Adult-Onset Nemaline Myopathy Presenting as Respiratory...
5
Case Reports Adult-Onset Nemaline Myopathy Presenting as Respiratory Failure Emer Kelly MD, Michael A Farrell MB FRCPI FRCPC FRCPath, and Noel G McElvaney MB BCh BAO FRCPI Nemaline myopathy is a rare congenital myopathy that generally presents in childhood. We report a case of a 44-year-old man who presented with severe hypoxic hypercapnic respiratory failure as the initial manifestation of nemaline myopathy. After starting noninvasive ventilation, his pulmo- nary function test results improved substantially, and over the 4 years since diagnosis his respira- tory function remained stable. There are few reported cases of respiratory failure in patients with adult-onset nemaline myopathy, and the insidious onset in this case is even more unusual. This case highlights the varied presenting features of adult-onset nemaline myopathy and that noninvasive ventilation improves respiratory function. Key words: nemaline myopathy, respiratory failure. [Respir Care 2008;53(11):1490 –1494. © 2008 Daedalus Enterprises] Introduction Nemaline myopathy is a rare congenital myopathy that can have a varied presentation. Despite the congenital na- ture of nemaline myopathy, it may not present until adult- hood. Its rarity and diverse symptoms can make it difficult to diagnosis. We saw a former athlete who presented with subacute respiratory insufficiency in middle age. Nonin- vasive ventilation (NIV) improved his symptoms and sta- bilized his respiratory function. Case Report A 44-year-old man was referred by his family doctor to the respiratory clinic for cough, dyspnea on climbing stairs, and reduced energy, for 8 –12 weeks. On detailed history, the patient stated that he had noted no weakness until 6 years ago, at age 38 years. Initially he had noted some mild lower-extremity weakness, which occasionally caused him to fall. He noted difficulty in moving his toes appropriately. He still walked approxi- mately 1 km each morning but noted difficulty climbing hills or stairs, due to the weakness. This progressed to involve the upper limbs, and he had some difficulty ab- ducting both arms and found it difficult to lift objects off a table. By the time of presentation to the respiratory clinic this had progressed to involve more proximal muscles, in particular the hip flexors. He had only noticed involve- ment of his shoulder girdle very recently. SEE THE RELATED EDITORIAL ON PAGE 1434 The cough and shortness of breath were present prior to 4 months preceding respiratory review, and he had noted some problems with his breathing over the last 6 years. This had been characterized by a very insidious onset of dyspnea, about which he was slow to comment. He had not suffered respiratory infections. He did note morning headaches, daytime somnolence, and decreased concentra- tion in the last year. He was the son of healthy, non-consanguineous white parents. He had 6 siblings, 5 of whom were alive and well. One of his brothers was a smoker and had respiratory difficulties thought to be related to chronic obstructive pulmonary disease. There was no family history of neu- romuscular disease. Our patient’s birth had been a full- term normal vaginal delivery and his mother did not note Emer Kelly MD is affiliated with the Department of Respiratory Re- search, Michael A Farrell MB FRCPI FRCPC FRCPath is affiliated with the Department of Neuropathology, and Noel G McElvaney MB BCh BAO FRCPI is affiliated with the Department of Respiratory Medicine, Beaumont Hospital, Dublin, Ireland. The authors report no conflicts of interest related to the content of this paper. Correspondence: Emer Kelly MD, Department of Respiratory Research, Royal College of Surgeons in Ireland (RCSI), Smurfit Building, Beau- mont Hospital, Dublin 9, Ireland. E-mail: [email protected]. 1490 RESPIRATORY CARE • NOVEMBER 2008 VOL 53 NO 11
Transcript of Adult-Onset Nemaline Myopathy Presenting as Respiratory...
Case Reports
Adult-Onset Nemaline Myopathy Presenting as Respiratory Failure
Emer Kelly MD, Michael A Farrell MB FRCPI FRCPC FRCPath, andNoel G McElvaney MB BCh BAO FRCPI
Nemaline myopathy is a rare congenital myopathy that generally presents in childhood. We reporta case of a 44-year-old man who presented with severe hypoxic hypercapnic respiratory failure asthe initial manifestation of nemaline myopathy. After starting noninvasive ventilation, his pulmo-nary function test results improved substantially, and over the 4 years since diagnosis his respira-tory function remained stable. There are few reported cases of respiratory failure in patients withadult-onset nemaline myopathy, and the insidious onset in this case is even more unusual. This casehighlights the varied presenting features of adult-onset nemaline myopathy and that noninvasiveventilation improves respiratory function. Key words: nemaline myopathy, respiratory failure. [RespirCare 2008;53(11):1490–1494. © 2008 Daedalus Enterprises]
Introduction
Nemaline myopathy is a rare congenital myopathy thatcan have a varied presentation. Despite the congenital na-ture of nemaline myopathy, it may not present until adult-hood. Its rarity and diverse symptoms can make it difficultto diagnosis. We saw a former athlete who presented withsubacute respiratory insufficiency in middle age. Nonin-vasive ventilation (NIV) improved his symptoms and sta-bilized his respiratory function.
