Agenda - Hauora Tairāwhiti · Rehette Stoltz Gisborne District Council: Deputy Mayor Sport...
82
Agenda HAUORA TAIRĀWHITI BOARD Tuesday, 18 December 2018, Boardroom, Corporate Offices, Hauora Tairāwhiti 9.00am Karakia 9.05am Presentation: 20 Good Things (Hauora Tairāwhiti Chief Executive) 12.30pm Staff 20/40 Long Service celebration lunch with Board Page APOLOGIES 1.1. As advised INTERESTS 2.1 Committee Members’ schedule of interests for review 3 2.2 Conflicts in relation to Agenda items verbal PREVIOUS MEETING 3.1 Previous Minutes for approval: 27/11/2018 6 3.2 Matters Arising n/a ACTION ITEMS 4.1 Actions from previous meeting 10 CORRESPONDENCE 5.0 Nil n/a PATIENT QUALITY & SAFETY 6.0 Nil n/a REPORTS 7.1 Performance Dashboard 11 7.2 Chair’s Report 13 7.3 Te Waiora o Nukutaimemeha Chair’s – no report n/a 7.4 Chief Executive’s Report 14 7.5 Finance Report 26 • Organisational Performance Graphs 32 7.6 Board Sub-Committee Reports 33 INFORMATION ITEMS 8.1 Health Workforce DHB Benchmarking Report – Human Resources to 30 September 2018 34 DECISION ITEMS 9.1 Submission on the Health (Drinking Water) Amendment Bill 80 GENERAL BUSINESS 10.0 Nil n/a Hauora Tairāwhiti
Transcript of Agenda - Hauora Tairāwhiti · Rehette Stoltz Gisborne District Council: Deputy Mayor Sport...

Agenda
HAUORA TAIRĀWHITI BOARD
Tuesday, 18 December 2018, Boardroom, Corporate Offices, Hauora Tairāwhiti
9.00am Karakia
9.05am Presentation: 20 Good Things (Hauora Tairāwhiti Chief Executive)
12.30pm Staff 20/40 Long Service celebration lunch with Board
Page
APOLOGIES
1.1. As advised
INTERESTS 2.1 Committee Members’ schedule of interests for review 3 2.2 Conflicts in relation to Agenda items verbal
PREVIOUS MEETING 3.1 Previous Minutes for approval: 27/11/2018 6 3.2 Matters Arising n/a
ACTION ITEMS 4.1 Actions from previous meeting 10
CORRESPONDENCE 5.0 Nil n/a
PATIENT QUALITY & SAFETY 6.0 Nil n/a
REPORTS 7.1 Performance Dashboard 11 7.2 Chair’s Report 13 7.3 Te Waiora o Nukutaimemeha Chair’s – no report n/a 7.4 Chief Executive’s Report 14 7.5 Finance Report 26 • Organisational Performance Graphs 32 7.6 Board Sub-Committee Reports 33
INFORMATION ITEMS 8.1 Health Workforce DHB Benchmarking Report – Human Resources to 30 September 2018 34
DECISION ITEMS 9.1 Submission on the Health (Drinking Water) Amendment Bill 80
GENERAL BUSINESS 10.0 Nil n/a
Hauora Tairāwhiti

RESOLUTION TO EXCLUDE THE PUBLIC RESOLVED that: In accordance with the provisions of Schedule 3, of the NZ Public Health and Disability Act 2000, that the public be excluded from the next part of the proceedings of this meeting. The reason for passing this resolution and the grounds on which the resolution is based, together with the particular interest or interests protected by the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the proceedings of the meeting in public areas are as follows:
11.1-2 12.1
As shown on resolution to exclude the public in Minutes.
13.1
Negotiations or Commercial Activities – The disclosure of that information would not be in the public interest because of the greater need to enable Hauora Tairāwhiti to carry on, without prejudice or disadvantage, negotiations or activities. [OIA 1982 S.9 (2) (j) & (i)]
Ground(s) under Clause 32 for passing this resolution: That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9(2) (g) (i)) of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S.32(a)]
PREVIOUS IN COMMITTEE MEETING 11.1 Previous Minutes for approval: 27/11/2018 85 11.2 Action Items (nil) 87
IN COMMITTEE REPORTS FROM HAUORA TAIRĀWHITI ADVISORY COMMITTEES 12.1 For noting and/or adoption 88
INFORMATION ITEMS 13.1 Nil n/a
DECISION ITEMS 14.0 New Pharmacy Providers 89
STAFFING & GOVERNANCE 15.0 Nil
DATE OF NEXT MEETING: Tuesday, 26 February 2019
Hauora Tairāwhiti

Member Interest Declared RoleDavid Scott Three Rivers Medical Centre Wife an employee
Treescape Farm Partnership Partner in BusinessTreescape Consultancy Business ConsultantTe Kuri a Tuatae Marae TrusteeEast Coast Rural Support Trust Rural Support Co-ordinatorGisborne District Council Civil Defence Shift Volunteer/Media Liaison OfficerGisborne Herald Casual non-paid columnistMiddle Mount Company Ltd DirectorCONNEXT Charitable Trust Trustee
Geoff Milner Ngati Hine Health Trust Chief ExecutiveTerenga Paraoa Lmited DirectorManaia PHO Limited DirectorTairāwhiti Laundry Services Limited DirectorTairāwhiti Laundry Services Limited Director
Gavin Murphy Tlab Limited DirectorEastland Community Trust Chief ExecutiveTe Ahi o Maui Limited Partnership DirectorPersonal friend of the Minister of HealthActivate Tairāwhiti Limited DirectorEastland Development Fund Limited DirectorWET Gisborne Limited Director
Prudence Younger Forest Industry Contractors Assoc Chief ExecutivePublic Impressions Limited Director
Kathy Sheldrake Motu Trails Charitable Trust ChairRehette Stoltz Gisborne District Council Deputy Mayor
Sport Gisborne Tairāwhiti TrusteeTairāwhiti Positive Aging Trust TrusteeE Tu Elgin Community Group MemberHusband employed by Hauora Tairāwhiti Deon Stoltz (Senior Medical Officer)Deon Stoltz Medical Services DirectorArt in Public Places TrusteeManaaki Tairāwhiti Governance Group memberSunshine Service Managment Team memberGisborne Walking & Cycling Trust TrusteeTairawhiti Laundry Services Limited DirectorTe Ha 1769 Sestercentennial Trust. Trustee
Hiki Pihema Hauora Tairāwhiti Team Leader, DietitiansDietitians Board Board Member Otago University Supervisor, Dietetics ProgrammeNgati Porou Hauora Dietitian via Hauora Tairāwhiti roleDietitians NZ MemberTe Runanganui o Ngati Porou Registered BeneficiaryTe Whaihanga ki Uawa MemberElgin Rangatahi Oral Health Project Daughter is Co-OrdinatingNational Heart Foundation Daughter is Nutrition Advisor
Na Raihania Whanau Trusts TrusteeHawkes’ Bay DHB Iwi Relationship Board MemberTRONPnui Board Trustee
Brian Wilson B & P Wilson Family Trust TrusteeGisborne District Council CouncillorYMCA PresidentGisborne Surf Lifesaving Charitable Trust TrusteeTLab Director
Board Members’ Register of Interests3

Josh Wharehinga Gisborne District Council CouncillorTe Wananga o Aotearoa Board memberGisborne Intermediate School Board memberMother employed by Hauora Tairāwhiti Maraea Cookson (Cultural Response Team)Ex Partner employed by Hauora Tairāwhiti Richelle Tarsau (Children’s Ward)Aotearoa Scholarships Trust TrusteeHorouta Waka Hoe Waka Ama Club Board member
Meredith Akuhata-Brown Gisborne District Council CouncillorCampion College Board memberTairawhiti Youth Workers Collective MemberPapawhariki Inc Board memberGisborne Herald Casual unpaid columnist
Jim Green (Chief Executive) Health Partnerships Limited (CE Sponsor – Food Services Programme)
Appointed by National CEs. First responsibility is to Hauora Tairāwhiti but there may be an occasion when this conflicts with the national programme.
Chief Executive Representative, Midland Alliance Leadership Team (Midland Health Network Trust)
Potential conflict exists in relation to decisions made by the Midland ALT which conflict with the interests of Hauora Tairāwhiti.
Interim Chair/Director, HealthShare Limited First responsibility is to Hauora Tairāwhiti but there may be an occasion where this conflicts with the needs of HSL.
Wife employed by Tūranga Health as Tamariki Ora Nurse and Team Coordinator for Tamariki Ora
Potential conflict exists over decisions related to funding of services provided by Tūranga Health affecting the employment status of his wife.
Son is employed as a Medical Registrar at Waikato DHB.
Potential conflict regarding decisions on terms and conditions of employment for Medical Registrars.
Daughter in-law is currently working in a community Pharmacy in the Waikato.
Potential conflict regarding my involvement with the national Community Pharmacy Agreement which could impact on her employment.
Manaaki Tairāwhiti Decisions at Manaaki Tairāwhiti may conflict with those in my role as CE of Hauora Tairāwhiti. The management is that decisions around funding are required to come back to Hauora Tairāwhiti.
National Oracle Solution Executive Steering Committee as CE representative
A possible conflict of interest arises for me in this role as opposed to my role as CE of Hauora Tairāwhiti. Management of the possible conflict can be effected by the fact that I have a responsibility to Hauora Tairāwhiti and the Midland Region ahead of the commitment to the NOS programme.
Member, National BiPartite Action Group Appointed by National CEs. First responsibility is to Hauora Tairāwhiti but there may be an occasion when this conflicts with the group programme.
Pay Equity Workstream Co-Lead, Employment Relations Strategy Group (ERSG),
Appointed by National CEs. First responsibility is to Hauora Tairāwhiti but there may be an occasion when this conflicts with the work programme.
National CE Lead, Holidays Act Appointed by National CEs. First responsibility is to Hauora Tairāwhiti but there may be an occasion when this conflicts with the work programme.
Midland Regional DHBs CE Lead, Child Health Action Group
Appointed by Midland DHBs. First responsibility is to Hauora Tairāwhiti but there may be an occasion when this conflicts with the work programme of Midland.
Management Attendees
4

