ADRENAL CORTEX DISEASE AND PHAEOCHROMOCYTOMAS.ppt
47
ADRENAL CORTEX DISEASE AND PHAEOCHROMOCYTOMAS Luthfan Budi Purnomo Sub Division of Endocrinology Internal Medicine Department
-
Upload
jamaluddin-ahmad-am -
Category
Documents
-
view
24 -
download
1
Transcript of ADRENAL CORTEX DISEASE AND PHAEOCHROMOCYTOMAS.ppt

ADRENAL CORTEX DISEASE AND PHAEOCHROMOCYTOMAS
Luthfan Budi Purnomo
Sub Division of Endocrinology
Internal Medicine Department

Competencies Adrenal Cortex failure 3B Phaeochromocytomas 1 Addison’s disease 1
DiscussionAdrenal hormones: glucocorticoid, mineralocorticoid, and adrenal androgenAdrenal cortex diseases: Cushing’s syndrome and Addison’s disease, mineralocorticoid excessPhaeochromocytoma

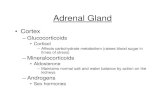
Adrenal Gland: Anatomy
Cortex
Capsule
Zona glomerulosa
Zona fasciculata
Zona reticularis
Medulla
MineralocorticoidsAldosterone
100 to 150 ug/day
Cortisol 10 to 20 mg/day
Adrenal androgens20 mg/day
Norepinephrine (NE)Epinephrine (EPI)Bioactive amines
(lack 17α-hydroxylase)
(lack aldosterone synthase)

Hormones of Adrenal Cortex
Mineralocorticoid: (aldosterone 100-150ug/d), zona glomerulosa, predominantly under the control of the renin-angiotensin system, only 5-10% under ACTH regulation.
It maintenances normal Na+ and K+ concentrations and extracellular fluid volume
Glucocorticoid: (cortisol 10-20 mg/d), zona fasciculata and reticularis, under ACTH control
Adrenal androgen: zona fasciculata and reticularis, under ACTH control

Synthesis of adrenal cortex hormones
Cholesterol Pregnenolone
Progesterone 17-hydroxypregnenolone
Deoxycortisone 17-hydroxyprogesterone
Dehydroepiandrosterone (DHEA)
Corticosterone 11-deoxycortisol Androstenedione
Aldosterone Cortisol Cortisone
17-hydroxylase

Adrenocortical Diseases
Glucocorticoid Excess Cushing’s syndrome Pseudo-Cushing’s syndromesGlucocorticoid ResistanceGlucocorticoid Deficiency Primary hypoadrenalism Secondary hypoadrenalism Post-chronic corticosteroid
replacement therapy
Mineralocorticoid ExcessMineralocorticoid Deficiency Defects in aldosterone
synthesis Defects in aldosterone action hyporeninemic
hypoaldosteronismAdrenal incidentalomas,
Adenomas, and Carcinomas

Production and secretion of aldosterone
Kidney
Lungs
Adrenal
Na+
Blood pressure
Sympathetic input
Angiotensinogen
Angiotensin I
Convertingenzyme (ACE)
PituitaryK+
ACTH
Angiotensin II
Angiotensin III
Aldosterone
Renin

Mineralocorticoid excess
The majority of cases are due to aldosterone excess production (primary or secondary), and are typically associated with hypertension and hypokalaemia
Primary hyper-aldosteronism is a disorder of autonomous hyper-secretion with suppressed renin level
Secondary hyper-aldosteronism when hyper-secretion occurs secondary to elevated circulating renin level

Causes of mineraloorticoid excess
Primary hyperaldosteronism Conn’s syndrome (aldosterone-producing adrenal adenoma bilateral adrenal hyperplasia, glucocorticoid suppressible
hyper-aldosteronism (GSH), aldosterone-producing adrenal carcinoma
Secondary hyper-aldosteronism Renal artery stenosis, renal hypo-perfusion, cirrhosis,
congestive cardiac failure, nephrotic syndrome, renin-secreting tumor
Other mineralocorticoid excess syndromes Apparent mineralocorticoid excess, liquorice ingestion,
deoxycorticosterone and corticosterone, extopic ACTH secretion, congenital adrenal hyperplasia, exogenous mineralocorticoid
Pseudoaldosteronism due to abnormal renal tubular transport Batters syndrome, Gitelman’s syndrome, Liddle’s syndrome