Case Report
A 44-year-old man was referred by his family doctor tothe respiratory clinic for cough, dyspnea on climbing stairs,and reduced energy, for 8–12 weeks.
On detailed history, the patient stated that he had notedno weakness until 6 years ago, at age 38 years. Initially he
had noted some mild lower-extremity weakness, whichoccasionally caused him to fall. He noted difficulty inmoving his toes appropriately. He still walked approxi-mately 1 km each morning but noted difficulty climbinghills or stairs, due to the weakness. This progressed toinvolve the upper limbs, and he had some difficulty ab-ducting both arms and found it difficult to lift objects offa table. By the time of presentation to the respiratory clinicthis had progressed to involve more proximal muscles, inparticular the hip flexors. He had only noticed involve-ment of his shoulder girdle very recently.
SEE THE RELATED EDITORIAL ON PAGE 1434
The cough and shortness of breath were present prior to4 months preceding respiratory review, and he had notedsome problems with his breathing over the last 6 years.This had been characterized by a very insidious onset ofdyspnea, about which he was slow to comment. He hadnot suffered respiratory infections. He did note morningheadaches, daytime somnolence, and decreased concentra-tion in the last year.
He was the son of healthy, non-consanguineous whiteparents. He had 6 siblings, 5 of whom were alive and well.One of his brothers was a smoker and had respiratorydifficulties thought to be related to chronic obstructivepulmonary disease. There was no family history of neu-romuscular disease. Our patient’s birth had been a full-term normal vaginal delivery and his mother did not note
Emer Kelly MD is affiliated with the Department of Respiratory Re-search, Michael A Farrell MB FRCPI FRCPC FRCPath is affiliated withthe Department of Neuropathology, and Noel G McElvaney MB BChBAO FRCPI is affiliated with the Department of Respiratory Medicine,Beaumont Hospital, Dublin, Ireland.
The authors report no conflicts of interest related to the content of thispaper.
Correspondence: Emer Kelly MD, Department of Respiratory Research,Royal College of Surgeons in Ireland (RCSI), Smurfit Building, Beau-mont Hospital, Dublin 9, Ireland. E-mail: [email protected].
1490 RESPIRATORY CARE • NOVEMBER 2008 VOL 53 NO 11
any respiratory or feeding difficulties in his neonatal pe-riod. His motor and speech development were normal andhe had met the developmental milestones within expectednorms. He described a normal childhood, in which he wasable to run and play games without any limitations. He hadplayed competitive football until his early thirties.
On initial examination he was noted to have cyanosisand chemosis. On respiratory examination he had poorchest expansion (only 3 cm), reduced air entry, crackles inthe base of the left lung, reduced tidal percussion, andmarked orthopnea. Cardiovascular examination was unre-markable.
Neurologic examination, including cranial nerve exam-ination and fundoscopy, was normal. No facial weaknessor fatigability was noted. There was bilateral muscle wast-ing at the superior head of the pectoralis major, the dorsalrotator cuff, and, to a lesser degree, the biceps and triceps.There was moderate and symmetrical weakness in: shoul-der abduction and adduction; elbow flexion and extension;wrist flexion and extension; finger flexion, extension, andabduction/adduction; hip flexion, extension, and abduc-tion/adduction; knee flexion and extension; ankle dorsi-flexion; and plantar flexion and inversion/eversion. Coor-dination was normal throughout. Reflexes were presentbut reduced throughout. Proprioception, vibration, temper-ature, pain, and light touch were normal in the upper andlower limbs. Gait examination revealed a high-steppinggait with bilateral foot drop.
Blood tests showed polycythemia (hemoglobin 17.8 g/dL) but normal creatine kinase, aldolase, erythrocyte sed-imentation rate, C-reactive protein, serum protein electro-phoresis, antinuclear antibody, rheumatoid factor, anti-neutrophilic cytoplasmic antibody, thyroid function,vitamin B12, and folate. Arterial blood gas analysis re-vealed hypoxic hypercapnic respiratory failure: pH 7.31,PaCO2
80 mm Hg, PO240 mm Hg, and HCO3 39 mmol/L.
