Aetiology,pathophysiology and diagnosis of dengue infection
40
AETIOLOGY,PATHOPHYSIOLOGY AND AETIOLOGY,PATHOPHYSIOLOGY AND DIAGNOSIS OF DENGUE INFECTION DIAGNOSIS OF DENGUE INFECTION DR LEE OI WAH DR LEE OI WAH PEG. PERUBATAN UD54 PEG. PERUBATAN UD54
-
Upload
lee-oi-wah -
Category
Health & Medicine
-
view
16.409 -
download
0
Transcript of Aetiology,pathophysiology and diagnosis of dengue infection

AETIOLOGY,PATHOPHYSIOLOGY AND AETIOLOGY,PATHOPHYSIOLOGY AND DIAGNOSIS OF DENGUE INFECTIONDIAGNOSIS OF DENGUE INFECTION
DR LEE OI WAHDR LEE OI WAH
PEG. PERUBATAN UD54PEG. PERUBATAN UD54

Dengue VirusDengue Virus
Causes dengue and dengue hemorrhagic feverCauses dengue and dengue hemorrhagic fever Is an arbovirusIs an arbovirus Transmitted by mosquitoesTransmitted by mosquitoes Composed of single-stranded RNAComposed of single-stranded RNA Has 4 serotypes (DEN-1, 2, 3, 4)Has 4 serotypes (DEN-1, 2, 3, 4)

Dengue VirusesDengue Viruses
Each serotype provides specific lifetime Each serotype provides specific lifetime immunity, and short-term cross-immunityimmunity, and short-term cross-immunity
All serotypes can cause severe and fatal All serotypes can cause severe and fatal diseasedisease
Genetic variation within serotypesGenetic variation within serotypes Some genetic variants within each serotype Some genetic variants within each serotype
appear to be more virulent or have greater appear to be more virulent or have greater epidemic potentialepidemic potential

4
1
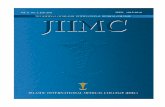
Circulating Dengue Virus Serotype : 1992-2007
0
10
20
30
40
50
60
70
80
90
100
DEN 1 DEN 2 DEN 3 DEN 4
DEN 1 3.7 0 4.8 14.7 48.7 63.5 44.4 28.2 9.3 5.4 29.8 46.9 73.4 58.6 33 30
DEN 2 8.6 4.1 9.5 29.5 48.7 33.4 51.9 69.2 58.1 39.2 23.8 20.6 7.4 8.4 36.4 53
DEN 3 83.7 93.1 84.1 54.6 2.6 2.1 3.7 2.7 32.6 50 33.3 27.8 14.6 17.1 19.3 11
DEN 4 4 2.8 1.6 1.2 0 0 0 0 0 5.4 13.1 4.7 4.6 1.2 4.5 6
1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007

Serotype Surveilan Di Ng Perak 2002 - 2007
YearYear No of No of Samples Samples Type 1Type 1 Type 2Type 2 Type 3Type 3 Type 4Type 4
20022002 113113 00 11 11 22
20032003 2222 00 00 00 00
20042004 88 00 11 00 00
20052005 250250 44 11 33 22
20062006 160160 44 00 44 11
20072007 243243 99 1919 77 00
TotalTotal 796796 1717 2222 1515 55

DENGUE VECTORS
Aedes aegypti Aedes albopictus

Larva
Pupa
1 - 2 Days
1 - 3 Days
6 - 8 Days
2 - 3 Days
Water
LIFE CYCLE OF THE AEDESLIFE CYCLE OF THE AEDES
Adult
Eggs Hatch 1- 48 hrs
Complete cycle 9 – 10 days

DENGUE TRANSMISSIONDENGUE TRANSMISSION
Infected Person Susceptible Person
Mosquito BiteInfected
Mosquito
Infected Mosquito
Bites next person
Becomes Sick
Mosquito Bite Infected
Mosquito
3 – 14 days laterRemains viremic
2 to 10 Days 8 – 12 DAYS

Manifestations of the dengue Manifestations of the dengue syndromesyndrome
Asymptomatic
Undifferentiatedfever
No h'rage Unusualhemorrhage
Dengue Fever
DHF I & II DSS
Dengue Hemorrhagic Fever(plasma leakage)
Symptomatic
Dengue virusInfection

Fever lasting 2-7 days, occasionally biphasic
Bleeding tendencies
Thrombocytopenia (100,000/mm3 or less)
Evidence of plasma leakage: Haemoconcentration (20% above baseline)
A drop in haematocrit following fluid replacement Pleural effusion, ascites (not obvious in early stage of critical phase), circulatory disturbances.
Hypovolemic shock
Dengue Haemorrhagic Fever (WHO 1997)

Dengue Shock Syndrome (WHO 1997)
All the above 4 criteria for DHF, plus evidence of circulatory failure:
rapid and weak pulsenarrow pulse pressure less than 20mmHgor hypotension for agecold clammy skin and restlessness

