Aesthetic Surgery Journal ......body contouring, massive weight loss, abdominoplasty, monsplasty...
10
http://aes.sagepub.com/ Aesthetic Surgery Journal http://aes.sagepub.com/content/32/7/877 The online version of this article can be found at: DOI: 10.1177/1090820X12455498 2012 32: 877 Aesthetic Surgery Journal Jacob M. P. Bloom, Emily Van Kouwenberg, Michael Davenport, Peter F. Koltz, Robert B. Shaw, Jr. and Jeffrey A. Gusenoff Aesthetic and Functional Satisfaction After Monsplasty in the Massive Weight Loss Population Published by: http://www.sagepublications.com On behalf of: American Society for Aesthetic Plastic Surgery can be found at: Aesthetic Surgery Journal Additional services and information for http://aes.sagepub.com/cgi/alerts Email Alerts: http://aes.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: What is This? - Aug 31, 2012 Version of Record >> at APRSSA on September 16, 2012 aes.sagepub.com Downloaded from
Transcript of Aesthetic Surgery Journal ......body contouring, massive weight loss, abdominoplasty, monsplasty...

http://aes.sagepub.com/Aesthetic Surgery Journal
http://aes.sagepub.com/content/32/7/877The online version of this article can be found at:
DOI: 10.1177/1090820X12455498
2012 32: 877Aesthetic Surgery JournalJacob M. P. Bloom, Emily Van Kouwenberg, Michael Davenport, Peter F. Koltz, Robert B. Shaw, Jr. and Jeffrey A. Gusenoff
Aesthetic and Functional Satisfaction After Monsplasty in the Massive Weight Loss Population
Published by:
http://www.sagepublications.com
On behalf of:
American Society for Aesthetic Plastic Surgery
can be found at:Aesthetic Surgery JournalAdditional services and information for
http://aes.sagepub.com/cgi/alertsEmail Alerts:
http://aes.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Aug 31, 2012Version of Record >>
at APRSSA on September 16, 2012aes.sagepub.comDownloaded from

Body Contouring
Aesthetic Surgery Journal32(7) 877 –885© 2012 The American Society for Aesthetic Plastic Surgery, Inc.Reprints and permission: http://www .sagepub.com/journalsPermissions.navDOI: 10.1177/1090820X12455498www.aestheticsurgeryjournal.com
The mons region is often affected by massive weight loss (MWL), with descent of the pubic area due to skin laxity and fullness due to residual adiposity. Aside from having a poor cosmetic appearance, pubic functionality can also be compromised, with difficulty in maintaining hygiene or altered sexual function. Since one of the most common procedures performed after MWL is abdominal contour-ing, either by panniculectomy or abdominoplasty, the monsplasty has become an integral part of body contour-ing procedures.1
Thinning of the mons region provides a smooth contour at the transition point from the abdomen to the pubic region. Resuspension allows for elimination of excess
Aesthetic and Functional Satisfaction After Monsplasty in the Massive Weight Loss Population
Jacob M. P. Bloom, MD, MS; Emily Van Kouwenberg, BS; Michael Davenport; Peter F. Koltz, MD; Robert B. Shaw Jr., MD; and Jeffrey A. Gusenoff, MD
AbstractBackground: The mons region is often affected by massive weight loss (MWL), with descent of the pubic area and residual adiposity. Thinning and resuspension are often performed concomitantly with abdominal contouring procedures.Objectives: Assess patient satisfaction, as well as functional and aesthetic results, after monsplasty in the MWL population.Methods: The authors identified 54 consecutive female MWL patients (≥50 lbs) who had undergone abdominal contouring and completed at least 3 months of follow-up as potential subjects. Subjects were asked to complete a Mons Satisfaction Survey, either by phone or in person. Demographic and procedural data were collected from our prospective registry. Descriptive statistics were calculated with significance set at P value <.05.Results: Thirty-one patients (57.8%) completed the survey. Average patient age was 46 ± 11.3 years. Mean maximum body mass index (BMI) was 52.0 ± 8.81 kg/m2, mean current BMI was 31.0 ± 6.22 kg/m2, and mean delta BMI was 20.7 ± 6.00 kg/m2. Average pannus resection weight was 3.25 ± 2.03 kg. Visualization of the genitalia improved from 25.8% to 100% (P < .01). Patients rated the appearance of their mons as 3.18 ± 2.11 prior to surgery and 8.58 ± 1.73 after surgery (P < .001) on a scale of 1 to 10. Hygiene improved in 61.3% of patients, and sex life improved in 51.6%, with 32.3% of patients reporting increased genital sensitivity. Incontinence decreased from 22.6% to 12.9%, and 6 patients reported a change in urinary stream.Conclusions: Monsplasty at the time of abdominal contouring yields significant improvement in patient satisfaction levels and functional scores. With proper incisional design, monsplasty can be performed safely during abdominal contouring with high patient satisfaction to improve both form and function of the pubic region.
