Advances in Cardiovascular Imagingcircimaging.ahajournals.org/content/circcvim/7/4/723.full.pdf ·...
13
723 D uring the past several years, the need to reduce radiation has become a central issue in cardiac imaging. During this time, radiation dose to the patient in cardiac computed tomography (CT), single-photon emission computed tomog- raphy (SPECT), and positron emission tomography (PET) has seen significant reductions without compromising image qual- ity, primarily because of new developments in scanner hard- ware and reconstruction software. Sub-mSv radiation doses have been reported for cardiac CT. 1–5 Stress and rest SPECT myocardial perfusion imaging (MPI) traditionally required ≈15 minutes to register the required number of photon events. New SPECT camera instrumentation and software have now enabled acquisition times as short as 2 minutes, to increase counting efficiency by up to a factor of 7. 6 These new systems can also be used to reduce radiation exposure to patients dur- ing the MPI scan, allowing a corresponding marked reduction in the administered dose of radioactivity when used with the standard imaging time. 7 It is important to keep radiation expo- sure as low as reasonably achievable. In this review, therefore, we briefly summarize recent technical advances in scanner hardware and reconstruction software, as well as the steps recommended to achieve very low radiation dose in cardiac imaging. We also review the current status of radiation in car- diac CT, SPECT, and PET as reported in multicenter studies and registries, as well as current clinical reports of radiation dose reduction, which illustrate the potential of the newest technology. Advances in Cardiac CT Direct imaging of the coronary arteries is challenging because of their small sizes and rapid motion. Cardiac CT requires high temporal resolution to freeze such motion and there- fore has benefited from steadily increasing CT gantry rota- tion speed. Imaging of the coronary arteries also requires high spatial resolution and reconstruction of submillimeter slices. Multiple transaxial slices need to be acquired simultaneously for complete coverage of the heart in 1 breath-hold. To meet these requirements, technical advances in CT hardware have focused on improved temporal and spatial resolution and more detectors for increased coverage. 8 Methods for Dose Reduction in CT Table 1 summarizes the practical criteria and the cardiac CT scan parameters that can be modified to achieve low radiation dose. Patient-based criteria include consideration of the heart rate and rhythm, body mass index, extent of calcified plaque in the coronary arteries, and prior intervention (eg, stent placement). A further important patient-based criterion may be the clinical indication of the patient (eg, acute versus stable chest pain). As listed in Table 1, the scan parameters include scan acquisition modes, x-ray tube potential (tube voltage), x-ray tube current, pitch for helical scanning (defined as table feed per tube rotation in mm/z coverage per rotation in mm), and scan length. 9 Scan Acquisition Modes in Cardiac CT CT data are acquired with the use of either helical (spiral) or axial scan mode. Helical data are acquired with continuous rotation of the gantry and simultaneous table movement. Axial data are acquired by rotation of the gantry around the stationary patient table, followed by translation of the patient table, if needed, to cover the heart. CT imaging of the heart can be performed with or without intravenous injection of contrast agent. For contrast- enhanced coronary CT angiography (CTA), the typical contrast volume ranges from 50 to 120 mL, delivered at a rate of 4 to 7 mL/s. 10 Coronary artery calcification can be detected and quanti- fied by noncontrast cardiac CT with very low radiation expo- sure. 10 Synchronization with the heart cycle is achieved by using the patient’s electrocardiogram (ECG). Image acquisition can be performed with prospective triggering, meaning that the CT sys- tem uses the patient’s ECG to trigger release of photons and data acquisition in a predefined segment of the cardiac cycle. Alter- natively, retrospective gating can be used where the x-ray data are acquired continuously during several cardiac cycles, allow- ing retrospective reconstruction of images at any time point dur- ing systole or diastole. Cardiac scan modes can be characterized as retrospective ECG-gated helical, prospective ECG-triggered axial, or high-pitch prospective ECG-triggered helical modes. 8 X-Ray Tube Current The x-ray tube current, expressed in units of milliamperes (mA), is the number of electrons accelerated across an x-ray (Circ Cardiovasc Imaging. 2014;7:723-734.) © 2014 American Heart Association, Inc. Circ Cardiovasc Imaging is available at http://circimaging.ahajournals.org DOI: 10.1161/CIRCIMAGING.113.000897 Received July 10, 2013; accepted April 25, 2014. From the Biomedical Imaging Research Institute, Department of Biomedical Sciences (D.D.), Departments of Imaging and Medicine (P.J.S., D.S.B.), and Cedars-Sinai Heart Institute (D.S.B.), Cedars-Sinai Medical Center, Los Angeles, CA. Correspondence to Damini Dey, PhD, Cedars-Sinai Medical Center, Taper Bldg, Room A238, 8700 Beverly Blvd, Los Angeles, CA 90048. E-mail [email protected] Achieving Very-Low-Dose Radiation Exposure in Cardiac Computed Tomography, Single-Photon Emission Computed Tomography, and Positron Emission Tomography Damini Dey, PhD; Piotr J. Slomka, PhD; Daniel S. Berman, MD Advances in Cardiovascular Imaging by guest on June 20, 2018 http://circimaging.ahajournals.org/ Downloaded from
Transcript of Advances in Cardiovascular Imagingcircimaging.ahajournals.org/content/circcvim/7/4/723.full.pdf ·...

723
During the past several years, the need to reduce radiation has become a central issue in cardiac imaging. During
this time, radiation dose to the patient in cardiac computed tomography (CT), single-photon emission computed tomog-raphy (SPECT), and positron emission tomography (PET) has seen significant reductions without compromising image qual-ity, primarily because of new developments in scanner hard-ware and reconstruction software. Sub-mSv radiation doses have been reported for cardiac CT.1–5 Stress and rest SPECT myocardial perfusion imaging (MPI) traditionally required ≈15 minutes to register the required number of photon events. New SPECT camera instrumentation and software have now enabled acquisition times as short as 2 minutes, to increase counting efficiency by up to a factor of 7.6 These new systems can also be used to reduce radiation exposure to patients dur-ing the MPI scan, allowing a corresponding marked reduction in the administered dose of radioactivity when used with the standard imaging time.7 It is important to keep radiation expo-sure as low as reasonably achievable. In this review, therefore, we briefly summarize recent technical advances in scanner hardware and reconstruction software, as well as the steps recommended to achieve very low radiation dose in cardiac imaging. We also review the current status of radiation in car-diac CT, SPECT, and PET as reported in multicenter studies and registries, as well as current clinical reports of radiation dose reduction, which illustrate the potential of the newest technology.
Advances in Cardiac CTDirect imaging of the coronary arteries is challenging because of their small sizes and rapid motion. Cardiac CT requires high temporal resolution to freeze such motion and there-fore has benefited from steadily increasing CT gantry rota-tion speed. Imaging of the coronary arteries also requires high spatial resolution and reconstruction of submillimeter slices. Multiple transaxial slices need to be acquired simultaneously for complete coverage of the heart in 1 breath-hold. To meet these requirements, technical advances in CT hardware have focused on improved temporal and spatial resolution and more detectors for increased coverage.8
Methods for Dose Reduction in CTTable 1 summarizes the practical criteria and the cardiac CT scan parameters that can be modified to achieve low radiation dose. Patient-based criteria include consideration of the heart rate and rhythm, body mass index, extent of calcified plaque in the coronary arteries, and prior intervention (eg, stent placement). A further important patient-based criterion may be the clinical indication of the patient (eg, acute versus stable chest pain). As listed in Table 1, the scan parameters include scan acquisition modes, x-ray tube potential (tube voltage), x-ray tube current, pitch for helical scanning (defined as table feed per tube rotation in mm/z coverage per rotation in mm), and scan length.9
Scan Acquisition Modes in Cardiac CTCT data are acquired with the use of either helical (spiral) or axial scan mode. Helical data are acquired with continuous rotation of the gantry and simultaneous table movement. Axial data are acquired by rotation of the gantry around the stationary patient table, followed by translation of the patient table, if needed, to cover the heart. CT imaging of the heart can be performed with or without intravenous injection of contrast agent. For contrast-enhanced coronary CT angiography (CTA), the typical contrast volume ranges from 50 to 120 mL, delivered at a rate of 4 to 7 mL/s.10 Coronary artery calcification can be detected and quanti-fied by noncontrast cardiac CT with very low radiation expo-sure.10 Synchronization with the heart cycle is achieved by using the patient’s electrocardiogram (ECG). Image acquisition can be performed with prospective triggering, meaning that the CT sys-tem uses the patient’s ECG to trigger release of photons and data acquisition in a predefined segment of the cardiac cycle. Alter-natively, retrospective gating can be used where the x-ray data are acquired continuously during several cardiac cycles, allow-ing retrospective reconstruction of images at any time point dur-ing systole or diastole. Cardiac scan modes can be characterized as retrospective ECG-gated helical, prospective ECG-triggered axial, or high-pitch prospective ECG-triggered helical modes.8
X-Ray Tube CurrentThe x-ray tube current, expressed in units of milliamperes (mA), is the number of electrons accelerated across an x-ray
(Circ Cardiovasc Imaging. 2014;7:723-734.)© 2014 American Heart Association, Inc.