Midland Regional DHBs CE Lead, Māori Health Appointed by Midland DHBs. First responsibility is to Hauora Tairāwhiti but there may be an occasion when this conflicts with the work programme of Midland.
(Vacant) Chief Medical Officer
0 0
Serita Karauria (Acting DoN) Nil 0
Craig Green (Chief Financial Officer)
Chamber of Commerce (Mentor) Possible conflict if mentored party is providing services to Hauora Tairāwhiti.
Mother employee of Compass Medirest Food Services
A conflict of interest exists in relation to negotiations with Compass Medirest Food services Tairāwhiti conflict where it affects or could affect staffing.
Partners daughter is employed by Hauora Tairāwhiti in the role of Purchasing Officer (3 month fixed term contract from 21 November 2018).
A conflict of interest exists in relation to employment matters given Logistics is a service managed by the CFO.
Nicola Ehau (Planning, Funding & Population Health)
Husband an employee of the Health Quality & Safety Commission
Low likelihood of conflict.
Manaaki Tairāwhiti Decisions at Manaaki Tairāwhiti may interest with those in my role as GM Planning & Funding in Hauora Tairāwhiti. The management is that decisions around funding require to come back to Hauora Tairāwhiti.
Fraser Hopkins (Communications)
Wife is employed by Hauora Tairāwhiti as Team Leader Community Services Admin.
Possible conflict depending on decisions made at leadership and committee level regarding community services administration.
Lynsey Bartlett (Surgical Services)
Company Director: Yesteryear Limos Low likelihood of conflicts.
Alternate Director, HealthShare Limited Appointed by Hauora Tairāwhiti. First responsibility is to Hauora Tairāwhiti but there may be an occasion where this conflicts with the needs of HSL.
5

Minutes
Hauora Tairāwhiti Board 27 November 2018, commencing 9.00am
Present David Scott (Board Chair) Meredith Akuhata-Brown Kathy Sheldrake Josh Wharehinga Brian Wilson Na Raihania Hiki Pihema Rehette Stoltz Geoff Milner (via videoconference) Gavin Murphy Prue Younger
Attending
Jim Green (Chief Executive) Dr Anne Kolbe (Acting Chief Medical Officer) Fraser Hopkins (Communications Manager) Nicola Ehau (Group Manager Planning, Funding and Population Health) Craig Green (Chief Financial Officer) Joyce O’Donnell (Minutes)
Public Wynsley Wrigley (Gisborne Herald)
Presentation WAKA award to Hauora Tairāwhiti grounds-keepers Patient Story – Mr & Mrs John Woods (Stroke/Addiction Services) Introduction: Dr Anne Kolbe (acting CMO)
Item 1 Apologies Rehette Stoltz, Brian Wilson and Prue Younger for an early departure.
Item 2 Interests 5.1 Changes to Register Dr Kolbe verbally advised the Board of her interests 5.2 Conflicts Related to Any Item on the Agenda Hiki Pihema - Item 7.4: Chief Executives Report/Eating Disorders
Hiki Pihema – Item 15: Staffing & Governance Report
Item 3 Minutes of Previous Meeting ADOPTED
The public minutes of the Tairāwhiti District Health Board meeting held on 30 October 2018 confirmed as a true and accurate record.
Matters Arising from Minutes The Group Manager Planning, Funding & Population Health responded to questions
6

regarding Hauora Tairāwhiti’s response to the korero from Hinerupe Marae rangatahi.
Item 4 Action Items Noted
Item 5 Correspondence Nil
Item 6 Patient Safety & Quality Nil
Item 7 Reports 7.1 Performance Dashboard Noted 7.2 Chair’s Report Noted 7.3 TWON Report Noted, in particular the report on the South Central Foundation (Nuka) Conference. The meeting was interrupted by a presentation from NZNO member representatives
from Ngāti Porou PHO and union organisers regarding nursing pay rates on the Coast. 7.4 Chief Executive’s Report In relation to the earlier declaration of an interest in this report related to Eating
Disorder and her role as Hauora Tairāwhiti Dietitian, the Board agreed Hiki Pihema could remain and discuss the issue. The Chief Executive expanded on his report throughout. The Group Manager Planning Funding & Population Health advised service provision for Eating Disorders was provided regionally and noted the feedback from Ms Pihema that patient care was focussed on providing dietary information and not mental health support. The Group Manager also responded to questions regarding NASC staffing and workload. Members noted the attached report on the Tairāwhiti Inter-professional Education (IPE) programme. The Chief Executive provided some feedback in relation to the representations of both Mr Wood and the Ngāti Porou Hauora Nurses claims.
7.5 Finance Report Noted and the Chief Financial Officer expanded throughout, commenting in particular
on the cash position; and that Hauora Tairāwhiti have activated the reduced programme for 2018/19 CAPEX.
7

7.6 Board Sub-Committee reports Noted
Item 8 Information Items Nil
Item 9 Decision Items 9.1 Speaking Up for Safety and the Promoting Professional Accountability
Programme (Cognitive Institute) The Chief Executive and Acting Chief Medical Officer elaborated on the programme and advised that success rested on the Board’s engagement and commitment as well. The Board noted that the Cognitive Institute’s programmes underpin Hauora Tairāwhiti’s WAKA values and behaviours policies which include cultural safety. ADOPTED: The recommendation that the Board gives their commitment to attend the PPA briefing with Dr O’Brien (Cognitive Institute) on 19 February 2019 (commencing as an adjunct to the HAC meeting).
Rehette Stoltz left the meeting 9.2 Hauora Tairāwhiti (draft) Plastic Free Strategy The Chief Executive commented that DHBs are all taking a common direction in terms
of reducing plastic waste and the Minister’s Letter of Expectations includes references to reducing the carbon footprint of the DHB. The Board noted that the aim is to implement as much as can be done locally and work collaboratively with regional/national purchasing partners over the longer term. ADOPTED: That the Board adopt the following recommendations: 1. That the draft Strategy attached is approved, “subject to the inclusion that Hauora
Tairāwhiti will continually monitor the reduction of plastic waste” in the Goals. 2. That subsequent to the Board adoption of the Strategy, management implement
measures and activities to see it successfully implemented, including formal reporting of appropriate measures and progress to the Board.
Item 10 General Business The Lease Agreement between Hauora Tairāwhiti and Hospice Tairāwhiti was signed.
RESOLUTION TO EXCLUDE THE PUBLIC RESOLVED that: In accordance with the provisions of Schedule 3, of the NZ Public Health and Disability Act 2000, that the public be excluded from the next part of the proceedings of this meeting. The reason for passing this resolution and the grounds on which the resolution is based, together with the particular interest or interests protected by the Official Information Act 1982 which would be prejudiced by the holding of the whole or the relevant part of the proceedings of the meeting in public
8

areas are as follows:
11-12 As shown on resolution to exclude the public in Minutes.
13.1-3 Negotiations or Commercial Activities – The disclosure of that information would not be in the public interest because of the greater need to enable Hauora Tairāwhiti to carry on, without prejudice or disadvantage, negotiations or activities. [OIA 1982 S.9 (2) (j) & (i)]
Ground(s) under Clause 32 for passing this resolution: That the public conduct of the whole or the relevant part of the proceedings of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist, under section 6, 7 or 9 (except section 9(2) (g) (i)) of the Official Information Act 1982. [NZPH&D Act 2000 Schedule 3, S.32(a)] 11.1 Previous Minutes for approval 30/10/18 11.2 Action Items 12.1 Sub Committee Reports 13.1 Mental Health Issues update 13.2 Manaaki Tairāwhiti 13.3 Request for Deficit Support (letter) 15.1 Staffing & Governance Committee Report
PUBLIC RELEASE OF INCOMMITTEE ITEMS 16.0 No In Committee decision items were released.
The Chief Executive, Chief Financial Officer, acting Chief Medical Officer, Communications Manager and the Minute Secretary were invited to remain for facilitation of Board discussion and recording.
Meeting closed: 12.15pm Date of Next Meeting: 18 December 2018
………………………………………….. ………………………………………. Chair Date
9

Action Items HAUORA TAIRĀWHITI BOARD
Item Description Who Deadline
Carried over Ambulatory Sensitive Hospitalisation (ASH) 45-64 Rate Increase
An update to the ASH 45-64 report in a year to gauge progress. • Carried over as scheduled
Nicola July 2019
Finance Report Consolidated Financial Performance Summary table – confirm what the year to date budget was last year. • Completed
CFO Oct
27 November 2018
Nil
10

