Advanced haemodynamics
111
Introduction to Introduction to HEMODYNAMIC MONITORING HEMODYNAMIC MONITORING
-
Upload
lambert-winston -
Category
Health & Medicine
-
view
905 -
download
2
description
Transcript of Advanced haemodynamics

Introduction to Introduction to
HEMODYNAMIC HEMODYNAMIC
MONITORINGMONITORING

22
DEFINITIONDEFINITION
PURPOSE
DEFINITION
HEMODYNAMIC MONITORING
Measuring and monitoring the factors that influence the force and flow of blood.
To aid in diagnosing, monitoring and managing critically ill patients.

33
INDICATIONSINDICATIONS To diagnose shock states To diagnose shock states
To determine fluid volume statusTo determine fluid volume status
To measure cardiac outputTo measure cardiac output
To monitor and manage unstable patients To monitor and manage unstable patients
To assess hemodynamic response to To assess hemodynamic response to therapies therapies
To diagnose primary pulmonary To diagnose primary pulmonary hypertension, valvular disease, intracardiac hypertension, valvular disease, intracardiac shunts, cardiac tamponade, and pulmonary shunts, cardiac tamponade, and pulmonary embolusembolus

44
CONTRAINDICATIONSCONTRAINDICATIONSfor an invasive PA Catheterfor an invasive PA Catheter
Tricuspid or pulmonary valve mechanical Tricuspid or pulmonary valve mechanical prosthesis prosthesis
Right heart mass (thrombus and/or tumor)Right heart mass (thrombus and/or tumor)
Tricuspid or pulmonary valve endocarditisTricuspid or pulmonary valve endocarditis

55
Clinical Scenario Use of PACClinical Scenario Use of PAC Management of complicated MIManagement of complicated MI
Severe LVF/RMI (precise management of heart failure)Severe LVF/RMI (precise management of heart failure) Assessment of respiratory distressAssessment of respiratory distress
Cardiogenic vs non-cardiogenic pulmonary edemaCardiogenic vs non-cardiogenic pulmonary edema Assessment/Diagnosis of shock/ cardiac Assessment/Diagnosis of shock/ cardiac
dysfunctiondysfunction Cardiogenic/hypovolemic/septicCardiogenic/hypovolemic/septic TamponadeTamponade Pulmonary embolismPulmonary embolism Severe dilated cardiomyopathySevere dilated cardiomyopathy
Management of Pulmonary HypertensionManagement of Pulmonary Hypertension Management of high-risk surgical patientsManagement of high-risk surgical patients
CABG, vascular, valvular, aneurysm repairCABG, vascular, valvular, aneurysm repair Management of volume requirements in the Management of volume requirements in the
critically ill critically ill ARF, GI bleed, trauma, sepsis (precise management)ARF, GI bleed, trauma, sepsis (precise management)

66
Hemodynamic ValuesHemodynamic Values CO / CICO / CI SV / SVI or SISV / SVI or SI SVOSVO22
RVEDVI or EDVIRVEDVI or EDVI SVR / SVRISVR / SVRI PVR / PVRIPVR / PVRI RVEFRVEF VOVO22 / VO / VO22II
DODO22 / DO / DO22II PAOPPAOP CVPCVP PAPPAP
Cardiac Output/Cardiac IndexCardiac Output/Cardiac Index Stroke Volume/Stroke Volume IndexStroke Volume/Stroke Volume Index Mixed Venous SaturationMixed Venous Saturation RV End-Diastolic VolumeRV End-Diastolic Volume Systemic Vascular ResistanceSystemic Vascular Resistance Pulmonary Vascular Resistance Pulmonary Vascular Resistance RV Ejection FractionRV Ejection Fraction Oxygen ConsumptionOxygen Consumption Oxygen DeliveryOxygen Delivery Pulmonary Artery Occlusive Pulmonary Artery Occlusive
PressurePressure Central Venous PressureCentral Venous Pressure Pulmonary Artery PressurePulmonary Artery Pressure