Circ Cardiovasc Imaging is available at http://circimaging.ahajournals.org DOI: 10.1161/CIRCIMAGING.113.000897
Received July 10, 2013; accepted April 25, 2014.From the Biomedical Imaging Research Institute, Department of Biomedical Sciences (D.D.), Departments of Imaging and Medicine (P.J.S., D.S.B.),
and Cedars-Sinai Heart Institute (D.S.B.), Cedars-Sinai Medical Center, Los Angeles, CA.Correspondence to Damini Dey, PhD, Cedars-Sinai Medical Center, Taper Bldg, Room A238, 8700 Beverly Blvd, Los Angeles, CA 90048. E-mail
Achieving Very-Low-Dose Radiation Exposure in Cardiac Computed Tomography, Single-Photon Emission Computed
Tomography, and Positron Emission TomographyDamini Dey, PhD; Piotr J. Slomka, PhD; Daniel S. Berman, MD
Advances in Cardiovascular Imaging
by guest on June 20, 2018http://circim
aging.ahajournals.org/D
ownloaded from

724 Circ Cardiovasc Imaging July 2014
tube per unit time. This is one of the primary factors that can be modified to reduce radiation exposure. The product of tube current and rotation time is defined as the tube current–time product, expressed in milliampere-seconds (mAs). Tube cur-rent and tube current–time product are related to the CT dose in a linear manner.11
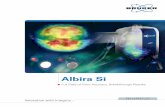
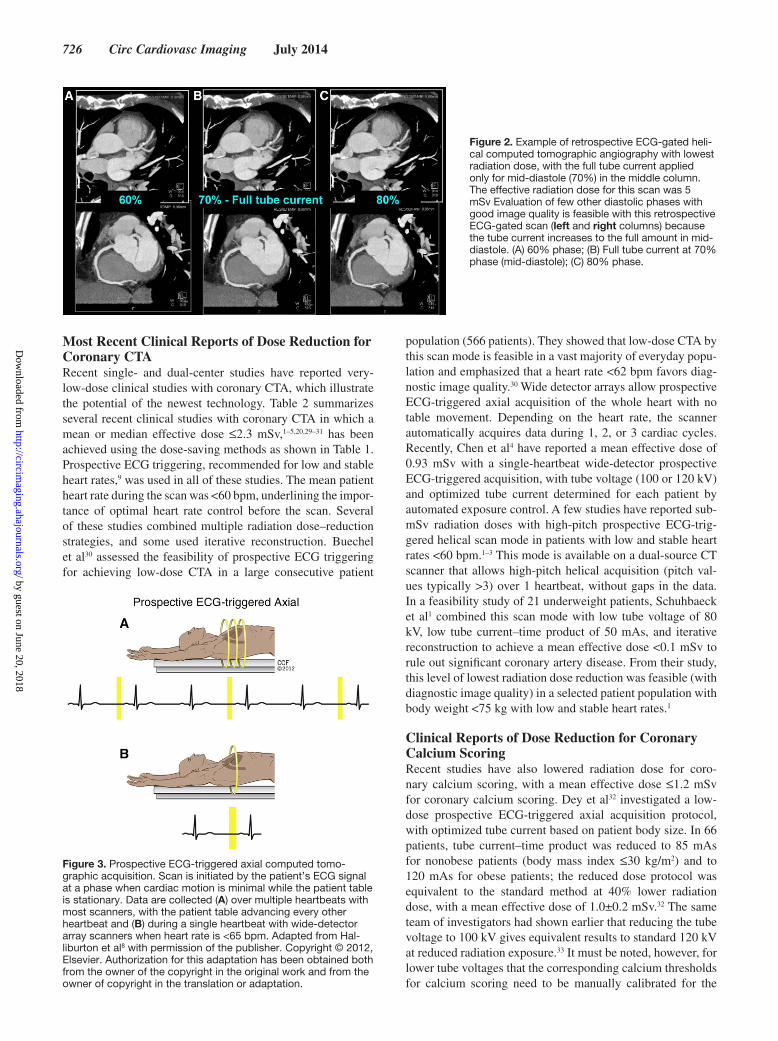
ECG-Based Tube Current ModulationFigure 1 shows a schematic example of retrospective ECG-gated scan mode for cardiac CT. For retrospective ECG-gated acquisitions, dose modulation is used to minimize the radia-tion dose in parts of the cardiac cycle that are not required for assessment of the coronary arteries. This is typically done by continuously modulating the x-ray tube current with the ECG signal (ECG-based dose modulation) so that the x-ray tube cur-rent is reduced during systole when there is the greatest motion (Figure 1B and 1C). In addition, the time interval for the maxi-mum x-ray tube current can be shortened to further reduce the radiation dose (Figure 1C). Figure 2 shows an example of low-dose retrospective ECG-gated helical acquisition with the full tube current applied only during a single mid-diastolic phase of the cardiac cycle (Figure 2),12 which still allows functional assessment of the heart. This is possible using the images in which the tube current was modulated because imaging for ventricular function does not require image quality as high as is needed for coronary artery assessment.12 Figures 3 to 4 illustrate an example case with prospective ECG-triggered axial acquisition. Figure 5 shows a schematic example of pro-spective ECG-triggered helical acquisitions for cardiac CT. A high-pitch prospective ECG-triggered helical mode in which the pitch can be ≥3.0 is currently available with a second-gen-eration dual-source CT scanner (Figure 5B).
X-Ray Tube VoltageThe tube potential (or voltage) is the electric potential applied across an x-ray tube to accelerate electrons toward the target
material, expressed in units of kilovolts (kV); this parameter determines the peak energy of the x-ray beam. Tube potentials ranging from 80 to 140 kV are available for diagnostic imag-ing on commercial CT scanners, with 100 and 120 kV being the tube potentials most commonly used. Radiation exposure with CT is approximately proportional to the square of the tube voltage. Several studies have shown the noninferiority of image quality of 100 versus 120 kV imaging of coronary arteries in nonobese adult patients (typically weight <85–90 kg or body mass index ≤30 kg/m2).13,14 Reducing tube volt-age also results in increased attenuation of the vessel lumen and cardiac chambers when iodinated contrast media are used (Figure 4), resulting in greater image contrast.
Scan RangeThe z-axis coverage of the scan (scan range or scan length) is linearly related to radiation dose. A simple step in radiation reduction for any CT scan is to limit the range to only cover only the part of the thorax as needed for the scan.9
It is to be noted that there is a fine balance between image quality and radiation dose reduction. When reducing radia-tion dose, effort must be made to ensure that sufficient image quality is maintained for confident diagnostic interpretation.15 Automated exposure control software that allows for selection of the optimal patient-specific scan parameters may be helpful in standardizing protocols by maintaining diagnostic image quality while reducing radiation dose to the patient.4,16 There are multiple steps and approximations in radiation dose esti-mation, including the commonly used conversion factor for the chest (k=0.014 mSv/[mGy.cm]), which has been shown to underestimate the radiation dose by a factor of ≈2.17,18
Iterative Reconstruction SoftwareIterative reconstruction software for CT represents another possibility for dose reduction. Because of better noise model-ing, it makes it possible to maintain image quality, even when
Table 1. Practical Considerations to Achieve a Low-Dose Cardiac CT Study
Criteria/CT Scan/Reconstruction Parameters Parameters That Can Be Modified in Practice Relationship to Radiation Dose
Patient-based criteria: heart rate and rhythm, body mass index, extent of calcified plaque in the coronary arteries, prior intervention (eg, stents), clinical indication
Optimal heart rate reduction with beta-blockade (for coronary CTA)
Optimal heart rate can allow selection ofscan parameters that lower dose,
as allowed by patient-based criteria
Scan mode Retrospective ECG-gated helicalProspective ECG-triggered axial*
High-pitch prospective ECG-triggered helical (stable heart rate ≤60 bpm)*
Scan range Minimal scan range should be selected, depending on the reason for the test
Decreasing scan range decreases dose linearly*
Tube current for the scan Tube current, mATube current×rotation time (mA×seconds)
Decreasing tube current×rotation time decreases dose linearly*
Peak voltage for the scan kV, adaptive kV by automated exposure control Decreasing kV decreases dose*Dose approximately proportional to square of kV
Pitch for the scan For helical scan modes, defined astable feed per tube rotation (mm)/z coverage
per rotation (mm)
Increasing pitch decreases dose*Dose proportional to inverse pitch (1/pitch)
Iterative reconstruction For all scans Improved image quality whenx-ray photons are reduced
CT indicates computed tomography; and CTA, CT angiography.*Reducing the total number of x-ray photons for the scan
by guest on June 20, 2018http://circim
aging.ahajournals.org/D
ownloaded from

Dey et al Achieving Very-Low-Dose Cardiac CT, SPECT, and PET 725
the number of x-ray photons is reduced in the acquisition pro-tocol. Although iterative reconstruction techniques have been clinically used for nearly a decade in nuclear MPI,19 they have only recently become available from all the major CT manu-facturers with feasible reconstruction times for clinical CT. A growing number of recent studies have reported radiation dose reduction while maintaining image quality using itera-tive reconstruction technique in CT.1,4,20,21
Current Status as Reported in Multicenter Studies and RegistriesThe large, prospective multicenter Rule Out Myocardial Infarc-tion Using Computer Assisted Tomography (ROMICAT) trial, which compared an evaluation incorporating coronary CTA with standard-of-care assessment in 1000 patients with symptoms suggestive of acute coronary syndrome between April 2010 and January 2012, reported a mean radiation dose of 11.3±5.3 mSv for coronary CTA and 14.1±4.8 mSv for cardiac SPECT.22 In 78 patients in this trial who underwent CTA with a newer 128-slice dual-source CT scanner, the mean radiation exposure was lower (6.2±3.8 mSv) than the other patients.22 From the multicenter Coronary Computed Tomographic Angiography for Systematic Triage of Acute Chest Pain Patients to Treatment (CT-STAT) study comparing early coronary CTA with rest–stress MPI
for the evaluation of acute low-risk chest pain in 699 patients from June 2007 to November 2008, the mean radiation dose was reported to be 11.5 mSv for CTA and 12.8 mSv for cardiac SPECT.23 In the multicenter Determination of Fractional Flow Reserve by Anatomic Computed Tomographic Angiography (DeFACTO) study evaluating 252 patients with stable coronary artery disease in 17 centers between 2010 and 2011, the median effective dose for coronary CTA was 6.4 mSv (interquartile range, 4.4–15.0 mSv).24 A multicenter international observa-tional study of 1965 patients undergoing coronary CTA in 2007 in 50 sites reported an average median dose of 12 mSv, with sig-nificant differences between study sites and CT systems.25 In the multicenter, international Coronary CT Angiography Evaluation For Clinical Outcomes: An International Multicenter Registry (CONFIRM) registry evaluating a consecutive cohort of 24 775 patients without known coronary artery disease who underwent coronary CTA between 2005 and 2009 in expert centers, the reported radiation dose range was 3 to 18 mSv.26
In the multicenter Coronary Artery Evaluation using 320-row Multidetector Computed Tomography Angiography and Myocardial Perfusion (CORE320) study evaluating the accu-racy of combined coronary CTA and CT perfusion to identify hemodynically significant coronary artery disease causing perfusion defect by SPECT (381 patients), the median effec-tive radiation dose for the coronary CTA portion of the study was 3.16 mSv (interquartile range, 2.8–3.6 mSv) for CTA and 9.75 mSv (interquartile range, 9.1–13.0 mSv) for SPECT; in this study, all CT images were acquired with a newer 320-slice multidetector CT scanner with 320×0.5 mm coverage.27 The median effective radiation dose for noncontrast CT used for coronary artery calcium scoring was 0.85 mSv (interquartile range, 0.82–0.93 mSv).27
Prospective Multicenter Studies Evaluating Radiation Dose ReductionIn a prospective, randomized, multicenter study evaluating 100 kVp tube voltage scan protocol in 400 nonobese patients, coronary CTA using 100 kVp was shown to maintain image quality with significantly reduced radiation exposure (31% rela-tive reduction), thus emphasizing that 100 kVp scan protocols should be considered for nonobese patients to reduce radiation exposure.13 A recent report from the multicenter, prospective imaging consortium participating in a quality improvement pro-gram, involving 11 901 consecutive patients undergoing CTA at 15 imaging centers in Michigan from 2008 to 2011, has shown that consistent application of radiation dose–reduction tech-niques was associated with sustained reduction of radiation dose without affecting the proportion of diagnostic scans.28 This mul-ticenter study also demonstrated that the use of newer scanner technology resulted in substantial dose reduction. In this study, reduction in tube potential from 120 to 100 kV was the strongest variable associated with achieving a target estimated dose of <10 mSv among all patients (odds ratio, 3.1 [95% confidence inter-val, 2.6–3.7]), followed by nonretrospective gating (prospective ECG triggering with axial and high-pitch helical scan mode; odds ratio, 2.2 [95% confidence interval, 1.97–2.54]), lower body mass index (odds ratio, 1.73 [95% confidence interval, 1.49–2.0]), and the number of coronary CTA scans per month in each site (odds ratio, 1.38 [95% confidence interval, 1.2–1.6]).
