Advances in TB Diagnostics

of 21
-
Upload
kelonericbana -
Category
Documents
-
view
234 -
download
0
Transcript of Advances in TB Diagnostics
-
8/6/2019 Advances in TB Diagnostics
1/21
INVITED REVIEW SERIES: TUBERCULOSISSERIES EDITORS: WING WAI YEW, GIOVANNI B. MIGLIORI AND CHRISTOPH LANGE
Advances in the diagnosis of tuberculosisCHRISTOPH LANGE 1 AND T ORU MORI 2
1Clinical Infectious Diseases, Research Center Borstel, Borstel, Germany, and 2Research Institute of Tuberculosis, Japan Anti-Tuberculosis Association, Tokyo, Japan
ABSTRACTTuberculosis ranges among the leading causes of mor-bidity and mortality worldwide. A diagnostic approachto a patient with possible tuberculosis includes a detailed medical history and clinical examination as well as radiological, microbiological, immunological,molecular-biological and histological investigations, where available. Recently, important advances havebeen achieved in these elds that have led to substan-tial improvementsin theaccuracy and the timingof thediagnosis of tuberculosis. Novel methods allow for a better identication of latently infected individuals who are at risk of developing active tuberculosis, they also offer the possibility for a rapid diagnosis of activetuberculosis in patients with negative sputum smearsfor acid-fast bacilli and enable prompt identication of drug-resistant strains of Mycobacterium tuberculosis directly from respiratory specimen with a high accu-racy. In addition, promising methods that will furtheroptimize the diagnosis of tuberculosis are under devel-opment. In the future,therapeutic interventions basedon the results of novel diagnostic procedures can bemade earlier leading to improvements in patient care.
Key words: diagnosis, imaging microbiology, immu-nology, tuberculosis.
INTRODUCTION resp_1692 220..240
Tuberculosis ranges among the leading causes of morbidity and mortality worldwide. Based on surveil-lance and survey data, the World Health Organisation(WHO) estimates in the latest report from the year
2009 that 13.7 million individuals were living withactive tuberculosis in the year 2007 (206 per 100 000population) and 9.27 million people (139 per 100 000population) developed tuberculosis in that year. Among the 1.76 million persons who died from tuber-culosis in the year 2007, 1.3 million were seronegativeand 455 000 seropositive for HIV infection. 1
Inclinicalpracticetherapiddetectionof individuals with tuberculosis can be difcult, 2 as only 44% of allnewcases(andonly1520%ofchildren 3)areidentiedby presence of acid-fast bacilli (AFB) on sputumsmears. 1 The gold standard for the diagnosis of tuber-culosis is thedetection of Mycobacteriumtuberculosis ,the causative microorganism of tuberculosis. In fact, whenever M. tuberculosis is recovered from humanspecimensby microbiological culture the diagnosis of active tuberculosis is regarded as denite.
However, culture growth of M. tuberculosis may take 2 or more weeks on average. The ad hoc decision
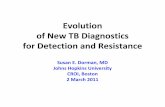
to initiate anti-tuberculosis treatment can be difcultin cases where AFB are not found on sputum smearmicroscopy despite the clinical suspicion of tubercu-losis. The clinical diagnosisof active tuberculosis thenclassically relies on the results of different methods,including the tuberculin skin test (TST), chest radiog-raphy, amplication of M. tuberculosis nucleic acidsand/or pathological examinations from biologicalspecimens (Fig. 1).
In this article we reviewtheepidemiologyandclini-cal manifestation of tuberculosis and we discussrecent advances that allow a better and earlier diag-nosis of active pulmonary tuberculosis in clinicalpractice. A continuous update on evidenced-based
tuberculosis diagnosis can also be found at http:// www.tbevidence.org
CURRENT TRENDS IN THEEPIDEMIOLOGY OF TUBERCULOSIS
The world can be divided into two parts based on theextent of tuberculosis epidemics. One part is the low-prevalence areas. They are composed of countriesthat experienced serious tuberculosis epidemics afterthe 18th century but have gradually overcome themand have nally reduced the incidence rate to 100 per100 000 or less. The other part is the high-prevalence
C.L. is a Pulmonologist and Infectious Diseases specialist. Heis leading the Division of Clinical Infectious Dieseases and theCenter for Clinical Studies at the Medical Clinic of the ResearchCenter Borstel, Germany, and he is chairing the Tuberculosissection of the European Respiratory Society (ERS) and the Tuber-culosis Network European Trials group (TBNET). T.M. is a tuber-culosis expert with a focus on epidemiological research andpublic health, and has been involved with tuberculosis control inJapan as well as in the developing world for the past 40 years.
Correspondence: Toru Mori, Research Institute of Tuberculo-sis, Japan Anti-Tuberculosis Association, 3-1-24, Matsuyama,Kiyose, Tokyo 204-8533, Japan. Email: [email protected]
Received 27 October 2009; invited to revise 30 October 2009;revised 5 November 2009; accepted 5 November 2009.
2010 The AuthorsJournal compilation 2010 Asian Pacic Society of Respirology Respirology (2010) 15 , 220240doi: 10.1111/j.1440-1843.2009.01692.x
-
8/6/2019 Advances in TB Diagnostics
2/21
areas comprising countries with an incidence rateexceeding100per 100 000 that have suffered tubercu-losis epidemics after the turn of the 20th century. Thelow-prevalence countries are industrialized coun-tries, while the high-prevalence countries are mostly developing counties or areas. The latter accounts fortwo-thirds of the world population, but as much as95% of the estimated number of newly occurring tuberculosis patients (of all forms) globally. Further-more, 98% of tuberculosis deaths occur in these high-prevalence areas. 1 Tuberculosis accounts for 2.7% of the total disability-adjusted life-years in low- andmiddle-income countries. 4 In addition to the differ-ence in its level, there are clear differences in charac-teristics of tuberculosis disease. In high-prevalencecountries, most tuberculosis patients are in their 20sto 40s, resulting in tremendous socioeconomic loss asthis is the most productive generation. In contrast,among low-prevalence countries, tuberculosis isdrifting to involve the elderly, socioeconomicallymar-ginalized people, medical high-risk groups (e.g. dia-betics 5 and those treated with immunosuppressiveagents, such as TNF-alpha blockers 6), which presentsa challenge to both medical and welfare services.
As a consequence of the global efforts in tuberculo-sis control under the Directly Observed TreatmentShort-course strategy since the 1990s, the incidenceof tuberculosis is estimated to have started to declinefor the rst time around 2003, although very slowly. 1 At the same time, issues that had been given only lower priority in the developing world have emergedas unavoidable challenges. One of these issues ismulti-drug resistant (MDR) tuberculosis that strikes ahalf million people annually and is a malignantburden to the patients and community, as well as tonational tuberculosis programmes with its poor treat-ment outcome. 7 In line with this problem, extensively drug resistant (XDR) strains of M. tuberculosis areemerging recently. 8 The use of effective secondary drugs based on the result of high-performance drug sensitivity tests is necessary in order to address theseissues, which requires technical innovation. 7
A second newly emerging issue is co-infection of the HIV and M. tuberculosis . Currently, 15% of thenew tuberculosis patients are infected with HIV, andin some areas or countries this proportion exceeds50%. One quarter of the global tuberculosis deathsare due to HIV, and this is equal to one-third of new
Figure 1 Flow diagram for the diagnosis of tuberculosis in clinical practice. *NTM NAAT may be helpful, whenavailable. In accordance with WHO recommendations (WHO. Treatment of tuberculosis. Guidelines for nationalprogrammes. Geneva; 2003), clinical response to antibiotic therapy may be considered before further investigations;however, in countries of low TB incidence immediate further diagnosis with bronchoscopy can be indicated at this stageto better rule out other diseases. BAL, bronchoalveolar lavage; IGRA, interferon- g release assay; MTB, Mycobacteriumtuberculosis ; NAAT, nucleic acid amplication test; NTM, non-tuberculous Mycobacteria; TB, tuberculosis; TBB, tuberclebacilli; TST, tuberculin skin test; WHO, World Health Organisation.
Diagnosis of tuberculosis 221
2010 The AuthorsJournal compilation 2010 Asian Pacic Society of Respirology Respirology (2010) 15 , 220240
-
8/6/2019 Advances in TB Diagnostics
3/21
HIV-positive tuberculosis cases and to 23% of theestimated two million HIV-related deaths in 2007. 1Diagnosing tuberculosis in these subjects withsputum smear examination alone cannot preventtheir infectiousness and save their lives; more aggres-sive case-nding and treatment of smear-negativecases are required. Another issue is tuberculosis inchildren for whom Mycobacterium bovis Bacille Cal-
mette Guerin (BCG) vaccination has been virtually the only control measure in developing countries.This also requiresaccuratediagnosis in theearly stageof tuberculosis. 9
As seen above, tuberculosis appears as a typicalsouth-north problem of health, but currently in many developed countries over half of the new tuberculosiscases are foreign-born, that is, immigrants from high-prevalence areas, or spill-over of tuberculosis. 10,11 Itis actually argued that to further reduce tuberculosisin the low-prevalence countries it is necessary tostrengthen control efforts in the high-prevalence,developing countries. 12
CLINICAL MANIFESTATION OFTUBERCULOSIS (PULMONARYAND EXTRAPULMONARY ANDCHILDHOOD TUBERCULOSIS)
In general, clinical manifestations of illness are therst clue to the diagnosis of tuberculosis. However,they are often non-specic and misleading, andtherefore the diagnosis is not always easy. This isespecially the case for tuberculosis in children and inelderly subjects, as seen below. Further, extrapulmo-nary tuberculosis often poses a challenge to early diagnosis, especially pertaining to its variety of pre-sentations. Clinical signs and symptoms of tubercu-losis of the organs other than the lungs aresummarized in Table 1.
Tuberculosis in children
Because of its paucibacillary nature, tuberculosis of children is difcult to diagnose. Bacteriological con-rmation seldom exceeds 3040% among children indeveloped as well as developing countries. 106,107 Con-sequently, the diagnosis of tuberculosis in childrenin resource-poor settings is largely dependent on acombination of a history of contact with a knowntuberculosis patient, clinical signs and symptoms,and special examinations, such as chest radiography and the TST when available. Edwards and colleaguesobserved a total of 91 tuberculosis cases youngerthan 15 years, of whom about half were HIV-infected, and found the following frequency of symptoms and signs in the HIV-seronegative chil-dren: weight loss 69%, fever 100%, cough 83%, nightsweat 43%, fatigue 21%, tuberculosis contact 60%,malnutrition 57%, lymphadenopathy 88%, orga-nomegaly 31%, positive TST 89%, elevated erythro-cyte sedimentation rate 79%, and chest X-ray inltration 100%. 108 Based on these observations,
several point-scoring systems, diagnostic classica-tions and diagnostic algorithms have been devel-oped to support an objective diagnostic judgment.Marais et al . tested such an approach and found thatcombining a persistent non-remitting cough lasting over 2 weeks, documented deterioration of health(in the preceding 3 months) and fatigue providedreasonable diagnostic accuracy in HIV-uninfected
children (sensitivity 62.6%; specicity 89.8%; positivepredictive value 83.6%). The performance waspoorer in HIV-infected children than in the low-risk group, which offers a serious challenge in resource-poor settings with high HIV epidemics. 109 However,given this set of sensitivity and specicity, the posi-tive predictive value is calculated as only 24% in apatient population with a prevalence of tuberculosisof as high as 5%.
