
Adverse Food Reactions Reactions Immunologic
15
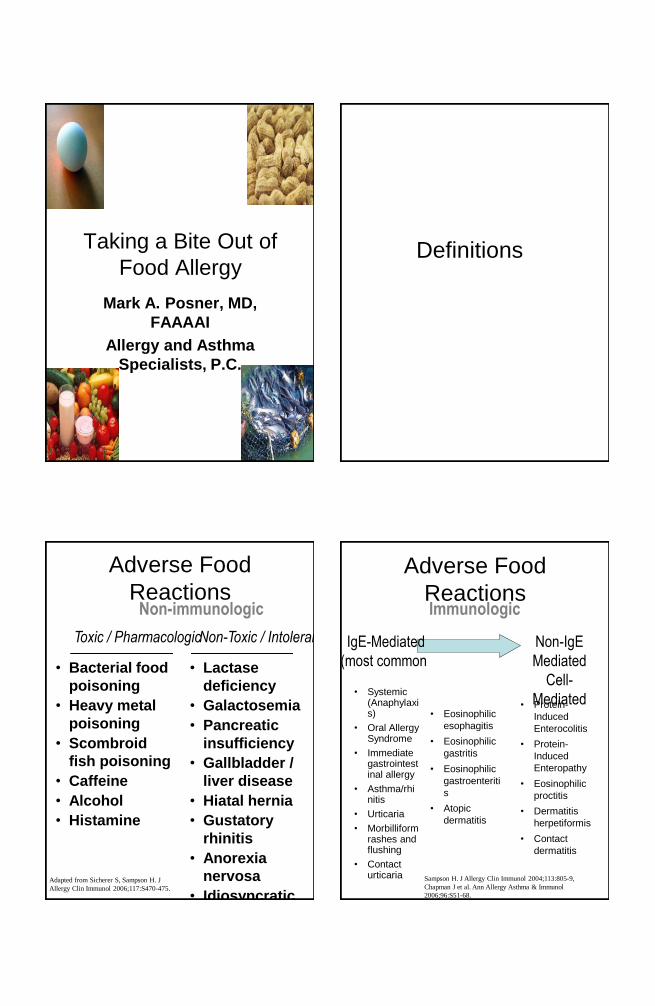
Taking a Bite Out of Food Allergy Mark A. Posner, MD, FAAAAI Allergy and Asthma Specialists, P.C. Definitions Adverse Food Reactions Toxic / Pharmacologic Non-Toxic / Intoleran • Bacterial food poisoning • Heavy metal poisoning • Scombroid fish poisoning • Caffeine • Alcohol • Histamine Non-immunologic • Lactase deficiency • Galactosemia • Pancreatic insufficiency • Gallbladder / liver disease • Hiatal hernia • Gustatory rhinitis • Anorexia nervosa • Idiosyncratic Adapted from Sicherer S, Sampson H. J Allergy Clin Immunol 2006;117:S470-475. • Eosinophilic esophagitis • Eosinophilic gastritis • Eosinophilic gastroenteriti s • Atopic dermatitis Adverse Food Reactions IgE-Mediated (most common) Non-IgE Mediated Cell- Mediated Immunologic • Systemic (Anaphylaxi s) • Oral Allergy Syndrome • Immediate gastrointest inal allergy • Asthma/rhi nitis • Urticaria • Morbilliform rashes and flushing • Contact urticaria • Protein- Induced Enterocolitis • Protein- Induced Enteropathy • Eosinophilic proctitis • Dermatitis herpetiformis • Contact dermatitis Sampson H. J Allergy Clin Immunol 2004;113:805-9, Chapman J et al. Ann Allergy Asthma & Immunol 2006;96:S51-68.
Transcript of Adverse Food Reactions Reactions Immunologic
Taking a Bite Out of
Food Allergy
Mark A. Posner, MD,
FAAAAI
Allergy and Asthma
Specialists, P.C.
Definitions
Adverse Food
Reactions
Toxic / Pharmacologic Non-Toxic / Intolerance
• Bacterial food
poisoning
• Heavy metal
poisoning
• Scombroid
fish poisoning
• Caffeine
• Alcohol
• Histamine
Non-immunologic
• Lactase
deficiency
• Galactosemia
• Pancreatic
insufficiency
• Gallbladder /
liver disease
• Hiatal hernia
• Gustatory
rhinitis
• Anorexia
nervosa
• Idiosyncratic
Adapted from Sicherer S, Sampson H. J
Allergy Clin Immunol 2006;117:S470-475.
• Eosinophilic
esophagitis
• Eosinophilic
gastritis
• Eosinophilic
gastroenteriti
s
• Atopic
dermatitis
Adverse Food
Reactions
IgE-Mediated
(most common)
Non-IgE
Mediated
Cell-
Mediated
Immunologic
• Systemic (Anaphylaxis)
• Oral Allergy Syndrome
• Immediate gastrointestinal allergy
• Asthma/rhinitis
• Urticaria
• Morbilliform rashes and flushing
• Contact urticaria
• Protein-
Induced
Enterocolitis
• Protein-
Induced
Enteropathy
• Eosinophilic
proctitis
• Dermatitis
herpetiformis
• Contact
dermatitis
Sampson H. J Allergy Clin Immunol 2004;113:805-9,
Chapman J et al. Ann Allergy Asthma & Immunol
2006;96:S51-68.