Nov-18 Nov-18
Ethnicity This Month Target Last Month 3 Month Average
Māori 96.2% 95.8% 96.1%
Total Pop 95.7% 95.1% 95.6%
Total Pop 86% ≥ 90% 100% 95%
Māori 79% 84% 82%
Total Pop 82% 86% 84%
Māori 80% 80% 80%
Total Pop 83% 83% 83%
Māori 95% 95% 96%
Total Pop 95% 95% 96%
Ethnicity This Month* Target Last Month 6 Month Average
Māori 96% 95% 90%
Total Pop 94% 94% 93%
Ethnicity Total This Month Monthly Target YTD Year to Date
Target
Māori 80 84 385 410
Total Pop 210 220 1,079 1,079
Ethnicity This Month Target Last Month 3 Month Average
8 ≤ 6 9 8
1 1 2
10 14 12
6 1 4
Māori 94% 92% 93%
Total Pop 94% 91% 93%
This Month Target Last Month 3 Month Average
80% ≥ 80% 82% 82%
1,037 ≤ 836 1,023 1030
2.30 ≤ 3.21 days 2.60 2.47
1,635 ≤ 1,523 1,720 1,651
66% ≤ 70% 69% 67%
*Target number of discharges and number of ED attendances is based on 5% reduction from 2015/16 year and displayed as 1/12 of that amount
This Month Target Last Month 3 Month Average
108 97 99
358 356 348
This Month Target 3 Month Average YTD Average
% 5.0% ≤ 6.1% 4.1% 4.3%
# 45 N/A 40.7 38.1
% 4.5% ≤ 7.8% 4.1% 6.3%
# 6 N/A 6.0 9.4
# of Enrolled Patients# of Māori
Enrolled
PHO % of enrolled
population
9,109 8,125 19%
38,960 16,630 89%
102% 108%
Ethnicity 12 months to 30 June 2018 Target Last Year (June 17)
Māori 7,205 8,135
Total Pop 6,479 7,631Māori 6,271 5,922Total Pop 3,992 4,197
Key
≤ Less Than or equal to ≥ Greater than or equal to
≥ 95%
12 Month Trend
≥ 95%
N/A
12 Month Trend
43%
PHO Enrolments (Oct-Dec 2018)
Patient Falls
Severity Assessment Code 1 and 2 Events
Complaints
Number of Medication Events
Hauora Tairāwhiti
Health Targets
Indicator
Shorter Stays in Emergency Departments
Shorter waits for Cancer Treatment - 62 day
target
Increased Immunisation
(8 Months) ≥ 95%
12 Month Trend
≥ 90%
≥ 95%
≤ 6,512
Percentage of Triage 4-5 attendances
Primary Care
Better help for Smokers to Quit - Secondary
Care
Better help for
Smokers to Quit**Maternity *Currently only Hospital Maternity Dept
Stats
≥ 90%
Raising Healthy Kids*
Improved Access to Elective Surgery
Indicator
Patient Safety and Quality - Hospital
12 Month Trend
81%
12 Month Trend
PHO
Hospital Events
Percentage of PHO Population who are Māori
Ambulatory Sensitive Hospitalisations per 100,000 population 2018 Year
Age Group
00-04
Number of Emergency Department Attendances*
12 Month Trend
Surgical Events
* only available on 8th of the Month following service.
45-64
Acute Readmission Rate
Indicator
Indicator
Bed Utilisation
Number of discharges*
Average Length Stay (days)
≤ 3,490
Indicator
Number of Acute Surgeries
Total Number of Surgeries
12 Month Trend
Acute Readmission
Rate
Total Population
75+ population
N/A
Ngāti Porou Hauora
Midlands Health Network - Tairāwhiti
Percentage of Tairāwhiti Population enrolled in a PHO Percentage of Tairāwhiti Māori Population enrolled in a PHO
7,253 6,330 6,053
7,320 6,738 6,479
4,031 4,197
2,163
4,280 4,164 3,992
0
2,000
4,000
6,000
8,000
12 to 03/17 12 m to 06/17 12 m to 09/17 12 m to 12/17 12 m to 03/18 12 m to 06/18
Ambulatory sensitive hospitalisations per 100,000 population
0-4 year olds -Total Pop 45-64 year olds - Total Pop
11

Nov-18 Nov-18
Indicator Ethnicity This Month Target Last Month 3 Month Average
Māori 86% 87% 86%
Total Pop 84% 85% 84%
Māori 291 260 276
Total Pop 643 564 596
Māori 18% 17% 19%
Total Pop 12% 12% 12%
2013/14 2014/15 2015/16 2016/17 2017/18 2018/19
5 6 2 1 4 0
12 months to June
2018Target
12 months to March
2018
Last year
12 m to June 2017
82% 71% 78%
70% 56% 69%
*Waiting times are sourced through National reporting (PP8), which reflect activity in the previously reported quarter.
Oct-18 Target Sep-18 3 Month Average
Computed Tomography (CT) < 42 days 94% ≥ 95% 94% 94%
Magnetic Resonance Imaging (MRI) < 42 days 93% ≥ 90% 93% 93%
Urgent Colonoscopy < 14 days 100% ≥ 90% 100% 100%
Non Urgent Colonoscopy < 42 days 69% ≥ 70% 56% 63%
Surveillance Colonoscopy < 84 days 67% ≥ 70% 68% 70%
This Month Target Last Month 3 Month Average
5% ≤ 10% 10% 6%
0 ≤ 7.6 2 1* Data won't be available till 12/11/2018.
Month Actual Month Budget Last Month Actual YTD Actual YTD Budget YTD Variance
$16,081 $16,169 $16,514 $82,172 $80,863 $1,309
$17,184 $16,997 $17,068 $85,706 $84,586 $1,120
($1,103) ($828) ($554) ($3,534) ($3,723) $189
($1,179) ($828) ($771) ($3,966) ($3,721) ($245)
$84 $0 $248 $441 $0 $441
($8) $0 ($31) ($9) ($2) ($7)
Diagnostic Waiting Times * 1 month behind due to data being collated Nationally
12 Month Trend
Consolidated Result
Provider Result
Funder Result
≤10%
Governance Result
Trend
Missed Appointments
Staff Injury (per 1m hours worked)
Finance ($'000)
Consolidated Revenue
Consolidated Expenditure
Immunisation at 2 years
First Specialist Assessments
Hauora Tairāwhiti
≥ 95%
N/A
Patient Safety and Quality - Community
12 Month Trend
Staff Turnover
12 Month Trend
Indicator
Trend
Rheumatic Fever Hospitalisations (Financial Year, First episode hospitalisation numbers)
Non-urgent Mental Health & Addiction waiting times for Child and Youth 0-19 (data reported Quarterly*)
Indicator
Mental Health waiting times (< 3 weeks)
Addiction Services Waiting times (< 3 weeks)≥ 80% < 3 Weeks
Indicator
Human Resources
Indicator
$12 $160
$109
$357 $441
$34 $31
$26
$1
-$7
$275 $376
$7
$106
-$245
-$466
-$1,175
-$2,016
-$2,787
-$3,966
$321
$567
$142 $464
$189
($4,400)
($4,000)
($3,600)
($3,200)
($2,800)
($2,400)
($2,000)
($1,600)
($1,200)
($800)
($400)
$0
$400
$800
Jul-
18
Au
g-1
8
Sep
-18
Oct
-18
No
v-1
8
Dec
-18
Jan
-19
Feb
-19
Mar
-19
Ap
r-1
9
May
-19
Jun
-19
Re
sult
($
00
0's
)
Hauora Tairāwhiti Financial Performance 2018 /19
Funder variance Governance varianceProvider variance Provider ActualConsolidated Variance
Funder and Governance Budgets are set to zero. Provider Budget is set to a deficit of $2.023m The new Provider Variance reflects the difference between Actual and Budgetted results while Provider Actual reflects net actual result.
12

Chair’s Report – December 2018
- The Annual Midland Board Development two-day seminar was held recently in Tauranga. The
two-day workshop was notable for the strong mandate from Māori regional Iwi Board members for increased participation in the Midland Chairs / CEOs monthly meetings. There was a concerted call from the floor for greater equality, power sharing, and a share of the regional resources. It was quite apparent that there were huge differences in the way each Health Board in the Midland region participated with their respective Iwi governance sub-committees / groups. There was a consensus by the seminar participants that more could be done and that strategies needed to be developed to allow this to happen.
- We have reached the end of yet another busy year for Hauora Tairāwhiti including two visits from the new Minister of Health the Hon Dr David Clark. The first an exploratory visit where he spent time with the Chief Executive and myself finding out about Hauora Tairāwhiti and the aspects that frustrate us the most. Hon David then returned later in the year to officially open the new Medical Day Centre.
- One of the most satisfying aspects of the year has been the attitudes of the new Minister and his
appointee to Director General of Health, Dr Ashley Bloomfield. The attitudes and philosophy of this duo has seen huge changes in the way the MoH interacts and responds to District Health Boards. The new budget setting half day meetings in Wellington with the Chair, Chief Executive and team has resulted in the first ‘realistic budget’ in my time as Chair. I am sure over time we will see more innovations from Dr David & Dr Ashley.
- Thanks to the Board and Sub-Committee members for positive interactions and participation
during the year. I wish Board and Committee members and the CE and his huge team of employees a restful and peaceful festive season as you all celebrate with family and friends.
Recommendation That the Board notes the report. David Scott, MNZM, JP Chair Hauora Tairāwhiti
13