Tuberculosis in old ages
In low-prevalence situations, tuberculosis is a
problem predominantly of the aged population andincludes many more cases of clinical development inimmunologically compromised subjects. This is why there are many tuberculosis cases with atypicalclinical presentation(s) in older persons. 110,111 Elderly patients are more likely to have extrapulmonary tuberculosis, including miliary disease. 111 The pro-portion of bacteriologically conrmed pulmonary tuberculosis patients was higher in the elderly than in the younger patients as reported in ameta-analysis. 112
Fever, sweating and haemoptysis are less frequentin older patients, but dyspnoea is more frequent. 112Laboratory ndings, such as the TST-positive rate,
serum total protein level and white blood cell counts, were lower in elderly patients. Also, cavity formation was less common in elderly patients, while lesions inthe upper lung were similar for both age groups. 112The most common chest X-ray ndings in the elderly or immunocompromized tuberculosis patients arelesion in the lower zone accompanied by basal effu-sion or thickening. 110 Such atypical clinical presenta-tion of tuberculosis in the elderly can often causedelay in diagnosis, which can be further complicateddue to underlying illnesses.
Delays in diagnosis
One of the basic indicators of quality in diagnosing tuberculosis is the delay in diagnosis (doctorsdelay, or health systems delay), that is, the timefrom the rst visit of a patient until the establish-ment of tuberculosis diagnosis. Figure 2 depicts thedelay separately for high-, intermediate- and low-prevalence settings, together with the patients delay,that is, the time from the onset of clinical symptomsuntil the rst visit to a health facility, based on pub-lished studies (T. Mori, pers. comm.). It is remark-able that these delays in the low-prevalence settingsare always longer than those in the high-prevalencesettings.
C Lange and T Mori 222
2010 The AuthorsJournal compilation 2010 Asian Pacic Society of RespirologyRespirology (2010) 15 , 220240
-
8/6/2019 Advances in TB Diagnostics
4/21
Table 1 Clinical presentations and laboratory examinations for diagnosis and differential diagnosis for major types ofextra-pulmonary tuberculosis 134,302
Site Symptoms & signs Laboratory tests Differential diagnosis
Pleurisy Primary infection cases have generally anacute course of symptoms thanreactivation-type TB.
Cough (non-productive) and chest pain(pleuriticsharp, stabbing, associatedwith respiration). Feverishness,dyspnea, chills, sweats, weight loss inmore advanced cases. TB pleuraleffusions are generally exudates.
Radiography, sputum bacteriology(for undiagnosed pulmonary TB),thoracocentesis with pleural uid forcell prole, protein, pH, glucose, LDH,smear, culture, NAAT, 1316 ADA, 1720
IFN-g ,20,21 IGRA, 2226 pleural biopsy forhistology, culture and NAAT. 27,28
Effusions due to congestive heartfailure, carcinoma, othertypes of infections andrheumatological disorders.
Lymphadenopathy Most often in the neck and head region,rare in the axillary & inguinal region.Right predominates but 1/4 havebiliateral & 78% have multiple lesions.41% have pulmonary TB.
In supercial LN, lesion starts as apainless enlargement, with noinammation over the skin, then mayundergo pustulation and stulation overseveral weeks or months. In a case withlimited lesion, general symptoms arerare.
Culture isolation of MTB, chestradiography, biopsy (total excisional)followed by bacteriological culture/ PCR 28 and histology. Fine needleaspiration. 29
NTM infections, lymphoma,sarcoidosis, Kikuchis disease,Castlemans disease, Kimurasdisease, corynebacteriumpseudotuberculosislymphadenitis. 30
Bone & Joint Commonest in vertebral column, followedby hip and knee. Fever and wasting
may appear in large inammatorycollections, but the local manifestationpredominates. Pain is commonest. Softtissue collection (cold abscess) at/nearthe bone or joint focus. Neurologicalsigns (weakness or numbness fromcompression of the spinal cord).
MTB from aspirate (abscess, synovialuid) and biopsy specimen (e.g.
synovia), 3134 CT & MRI. 3538
For arthritis: pyogenic,rheumatoid, gout, regional
osteoporpsis, idiopathicchondrolysis. For cystic bonelesions: eosinophilicgranuloma, sarcoidosis, cysticangiomatosis, plasma cellmyeloma, fungal infection,metastatic malignancy.
Disseminatedor miliary TB
Diverse depending on the organsinvolved.
Feverishness, weakness or debility,anorexia, weight loss, headache(meningeal complication), abdominalpain/swelling (peritoneal involvement),cough. 39,40
Chest radiography (often no abnormalityin the beginning), CT (HRCT), 41,42
beroptic bronchoscopy, TBLB, 43
haematology (anaemia, leukopenia orleukocytosis, rarely leukemoidreaction). Liver function, bone marrowbiopsy, liver biopsy (includingNAAT 44), fundoscopy. 45
Alveolar microlithiasis,disseminated carcinoma,sarcoidosis, NTM infections,hypersensitivity pneumonitis.
Central nervoussystem
The presentation depends on the size andlocation of the tuberculoma and thepressure it produces.Early symptoms(feverishness, malaise, anorexia,irritability, headache) followed byneurological symptoms (progressiveheadache, lethargy, personalitychanges, memory disturbance, impairedcognition, confusion), and thenstupor-coma with or withoutneurological decit.
Cerebrospinal uid for pressure,cellularity, protein, glucose, 46
MTB (microscopy, culture 47,48 andPCR 49,50 ), immunology (ELISA,IgG immune complex, antibodyassays and IGRA 5156 ), and ADA.Radiography, CT, MRI. 5761 Meningealbiopsy (histology, MTB).
Other infections (fungal, viral,trypanosomal, bacterial),vascular (multiple emboli, SBE,thrombosis of sagittal vein),collagen vascular (SLE,polyarteritis, and others).
Abdominal Frequency: peritonitis, followed byileocaecal, anorectal and mesentericlymph node infection.In peritoneal TB,abdominal swelling, fever, ascites, pain,anorexia/weight loss are common. 62,63
Peritonitis: ultrasound, 6466 laparoscopy(with guided biopsy), 6770 paracentesisof ascites for culture and IGRA 71,72 andADA. 73
Malignant ascites, cirrhosis withspontaneous bacterialperitonitis, starch peritonitis,sarcoidosis, NTM peritonitis.
Pericarditis Dyspnoea, tachycardia, neck veindistension, oedema, hepatomegaly,paradoxical pulse, pericardial rub,fever. 74,75
Pericardial tissue/uid for bacteriology,histology, 76,77 IGRA, 78,79 and ADA. 8082
Echocardiography, 8385 CT and MRI(pericardial effusion and thickening), 86
ECG (low voltage, inversion of T). 87
Bacterial (e.g. Pneumococcus),viral (e.g. CMV, HSV,Coxsackievirus) or fungal (e.g.Aspergillus) infections;collagen vascular diseases;uremia; post-myocardial
infarction orpost-pericardiotomie;malignancy; trauma.
Genitourinary Dysuria, frequency, nocturia, urgency,pain in the back, ank or abdomen,tenderness/swelling of the testis orepididymis, haematuria. Superimposedurinary tract infection with otherbacteria in urinary stasis cases. 8893
Urine or secretion (early morningspecimen) for MTB (smear, culture,PCR), 94 ultrasound, 95 plain abdominalradiograph, i.v. urography (high-dose),image-intensied endoscopy,percutaneous antegradepyelography, 96102 biopsy for suspectof genital lesion. 103105
Benign and malignant tumor,cystic kidney, pyelonephritis,xanthogranulomatouspyelonephritis, urinarymalakoplakia.
ADA, adenosine deaminase; CT, computed tomography; ECG, electrocardiogram; HRCT, high resolution computed tomography;IGRA, interferon-gamma release assay; LDH, lactate dehydrogenase; LN, lymph node; MRI, magnetic resonance imaging; MTB,Mycobacterium tuberculosis ; NTM, non-tuberculous mycobacterium; PCR, polymerase chain reaction; SBE, subacute bacterialendocarditis; SLE, systemic lupus erythematosus; TB, tuberculosis; TBLB, transbronchial lung biopsy.
Diagnosis of tuberculosis 223
2010 The AuthorsJournal compilation 2010 Asian Pacic Society of Respirology Respirology (2010) 15 , 220240
-
8/6/2019 Advances in TB Diagnostics
5/21
Sasaki et al . reviewed the diagnostic process of private practitioners with Japanese patients and con-cluded that insufcient medical work-ups, including AFB examinations of sputa and chest X-rays of sub- jects with a high suspicion for tuberculosis, was theprincipal cause of delayed diagnoses. 113,114 In Hong Kong, general practitioners practice was reviewed,and it became clear that they depend too much on X-rays rather than sputum examinations, and thatthey were slow in referring tuberculosis patients tothe government tuberculosis service. 115 Rozovsky- Weinberger et al . compared the management of suspect tuberculosis cases at three public hospitalsand seven not-for-prot private hospitals in the USA in terms of their rates of ordering acid-fast smearsand isolations, and urged private hospitals to bemore alert to tuberculosis. 116 Similar reviews of hospital management were reported by severalother studies, 117119 the results of which illustratethe need for improved education of doctors. Allof these studies urge a higher index of suspicionfor tuberculosis in medical staff in low-prevalencecountries.