77
Index ValuesIndex Values
Values normalized for body size (BSA)Values normalized for body size (BSA)
CI CI is 2.5 – 4.5 L/min/mis 2.5 – 4.5 L/min/m22
SVRI SVRI is 1970 – 2390 dynes/sec/cm-is 1970 – 2390 dynes/sec/cm-5/m5/m22
SVI or SI SVI or SI is 35 – 60 mL/beat/mis 35 – 60 mL/beat/m22
EDVI EDVI is 60 – 100 mL/m2is 60 – 100 mL/m2

88
Importance of Index ValuesImportance of Index Values
Mr. SmithMr. Smith 47 y/o male47 y/o male 60 kg60 kg CO = 4.5CO = 4.5 6 ft tall (72 inches)6 ft tall (72 inches) BSA = 1.8BSA = 1.8 CI = 2.5 L/min/mCI = 2.5 L/min/m22
Mr. JonesMr. Jones 47 y/o male47 y/o male 120 kg120 kg CO = 4.5CO = 4.5 6 ft tall (72 inches)6 ft tall (72 inches) BSA = 2.4BSA = 2.4 CI = 1.9 L/min/m2CI = 1.9 L/min/m2

99
BasicBasic ConceptsConcepts Cardiac Output Cardiac Output - - amount of blood pumped amount of blood pumped
out of the ventricles each minuteout of the ventricles each minute Stroke Volume Stroke Volume - - amount of blood ejected amount of blood ejected
by the ventricle with each contractionby the ventricle with each contraction CO = HR x SVCO = HR x SV
Decreased SV usually produces compensatory Decreased SV usually produces compensatory tachycardia.. tachycardia..
So. . .changes in HR can signal changes in So. . .changes in HR can signal changes in COCO

1010
BasicBasic ConceptsConcepts Systemic Vascular ResistanceSystemic Vascular Resistance
Measurement of the resistance (afterload) of Measurement of the resistance (afterload) of blood flow through systemic vasculatureblood flow through systemic vasculature
*Increased SVR/narrowing PP = vasoconstriction*Increased SVR/narrowing PP = vasoconstriction *Decreased SVR/widening PP = vasodilation*Decreased SVR/widening PP = vasodilation
Blood Pressure Blood Pressure BP = CO x SVRBP = CO x SVR
** ** SVR can increase to maintain BP SVR can increase to maintain BP despite inadequate COdespite inadequate CORememberRemember CO = HR x SV CO = HR x SV

1111
BasicBasic ConceptsConcepts
BP = CO x SVRBP = CO x SVR CO and SVR are inversely relatedCO and SVR are inversely related
CO and SVR will change before BP CO and SVR will change before BP changeschanges
* Changes in BP are a late sign of * Changes in BP are a late sign of hemodynamic alterationshemodynamic alterations

1212
StrokeStroke VolumeVolume Components Stroke VolumeComponents Stroke Volume
Preload: the volume of blood in the the volume of blood in the ventricles at end diastole and the ventricles at end diastole and the stretch placed on the muscle fibersstretch placed on the muscle fibers
Afterload: the resistance the ventricles the resistance the ventricles must overcome to eject it’s volume of must overcome to eject it’s volume of bloodblood
Contractility: the force with which the the force with which the heart muscle contracts (myocardial heart muscle contracts (myocardial compliance)compliance)

1313
StrokeStroke VolumeVolume PreloadPreload AfterloadAfterload ContractilitContractilit
yyFilling Pressures Filling Pressures & Volumes& Volumes
ResistanceResistance to to OutflowOutflow
Strength of Strength of ContractionContraction
CVPCVP
PAOP (PAD may PAOP (PAD may be used to be used to estimate PAOP)estimate PAOP)
PVR, MPAPPVR, MPAP
SVR, MAPSVR, MAPRVSVRVSV
LVSVLVSV
Fluids, Volume Fluids, Volume ExpandersExpanders
DiureticsDiuretics
VasoconstrictorVasoconstrictorss
VasodilatorsVasodilators
InotropicInotropic
MedicationsMedications

