo Parkinson
Senior Development and Engagement Officer, SEH and F&G CCGs
Amanda Stewart Complaints Officer, SEH, F&G CCGs
Peter Tier Friends of Emsworth Community Health Sara Tiller
Chief Development Officer, SEH and F&G CCGs
Sandra Theckston Head of Region (East) Radian Nick Wilson Chairman, East Hants
Community Partnership Apologies: Keith Barnard Chair, Fareham and Gosport Community Engagement Committee Julia Barton Chief Quality Officer, SEH and F&G CCGs Mariya Hardy Adult Services Marge Harvey District Councillor, East Hants/ County Councillor Dr Andrew Holden GP lead for SEH CCG Tim Houghton Chief Executive, Community First HEH. Voluntary Sector representative
Claire Hughes Service Manager (Community), East Hampshire District and Havant Borough Councils
Louise Spencer Deputy Chief Quality Officer, SEH and F&G CCGs Brenda Woon Development and Engagement Officer, SEH and F&G CCGs In attendance:
Lao Cooper Strategic Lead for Emotional Wellbeing Review (Children and Young People)
Madeline Close Voluntary Sector and Diverse Communities Officer, Health Watch
Howard Lewis GMC Regional Liaison Adviser for the South East Coast region
Steve Manley Community Outreach and Engagement Officer, Health Watch
1
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�232�of�237Page�47�of�52

Item Minute Actions 1 Welcome and Introductions
Tracey Faraday-Drake welcomed everyone to the meeting.
2 Minutes of the last meeting No changes were made to the minutes that were approved by email.
3 Matters arising (not on the agenda) Commissioning Priorities for 2014-15 Tracey Faraday-Drake met with Alex Berry, Chief Commissioning Officer and Sara Tiller to start to build up a picture of the commissioning priorities that will develop the forums the CEC sets up. Sara Tiller will bring a list of the priority areas for next year that the CCG will need engagement with patients and the public. It was acknowledged that this is an important piece of work for the CEC to take forward. Mental Health Tracey Faraday-Drake had met with Alex Berry to discuss mental health commissioning and has another meeting next week to discuss the wider review and key performance indicators. Southern Health Focus Group Nick Wilson noted that the CCG’s approach was welcomed by Southern Health FT and Sue Harriman, CEO, is keen to have a dialogue with the CCG. There is a working party in December and Nick Wilson will report back following this meeting. Website Elizabeth Kerwood reported that the website is live and being constantly reviewed and evolving. More information on the CEC has been added and as soon as Elizabeth has received confirmation from all members, their details will be added onto the site. The list of contacts that each member has will also be added to the website. Communications Elizabeth Kerwood is working on the wording and this will be sent out with the minutes.
Sara Tiller to bring list of priorities to the next meeting. Nick Wilson to report back to the next meeting. Send out the communications with the minutes.
COMMISSIONING PRIORITIES
4 Commissioning Update Debra Purdy updated the committee on the key areas that the commissioning team is working on. There fall into 4 key area. The handout attached provides the details. There were questions on the links between social and health services, and how important it is to develop these links, including the voluntary sector. There were concerns that there are not enough staff to deal with the commissioning intentions of the CCG. Several committee members stressed the importance on involving the housing sector in commissioning decisions. Sara Tiller summed up, to say that as this is a massive programme of work the CCG is looking at the priority areas where the Committee can add the most value. This will be brought back to the next meeting.
Sara Tiller will report back to the next meeting with the
2
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�233�of�237Page�48�of�52

Item Minute Actions priority areas.
5 Autism update
Lao Cooper the Strategic Lead for Emotional Wellbeing Review (Children and Young People) for the five local CCGs and Hampshire County Council attended to update the committee.
The key areas of work are a need analysis for Hampshire and user engagement. To date they have received over 1,000 responses from professionals, the voluntary sector, families and children. The closing date is 20 December and a preliminary report is due on 2 January. This work will inform how the CCGs and HCC support mental health and ensure that the services meet the identified needs.
The review of Child and Adolescent Mental Health Services strategy is due at the end of January.
There is a review of the current pathways for autism as referrals and MDTs vary across the county as there are different providers. They are drafting a pathway with a GP lead which will provide a consistent service across the county. When the pathway is available it will come to the Governing Body meeting.
Committee members commented on the poor provision of services for adults with autism who are often treated as if they have dementia and the issues of transition from child (up to 18) and adult care of autism patients.
The adult autism strategy is available on the HCC website http://documents.hants.gov.uk/adultservices/publications/AutismStrategy86468fullguide.pdf
QUALITY/ EQUALITY AND DIVERSITY
6. Quality report Amanda Stewart gave an overview of the key concerns with providers. Portsmouth Hospital Trust -Ophthalmology backlog - a large number of patients are overdue a follow up appointment in ophthalmology. An action plan is in place to clear the backlog and priority is given to patients based on their clinical need. -Cancer Waits – there are a number of patients breaching the national waiting times target. The hospital has been asked for assurance that the cancer wait times are based on real time data. The CCG is monitoring this closely. -Friends and Family Test - the Hospital scores are worse than the national average for the Friends and family score for inpatients, but the scores are better for A&E. The CCG is working with the hospital to look at the reasons behind this so that the scores can be understood better. SCAS -Long waits/response times/ vehicles off road - the report covers a very wide area, so not all of it is relevant locally but provides an overview of the whole service. There have been long waits reported and the CCG is working with SCAS to identify any problem areas. High numbers, of vehicles are off the road (25%). The fleet is being replenished with new vehicles due in November and new cars in the new year. Royal Surrey County Hospital
3
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�234�of�237Page�49�of�52