Chief Executive’s Board Report November 2018
Merry Christmas and Happy New Year Everyone I always take a look at my last year message before embarking on the current and I am glad I did look back on what I said. The theme was the challenges we face in health in Aotearoa, and the effort that goes in from so many people working within the sector to make sure people get good care, and their health is maintained. I said the challenges were increasing and it is not satisfying to reflect back on 2018 and have confirmed how right I was. The year has been turbulent not just with regard to the clinical and service pressures, or the financial situation the sector, and Hauora Tairāwhiti along with it, is in. We have also had industrial unrest and now a sobering report into Mental Health in our country, one that puts down the facts as we ourselves know them to be as part of living and working here in Tairāwhiti. I am however satisfied in the responses we are making to these challenges and it is important to see and make seen the real improvements that all the hard work put in by people from governance level to all parts of our organisation and wider in the sector is making. We are seeing significant improvements in equity for Māori. We are seeing expanded services for people in our community, with much more of that occurring here closer to home. We were able to be part of a better winter for Tairāwhiti people and have learned more about how that can be even better in Winter 2019, as well as every day. We are further improving the quality of care and taking on new ways of working to keep up the momentum. Our work is also linked strongly to the wider emphasis on the wellbeing of our total community. We are a key player in doing our bit to improve the lives of Tairāwhiti people directly through the services we fund and provide. More than this, we have a role which we exercise to support and hold true to the kaupapa, the work of our government agency, Council and iwi partners. This time of the year is devoted to two things in respect of all this. The first to say thank you for all who have taken part and advanced our cause of hauora for Tairāwhiti. You know the difference you make and it is deeply appreciated by those receiving the direct benefit and the whole community. The second is to ensure that everyone has a Merry Christmas and is looking forward to a Happy New Year. For many people working in health that will mean grabbing relaxation fellowship with family and friends around commitment to people getting care over the holiday period. We are indebted to them all. For others of us it is a period for time out, to recover and recharge for the year ahead. Please also spare a though for those less fortunate and include a donation of food to one of the many causes as part of your Christmas planning. In 2019 there is much to be done. We have many work areas within our organisation that will take us to a new plane of operating, with services that have never been provided here before. This will extend to the community also. There is likely to be more unrest and many of the challenges really putting us to the test in terms of our determination to succeed. I am certain that we will. And so, Merry Christmas everyone. As you do take the time to share with family and friends please include in that this appreciation of all that you have done. I look forward to working with all in 2019 which will be another year of promise for yet further health gain for Tairāwhiti.
14

Health Targets
Better Help for Smokers to Quit
For the month of November we offered support to 94% of smokers admitted to hospital and 94% for Māori, close to the target with some results still to be checked. Again ED is the area where the most people have not been provided the opportunity of smoking advice although this is much improved on last month. Faster Cancer Treatment (FCT) 62 day pathway – 83%, 4 out of 6 people had the timeframes for their diagnosis and first treatment met but one delay was for clinical reasons. The target timeframe was met for one woman with breast cancer, two people with melanoma and one person with a head and neck lesion. One person with lung cancer experienced a delay that was due to clinical considerations. One woman with a gynaecological cancer experienced a delay due to capacity constraints – she had local surgery. 31 day pathway – 91% (10 out of 11). One man with prostate cancer experienced a significant delay to radical laparoscopic surgery which was a preferred option. There are a large amount of people on the 31 day pathway this month. Several are understandable as they came from screening or acute ED presentations. However, others need further investigation which will occur with the Cancer Nurse Coordinators over the next couple of weeks. Elective Production Elective discharges are on target at 100 % or 1079 discharges delivered against a target of 1079. Case weights are currently sitting at 95.8%. This is -60 CWDs behind the target of 1432. First Specialist Assessments are ahead of target at 108.4%, 232 FSAs ahead of a target of 2744. Elective Services Performance Indicators (ESPI) remain non-compliant at an organisational level in ESPI 2 – First Specialist Assessments and ESPI 5 – Time to treatment. An exemption is in place for Orthopaedics. Other specialities requiring close monitoring and additional sessions to mitigate risk of non-compliance include ENT, Neurology and Urology. Emergency Department 6 Hours ED did achieve the ED target of 95% this month coming in at 95.6%.
15

Immunisation November figures 8 months - Overall is 82%, (↓4%) Māori 79% (↓5%) and an overall decline rate of 10% (↑2 %) (17 children) 2 years - Overall is 84 % (↓1%) Māori 86 %(↓1%) and an overall decline rate of 9.5% (↓1%) (18 children) 5 years – Overall is 94% (↑1 %) Māori 96% (↑3 %) and an overall decline rate of 2% (↓1% %) (6 children) The decline rate at 8 months is going up again and 2yr and 5 yr looks as if the rate is finally on the decline. Samoa has recommenced their MMR immunisation programme so hopefully this will encourage families to be vaccinated. Outreach immunisation service (OIS) has had a lot of discussions with families concerning the safety of the NZ vaccination programme. Raising Healthy Kids
94% for total population and for Māori at 96%, against the target of 95%. Good bunce back in this indicator and encouraging for a good result across the year.
16

Financial Nov 18
Actual Nov 18
Var YTD Var
Oct 18 Actual
Oct 18 Var
Provider ($1,179k) ($351k) ($245k) ($771k) $98k Governance ($8k) ($8k) ($7k) ($25k) ($25k) Funder $83k $83k $441k $248k $248k Consolidated ($1,104k) ($276k) $188k ($553k) $321k The management accounts result to November includes $200k of the non-specific expense accrual. The Provider Arm operating result for the month was a deficit of ($1,179k) – negative variance ($351k). This is a worse result than the ($771k) deficit of last month and the $98k. Expenditure is up on last year 7.8% or $3,400k and the Provider Arm is now behind budgeted. While staff costs are under budget they are 9.8% up on last year, although this drops to 8.5% if the effect of the Cleaning, Orderly and Security staff transfer is removed. The nurses’ back pay was paid in November and this had a negative effect on leave liability. The staff costs are inflated by the increase in staffing mandated through the additional funding as part of the NZNO settlement. Acute loading on the hospital was down in November and this confirms that the surge in October was comparatively short lived. Acute admissions are now 1.3% down on last year to date as compared to 1.9% up last month and the situation has changed from 12% up two months ago. November had the lowest acute admissions since February 18 and then prior to that, February 17. November 18 had the lowest amount of admissions since 2014. In Medicine acute admissions were the lowest since February 18 and there were less admissions in November 18 as compared to 17, going back to 2012 to find a lower November. Overall medical acute admissions are now down 2.8% on last year to date. These are all encouraging trends. Staff costs were overspent for the month by ($21k), and as noted above, while significantly up on last year this is mainly related to the change in cost centres and the higher than usual salary increases. Outsourced staff cost increased in the month, medical ($167k) over budget, and overall up 11.3% on last year. Reliance is high on locum staff for orthopaedics and psychiatry, with the former in catch up mode and the latter having recruited to vacancies although there is now a further resignation. Between insourced and outsourced staff we remain ahead of budget though. Clinical supplies costs are up 10.7% on last year with the boost in electives combined with notable additional cost in medication (23.7% up on cancer drugs) and air ambulance costs (up 27.1% on last year). The Funder arm result was a surplus of $83k – positive variance $83k and year to date $441k – positive variance $441k. There was no further deterioration in IDFs for the month as due to reporting timeframes the updated figure from Waikato was not reflected. Waikato DHB has adjusted their estimates negatively again this month by $350k which will be reflected in the December Result. Comparisons to 2017/18 (YTD)
Result Actual Variance 2017/18 ($2,168k) ($2,550k) 2018/19 ($3,534k) $188k
Result Drivers Provider Revenue • Over budget for the month by $116k with YTD $242K ahead of budget. Health Workforce NZ receipts are
under this month ($22k) making YTD under ($38k). ACC income over budget $27k for the month making YTD under by ($61k). Claims processing has been prioritised for data entry. Patient and consumer sourced being over budget for month by $42k being primarily one non-resident patient.
Expenditure
17

• Overspent ($351k) for the month compared with underspend of $98k last month, YTD overspend ($245k) • Staff costs were overspent by ($21k) for the month. The leave liability increased from last month by ($153k),
mainly as a result of the revaluation of nurse leave from the processed back pay. Medical Staff were under spent $146k and there remains a positive between insourced and outsourced staff. Nursing staff costs were over budget by ($177k), mainly related to the leave revaluation. Allied Health was $66k under budget, Support under by $5k. Sick leave was 1.8% for the month, up from 1.7% last month. Sick leave is down on last year when it was 1.9% in November 2018.
• Paid FTE was up 10 for the month. There were 746 FTE paid for the month. This includes the transferred staff and net of these the figure is 711, which compares to 706 last November. This is a stabilisation with the staff growth from winter preparedness and increased revenue for nursing positions.
• Outsourced services were overspent ($199k) for the month. Year to date this is ($259k) more than last year. Recruitment and cover remains problematic in orthopaedics, anaesthetics and ED.
• Clinical supplies were overspent by ($249k) for the month. Usage of blood was $11k under for the month. Cancer treatment costs were overspent by ($7k) and are ($166k) or 23.7% higher than last year. Air transport expenditure was ($47k) over for the month and is ($229k) higher than year to date last year. Patient transport and lodging is overspent YTD by ($37k) and is 4.1% more than last year.
• Infrastructure and non-clinical supplies costs were underspent $2k for the month. The non-specific accrual is $200k.
Winter 2018 had a small sting in the tail but as identified earlier it has overall seen less acute admissions. The early surge in admissions at the start of November dissipated and in a changed pattern medical admissions reduced which meant that with surgery up there was some uncharacteristic over flow from surgery to medicine.
At the same time, surgery continues to fun ahead in Orthopaedics to catch up on people waiting for surgery, and to address the people who have been waiting for a first assessment. The orthopaedic work also continues in reviewing all the referrals which is proving a good way to ascertain the actual workload and support people in the community.
18

General medicine admissions were sharply down.
Paediatric medicine acute admissions November results shows a large reduction also.
19

General Surgery as a slight correction on last month and up overall at a higher rate than medicine. Time to look at the reasosn for this trend.
Orthopaedic admissions continue on a saw tooth
20