1414
ClinicalClinical MeasurementsMeasurements ofof PreloadPreload
Left Side: PAOP/LAP Left Side: PAOP/LAP PAD may be used to estimate PAOP in the PAD may be used to estimate PAOP in the
absence of pulmonary disease/HTNabsence of pulmonary disease/HTN
The pulmonary vasculature is a low pressure The pulmonary vasculature is a low pressure system in the absence of pulmonary diseasesystem in the absence of pulmonary disease
These pressures are “accurate” estimations These pressures are “accurate” estimations of preload only with of preload only with perfect complianceperfect compliance of of heart and lungsheart and lungs
Right Side: CVP/RAP Right Side: CVP/RAP ** filling pressures filling pressures

1515
ClinicalClinical MeasurementsMeasurements ofof AfterloadAfterload
RV AfterloadRV Afterload MPAPMPAP PVR = 150-250 dynes/sec/cmPVR = 150-250 dynes/sec/cm-5-5
PVRI = 255-285 dynes/sec/cmPVRI = 255-285 dynes/sec/cm-5/-5/mm22
LV AfterloadLV Afterload MAPMAP SVR = 800–1300 dynes/sec/cm-5SVR = 800–1300 dynes/sec/cm-5 SVRI = 1970-2390 dynes/sec/cm-5/m2SVRI = 1970-2390 dynes/sec/cm-5/m2

1616
ClinicalClinical EstimationEstimation ofof ContractilityContractility
Cardiac Output Cardiac Output * flow* flow
Normal = 4-8 L/minNormal = 4-8 L/min Cardiac IndexCardiac Index
Normal = 2.5-4.5 L/min/m2Normal = 2.5-4.5 L/min/m2
Stroke VolumeStroke Volume *pump performance*pump performance
Normal = 50-100 ml/beatNormal = 50-100 ml/beat Stroke volume IndexStroke volume Index
Normal = 30-50 ml/beat/m2Normal = 30-50 ml/beat/m2

1717
Ventricular ComplianceVentricular Compliance
Ability of the ventricle to stretchAbility of the ventricle to stretch
Decreased with LV hypertrophy, MI, Decreased with LV hypertrophy, MI, fibrosis, HOCMfibrosis, HOCM
*If compliance is decreased, *If compliance is decreased, smallsmall changes in changes in volumevolume produce produce large large changes in changes in pressurepressure

1818
The PA CatheterThe PA Catheter

1919
Pulmonary Artery CathetersPulmonary Artery Catheters

2020
The Pulmonary Artery The Pulmonary Artery CatheterCatheter

2121
““Swan-Ganz” PA CatheterSwan-Ganz” PA Catheter
Large Markers Large Markers = 50cm= 50cm Small Markers Small Markers = 10cm= 10cm 10 cm between small black markers on 10 cm between small black markers on
cathetercatheter Several typesSeveral types
Thermodilutional COThermodilutional CO CCOCCO PrecepPrecep NICCONICCO
Multiple lumensMultiple lumens

2222
BREAKBREAKTake 5 MINUTESTake 5 MINUTES

2323
Demonstration of PA catheterDemonstration of PA catheterand and
Hands-on practiceHands-on practice

2424
BleedingBleeding InfectionInfection DysrhythmiasDysrhythmias Pulmonary Artery Pulmonary Artery
RuptureRupture PneumothoraxPneumothorax HemothoraxHemothorax Valvular DamageValvular Damage EmbolizationEmbolization Balloon RuptureBalloon Rupture Catheter MigrationCatheter Migration
Risks With The PA CatheterRisks With The PA Catheter

2525

Hemodynamic Hemodynamic WaveformsWaveforms

2727
PA-Catheter PositioningPA-Catheter Positioning
RightRight AtriumAtrium
RightRight VentricleVentricle
PulmonaryPulmonary ArteryArtery
PulmonaryPulmonary ArteryArtery OcclusionOcclusion PressurePressure