Figure 1. Retrospective ECG-gated helical computed tomo-graphic acquisition, with continuous gantry rotation and simulta-neous patient table translation. Radiation dose from the scan is (A) highest with ECG-based tube current modulation turned off, (B) lower with the full tube current applied for a diastolic portion (eg, 40%–80%) of the cardiac cycle, and (C) lowest with full tube current applied during only a single phase of the cardiac cycle. Adapted from Halliburton et al8 with permission of the publisher. Copyright ©2012, Elsevier. Authorization for this adaptation has been obtained both from the owner of the copyright in the origi-nal work and from the owner of copyright in the translation or adaptation.
by guest on June 20, 2018http://circim
aging.ahajournals.org/D
ownloaded from
726 Circ Cardiovasc Imaging July 2014
Most Recent Clinical Reports of Dose Reduction for Coronary CTARecent single- and dual-center studies have reported very-low-dose clinical studies with coronary CTA, which illustrate the potential of the newest technology. Table 2 summarizes several recent clinical studies with coronary CTA in which a mean or median effective dose ≤2.3 mSv,1–5,20,29–31 has been achieved using the dose-saving methods as shown in Table 1. Prospective ECG triggering, recommended for low and stable heart rates,9 was used in all of these studies. The mean patient heart rate during the scan was <60 bpm, underlining the impor-tance of optimal heart rate control before the scan. Several of these studies combined multiple radiation dose–reduction strategies, and some used iterative reconstruction. Buechel et al30 assessed the feasibility of prospective ECG triggering for achieving low-dose CTA in a large consecutive patient
population (566 patients). They showed that low-dose CTA by this scan mode is feasible in a vast majority of everyday popu-lation and emphasized that a heart rate <62 bpm favors diag-nostic image quality.30 Wide detector arrays allow prospective ECG-triggered axial acquisition of the whole heart with no table movement. Depending on the heart rate, the scanner automatically acquires data during 1, 2, or 3 cardiac cycles. Recently, Chen et al4 have reported a mean effective dose of 0.93 mSv with a single-heartbeat wide-detector prospective ECG-triggered acquisition, with tube voltage (100 or 120 kV) and optimized tube current determined for each patient by automated exposure control. A few studies have reported sub-mSv radiation doses with high-pitch prospective ECG-trig-gered helical scan mode in patients with low and stable heart rates <60 bpm.1–3 This mode is available on a dual-source CT scanner that allows high-pitch helical acquisition (pitch val-ues typically >3) over 1 heartbeat, without gaps in the data. In a feasibility study of 21 underweight patients, Schuhbaeck et al1 combined this scan mode with low tube voltage of 80 kV, low tube current–time product of 50 mAs, and iterative reconstruction to achieve a mean effective dose <0.1 mSv to rule out significant coronary artery disease. From their study, this level of lowest radiation dose reduction was feasible (with diagnostic image quality) in a selected patient population with body weight <75 kg with low and stable heart rates.1
Clinical Reports of Dose Reduction for Coronary Calcium ScoringRecent studies have also lowered radiation dose for coro-nary calcium scoring, with a mean effective dose ≤1.2 mSv for coronary calcium scoring. Dey et al32 investigated a low-dose prospective ECG-triggered axial acquisition protocol, with optimized tube current based on patient body size. In 66 patients, tube current–time product was reduced to 85 mAs for nonobese patients (body mass index ≤30 kg/m2) and to 120 mAs for obese patients; the reduced dose protocol was equivalent to the standard method at 40% lower radiation dose, with a mean effective dose of 1.0±0.2 mSv.32 The same team of investigators had shown earlier that reducing the tube voltage to 100 kV gives equivalent results to standard 120 kV at reduced radiation exposure.33 It must be noted, however, for lower tube voltages that the corresponding calcium thresholds for calcium scoring need to be manually calibrated for the
Figure 2. Example of retrospective ECG-gated heli-cal computed tomographic angiography with lowest radiation dose, with the full tube current applied only for mid-diastole (70%) in the middle column. The effective radiation dose for this scan was 5 mSv Evaluation of few other diastolic phases with good image quality is feasible with this retrospective ECG-gated scan (left and right columns) because the tube current increases to the full amount in mid-diastole. (A) 60% phase; (B) Full tube current at 70% phase (mid-diastole); (C) 80% phase.
Figure 3. Prospective ECG-triggered axial computed tomo-graphic acquisition. Scan is initiated by the patient’s ECG signal at a phase when cardiac motion is minimal while the patient table is stationary. Data are collected (A) over multiple heartbeats with most scanners, with the patient table advancing every other heartbeat and (B) during a single heartbeat with wide-detector array scanners when heart rate is <65 bpm. Adapted from Hal-liburton et al8 with permission of the publisher. Copyright © 2012, Elsevier. Authorization for this adaptation has been obtained both from the owner of the copyright in the original work and from the owner of copyright in the translation or adaptation.
by guest on June 20, 2018http://circim
aging.ahajournals.org/D
ownloaded from

Dey et al Achieving Very-Low-Dose Cardiac CT, SPECT, and PET 727
scanner,34,35 whereas similar level of radiation dose reduction can be obtained without requiring such calibration by optimi-zation of the tube current.32 In a recent study, Marwan et al35
investigated the use of high-pitch prospective ECG-triggered helical scan mode for coronary calcium scoring in 150 patients. This scan mode allowed coronary calcium scor-ing with effective doses with a mean dose of 0.3 mSv (and consistently <0.5 mSv) at 120 kV.
Advances in Cardiac SPECT
Hardware AdvancesThe key feature of the new dedicated SPECT cardiac imaging systems now available from several instrumentation vendors is significantly increased photon sensitivity. The higher sensitivity is primarily achieved by a radical redesign of the collimation methods. Traditional systems using low-energy high-resolu-tion collimators are only able to detect <0.02% of the photon events.36 The new designs of collimation include the multiple pinhole collimators or ultra–high-sensitivity parallel detectors focusing on the heart. In systems being considered for develop-ment, the overall system sensitivity can be further improved by dedicated scanner geometry surrounding the patient. This opti-mized scanner geometry would allow simultaneous collections of counts from all directions without camera rotation.37–39 The combination of scintillation crystals with photomultiplier tubes, the standard for >50 years, has been replaced with solid-state photon detectors (cadmium zinc telluride) or alternatively with cesium iodide scintillation detector coupled with photodiodes. The use of CZT solid-state detectors results in improved energy resolution and consequently less undesirable scatter events,40 thus potentially reducing the number of events required dur-ing acquisition and consequently the injected dose. These new dedicated cardiac cameras often have a reduced footprint, allow
easier patient positioning, and, in some cases, upright imaging, increasing patient comfort. To date, several clinical studies have been reported. The studies have primarily focused on shorter scan times—as short as 2 minutes using a dedicated cardiac sys-tem with semistationary CZT pixelated detectors, high-sensi-tivity collimation, and reconstruction optimized specifically for cardiac imaging.40,41 Figure 6 illustrates at least a 7-fold increase in sensitivity for a dedicated cardiac scanner with high-sensi-tivity collimators and optimized focusing of the collimation on the heart region compared with a standard SPECT gamma camera. With standard acquisition times, these systems allow for marked reduction in the administered dose of radioactivity. Several clinical studies have also been published with another stationary imaging camera design, based on multi-pinhole col-limation,37–39 and CZT detectors,42 including optional attenua-tion correction,43 with similar scan times as short as 2 minutes.44 Another cardiac solid-state camera with indirect photon con-version has been combined with new 3-dimensional (3D) itera-tive ordered-subsets expectation maximization reconstruction algorithm. Clinical studies on this system have shown that rapid gated MPI may be achieved with <5-minute imaging time with-out compromising perfusion or function information.45
Software AdvancesThe new SPECT scanners are coupled with improved image reconstruction algorithms implemented in software. New reconstruction algorithms include physical modeling of the collimators and detectors, as well as resolution recovery.19 Most systems now offer compensation for image resolu-tion loss (especially needed for high-sensitivity collimation) via accelerated iterative reconstruction.46 Sophisticated soft-ware reconstruction methods can also improve image quality obtained by standard SPECT cameras, which can be exploited to reduce imaging time or radiation dose.