Pathophysiology
Allergens
• Proteins or glycoproteins (not fat or carbohydrate) – Generally heat resistant, acid
stable
• Major allergenic foods (>85% of food allergy)
– Children: milk, egg, soy, wheat,
peanut, tree nuts – Adults: peanut, tree nuts,
shellfish, fish, fruits and vegetables
CASE: Crustacean Allergy:
IgE Towards Protein in the
Food, NOT Iodine
• 79 year old man had anaphylaxis to
shrimp at age 20, 25
• Doctors told him he was allergic to iodine in seafood
• Avoided seafood, iodized salt for years
• Age 70: retirement dinner, hostess picked shrimp out of his portion and gave it to him --- ER visit for anaphylaxis
• At age 79, specific IgE measurement extremely high to shrimp: >100 kU/L
• On follow-up after education on avoidance, happily consuming foods with iodized salt because he didn’t have to screen salt source any more
Pan-allergens
• Proteins in food, pollen or plants that possess homologous IgE binding epitopes across species
• Tropomyosins: crustacea, dust mites, cockroach, mollusks
• Parvalbumins: fish
• Bovine IgG: beef, lamb, venison, cow’s milk
• Lipid transfer protein: fruits (peach, apple), vegetables, peanut, tree nuts
• Profilin: fruits, vegetables
• Class 1 chitinases: fruits, wheat, latex

Amino Acid Structural
Characteristics
• Allergenic proteins have been identified for common food allergens; genes have been cloned and sequenced for many of them
• Sequential vs conformational B
cell epitopes – IgE towards sequential epitopes
are associated with persistence of allergy
– Cross Reactivity: more likely if AA sequence homology >70%
IgE-Mediated
IgE-receptor
Histamine
Protein digestion
Antigen
processing
Some Ag enters
blood
Mast cell APC
B cell T cell
TNF-
IL-5
Non-IgE
Mediated
Immune Mechanisms
Risk Factors
Risk Factors for
Development of Food
Allergy
Local Factors
(Rodent
Models)
• Genetic
susceptibility
•Pepsin
digestion
•
Gastrointestin
al infections?
•
Malabsorption
Host
Factors
• Age (esp
neonates)
• Genetic
susceptibilit
y
• FHx of
atopy
• FHx of
food allergy
• Atopic
Chapman J et al. Ann Allergy Asthma & Immunol
2006;96:S51-68.

Food Allergy Disorders
Anaphylaxis Syndromes
• Food-induced anaphylaxis – Food allergy = #1 cause of
anaphylaxis in the ED
– Rapid-onset, up to 30% biphasic
– May be localized (single organ) or generalized
– Potentially fatal
– Any food, highest risk:
• peanut, tree nut, seafood (cow’s milk and egg in young children)
• Food-dependent, exercise-induced: 2 forms
– Specific foods (wheat, celery most common)
– Any food (post-prandial)
Fatal Food
Anaphylaxis
• Frequency: ~ 150 deaths / year
• Clinical features:
– Biphasic reaction can contribute –initially better, then recurs
– Cutaneous symptoms may not be present
– Respiratory symptoms prominent
• Risk factors:
– Underlying asthma – Delayed epinephrine
– Symptom denial – Previous severe reaction
– Adolescents, young adults
• History: known food allergen
• Key foods: peanuts and tree nuts dominate (~90% of fatalities), fish,crustaceans
• Most events occurred away from home
Bock SA, et al. J Allergy Clin Immunol
2001;107:191-3.
Cutaneous Reactions
• Acute urticaria/angioedema – common
• Contact urticaria - common
• Food allergy rarely causes chronic urticaria/angioedema
• 1/3 of children with moderate to severe atopic dermatitis may have food allergy (especially cow’s milk, egg, soy, wheat). Morbilliform rashes may be seen in these children upon food challenge.
• Contact dermatitis (food handlers)