2828
PAC Insertion SequencePAC Insertion Sequence

2929
Post PA Catheter InsertionPost PA Catheter Insertion Assess ECG for dysrhythmias.Assess ECG for dysrhythmias. Assess for signs and symptoms of respiratory distress.Assess for signs and symptoms of respiratory distress. Ascertain sterile dressing is in place.Ascertain sterile dressing is in place. Obtain PCXR to check placement.Obtain PCXR to check placement. Zero and level transducer(s) at the phlebostatic axis. Zero and level transducer(s) at the phlebostatic axis. Assess quality of waveforms (i.e., proper configuration, dampening, Assess quality of waveforms (i.e., proper configuration, dampening, catheter whip). catheter whip). Obtain opening pressures and wave form tracings for each Obtain opening pressures and wave form tracings for each waveform.waveform. Assess length at insertion site. Assess length at insertion site. Ensure that all open ends of stopcocks are covered with sterile dead-Ensure that all open ends of stopcocks are covered with sterile dead-end caps (red dead-end caps, injection caps, or male Luer lock caps). end caps (red dead-end caps, injection caps, or male Luer lock caps). Update physician of abnormalities.Update physician of abnormalities.

3030
General Rules for General Rules for Hemodynamic Hemodynamic MeasurementsMeasurements
Measure all pressures at End-ExpirationMeasure all pressures at End-Expiration
““Patient Peak”Patient Peak”
““Vent Valley”Vent Valley”

3131
Phlebostatic AxisPhlebostatic Axis
4th ICS Mid-chest, regardless of head elevation4th ICS Mid-chest, regardless of head elevation

3232
Phlebostatic AxisPhlebostatic Axis
4th ICS Mid-chest, regardless of head elevation4th ICS Mid-chest, regardless of head elevation

3333
Spontaneous RespirationsSpontaneous Respirations
Measure all pressures at Measure all pressures at end-expirationend-expiration At At top curve top curve with spontaneous with spontaneous
respirationrespiration
““patient-peak”patient-peak” Intrathoracic pressure Intrathoracic pressure decreasesdecreases
during spontaneous during spontaneous inspirationinspiration Negative deflection on waveformsNegative deflection on waveforms
Intrathoracic pressure Intrathoracic pressure increasesincreases during during spontaneous spontaneous expirationexpiration
Positive deflection on waveformsPositive deflection on waveforms

3434
Spontaneous RespirationsSpontaneous Respirations

3535
Mechanical VentilationMechanical Ventilation Measure all pressures at Measure all pressures at end-expirationend-expiration At At bottom curvebottom curve with mechanical with mechanical
ventilatorventilator
““vent-valley”vent-valley” Intrathoracic pressure Intrathoracic pressure increases increases during during
positive pressure ventilations positive pressure ventilations ((inspirationinspiration))
Positive deflection on waveformsPositive deflection on waveforms Intrathoracic pressure Intrathoracic pressure decreases decreases
during positive pressure during positive pressure expirationexpiration Negative deflection on waveformsNegative deflection on waveforms

3636

3737

3838
General Rules for General Rules for Hemodynamic MeasurementsHemodynamic Measurements
Measure all pressures with the HOB at a … Measure all pressures with the HOB at a … consistentconsistent level of elevationlevel of elevation
Level the transducer at the Level the transducer at the phlebostatic axisphlebostatic axis 4th intercostal space, mid-chest4th intercostal space, mid-chest
Print strips with one ECG and one pressure Print strips with one ECG and one pressure channelchannel adequate scaleadequate scale allows accurate waveform analysisallows accurate waveform analysis
Confirm monitor pressures with pressures Confirm monitor pressures with pressures obtained by waveform analysisobtained by waveform analysis ** correct waveform analysis is more accurate than ** correct waveform analysis is more accurate than
pressures from the monitorpressures from the monitor

3939
Review of Normal ValuesReview of Normal Values
RAP (CVP)RAP (CVP)
RVPRVP
PAPPAP
PAOPPAOP
0-8 mmHg0-8 mmHg
15-30/0-8 15-30/0-8 mmHgmmHg
15-30/6-12 15-30/6-12 mmHgmmHg
8 - 12 mmHg8 - 12 mmHg

4040
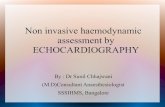
PA INSERTION WAVEFORMSPA INSERTION WAVEFORMS
A = A = RA (CVP) WaveformRA (CVP) Waveform B = RV WaveformB = RV Waveform C = PA WaveformC = PA Waveform D = PAWP WaveformD = PAWP Waveform
B
C D
A

