


Advanced abdominal ultrasound. 4th IFAD, Antwerp Hilton Jeoffrey Schouten AZ Nikolaas.
67
Advanced abdominal ultrasound. 4th IFAD, Antwerp Hilton Jeoffrey Schouten AZ Nikolaas
-
Upload
milton-barton -
Category
Documents
-
view
217 -
download
0
Transcript of Advanced abdominal ultrasound. 4th IFAD, Antwerp Hilton Jeoffrey Schouten AZ Nikolaas.

Advanced abdominal ultrasound.
4th IFAD, Antwerp Hilton
Jeoffrey Schouten
AZ Nikolaas

2
Summary
1. Diffuse liver disease
2. Gallbladder and bile duct disorders
3. Renal disorders
4. Abdominal aneurysm
5. Abdominal trauma

Diffuse liver disease
1. Cardiac liver
2. Liver steatosis/dark liver
3. Liver cirrhosis
4. Budd Chiari syndrome
5. Portal vein thrombosis

Cardiac liver
• Aspecific hepatomegaly (‘trop belle image du foie’)
• Pericardial/pleural effusion • Ascites • Dilatation inferior caval vein, loss
respiratory variation• Dilatation hepatic veins (> 1 cm at 2 cm
from the confluence)

Cardiac liver

Cardiac liver
InspirationExpiration

Diffuse liver disease
1. Cardiac liver
2. Liver steatosis/dark liver
3. Liver cirrhosis
4. Budd Chiari syndrome
5. Portal vein thrombosis

Global steatosis
• Detecting liver fat• Sensitivity: 60-94%• Specificity: 66-95%
• US CAN NOT DIFFERENTIATE BETWEEN STEATOSIS AND FIBROSIS

Echostructure: ‘dark liver’
Diffuse liver disease
1. Cardiac liver
2. Liver steatosis/dark liver
3. Liver cirrhosis
4. Budd Chiari syndrome
5. Portal vein thrombosis

Liver cirrhosis
• Hepatic signs of liver cirrhosis• Rounded marginal edges• Irregular surface• Dysmorphism • Regeneration nodules • Increased echogenicity (subjective)• Heterogeneous echostructure (subjective)• Retraction hepatic veins, loss triphasic flow pattern
• Extrahepatic signs of liver cirrhosis• Signs of portal hypertension

Cirrhosis
CAVE: DD inflammation

Cirrhosis: nodularity

Cirrhosis US signs: nodularity
• Alterations at liver surface • Low frequency probe (5 MHz): lower liver border • ONLY macronodular cirrhosis/ low sensitivity !!!
• High frequency probe (7.5MHz):• Observation subcutaneous liver border (micronodular
cirrhosis)• Nodularity no exclusive sign of liver cirrhosis• Nodular regenerative hyperplasia• Metastasis• Steatosis

Macronodular cirrhosis


Cirrhosis: hepatic vein border irregularities

HF probe: diagnosis micronodular cirrhosis
Sensitivity: 91,1% PPV: 93,2%Specificity: 93,5% NPV: 91,5%

Acute liver failure: contours abnormalities

Cirrhosis: dysmorfism
• Liver dysmorfism in patients with cirrhosis• Hypertrophy caudate lobe• Different indices possible• CAVE Budd Chiari Syndrome
• Hypotrophy right liver• Hypertrophy left liver
• Pathological mechanism:• Anatomy of caudate lobe (changes in blood supply)