Level of Evidence: 4
Keywordsbody contouring, massive weight loss, abdominoplasty, monsplasty
Accepted for publication April 24, 2012.
Dr Bloom is a resident, Ms Van Kouwenberg is a medical student, Mr Davenport is a research intern, Dr Koltz is a resident, and Dr Shaw is a former resident in the Division of Plastic Surgery, University of Rochester Medical Center, Rochester, New York. Dr Gusenoff is an attending physician in the Department of Plastic Surgery, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania.
Corresponding Author:Dr Jeffrey A. Gusenoff, Department of Plastic Surgery, University of Pittsburgh Medical Center, 3380 Boulevard of the Allies, Suite 180, Pittsburgh, PA 15213, USA. E-mail: [email protected]
at APRSSA on September 16, 2012aes.sagepub.comDownloaded from

878 Aesthetic Surgery Journal 32(7)
hooding of the genital region and restores a youthful con-tour. Variations in the monsplasty technique have been described in the literature; however outcomes, including patient satisfaction, have not been measured.1-5
Neglecting to treat the mons area during abdominal contouring may leave the patient with residual contour irregularities, ultimately affecting the aesthetic or func-tional result. We investigated whether there were signifi-cant improvements in patient satisfaction, functional outcomes, and aesthetic results in women who underwent abdominal contouring surgery with monsplasty after MWL.
MEthOds
We selected 54 consecutive female MWL patients (≥50 lbs) who had undergone either abdominoplasty or panniculec-tomy at the University of Rochester Life After Weight Loss Program as potential subjects for this study. All patients were retrospectively recruited from our registry database, as approved by the Institutional Research Studies Review Board at the University of Rochester.
Of the 54 potential patients, 31 completed the survey. Of the 23 patients who did not participate, 12 declined participation, 10 were unreachable by phone, and 1 patient placed us on the “Do not call” list. We did not have an opportunity to inquire about the reasoning behind the declined participation for the 12 patients who elected not to complete the survey. Each patient who did respond was surveyed after a postoperative period of at least 3 months. All potential subjects were asked to complete a 15-question Mons Satisfaction Survey by phone or at routine follow-up. This survey was created by the PI and lead author. It is not a validated tool nor had it been used previously. The initial questions on the survey assessed patients’ preopera-tive and postoperative satisfaction with the aesthetic appearance of their mons region. Satisfaction scores were rated using a 10-point Likert scale (0 = very unsatisfied, 5 = neutral, and 10 = very satisfied). The remaining sur-vey questions sought to identify functional changes after monsplasty. Additional demographic and procedural data were collected from the database, including patient age, body mass index (BMI), and pannus resection weight. Body mass indices were defined as maximum BMI, current BMI, and delta BMI (maximum − current BMI).