4141
PAC Insertion SequencePAC Insertion Sequence

4242
Right Atrium (CVP)Right Atrium (CVP)
Normal Value 0-8 mmHgRAP = CVPWave Fluctuations Due To Contractions

4343
Components of the RA Components of the RA (CVP) Waveform(CVP) Waveform
a-wavea-wave atrial contraction (systole)atrial contraction (systole) begins in the PR interval and QRS on the begins in the PR interval and QRS on the
ECGECG correct location for measurement of correct location for measurement of
CVP/RAPCVP/RAP * average the peak & trough of the a-wave* average the peak & trough of the a-wave * (a-Peak + a-trough)/2 = CVP* (a-Peak + a-trough)/2 = CVP
May not see if no atrial contractions as with. May not see if no atrial contractions as with. . .. .

4444
Absent a wavesAbsent a waves
Atrial fibrillationAtrial fibrillation
Paced rhythmPaced rhythm
Junctional rhythmJunctional rhythm
Measure at the end of the QRSMeasure at the end of the QRS
Components of the RA Components of the RA (CVP) Waveform(CVP) Waveform

4545
Absent A WaveAbsent A Wave
*PACEP.ORG 2007
* Measure at end of QRS!

4646
c-wavec-wave tricuspid valve closuretricuspid valve closure Between ST segmentBetween ST segment Between a and v wavesBetween a and v waves *may or may not be present*may or may not be present
v-wavev-wave Atrial fillingAtrial filling begins at the end of the QRS to the begins at the end of the QRS to the
beginning of the T wave (QT interval)beginning of the T wave (QT interval)
Components of the RA Components of the RA (CVP) Waveform(CVP) Waveform

4949
Reading the RA CVP) Reading the RA CVP) WaveformWaveform

5050
CVP WaveformCVP Waveform
Vented Patient

5151
CVP WaveformCVP Waveform
Vented Patient – “Vent Valley”
a wave

5353
Right VentricleRight Ventricle
Normal Value 15-25/0-8 mmHgCatheter In RV May Cause EctopySwan Tip May Drift From PA to RV

5454
RV WaveformRV Waveform

5555
Components of the RV Components of the RV WaveformWaveform
Usually only seen with insertionUsually only seen with insertion Systole Systole
measured at the peakmeasured at the peak peak occurs after the QRSpeak occurs after the QRS
DiastoleDiastole measured just prior to the the onset of systolemeasured just prior to the the onset of systole
No dicrotic notchNo dicrotic notch Dicrotic notch indicates valve closureDicrotic notch indicates valve closure *** Aids in differentiation from the PA tracing*** Aids in differentiation from the PA tracing

5656
Reading the RV WaveformReading the RV Waveform

5757
RV Waveform InterventionsRV Waveform Interventions After PA catheter is correctly placed, RV After PA catheter is correctly placed, RV
waveform should not be seen. If it is, waveform should not be seen. If it is, then interventions are necessary:then interventions are necessary: Check for specific unit protocol firstCheck for specific unit protocol first Inflate balloon with patient lying on their left Inflate balloon with patient lying on their left
side (catheter may float back into PA)side (catheter may float back into PA) With deflated balloon, pull catheter into RA With deflated balloon, pull catheter into RA
placement or remove completelyplacement or remove completely Document your actions and notify physicianDocument your actions and notify physician
** An RN should NEVER advance the ** An RN should NEVER advance the catheter!catheter!

5858
Pulmonary ArteryPulmonary Artery
Normal Value 15-25/8-15 mmHgDicrotic Notch Represents PV ClosurePAD Approximates PAWP (LVEDP) (in absence of lung or MV disease)

5959
PA WaveformPA Waveform

6060
Components of the PA Components of the PA WaveformWaveform
SystoleSystole measured at the peak of the wavemeasured at the peak of the wave
DiastoleDiastole measured just prior to the upstroke of measured just prior to the upstroke of
systole (end of QRS)systole (end of QRS) Higher than RV diastolic pressureHigher than RV diastolic pressure