ADVANCES IN THE IMAGINGDIAGNOSIS OF TUBERCULOSIS
None of the radiological abnormalities seen inpulmonary tuberculosis are pathognomonic for thisdisease. Nevertheless, several features are typical of tuberculosis. Classical radiographic abnormalitieshave recently been reviewed. 120 They include featuresof primary tuberculosis, for example, unilateralhilar lymphnode enlargement, parenchymal air-space consolidation and/or pleural effusion, 121123 orfeatures of reactivation tuberculosis, for example,focal or patchy heterogeneous consolidation involv-ing the apical and posterior segments of the upperlobes and the superior segments of the lower lobes,poorly dened nodules, linear opacities andcavitations. 123125
While the classication in primary and reactiva-tion tuberculosis is still widely en vogue , evidencefrom genotype ngerprinting studies conrms thatthe radiographic feature in tuberculosis following recent and remote infection are very similar and thatintegrity of the immune system predicts the appear-ance of the patterns of active tuberculosis on chestimaging: immunocompromized individuals (e.g.those with advanced HIV infection) having theappearance of primary tuberculosis and immuno-competent individuals having the appearance of reactivation tuberculosis. 126,127
The conventional chest X-ray is still the most com-monly used method for screening, diagnosis andfollow up of treatment responses in patients with pul-monary tuberculosis. However, chest computedtomography (CT), in particular high-resolution CT, ismore sensitive than conventional chest X-ray to iden-tify early parenchymal lesions or mediastinal lymph
node enlargements and to determine disease activity in tuberculosis. 128131Radiographic features on CT that are suggestive of
active tuberculosis include cavitations and parenchy-mal abnormalities and/or centrilobular nodules andthe tree-in-bud pattern .120
Recently, serial pulmonary [(18)F]-2-uoro-deoxy-D-glucose positron emission tomography has beeninvestigated as a promising non-invasive method tomonitor disease activity and responses to anti-tuberculosis chemotherapy. 132,133 Although highly expensive, this techniquecould be useful and even becost-effective for the managment of patients withMDR and XDR tuberculosis in selected cases.
MICROBIOLOGICAL DIAGNOSIS:CONVENTIONAL METHODS
Remarkable efforts have been made globally toaccelerate the development and expansion of new diagnostic technologies. However, tuberculosis casedetection still remains dependent upon sputumsmear and culture, radiography and clinical symp-tomatology, and currently 57% of global tuberculosispatients receive a bacteriological diagnosis. There-fore, efforts to improve thequality of existing methods
Figure 2 Box plots of delay in case detection for coun-tries with high, intermediate and low prevalence of tuber-culosis. Figures in parentheses indicate the number ofstudies analysed. (a) Patients delay (time a patient needsfrom the occurence of the rst symptoms to seekinghealthcare) and (b) health systems delay (time to estab-lish the diagnosis of tuberculosis after the rst presenta-tion of a patient to a healthcare facility).
C Lange and T Mori 224
2010 The AuthorsJournal compilation 2010 Asian Pacic Society of RespirologyRespirology (2010) 15 , 220240
-
8/6/2019 Advances in TB Diagnostics
6/21
are necessary, and there actually have been certainachievements in this direction.
Sputum smear examination by microscopy
One recent achievement in conventional tuberculosismicroscopy is therecognitionof thebenetof uores-
cent microscopy for enhancing sensitivity over that of ordinary lightmicroscopy without anyloss in specic-ity. 135 The uorescence microscopy widely used inresource-rich countries has been accepted as moresensitive than ordinary microscopy, although with aconcern of loss of specicity, especially under condi-tions in the developing world. Nonetheless, a recentliterature review has conrmed that it may be alsobenecial in the latter as well. This could be furtherimproved byattachinga strongerlight sourcecalled anultra-bright (Lumin TM, LifeEnergy , Germany) light-emitting diode. 136,140 Another systematic review on thesputum processing in sputum smear testing demon-strated that centrifugation combined with any of
several chemical methods (including bleach) is moresensitive, and overnight sedimentation preceded by
chemical processing is more sensitive with similarspecicity. 137 Operational studies are needed to deter-mine the balance between the benet from increasedsensitivity and the costs in terms of complexity andpotential biohazards.
In order to enhance the sensitivity of sputumsmeartests, the examination must be done three times, butthis principle was challenged so that the third exami-
nation adds very little to the rst two examinations, atleast in laboratories with good-quality control. 138141This is incorporated in the International Standards of Tuberculosis Care in routine practice. 142
If a patient cannot produce sputum, any methodfor sputuminduction is encouraged.This is especially benecial to ensure high sensitivity of sputum smeartests in resource-poor settings where such drasticmethods as gastric washing or bro-optic bronchos-copy cannot be used. 143 It was shown that inductionperformed well in developing countries with littleadded costs. 144 Recently, a new device for sputuminduction called the lung ute has been developedand may be worth trying 145 (refer to Table 2 for collect-
ing and processing specimens for the diagnosis of tuberculosis).
Table 2 Biological specimen for the diagnosis of tuberculosis
Specimen Amount Application Preservation/transport Comment
Sputum 25 mL A, B, C Unprocessed 3 in the morning on an emptystomach
Induced sputum 25 mL A, B, C Unprocessed Expectoration following inhalationof 3% NaCl solution
Bronchial secretion orbronchoalveolar-lavage
25 mL A, B, C, D Unprocessed BAL-ELISPOT should beperformed on the day of sample
collectionGastric aspirate > 2 mL A, B, C In 12 mL phosphate buffer(trinatrium phosphate)
Only when sputum cannot beobtained and bronchoscopy(BAL) is not indicated
Biopsy, survivalspecimen (e.g.lmph nodes)
2 separateportions(1) and (2)
A, B, C, E (1) In 0,9% NaCl formicrobiological examination;(2) in formalin forhistopathologicalexamination
(1) Not in formalin
Pleural effusion,ascites
20 mL A, B, C, D, Unprocessed ELISPOT should be performed onthe day of sample collection
Cerebrospinaluid
23 mL A, B, C, D Unprocessed ELISPOT should be performed onthe day of sample collection
Urine 30 mL A, B, C Unprocessed 3 First specimen of urine inthe morning Fluid restrictionthe evening/night before
Stool 510 mL A, B, C Unprocessed 3 Blood 510 mL A, B, C, D Heparin- or lithium-citrate
tubes Indicated only in
immunosuppressed patients Do not use EDTA blood
Bonemarrow
2 separateportions(1) and (2)
A, B, C, E (1) In heparin- or lithium-citratetubes; (2) air-dried smearsand/or formalin preservedbiopsies
Indicated only inimmunosuppressed patients
Biopsy or aspirate for (1) not inEDTA or formalin
Application in different tests: A, microscopy; B, culture; C, NAAT; D, IGRA; E, histopathology.BAL, bronchoalveolar lavage; ELISA, enzyme-linked immunosorbent assay; ELISPOT, enzyme-linked immunospot;
EDTA, ethylenediaminetetraacetic acid.
Diagnosis of tuberculosis 225
2010 The AuthorsJournal compilation 2010 Asian Pacic Society of Respirology Respirology (2010) 15 , 220240
-
8/6/2019 Advances in TB Diagnostics
7/21
The quality of smear examination has become widely recognized as so important that the need forimplementing quality assurance in every laboratory has been strongly advocated. 146
Progress in culture examinations
Since the 1990s, a series of culture examinationsystems has been developed using liquid media forrapidly detecting M. tuberculosis . A systematic review demonstrates that these liquid cultures are morerapid and sensitive than solid medium cultures. 147,148The mean time to detection was 12.9 days by BACTEC MGIT960, and 15.0 days with BACTEC 460,compared with 27.0 days with Lowenstein Jensensolid medium. 148 Thus, WHO recently endorsed theuse of liquid tuberculosis culture and drug suscepti-bility testing for M. tuberculosis in low-resource set-tings. 149 The newly developed rapid liquid culturesystems have unique sensing systems to detect asmall amount of bacterial growth, such as by
radioactivity or oxygen concentration changes, asquickly as possible. These systems can also be usedfor drug susceptibility testing as well as detecting M. tuberculosis .150,151
Novel diagnostic test using mycobacteriophages toidentify M. tuberculosis from biological specimenrequire only 2 days of turnaround time in the labora-tory. They have a high specicity (range 83% to 100%),but lack sufcient sensitivity (range 21% to 88%)to substitute conventional culture techniques. 152Bacteriophage-based assays have also been devel-oped for the rapid detection of rifampicin resistancein M. tuberculosis . However, the diagnostic accuracy of these assays is insufcient when applied directly to
clinical isolates.153
Still other systems based on phenotypes have beendevised mainly for drug susceptibility testing. Onesuch system is the microscopic observation drug sus-ceptibility, 154 where the characteristicgrowth of M. tu-berculosis in the liquid medium in a well is checkedunder an inverted light microscope. In anothersystem, bacterial growth is conrmed from the bacte-rial activity to reduce nitrate to nitrite in the liquidmedia, which is indicated by the change in colourof the media (nitrate reductase assay). 155,156 Othercolorimetric redox indicator methods are also being evaluated for the rapid detection of MDR in M. tuber-culosis .157 These DST methods can be applied to clini-cal sputumsamples andhave been shown useful withperformance comparable to genetic methods, in theirsensitivityandspecicity, andthemeantime to results was 2123 days. 158
Given the technical difculty of the procedure andthe wide variation of the results, the need for quality assurance is indeed very pressing for drug suscepti-bility testing, especially with solid media. WHO/IUATLD established a system of prociency testing toquantify the technical level of local laboratories 159 andintroduced the system of a supra-national referencelaboratory network in which a laboratory so desig-nated should technically support the nearby locallaboratories. 160
MICROBIOLOGICAL DIAGNOSIS:MOLECULAR METHODS
Nucleic acid amplication techniques
The M. tuberculosis -specic nucleic acid amplica-tion tests (NAAT) performed on bronchopulmonary specimen are the most frequently used moleculartests for laboratory diagnosis of pulmonary tubercu-losis. NAAT results can be available to the clinician within 1 day afterobtainingsputum or bronchoalveo-lar lavage (BAL) uid and can have importantimplication for the management of a patient.Unfortunately, NAAT amplication targets are notstandardized and the diagnostic accuracy of the testsis highly heterogenous.
The clinical value of in-house and/or commercialNAAT performed on respiratory specimens for diag-nosis of pulmonary tuberculosis have recently beenrepeatedly reviewed in meta-analyses. 161164
In individuals with positive AFB sputum smears,the sensitivity of NAAT to detect M. tuberculosis nucleic acid on these specimens is greater than95%. 161,162 When AFB are found on sputum or BALsmears, the presumptive diagnosis of tuberculosiscan thus be rapidly conrmed. Apart from rare excep-tions, a negative NAAT result in this situation strongly indicates the presence of a non-tuberculous Myco-bacteria (NTM) species in this specimen.
In contrast, in individuals with negative AFBsputum smears, the estimated sensitivity of NAAT forthe diagnosis of active tuberculosis is highly hetero-geneous (especially when in-house assays are com-pared) and is not consistently accurate enough to beroutinely recommended for the diagnosis of tubercu-losis. 163,164 In general, nested NAAT methods, and the
use of IS6110 as the amplication target are related toa higher diagnostic accuracy.In individuals with a negative sputum smear, the
specicity of NAAT for the diagnosis of active tuber-culosis has been 97% and 98% in an earlier meta-analysis and an independant recent study. 161,165 A positive result in a M. tuberculosis -specic NAAT per-formed on a respiratory specimen is therfore highly indicative of pulmonary tuberculosis. However, in ourexperience far less than 50% of patients with smear-negative tuberculosis have a positive sputum or BALNAAT result. 165 False positive results are seen in indi-viduals with a past medical history of tuberculosisand in patients with bronchogenic carcinoma.