Respiratory Responses
• Upper and lower respiratory
tract symptoms may be seen
(rhinoconjunctivitis, laryngeal
edema, asthma)
• Rarely isolated, usually
accompany skin and GI
symptoms
• Inhalational exposure may
cause respiratory symptoms
that can be severe • Occupational
• Restaurants
• Kitchen/Home Examp
le:
crabs
to be
boiled
Birch Apple, carrot, celery,
cherry, pear, hazelnut
Ragweed Banana, cucumber,
melons
Grass Melon, tomato, orange
Mugwort Melon, apple, peach,
cherry
Pollen-Food
Syndrome or Oral
Allergy Syndrome
• Clinical features: rapid onset oral
pruritus, rarely progressive
• Epidemiology: prior sensitization to
pollens
• Key foods: raw fruits and vegetables
• Allergens: Profilins and pathogenesis–
related proteins
– Heat labile (cooked food usually
OK)
• Cause: cross reactive proteins
pollen/food
Latex-Fruit
Syndrome
• 30-50% of those with latex allergy are sensitive to some fruits due to cross-reactive IgE
• Most common fruits: banana, avocado, kiwi, chestnut but other fruits and nuts have been reported
• Can clinically present as anaphylaxis to fruit
• Warn latex-sensitive patients of potential cross-reactivity
• Some fruit-allergic patients may be at risk for latex allergy
Enterocolitis Enteropathy Proctitis Age Onset: Infant Infant/Toddler Newborn Duration: 12-24 mo ? 12-24 mo 9 mo-12 mo Characteristics: Failure to thrive Malabsorption Bloody stools Shock Villous atrophy No systemic sx Lethargy Diarrhea Eosinophilic Vomit Diarrhea
Non-IgE-mediated, typically milk and soy
induced
Spectrum may include colic, constipation
and occult GI blood loss
Pediatric
Gastrointestinal
Syndromes
Fully reviewed in: Sicherer SH. Pediatrics
2003;111:1609-1616.

GI Syndromes of Children
and Adults:
Celiac Disease (Gluten-sensitive enteropathy) – In children:
• FTT, or weight loss
• Malabsorption, diarrhea, abdominal pain
• May be subtle
– In adults, average 10 years of nonspecific symptoms:
• Diarrhea, abdominal pain
• GERD
• Malabsorption
• May present atypically with osteoporosis, infertility, neurologic sx
Pathophysiology: an immune-mediated enteropathy triggered by gluten peptides in genetically predisposed patients (DQ2 or DQ8)
– Lymphocytic infiltration of small bowel
– Villus atrophy
Celiac Disease
(Gluten-sensitive
enteropathy) Cont’d: • Diagnosis
– ~1/133 people in US have celiac disease – many are currently undiagnosed
– IgA anti-tissue transglutaminase (IgG if IgA-deficient), anti-endomysial Ab, little role for anti-gliadin Ab currently due to poor specificity
– Upper endoscopy with biopsy; refer to gastroenterologist
• Management – Strict, lifelong, gluten avoidance
(wheat, barley, rye)
– Rare risk of GI lymphoma
– Oats almost always OK
– Link with resources: dietician, local support groups, national organizations (listed at www.celiac.nih.gov)
GI Syndromes of Children
and Adults
Gastrointestinal Anaphylaxis
or Immediate
Gastrointestinal Allergy
– IgE-mediated
– Acute
emesis/diarrhea/abdominal pain
– Can present without other signs
or symptoms of an allergic
reaction to food
GI Syndromes of Children
and Adults Eosinophilic Gastrointestinal
Disorders: eosinophilic esophagitis/gastritis/gastroenteritis
• Prevalence increasing, eosinophilic esophagitis is the most common syndrome, all rare in adults
• Symptoms
– Post-prandial N/V/D/abdominal pain, weight loss
– FTT in infants and young children, irritability, sleep disturbance
– GER, often refractory, may be seen
– In teens/adults: dysphagia, food impaction