Figure 4. Example of prospective ECG-triggered axial computed tomographic scan with 100 kV in a 43-year-old woman with heart rate of 65 bpm, with excellent image quality. The effective radiation dose for this scan was 1.5 mSv. LAD indicates left anterior descending coronary artery; and RCA, right coronary artery.
by guest on June 20, 2018http://circim
aging.ahajournals.org/D
ownloaded from

728 Circ Cardiovasc Imaging July 2014
Current Status for Cardiac SPECTEstimated radiation doses for single-isotope (99mTc) stress–rest scans range from 10 to 15 mSv as reported by recent multicenter studies.40,47,48 A recent multiple site survey in 2011 by the American Society of Nuclear Cardiology found that dual-isotope stress–rest imaging, which is associated
with a significantly higher radiation dose, dropped from 72% to 15.6% in 10 years since 2001.49In this survey based on participating site responses, 51% of the sites reported using ≥1 approaches to reducing radiation exposure, by reducing injected radiopharmaceuticals while increasing imaging time (33%), the use of stress-only imaging (23%), newer cam-era systems (20.5%), and changing radiopharmaceuticals (19.2%).50 The survey results reported the underutilization of dose-reduction approaches and suggested significant opportu-nities for improving radiation safety for patients undergoing nuclear stress testing. Practical recommendations by Ameri-can Society of Nuclear Cardiology to improve patient radia-tion safety in cardiac SPECT included increasing the use of low-dose stress-first imaging, further decreasing dual-isotope imaging, promoting wider integration of the appropriate use criteria into clinical practice, and fostering validation, use, and affordability of advanced technologies permitting reduced administered activity of radiotracers.50
Clinical Reports of Dose ReductionA few clinical studies have been conducted to evaluate reduced dose protocols with standard and new gamma cameras. In one of these studies, low-dose stress-only protocols allowed radia-tion dose as low as 4.2 mSv for a 12.5 mCi 99mTc scan.51 A low-dose rest–stress 99mTc protocol has been studied, resulting in 5.1 to 6.1 mSv exposure.52,53 Low-dose imaging was also demon-strated on a standard SPECT camera using an iterative recon-struction technique with standard acquisition times.54 In another study, the patient dose was reduced to 4.3 mSv for stress–rest protocols when background activity subtraction was applied.55
Stress-Only ImagingMPI radiation dose to the patient can be significantly reduced if the rest scan is not performed. Furthermore, stress-only protocols
Figure 5. Prospective ECG-triggered helical computed tomo-graphic acquisition. Helical data acquisition is initiated by the patient’s ECG signal. Data are collected (A) over multiple heart-beats or (B) during a single heartbeat with dual-source scanners, which can achieve high-pitch (≈3) values. Adapted from Hal-liburton et al8 with permission of the publisher. Copyright © 2012, Elsevier. Authorization for this adaptation has been obtained both from the owner of the copyright in the original work and from the owner of copyright in the translation or adaptation.
Table 2. Very-Low-Dose Coronary Computed Tomographic Angiography Clinical studies With Mean or Median Effective Dose <3.0 mSv
Study n Heart Rate, bpm BMI, kg/m2 Dose-Reduction Methods Mean Effective Dose, mSv
Schuhbaeck et al1 21 50±6 23.9±3.2 Prospective ECG-triggered helical, tube voltage 80 kV, tube current 50 mAs, iterative reconstruction
0.06±0.01
Achenbach et al2 50 54±4 Body weight 77±11 kg Prospective ECG-triggered helical, tube voltage 100 kV, tube current 320 mAs
0.87±0.07
Achenbach et al3 50 54±6 ... Prospective ECG-triggered helical, tube voltage 100 kV, tube current 320 mAs
0.76±0.08
LaBounty et al5 208 normal BMI patients, 103 with low- dose protocol
54.3±6.3 22.3±2.2 80 vs 100 kV 0.9 (0.8–1.7) mSv
Chen et al4 107 57.1±11.2 27.3 (24.6–32.3) 100 kV, single-heartbeat wide-detector prospective ECG-triggered axial scan, tube voltage, and tube
current by automated exposure control
0.93 (0.58–1.74)
LaBounty et al29 449, 202 with low-dose protocol
57±9 27±5 100 kV, lowered tube current 412 mA, prospective ECG-triggered axial
1.3 (0.8–1.9)
Buechel et al30 566 consecutive patients
56.9±6.6 26±5 (range, 18–49) Prospective ECG-triggered axial 1.8±0.6
Hausleiter et al31 14 52.6±5.5 26.4±4.4 Prospective ECG-triggered helical, tube voltage 100 kV/120 kV, tube current 362–438 mAs
2.0±0.7
Leipsic et al20 574, 243 with low-dose protocol
58±10 26±5 Prospective ECG-triggered axial, lowered tube current 450 mA with iterative reconstruction
2.3 (1.9–3.5)
BMI indicates body mass index.
by guest on June 20, 2018http://circim
aging.ahajournals.org/D
ownloaded from

Dey et al Achieving Very-Low-Dose Cardiac CT, SPECT, and PET 729
could improve the overall efficiency of the imaging laboratory, lower the radiation exposure to the laboratory personnel, and enhance patient convenience because of less time needed for the overall test.56 There is ample evidence in the literature that when stress images are normal, there is no additional prognostic information added by performing the rest study.51,52,57 Similarly, when the stress scan is performed with attenuation correction (AC), it has been shown that the visual diagnostic performance is similar to that of a stress–rest scan.58 Without AC, the accu-racy of stress-only imaging can be improved and the frequency of needing rest scans can be reduced with combined analysis of stress supine–prone or supine–upright data, which is aided by quantitative analysis.59,60 The supine–prone studies are per-formed with 1 injected stress dose.60 Stress-only protocols have been also proposed in conjunction with CTA imaging for sites that are equipped with CTA scanners. Husmann et al61 proposed a low-dose stress-only scan in combination with CTA. The total radiation dose for the MPI and CTA scan was 5.4±0.8 mSv (the dose for the CTA scan was 2.2±0.7 mSv), which is lower than for most current stress–rest MPI protocols. Table 3 lists the pub-lished clinical cardiac SPECT studies with reduced radiation dose and new instrumentation.
Low-Dose SPECT MPI With Newer ScannersThe initial applications of the new cardiac imaging instrumen-tation for SPECT MPI were directed toward drastic reduction of scan times, with only a few recent studies focusing on dose reduction. It should be noted from a technical point of view that the improvements in sensitivity provided by the new instrumen-tation can equally reduce time, acquisition, or radiation dose. As seen in Figure 6, improvement in the sensitivity of the new sys-tems is of the order of 7× to 8×. Thus, the dose can theoretically be reduced by the same amount with standard imaging times. The minimum imaging time or dose needed for one of these scanners has recently been assessed by retrospective analysis of full-dose full-time data and reconstruction of only a fraction of
the counts. This is made possible by the list-mode capabilities of new scanners for SPECT and PET, which allow retrospective simulation of a scan with an arbitrary activity or alternatively duration, from the original full-dose/full-time acquisition data. Nakazato et al7 determined the feasibility of very-low-dose MPI quantitatively, simulating gradually lowered count levels from list-mode data by reconstruction of various fractions of acquired counts (Figure 7). In 79 patients, 1 million counts in the myo-cardium produced MPI images that agreed well with standard 8 million count images for quantitative perfusion and function parameters. With a dedicated fast cardiac camera, these images can be obtained for 10 minutes with an effective radiation dose <1 mSv without significant loss of accuracy.7 Consequently, the results obtained in the studies with reduced imaging times (Figure 8) can be extrapolated to future studies with lower dose protocols if a similar count level in the left ventricular myocar-dium is maintained. In 101 patients, Einstein et al62 have recently reported a multicenter comparison of image quality, quantitative function, and perfusion parameters for low-dose (3.5 mCi) 99mTc injection at rest, imaged by solid-state CZT camera and with standard SPECT, and showed that ultra–low-dose rest imaging correlates highly with standard SPECT, with improved image quality while achieving a radiation dose reduction of 55% to 1 mSv. Because the proportion of the injected 99mTc dose that is retained in the myocardium is slightly higher with stress imag-ing than with rest imaging and because the extracardiac uptake is lower after stress injections than rest injections, these data from a low-dose rest protocol suggest that stress-only studies with 1 mSv radiation are possible with the CZT systems. Tay-lor et al63 have recently evaluated the diagnostic accuracy of 37
Figure 6. System sensitivity for a dedicated solid-state cardiac camera. The higher system sensitivity of high-speed system is demonstrated by significantly higher myocardial count rate (7–8×) compared with conventional single-photon emission computed tomography (SPECT) at stress and rest images. CPM indicates counts/min. Adapted from Sharir et al41 with permission of the publisher. Copyright © 2008, Elsevier. Authorization for this adap-tation has been obtained both from the owner of the copyright in the original work and from the owner of copyright in the transla-tion or adaptation.