LINE PROBE ASSAYS
Line probe assays are NAAT to detect commongenomic mutations responsible for antibiotic resis-tance from a biological probe or culture by DNA hybridization (GenoType MTBDR assay, Hain Life-science, Nehren, Germany 166 or INNO-LiPA Rif. TB kit,Innogenetics, Zwijndrecht, Belgium 167). In brief, thetests involve DNA extraction, multiplex NAAT, solidphase reverse hybridization on the test strip anddetection of the resistance mutations. 168170 The Geno-type MTBDR plus assay detects several mutations in
C Lange and T Mori 226
2010 The AuthorsJournal compilation 2010 Asian Pacic Society of RespirologyRespirology (2010) 15 , 220240
-
8/6/2019 Advances in TB Diagnostics
8/21
the rpoB gene, in the katG gene and the inhA genepromoter regions. 168,171174 In a meta-analysis, thepooled sensitivity in resistance detection on clinicalspecimen for rifampicin was similar to conventionalDST following culture. However, the pooled sensitiv-ity for isoniazid-resistance testing was less optimal at85% (7292%). 175 The latest version of the line probeassays, the Genotype MTBDR sl assay in addition can
detectgenetic mutationsthat are related to drug resis-tance of strains of M. tuberculosis , including those foruoroquinolones and injectable drugs (amikacin orcapreomycin) enabling the rapid diagnosis of XDRtuberculosis in > 85% of all cases, including directtesting on clinical specimen. 176
IMMUNOLOGICAL DIAGNOSIS
Avances in serology forantibody/antigen detection
There has been a long history of developing systemsto diagnose tuberculosis based on the serologicalreaction, that is, detection of a specic antibody. Cur-rently, the development of such systems is very urgently needed due to the pressure for strengthening earlier diagnosis of diseases in the paucibacillary stage, including pulmonary tuberculosis with nega-tive sputum smears of adults, extrapulmonary tuber-culosis, childhood tuberculosis and tuberculosispatients with HIV coinfection. The system must beoperationally simple for use at the point of care in thedeveloping world and must have rapidity, in additionto diagnostic accuracy in terms of sensitivity andspecicity. Sometimes the systems are specically
expected to detect latent tuberculosis infection (LTBI)and monitor the progress of tuberculosis treatment.However, in contrast to many cases of other acutebacterial and viral infections, there are several barri-ers to the successful application of the serologicalreactions for diagnosing tuberculosis, including thegap between active disease and latent infection, the wide prole of the disease from one with extensivecavitary lesions to an almost inactive, minimaldisease, and distinction from NTM infection. 134 Thesecharacteristics of tuberculosis comprise formidablefactors against sensitivity and specicity of theexpected diagnostics. There is a long list of systems sofar proposed and developed as serological diagnos-tics, each having different characteristics in terms of antigens used and other characteristics (Table 3).
Recently, Steingart and colleagues conducted a sys-tematic review and meta-analysis of the publishedstudies of these techniques. They found 254 studiesevaluating 51distinct singleantigens and30multiple-antigen combinations in terms of their performancein diagnosing pulmonary tuberculosis. 177 The authorsnoted that the data in sputum smear-negative orpediatric patients were not enough but concludedthat none of the antigens sensitivity washigh enoughto replace sputum smear microscopy. In a separatereview, the same authors group made a similar con-clusion for extrapulmonary tuberculosis. 178
Furthermore, WHO/TDR evaluated commercially available tuberculosis testswithregard to theirperfor-mance, reproducibility and operational characteris-tics. 180 They used 355 well-characterized archivedserum samples to evaluate 19 rapid tuberculosis testsat one laboratory. The sensitivity of these rapid testsranged from 1% to 60%; the specicity, from 53% to99%; and in general, tests with high specicity hadvery low sensitivity. Test performance was poorer inpatients with sputum smear-negative tuberculosisand in HIV-positive patients. Again they concludedthat none of the assays performed well enough toreplace microscopy.
As suggested by the above reviews, combinationsof existing potential candidate antigens may enhancesensitivity without losing much specicity, and there-fore related research should be pursued, as well asefforts to discover novel antigens. At the same time,the quality of assessing new techniques should beimproved, including a better study design and devel-opment of effective performance indicators beyondsensitivity and specicity, and establishment of atuberculosis specimen bank, such as the one used inthe WHO/TDR project above. Currently availableserological tests cannot be recommended for the
diagnosis of tuberculosis.
Advances in cellular immunodiagnosis
The TST and interferon- g release assays (IGRA)evaluate in vivo (TST) and ex vivo (IGRA) thepresence of persistent mycobacteria-specic T cellresponses. 183,184 They are indirect marker for past orpresent infection. TST and IGRA performed onperipheral blood alone cannot distinguish betweenindividuals with LTBI, active tuberculosis or pasttuberculosis. 185,186
Table 3 Types and nature of serodiagnostic methods(based on 134,177182 )
Antigens 38 kDa, 16 kDa, 88 kDa, MPT51,malate synthase, CFP-10, TbF6polyprotein, antigen 85B, antigenA60, antigen 5, alpha-crystallin,2,3-diacyltrehalose,
2,3,6-triacyltrehalose,2,3,6,6-tetraacyltrehalose 2-sulfate(SL-1), cord factor,tuberculophosphatide,lipoarabinomannan, Rv3425
Compound Protein, l ipid, polysaccharide (andtheir complex)
Composition Single antigen, multiple antigenSource Native, recombinantIg class IgG, IgA, IgG (single or combined)Laboratory
techniqueEnzyme-linked immunosorbent
assay, immunochromatography,immunodot rapid test, kaolinagglutination test
Diagnosis of tuberculosis 227
2010 The AuthorsJournal compilation 2010 Asian Pacic Society of Respirology Respirology (2010) 15 , 220240
-
8/6/2019 Advances in TB Diagnostics
9/21
Tuberculin skin test
The TST was developed by the Austrian paediatricianClemens v. Pirquet as an allergy-test for the diagnosisof tuberculosis in children. 187 It has been the standardtest for the immunodiagnosis of tuberculosis sincethe beginning of the 20th century. Despite the recentinvention of IGRA, the TST is still much more widely used as a screening method for the identication of persons with a positive immune response against M. tuberculosis .188
A standard preparation of puried protein derivate(PPD), an extract of the sterile supernatant of M. tuberculosis -cultered ltrate, is administeredintradermaly and results in a delayed type hypersen-sitivity reaction represented by a local skin indura-tion. 189 For the best test result reliability, TST reactionsin humans are ascertained by the diameter of indura-tion, measured 4872 h after antigen injection withthe ballpoint technique. 190
A recent meta-analysis stated that the overall sen-sitivity of the TST for active tuberculosis is 77%; 191
however, the sensitivity of the test canbe dramatically impaired, for example, in infants and toddlers 192 as well as in elderly persons, 193 in individuals with con-genital or acquired immunodeciencies (e.g. those with HIV infection 194196), patients being treated withcorticosteroids 197 or other immunosuppressivedrugs, 198 patients with chronic renal failure, 199,200 mal-nutrition, 201,202 cancer 203 or overt forms of tuberculo-sis. 204,205 The specicity of theTST is dependent on theBCG vaccination status 206 and the immune status of the individual who is tested. 191 Cross-reactivity of antigens may result in a positive TST reaction afterexposure to NTM 207 or following M. bovis BCG vacci-nation. 206,208 TST induration reactions exceeding
15 mm are likely related to tuberculosis or LTBI,209
irrespectively of the BCG vaccination status. 210 Whilethe sensitivity of the TST decreases from a cut-off of 5to 10 and 15 mm, the specicity of the TST increases with the increase of the cut-off used to dene a posi-tive induration. 211,212 Depending on the level of expo-sure to an index case in contact tracing and theimmune status of the individual, different cut-offs fora positive test reaction have been recommendedranging from 5- to 15-mm induration. 213 Recently,results of a phase I trial of a skin test that uses recom-binant early secretory antigenic target (ESAT)-6instead of tuberculin have demonstrated safety andtolerability of such a test. 214 In combination withculture ltrate protein (CFP)-10 antigen to increasediagnostic sensitivity, such a skin test could overcomesome of the obstacles currently related to the use of the TST. If clinical trials show superiority to the TSTthis test could be made widely available for the diag-nosis of LTBI in resource-limited settings where theuse of IGRA is prohibited by their costs and demandsfor an established laboratory infrastructure.
Interferon- g release assays
Introduction of IGRA into clinical practice is regardedby many as the most important development in the
diagnosis of M. tuberculosis infection over the lastdecade. IGRA isa couplingof thediscovery ofantigensESAT-6 and CFP-10, which are relatively specic to M. tuberculosis ,215 and the development of simpliedtechnologies of measuring interferon- g . There are twocommercialized systems for the latter technology.QuantiFERON-Gold (QFT-G) (Cellestis Ltd, Carnegie, Australia 216) measures interferon- g in IU/mL using an
enzyme-linked immunosorbent assay (ELISA) andT-SPOT.TB (Oxford Immunotec Ltd, Abingdon, UK 217)counts the cells releasing interferon- g visualized asspots withthe enzyme-linkedimmunospot (ELISPOT)technique. During the last severalyears, these systemshave been approvedin various countriesandthend-ings of their diagnostic performance have been accu-mulated and characterized. The QFT-G test is now availableas anin tube version(QFT-G-IT),whichalsoincludes, in addition to ESAT-6 and CFP-10, theantigen TB7.7. We present a summary of the perfor-mance of these systems in various settings, based onreview and meta-analysis. 191,218 IGRA were originally intended to diagnose LTBI, but because there is no
gold standard of tuberculosis infection, the activedisease is usually used as a surrogate for the infection when quantifying sensitivity. Specicity is measuredin subjects with low risk of M. tuberculosis infection,for example, healthy young subjects without knowncontact with tuberculosis patients.