Eosinophilic Gastrointestinal
Disorders: eosinophilic
esophagitis/gastritis/gastroente
ritis cont’d:
• Diagnosis
– Biopsy: eos infiltration (mucosa
serosa): >20/HPF
– Presence of eos doesn’t necessarily
invoke food allergy
– May affect esophagus to rectum
• Response to specific food elimination
found in a subset of patients
(especially eosinophilic esophagitis):
can screen for food allergy with
prick/in vitro IgE, patch testing with
food is currently under investigation
Prevalence and Natural
History
Prevalence of
Food Allergy
• Perception by public: 20-25%
• Confirmed allergy (oral challenge) – Adults: 2-3.5%
– Infants/young children: 6-8%
• Specific Allergens – Dependent upon societal eating and
cooking patterns
• Prevalence higher in those with: – Atopic dermatitis
– Certain pollen allergies
– Latex allergy
• Prevalence seems to be increasing
Estimated Prevalence of
Food Allergy
Food Children
(%)
Adults
(%)
Cow’s
milk
2.5 0.3
Egg 1.3 0.2
Soy 0.3-0.4 0.04
Peanut 0.8 0.6
Tree nut 0.2 0.5
Crustace
ans
0.1 2.0
Fish 0.1 0.4 Sampson H. J Allergy Clin
Immunol;113:805-19.

Prevalence of Clinical
Cross Reactivity Among
Food “Families”
Food Allergy
Prevalence of Allergy to
> 1 Food in Family
Fish 30% -100%
Tree Nut 15% - 40%
Grain 25%
Legume 5%
Any 11%
Sicherer SH. J Allergy Clin Immunol. 2001
Dec;108(6):881-90.
Natural History
• Dependent on food &
immunopathogenesis
• ~ 85% of cases of cow milk,
soy, egg and wheat allergy
remit by age 3 yrs
– Declining/low levels of
specific-IgE predictive
– IgE binding to conformational
epitopes predictive
• Non-IgE-mediated GI allergy
– Infant forms resolve in 1-3
years
– Toddler / adult forms more
persistent
Natural History
(cont’d) • Allergies to peanuts,
tree nuts, seafoods, and seeds typically persist
• ~20% of cases of peanut allergy resolve by age 5 years.
Prognostic factors include: – PST <6mm
– ≥2 years avoidance
– History of mild reaction
– Few other atopic diseases
– Low levels of peanut-specific IgE
– Rarely re-develop allergy: role for regular ingestion?
Evaluation

Evaluation of Food
Allergy • Suspect IgE-mediated
– Panels/broad screening should NOT be done without supporting history because of high rate of false positives.
– Prick skin tests (prick-prick with fresh food if pollen-food syndrome)
– In vitro tests for food-specific IgE
• Suspect non-IgE-mediated – Consider biopsy of gut, skin
• Suspect non-immune, consider: – Breath hydrogen
– Sweat test
– Endoscopy
Evaluation:
Interpretation of
Laboratory Tests
• Positive prick test or specific IgE – Indicates presence of IgE
antibody NOT clinical reactivity
– ~90% sensitivity
– ~50% specificity
– ~50% false positives
– Larger skin tests/higher IgE correlates with likelihood of reaction but not severity
• Negative prick test or specific IgE – Essentially excludes IgE
antibody (>95% specific)
Evaluation:
Elimination Diets & Food
Challenges
• Elimination diets (1 - 6 weeks) most useful for chronic disease (eg. AD, GI syndromes) – Eliminate suspected food(s)
or – Prescribe limited “eat only”
diet or – Elemental diet
• Oral challenge testing (MD supervised, emergency meds available) – Open – Single-blind – Double-blind, placebo-
controlled (DBPCFC) * Unless convincing history warrants supervised challenge
Diagnostic Approach: IgE-
Mediated Allergy
• If test for specific-IgE
antibody is
– Negative: reintroduce food*
– Positive: start elimination diet
• If elimination diet is
associated with
– No resolution: reintroduce
food*
– Resolution
• Open / single-blind
challenges to “screen”
• DBPCFC for equivocal open
challenges