Our technique for monsplasty has been described previ-ously.2,6 In the preoperative area, with the patient lying supine, the lower abdominal incision was marked. With the tissues at maximal upward stretch, the incision for the lower margin of resection was placed 6 cm above the ante-rior vulvar commissure. To properly reapproximate the pubic hairline, the incision was designed to fall just above
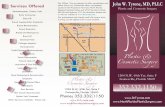
the pubic symphysis and, if needed, could be extended past 6 cm. The patient was then asked to stand, and the rest of the abdominal markings were completed. Guided by the aforementioned markings, a wedge resection of adipose tissue (Figure 1A) was excised to the level of the pubic symphysis and performed as appropriate to achieve a similar thickness to the upper abdominal flap (Figure 1B,C). By staying cephalad to the pubic symphysis, injury to the genital anatomy was avoided. The mons was then resuspended to the abdominal wall fascia using 3 horizon-tal mattress 2-0 Vicryl sutures (Ethicon, Inc, Somerville, New Jersey) placed in the deep layers of the mons super-ficial fascial system (SFS), which is contiguous with the deep Scarpa’s fascia layer (Figure 1D,E).
Statistics
Pre- and postoperative (body contouring) functional out-comes ratings were compared using Student t test and χ2 tests as appropriate. A multiple regression was carried out to examine the association between body mass indices and resection weight as predictors for improvement in Mons Satisfaction Survey scores. Linear regressions were per-formed to individually examine whether maximum BMI, current BMI, delta BMI, and resection weight predicted improvement in patient satisfaction of the mons area. This analysis was performed using the statistical software SPSS, version 17.0 (IBM, Inc, an IBM Company, Chicago, Illinois). Statistical significance was set at a P value of <.05.
REsuLts
Thirty-one of 54 patients (57.8%) completed the Mons Satisfaction Survey. Average patient age was 46 ± 11.3 years. Mean maximum BMI was 52.0 ± 8.81 kg/m2, mean current BMI was 31.0 ± 6.22 kg/m2, and mean delta was BMI 20.7 ± 6.00 kg/m2. Average pannus resection weight was 3.25 ± 2.03 kg. Just over half of the patients (51.6%) underwent abdominoplasty, whereas 48.4% had a pan-niculectomy (Table 1). Prior to surgery, 25.8% of respond-ents reported that they had been able to see their genital region, compared with 100% postoperatively (P < .01). Patients rated the appearance of their mons as 3.18 ± 2.11 prior to surgery and 8.58 ± 1.73 after surgery (P < .001). Hygiene was problematic for 48.4% of patients but improved in 61.3% of patients following surgery. Sex life improved for 51.6% of patients; however, 32.3% reported not being sexually active. Approximately one-third of patients (32.3%) reported an increase in genital sensitiv-ity, while 67.7% had no change. Most patients (77.4%)
A poster version of this manuscript was presented at the American Association of Plastic Surgeons 90th Annual Meeting and Symposium, Boca Raton, Florida, April 2011. This paper was also presented at the American Society for Aesthetic Plastic Surgery (ASAPS) annual Aesthetic Meeting, Boston, Massachusetts, May 2011.
at APRSSA on September 16, 2012aes.sagepub.comDownloaded from

Bloom et al 879
Figure 1. (A) A wedge resection of adipose tissue is planned after completion of rectus plication. (B, C) Excision is carried out to the level of the pubic symphysis and performed as appropriate to achieve a similar thickness to the upper abdominal flap. (D, E) The mons is then resuspended to the abdominal wall fascia using 3 horizontal mattress 2-0 Vicryl sutures placed in the deep layers of the mons superficial fascial system, which is contiguous with the deep Scarpa’s fascia layer.
at APRSSA on September 16, 2012aes.sagepub.comDownloaded from

880 Aesthetic Surgery Journal 32(7)
reported the current position of their mons pubis to be at the right level; 9.7% of patients thought it was positioned too high and 12.9% were unsure of its new position. Rates of bladder incontinence were reported to decrease from 22.6% to 12.9%; however, this was not significantly differ-ent (P = .319). Six patients (19.4%) reported a change in their urinary stream, and only 1 of these patients identi-fied this as problematic (she felt that it was difficult to control the direction of her urine). Of the 6 patients who identified a change in urinary stream, 5 stated their stream was more horizontal. Two patients (6.5%) reported inci-sional or pubic pain after surgery. Nearly all of the patients (96.8%) reported that they would both undergo this pro-cedure again and recommend it to a friend.