Those values indicate severe hypoxia and hypercapnia.The elevated HCO3 indicates a compensatory metabolicalkalosis. However, that pH is low, which indicates onlypartial compensation and an element of acute-on-chronicrespiratory failure.
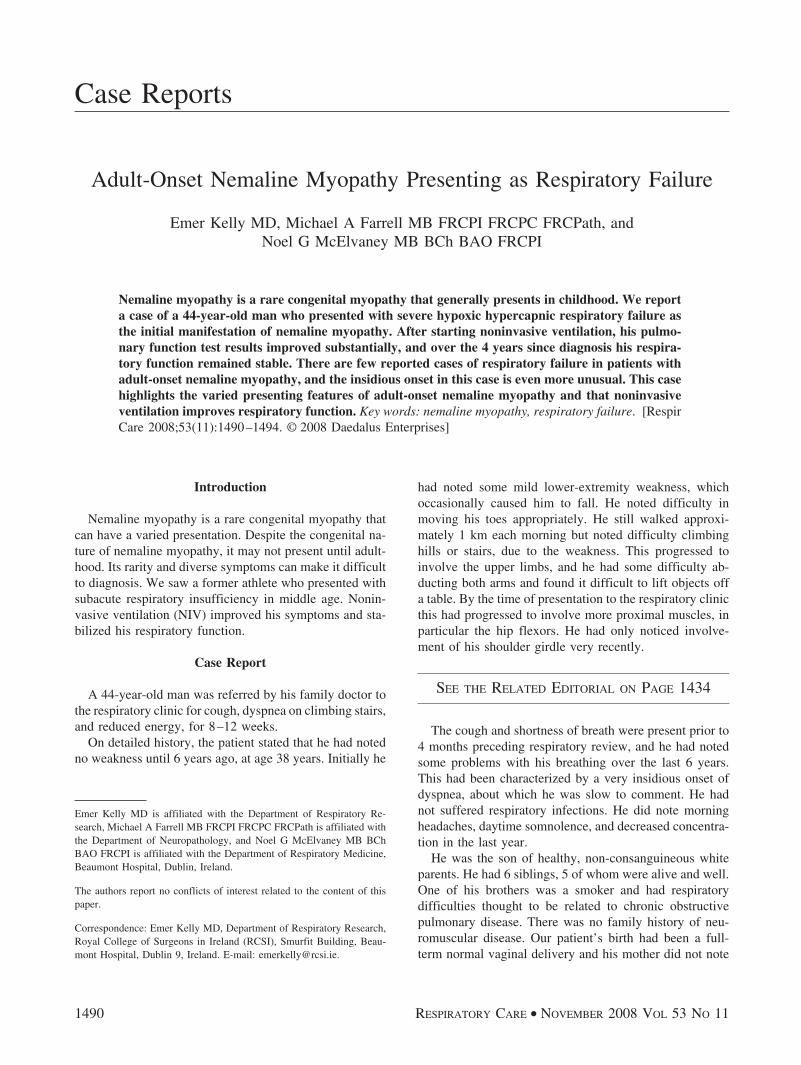
Pulmonary function tests showed a classic restrictivepattern, with mainly extrathoracic involvement, consistentwith neuromuscular problems (Fig. 1 and Table ).
Electromyogram showed spontaneous activity in mostof the muscles tested, along with the predominantly shortand low-amplitude motor action potentials, which suggestmyopathy. He also had high-amplitude long action poten-tials, which is a mixed result that can sometimes be con-sistent with inflammatory myopathies. There was no neu-rophysiologic evidence of a multifocal motor neuropathyor demyelinating process.