Diagnostic Approach: Non-IgE-
Mediated Disease or those with
unclear mechanism
• Elimination diets (may need elemental diet)
• Oral Challenges – Timing/dose/approach
individualized for disorder
• Enterocolitis syndrome can induce shock
• Eosinophilic gastroenteritis may need prolonged feedings before symptoms develop
– DBPCFCs preferred
– May require ancillary testing (endoscopy/biopsy)
Management
Management of Food
Allergy
• Complete avoidance of
specific food trigger
• Ensure nutritional needs
are being met
• Education
• Anaphylaxis Emergency
Action Plan if applicable
– most accidental exposures
occur away from home
This frozen dessert
could have peanut,
tree nut, cow’s milk,
egg, wheat
Management: Dietary
Elimination • Hidden ingredients in
restaurants/homes (peanut in
sauces,egg rolls)
• Labeling issues (“spices”,
changes, errors)
• Cross contamination (shared
equipment)
• Seeking assistance
– Food allergy specialist
– Registered dietitian:
(www.eatright.org)
– Food Allergy & Anaphylaxis
Network (www.foodallergy.org;
800-929-4040) and local support
groups

Contain cow’s milk: Artificial butter flavor, butter, butter fat, buttermilk, casein, caseinates (sodium, calcium, etc.), cheese, cream, cottage cheese, curds, custard, Half&Half®, hydrolysates (casein, milk, whey), lactalbumin, lactose, milk (derivatives, protein, solids, malted, condensed, evaporated, dry, whole, low-fat, non-fat, skim), nougat, pudding, rennet casein, sour cream, sour cream solids, sour milk solids, whey (delactosed, demineralized, protein concentrate), yogurt. MAY contain milk: brown sugar flavoring, natural flavoring, chocolate, caramel flavoring, high protein flour, margarine, Simplesse®.
AS of January 1, 2006, all food containing “Big Eight Allergens” (cow’s milk, peanut, tree nut, hen’s egg, soy, wheat, fish, crustacean) in the U.S. MUST declare the ingredient on the label in COMMON language. Does NOT apply to non-Big 8 allergens (e.g., sesame).
Label reading used to be very
challenging!
Example: Cow’s Milk
Food Allergen Labeling and Consumer
Protection Act of 2004 (P.L. 108-282)
(FALCPA)
Management: Infant
Formulas
• Soy (confirm soy IgE negative)
– <15% soy allergy among IgE-CMA
– ~50% soy allergy among non-IgE CMA
• Cow’s milk protein extensive hydrolysates
– >90% tolerance in IgE-CMA
• Partial hydrolysates
– Not hypoallergenic!
• Elemental amino acid-based formulas
– Lack allergenicity
* CMA=cow’s milk allergy
Management:
Emergency Treatment of
Anaphylaxis • Epinephrine: drug of choice
– Self-administered epinephrine readily available at all times
– If administered, seek medical care IMMEDIATELY
– Train patients, parents, contacts: indications/technique
• Antihistamines: secondary therapy only: WILL NOT STOP ANAPHYLXAXIS
• Written Anaphylaxis Emergency Action Plan
– Schools, spouses, caregivers, mature sibs / friends
• Emergency identification bracelet
MYTH: Prior Episodes
Predict Future Reactions
• No predictable pattern
• Severity depends on:
– Sensitivity of the individual
– Dose of the allergen
– Other factors (e.g., food matrix
effects, exercise, concurrent
medications, airway
hyperresponsiveness)
• Must always be prepared for an emergency
.

Key Point: Diphenhydramine
will not block anaphylaxis
• Unfortunately, reaction
severity CANNOT be
predicted to again be mild with
the next episode
– In a United Kingdom series of
anaphylaxis fatalities, 1/3 of
food allergy deaths were in
patients with such mild
reactions to foods (mainly
peanuts/tree nuts) that they
had not been prescribed self-
injectable epinephrine*
– Consider self-injectable
epinephrine for all at risk of
anaphylaxis *Pumphrey RS. Clin Exp Allergy. 2000
Aug;30(8):1144-50.
This is
available for
download.
Parents can
add their
child’s photo
on the plan
and review it
with
caregivers/sch
ools.
Available at:
www.aaaai.org
The form was adapted from J
Allergy Clin Immunol
1998;102:173-176 and J Allergy
Clin Immunol 2006;117:367-
377.
Management: Follow-
Up
• Re-evaluate for tolerance
periodically
• Interval and decision to re-
challenge:
– Type of food allergy (IgE vs non-
IgE)
– Severity of previous symptoms
– Allergen/Prognosis (cow’s milk vs
peanut)
• Ancillary testing
– Skin prick test/in vitro specific IgE
may remain positive
– Decline in concentration of food
specific-IgE is suggestive of
development of tolerance
Prevention