As indicated in Table 4, the specicity of IGRA isconsistently high and obviously superior to TST, whereas sensitivity is rather variable between studies.This variability may be greatly ascribed to thedifference in patients characteristics in terms of tuberculosis disease condition, age, extent of immu-nosuppression due to underlying illnesses, etc.However, IGRA generally perform better than TST in
its sensitivity. Comparing QFT-G and T-SPOT.TB,T-SPOT.TB seems to be more sensitive than QFT-G,and vice versa for specicity. This comparison isclearer when they are compared head to head in thesamesubjects. 191 Thesameisalsotrueforthecompari-son between QFT-G and QFT-G-IT, where the latterexhibits higher sensitivity in head-to-head compari-son, 219 perhaps due to addition of the third antigenTB7.7, while the difference was in an opposite direc-tion in the comparison between the different subjectgroups, as seen in series 1 and series 2 in Table 4.
The performance of the IGRA for the immuno-diagnosis of M. tuberculosis infection has beeninvestigated in immunocompromised hosts, suchas in HIV-infected, 195,220233 elderly, 234236 chronic-renal-failure 237239 patients and those taking corticosteroids 240242 or TNF-alpha blockers. 243248 Ingeneral, the responses to IGRA (T-SPOT.TB > QFT-G-IT) are more frequently present in individuals fromthese patient groups when compared with the TST.This is commonly interpreted that these assays aresuperior to the TST to detect LTBI. 218,233
Apart from the performance using tuberculosispatients as surrogates of M. tuberculosis infection,there are arguments concerning the discordancebetween IGRA and TST in those suspected of recentinfection. 249,250 However, it is now considered thatIGRA may reect the dynamics of infection immunity
C Lange and T Mori 228
2010 The AuthorsJournal compilation 2010 Asian Pacic Society of RespirologyRespirology (2010) 15 , 220240
-
8/6/2019 Advances in TB Diagnostics
10/21
more sensitively, so that the interferon- g level may uctuate above and below the cut-off. 251 Similarconcern is raisedabout thepredictability of the futureclinical development according to the IGRA responselevel, which is the main purpose of testing contactsfor possible latent infections. One report suggests thehigher risk of developing tuberculosis in cases withhigher response at the time of infection. 252 This shouldbe further conrmed and the discussion should beexpanded to the level of response that persists aftermany years of infection.
For the diagnosis of tuberculosis in non-immunocompromised hosts the best useof IGRA is torule out active tuberculosis, 186 as the negative predic-tive value for tuberculosis is higher than 95% if com-bined IGRA and TST test results are negative. 253,254
Other biomarkers for tuberculosis diseasestatus and diagnosis
Evaluation of otherbiomarkers for active tuberculosisor LTBI is a research priority in the eld of tuberculo-sis. The details on the advances that have beenachieved in the search for new biomarkers haverecently been reviewed 255262 and they are beyond thescope of this review (a selection of methods underdevelopment for the diagnosis of tuberculosis isshown in Table 5).
Based on the IGRA technology, other combinationsof M. tuberculosis -specic antigens 253,254,273275 andcytokine readouts 265,276 are being explored to improvethe accuracy of these assays for the diagnosis of tuberculosis and LTBI.
Among the biomarkers under investigation,interferon-induced protein IP-10, a CXC chemokineand monocyte chemoattractant protein MCP-2, a CCchemokine, have been clinically evaluated. 266,276279
When quantied in the supernatants from wholeblood stimulated with ESAT-6 and CFP-10 antigens inindividuals with tuberculosis IP-10 > MCP-2 wasfound highly upregulated, when compared with pre-sumptively uninfected controls. 279 However, the diag-nostic accuracy of the IP-10 or MCP-2 assay was notsuperior when compared with the QFT-G-IT assay and this test was also not able to identify individuals with active tuberculosis when performed with cellsfrom the peripheral blood.
Local immunodiagnosis for active tuberculosisby IGRA
The inability to distinguish individuals with activetuberculosis from those with LTBI by blood tests islikely related to the fact that effector memory T cellsare nothighly prevalent in this compartment in activedisease. 254,280,281 However, in active tuberculosisantigen-specic T cells clonally expand and areconcentrated at the site of infection. 22,51,71,78,282286 Insuspects of tuberculosis with negative AFB sputumsmears, comparison of systemic (peripheral blood)and local (BAL) T cell responses against mycobacte-rial antigens assayed by ELISPOT are useful to rapidly distinguish cases of active pulmonary tuberculosisfrom those with LTBI. 165,287289 As the majority of patients with active pulmonary tuberculosis havenegative AFB sputum smears, local immunodiagnosisfor active tuberculosis by BAL-ELISPOT can have animportant impact on the early diagnosis of tubercu-losis. In a recent clinical trial local immunodiagnosisfor mycobacteria-specic T cellsbyBAL-ELISPOT hada sensitivity and specicity for the detection of sputum AFB smear-negative pulmonary tuberculosisof 91% and 80%, respectively. 165 BAL-ELISPOT wasmarkedly more sensitive for the rapid diagnosis of
Table 4 Summary sensitivity and specicity of IGRA (meta-analysis)
Series Diagnostics Subject No. studies Summary Range
Sensitivity1 QFT-G TB patients, adult 21 0.80 (0.780.82) 0.620.952 QFT-G-IT TB patients, adult 6 0.74 (0.690.78) 0.640.933 QFT-G/G-IT TB patients, child 9 0.82 (0.750.87) 0.531.00
4 QFT-G/G-IT, T-SPOT.TB HIV-infected TB patients 5 0.70 (0.600.79) 0.630.857 T-SPOT.TB TB patients 13 0.90 (0.860.93) 0.831.008 TST Healthy subjects 20 0.77 (0.710.82) 0.571.00Specicity1 QFT-G/G-IT Healthy young adults 12 0.98 (0.970.99) 0.921.002 QFT-G/G-IT Healthy young adults, BCG( - ) 8 0.99 (0.981.00) 0.951.003 QFT-G/G-IT Healthy young adults, BCG( + ) 8 0.96 (0.940.98) 0.890.994 T-SPOT.TB Predominantly BCG vaccinated 8 0.93 (0.861.00) 0.851.005 TST BCG not vaccinated 6 0.97 (0.950.99) 0.931.006 TST BCG vaccinated 6 0.59 (0.460.73) 0.350.79
Figures in parentheses in column Summary indicate 95% condence limits. For specicity, several studies underseries 1 are included in series 2 or 3.
IGRA, interferon-gamma release assay; QFT-G, QuantiFERON-TB Gold; QFT-G-IT, QuantiFERON-TB Gold In-Tube; TB,tuberculosis; TST, tuberculin skin test.
Diagnosis of tuberculosis 229
2010 The AuthorsJournal compilation 2010 Asian Pacic Society of Respirology Respirology (2010) 15 , 220240
-
8/6/2019 Advances in TB Diagnostics
11/21
T a
b l e 5
S e l e c t e d m e t h o d s u n d e r
i n v e s t i g a t i o n f o r t h e d i a g n o s i s o f t u b e r c u l o s i s
M e t h o d
I n v e s t i g a t i o n a l t a r g e t
S p e c i m e n
S e n s i t i v i t y / s p e c i c i t y
T e s t r e s u l t s
a v a i l a b l e w i t h i n
C i t a t i o n
F A C S a n a l y s i s o f s h o r t - t e r m s t i m u l a t e d
b l o o d o r c e l l c u l t u r e s
F r e q u e n c y o f C D 2 7 +
l y m p h o c y t e s
B l o o d
1 0 0 % / 8 6 %
2 4 h
2 6 3
I d e n t i c a t i o n o f i n t r a c e l l u l a r I F N - g
S p u t u m
8 9 % / 8 0 %
2 4 h
2 6 4
I d e n t i c a t i o n o f I F N - g - a n d I L - 2 - s e c r e t i n g
c e l l s
B l o o d
N o t y e t d e t e r m i n e d
2 4 h
2 6 5
C h e m o k i n e p r o d u c t i o n f o l l o w i n g
s t i m u l a t i o n w i t h E S A T - 6
/ C F P 1 0 / T B 7 . 7
I F N - g - i n
d u c i b l e p r o t e i n I P - 1 0
B l o o d
8 2 % / 9 7 %
2 4 h
2 6 6
I F N - g - p r o d u c t i o n f o l l o w i n g s t i m u l a t i o n
w i t h E S A T - 6
/ C F P 1 0
I d e n t i c a t i o n o f I F N - g - s e c r e t i n g c e l l s
B A L
9 1 % / 8 0 %
2 4 h
1 6 5
I d e n t i c a t i o n o f I F N - g - s e c r e t i n g c e l l s
P l e u r a l u i d
9 5 % / 7 6 %
2 4 h
2 2
I d e n t i c a t i o n o f I F N - g
g - s e c r e t i n g c e l l s
C e r e b r o s p i n a l u i d
9 0 % / 1 0 0 %
2 4 h
5 1
I d e n t i c a t i o n o f I F N - g - s e c r e t i n g c e l l s
P e r i t o n e a l u i d
8 9 % / 7 8 %
2 4 h
7 1
I F N - g - p r o d u c t i o n f o l l o w i n g s t i m u l a t i o n
w i t h a n t i g e n s d i f f e r e n t f r o m E S A T - 6 /
C F P 1 0
I F N - g p r o d u c t i o n f o l l o w i n g s t i m u l a t i o n
w i t h h e p a r i n - b i n d i n g h e m a g g l u t i n i n
B l o o d
9 2 % / 9 4 %
4 d a y s
2 6 7
I F N - g p r o d u c t i o n f o l l o w i n g s t i m u l a t i o n
w i t h R v 3 8 7 9 c p e p t i d e s i n a d d i t i o n t o
E S A T - 6 a n d C F P 1 0
B l o o d
8 9 % / 6 9 %
2 4 h
2 5 3
I F N - g p r o d u c t i o n f o l l o w i n g s t i m u l a t i o n
w i t h R D - 1 s e l e c t i v e p e p t i d e s
B l o o d
7 3 % / 7 1 %
2 4 h
2 5 4
P r o t e o m i c s
M a s s s p e c t r o m e t r y a n a l y s i s o f s e r u m
p r o t e i n s t o i d e n t i f y a T B - s p e c i c
n g e r p r i n t
B l o o d
9 4 % / 9 5 %
S e v e r a l d a y s
2 6 8
D e t e c t i o n o f M T B - s p e c i c c e l l w a l l
c o m p o n e n t s
L i p o a r a b i n o m a n n a n
U r i n e
1 8 % / 8 8 %
4 h
2 6 9
G o l d n a n o p a r t i c l e p r o b e a s s a y
H y b r i d i z a t i o n o f M T B - s p e c i c
D N A w i t h
g o l d n a n o p a r t i c l e p r o b e s
S p u t u m
9 5 % / 1 0 0 %
2 4 h
2 7 0
L o o p m e d i a t e d i s o t h e r m a l a m p l i c a t i o n
a s s a y
H y b r i d i z a t i o n o f M T B - s p e c i c
D N A
S p u t u m
1 0 0 % / 9 4 %
2 4 h
2 7 1
B r e a t h t e s t
I d e n t i c a t i o n o f v o l a t i l e b i o m a r k e r s
B r e a t h
8 3 % / 1 0 0 %
2 4 h
2 7 2
B C G
, B a c i l l e C a l m e t t e G u e r i n ; C D
, c l u s t e r o f d i f f e r e n t i a t i o n ; F A C S , u o r e s c e n c e a c t i v a t e d c e l l s o r t i n g ; I F N - g ,
i n t e r f e r o n - g ; L T B I , l a t e n t t u b e r c u l o s i s i n f e c t i o n ; M T B
,
M y c o b a c t e r i u m t u b e r c u l o s i s ; R D , r e g i o n o f d i f f e r e n c e .