Causes of primary hyperaldosteronism
Conditon Relative frequency
Age Sex Pathology
Aldosteronoma
(Conn’s adenoma)
70% 3rd – 6th decade Female> Beningn, <2.5 cm in diameter, adenoma
Idiopathic aldosteronism/ adrenal hyperplasia
Common Older than Conn’s
No sex difference
Macronodular or micronodular hypeplasia
Adrenal carcinoma Rare 5th -7th decade Female> >4 cm in diameter or larger, local invasion
Glucoorticoid suppressible hyperaldosteronism
Rare Childhood No sex differance
Bilateral hyperplasia of zona glomerulosa

Primary hyperaldosteronism: screening
Resistance to conventional antihypertensive therapy, hypertension with hypokalaemia, hypertension before age 40 years
Serum potassium (hypokalaemic alkalosis), 20-40% normokalaemia
Urinary potassium excretion >30 mmol/24 h with hypokalaemia
Plasma renin (supressed) Aldosterone: renin ratio (pmol/L:ng/ml/h >750) or
(ng/dl:ng/ml/h >30-50)

Drugs and investigation of renin-angiotensin II axis
Drugs Effect Duration of washout (weeks)
ACEI & Angiotensin II antagonistsDiureticsSpironolactoneBeta blockersCalcium channel blockers
PRA PRA PRA PRA PRA
22622

Confirmation
Oral salt loading (120 mmol sodium/d for 3 days) Postural test: failure of aldosterone to rise to more than a
third above baseline is suggestive of an adenoma (ACTH dependent)
Urinary 18 hydroxycortisol (elevated): GSH>> Conn’s> adrenal hyperplasia
Dexamethasone suppression test. Treatment with dexamethasone 0.5 mg/6 h for >3 days leads to lowering of aldosterone and blood pressure in GSH

Differential diagnosis of primary hyperaldosteronism
Test Upright posture
and time
ACEI Dexametha-sone
suppression
Normal PRA Aldosterone
Aldosterone producing PRAadenoma Aldosterone
Angiotensin- PRAresponsive adenoma Aldosterone
Idiopathic adrenal PRAhyperplasia AldosteroneGSH PRA Aldosterone
→
→
→
→
→
→
→
→
→
→
→
→
→
→

Treatment of primary hyperaldosteronism
Surgery Medical treatment: spironolactone (200-400
mg/d), or combination with ACEI and calcium channel blockers. Side effect: gynaecomastia, impotence, menstrual irrigularities, gastrointestinal effects
GSH: dexamethasone 0.5 mg on going to bed and 0.25 mg on waking, or spironolactone

Glucocorticoids
In the liver: increased glycogen deposition; increased gluconeogenesis
Muscle & Fat: inhibits glucose uptake & utilization; increased lipolysis FFA increased cholesterol & triglycerides; decreased HDL-cholesterol
Permissive effect of other hormones
increase blood glucose; protein & lipid catabolism

ACTION OF GLUCOCORTICOIDS
Brain/CNS: depression, psychosis Eye: glaucoma Endocrine system: LH, FSH release, TSH release,
GH secretion GI tract: peptic ulceration Carbohydrate/lipid metabolism: hepatic glycogen
deposition, peripheral insulin resistance, gluconeogenesis, free fatty acid production Overall diabetogenic effect
Adipose tissue distribution: promotes visceral obesity

ACTION OF GLUCOCORTICOID cont.
Cardiovascular/renal: salt and water retention, hypertension
Skin/muscle/connective tissue: protein catabolism/ collagen breakdown, skin thinning, muscular atrophy
Bone and calcium metabolism: bone formation, bone mass and osteoporosis, linear growth
Immune system: anti-inflammatory action, immuno-suppression

Adrenal Cushing’s syndrome
Cushing’s syndrome is resulting from cortisol excess The commonest cause is iatrogenic (exogenous steroid) ACTH- dependent and ACTH- independent ACTH- dependent: pituitary dependent (Cushing’s disease)
or ectopic secretion
Causes of Cushing’s syndrome@ Pseudo-Cushing’s syndrome: alcoholism (<1%), severe depression (1%)
@ ACTH-dependent: pituitary adenoma/Cushing’s disease (68%), Ectopic ACTH syndrome (12%), ectopic CRH secretion (<1%)
@ ACTH-independent: adrenal adenoma (10%), adrenal ca (8%), nodular hyperplasia (1%)