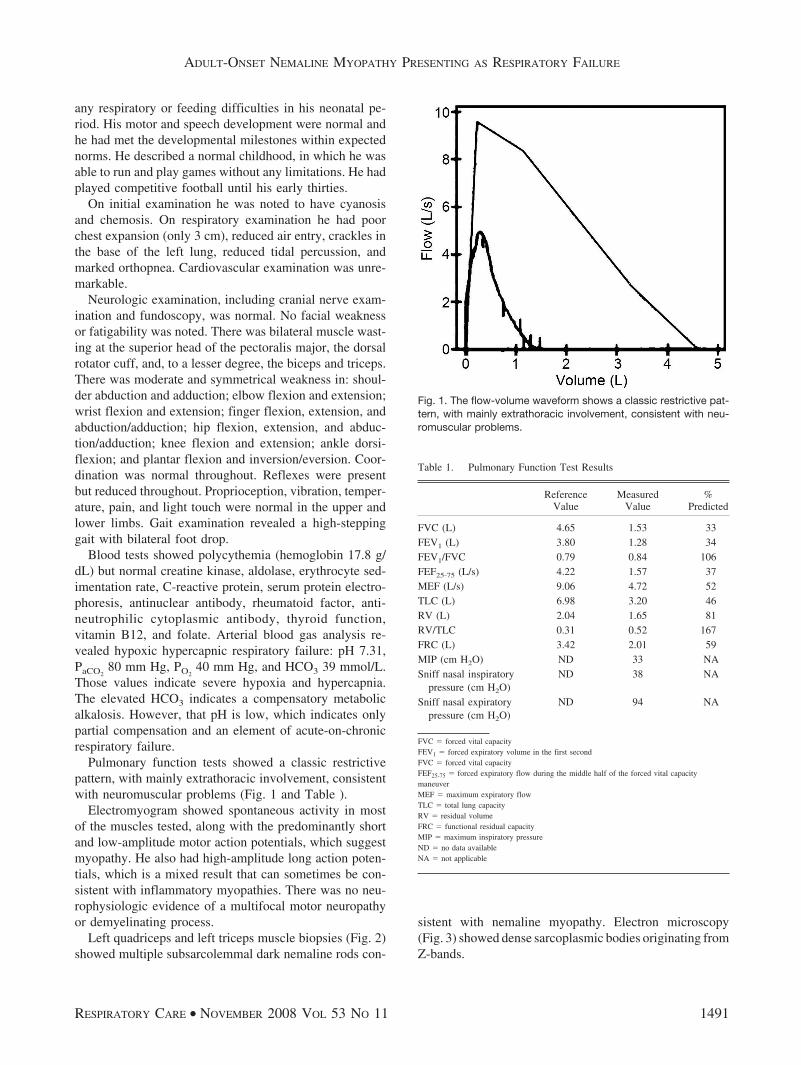
Left quadriceps and left triceps muscle biopsies (Fig. 2)showed multiple subsarcolemmal dark nemaline rods con-
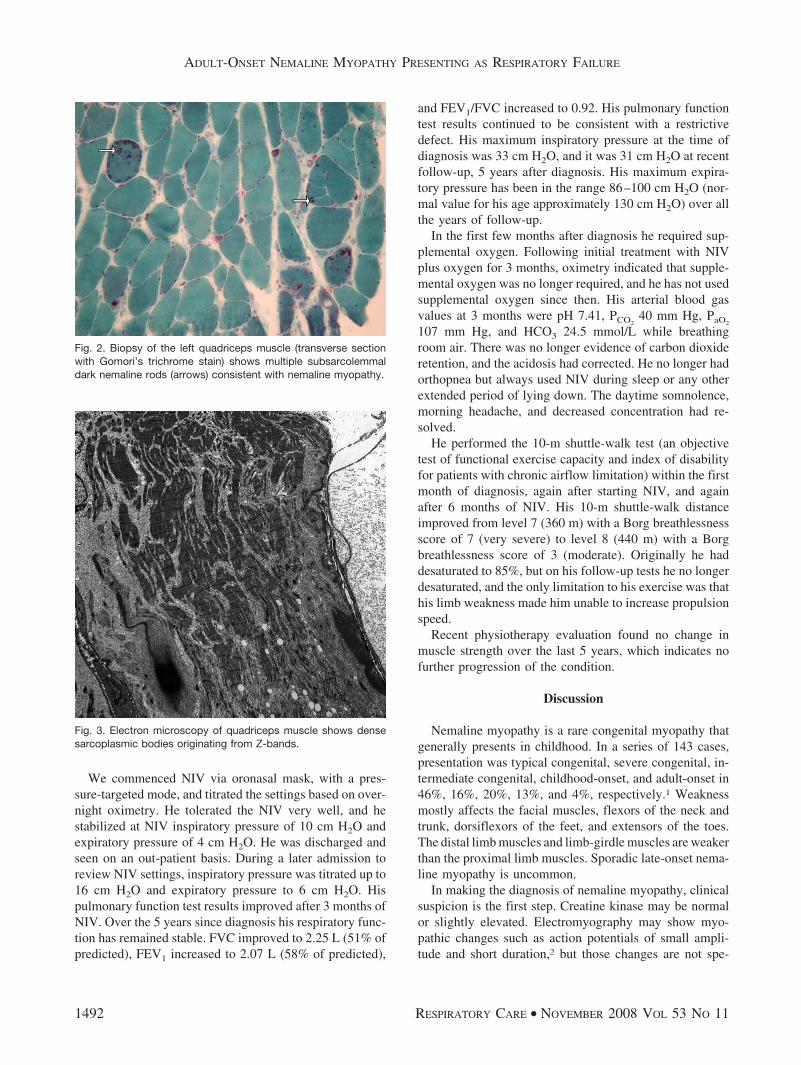
sistent with nemaline myopathy. Electron microscopy(Fig. 3) showed dense sarcoplasmic bodies originating fromZ-bands.