November ED admissions are down again to below the trend line and are higher than this time last year.
Governance and Administration Revenue • On budget for the month. Expenditure • Overspent ($8k) for the month and over $7k YTD. • Staff costs over budget $9.5k for the month and YTD. • Non staff expenses are over budget $9k for the month. Healthshare is $15k over budget and will continue
to be as the year progresses due to budgeting error. • Democracy costs are $16k under budget and under budget $23k YTD.
Funder
Revenue • Negative ($158kk) for the month, mainly a result of rework of the Pharmac rebate mechanism. Expenditure
• Underspent $242k for the month, includes offsetting expenditure for pay equity and Te Kūwatawata.
Better Outcomes for People Our drive to improve health outcomes for Māori continues with tangible effort being made to increase the proportion of Māori on staff at Hauora Tairāwhiti. This is being effected through our policy of employing Māori first, followed by local people and then people who have links to the region in our employment strategy. The latest figures from national reporting show the progress being made in Te Tairāwhiti and in the wider Midland region. Our policy and local training programme have enabled us to have the highest proportion of nursing staff who are Māori in the country, with the highest proportion of Māori overall by a considerable distance.
21

22

Primary & Community Health Services Changes to Very Low Cost Access Funding From the 1st December 2018 all Primary Healthcare Medical Centres in Tairāwhiti offer • All enrolled children aged 13 and under are free of charge to visit GP or nurse
o Their regular $5 prescription fee will be free. o After-hours fee will be free.
Child, Youth and Population Health Annual Planning Cafés Two cafés were provided during late November to early December, specific to Children, Youth and Population Health. These were based in community settings and were well attended. • Child, Youth and Whānau. Key themes discussed were Child Health and Wellbeing, utilising the questions
from the national DPMC Child and Youth Wellbeing Strategy consultation, underway at the time. The other themes were Maternal and Infant Health – Enrolling New-borns and ASH Rates 0 – 4 Years Respiratory. Common points emerged, such as working with whānau, connecting with external colleagues where referral pathways exist, including feedback loops; and ensuring whānau at all times are supported to realise their health aspirations and make decisions that they’re capable of achieving for the health and wellbeing of their tamariki and themselves
• Prevention OR Intervention. Key themes discussed were Screening Programmes, Health Promotion & Education and Health Literacy. Common points emerged from discussions - ‘the messenger is key’ in terms of relating to whānau; ‘community-based services’ and ‘health promotion included in planning, prior to a screening programme’; ‘engage local, building on what’s working well in community not adding to’; and ‘keep your messages simple’.
The questions for all of these themes included achieving equity elements and improving quality clinical health literacy to be whānau centred. This information will inform the full cafés workshop summary learning report. Rheumatic Fever – Healthy Homes Initiative Completed the year with a celebration of the Rheumatic Fever Community Champions and the success of this year’s campaign. Five champions, ranging in ages from 70+ to 11, have demonstrated that local stories make a difference to communities. We will expand on their stories for next year’s winter campaign, and also build into it finding our services / clinical champions - a ‘good sorts’ approach to recognising those that go that extra mile,
23

who whānau want to identify. Profiling good practise models, health literacy effectiveness and support for whānau where Rheumatic Fever and Healthy Homes touches their lives.
Safe-sleeping & Wahakura ‘Mokopuna Ora’ project Safe-sleeping service specifications for provider-based services developed and progressing through approval and sign-off. Seven wahakura weavers have confirmed their participation in the Mokopuna Ora project, inclusive of being profiled as a weaver within the project, weaving wahakura for supply. At this point three have confirmed that they are available for tutoring small wahakura weaving wānanga sessions. Note: Ngāti Porou currently delivers four wānanga/year on the coast. Coordination of the SUDI Prevention and Safe-sleeping programme will sit within the Population Health team, to ensure overall connectedness between services, and that communities are provided for. Health promotion, communication and SUDI prevention training will also be provided for within this role. Weavers’ relationship, supply and distribution of wahakura will sit within the E Tipu E Rea programme, and the three partner services (Tūranga Health, Ngāti Porou Hauora and Hauiti Hauora) Māmā and Pēpi services will liaise directly with LMCs, hapū māmā and other maternal and infant services.
Mental Health, Alcohol and other Drugs Request for Proposal A review of the mental health services has been agreed. The review will take a comprehensive approach including looking at outsourced services, and the range of services provided across the different health settings. The Request for proposal was placed on the GETS site early in December 2018, will close in January 2019 hopefully with a team on the ground early in February 2019. Suicide Prevention and Postvention. We have had a successful recruitment to the Suicide Postvention, Prevention Coordinator, the person starts 10 December. Mental Health Review The findings of the mental health review have been received, the recommendations and link to the full document are to be provided. Health of Older People and Disability Support Services Home and Community Support Services Registration of Interest (ROI) There has been good interest in the ROI. The Probity Audit review recommended actions are on track. Advance Care Planning The first locally provided Level 1 (L1) ACP workshop is booked for 20th February 2019 • St John trainer in the process of training local St John staff • Tūranga Health trainer is working alongside staff and consumers to provide information and encourage the update of ACPs • District nursing is coming on board with spreading the ACP message • A national ACP implementation guide has been produced. Whānau Falls Prevention Hip fracture registry: We are below the national standard for length of stay. The survival rates are good, with a slight improvement in bone medications on discharge, Community group Strength and Balance Class: the quarter target was 255, and we are at 280 (though this will drop over the summer holidays). Average utilisation of classes is at 48%.
24

Sport Gisborne in-home strength and balance has 70 active clients, 25 home visits in October. Planning for April Falls 2019 is underway. Space at the public library has been booked. Needs Assessment Support Coordination (NASC) Higher than usual volumes of referrals requesting rest home placement have been received.
Population Health Supporting stop smoking • Gisborne District Council Policy Analyst is working alongside Taki Tahi Toa Mano to promote council’s
Smokefree Outdoor Spaces policy, although Smokefree CBD is yet to be added to council’s agenda. • Tūranga Health, Pinnacle Midland Health, Population Health and Planning & Funding met collectively with
the hospital Radiology staff to discuss how to improve services for hapū māmā who smoke. Tūranga Health and Pinnacle will develop a pathway with the radiology team regarding referrals. More discussions to be held with Maternity Care and Oral Health services.
• Engagement with Mental Health to eradicate smoking among Tangata Whaiora. o A meeting with Mental Health senior management, Population Health, and our Stop Smoking
service, to collectively look at reducing smoking among our tangata whaiora. o A plan of action to be implemented in the new year.
• In support of the National Smokefree Cars campaign, Taki Tahi Toa Mano (Tairāwhiti Smokefree Coalition) is developing a plan to collect data on the number of people smoking in cars that have children in them. This will determine the level of action we need to take as a region.
Work well • Downer is discussing challenging other workplaces to take part in the Relay for Life - Cancer Fundraising
event next year. • Downer has included WorkWell in their staff induction process & booklet. • The first whānau day held in Ruatoria, with over 1000 locals attending and over 15 services collaborating
together for whānau to access. Rhythm and Vines (RnV) A Hauora Village is being established this year: One wellness space at Rhythm and Vines confirmed with Women-Only space attached to it. This means staff will spend time on location to support wellness vision with management. Activities over the festive season: Pa wars • Promoting Ae to Wai at Pa Wars at Tokomaru Bay in conjunction Hauiti Hauora. Lean On Me concert • Prevention/Intervention Suicide Awareness Concert/Whānau day in Te Araroa 15th Dec 2018. East Coast Vibes Concert 2019. • Supporting safe sex
25

Hauora Tairāwhiti Board
Title: Summary Financial Report
Prepared By: Craig Green, GM Finance
Date: Tuesday, 4 December 2018
Information Item
1. GM FINANCE COMMENTS Financial Performance Result and Overview The DHB has a Board approved $9.5 million deficit budget for the 2018/19 financial year. The DHB result for the period ending 30 November 2018 is $376k adverse to budget with a deficit of $1,104k for the month. For the month, the:
• Provider Arm is $ 351k adverse • Funder Arm is $ 83k favourable, and • Governance Arm is $ 8k adverse
Provider Arm: For the month, the Provider Arm’s adverse variance of $351k driven by: • Revenue: $116k favourable for the month ($49k in Non-resident income, $48k in side contracts and $45k
in ISLA income) • Expenditure: $446k adverse. Key variances:
o Personnel costs: $21k adverse to budget of $6,298k o Outsourced Services: $199k adverse (Medical personnel adverse $167k and Allied Health $32k) o Clinical Supplies: $249k adverse (Treatment Disposals $88k adverse – driven by recovery costs of
$77k paid to Tūranga Health for incontinence products up to 30/06/2018; Implants/Prostheses $66k adverse; Pharms $41k, Air Ambulance $47k and ambulance $6k).
Funder Arm: For the month, the Funder Arm’s favourable variance of $83k driven by:
• Revenue: $162k adverse; MoH subcontracts $178k, off-set by Pharmac rebate correction $346k • Expenditure: $192k adverse; driven by:
o Personal Health: $223k favourable; IDF Outflows $122k, Medical Outpatients $50k, Pharmacy $73k offset by General Medical Subsidy $22k.
o Mental Health: $55k favourable; kaupapa Maori $18k, community residential beds $26k, minor mental health expenditure $18k
2. CONSOLIDATED FINANCIAL PERFORMANCE SUMMARY
Note: due to the delay in receiving the Waikato IFD accrual, these figures do not include the November 2018 IDF accrual increase for the month of $142k
$000 Actual Budget Var Var%YTD
ActualYTD
BudgetYTD Var
YTD Var%
Last YTD Actual
% Change
Income 16,081 16,169 (88) (0.5%) 82,172 80,863 1,309 1.6% 78,548 4.6%LessProviding Health Services 9,832 9,365 (466) (5.0%) 46,912 46,425 (487) (1.0%) 43,512 (7.8%)Funding Other Providers 7,121 7,408 287 3.9% 37,666 37,041 (626) (1.7%) 36,198 (4.1%)Governance 232 223 (8) (3.8%) 1,128 1,121 (7) (0.7%) 1,007 (12.0%)Total Expenses 17,185 16,997 (188) (1.1%) 85,706 84,586 (1,120) (1.3%) 80,717 (6.2%)
- - -Surplus / (Deficit) (1,104) (828) (276) (33.3%) (3,535) (3,723) 188 5.1% (2,168) (63.0%)
For the month ended 30 November 2018 Year to Date
26