The multiple regression analysis assessing the effect of body mass indices and pannus resection weight on change in patient satisfaction was not significant. Mons satisfac-tion scores are not predicted by maximum BMI, current BMI, delta BMI, or pannus weight. In addition, linear
Table 1. Mons Satisfaction Survey Results (N = 31)
No. (%) or Mean ± SD P Value
Surgical procedure
Abdominoplasty 16 (51.6)
Panniculectomy 15 (48.4)
Mons Satisfaction Survey score
Prior to surgery 3.18 ± 2.11 <.001a
After surgery 8.58 ± 1.73
Visualize genitalia before surgery?
Yes 8 (25.8) <.001b
No 23 (74.2)
Visualize genitalia after surgery?
Yes 31 (100)
No 0
Position of genital region
Too high 3 (9.7)
Too low 0
At the right level 24 (77.4)
Not sure 4 (12.9)
Problems with hygiene before surgery?
Yes 15 (48.4)
No 16 (51.6)
Improvement in hygiene after surgery?
Yes 19 (61.3)
No 12 (38.7)
Improved sex life since surgery?
Yes 16 (51.6)
No 5 (16.1)
Not sexually active 10 (32.3)
Change in genital sensitivity?
Yes 10 (32.3)
No 21 (67.7)
Urinary incontinence before surgery?
Yes 7 (22.6) .319b
No 24 (77.4)
No. (%) or Mean ± SD P Value
Urinary incontinence after surgery?
Yes 4 (12.9)
No 27 (87.1)
Change in urinary stream after surgery?
Yes 6 (19.4)
No 25 (80.6)
If yes, is it problematic? (n = 6)
Yes 1 (16.7)
No 5 (83.3)
Experience pubic pain?
Yes 2 (6.5)
No 29 (93.5)
Undergo procedure again?
Yes 30 (96.8)
No 0
Not sure 1 (3.2)
Recommend this procedure to a friend?
Yes 30 (96.8)
No 1 (3.2)
aStudent t test.bχ2 test.
(continued)
Table 1. (continued)
at APRSSA on September 16, 2012aes.sagepub.comDownloaded from

Bloom et al 881
regressions show that patients’ maximum BMI (P = .57), current BMI (P = .88), delta BMI (P = .47), and pannus resection weight (P = .51) were not predictive of change in Mons Satisfaction Survey scores (see Table 2).
Representative cases of the highest and lowest monsplasty satisfaction score results are presented in Figures 2 to 5.
disCussiOn
As the number of patients undergoing body contouring pro-cedures after MWL grows, further outcomes data on new or established techniques are necessary to optimize patient safety and aid in patient education. We demonstrate that monsplasty, which is frequently performed during abdomi-nal contouring procedures, improves patient satisfaction and functional outcomes in this population. The low abdominal incision allows direct access to the mons area for appropriate contouring, so it matches the thickness of the upper abdom-inal wall and also allows direct removal of excess skin. Although many techniques have been described in the litera-ture, most improvements in satisfaction and functionality have been reported anecdotally.1-5
Prior to beginning our study, we placed permanent Ethibond sutures (Ethicon, Inc, Somerville, New Jersey) to secure the pubic region to the abdominal wall. A few patients developed problematic suture granulomas, so this technique was abandoned. Of note, we observed similar problems when placing this suture material in the axilla for brachioplasty or the groin for thighplasty procedures. One patient required a return to the operating room to remove a sinus tract which had formed from the skin to the underlying permanent suture material. Several other patients had delayed suture extrusion several months after the procedure. Replacement of these sutures with Vicryl material has eliminated this complication and has not altered the long-term results of the monsplasty procedure. A head-to-head comparison of the 2 suture materi-als has not been performed due to the small number of patients in whom we placed Ethibond initially.
On the basis of the statistical analysis, we were unable to identify which factors influenced satisfaction scores. The multiple regression analysis assessing the effect of body mass indices, pannus resection weight, maximum BMI, current BMI, and delta BMI did not reveal any sig-nificant influence on satisfaction scores. Perhaps by increasing our patient population, we could have achieved
Figure 2. (A) This 43-year-old woman presented with a chief complaint of skin laxity after a 90-lb weight loss following gastric bypass surgery. (B) Three months after abdominoplasty, upper body lift, and medial thigh lift, the patient reported an increase in Mons Satisfaction Survey score from 1 to 10.
at APRSSA on September 16, 2012aes.sagepub.comDownloaded from

882 Aesthetic Surgery Journal 32(7)
a more robust statistical analysis, which might have helped us to determine the factors influencing satisfaction or dissatisfaction. Another limiting factor of our study is that it lacks a control group. Ongoing investigation will focus on assessing satisfaction scores in patients who undergo abdominal contouring surgery without concomi-tant monsplasty.