T h e r e p o r t e d s e n s i t i v i t i e s a n d s p e c i c i t i e s f r o m t h e s e p i l o t s t u d i e s m a y n o t r e e c t t h e d i a g n o s t i c a c c u r a c y o f t h e t e s t s i n c l i n i c a l p r a c t i c e .
C Lange and T Mori 230
2010 The AuthorsJournal compilation 2010 Asian Pacic Society of RespirologyRespirology (2010) 15 , 220240
-
8/6/2019 Advances in TB Diagnostics
12/21
sputum AFB smear-negative tuberculosis than M. tuberculosis -specic NAAT. A similar diagnosticaccuracy of the BAL-ELISPOT for the diagnosis of AFBsmear-negative pulmonary tuberculosis was recently observed in a study performed in the Republic of South Africa, although in this study up to 1/3 of testresults were inconclusive due to failure of the positiveand negative controls. 290
In countries of high tuberculosis incidence, pulmo-nary immune responses to antigens of M. tuberculosis assayed by ELISPOT may be different from thoseobserved in individuals from areasof low incidenceof tuberculosis due to the frequent exposure to M. tuber-culosis .291 For clinicians, BAL-ELISPOT may thus bemost applicable for a rapid decision to initiate anti-tuberculosis treatment in countries of low tuberculo-sis incidence, where bronchoscopy is routinely performed for individuals suspected to be affected by sputum AFB smear-negative tuberculosis and wherethe technology for ELISPOT is available.
Fluorescence-activated cell sortingImmunophenotyping of antigen-stimulated cells by uorescence-activated cell sorting of BAL cells 286,292,293or sputumcells 264 has also been performed in order toobtain a rapid diagnosis of tuberculosis in suspects with negative AFB sputum smears. While multicolourow cytometry analysis allows for a better identica-tion of cell populations that react following antigenencounter, the method is technically more demand-ing than IGRA for the immunodiagnosis of tubercu-losis. In individuals with LTBI, BAL cells 294 andsputum T cells 264 are preferentially enriched for PPD-specic lymphocytes, and ow cytometry assays
stimulated with PPD do not distinguish individuals with active tuberculosis and LTBI. Unfortunately, thefrequency of region of difference-1 M. tuberculosis -specic T cells is too low in the sputum to be used asstimulants for ow cytometry cultures and otherimmune based assays. 264,295 However, where available,ow cytometry is a very promising tool to furtherimprove the diagnostic accuracy of local immuno-diagnostic assays for the diagnosis of AFB smear-negative tuberculosis. 286
Other possibilities of tuberculosis diagnosis
Being the science of the structure and function of proteins, proteomics has identied proteins signi-cant as diagnostic or prognostic biomarkers, or astherapeutic targets in a range of illnesses, including tuberculosis. 296298 Agranoff et al . applied this tech-nique to analysis of serum proteomic ngerprinting,or individual recognition of proteomic prole, forthe purpose of distinguishing subjects with and without tuberculosis. 268 Its diagnostic efcacy wasfairly good with sensitivity of 93.5% and specicity of 94.9%. Also, to translate from proteomic signaturesto conventional test formats, they identied amyloid A and transthyretin from highly informative peaks,and measured their levels by immunoassay, together
with previously known parameters of C-reactiveprotein and neopterin. The combination of thesefour biomarkers provided diagnostic accuracies upto 84%. 268
Apart from serological diagnosis, lipoarabinoman-nan is considered as an attractive urine marker in anantigen capture ELISA-based system for detecting tuberculosis. According to the evaluations of a com-
mercial kit, both sensitivity of this lipoarabinoman-nan ELISA were low, 269 but the sensitivity was greaterin HIV-seropositive subjects in some of the stud-ies, 299,300 which suggests the possible efcacy to use itin combination with sputum smear examination inHIV-infected patients.
CONCLUSION
The good combination of diagnosis and treament isthe most critical element of tuberculosis control andit will remain so until the advent of novel vaccines or
drugs powerful enough to prevent development of tuberculosis perfectly. In the middle of the 20thcentury the treatment of tuberculosis made a revolu-tionary progress with the development of a series of chemotherapeutics, while only very little change wasseen in the diagnostics. This caused disruption of theabove combination leading to a low case detectionrate in contrast with a fairly high treatment successrate as we see today worldwide. However, tuberculo-sis control is not possible, if the diagnosis of activecases is delayed as M. tuberculosis continues to betransmitted from cases to contacts. In addition, falsepositve diagnosis of LTBI has caused unnecessary burden to individuals and healthcare systems.
The urgent need for innovation in diagnostics isobvious.However, it is good to see that the changes in diag-
nostics have started towards the end of the lastcentury, assistedby the progressof biotechnologyandthe late risers alertness to the problem. The balancebetween developments in the diagnosis and in thetreatment of tuberculosis has changed. Recent diag-nostic advances overweigh the inefcient progress of new drug development against tuberculosis by far.Today, we have the technology to rapidly identify indi-viduals with smear-positive MDR or XDR tuberculo-sis, but we do not have the drugs to treat thesepatients adequately. 8,301
This article has overviewed such changing aspectsof each of the established diagnostic techniques assummarized in Table 6. Every technique listed here was discussed in respective chapters focussing on itscurrent and possible further improvement. Also, wehave reviewed the ongoing efforts of innovations fornovel modalities. Many of them are quite promising,so that we will be able to make it out of the anti-quated techniques and make a full use of new tech-niques tted to various situations. Only in that way can we combine our case-nding activities well with treatment services that are still progressing inorder to make our tuberculosis control maximally effective.
Diagnosis of tuberculosis 231
2010 The AuthorsJournal compilation 2010 Asian Pacic Society of Respirology Respirology (2010) 15 , 220240
-
8/6/2019 Advances in TB Diagnostics
13/21
-
8/6/2019 Advances in TB Diagnostics
14/21
ACKNOWLEDGEMENTS
The authors thank Dr Martina Sester (University of Saarland, Homburg, Germany) for stimulating discussions on the diagnosis of tuberculosis.
REFERENCES
1 WHO. Global Tuberculosis Control 2009 . Epidemiology,Strategy, Financing, Geneva, 2009.
2 Pai M, OBrien R. New diagnostics for latent and active tuber-culosis: state of the art and future prospects. Semin. Respir.Crit. Care Med. 2008; 29 : 56068.
3 Newton SM, Brent AJ, Anderson S et al. Paediatric tuberculosis.Lancet Infect. Dis. 2008; 8: 498510.
4 Lopez AD, Mathers CD. Measuring the global burden of diseaseand epidemiological transitions: 2002-2030. Ann. Trop. Med.Parasitol. 2006; 100 : 48199.
5 Stevenson CR, Forouhi NG, Roglic G et al. Diabetes and tuber-culosis: the impact of the diabetes epidemic on tuberculosisincidence. BMC Public Health 2007; 7: 234.
6 Tubach F, Salmon D, Ravaud P et al. Risk of tuberculosis ishigher with anti-tumor necrosis factor monoclonal antibody therapy than with soluble tumor necrosis factor receptortherapy: the three-year prospective french research axed ontolerance of biotherapies registry. Arthritis Rheum. 2009; 60 :188494.
7 WHO/IUATLD. Global Project on Antituberculosis Drug Resis-tance Surveillance . Anti-Tuberculosis Drug Resistance in the World, Geneva, 2008.
8 Sotgiu G, Ferrara G, Matteelli A et al. Epidemiology and clinicalmanagement of XDR-TB: a systematic review by TBNET. Eur.Respir. J. 2009; 33 : 87181.
9 Gie RP, Matiru RH. Supplying quality-assured child-friendly anti-tuberculosis drugs to children [Editorial]. Int. J. Tuberc.Lung Dis. 2009; 13 : 2778.
10 CDC. Reported Tuberculosis in the United States, 2007 . U.S.Department of Health and Human Services, Atlanta, GA, 2008.
11 EuroTB.Reporton tuberculosiscasesnotiedin 2005. [Accessed20 Dec 2009.] Available from URL: http://www.eurotb.org.12 Bloom BR,SalomonJA. Enlightenedself-interest andthe control
of tuberculosis [Editorial]. N.Engl. J.Med. 2005; 353 : 10579.13 Villegas MV, Labrada LA, Saravia NG. Evaluation of polymerase
chain reaction, adenosine deaminase, and interferon-gammain pleural uid for the differential diagnosis of pleural tubercu-losis. Chest 2000; 118 : 135564.
14 Nagesh BS, Sehgal S, Jindal SK et al. Evaluation of polymerasechain reaction for detection of Mycobacterium tuberculosis inpleural uid. Chest 2001; 119 : 173741.
15 Lima DM, Colares JK, da Fonseca BA. Combined use of thepolymerase chain reaction and detection of adenosine deami-nase activity on pleural uid improves the rate of diagnosis of pleural tuberculosis. Chest 2003; 124 : 90914.
16 Kim SY, Park YJ, Kang SJ et al. Comparison of the BDProbeTec
ET system with the roche COBAS AMPLICOR system for detec-tion of Mycobacterium tuberculosis complex in the respiratory and pleural uid specimens. Diagn.Microbiol. Infect. Dis. 2004;49 : 1318.
17 Zemlin AE, Burgess LJ, Carstens ME. The diagnostic utility of adenosine deaminase isoenzymes in tuberculous pleural effu-sions. Int. J. Tuberc. Lung Dis. 2009; 13 : 21420.
18 Baba K, Hoosen AA, Langeland N et al. Adenosine deaminaseactivity is a sensitive marker for the diagnosis of tuberculouspleuritis in patients with very low CD4 counts. PLoS ONE 2008;3: e2788.
19 Liang QL, Shi HZ, Wang K et al. Diagnostic accuracy of adenos-ine deaminase in tuberculous pleurisy: a meta-analysis. Respir. Med. 2008; 102 : 74454.
20 Greco S, Girardi E, Masciangelo R et al. Adenosine deaminaseand interferon gamma measurements for the diagnosis of tuberculous pleurisy: a meta-analysis. Int. J. Tuberc. Lung Dis.2003; 7: 77786.