Fig. 1. The flow-volume waveform shows a classic restrictive pat-tern, with mainly extrathoracic involvement, consistent with neu-romuscular problems.
Table 1. Pulmonary Function Test Results
ReferenceValue
MeasuredValue
%Predicted
FVC (L) 4.65 1.53 33FEV1 (L) 3.80 1.28 34FEV1/FVC 0.79 0.84 106FEF25-75 (L/s) 4.22 1.57 37MEF (L/s) 9.06 4.72 52TLC (L) 6.98 3.20 46RV (L) 2.04 1.65 81RV/TLC 0.31 0.52 167FRC (L) 3.42 2.01 59MIP (cm H2O) ND 33 NASniff nasal inspiratory
pressure (cm H2O)ND 38 NA
Sniff nasal expiratorypressure (cm H2O)
ND 94 NA
FVC � forced vital capacityFEV1 � forced expiratory volume in the first secondFVC � forced vital capacityFEF25-75 � forced expiratory flow during the middle half of the forced vital capacitymaneuverMEF � maximum expiratory flowTLC � total lung capacityRV � residual volumeFRC � functional residual capacityMIP � maximum inspiratory pressureND � no data availableNA � not applicable
ADULT-ONSET NEMALINE MYOPATHY PRESENTING AS RESPIRATORY FAILURE
RESPIRATORY CARE • NOVEMBER 2008 VOL 53 NO 11 1491
We commenced NIV via oronasal mask, with a pres-sure-targeted mode, and titrated the settings based on over-night oximetry. He tolerated the NIV very well, and hestabilized at NIV inspiratory pressure of 10 cm H2O andexpiratory pressure of 4 cm H2O. He was discharged andseen on an out-patient basis. During a later admission toreview NIV settings, inspiratory pressure was titrated up to16 cm H2O and expiratory pressure to 6 cm H2O. Hispulmonary function test results improved after 3 months ofNIV. Over the 5 years since diagnosis his respiratory func-tion has remained stable. FVC improved to 2.25 L (51% ofpredicted), FEV1 increased to 2.07 L (58% of predicted),
and FEV1/FVC increased to 0.92. His pulmonary functiontest results continued to be consistent with a restrictivedefect. His maximum inspiratory pressure at the time ofdiagnosis was 33 cm H2O, and it was 31 cm H2O at recentfollow-up, 5 years after diagnosis. His maximum expira-tory pressure has been in the range 86–100 cm H2O (nor-mal value for his age approximately 130 cm H2O) over allthe years of follow-up.
In the first few months after diagnosis he required sup-plemental oxygen. Following initial treatment with NIVplus oxygen for 3 months, oximetry indicated that supple-mental oxygen was no longer required, and he has not usedsupplemental oxygen since then. His arterial blood gasvalues at 3 months were pH 7.41, PCO2
40 mm Hg, PaO2
107 mm Hg, and HCO3 24.5 mmol/L while breathingroom air. There was no longer evidence of carbon dioxideretention, and the acidosis had corrected. He no longer hadorthopnea but always used NIV during sleep or any otherextended period of lying down. The daytime somnolence,morning headache, and decreased concentration had re-solved.
He performed the 10-m shuttle-walk test (an objectivetest of functional exercise capacity and index of disabilityfor patients with chronic airflow limitation) within the firstmonth of diagnosis, again after starting NIV, and againafter 6 months of NIV. His 10-m shuttle-walk distanceimproved from level 7 (360 m) with a Borg breathlessnessscore of 7 (very severe) to level 8 (440 m) with a Borgbreathlessness score of 3 (moderate). Originally he haddesaturated to 85%, but on his follow-up tests he no longerdesaturated, and the only limitation to his exercise was thathis limb weakness made him unable to increase propulsionspeed.
Recent physiotherapy evaluation found no change inmuscle strength over the last 5 years, which indicates nofurther progression of the condition.
Discussion
Nemaline myopathy is a rare congenital myopathy thatgenerally presents in childhood. In a series of 143 cases,presentation was typical congenital, severe congenital, in-termediate congenital, childhood-onset, and adult-onset in46%, 16%, 20%, 13%, and 4%, respectively.1 Weaknessmostly affects the facial muscles, flexors of the neck andtrunk, dorsiflexors of the feet, and extensors of the toes.The distal limb muscles and limb-girdle muscles are weakerthan the proximal limb muscles. Sporadic late-onset nema-line myopathy is uncommon.