Table 3. Recent Published Clinical Cardiac Single-Photon Emission Computed Tomographic Studies With Reduced Dosing and New Instrumentation
Study n Protocol Injected DoseTotal Radiation
Dose, mSv
Husmann et al61
100 Stress-only/ prospective gated CTA.
Stress: 8.1 mCi 5.4+0.8
Duvall et al51
209 Stress- only 99mTc sestamibi
Stress: 12.5 mCi 4.2
DePuey et al54
160 99mTc sestamibi
Rest: 5.8±0.6 mCiStress: 17.5±2.5 mCi
6.8
Nkoulou et al55
50 1-day 99mTctetrofosmin adenosine stress–rest
Stress/rest 8.6/17.3 mCi5 min/5 min
4.3
Duvall et al52
131 99mTc sestamibi5- to 8- min rest3- to 5-
min stress
Rest: 5 mCiStress: 15 mCi
5.8
Gimelli et al53
137 99mTc tetrofosmin
Stress: 5–6 mCiRest: 10–12 mCi
5.10 (men)6.12 (women)*
Einstein et al62
101 at 3 sites 99mTc sestamibi
Rest: 3.5 mCi 1.2
*Established by sex-specific phantom scans
by guest on June 20, 2018http://circim
aging.ahajournals.org/D
ownloaded from

730 Circ Cardiovasc Imaging July 2014
patients who underwent coronary angiography and ultra–low-dose SPECT within 30 days with a stress-first protocol using <4 mCi 99mTc-sestaMIBI, imaged by a solid-state CZT camera. They showed that ultra–low-dose SPECT with patient dosimetry of 10% of typical rest–stress SPECT is diagnostically accurate for identification of significant coronary artery disease.63
Low-Dose Attenuation Correction with Newer ScannersAttenuation correction (AC) has the potential to improve the diagnostic accuracy of cardiac SPECT imaging. It has been shown that AC can be used with stress-only imaging to reduce the frequency of requiring additional rest studies.58 AC is associated with a small additional radiation dose. The typi-cal stress and rest doses from such AC scans obtained using SPECT/CT or PET/CT systems are low, in the order of 0.3 to 1.3 mSv.64 To reduce the AC radiation dose with SPECT/CT, 2 new designs have been developed by equipment vendors. An integrated system has been developed in which photons from x-ray source are detected by solid-state detectors with a fan beam collimator operating in high counting rate mode with an effective dose of 5 μSv.65 Another example of new AC tech-nology uses a flat panel and achieves low-dose (0.12 mSv) CT AC imaging. The attenuation scan of the entire heart volume (14 cm axial field of view) is acquired in a single 60-second rotation with the patient breathing normally; the attenuation data are averaged over multiple respiratory cycles to match the position of the heart during the SPECT acquisition.66
Advances in Cardiac PET
Technical AdvancesModern PET/CT scanners from all the vendors operate in 3D coincidence detection mode. In PET, each annihilation event
between emitted positron and electron produces two 511 keV photons traveling in opposite directions. Two detectors ori-ented at 180° to each other, within a certain time window (typi-cally 5–20 nanoseconds), are used to detect these photons; this is known as annihilation coincidence detection. Three-dimen-sional acquisition and new software methods offer a potential for dose reduction in cardiac imaging, beyond already very low radiation levels associated with the short-lived PET myocardial perfusion tracers. Specifically for cardiac applications, current PET scanners have been optimized to cope with high count lev-els in first-pass 82Rb imaging for myocardial blood flow mea-surements67 and with additional 82Rb γ-prompt decays affecting 3D imaging.68 The system sensitivity of 3D PET scanners is 4× to 6× higher than scanners operating in 2D mode.69 Further technical advances include developments of photon time-of-flight methods70 and new high-definition iterative reconstruc-tion techniques based on scanner-specific 3D modeling of system resolution with effective tomographic resolution as low as 2 mm.71 Preliminary reports have been published demon-strating the application of these improved PET reconstruction methods to cardiac imaging.72 Further image quality improve-ments have been proposed73 by combining new reconstruc-tion with cardiac motion–frozen techniques to reduce blurring because of cardiac motion.74
It should be noted that as with SPECT, there is a small addi-tional radiation dose associated with CT AC scans for PET imaging. Unlike SPECT, AC in PET is mandatory because of photon coincidence detection. In a recent study of 91 consecu-tive patients, Mylonas et al have shown that quantification of coronary artery calcium from standard nongated PET attenu-ation correction CT is feasible and accurate.75 Furthermore, it has also been shown that standard coronary calcium scoring scans can be used for attenuation correction.76 These studies suggest that in the future, the same low-dose CT scans could be used for both attenuation correction and allow assessment of coronary artery calcium.
8.0 million
3.6 million
2.0 million
1.0 million
0.7 million
0.5 million
1.3 million
Accuracy of simulated very-low dose quantitative MPITPD
11%
12%
12%
12%
12%
12%
9%
Counts in left ventricle
Gradually lowered count level (list mode reconstruction)
Effective dose 1 mSv
Figure 7. Figure showing the quantitative accuracy of very-low-dose myocardial perfusion imaging (MPI) by simulating gradually lowered count levels from list-mode data by reconstruction of various fractions of acquired counts, as described by Nakazato et al.7 One million counts in the myocardium produced MPI images that agreed well with standard images for quantitative perfusion and function parameters. Adapted from Nakazato et al7 with permission of the publisher. Copyright @ 2013, the Society of Nuclear Medicine and Molecular Imaging, Inc. Authorization for this adaptation has been obtained both from the owner of the copyright in the original work and from the owner of copyright in the translation or adaptation.
Figure 8. Myocardial perfusion images by conventional single-photon emission computed tomography (SPECT) and high-speed SPECT (with a cadmium zinc telluride camera) showing moderate ischemia (total perfusion deficit >5% of myocardium by both sets of images). Total acquisition indicated on the left-hand side: 35 minutes by conventional SPECT and 6 minutes by high-speed SPECT. Adapted from Sharir et al40 with permission of the pub-lisher. Copyright © 2010, Elsevier. Authorization for this adapta-tion has been obtained both from the owner of the copyright in the original work and from the owner of copyright in the transla-tion or adaptation.
by guest on June 20, 2018http://circim
aging.ahajournals.org/D
ownloaded from

Dey et al Achieving Very-Low-Dose Cardiac CT, SPECT, and PET 731
Current Status of Cardiac PETEstimated patient radiation doses have recently been revised down to 2.0 to 3.7 mSv for standard 82Rb PET scans by precise patient-specific calculations, with 3.7 mSv corresponding to 80 mCi total injected dose for stress and rest with a standard 2D PET scanner.77 Because several of the other radiotracers for cardiac PET MPI are short-lived, the associated radiation doses are low. Typical radiation dose ranges from 2 to 3 mSv for stress–rest 13N-Ammonia (2.4 mSv for injected activity, 15 mCi for each stress and rest scan), 2 to 2.5 mSv for stress–rest 15O-water (2.5 mSv for injected activity, 29.7 mCi for each stress and rest scan), and is ≈7 mSv for 18F-Fluorodeoxyglu-cose viability studies (for 10 mCi injected activity).47
Clinical ApplicationsAlthough PET MPI is currently not widely used compared with SPECT, it offers significant potential advantages because in addition to relative perfusion, it allows measurements of myocardial blood flow and perfusion flow reserve.78 New PET systems registering the photon events in list mode allow recon-struction of both perfusion and blood flow data from 1 scan. As a result of increased sensitivity of 3D PET, it is possible to obtain high-quality 82Rb perfusion images at injected activi-ties as low as 20 mCi.79 Estimated patient radiation doses have recently been revised down to 3.7 mSv for 82Rb PET scans obtained on a standard 2D scanner with 80 mCi total injected activity for stress and rest.77 Therefore, the effective radiation dose of stress–rest 82Rb scans obtained in 3D mode could be further reduced to ≈1.85 mSv (<1 mSv for stress scan). For the newly introduced fluorine-18 labeled radiotracer 18F flur-piridaz, a mean effective combined rest–stress dose has been reported to be 5 to 6 mSv in phase I and II trials.80,81 It is to be noted that pharmacological PET imaging offers true stress (rather than poststress) functional measurements and allows time-efficient (<30 minutes) stress–rest protocols.78 Analo-gous to stress-only SPECT MPI imaging, it is also possible to perform stress-only low-dose PET imaging. A recent study of 200 patients has shown that stress-only 82Rb PET MPI is a feasible approach to reduce resource utilization and radia-tion exposure associated with MPI; this strategy would be most applicable to patients with lower pretest likelihood.82 With F-18 flurpiridaz, exercise PET has been reported, with an injected activity of 6.48±1.23 mCi for exercise stress.80 It is likely that stress-only PET MPI studies will become common with this agent.
SummaryCardiac imaging with CT, SPECT, and PET has recently reached new standards in terms of radiation dose reduction. Recent multicenter trials and studies when using the newer scanner technology have reported mean effective doses <10 mSv; however, this is not available in all centers. Mean effective doses from several clinical studies have shown the potential of the newest technology to be associated with radia-tion below the average annual dose from naturally occurring sources of radiation. Advances in instrumentation in CT, cou-pled with iterative reconstruction software, have shown the feasibility of sub-mSv radiation dose for coronary CTA. For
coronary CTA, optimal heart rate control with beta-blockade is important for both achieving optimal image quality and use of scan parameters that reduce radiation dose, as allowed by patient-based criteria. Recently introduced automated expo-sure control software can help imaging maintain diagnostic image quality while reducing radiation dose to the patient. Advances in new SPECT instrumentation allow routine stress–rest MPI imaging with low radiation doses. For cardiac SPECT, stress-only protocols can be used to reduce the radia-tion dose and the overall test time and are increasingly used. With the new systems, stress-only SPECT MPI may be per-formed with doses as low as 1 mSv. PET perfusion imaging can be performed with very low doses, particularly on new 3D scanners.