21 Jiang J, Shi HZ, Liang QL et al. Diagnostic value of interferon-gamma in tuberculous pleurisy: a metaanalysis. Chest 2007;131 : 113341.
22 Losi M, Bossink A, Codecasa L et al. Use of a T-cell interferon-{gamma}releaseassay for thediagnosis of tuberculouspleurisy.
Eur. Respir. J. 2007; 30 : 11739.23 Lange C, Hellmich B, Ernst M et al. Rapid immunodiagnosis of
tuberculosis in a woman receiving anti-TNF therapy. Nat.Clin.Pract. Rheumatol. 2007; 3: 52834.
24 Kobashi Y, Shimizu H, Mouri K et al. Rapid diagnosis of tuber-culous pleuritis by a T-cell interferon-gamma release assay.Scand. J. Infect. Dis. 2009; 41 : 2326.
25 Lee LN, Chou CH, Wang JY et al. Enzyme-linked immunospotassay for interferon-gamma in the diagnosis of tuberculouspleurisy. Clin. Microbiol. Infect. 2009; 15 : 1739.
26 Hooper CE, Lee YC, Maskell NA. Interferon-gamma releaseassays for the diagnosis of TB pleural effusions: hype or realhope? Curr. Opin. Pulm. Med. 2009; 15 : 35865.
27 Hasaneen NA, Zaki ME, Shalaby HM et al. Polymerase chainreaction of pleural biopsy is a rapid and sensitive method forthe diagnosis of tuberculous pleural effusion. Chest 2003; 124 :210511.
28 Gopi A, Madhavan SM, Sharma SK et al. Diagnosis and treat-ment of tuberculous pleural effusion in 2006. Chest 2007; 131 :88089.
29 Schaaf B, Zumla A. Tuberculosis . Elsevier, Europe, 2009.30 Peel MM, Palmer GG, Stacpoole AM et al. Human lymphadeni-
tis due to Corynebacterium pseudotuberculosis: report of tencases from Australia and review. Clin. Infect. Dis. 1997; 24 : 18591.
31 Jain AK, Dhammi IK. Tuberculosis of the spine: a review. Clin.Orthop. Relat. Res. 2007; 460 : 3949.
32 Dunn R, Zondagh I. Spinal tuberculosis: diagnostic biopsy ismandatory. S. Afr. Med. J. 2008; 98 : 36062.
33 Abou-Raya S, Abou-Raya A. Spinal tuberculosis: overlooked? J. Intern. Med. 2006; 260 : 16063.
34 Lange CG, Getty PJ, Morrissey AB et al. Destructive osteoarthri-tis after delayed diagnosis of tuberculosis. Infection 2002; 30 :469.
35 Akman M, Sirvanci M, Talu U et al. Magnetic resonace imaging of tuberculous spondylitis. Orthopedics 2003; 26 : 6973.
36 Jung NY, Jee WH, Ha KY et al. Discrimation of tuberculousspondylitis from pyogenic spondylitis on MRI. Am. J.Roentgenol. 2004; 182 : 140510.
37 Anik Y, Ciftci E, Sarisoy HT et al. MR spectroscopy ndings intuberculous spondylitis; comparison with Modic type-I end-plate changes and metastatic vertebral disease. Eur. J. Radiol.2009; 71 : 32432.
38 Harada Y, Tokuda O, Matsunaga N. Magnetic resonanceimaging characteristics of tuberculous spondylitis vs. pyogenicspondylitis. Clin. Imaging 2008; 32 : 3039.
39 Hussain SF, Irfan M, Abbasi M et al. Clinical characteristics of
110 miliary tuberculosis patients from a low HIV prevalencecountry. Int. J. Tuberc. Lung Dis. 2004; 8: 4939.
40 Sharma SK, Mohan A, Sharma A et al. Miliary tuberculosis: new insights into an old disease. Lancet Infect. Dis. 2005; 5: 41530.
41 Fujita J, Bandoh S, Kubo A et al. HRCT shows variations inappearance in disseminated tuberculosis in adults. Int. J.Tuberc. Lung Dis. 2006; 10 : 2226.
42 Pipavath SNJ, Sharma SK, Sinha S et al. High resolution CT(HRCT) in miliary tuberculosis (MTB) of the lung: correlation with pulmonary function test & gas exchange parameters innorth Indian patients. Indian J. Med Res. 2007; 126 : 1938.
43 Sawy MS,Jayakrishnan B, Behbehani N et al. Flexible beropticbronchoscopy. Diagnostic yield. Saudi. Med. J. 2004; 25 : 145963.
Diagnosis of tuberculosis 233
2010 The AuthorsJournal compilation 2010 Asian Pacic Society of Respirology Respirology (2010) 15 , 220240
-
8/6/2019 Advances in TB Diagnostics
15/21
44 Escobedo-Jaimes L, Cicero-Sabido R, Criales-Cortez JL et al.Evaluation of the polymerase chain reaction in the diagnosis of miliary tuberculosis in bone marrow smear. Int. J. Tuberc.Lung Dis. 2003; 7: 58086.
45 Golden MP, Vikram HR. Extrapulmonary tuberculosis: an over-view. Am. Fam. Physician 2005; 72 : 17618.
46 Scarborough M, Thwaites GE. The diagnosis and managementof acute bacterial meningitis in resource-poor settings. Lancet Neurol. 2008; 7: 63748.
47 Baveja CP, Gumma V, Jain M et al. Newer methods over theconventional diagnostic tests for tuberculous meningitis: dothey really help? Trop. Doct. 2009; 39 : 1820.
48 Caws M, Dang TM, Torok E et al. Evaluation of the MODSculture technique for the diagnosis of tuberculous meningitis.PLoS ONE 2007; 2: e1173.
49 HaldarS, Sharma N, GuptaVK et al. Efcient diagnosis of tuber-culous meningitis by detection of Mycobacterium tuberculosisDNA in cerebrospinal uid ltrates using PCR. J. Med. Micro-biol. 2009; 58 : 61624.
50 Takahashi T, Tamura M, Asami Y et al. Novel wide-range quan-titative nested real-time PCR assay for Mycobacterium tuber-culosis DNA: development and methodology. J.Clin.Microbiol.2008; 46 : 170815.
51 Thomas MM, Hinks TS, Raghuraman S et al. Rapid diagnosisof Mycobacterium tuberculosis meningitis by enumeration of cerebrospinal uid antigen-specic T-cells. Int. J. Tuberc. Lung Dis. 2008; 12 : 6517.
52 Kosters K, Nau R, Bossink A et al. Rapid diagnosis of CNStuberculosis by a T-Cell interferon-gamma release assay oncerebrospinal uid mononuclear cells. Infection 2008; 36 : 597600.
53 Pai M, Ling DI. Rapid diagnosis of extrapulmonary tuberculosisusing nucleic acid amplication tests: what is the evidence?Future Microbiol. 2008; 3: 14.
54 Restrepo BI, Pino PA, Volcy M et al. Interpretation of myco-bacterial antibodies in the cerebrospinal uid of adults withtuberculous meningitis. Trop. Med. Int. Health 2008; 13 : 6538.
55 Senol G, Ecevit C, Ozturk A. Humoral immune response against38- and 16-kDa mycobacterial antigens in childhood tubercu-losis. Pediatr. Pulmonol. 2009; 44 : 83944.
56 Murakami S, Takeno M, Oka H et al. Diagnosis of tuberculousmeningitis due to detection of ESAT-6-specic gamma inter-feron production in cerebrospinal uid enzyme-linked immu-nospot assay. Clin. Vaccine Immunol. 2008; 15 : 8979.
57 Sonmez G, Ozturk E, Sildiroglu HO et al. MRI ndings of intrac-ranial tuberculomas. Clin. Imaging 2008; 32 : 8892.
58 Oztoprak I, Gumus C, Oztoprak B et al. Contrast medium-enhanced MRI ndings and changes over time in stage I tuber-culous meningitis. Clin. Radiol. 2007; 62 : 120615.
59 Janse van Rensburg P, Andronikou S, van Toorn R et al. Mag-netic resonance imaging of miliary tuberculosis of the centralnervous system in children with tuberculous meningitis.Pediatr. Radiol. 2008; 38 : 130613.
60 Pienaar M, Andronikou S, van Toorn R. MRI to demonstratediagnostic features and complications of TBM not seen withCT. Childs Nerv. Syst. 2009; 25 : 9417.
61 Andronikou S, van Toorn R, Boerhout E. MR imaging of theposterior hypophysis in children with tuberculous meningitis.Eur. Radiol. 2009; 19 : 224954.
62 LeeJ, PastagiaM. Peritoneal tuberculosis. Int.J. Infect.Dis. 2009;13 : 117.
63 Poyrazoglu OK, Timurkaan M, Yalniz M et al. Clinical review of 23 patients with tuberculous peritonitis: presenting featuresand diagnosis. J. Dig. Dis. 2008; 9: 17074.
64 Que Y, Tao C, Wang Y et al. Nodules in the thickened greateromentum: a good indicator of lesions? J. UltrasoundMed. 2009;28 : 7458.
65 Que Y, Wang X, Liu Y et al. Ultrasound-guided biopsy of greateromentum: an effective method to trace the origin of unclearascites. Eur. J. Radiol. 2009; 70 : 3315.
66 Tongsong T, Sukpan K, Wanapirak C et al. Sonographicfeaturesof female pelvic tuberculous peritonitis. J. Ultrasound Med.2007; 26 : 7782.
67 Bedioui H, Ksantini R, Nouira K et al. Role of laparoscopicsurgery in the etiologic diagnosis of exsudative ascites: a pro-spective study of 90 cases. Gastroenterol. Clin. Biol. 2007; 31 :11469.
68 Krishnan P, Vayoth SO, Dhar P et al. Laparoscopy in suspectedabdominaltuberculosisis useful as an early diagnostic method.
ANZ J. Surg. 2008; 78 : 9879.69 Meshikhes AW. Pitfalls of diagnostic laparoscopy in abdominal
tuberculosis. Surg. Endosc. 2009; doi 10.1007/s00464-009-0692-z.
70 Wang WN, Wallack MK, Barnhart S et al. Tuberculous peritoni-tis: denitive diagnosis by laparoscopic peritoneal biopsy. Am.Surg. 2008; 74 : 12234.
71 Kim SH, Cho OH, Park SJ et al. Diagnosis of abdominal tuber-culosis by T-cell-based assays on peripheral blood and perito-neal uid mononuclear cells. J. Infect. 2009; 59 : 40915.
72 Ariga H, Kawabe Y, Nagai H et al. Diagnosis of active tubercu-lousserositis byantigen-specicinterferon-gamma responseof cavity uid cells. Clin. Infect. Dis. 2007; 45 : 155967.