In making the diagnosis of nemaline myopathy, clinicalsuspicion is the first step. Creatine kinase may be normalor slightly elevated. Electromyography may show myo-pathic changes such as action potentials of small ampli-tude and short duration,2 but those changes are not spe-
Fig. 2. Biopsy of the left quadriceps muscle (transverse sectionwith Gomori’s trichrome stain) shows multiple subsarcolemmaldark nemaline rods (arrows) consistent with nemaline myopathy.
Fig. 3. Electron microscopy of quadriceps muscle shows densesarcoplasmic bodies originating from Z-bands.
ADULT-ONSET NEMALINE MYOPATHY PRESENTING AS RESPIRATORY FAILURE
1492 RESPIRATORY CARE • NOVEMBER 2008 VOL 53 NO 11

cific. Diagnosis is confirmed with muscle biopsy, whichshows characteristic rod bodies, best seen with modifiedGomori trichrome staining.
The initial differential diagnosis in our patient includedmany causes of neuromuscular respiratory failure, includ-ing demyelinating neuropathy, an unusual myopathy, ormitochondrial disease. Motor neuron disease was consid-ered, but the absence of wasting and symmetry was againstthat diagnosis. Myasthenia gravis was also considered, butthere were no bulbar symptoms. Muscle biopsy providedthe definitive diagnosis of nemaline myopathy.
Nemaline myopathy derives its name from the charac-teristic rod bodies in muscle, which appear threadlike inlongitudinal section. Engel first described sporadic late-onset nemaline myopathy in 1966, in 2 patients.3 Sincethen much has been discovered about nemaline myopathyand its complex genetics.
Nemaline myopathy is clinically and genetically heter-ogeneous.4 Mutations in 5 different genes that code forsarcomeric proteins have been reported to cause nemalinemyopathy: the nebulin gene,5 �-tropomyosin gene,6,7 �-tro-pomyosin gene,8 �-actin gene,9,10 and the gene that en-codes slow skeletal muscle troponin T.11 The 70th Inter-national Workshop on Nemaline Myopathy in 1999 reachedconsensus on 5 categories of nemaline myopathy:12 severecongenital (which is the typical form); intermediate con-genital; mild childhood-onset or juvenile-onset; adult-on-set forms; and other forms. Although the adult-onset formshave the inclusion criterion that onset is as an adult, age ofonset is clearly not always the same as age at presentation,thus careful history-taking and scrutinizing of clinical notesare necessary to determine age of onset in individual cases.After a normal childhood and appropriately reaching de-velopmental milestones, our patient developed muscleweakness in adult life, so his was adult-onset nemalinemyopathy.
Nemaline myopathy with respiratory symptoms is veryuncommon. In 2005, Chahin et al described observationsand long-term follow-up in 14 patients with sporadic late-onset nemaline myopathy, examined at the Mayo Clinicbetween 1975 and 2003.13 A conclusion of that study wasthat sporadic late-onset nemaline myopathy presents withsubacutely evolving weakness after age 40. The weaknesswas predominantly proximal in 11 patients, equally prox-imal and distal in 3 patients, and asymmetric in 4 patients.The weakness began in the arms in 6 patients, and in8 patients the arms were more severely affected than thelegs. One patient had head-drop and 2 patients also hadsubstantial abdominal-muscle weakness. Six patients haddysphagia. Sensory examination was normal in all the pa-tients. No patient in that study presented with respiratorycomplaints.
Falga-Tirado et al reported on a 49-year-old womanwho presented with respiratory insufficiency from nema-
line myopathy.14 Another case report was of a patient withmild nemaline myopathy and sleep hypoventilation due toa mutation in the skeletal muscle �-actin gene.15 That39-year-old woman had a previous diagnosis of nemalinemyopathy when she developed life-threatening respiratoryfailure following a pneumonia. Kudou et al described 2cases of congenital nemaline myopathy that presented withrespiratory failure: one had muscle weakness since birth,and the other presented with slowly progressing respira-tory failure.16
Our 44-year-old male patient presented with minimalclinical symptoms but severe hypoxic hypercapnic respi-ratory failure as the initial manifestation of adult-onsetnemaline myopathy. Presentation with respiratory failureis exceptionally rare in nemaline myopathy. Previous pub-lished cases often had either preexisting nemaline myop-athy or known muscle weakness from birth.15,16 Two casereports have described adult-onset nemaline myopathy thatpresented with respiratory failure.14,16 Our patient’s respi-ratory function initially improved and then stabilized withnocturnal NIV and has remained stable for the 5 yearssince diagnosis.