Radiation dose reduction is associated with the potential benefit of lowered cumulative cancer risk to the patient.47 However, if sufficient image quality is not maintained for con-fident diagnostic interpretation,15 such radiation dose–reduc-tion strategies can decrease the diagnostic accuracy and may lead to increased downstream testing. Therefore, a balanced approach that applies the newest technology reasonably, achieving radiation dose reduction but assuring sufficient image quality, is the most desirable. Finally, technological advances that are at the same time cost-saving, diagnosti-cally accurate, and with low associated radiation exposure are likely to be favored by the current healthcare environment. Introduction of the technologies as discussed above and devel-opment of new balanced imaging protocols and reconstruction and postprocessing software for cardiac CT, SPECT, and PET have the potential to address these demands.
Sources of FundingDr Damini Dey has received research support from the American Heart Association; this work was partially supported by American Heart Association grant 12GRNT9450056.
DisclosuresDr Berman is a shareholder in Spectrum Dynamics and is a mem-ber of the Medical Advisory Board and consultant for Spectrum Dynamics. Dr Berman and Dr. Slomka received research support for Siemens Healthcare. The other authors report no conflicts.
References 1. Schuhbaeck A, Achenbach S, Layritz C, Eisentopf J, Hecker F, Pflederer
T, Gauss S, Rixe J, Kalender W, Daniel WG, Lell M, Ropers D. Image quality of ultra-low radiation exposure coronary CT angiography with an effective dose <0.1 mSv using high-pitch spiral acquisition and raw data-based iterative reconstruction. Eur Radiol. 2013;23:597–606.
2. Achenbach S, Marwan M, Ropers D, Schepis T, Pflederer T, Anders K, Kuettner A, Daniel WG, Uder M, Lell MM. Coronary computed tomog-raphy angiography with a consistent dose below 1 mSv using prospec-tively electrocardiogram-triggered high-pitch spiral acquisition. Eur Heart J. 2010;31:340–346.
3. Achenbach S, Goroll T, Seltmann M, Pflederer T, Anders K, Ropers D, Daniel WG, Uder M, Lell M, Marwan M. Detection of coronary artery stenoses by low-dose, prospectively ECG-triggered, high-pitch spi-ral coronary CT angiography. J Am Coll Cardiol Cardiovasc Imaging. 2011;4:328–337.
4. Chen MY, Shanbhag SM, Arai AE. Submillisievert median radiation dose for coronary angiography with a second-generation 320-detector row CT scanner in 107 consecutive patients. Radiology. 2013;267:76–85.
5. LaBounty TM, Leipsic J, Poulter R, Wood D, Johnson M, Srichai MB, Cury RC, Heilbron B, Hague C, Lin FY, Taylor C, Mayo JR, Thakur Y,
by guest on June 20, 2018http://circim
aging.ahajournals.org/D
ownloaded from

732 Circ Cardiovasc Imaging July 2014
Earls JP, Mancini GB, Dunning A, Gomez MJ, Min JK. Coronary CT angiography of patients with a normal body mass index using 80 kVp versus 100 kVp: a prospective, multicenter, multivendor randomized trial. AJR Am J Roentgenol. 2011;197:W860–W867.
6. Slomka PJ, Patton JA, Berman DS, Germano G. Advances in techni-cal aspects of myocardial perfusion SPECT imaging. J Nucl Cardiol. 2009;16:255–276.
7. Nakazato R, Berman DS, Hayes SW, Fish M, Padgett R, Xu Y, Lemley M, Baavour R, Roth N, Slomka PJ. Myocardial perfusion imaging with a solid-state camera: simulation of a very low dose imaging protocol. J Nucl Med. 2013;54:373–379.
8. Halliburton S, Arbab-Zadeh A, Dey D, Einstein AJ, Gentry R, George RT, Gerber T, Mahesh M, Weigold WG. State-of-the-art in CT hardware and scan modes for cardiovascular CT. J Cardiovasc Comput Tomogr. 2012;6:154–163.
9. Halliburton SS, Abbara S, Chen MY, Gentry R, Mahesh M, Raff GL, Shaw LJ, Hausleiter J; Society of Cardiovascular Computed Tomography. SCCT guidelines on radiation dose and dose-optimization strategies in cardiovascular CT. J Cardiovasc Comput Tomogr. 2011;5:198–224.
10. Abbara S, Arbab-Zadeh A, Callister TQ, Desai MY, Mamuya W, Thomson L, Weigold WG. SCCT guidelines for performance of coro-nary computed tomographic angiography: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr. 2009;3:190–204.
11. Huda W. Review of Radiologic Physics. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009.
12. Gutstein A, Dey D, Cheng V, Wolak A, Gransar H, Suzuki Y, Friedman J, Thomson LE, Hayes S, Pimentel R, Paz W, Slomka P, Le Meunier L, Germano G, Berman DS. Algorithm for radiation dose reduction with helical dual source coronary computed tomography angiography in clini-cal practice. J Cardiovasc Comput Tomogr. 2008;2:311–322.
13. Hausleiter J, Martinoff S, Hadamitzky M, Martuscelli E, Pschierer I, Feuchtner GM, Catalán-Sanz P, Czermak B, Meyer TS, Hein F, Bischoff B, Kuse M, Schömig A, Achenbach S. Image quality and radiation ex-posure with a low tube voltage protocol for coronary CT angiography results of the PROTECTION II Trial. J Am Coll Cardiol Cardiovasc Imaging. 2010;3:1113–1123.
14. Leipsic J, LaBounty TM, Mancini GB, Heilbron B, Taylor C, Johnson MA, Hague C, Earls JP, Ajlan A, Min JK. A prospective randomized con-trolled trial to assess the diagnostic performance of reduced tube voltage for coronary CT angiography. AJR Am J Roentgenol. 2011;196:801–806.
15. Gerber TC, Carr JJ, Arai AE, Dixon RL, Ferrari VA, Gomes AS, Heller GV, McCollough CH, McNitt-Gray MF, Mettler FA, Mieres JH, Morin RL, Yester MV. Ionizing radiation in cardiac imaging: a science advisory from the American Heart Association Committee on Cardiac Imaging of the Council on Clinical Cardiology and Committee on Cardiovascular Imaging and Intervention of the Council on Cardiovascular Radiology and Intervention. Circulation. 2009;119:1056–1065.
16. Eller A, Wuest W, Scharf M, Brand M, Achenbach S, Uder M, Lell MM. Attenuation-based automatic kilovolt (kV)-selection in computed to-mography of the chest: effects on radiation exposure and image quality. Eur J Radiol. 2013;82:2386–2391.
17. Einstein AJ, Elliston CD, Arai AE, Chen MY, Mather R, Pearson GD, Delapaz RL, Nickoloff E, Dutta A, Brenner DJ. Radiation dose from single-heartbeat coronary CT angiography performed with a 320-detec-tor row volume scanner. Radiology. 2010;254:698–706.
18. Christner JA, Kofler JM, McCollough CH. Estimating effective dose for CT using dose-length product compared with using organ doses: consequences of adopting International Commission on Radiological Protection publication 103 or dual-energy scanning. AJR Am J Roentgenol. 2010;194:881–889.
19. Hudson HM, Larkin RS. Accelerated image reconstruction using ordered subsets of projection data. IEEE Trans Med Imaging. 1994;13:601–609.
20. Leipsic J, Labounty TM, Heilbron B, Min JK, Mancini GB, Lin FY, Taylor C, Dunning A, Earls JP. Estimated radiation dose reduction using adaptive statistical iterative reconstruction in coronary CT angiography: the ERASIR study. AJR Am J Roentgenol. 2010;195:655–660.
21. Noël PB, Renger B, Fiebich M, Münzel D, Fingerle AA, Rummeny EJ, Dobritz M. Does iterative reconstruction lower CT radiation dose: evalu-ation of 15,000 examinations. PLoS One. 2013;8:e81141.
22. Hoffmann U, Truong QA, Schoenfeld DA, Chou ET, Woodard PK, Nagurney JT, Pope JH, Hauser TH, White CS, Weiner SG, Kalanjian S, Mullins ME, Mikati I, Peacock WF, Zakroysky P, Hayden D, Goehler A, Lee H, Gazelle GS, Wiviott SD, Fleg JL, Udelson JE; ROMICAT-II
Investigators. Coronary CT angiography versus standard evaluation in acute chest pain. N Engl J Med. 2012;367:299–308.
23. Goldstein JA, Chinnaiyan KM, Abidov A, Achenbach S, Berman DS, Hayes SW, Hoffmann U, Lesser JR, Mikati IA, O’Neil BJ, Shaw LJ, Shen MY, Valeti US, Raff GL; CT-STAT Investigators. The CT-STAT (Coronary Computed Tomographic Angiography for Systematic Triage of Acute Chest Pain Patients to Treatment) trial. J Am Coll Cardiol. 2011;58:1414–1422.
24. Min JK, Leipsic J, Pencina MJ, Berman DS, Koo BK, van Mieghem C, Erglis A, Lin FY, Dunning AM, Apruzzese P, Budoff MJ, Cole JH, Jaffer FA, Leon MB, Malpeso J, Mancini GB, Park SJ, Schwartz RS, Shaw LJ, Mauri L. Diagnostic accuracy of fractional flow reserve from anatomic CT angiography. JAMA. 2012;308:1237–1245.
25. Hausleiter J, Meyer T, Hermann F, Hadamitzky M, Krebs M, Gerber TC, McCollough C, Martinoff S, Kastrati A, Schömig A, Achenbach S. Estimated radiation dose associated with cardiac CT angiography. JAMA. 2009;301:500–507.