Venosum ligament
nodularity

US signs of PHT
• Portal vein changes• Collaterals (umbilical vein, splenic collaterals, epigastric
collaterals)• Ascites• Small amounts: in more dependent positions• Paracolic pouch• Hepatorenal pouch (Morrison)• Douglas pouch
• Gallbladder wall dilatation• Splenomegaly
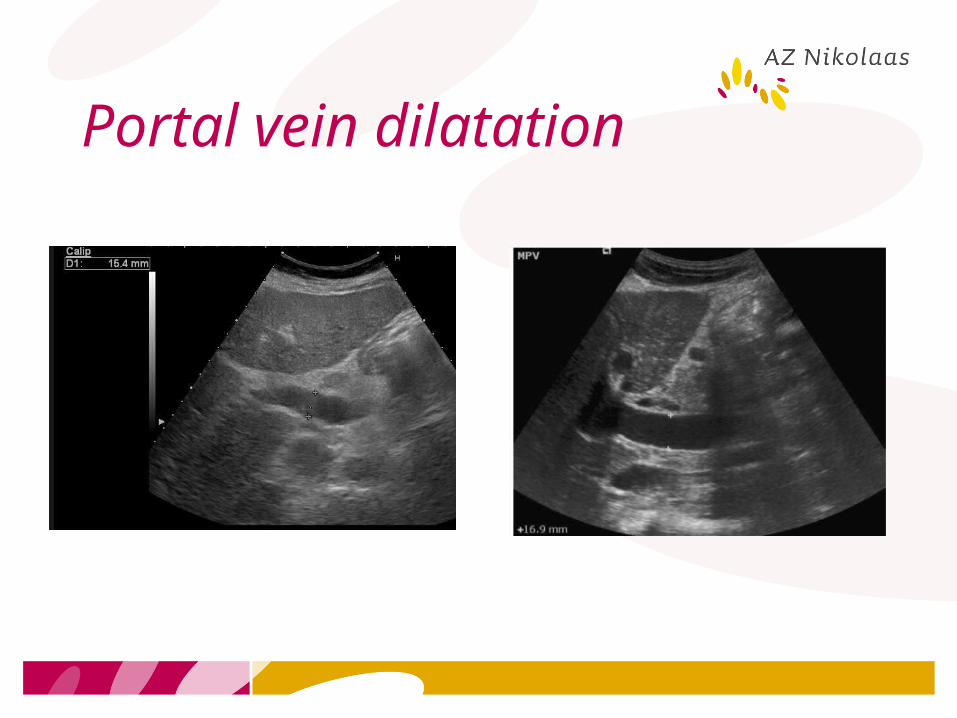
Portal vein dilatation

Hepatofugal flow in portal vein branch

Umbilical vein
• Recanalization in presence of PHT• Normally obliterated fibrous remnant in ligament teres• Extends from the umbilicus to the left portal vein• From the umbilicus it extends to inferior epigastric veins
communicating with the iliofemoral system• US features:• Hypoechogenic band running in lig teres

Umbilical vein

Collaterals: umbilical vein

Collaterals: umbilical vein: collaterals

Splenic collaterals

Ascites: ‘crescent sign’
Morrison pouch
250mL fluid

Gross ascites

Diffuse liver disease
1. Cardiac liver
2. Liver steatosis/dark liver
3. Liver cirrhosis
4. Budd Chiari syndrome
5. Portal vein thrombosis

Budd Chiari Syndrome
• US diagnosis of BCS• Specific signs• Hepatic vein obstruction (acute vs chronic)
• Suggestive signs• Intrahepatic collaterals• Caudate vein > 3mm
• Non-specific signs• Caudate lobe hypertrophy• Inhomogeous parenchyma• Extrahepatic collaterals

BCS: chronic

Budd Chiari Syndrome (BCS)

BCS: IVC thrombus

Diffuse liver disease
1. Cardiac liver
2. Liver steatosis/dark liver
3. Liver cirrhosis
4. Budd Chiari syndrome
5. Portal vein thrombosis

39
Acute portal vein thrombosis

40

41
Chronic portal vein thrombosis

42
Summary
1. Diffuse liver disease
2. Gallbladder and bile duct disorders
3. Renal disorders
4. Abdominal aneurysm
5. Trauma

43
Gallbladder and bile ducts
1. Cholecystitis
2. Bile duct dilatation

Acute cholecystitis
• Thickening gallbladder wall
• Oedema gallbladder wall (continuous echo-poor rim around gallbladder or focal echopoor zone in the wall)
• Ultrasonic Murphy’s sign• Pericholecystic fluid• Round shape• Gallstones

Acute cholecystitis


Gallbladder empyema

Common bile duct: size
• Measurement: proximal portion, just caudal to porta hepatis• Average in adults 4
mm, up to 6 mm is normal
• Increase with age up to 10 mm ??
• Increase after cholecystectomy up to 8-10 mm ??


Bile duct stonesDifficulties• Superposition of duodenum air• Absence of acoustic shadowing • Air in the common bile duct

Dilated intrahepatic bile ducts



Dilated intrahepatic bile ducts

55
Summary
1. Diffuse liver disease
2. Gallbladder and bile duct disorders
3. Renal disorders
4. Abdominal aneurysm
5. Abdominal trauma

56
Renal stones

57
Hydronephrosis

58
Summary
1. Diffuse liver disease
2. Gallbladder and bile duct disorders
3. Renal disorders
4. Abdominal aneurysm
5. Trauma

60
Abdominal aorta aneurysm
Longitudinal Transverse

61
Summary
1. Diffuse liver disease
2. Gallbladder and bile duct disorders
3. Renal disorders
4. Abdominal aneurysm
5. Abdominal trauma

62
Splenic trauma

63
Splenic rupture

64
Renal trauma

65
Liver trauma

66
Subcapsular hematoma

67
TIPS and TRICKS
1. Investigate the whole abdomen
2. If possible, ask the patient the region of pain
3. In trauma patients, parenchymal lesions can show subtle abnormalities


