3. STATEMENT OF FINANCIAL PERFORMANCE – CONSOLIDATED
AnnualActual Budget Variance Actual Budget Variance Actual % Budget$000 $000 $000 $000 $000 $000 000 Change $000
Revenue Government and Crown Agency Sourced MOH - Vote Health 14,919 14,741 178 75,068 73,706 1,363 72,792 3.1% 176,894 MOH - Personal Health 354 306 48 1,793 1,531 262 1,709 4.9% 3,674 MOH - Public Health 195 230 (35) 975 1,148 (173) 712 37.0% 2,754 MOH - Disability Support 62 62 0 309 309 0 304 1.5% 740 Clinical Training Agency 68 89 (22) 407 445 (38) 432 (5.8%) 1,069 Inter District Flows 199 192 7 963 960 3 904 6.4% 2,304 Other DHB's 18 1 17 51 6 45 8 553.1% 14 Accident Insurance 220 191 29 974 970 5 1,131 (13.8%) 2,315 Government (non DHBs) (66) 277 (343) 1,217 1,386 (170) 107 1041.1% 3,327 Total Government and Crown Agency 15,968 16,089 (121) 81,757 80,460 1,296 78,098 4.7% 193,092 Patient and Consumer Sourced 67 25 42 121 127 (7) 120 0.3% 306 Other Income 46 55 (9) 294 275 19 330 (10.8%) 599Total Revenue 16,081 16,169 (88) 82,172 80,863 1,309 78,548 4.6% 193,998Expenditure Personnel Costs Medical Personnel 1,902 2,047 146 8,901 9,884 984 8,603 (3.5%) 24,080 Nursing Personnel 2,455 2,279 (177) 11,813 11,311 (502) 10,375 (13.9%) 27,783 Allied Health Personnel 949 1,013 64 4,630 5,037 407 4,462 (3.8%) 12,015 Support Personnel 220 225 5 1,103 1,146 43 691 (59.6%) 2,722 Management/Administration Personnel 909 841 (67) 4,230 4,209 (20) 3,806 (11.1%) 9,984 Total Personnel Costs 6,435 6,405 (30) 30,676 31,588 912 27,936 (9.8%) 76,583 Outsourced Services Medical Personnel 416 250 (167) 1,899 1,157 (742) 1,777 (6.9%) 2,601 Nursing Personnel 0 1 1 3 2 (1) 39 93.4% 3 Allied Health Personnel 42 10 (32) 160 52 (108) 48 (231.1%) 127 Support Personnel 1 0 (1) 1 0 (1) 0 (238.6%) 0 Management/Administration Personnel 1 0 (1) 30 0 (30) 17 (80.4%) 0 Clinical Services 282 277 (5) 1,434 1,399 (35) 1,423 (0.8%) 3,342 Corporate/Governance 0 7 7 0 34 34 0 0.0% 82 Funder Services 35 20 (15) 166 99 (67) 103 (61.2%) 239 Total Outsourced Services 778 564 (214) 3,695 2,744 (951) 3,407 (8.4%) 6,393 Clinical Supplies Treatment Disposables 422 334 (88) 1,767 1,703 (65) 1,738 (1.7%) 4,062 Diagnostic Supplies & Other Clinical 39 41 2 179 207 28 195 8.1% 494 Instruments & Equipment 158 150 (7) 768 767 (2) 702 (9.5%) 1,829 Patient Appliances 50 36 (15) 210 182 (28) 170 (23.4%) 433 Implants & Prostheses 175 109 (66) 706 558 (148) 584 (21.0%) 1,332 Pharmaceuticals 355 314 (41) 1,799 1,602 (197) 1,588 (13.3%) 3,821 Other Clinical & Client Costs 377 338 (40) 1,807 1,556 (251) 1,507 (19.9%) 3,802 Depreciation - Clinical Equipment 132 138 6 654 704 50 644 (1.5%) 1,679 Total Clinical Supplies 1,709 1,460 (249) 7,891 7,278 (613) 7,127 (10.7%) 17,452 Infrastructure & Non Clinical Supplies Hotel Services, Laundry & Cleaning 197 172 (24) 979 901 (78) 1,267 22.7% 2,158 Facilities 187 216 28 1,015 1,101 85 1,141 11.1% 2,626 Transport 46 42 (3) 198 216 18 189 (5.1%) 516 IT Systems & Communications 161 169 8 768 860 92 678 (13.4%) 2,053 Interest Charges 2 8 7 34 42 9 46 27.2% 101 Bank and Facility Charges 1 1 0 3 3 0 3 18.8% 7 Capital Charge 220 220 0 1,122 1,122 0 1,036 (8.3%) 2,678 Professional Fees & Expenses 72 77 4 318 391 72 275 (15.9%) 932 Other Operating Expenses 134 119 (15) 692 605 (87) 766 9.6% 1,445 Democracy 18 28 10 122 145 23 127 4.0% 345 Subsidiaries & Joint Ventures (29) (29) 0 (147) (147) 0 (147) 0.0% (350) Depreciation - Non Clinical 133 137 4 673 696 23 667 (1.0%) 1,661 Total Infrastructure & Non Clinical Supplies 1,142 1,160 18 5,779 5,936 157 6,049 4.5% 14,172 Provider Payments Personal Health Expenditure 4,689 4,957 269 25,233 24,787 (445) 23,199 (8.8%) 59,490 Mental Health Expenditure 581 626 45 3,396 3,131 (265) 3,603 5.7% 7,514 Public Health Expenditure 115 105 (10) 534 524 (10) 514 (3.9%) 1,258 Disability Support Expenditure 1,504 1,490 (14) 7,327 7,450 122 7,699 4.8% 17,879 Hauora Maori Services Expenditure 233 230 (3) 1,176 1,148 (28) 1,183 0.6% 2,756 Total Provider Payments 7,121 7,408 287 37,666 37,041 (626) 36,198 (4.1%) 88,897Total Expenditure 17,185 16,997 (188) 85,706 84,586 (1,120) 80,717 (6.2%) 203,498Net Surplus/(Deficit) (1,104) (828) (276) (3,535) (3,723) 188 (2,168) (63.0%) (9,500)
November 2018 Year to Date Last YTDConsolidated Statement of Financial
Performance
27

4. FINANCIAL POSITION - SUMMARY The financial position as at November 2018 is below. This indicates a weak balance sheet, with $18.1m in negative working capital and a net worth of $45.5m.
June 2018 November 2018 June 2019Actual Actual Budget
49,045 Crown Equity 45,511 50,369Represented by:
8,548 Current Assets 11,259 5,85022,976 Current Liabilities 29,968 22,052
(14,428) Net Working Capital (18,710) (16,202)65,174 Fixed Assets 65,849 67,838
1,702 Term Liabilities 1,629 1,26749,045 Total Employment of Capital 45,511 50,369
CONSOLIDATED STATEMENT OF FINANCIAL POSITION ('000s)
Actual Actual BudgetJune 2018 November 2018 June 2019
ASSETS:Current Assets
0 Cash and cash Equivalents 74 00 NZ Health Partnership Ltd - DHB Sweep 0 0
1,133 Receivables (Net of provision for Doubtful Debts) 1,558 1,8144,527 Accrued Income 6,207 1,1481,026 Prepayments 1,568 1,0261,862 Inventories 1,852 1,8628,548 Total Current Assets 11,259 5,850
Non Current Assets923 Investment in Associates 925 626
61,483 Property, Plant & Equipment 62,249 62,4902,768 Intangible Assets 2,675 4,722
65,174 Total Non Current Assets 65,849 67,83873,722 Total Assets 77,108 73,688
LIABILITIESCurrent Liabilities
42 Cash and cash Equivalents 0 01,597 NZ Health Partnership Ltd - DHB Sweep 3,958 2,412
10,612 Payables and deferred revenue 14,781 9,568138 Current Portion of term Loans 143 138
10,586 Employee Entitlements 11,086 9,93422,975 Total Current Liabilities 29,968 22,052
NON Current Liabilities991 Employee Entitlements 991 557711 Term Loans 638 710
1,702 Total Non Current Liabilities 1,629 1,26724,677 Total Liabilities 31,597 23,319
49,045 NET ASSETS 45,511 50,369
EQUITY:49,861 General Funds 49,861 63,794
(39,847) Accumulated Deficit (43,381) (50,114)39,004 Asset Revaluation Reserve 39,004 36,689
28 Bequests and James Cook reserve 28 049,045 Total Equity 45,511 50,369
CONSOLIDATED STATEMENT OF FINANCIAL POSITION ('000s)
28

5. CASH FLOW POSITION
Cash Position The cash balance was in debit by $3,958k with the DHB pool at month end; being $532k favourable to forecast debit balance of $4,490k. Operating cash was $28k adverse to forecast; Investing in capital equipment $83k adverse to budget and Financing in-line with expectations. The DHBs swift balance debit highpoint was 29 November 2018, at $3,967k.
Inwards: Inward cash was $192k favourable to forecast, driven by MoH side contracts.
Outwards: Operating Cash outflow adverse $220k to forecast; IDFs of $137k, payments to non-DHB providers $594k offset by adverse supplier payments of $154k , GST of $86k and payroll costs of $716k.
Capital Expenditure: $83k adverse to budget.
Outlook: Closing cash projected $4,836k cash negative in December; net cash expected to be $878k negative.
6. CAPITAL EXPENDITURE (CAPEX) Depreciation funded capital expenditure planned for the 2018/19 year is $2.821m. The table below summarises performance against budget (depreciation funded and Carry Forward from prior year) for the month and year-to-date.
A total of $326k spent on CAPEX during the month of November 2018 and is adverse year-to-date to the revised linear budget by $78k.
Actual Budget Var Actual Budget VarOpening cash (3,625) (4,268) 644 (1,597) (1,597) 0Operating (7) 22 (28) (337) (1,027) 690Investing (327) (243) (83) (2,024) (1,866) (158)Financing 0 0 0 0 0 0Closing cash (3,958) (4,490) 532 (3,958) (4,490) 532Closing cash Balance in NZHP Swift account (3,958) (3,958)
$'000s Month YTD
29