26. Min JK, Dunning A, Lin FY, Achenbach S, Al-Mallah M, Budoff MJ, Cademartiri F, Callister TQ, Chang HJ, Cheng V, Chinnaiyan K, Chow BJ, Delago A, Hadamitzky M, Hausleiter J, Kaufmann P, Maffei E, Raff G, Shaw LJ, Villines T, Berman DS; CONFIRM Investigators. Age- and sex-related differences in all-cause mortality risk based on coronary com-puted tomography angiography findings results from the International Multicenter CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter Registry) of 23,854 patients without known coronary artery disease. J Am Coll Cardiol. 2011;58:849–860.
27. Rochitte CE, George RT, Chen MY, Arbab-Zadeh A, Dewey M, Miller JM, Niinuma H, Yoshioka K, Kitagawa K, Nakamori S, Laham R, Vavere AL, Cerci RJ, Mehra VC, Nomura C, Kofoed KF, Jinzaki M, Kuribayashi S, de Roos A, Laule M, Tan SY, Hoe J, Paul N, Rybicki FJ, Brinker JA, Arai AE, Cox C, Clouse ME, Di Carli MF, Lima JA. Computed tomogra-phy angiography and perfusion to assess coronary artery stenosis causing perfusion defects by single photon emission computed tomography: the CORE320 study. Eur Heart J. 2014;35:1120–1130.
28. Chinnaiyan KM, Boura JA, DePetris A, Gentry R, Abidov A, Share DA, Raff GL; Advanced Cardiovascular Imaging Consortium Coinvestigators. Progressive radiation dose reduction from coronary computed tomogra-phy angiography in a statewide collaborative quality improvement pro-gram: results from the Advanced Cardiovascular Imaging Consortium. Circ Cardiovasc Imaging. 2013;6:646–654.
29. LaBounty TM, Earls JP, Leipsic J, Heilbron B, Mancini GB, Lin FY, Dunning AM, Min JK. Effect of a standardized quality-improvement protocol on radiation dose in coronary computed tomographic angiogra-phy. Am J Cardiol. 2010;106:1663–1667.
30. Buechel RR, Husmann L, Herzog BA, Pazhenkottil AP, Nkoulou R, Ghadri JR, Treyer V, von Schulthess P, Kaufmann PA. Low-dose com-puted tomography coronary angiography with prospective electrocar-diogram triggering: feasibility in a large population. J Am Coll Cardiol. 2011;57:332–336.
31. Hausleiter J, Bischoff B, Hein F, Meyer T, Hadamitzky M, Thierfelder C, Allmendinger T, Flohr TG, Schömig A, Martinoff S. Feasibility of dual-source cardiac CT angiography with high-pitch scan protocols. J Cardiovasc Comput Tomogr. 2009;3:236–242.
32. Dey D, Nakazato R, Pimentel R, Paz W, Hayes SW, Friedman JD, Cheng VY, Thomson LE, Slomka PJ, Berman DS. Low radiation coronary cal-cium scoring by dual-source CT with tube current optimization based on patient body size. J Cardiovasc Comput Tomogr. 2012;6:113–120.
33. Nakazato R, Dey D, Gutstein A, Le Meunier L, Cheng VY, Pimentel R, Paz W, Hayes SW, Thomson LE, Friedman JD, Berman DS. Coronary artery calcium scoring using a reduced tube voltage and radiation dose protocol with dual-source computed tomography. J Cardiovasc Comput Tomogr. 2009;3:394–400.
34. Voros S, Rivera JJ, Berman DS, Blankstein R, Budoff MJ, Cury RC, Desai MY, Dey D, Halliburton SS, Hecht HS, Nasir K, Santos RD, Shapiro MD, Taylor AJ, Valeti US, Young PM, Weissman G; Society for Atherosclerosis Imaging and Prevention Tomographic Imaging and Prevention Councils; Society of Cardiovascular Computed Tomography. Guideline for minimizing radiation exposure during acquisition of coro-nary artery calcium scans with the use of multidetector computed tomog-raphy: a report by the Society for Atherosclerosis Imaging and Prevention Tomographic Imaging and Prevention Councils in collaboration with the Society of Cardiovascular Computed Tomography. J Cardiovasc Comput Tomogr. 2011;5:75–83.
by guest on June 20, 2018http://circim
aging.ahajournals.org/D
ownloaded from

Dey et al Achieving Very-Low-Dose Cardiac CT, SPECT, and PET 733
35. Marwan M, Mettin C, Pflederer T, Seltmann M, Schuhbäck A, Muschiol G, Ropers D, Daniel WG, Achenbach S. Very low-dose coronary artery calcium scanning with high-pitch spiral acquisition mode: compari-son between 120-kV and 100-kV tube voltage protocols. J Cardiovasc Comput Tomogr. 2013;7:32–38.
36. Gunter DL. Gamma camera collimator characteristics and design. In: Henkin RE, ed. Nuclear Medicine. Vol. 1. Philadelphia, PA: Elsevier; 2006:107–126.
37. Jaszczak RJ, Li J, Wang H, Zalutsky MR, Coleman RE. Pinhole col-limation for ultra-high-resolution, small-field-of-view SPECT. Phys Med Biol. 1994;39:425–437.
38. Schramm NU, Ebel G, Engeland U, Schurrat T, Behe M, Behr TM. High-resolution SPECT using multipinhole collimation. IEEE Trans Nucl Sci. 2003;50:315–320.
39. Beekman FJ, Vastenhouw B. Design and simulation of a high-reso-lution stationary SPECT system for small animals. Phys Med Biol. 2004;49:4579–4592.
40. Sharir T, Slomka PJ, Hayes SW, DiCarli MF, Ziffer JA, Martin WH, Dickman D, Ben-Haim S, Berman DS. Multicenter trial of high-speed versus conventional single-photon emission computed tomography im-aging: quantitative results of myocardial perfusion and left ventricular function. J Am Coll Cardiol. 2010;55:1965–1974.
41. Sharir T, Ben-Haim S, Merzon K, Prochorov V, Dickman D, Ben-Haim S, Berman DS. High-speed myocardial perfusion imaging: initial clinical comparison with conventional dual detector anger camera imaging. J Am Coll Cardio. Cardiovasc Imaging. 2008;1:156–163.
42. Volokh L, Hugg J, Blevis I, Asma E, Jansen F, Manjeshwar R. Effect of detector energy response on image qualityof myocardial perfusion SPECT. Paper presented at IEEE Nuclear Science Symposium and Medical Imaging conference, Dresden, Germany, October 19–26, 2008.
43. Herzog BA, Buechel RR, Husmann L, Pazhenkottil AP, Burger IA, Wolfrum M, Nkoulou RN, Valenta I, Ghadri JR, Treyer V, Kaufmann PA. Validation of CT attenuation correction for high-speed myocardial perfu-sion imaging using a novel cadmium-zinc-telluride detector technique. J Nucl Med. 2010;51:1539–1544.
44. Slomka P, Berman D, Germano G. New imaging protocols for new sin-gle photon emission CT technologies. Curr Cardiovasc Imaging Rep. 2010;3:162–170.
45. Maddahi J, Mendez R, Mahmarian JJ, Thomas G, Babla H, Bai C, Arram S, Maffetone P, Conwell R. Prospective multicenter evaluation of rapid, gated SPECT myocardial perfusion upright imaging. J Nucl Cardiol. 2009;16:351–357.
46. Lau YH, Hutton BF, Beekman FJ. Choice of collimator for cardiac SPET when resolution compensation is included in iterative reconstruction. Eur J Nucl Med. 2001;28:39–47.
47. Einstein AJ, Moser KW, Thompson RC, Cerqueira MD, Henzlova MJ. Radiation dose to patients from cardiac diagnostic imaging. Circulation. 2007;116:1290–1305.
48. Esteves FP, Raggi P, Folks RD, Keidar Z, Askew JW, Rispler S, O’Connor MK, Verdes L, Garcia EV. Novel solid-state-detector dedicated cardiac camera for fast myocardial perfusion imaging: multicenter comparison with standard dual detector cameras. J Nucl Cardiol. 2009;16:927–934.
49. Tilkemeier P, Green J, Einstein AJ, Fazel R, Reames P, Shaw LJ. The evolving practice of nuclear cardiology: results from the 2011 ASNC member survey. J Nucl Cardiol. 2012;19:1170–1175.
50. Einstein AJ, Tilkemeier P, Fazel R, Rakotoarivelo H, Shaw LJ; American Society of Nuclear Cardiology. Radiation safety in nuclear cardiolo-gy-current knowledge and practice: results from the 2011 American Society of Nuclear Cardiology member survey. JAMA Intern Med. 2013;173:1021–1023.
51. Duvall WL, Croft LB, Godiwala T, Ginsberg E, George T, Henzlova MJ. Reduced isotope dose with rapid SPECT MPI imaging: initial experience with a CZT SPECT camera. J Nucl Cardiol. 2010;17:1009–1014.
52. Duvall WL, Croft LB, Ginsberg ES, Einstein AJ, Guma KA, George T, Henzlova MJ. Reduced isotope dose and imaging time with a high-effi-ciency CZT SPECT camera. J Nucl Cardiol. 2011;18:847–857.
53. Gimelli A, Bottai M, Genovesi D, Giorgetti A, Di Martino F, Marzullo P. High diagnostic accuracy of low-dose gated-SPECT with solid-state ultrafast detectors: preliminary clinical results. Eur J Nucl Med Mol Imaging. 2012;39:83–90.
54. DePuey EG, Bommireddipalli S, Clark J, Leykekhman A, Thompson LB, Friedman M. A comparison of the image quality of full-time myo-cardial perfusion SPECT vs wide beam reconstruction half-time and half-dose SPECT. J Nucl Cardiol. 2011;18:273–280.