6161
Dicrotic notchDicrotic notch indicates pulmonic valve closureindicates pulmonic valve closure aids in differentiation from RV waveformaids in differentiation from RV waveform aids in determining waveform qualityaids in determining waveform quality
Anachrotic NotchAnachrotic Notch Before upsweep to systoleBefore upsweep to systole Opening of pulmonic valveOpening of pulmonic valve
Components of the PA Components of the PA WaveformWaveform

6262
Reading the PA WaveformReading the PA Waveform
Dicrotic notch

6363
PA WaveformPA Waveform
Identify that it is the PA tracing
Look at the scale
What is the PAP?
10/20/30

6464
PA WaveformPA Waveform
Look for dichrotic notch
Look at scale
What is the PAP?

6565
PAOP / WedgePAOP / Wedge
Normal Value 8-12 mmHgBalloon Floats and Wedges in Pulmonary Artery PAWP = LAP = LVEDP Wedging Can Cause Capillary Rupture

6666
a-wavea-wave atrial contractionatrial contraction correct location for measurement of correct location for measurement of
PAOPPAOP average the peak & trough of the a-waveaverage the peak & trough of the a-wave
begins near the end of QRS or the QT begins near the end of QRS or the QT segmentsegment
* Delayed ECG correlation from CVP since * Delayed ECG correlation from CVP since PA catheter is further away from left atriumPA catheter is further away from left atrium
Components of the PA Components of the PA WaveformWaveform

6767
c-wavec-wave rarely presentrarely present represents mitral valve closurerepresents mitral valve closure
v-wavev-wave represents left atrial fillingrepresents left atrial filling begins at about the end of the T begins at about the end of the T
wave wave
Components of the PA Components of the PA WaveformWaveform

6868
Reading the PAOP WaveformReading the PAOP Waveform
Begins within the QRS or the QT segment

6969
Wedging Can Cause Wedging Can Cause Pulmonary Artery Pulmonary Artery
RuptureRupture

7070
PA Tracing to PAOP Tracing to PA Tracing to PAOP Tracing to PA TracingPA Tracing

7171
Post PAC InsertionPost PAC Insertion Assess ECG for dysrythmiasAssess ECG for dysrythmias Assess for S/S of respiratory distressAssess for S/S of respiratory distress Be sure sterile dressing is appliedBe sure sterile dressing is applied Order CXR for placement Order CXR for placement
Get MD order before infusing through portsGet MD order before infusing through ports
Zero and level all transducersZero and level all transducers Assess quality of waveformsAssess quality of waveforms
Dampening, proper configuration, scaleDampening, proper configuration, scale
Obtain opening pressures and waveform tracings for Obtain opening pressures and waveform tracings for each waveformeach waveform
Note length at insertion siteNote length at insertion site Place proper luer-lock connectors to lumens and cap Place proper luer-lock connectors to lumens and cap
all portsall ports Notify MD of any abnormalitiesNotify MD of any abnormalities

7272
PrecautionsPrecautions Always set alarms on monitor Always set alarms on monitor
20mmHg above and below pt baseline20mmHg above and below pt baseline
If in PAOP with balloon down, have pt If in PAOP with balloon down, have pt cough, deep breath, change positioncough, deep breath, change position
If unable to dislodge from PAOP, notify MD If unable to dislodge from PAOP, notify MD immediately to reposition catheterimmediately to reposition catheter CXR to reconfirm placementCXR to reconfirm placement
If pt coughs up blood or it is suctioned via If pt coughs up blood or it is suctioned via ETT, suspect PA rupture and notify MD ETT, suspect PA rupture and notify MD immediatelyimmediately

7373
Intermittent Thermodilution Intermittent Thermodilution COCO
Based on measuring blood temperature Based on measuring blood temperature changeschanges
Must know the following:Must know the following: Computation constantComputation constant
Volume of injectateVolume of injectate
Temperature of injectate Temperature of injectate Iced or room temperatureIced or room temperature
Inject rapidly and smoothly over 4 seconds maxInject rapidly and smoothly over 4 seconds max Thermister at end of PA catheter detects Thermister at end of PA catheter detects
change in temperature and creates CO curvechange in temperature and creates CO curve At least 3 measurements and average resultsAt least 3 measurements and average results