7. FINANCIAL FORECAST
30

9. VALUE RELEASE PROGRAMME – SAVINGS PLAN
Period: 5
Description Responsible PersonNet Savings
Value ($000)
Year-to-Date Savings ($000)
Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18 YTD TotalHolters - now being read locally
CNM Med/Mental Health
- - Cardiology service development CCM/Director 100 - - Registra service development CCM/Director 100 - - Removed 20 people off the GA list for dental Director Allied Health 120 - - - MBIE - 2018/19 savings uptake of AoG contracts - QUARTERLY CFO 40 9 8.7 8.7 Staff cost reduction (watches, casual staff, OT, non-replaced positions) CCMs/GM/accountants 100 - - - - - - - - - - - Transport Service reconfiguration - 3 months from April 2019 CFO 30 - - - - - - - - - - - National and Regional Savings (AoG, Pharmac, Health Partnerships) CFO 100 - - - - - - - - - - - Cleaning, Orderly and Security (July - September) CFO 115 115 40.6 37.6 36.9 115.1 Concession rates - possible claw back from CM - tbc CFO - - NOS - deferral option CFO 100 41 8.3 8.3 8.3 8.3 8.3 41.5 Microsoft licence renewal CFO 35 15 2.9 2.9 2.9 2.9 2.9 14.6 Office Max CFO 15 - - Air NZ CFO 30 - - fCM - reduction in use for patient transport - 6 months (Dec-Jun) CFO 30 - - Miscellaneous Savings (Collected smaller projects) CCMs, CDs and GMs 85 - - - - - - - - - - - - - - Total 1,000 180 51.8 48.8 56.9 11.2 11.2 - - - - - - - 180.0 Completion rate 18.0% 18.0%
Valur Flow Savings - clinical/non-clinical initiatives All 85 - Lease Equiment - Panoramic x-rays - Staff travel and accomodation - Total 85 - - - - - - - - - - - - -
MONTH BY MONTH SAVINGS ('000s)2018/19 Operational_Value Release Plan
31

9. PERFORMANCE GRAPHS
32

Hauora Tairāwhiti Board Sub-Committee Reports
AGENDA ITEM
AGED & DISABILITY SUPPORT ADVISORY COMMITTEE 4.12.18
No public included decision items for consideration.
COMMUNITY & PUBLIC HEALTH ADVISORY COMMITTEE 4.12.18
No public included decision items for consideration
HOSPITAL ADVISORY COMMITTEE 11.12.18
No public included decision items for consideration
FINANCE, AUDIT & IT COMMITTEE 11.12.18
No public included decision items for consideration
33

Hauora Tairāwhiti BoardHealth Workforce DHB Benchmarking Report - Human Resources KPI's to 30 September 2018
Title:
Prepared
By: Date:
Jim Green, Chief Executive Wednesday,
12 December 2018
Information Item
EXECUTIVE SUMMARY
A summary of DHB benchmarking of Human Resources KPI’s for your information.
34

HUMAN RESOURCES KPI’S
DHB Benchmarking
Quarter ended 30 Sept 2018
Data for this report is from the Health Workforce Information Programme (HWIP) data repository. Data is divided into chart of accounts groupings. Midwifery data is reported separate from nursing where separate data is available.
All graphs compare against the same quarter one year ago.
Appendix A – Graph elements provides a quick guide on how to read the graphs (see page 56).
35

Sick leave – all staff
The percentage of sick leave taken hours (paid and unpaid) to paid hours.
All DHB Staff Sick Leave – Qtr end 30 Sept 2018
36

SMO Staff Sick Leave – Qtr end 30 Sept 2018
37

RMO Staff Sick Leave – Qtr end 30 Sept 2018
38

Nursing Staff Sick Leave – Qtr end 30 Sept 2018 (includes midwifery)
39

Allied Health Staff Sick Leave – Qtr end 30 Sept 2018 (includes scientific and technical)
40

Support Staff Sick Leave – Qtr end 30 Sept 2018
41

Management & Admin Staff Sick Leave – Qtr end 30 Sept 2018
42

Staff Turnover – all staff
Incidence of staff resignations in an organisation. Comprises # voluntary resignations / Total headcount at the beginning of the period.
Note RMO’s, Temporary (fixed term) employees and casual employees are excluded from this measure. Note also that employment terminations due to redundancy, death, dismissal and medical grounds are excluded.
All DHB Staff Turnover – Qtr end 30 Sept 2018
43

SMO Staff Turnover – Qtr end 30 Sept 2018
44

Nursing Staff Turnover – Qtr end 30 Sept 2018 (includes midwifery)
45

Allied Health Staff Turnover – Qtr end 30 Sept 2018 (includes scientific and technical)
46

Support Staff Turnover – Qtr end 30 Sept 2018
47

Management & Administration Staff Turnover – Qtr end 30 Sept 2018
48

Accrued Annual Leave (2+ years) – all staff
The percentage of employees where accrued Annual Leave balance is greater than 2 years Annual Leave entitlement.
Accrued Annual Leave (2+ years) all staff – Qtr end 30 Sept 2018
49

SMO Annual Leave 2+ years – Qtr end 30 Sept 2018
50

RMO Annual Leave 2+ years – Qtr end 30 Sept 2018
51
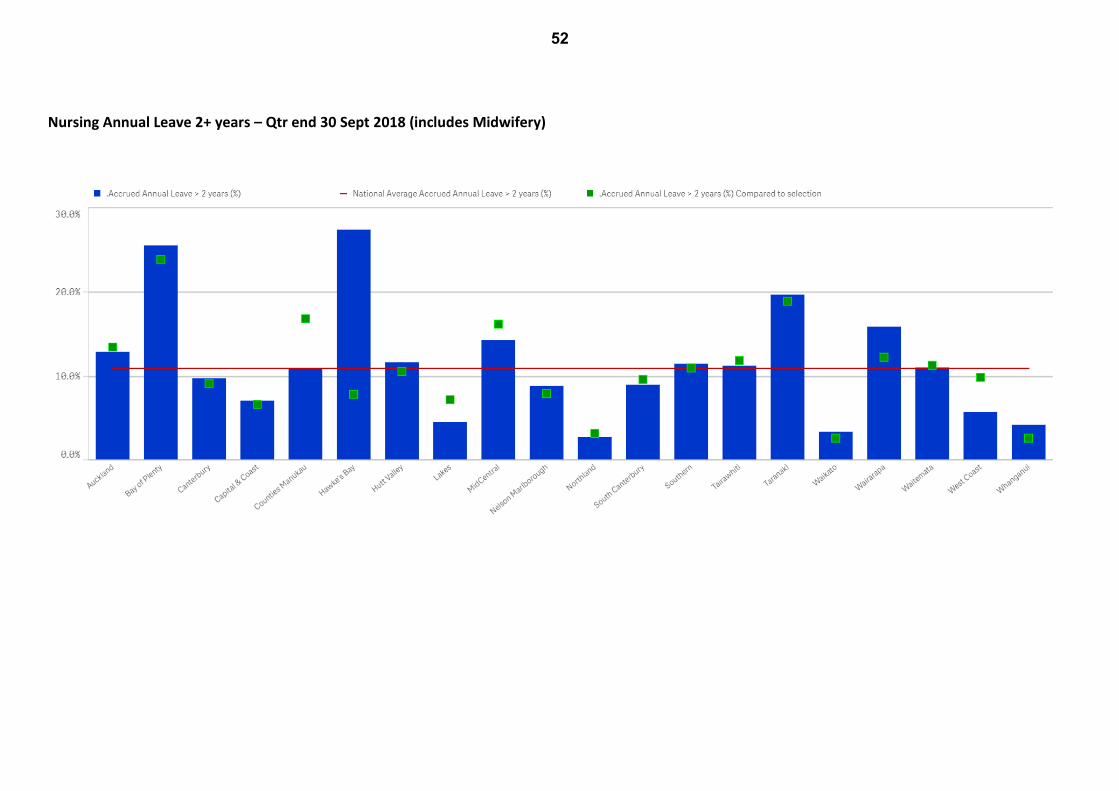
Nursing Annual Leave 2+ years – Qtr end 30 Sept 2018 (includes Midwifery)
52

Allied Health Annual Leave 2+ years – Qtr end 30 Sept 2018 (includes scientific and technical)
53

Support Annual Leave 2+ years – Qtr end 30 Sept 2018
54

Management and Administration Annual leave 2+ years – Qtr end 30 Sept 2018
55

Average Leave Balance per Employee
The average hours of leave owing to each employee. Leave consists of annual leave, statutory lieu leave, shift leave and lieu of overtime leave.
All DHB Average Leave Balances – 30 Sept 2018
56

SMO Average Leave Balances – Qtr end 30 Sept 2018
57

RMO Average Leave Balances – Qtr end 30 Sept 2018
58

Nursing Average Leave Balances – Qtr end 30 Sept 2018 (includes midwifery)
59

Allied Health Average Balances – Qtr end 30 Sept 2018 (includes scientific and technical)
60

Support Average Leave Balances – Qtr end 30 Sept 2018
61

Management & Admin Average leave balances – Qtr end 30 Sept 2018
62

Lost Time Injury Rate
All workplace injuries or illnesses that result in lost work time / worked hours (in millions).
DHB Total Lost Time Injuries – Qtr end 30 Sept 2018
63