55. Nkoulou R, Pazhenkottil AP, Kuest SM, Ghadri JR, Wolfrum M, Husmann L, Fiechter M, Buechel RR, Herzog BA, Koepfli P, Burger C, Gaemperli O, Kaufmann PA. Semiconductor detectors allow low-dose-low-dose 1-day SPECT myocardial perfusion imaging. J Nucl Med. 2011;52:1204–1209.
56. Mahmarian JJ. Stress only myocardial perfusion imaging: Is it time for a change? J Nucl Cardiol. 2010;17:529–535.
57. Chang SM, Nabi F, Xu J, Raza U, Mahmarian JJ. Normal stress-only versus standard stress/rest myocardial perfusion imaging: similar pa-tient mortality with reduced radiation exposure. J Am Coll Cardiol. 2010;55:221–230.
58. Bateman TM, Heller GV, McGhie AI, Courter SA, Golub RA, Case JA, Cullom SJ. Multicenter investigation comparing a highly efficient half-time stress-only attenuation correction approach against standard rest-stress Tc-99m SPECT imaging. J Nucl Cardiol. 2009;16:726–735.
59. Nishina H, Slomka PJ, Abidov A, Yoda S, Akincioglu C, Kang X, Cohen I, Hayes SW, Friedman JD, Germano G, Berman DS. Combined supine and prone quantitative myocardial perfusion SPECT: method develop-ment and clinical validation in patients with no known coronary artery disease. J Nucl Med. 2006;47:51–58.
60. Nakazato R, Tamarappoo BK, Kang X, Wolak A, Kite F, Hayes SW, Thomson LE, Friedman JD, Berman DS, Slomka PJ. Quantitative up-right-supine high-speed SPECT myocardial perfusion imaging for de-tection of coronary artery disease: correlation with invasive coronary angiography. J Nucl Med. 2010;51:1724–1731.
61. Husmann L, Herzog BA, Gaemperli O, Tatsugami F, Burkhard N, Valenta I, Veit-Haibach P, Wyss CA, Landmesser U, Kaufmann PA. Diagnostic accuracy of computed tomography coronary angiography and evaluation of stress-only single-photon emission computed tomography/computed tomography hybrid imaging: comparison of prospective electrocardio-gram-triggering vs. retrospective gating. Eur Heart J. 2009;30:600–607.
62. Einstein AJ, Blankstein, R, Andrews H, Fish M, Padgett, R, Hayes, S, Friedman J, Feng M, Qureshi M, Rakotoarivelo H, Gerlach J, Sabahat B, Johnson L, Di Carli M, Berman DS. Comparison of image quality, myocar-dial perfusion and left ventricular function between ultra-low-dose imaging using a high-efficiency solid-state SPECT camera and standard low-dose imaging using an Anger SPECT camera: results from the multicenter nu-clear low-dose imaging at a millisievert (MILLISIEVERT) study. J Am Coll Cardiol. 2013;61:(10_S) doi:10.1016/S0735-1097(13)61007-4 (abstract).
63. Taylor MG, Bateman TM, McGhie AI. Performance of ultra-low dose Tc-99m sestamibi myocardial perfusion imaging using solid-state SPECT: comparison to coronary angiography. Circulation. 2012;2012:A19783 (abstract).
64. Einstein AJ, Johnson LL, Bokhari S, Son J, Thompson RC, Bateman TM, Hayes SW, Berman DS. Agreement of visual estimation of coro-nary artery calcium from low-dose CT attenuation correction scans in hybrid PET/CT and SPECT/CT with standard Agatston score. J Am Coll Cardiol. 2010;56:1914–1921.
65. Bai C, Conwell R, Kindem J, Babla H, Gurley M, De Los Santos R II, Old R, Weatherhead R, Arram S, Maddahi J. Phantom evaluation of a cardiac SPECT/VCT system that uses a common set of solid-state detectors for both emission and transmission scans. J Nucl Cardiol. 2010;17:459–469.
66. Franc BL, Myers R, Pounds TR ,Bolton G, Conte F, Bartheld M, Da Silva AJ. Clinical utility of SPECT-(low-dose) CT versus SPECT alone in patients presenting for bone scintigraphy. Clin Nucl Med. 2012;37: 26–34.
67. Klein R, Beanlands RS, deKemp RA. Quantification of myocar-dial blood flow and flow reserve: Technical aspects. J Nucl Cardiol. 2010;17:555–570.
68. Esteves FP, Nye JA, Khan A, Folks RD, Halkar RK, Garcia EV, Schuster DM, Lerakis S, Raggi P, Votaw JR. Prompt-gamma compensation in Rb-82 myocardial perfusion 3D PET/CT. J Nucl Cardiol. 2010;17:247–253.
69. Knesaurek K, Machac J, Krynyckyi BR, Almeida OD. Comparison of 2-dimensional and 3-dimensional 82Rb myocardial perfusion PET imag-ing. J Nucl Med. 2003;44:1350–1356.
70. Jakoby BW, Bercier Y, Conti M, Casey ME, Bendriem B, Townsend DW. Physical and clinical performance of the mCT time-of-flight PET/CT scanner. Phys Med Biol. 2011;56:2375–2389.
71. Panin VY, Kehren F, Michel C, Casey M. Fully 3-D PET reconstruc-tion with system matrix derived from point source measurements. IEEE Trans Med Imaging. 2006;25:907–921.
72. Le Meunier L, Slomka PJ, Dey D, Ramesh A, Thomson LE, Hayes SW, Friedman JD, Cheng V, Germano G, Berman DS. Enhanced definition PET for cardiac imaging. J Nucl Cardiol. 2010;17:414–426.
73. Le Meunier L, Slomka PJ, Dey D, Ramesh A, Thomson LE, Hayes SW, Friedman JD, Cheng V, Germano G, Berman DS. Motion frozen F-18-FDG cardiac PET. J Nucl Cardiol. 2011;18:259–266.
by guest on June 20, 2018http://circim
aging.ahajournals.org/D
ownloaded from

734 Circ Cardiovasc Imaging July 2014
74. Slomka PJ, Nishina H, Berman DS, Kang X, Akincioglu C, Friedman JD, Hayes SW, Aladl UE, Germano G. “Motion-frozen” display and quantifi-cation of myocardial perfusion. J Nucl Med. 2004;45:1128–1134.
75. Mylonas I, Kazmi M, Fuller L, deKemp RA, Yam Y, Chen L, Beanlands RS, Chow BJ. Measuring coronary artery calcification using positron emission tomography-computed tomography attenuation correction im-ages. Eur Heart J Cardiovasc Imaging. 2012;13:786–792.
76. Burkhard N, Herzog BA, Husmann L, Pazhenkottil AP, Burger IA, Buechel RR, Valenta I, Wyss CA, Kaufmann PA. Coronary calcium score scans for attenuation correction of quantitative PET/CT 13N-ammonia myocardial perfusion imaging. Eur J Nucl Med Mol Imaging. 2010;37:517–521.
77. Senthamizhchelvan S, Bravo PE, Esaias C, Lodge MA, Merrill J, Hobbs RF, Sgouros G, Bengel FM. Human biodistribution and radiation dosim-etry of 82Rb. J Nucl Med. 2010;51:1592–1599.
78. Di Carli MF, Dorbala S, Meserve J, El Fakhri G, Sitek A, Moore SC. Clinical myocardial perfusion PET/CT. J Nucl Med. 2007;48:783–793.
79. Schwaiger M, Ziegler SI, Nekolla SG. PET/CT challenge for the non-invasive diagnosis of coronary artery disease. Eur J Radiol. 2010;73:494–503.
80. Berman DS, Maddahi J, Tamarappoo BK, Czernin J, Taillefer R, Udelson JE, Gibson CM, Devine M, Lazewatsky J, Bhat G, Washburn D. Phase II safety and clinical comparison with single-photon emission computed tomography myocardial perfusion imaging for detection of coronary ar-tery disease: flurpiridaz F 18 positron emission tomography. J Am Coll Cardiol. 2013;61:469–477.
81. Maddahi J, Czernin J, Lazewatsky J, Huang SC, Dahlbom M, Schelbert H, Sparks R, Ehlgen A, Crane P, Zhu Q, Devine M, Phelps M. Phase I, first-in-human study of BMS747158, a novel 18F-labeled tracer for myocardial perfusion PET: dosimetry, biodistribution, safety, and imaging characteristics after a single injection at rest. J Nucl Med. 2011;52:1490–1498.
82. McMahon SR, Kikut J, Pinckney RG, Keating FK. Feasibility of stress only rubidium-82 PET myocardial perfusion imaging. J Nucl Cardiol. 2013;20:1069–1075.
KEY WORDS: cardiac imaging techniques ◼ computed tomography ◼ positron-emission tomography ◼ radiation dosage ◼ tomography, emission-computed, single-photon
by guest on June 20, 2018http://circim
aging.ahajournals.org/D
ownloaded from

Damini Dey, Piotr J. Slomka and Daniel S. BermanSingle-Photon Emission Computed Tomography, and Positron Emission Tomography
Achieving Very-Low-Dose Radiation Exposure in Cardiac Computed Tomography,
Print ISSN: 1941-9651. Online ISSN: 1942-0080 Copyright © 2014 American Heart Association, Inc. All rights reserved.
Dallas, TX 75231is published by the American Heart Association, 7272 Greenville Avenue,Circulation: Cardiovascular Imaging
doi: 10.1161/CIRCIMAGING.113.0008972014;7:723-734Circ Cardiovasc Imaging.
http://circimaging.ahajournals.org/content/7/4/723World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circimaging.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Imaging Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
requested is located, click Request Permissions in the middle column of the Web page under Services. FurtherCenter, not the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright ClearanceCirculation: Cardiovascular Imagingin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 20, 2018http://circim
aging.ahajournals.org/D
ownloaded from


