7474
Cardiac Output via Cardiac Output via ThermodilutionThermodilution
*PACEP.ORG 2007

7575
Averaging CO Averaging CO MeasurementsMeasurements
*PACEP.ORG 2007

7676
Continuous Cardiac OutputContinuous Cardiac Output A heat signal is produced by the thermal A heat signal is produced by the thermal
filament of the PA catheterfilament of the PA catheter
The signal is detected by the thermistor on The signal is detected by the thermistor on the PA catheter and is converted into a the PA catheter and is converted into a time/temperature curvetime/temperature curve
The CCO computer produces a time-The CCO computer produces a time-averaged calculationaveraged calculation Over 3 minutesOver 3 minutes
Updates every 30-60 secondsUpdates every 30-60 seconds

7777
Mixed Venous Oxygen Mixed Venous Oxygen SaturationSaturation

7878
Mixed Venous Oxygenation Mixed Venous Oxygenation Monitoring Monitoring
(SvO2)(SvO2) Measures the amount of OMeasures the amount of O22 in the blood (on in the blood (on
the Hgb molecule) returned to the heartthe Hgb molecule) returned to the heart
Helps to demonstrate the balance between OHelps to demonstrate the balance between O2 2
supply & demand in the body supply & demand in the body (tissue (tissue oxygenation)oxygenation)
Helps to interpret hemodynamic dysfunction Helps to interpret hemodynamic dysfunction when used with other measurementswhen used with other measurements
Normal: 70% (60-80)Normal: 70% (60-80)

7979
Mixed Venous Oxygen Mixed Venous Oxygen SaturationSaturation
End result of OEnd result of O22 delivery and delivery and consumptionconsumption
Measured in the Measured in the pulmonary arterypulmonary artery An average estimate of venous An average estimate of venous
saturation for the whole body.saturation for the whole body.
**Does not reflect separate tissue **Does not reflect separate tissue perfusion or oxygenationperfusion or oxygenation

8080
Mixed Venous Oxygen Mixed Venous Oxygen SaturationSaturation
Continuous measurementContinuous measurement
““Early” warning signal to detect Early” warning signal to detect oxygen transport imbalancesoxygen transport imbalances
Evaluates the effect of the Evaluates the effect of the therapeutic interventionstherapeutic interventions
Identify potential patient care Identify potential patient care consequences (turning, suctioning)consequences (turning, suctioning)

8181
Mixed Venous Oxygen Mixed Venous Oxygen SaturationSaturation
There are four factors that affect SVOThere are four factors that affect SVO22::
1.1. HemoglobinHemoglobin
2.2. Cardiac outputCardiac output
3.3. Arterial oxygen saturation (SaOArterial oxygen saturation (SaO22))
4.4. Oxygen consumption (VOOxygen consumption (VO22))

8282
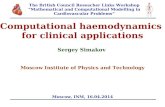
SvO2 ApplicationSvO2 Application
In a case of increased SVR with decreased CO. Nitroprusside was started. The increase in SvO2 and increase in CO reflects the appropriateness of therapy.

8383
Ways To Increase O2 Ways To Increase O2 DeliveryDelivery
Increase COIncrease CO increase HR, optimize preload, decrease increase HR, optimize preload, decrease
afterload, add positive inotropes afterload, add positive inotropes
Increase Hgb, increase SaO2Increase Hgb, increase SaO2
Improve pulmonary functionImprove pulmonary function pulmonary toilet, prevent atelectasispulmonary toilet, prevent atelectasis
ventilation strategiesventilation strategies

8484
Ways To Decrease O2 DemandWays To Decrease O2 Demand Decrease muscle activityDecrease muscle activity
sedatives, (paralytics)sedatives, (paralytics)
prevent/control seizuresprevent/control seizures
prevent/control shiveringprevent/control shivering
space care activitiesspace care activities
Decrease temperatureDecrease temperature prevent/control feverprevent/control fever

8585
Removal of the PA CatheterRemoval of the PA Catheter
Usually performed by the nurse Usually performed by the nurse withwith an MD order an MD order
Place patient supine with HOB flatPlace patient supine with HOB flat (reduces chance of air embolus)(reduces chance of air embolus)