Correct placement of the lower abdominal incision is critical to obtaining an optimal result. In our study, 77.4% of patients believed that their pubic region was repositioned at the right level. Approximately 1 of 10 patients thought that their genital region was raised too high as a result of their monsplasty. We typically rely on our own intraopera-tive judgment to determine where the tacking sutures should be placed to resuspend the mons region. The thick tissues of the SFS are held up to an area at or slightly above the pubic symphysis and the contour is assessed; the sur-geon is careful to not expose the clitoral hood. The final resting position of the mons region is likely also influenced by the balance of opposing forces occurring at the incision line. There is no obvious explanation for why almost 10% of our patients thought that the final position of the pubic area was “too high.” This subjective self-evaluation may be
influenced by a number of factors. Of note, in this small group (n = 3), the average patient satisfaction score was 6, as compared with 8.58 in the rest of the group. Further studies will aim to add objective measures to the subjective grading system, such as a postoperative measurement from the vulvar commissure to the superior border of the hairline and from the umbilicus to the pubic hairline. In addition, we have found that it is easier to overcorrect thinner patients undergoing body contouring. Each of the patients reporting a high pubic region had a BMI of 31 or lower at the time of body contouring surgery, which may have played a role in the final aesthetic result. The work by Seitz et al7 in defining the proportions of the mons region as a subunit to help intraoperative redraping of this area may someday aid in further guiding surgeons with optimizing the aesthetics of the mons region.
Patients’ changing perceptions of the appearance of the mons region were accompanied by many functional improvements as well. All patients were able to visualize their genitalia postoperatively, representing a 75% increase in the number of patients who were able to do so. In addi-tion, over half of the patients experienced improvements in hygiene and sex life. Again, although the urinary stream
Figure 3. (A) This 35-year-old woman presented with a chief complaint of bilateral macromastia and symptomatic pannus after a 161-lb weight loss following gastric bypass surgery. (B) Three months after panniculectomy and mammaplasty reduction, the patient reported an increase in Mons Satisfaction Survey score from 1 to 10.
at APRSSA on September 16, 2012aes.sagepub.comDownloaded from

Bloom et al 883
was altered in some patients, this was largely not prob-lematic in our study. A prior report by Michaels et al4 examined over 400 MWL patients and noted that this was a potential complication but did not quantify the inci-dence in their patient population. Patients also reported improvements in bladder incontinence; however, the change was not statistically significant. Although we do not have an explanation for this improvement, we hypoth-esize that it may be related to other factors such as con-comitant abdominal wall plication. Future studies will investigate how these factors influence changes in blad-der incontinence.
Multiple methods of approaching the mons region in the MWL patient have been described in the literature. The Pittsburgh Rating Scale is a validated tool for assess-ment of and treatment planning for mons ptosis and full-ness after MWL.8 Although authors have cited different combinations of liposuction and fat excision, it is univer-sally recognized that resuspension using the SFS is imper-ative in achieving long-lasting results and improving both early and late wound healing.1-6 Liposuction may be used to thin the thick fibrofatty tissue of the mons region, but we have not utilized this technique.2,3 Liposuction has
been theorized to contribute to genital lymphedema in this region, especially if it is carried into the inguinal area.2 Although edema usually resolves after direct excision, we did not directly ask our patients if they felt they had residual edema from the procedure. There may still be a role for liposuction in patients who have undergone a monsplasty procedure with inadequate tissue resection.