The reason(s) for our patient’s improvement and stabi-lization is unclear. Long-term mechanical ventilation hasan established role in the management of ventilatory fail-ure due to neuromuscular disease, having gained credenceduring the polio myelitis epidemics in the middle of thelast century.17 It was not until the early 1980s that NIV viamask was pioneered by Rideau et al18 in France, and sub-sequently by Bach et al19 in the United States. Large-cohort studies found that NIV can extend survival in pa-tients with nonprogressive conditions, such that theseindividuals are likely to have a nearly normal life expect-ancy.20-22 The benefits of nighttime NIV are sustained dur-ing the day. Several possible mechanisms have been con-sidered. Hill suggested that NIV may work by improvingventilatory mechanics, resting fatigued respiratory mus-cles and thereby improving strength and endurance, orenhancing ventilatory sensitivity to CO2.23 Some of theinitial improvement in our patient may have been due toreversal of atelectasis, which is likely to be present be-cause of chronic hypoventilation. Reversing the micro-atelectasis probably accounts for the improved FVC.
After intermittent ventilation, Annane et al found: in-creased daytime PaO2
; decreased PaCO2and total bicarbon-
ate; unchanged vital capacity, total lung capacity, maxi-mum inspiratory or expiratory pressure, or alveolar-arterialoxygen difference; decreased apnea-hypopnea index andtime spent with arterial oxygen saturation � 90%; in-creased sleep efficiency and mean arterial oxygen satura-tion; and significantly increased ventilatory response toCO2.24 The reduction in PaCO2
after NIV correlated solelywith the increase in the slope of ventilatory response to theCO2 curve (r � �0.68, P � .008). They concluded that
ADULT-ONSET NEMALINE MYOPATHY PRESENTING AS RESPIRATORY FAILURE
RESPIRATORY CARE • NOVEMBER 2008 VOL 53 NO 11 1493

improvement of daytime hypoventilation with nocturnalNIV may be from an adaptation of the central chemore-ceptors to the reduction of profound hypercapnia duringsleep, or from better sleep quality. Further work found thatpatients who used NIV for � 4 h per night had signifi-cantly improved hypercapnic ventilatory response andPaCO2
after 3 months, whereas in patients who averaged� 4 h of NIV per night, chemosensitivity and arterialblood gas values returned to baseline at 3 months, afterinitial improvement at 5 days.25 A Cochrane review fromAnnane et al, however, concluded that, although the evi-dence is directionally consistent, more randomized con-trolled trials of long-term nocturnal NIV in neuromusculardisease are required.26
Our patient made a rare presentation of a very uncom-mon condition. The case highlights the broad differentialdiagnosis of dyspnea, the varied presentation of adult-onset nemaline myopathy, and the potential respiratory-function benefit of NIV.
REFERENCES
1. Ryan MM, Schnell C, Strickland CD, Shield LK, Morgan G, Ian-naccone ST, et al. Nemaline myopathy: a clinical study of 143 cases.Ann Neurol 2001;50(3):312-320.
2. Wallgren-Pettersson C, Sainio K, Salmi T. Electromyography incongenital nemaline myopathy. Muscle Nerve 1989;12(7):587-593.
3. Engel AG. Late onset rod myopathy (a new syndrome?): light andelectron microscopic observations in two cases. Mayo Clin Proc1966;41(11):713-741.
4. Pelin K, Donner K, Holmberg M, Jungbluth H, Muntoni F, Wall-gren-Pettersson C. Nebulin mutations in autosomal recessive nema-line myopathy: an update. Neuromuscul Disord 2002;12(7-8):680-686.
5. Pelin K, Hilpela P, Sewry C, Akkari PA, Wilton SD, Wattanasir-ichaigoon D, et al. Mutations in the nebulin gene associated withautosomal recessive nemaline myopathy. Proc Natl Acad Sci USA1999;96(5):2305-2310.
6. Laing NG, Wilton SD, Akkari PA, Dorosz S, Boundy K, KneeboneC, et al. A mutation in the alpha-tropomyosin gene TPM3 associatedwith autosomal dominant nemaline myopathy NEM1. Nat Genet1995;10(2):249.
7. Tan P, Briner J, Boltshauser E, Davis MR, Wilton SD, North K, etal. Homozygosity for a nonsense mutation in the alpha-tropomyosinslow gene TPM3 in a patient with severe infantile nemaline myop-athy. Neuromuscul Disord 1999;9(8):573-579.