8686
Removal of the PA CatheterRemoval of the PA Catheter
Make sure balloon is down, have Make sure balloon is down, have patient inhale and hold breath, patient inhale and hold breath, pull PA catheter out smoothlypull PA catheter out smoothly monitor for ventricular ectopymonitor for ventricular ectopy stop immediately & notify MD if stop immediately & notify MD if
resistance is metresistance is met

8787
Removal of the PA CatheterRemoval of the PA Catheter

8888
Removal of the PA CatheterRemoval of the PA Catheter
If patient is unable to perform breath If patient is unable to perform breath hold:hold: Pull PA catheter during period of positive Pull PA catheter during period of positive
intrathoracic pressure to minimize chance of intrathoracic pressure to minimize chance of venous air embolusvenous air embolus
Mechanically ventilated patientMechanically ventilated patient pull PA catheter during delivery of vent pull PA catheter during delivery of vent
breath breath Spontaneously breathing patientSpontaneously breathing patient pull PA catheter during exhalationpull PA catheter during exhalation

8989
Removal of the PA CatheterRemoval of the PA Catheter If introducer sheath (cordis) is to remain in If introducer sheath (cordis) is to remain in
place, it place, it must be cappedmust be capped..
If introducer sheath (cordis) is to be If introducer sheath (cordis) is to be removed, repeat the steps used for PA removed, repeat the steps used for PA catheter removal.catheter removal.
Hold pressure on the site (5-10 min.), keep Hold pressure on the site (5-10 min.), keep patient flat until hemostasis is achieved.patient flat until hemostasis is achieved.
Apply sterile dressing or band-aid.Apply sterile dressing or band-aid.

9090
BreakBreakTake 5 MinutesTake 5 Minutes

9191
Hemodynamic Hemodynamic Waveform PracticeWaveform Practice

9292
MEASUREMENTSMEASUREMENTS

9393
SAMPLE MEASUREMENTSSAMPLE MEASUREMENTS

9494
SAMPLE MEASUREMENTSSAMPLE MEASUREMENTS

9595
SAMPLE MEASUREMENTSSAMPLE MEASUREMENTS

9696
SAMPLE MEASUREMENTSSAMPLE MEASUREMENTS

9797
SAMPLE MEASUREMENTSSAMPLE MEASUREMENTS

9898
SAMPLE MEASUREMENTSSAMPLE MEASUREMENTS

9999
SAMPLE MEASUREMENTSSAMPLE MEASUREMENTS

100100
SAMPLE MEASUREMENTSSAMPLE MEASUREMENTS

101101
SAMPLE MEASUREMENTSSAMPLE MEASUREMENTS

102102
SAMPLE MEASUREMENTSSAMPLE MEASUREMENTS

103103
SAMPLE MEASUREMENTSSAMPLE MEASUREMENTS

104104
SAMPLE MEASUREMENTSSAMPLE MEASUREMENTS

105105
SAMPLE MEASUREMENTSSAMPLE MEASUREMENTS

106106
SAMPLE MEASUREMENTSSAMPLE MEASUREMENTS

107107
ReviewReview

108108
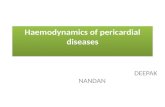
ReviewReview
The PA diastolic pressure is The PA diastolic pressure is measured at which part of measured at which part of the waveform?the waveform?
Just prior to the upstroke of
systole

109109
ReviewReview
Which part of the CVP and Which part of the CVP and PAOP waveforms is used to PAOP waveforms is used to calculate pressures?calculate pressures?
The a wave

110110
ReviewReview
The RV waveform can be The RV waveform can be distinguished from the PA distinguished from the PA waveform by:waveform by:
RV has lower diastolic pressure and no dicrotic
notch

111111
ReviewReview
The v wave of the CVP & The v wave of the CVP & PAOP waveforms represents:PAOP waveforms represents:
Atrial filling

112112
ReviewReview
The a wave of the CVP The a wave of the CVP waveform correlates with waveform correlates with which electrical event?which electrical event?
The PR interval on the ECG

113113
ReviewReview
The a wave of the PAOP The a wave of the PAOP waveform correlates with waveform correlates with which electrical event?which electrical event?
The QRS on the ECG

114114
Questions?Questions?