WHO grading of DHF/DSS (WHO WHO grading of DHF/DSS (WHO 19971997))
Grade 1In the presence of haemoconcentration, fever and symptoms, a positive TTGrade 2spontaneous bleeding in addition to the manifestation from Grade 2Grade 3*circulatory failure, pulse pressure less than 20 mmHg but systolic pressure normalGrade 4*profound shock, hypotension or unrecordable blood pressure.
Simplification:Grade 1 & 2: Non-shock DHFGrade 3: COMPENSATED shockGrade 4: DECOMPENSATED shock #

Dengue Case ClassificationDengue Case Classification
13Dengue Perak 5/2010

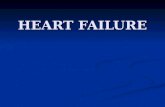
PATHOPHYSIOLOGY OF DENGUE PATHOPHYSIOLOGY OF DENGUE INFECTIONINFECTION







Deferversence
24-48 hours





Recognition of onset of reabsorption Recognition of onset of reabsorption phase is also important because i.v fluid phase is also important because i.v fluid regime needs to be progressively reduced/ regime needs to be progressively reduced/ discontinued at this stage.discontinued at this stage.




Thrombocytopenia



12011010090807060
Blood pressure, pulse pressure, heart rate in hypovolemic shock
Time LCS Lum
Compensated shock Decompensated shock
First sign of shock is tachycardiaFollowed by increasing diastolic BP
Drop is systolic BP is relatively late event
PR

DIAGNOSIS OF DF OR DHFDIAGNOSIS OF DF OR DHF

Important points to evaluate:Important points to evaluate:
History:History:date of onset of fever/ illnessdate of onset of fever/ illnessnausea, vomiting, abdominal pain, diarrhoea nausea, vomiting, abdominal pain, diarrhoea bleeding tendencybleeding tendencychange in mental state/seizure/dizzinesschange in mental state/seizure/dizzinessurine output (frequency, volume and time of last voiding)urine output (frequency, volume and time of last voiding)other important relevant histories:other important relevant histories:
family or neighbourhood history of denguefamily or neighbourhood history of denguejungle trekking and swimming in waterfall (consider leptospirosis, jungle trekking and swimming in waterfall (consider leptospirosis,
typhus, malaria)typhus, malaria)travellingtravellingrecent unprotected sexual or drug use behaviour (consider acute recent unprotected sexual or drug use behaviour (consider acute
HIV seroconversion illness)HIV seroconversion illness)
co-morbidities (consider sepsis in patients with diabetesco-morbidities (consider sepsis in patients with diabetes mellitus) mellitus)

Physical examination: Physical examination:
Assess mental state and GCS scoreAssess mental state and GCS score Assess haemodynamic status Assess haemodynamic status
Cold/ warm extremitiesCold/ warm extremities
Capillary filling time (normal < 2 seconds); Capillary filling time (normal < 2 seconds);
Pulse rate and Pulse volumePulse rate and Pulse volume
Blood pressure and Pulse pressureBlood pressure and Pulse pressure
Look out for tachypnoea/ acidotic breathing/ pleural effusionLook out for tachypnoea/ acidotic breathing/ pleural effusion Check for abdominal tenderness/ hepatomegaly/ ascitesCheck for abdominal tenderness/ hepatomegaly/ ascites Examine for bleeding manifestationExamine for bleeding manifestation Tourniquet test (repeat if previously negative or if there is Tourniquet test (repeat if previously negative or if there is
no bleeding manifestation) no bleeding manifestation)

Investigations:Investigations:
FBC & HCT FBC & HCT Renal and liver function testsRenal and liver function tests INR & APTTINR & APTT Dengue serologyDengue serology BFMPBFMP Other relevent tests Other relevent tests

After clinical assessmentAfter clinical assessment1.1. Day…….feverDay…….fever2.2. Temp chart – Febrile phase / Temp chart – Febrile phase / Critical phaseCritical phase
Hours of defervescenceHours of defervescence3.3. Alarm signalsAlarm signals – Yes/No – Yes/No
Abdominal pain and vomiting / Restlessness / Cold and Abdominal pain and vomiting / Restlessness / Cold and clammy extrimities / Altered conscious level / A sudden clammy extrimities / Altered conscious level / A sudden change from fever to hypothermiachange from fever to hypothermia
4.4. Bleeding tendencyBleeding tendency – Yes/No – Yes/No5.5. Evidence of plasma leakageEvidence of plasma leakage – Yes/No – Yes/No
Pleural effusion / AscitesPleural effusion / Ascites Hemodynamic instability - INCLUDING Hemodynamic instability - INCLUDING
TACHYCARDIA (PR>90)TACHYCARDIA (PR>90) Increase in HCTIncrease in HCT

Diagnosis :Diagnosis :
Dengue Haemorrhagic FeverDengue Haemorrhagic Fever D6 illnessD6 illness Deferversence 12 hoursDeferversence 12 hours With right pleural effusion and ascitesWith right pleural effusion and ascites Clinically no alarming signs / bleedingClinically no alarming signs / bleeding
(EXAMPLE)(EXAMPLE)