8. Donner K, Ollikainen M, Ridanpaa M, Christen HJ, Goebel HH, deVisser M, et al. Mutations in the �-tropomyosin (TPM2) gene: a rarecause of nemaline myopathy. Neuromuscul Disord 2002;12(2):151-158.
9. Nowak KJ, Wattanasirichaigoon D, Goebel HH, Wilce M, Pelin K,Donner K, et al. Mutations in the skeletal muscle alpha actin gene in
patients with actin myopathy and nemaline myopathy. Nat Genet1999;23(2):208-212.
10. Ilkovski B, Cooper ST, Nowak K, Ryan MM, Yang N, Schnell C, etal. Nemaline myopathy caused by mutations in the muscle �-skele-tal-actin gene. Am J Hum Genet 2001;68(6):1333-1343.
11. Johnston JJ, Kelley RI, Crawford TO, Morton DH, Agarwala R,Koch T, et al. A novel nemaline myopathy in the Amish caused bya mutation in troponin T1. Am J Hum Genet 2000;67(4):814-821.
12. Wallgren-Pettersson C, Laing NG. Report of the 70th ENMC Inter-national Workshop: nemaline myopathy. June 11th-13th, 1999, Naar-den, The Netherlands. Neuromuscul Disord 2000;10(4-5):299-306.
13. Chahin N, Selcen D, Engel A. Sporadic late onset nemaline myop-athy. Neurology 2005;65(8):1158-1164.
14. Falga-Tirado C, Perez-Peman P, Ordi-Ros J, Bofill JM, Balcells E.Adult onset nemaline myopathy presenting as respiratory insuffi-ciency. Respiration 1995;62(6):353-354.
15. Jungbluth H, Sewry CA, Brown SC, Nowak KJ, Laing NG, Wall-gren-Pettersson C, et al. Mild phenotype of nemaline myopathy withsleep hypoventilation due to a mutation in the skeletal muscle �-ac-tin (ACTA1) gene. Neuromusc Disord 2001;11(2):35-40.
16. Kudou M, Kobayashi Y, Yamashita K, Kita H, Yasuba H, HamadaK. [Two cases of nemaline myopathy diagnosed after episodes ofrespiratory failure.] Nihon Kokyuki Gakkai Zasshi 2006;44(6):474-478. Article in Japanese.
17. Simonds AK. Recent advances in respiratory care for neuromusculardisease. Chest 2006;130(6):1879-1886.
18. Rideau Y, Janoski LW, Grellet G. Respiratory function in the mus-cular dystrophies. Muscle Nerve 1981;4(2):155-164.
19. Bach JR, Alba A, Mosher, Delaubier A. Intermittent positive pres-sure ventilation via nasal access in the management of respiratoryinsufficiency. Chest 1987;94(1):168-170.
20. Leger P, Bedicam JM, Cornette A, Reybet-Degat O, Langevin B,Polu JM, et al. Nasal intermittent positive pressure ventilation:longtem follow-up in patients with severe chronic respiratory insuffi-ciency. Chest 1994;105(1):100-105.
21. Simonds AK, Elliott MW. Outcome of domiciliary nasal intermittentpositive pressure ventilation in restrictive and obstructive disorders.Thorax 1995;50(6):604-609.
22. Baydur A, Layne E, Aral H, Krishnareddy N, Topacio R, FrederickG, Bodden W. Long term noninvasive ventilation in the communityfor patients with musculoskeletal disorders: a 46 year experience andreview. Thorax 2000;55(1):4-11.
23. Hill NS. Noninvasive ventilation: does it work, for whom, and how?Am Rev Respir Dis 1993;147(4):1050-1055.
24. Annane D, Quera-Salva MA, Lofaso F, Vercken JB, Lesieur O,Fromageot C, et al. Mechanisms underlying the effects of nocturnalventilation on daytime blood gases in neuromuscular diseases. EurRespir J 1999;13(1):157-162.
25. Nickol AN, Hart N, Hopkinson NS, Moxham J, Simonds A, PolkeyMI. Mechanisms of improvement of respiratoyr failure in patientswith restrictive thoracic disease treated with noninvasive ventilation.Thorax 2005;60(9):754-760.
26. Annane D, Orlikowski D, Chevret S, Chevrolet JC, Raphael JC.Nocturnal mechanical ventilation for chronic hypoventilation in pa-tients with neuromuscular and chest wall disorders. Cochrane Data-base Syst Rev 2007;(4):CD001941.
ADULT-ONSET NEMALINE MYOPATHY PRESENTING AS RESPIRATORY FAILURE
1494 RESPIRATORY CARE • NOVEMBER 2008 VOL 53 NO 11