73 Riquelme A, Calvo M, Salech F et al. Value of adenosine deami-nase (ADA) in ascitic uid for the diagnosisof tuberculous peri-tonitis: a meta-analysis. J. Clin. Gastroenterol. 2006; 40 : 70510.
74 Imazio M, Brucato A, Derosa FG et al. Aetiological diagnosis inacute and recurrent pericarditis: when and how. J. Cardiovasc. Med. (Hagerstown) 2009; 10 : 21730.
75 Mayosi BM, Burgess LJ, Doubell AF. Tuberculous pericarditis.Circulation 2005; 112 : 360816.
76 Reuter H, Burgess LJ, Schneider J et al. The role of histopathol-ogy inestablishingthe diagnosis of tuberculouspericardialeffu-sions in the presence of HIV. Histopathology 2006; 48 : 295302.
77 Zamirian M, Mokhtarian M, Motazedian MH et al. Constrictivepericarditis: detection of mycobacterium tuberculosis inparafn-embedded pericardial tissues by polymerase chainreaction. Clin. Biochem. 2007; 40 : 3558.
78 Biglino A, Crivelli P, Concialdi E et al. Clinical usefulness of ELISPOTassayon pericardialuid in a case of suspectedtuber-
culous pericarditis. Infection 2008; 36 : 6014.79 Jolobe OM. Interferon-gamma may be a better test for tubercu-lous pericarditis. Am. J. Med. Sci. 2008; 336 : 215; author reply 2156.
80 Arroyo M, Soberman JE. Adenosine deaminase in the diagnosisof tuberculous pericardial effusion. Am. J. Med. Sci. 2008; 335 :2279.
81 Reuter H, Burgess L, van Vuuren W et al. Diagnosing tubercu-lous pericarditis. QJM 2006; 99 : 82739.
82 Tuon FF, Silva VI, Almeida GM et al. The usefulness of adenos-ine deaminase in the diagnosis of tuberculous pericarditis. Rev.Inst. Med. Trop. Sao Paulo 2007; 49 : 16570.
83 George S, Salama AL, Uthaman B et al. Echocardiography indifferentiating tuberculous from chronic idiopathic pericardialeffusion. Heart 2004; 90 : 13389.
84 Kim SH, Song JM, Jung IH et al. Initial echocardiographic char-
acteristics of pericardial effusion determine the pericardialcomplications. Int. J. Cardiol. 2009; 136 : 1515.
85 Zagol B, Minderman D, Munir A et al. Effusiveconstrictiveperi-carditis: 2D, 3D echocardiography and MRI imaging. Echocar-diography 2007; 24 : 111014.
86 Ha JW, Ko YG, Choi BW. Images in cardiology. Delayed hyper-enhancement of the pericardium by magnetic resonanceimaging as a marker of pericardial inammation in a patient with tuberculous effusive constrictive pericarditis. Heart 2006;92 : 494.
87 Habashy AG, Mittal A, Ravichandran N et al. The electrocardio-gram in large pericardial effusion: the forgotten P wave andthe inuence of tamponade, size, etiology, and pericardialthickness on QRS voltage. Angiology 2004; 55 : 3037.
C Lange and T Mori 234
2010 The AuthorsJournal compilation 2010 Asian Pacic Society of RespirologyRespirology (2010) 15 , 220240
-
8/6/2019 Advances in TB Diagnostics
16/21
-
8/6/2019 Advances in TB Diagnostics
17/21
136 Trusov A, Bumgarner R, Valijev R et al. Comparison of LuminLED uorescent attachment, uorescent microscopy andZiehl-Neelsen for AFB diagnosis. Int. J. Tuberc. Lung Dis. 2009;13 : 83641.
137 Steingart KR, Ng V, Henry M et al. Sputum processing methodsto improvethe sensitivity of smear microscopy for tuberculosis:a systematic review. Lancet Infect. Dis. 2006; 6: 66474.
138 Gilpin C, Kim SJ, Lumb R et al. Critical appraisal of currentrecommendationsandpractices for tuberculosissputumsmear
microscopy. Int. J. Tuberc. Lung Dis. 2007; 11 : 94652.139 Rieder HL, Chiang CY, Rusen ID. A method to determine the
utility of the third diagnostic and the second follow-up sputumsmear examination to diagnose tuberculosis cases and failures.Int. J. Tuberc. Lung Dis. 2005; 9: 38491.
140 FIND. Carl Zeiss GmbH is commited to the ght against tuber-culosis. [Accessed 20 Dec 2009.] Available from URL: http:// www.nddiagnostics.org/media/press/091204.html
141 Mase SR, Ramsay A, Ng V et al. Yield of serial sputum specimenexaminations in the diagnosis of pulmonary tuberculosis:a systematic review. Int. J. Tuberc. Lung Dis. 2007; 11 : 48595.
142 Tuberculosis Coalition for Technical Assistance. International Standards for Tuberculosis Care (ISTC) . Tuberculosis Coalitionfor Technical Assistance, The Hague, 2006.
143 Brodie D, Schluger NW. The diagnosis of tuberculosis. Clin.Chest Med. 2005; 26 : 24771, vi.
144 HartungTK, MauluA, Nash J et al. Suspected pulmonary tuber-culosis in rural South Africasputum induction as a simplediagnostic tool? S. Afr. Med. J. 2002; 92 : 4558.
145 Fujita A, Murata K, Takamori M. Novel method for sputuminduction using the lung ute in patients with suspected pul-monary tuberculosis. Respirology 2009; 14 : 899902.
146 Aziz MA, Ba F, Becx-Bleumink M et al. External Quality Assess-ment for AFB Smear Microscopy . Association of Public HealthLaboratories, Washington DC, 2002.
147 Dinnes J, Deeks J, Kunst H et al. A systematic review of rapiddiagnostic tests for the detection of tuberculosis infection.Health Technol. Assess. 2007; 11 : 1196.
148 Cruciani M, Scarparo C, Malena M et al. Meta-analysis of BACTEC MGIT 960 and BACTEC 460 TB, with or without solidmedia, for detection of mycobacteria. J. Clin. Microbiol. 2004;
42 : 23215.149 WHO. New WHO policy and retooling activities for liquidculture systems. [Accessed 20 Dec 2009.]. Available from URL:http://www.who.int/tb/research/retooling/en/index.html
150 Siddiqi SH, Hwangbo CC, Silcox V et al. Rapid radiometricmethods to detect and differentiate Mycobacteriumtuberculosis/M. bovis from other mycobacterial species. Am.Rev. Respir. Dis. 1984; 130 : 63440.
151 Reisner BS, Gatson AM, Woods GL. Evaluation of mycobacteriagrowth indicator tubes for susceptibility testing of Mycobacte-rium tuberculosis to isoniazid and rifampin. Diagn. Microbiol.Infect. Dis. 1995; 22 : 3259.
152 Kalantri S, Pai M, Pascopella L et al. Bacteriophage-based testsfor the detection of Mycobacterium tuberculosis in clinicalspecimens: a systematic review and meta-analysis. BMC Infect.Dis. 2005; 5: 59.
153 Pai M, Kalantri S, Pascopella L et al. Bacteriophage-basedassays for the rapid detection of rifampicin resistance in Myco-bacteriumtuberculosis: a meta-analysis. J. Infect. 2005; 51 : 17587.
154 Moore DA, Evans CA, Gilman RH et al. Microscopic-observation drug susceptibility assay for the diagnosis of TB. N.Engl. J. Med. 2006; 355 : 153950.
155 Angeby KAK, Klintz L, Hoffner SE. Rapid and inexpensive drug susceptibility testing of Mycobacterium tuberculosis withnitrate reductase assay. J. Clin. Microbiol. 2002; 40 : 5535.
156 Martin A, Panaiotov S, Portaels F et al. The nitrate reductaseassay for the rapid detection of isoniazid and rifampicin resis-tance in Mycobacterium tuberculosis: a systematic review andmeta-analysis. J. Antimicrob. Chemother. 2008; 62 : 5664.
157 Martin A, Portaels F, Palomino JC. Colorimetric redox-indicatormethods for the rapid detection of multidrug resistance inMycobacterium tuberculosis: a systematic review and meta-analysis. J. Antimicrob. Chemother. 2007; 59 : 17583.
158 Bwanga F, Hoffner S, Haile M et al. Direct susceptibility testing for multi drug resistant tuberculosis: a meta-analysis. BMC Infect. Dis. 2009; 9: 67.
159 Laszlo A, Rahman M, Espinal M et al. Quality assurance pro-gramme for drug susceptibility testing of Mycobacterium
tuberculosis in the WHO/IUATLD Supranational ReferenceLaboratory Network: ve rounds of prociency testing, 1994-1998. Int. J. Tuberc. Lung Dis. 2002; 6: 74856.
160 World Health Organization. The WHO/IUATLD Global Projecton Anti-Tuberculosis Drug Resistance Surveillance. Anti-tuberculosis drug resistance in the world. Report No.: 4. World Health Organization Document. 2008; WHO/HTM/TB/2008.394: 1120.
161 Greco S, Girardi E, Navarra A et al. Current evidence on diag-nostic accuracy of commercially based nucleic acid amplica-tion tests for the diagnosis of pulmonary tuberculosis. Thorax 2006; 61 : 78390.
162 GrecoS, RulliM, Girardi E et al. Diagnostic accuracyof in-housePCR for pulmonary tuberculosis in smear-positive patients:meta-analysis and metaregression. J. Clin. Microbiol. 2009; 47 :56976.
163 Flores LL, Pai M, Colford JM et al. In-house nucleic acid ampli-cation tests for the detection of Mycobacterium tuberculosisin sputum specimens: meta-analysis and meta-regression.BMC Microbiol. 2005; 5: 55.
164 Sarmiento OL, Weigle KA, Alexander J et al. Assessment by meta-analysis of PCR for diagnosis of smear-negativepulmonary tuberculosis. J. Clin. Microbiol. 2003; 41 : 323340.
165 Jafari C, Thijsen S, Sotgiu G et al. Bronchoalveolar lavageenzyme-linked immunospot for a rapid diagnosis of tuberculo-sis: a TBNET study. Am. J. Respir. Crit. Care Med. 2009; 180 :66673.
166 Hillemann D, Weizenegger M, Kubica T et al. Use of the geno-typeMTBDR assayfor rapid detection of rifampinand isoniazidresistance in Mycobacterium tuberculosis complex isolates.
J. Clin. Microbiol. 2005; 43 : 3699703.167 Morgan M, Kalantri S, Flores L et al. A commercial line probeassay for the rapid detection of rifampicin resistance in Myco-bacteriumtu