Item Minute Actions The CCG is working with the lead commissioner for the hospital. The low scoring CQC inspection is being challenged. The 3 never events this year are being investigated. Children and Adolescent Mental Health Services There are capacity issues and staff vacancies. The CCG is working to identify quality markers to be used in next year’s contract.. Southern Health FT The use of restraint has been reviewed by the Trust and the report is due at the end of December. The Trust is working with HCC and the Constabulary on the use and provision of Section 136 suites. University Hospital Southampton There has been a norovirus outbreak. The committee agreed that its place was to provide assurance to the stakeholders represented, that issues are being dealt with. The committee is also placed to raise issues based on information and customer experience. It was noted that this year the CCG has levied fines on providers that have not met their KPIs.
7 Equality and diversity
All public sector organisations have a Public Sector Equality duty. The CCG has to assess itself against key criteria and publish the results of this by the end of January 2014. The CCG would like a group to look at the self-assessment and comment on this to ensure that the CCG is delivering for different communities appropriately. Jim Harrison, (who has done a lot of work in Equality and Diversity for different organisations) and Nick Wilson volunteered to be on the group. Claire Hughes was nominated and Sue Williams, who is the chair of the disability forum for East Hants District Council were suggested.
Contact Claire Hughes and Sue Williams and ask if they will be on the equality and diversity group.
COMMUNICATION
8. NHS Call to Action Sara Tiller spoke to presentation (attached). Members of the committee are encouraged to provide feedback to the CCG and ask others to look at the information on the CCG’s website and feedback. Jo Hockley noted that practices are not aware of this and information will be put onto the weekly email to the practices.
Put information on the Call to Action on Top Tips
9. Healthwatch Madeline Close and Steve Manley attended the meeting to give a presentation (attached). Locally there is a team of 6 people. Healthwatch has a statutory requirement to represent all of the communities they serve locally. Sara Tiller noted that the CCG is keen to work with Healthwatch and it was agreed that it was important to share and not to repeat work. Healthwatch will be doing more focused research projects next year. It was noted that Jim Harrison has been confirmed as the Healthwatch Champion in this area and he will remain the conduit, along with Sara Tiller and Dr Rushton, who both sit on the Health and Wellbeing Board along with Healthwatch.
10 GMC Update Howard Lewis, GMC Regional Liaison Adviser for the South East Coast
4
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�235�of�237Page�50�of�52

Item Minute Actions region gave a presentation to the committee (attached).
11 Locality Patient Group UpdateThe first meetings for the two groups, north and south of Butser will take place in January 2014.
12 Chase Community Hospital Update Progress continues to go well on the project. The four beds at Wenham Holt have received positive feedback from the local GPs and 8 patients have used the facility to date. Work continues on the business plan. The NHS Property services have to complete a transfer agreement which may delay the process and no-one is currently sure of the time scale and it will delay the start of the works on site. The services will continue as normal until the work can start.
13 Date of next meeting 5 February 2014 9.30 – 11.30, Ante Room, East Hants District Council, Penns Place, Petersfield.
5
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�236�of�237Page�51�of�52

About our Community Engagement Committee One of the most important things we need to do as a Clinical Commissioning Group (CCG) is to ensure that we understand what people think about their local NHS services. Your views really do help us to plan and deliver more responsive and effective health services that are designed to meet the needs of local patients and remain affordable to run. And, as a patient, we want you to be at the heart of decisions that are made about the care and support you receive, when you need it. There are all sorts of ways we can collect feedback about local services and it is important that we ensure that this reaches all parts of the organisation. It is equally important that we have effective means in place to communicate with our main partners and those we work with closely. To that end we have established a Community Engagement Committee, which links directly to our CCG Governing Body to ensure that we can conduct two-way communication and engagement through existing, trusted groups. The ‘two-way’ element is important because we want the agenda to be driven just as much by those participating in the group as by the CCG itself. We ask everyone who attends the meeting to take back the key messages from it into their own organisations and working groups. We are especially keen to ensure that those groups who are traditionally seldom heard are played into this way of working, too. Above all we want to ensure that this meeting provides us with the opportunity where we can look at how we ensure continuous and meaningful engagement with the public, patients and carers so that your feedback really does influence the shaping of local NHS services. It is our intention to provide you with a regular update from the meeting so that you can be aware of the types of issues and topics that are being discussed. We will also provide you with opportunities to add your own comments to the discussions too. Recently we have been discussing:
• NHS Call to Action and how we are seeking the views of local residents to help us develop our five year strategy
• The progress in meeting our requirements under the Public Sector Equality Duty • The progress in the redevelopment of Chase Community Hospital in Bordon • The development of Locality Patient Groups which will consist of representatives from
the Patient Participation Groups at GP Practices. To find out how to get involved with the CCG visit our website at www.southeasternhampshire.nhs.uk. December 2013
6
18�Minutes�Notes�of�Other�Meet
Top
Overall�Page�237�of�237Page�52�of�52


