DHB Total Time to Hire – Qtr end 30 Sept 2018
64

Overtime – all staff
The percentage of overtime hours to paid hours.
All DHBs Overtime % - Qtr end 30 Sept 2018
65

SMO Overtime % - Qtr end 30 Sept 2018
66

RMO Overtime % - Qtr end 30 Sept 2018
67

Nursing Overtime % - Qtr end 30 Sept 2018
68

Allied Health Overtime % - Qtr end 30 Sept 2018 (includes scientific and technical)
69

Support Overtime % - Qtr end 30 Sept 2018
70

Management & Admin Overtime % - Qtr end 30 Sept 2018
71

Maori representation in the workforce – all staff
The percentage of Maori staff to total staff.
DHB Maori Staffing Percentage – Qtr end 30 Sept 2018
72

SMO Maori Staffing Percentage – Qtr end 30 Sept 2018
73

RMO Maori Staffing Percentage – Qtr end 30 Sept 2018
74

Nursing Maori Staffing Percentage – Qtr end 30 Sept 2018 (includes Midwifery)
75

Allied Health Maori Staffing Percentage – Qtr end 30 Sept 2018 (includes scientific and technical)
76

Support Maori Staffing Percentage – Qtr end 30 Sept 2018
77

Management & Admin Maori Staffing Percentage – Qtr end 30 Sept 2018
78

Hauora Tairāwhiti BoardTitle: Submission on the Health (Drinking Water) Amendment Bill
Prepared By: Bruce Duncan, Medical Officer of Health
Date: Thursday, 6 December 2018
Decision Item
EXECUTIVE SUMMARY
In general, Hauora Tairāwhiti supports the clauses within the Bill.
Specifically, we support the removal of the 3-year consultative timeframe (s69P of the principal Act) and the requirement for change to wait for 2 years post Gazetting (s69R of the principal Act) (clauses 5 and 6).
We support the inclusion of timeframes (for the implementation of measures to mitigate risks) in Water Safety Plans (s69Z of the principal Act) (clause 8).
Hauora Tairāwhiti does not support all the amendments in clause 9. We believe that the repeal of section of 69KZ (2) (b) is premature. The Havelock Inquiry Stage 2 report found that “the question of accreditation should be reviewed, but once the questions of structure, employment, accountability and qualifications are resolved” (para 563, Report of the Havelock North Drinking Water Inquiry: Stage 2). We further note that the IANZ accreditation underpins the quality systems, technical training and support, and improved consistency amongst drinking-water assessors linked under the Central North Island Drinking Water Assessment Unit (CINDWAU). Hauora Tairāwhiti further suggests that, If IANZ is discontinued as a consequence of a review, then a fit for purpose, and adequately resourced and mandated framework must replace it. Such a quality assurance framework could support all the regulatory activities of Public Health Units.
BACKGROUND
There has been discussion around the proposals contained in the Bill. The changes come from the findings of the Havelock North Drinking Water Inquiry, parts 1 and 2. They represent the more urgent legislative changes recommended by the Inquiry in light of the events in Havelock North. They came out of submissions from various agencies, highlighting issues that challenge the provision of safe drinking water.
Some of the changes that were recommended, for example, removal of the need to be a Health Protection Officer (HPO) as an essential prerequisite for a Drinking Water Assessor, have been managed though other processes that do not require legislative change.
There is some concern in the sector that the removal of international accreditation is purely an opportunistic cost reduction activity, and pre-empting a review (which might not reach the same conclusion). Many in the sector would not necessarily oppose the removal of international accreditation (IANZ) per se; however, we recognise that it has brought a rigour to the sector.
80

OPTIONS
Explanatory note provided with Bill: General policy statement The policy objectives of the Bill are to improve the effectiveness and efficiency of Part 2A (drinking water) of the Health Act 1956 (the Act) without materially affecting any party or imposing new or additional costs. Following the Government Inquiry into Havelock North Drinking Water, Cabinet agreed to a range of measures to address the Inquiry’s recommendations, including some immediate amendments to Part 2A of the Act. The amendments proposed as a result of the Inquiry will be supplemented with a small number of additional, minor improvements to Part 2A of the Act. The main provisions in the Bill
• Remove requirements for the Ministry of Health to consult for 3 years and gazette changes for 2 years prior to making any changes to the drinking-water standards:
• Clarify that water safety plans must include timetables to implement measures that mitigate risks to drinking water:
• Streamline processes for the appointment of drinking-water assessors: • Remove unnecessary references to designated ports and airports.
Clause by clause analysis
1. Clause 1 relates to the Title. 2. Clause 2 relates to commencement and provides that the legislation will come into force on the
day after the date on which it receives the Royal assent. 3. Clause 3 provides that the Health Act 1956 is the principal Act amended by this Bill. 4. Clause 4 amends section 69C of the principal Act, which relates to the application of sections 69S
to 69ZC of that Act, by deleting references to the operator of a designated port or airport. It is considered no longer necessary to impose duties on those operators under Part 2A of the principal Act because ports and airports generally receive water from networked suppliers who are subject to Part 2A.
5. Clause 5 amends section 69P of the principal Act, which requires the Minister of Health to consult before issuing, adopting, or amending drinking-water standards. Currently, section 69P requires the Minister to be satisfied that adequate consultation has been carried out over a period of at least 3 years. The reference to the 3-year period is removed by this amendment.
6. Clause 6 replaces section 69R of the principal Act, which relates to the commencement of drinking-water standards. Currently, most drinking-water standards come into force at least 2 years after the date of publication of the relevant Gazette notice. This amendment provides for standards to come into force at least 28 days after the date of publication of the relevant Gazette notice.
7. Clause 7 repeals section 69U(4) of the principal Act, which sets out examples of reasonable steps that contribute to the protection of the source of drinking water. It is intended that the Ministry of Health will provide examples through guidelines.
8. Clause 8 amends section 69Z of the principal Act, which requires drinking-water suppliers to prepare and implement a water safety plan. This amendment replaces an incorrect reference to a risk management plan with a reference to a water safety plan and requires a supplier to comply with the timetable in the supplier’s water safety plan.
9. Clause 9 amends section 69ZK of the principal Act, which enables the Director-General of Health to appoint drinking-water assessors. This amendment—
a. deletes references to agencies and ensures that only individuals (natural persons) will be appointed as assessors:
b. removes the requirement that individual assessors and any agency that employs them be internationally accredited.
81

10. Clause 10 amends section 69ZP of the principal Act, which sets out the powers of drinking-water assessors and designated officers. There is an overlap between the powers in section 69ZP and those available to designated officers in sections 128 (powers of entry and inspection) and 128A (powers under the Building Act 2004). This overlap in the relevant powers has caused some confusion among people performing official functions under Part 2A of the principal Act. This amendment will—
a. provide that the general powers in sections 128 and 128A apply for the purposes of Part 2A, whether or not a drinking-water assessor or designated officer is a medical officer of health, a health protection officer, or a person authorised in writing by the medical officer of health or by any local authority:
b. make the exercise of those powers subject to sections 69ZR (which restricts the exercise of powers) and 69ZS (which requires a warrant to enter a dwellinghouse).
11. Clause 11 amends section 69ZZZB of the principal Act. This amendment replaces subsection (1) of that section, which requires the Director-General to prepare and publish an annual report on drinking water. The new subsection (1) carries over the requirement for an annual report, but enables the Director-General to use contractors to prepare and publish the report.
12. Clauses 12 to 19 make technical amendments to various provisions in Part 2A of the principal Act, principally to align them with the amendments set out in Part 1 of this Bill. In these amendments,—
a. the definition of rural agricultural drinking-water supply in section 69G is amended to remove the reference to commercial agriculture so that all supplies used primarily for agricultural purposes of any kind will be caught by this definition:
b. references to port and airport operators are deleted: c. the requirement in section 69ZR(1)(c) for designated officers to obtain the written
approval of a medical officer of health before exercising a power of entry is removed because designated officers have that power already under section 128 in their capacity as health protection officers. This amendment reflects the changes made by clause 10 of this Bill:
d. section 69ZX is replaced by a new section that requires the Director-General to keep a register of individuals appointed as drinking-water assessors, which reflects the amendments made by clause 9 of this Bill that ensure that only individuals (not agencies) are appointed as drinking-water assessors. The current section 69ZX provides only for the registration of agencies appointed as drinking-water assessors, but no agencies have been appointed.
RECOMMENDATION
The Board 1. Notes the contents of this paper 2. Supports the formal submission as follows
a) Specifically, we support the removal of the 3-year consultative timeframe (s69P of the principal Act) and the requirement for change to wait for 2 years post Gazetting (s69R of the principal Act) (clauses 5 and 6).
b) We support the inclusion of timeframes (for the implementation of measures to mitigate risks) in Water Safety Plans (s69Z of the principal Act) (clause 8).
c) Hauora Tairāwhiti does not support all the amendments in clause 9. d) We believe that the repeal of section of 69KZ (2) (b) is premature. The Havelock Inquiry Stage
2 report found that “the question of accreditation should be reviewed, but once the questions of structure, employment, accountability and qualifications are resolved” (para 563, Report of the Havelock North Drinking Water Inquiry: Stage 2). We further note that the IANZ accreditation underpins the quality systems, technical training and support, and improved consistency amongst drinking-water assessors linked under the Central North Island Drinking Water Assessment Unit (CINDWAU). Hauora Tairāwhiti further suggests that, If IANZ is
82

discontinued as a consequence of a review, then a fit for purpose, and adequately resourced and mandated framework must replace it. Such a quality assurance framework could support all the regulatory activities of Public Health Units.
83