Food Allergy Prevention
• Expect revisions – research
is ongoing
( American Academy of Pediatrics
recommendations for children at risk of
food allergy include a delay in
introduction of certain foods:
– Solid foods: after age
6 mos
– Cow’s milk/dairy: after age
1 yr
– Egg: after age
2 yrs
– Peanut, tree nut, seafood: after age
3-4 yrs)
(2008 Committee report states that there
is NO CONVINCING EVIDENCE that
delaying solids beyond 4-6 mos has a
significant protective effect on
American Academy of Pediatrics Committee on Nutrition.
Pediatrics 2000;106:346-9.
Food Allergy Prevention
• Exclusive breastfeeding for at least 4 months decreases eczema and cow milk allergy in the first 2 years of life in infants at high risk for atopy
• Recent studies (Fox) show early oral intake of peanuts decreases peanut allergy while env. exposure alone increases the risk
• Du Toit showed that peanut allergy was 10-fold higher in Jewish children in the UK vs. Israel where peanut is introduced early
Fox AT, et al. J Allergy Clin Immunol 2009;123:417-23.
Du Toit G, et al. J Allergy Clin Immunol 2009;122:984-91.
Ongoing Studies
• The Food Allergy Research
Consortium-NIH sponsored
consortium to study food
allergy
• Now underway:
Observational study of solids in
infants>4mo
Egg oral immunotherapy
Peanut sublingual
immunotherapy
Recombinant peanut vaccine
safety study
Future Approaches

Future Immunomodulatory
Approaches
• Recombinant anti-IgE antibody
• Gene (naked DNA) immunization
• Mutated B-cell epitopes
• Minimal T-cell epitopes
• Immune-modulating adjuvants (ISS)
• Probiotics
• T lymphocyte manipulation to induce
tolerance
• Chinese herbal remedies (Food
Allergy Herbal Formula)
TH0 TH1
TH2
TH2
TH1
Tolerance (immune deviation)
Sensitization
“atopics”
“Non-
atopics”
antigen
IgE
cDNA, Probiotics Peptides/Epitopes
Immune
Modulation
Anti-IgE Sicherer SH, unpublished
Role of the Allergist
Reasons for Allergy
Referral
• Persons who have limited their diet based upon perceived adverse reactions to foods or additives.
• Persons with a diagnosed food allergy
• Atopic families with, or expecting, a newborn who are interested in identifying risks for, and preventing, allergy.
• Persons who have experienced allergic symptoms in association with food exposure.
• Persons who experience an itchy mouth from raw fruits and vegetables.
Leung D, et al. J Allergy Clin Immunol
2006;117:S495-523.

Reasons for Allergy
Referral (Cont’d)
• Infants with recalcitrant gastroesophageal reflux or older individuals with recalcitrant reflux symptoms, particularly if they experience dysphagia.
• Infants with gastrointestinal symptoms including vomiting, diarrhea (particularly with blood), poor growth, and/or malabsorption whose symptoms are otherwise unexplained, not responsive to medical management, and/or possibly food-responsive (even if screening allergy tests are negative).
• Persons with known eosinophilic inflammation of the gut.
Leung D, et al. J Allergy Clin Immunol
2006;117:S495-523.
Role of the Allergist
• Identification of causative food
• Institution of elimination diet
• Education on food avoidance
• Development of an Anaphylaxis
Emergency Action Plan
• Prevention of other allergies
• Follow-up to ascertain tolerance
Summary and
Conclusions • IgE & non-IgE-mediated
conditions exist
• The history and physical are
paramount
• Elimination diets, skin testing, in
vitro assays, and food challenges
also have roles in diagnosis
• Avoidance, education, and
preparation for emergencies are
the pillars of current management
• Periodic re-challenge to monitor
tolerance as indicated by history,
allergen, and level of food-
specific IgE is an important part
of ongoing follow-up


