Concomitant procedures in body contouring after MWL are common. When monsplasty is combined with a medial thighlift, preoperative marks are placed 4 cm from the midline to define the border of the mons region and keep the scar off the thigh.1 The lipectomy, completed while thinning the mons region, does not usually extend past these borders during our standard monsplasty. This allows us to combine these procedures safely. All dissec-tion performed lateral to the mons region over the femoral region is kept superficial in the subdermal plane to avoid damage to the lymphatics.
Body mass indices and pannus resection weights were not predictors of satisfaction scores in our population. It is possible that with a larger sample size, these variables would have become more significant. Our study is limited by the subjective nature of the responses from our surveyed
Figure 4. (A) This 63-year-old woman presented with a chief complaint of skin laxity after a 172-lb weight loss following gastric bypass surgery. (B) Three months after fleur-de-lis abdominoplasty, brachioplasty, and mastopexy, the patient reported a minimal increase in Mons Satisfaction Survey score from 5.5 to 6.5.
at APRSSA on September 16, 2012aes.sagepub.comDownloaded from

884 Aesthetic Surgery Journal 32(7)
patients. Unfortunately, we were unable to establish full participation of our identified patient population. However, the opinions expressed by our patients in this study consistently displayed improvements in both aes-thetic and functional properties after monsplasty. Another limitation is that each monsplasty is carried out with slight variations in technique. The difference in the thickness of the upper flap as compared with the mons region dic-tates how much thinning is undertaken. Future long-term
follow-up is warranted to examine the durability of the monsplasty technique. In addition, we plan on examining similar functional and aesthetic outcome measures in our male population.
COnCLusiOns
With proper incisional design, monsplasty can be per-formed safely during abdominal contouring with a high rate of patient satisfaction to improve both form and func-tion of the pubic region.
disclosures
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
Figure 5. (A) This 32-year-old woman presented with a chief complaint of symptomatic pannus after an 87-lb weight loss following gastric bypass surgery. (B) Three and a half months after panniculectomy, the patient reported a minimal increase in Mons Satisfaction Survey score from 1 to 5, citing that her pubic hairline was too high.
Table 2. Linear Regressions: Evaluation of Predictors of Change in Patient Satisfaction
β t(29) R2 F(1, 29) P Value
Max BMI .11 .58 .01 .34 .57
Current BMI .03 .17 .00 .02 .88
Delta BMI .14 .74 .02 .55 .47
Pannus resection weight –.12 –.66 .02 .44 .51
BMI, body mass index.
at APRSSA on September 16, 2012aes.sagepub.comDownloaded from

Bloom et al 885
REFEREnCEs
1. Rubin P, Gusenoff J. Bodylifts and post massive weight loss body contouring. In: Chung KC, Disa JJ, Gosain AK, Kinney B, Rubin JP, eds. Plastic Surgery: Indications and Practice. Philadelphia, PA: Saunders; 2008:1627-1664.
2. Alter GJ. Management of the mons pubis and labia majora in the massive weight loss patient. Aesthetic Surg J. 2009;29(5):432-442.
3. El-Khatib HA. Mons pubis ptosis: classification and strat-egy for treatment. Aesthetic Plast Surg. 2011;35(1):24-30.
4. Michaels J 5th, Friedman T, Coon D, Rubin JP. Mons rejuvenation in the massive weight loss patient using superficial fascial system suspension. Plast Reconstr Surg. 2010;126(1):45e-46e.
5. Matarasso A, Wallach SG. Abdominal contour surgery: treating all aesthetic units, including the mons pubis. Aesthetic Surg J. 2001;21(2):111-119.
6. Lockwood T. Lower body lift with superficial fascial sys-tem suspension. Plast Reconstr Surg. 1993;92(6):1112-1122; discussion 1123-1125.
7. Seitz IA, Wu C, Retzlaff K, Zachary L. Measurements and aesthetics of the mons pubis in normal weight females. Plast Reconstr Surg. 2010;126(1):46e-48e.
8. Song AY, Jean RD, Hurwitz DJ, Fernstrom MH, Scott JA, Rubin JP. A classification of contour deformities after bariatric weight loss: the Pittsburgh Rating Scale. Plast Reconstr Surg. 2005;116(5):1535-1544; discussion 1545-1546.
at APRSSA on September 16, 2012aes.sagepub.comDownloaded from