Prevalence of Symptoms and Signs of Cushing’s Syndrome and Discriminant Index Compared with Prevalence of Features in Patients with Simple Obesity
Findings (Symptoms) %Discriminan
t Index
Weight gainMenstrual irregularityHirsutismPsychiatric DysfunctionHeadacheMuscle weaknessFracturesLoss of scalp hair
9184826243291913
1.62.8
8.0

Prevalence of Symptoms and Signs of Cushing’s Syndrome and Discriminant Index Compared with Prevalence of Features in Patients with Simple Obesity
Findings (Signs) %Discriminant Index
Obesity Truncal GeneralizedPlethoraMoon faceHypertensionBruisingRed-purple striae
9746559488746256
1.60.83.0
4.410.32.5


Prevalence of Symptoms and Signs of Cushing’s Syndrome and discriminant Index Compared with Prevalence of Features in Patients with Simple Obesity
Findings (Signs) %Discriminant Index
Muscle weaknessAnkle edemaPigmentationHypertensionDiabetes Overt IGTOsteoporosis
5650 47450133750

ADRENAL INSUFFICIENCY
Inadequate adrenocortical function Destruction of adrenal cortex (primary or
Addison’s disease), or due to disordered pituitary and hypothalamic function (secondary)
The incidence of Addison’s disease 40-60/million adults
Secondary adrenal insufficiency is most commonly due to suppression of pituitary-hypothalamic function by exogenous glucocorticoid administration

Clinical Features of Primary Adrenal Insufficiency
SymptomWeakness, tiredness, fatigue
(100%)Anorexia (100%)Gastrointestinal symptoms
(92%) Nausea (86%) Vomiting (75%) Constipation (33%) Abdominal pain (31%) Diarrhea (16%)
Salt craving (16%)Postural dizziness (12%)Muscle or joint pains (6–13%)
Sign Weight loss (100%) Hyperpigmentation (94%) Hypotension (<110 mm Hg
systolic) (88–94%)
Vitiligo (10–20%) Auricular calcification (5%)
Laboratory Finding Electrolyte disturbances (92%)
Hyponatremia (88%) Hyperkalemia (64%) Hypercalcemia (6%)
Azotemia (55%) Anemia (40%) Eosinophilia (17%)

Addison’s Disease
Described by Thomas Addison in 1855 The incidence in the developed world of
0.8 cases per 100,000 and prevalence of 4 - 11 cases per 100,000 population
Associated with significant morbidity and mortality; can be easily treated

Essential of D/: Addison’s Disease
Weakness, easy fatigability, anorexia, weight loss; nausea & vomiting, diarrhea; abdominal pain, muscle & joint pains; amenorrhea
Sparse axillary hair; increased pigmentation of skin, esp. of creases, pressure area, and nipples
Hypotension, small heart Low sodium (Na), elevated K, Ca, and BUN;
neutropenia, mild anemia, relative lymphocytosis Low plasma cortisol, elevated ACTH

Therapy of Addison’s disease General measures
Treat all infections if occurred Increases the dose of hydrocortisone
appropriately Maximal dose of hydrocortisone for severe
stress is 50 mg IV or IM every 6 hours Advice patients to wear a medical alert
bracelet or medal reading “Adrenal insufficiency—takes hydrocortisone”

Therapy of Addison’s diseaseSpecific
Hydrocortisone – 15-25 mg/d Prednisone 2-3 mg/morning; 1-2 mg/early
evening Fludrocortisone acetate, has a potent Na-
retaining effect; 0.05-0.3 mg/d Dehydroepiandrosterone (DHEA) 50 mg/d
for some women improvement of the sense of well being, mood, and sexuality

Adrenal Crisis Dehydration, hypotension, or shock out of
proportion to current illness severity Nausea and vomiting with a history of
weight loss and anorexia Abdominal pain so-called acute abdomen Unexplained hypoglycemia Unexplained fever

Adrenal Crisis Hyponatremia, hyperkalemia, azotemia,
hypercalcemia, or eosinophilia Hyperpigmentation or vitiligo Other autoimmune endocrine deficiencies,
such as gonadal failure or hypothyroidism If suspected: give hydrocortisone 100-300
mg I.V.; refer to hospital

INTRODUCTION
The adrenal medulla is a part of the sympathetic nervous system that secretes catecholamines
The sympathetic nervous system secretes norepinephrine as a local neurotransmitter directly in target organ
The adrenal medulla secretes epinephrine and other substances into the general circulation for widespread distribution and effect
It’s importance is to maintain the body’s homeostasis during stress

HISTORY
Early 19th century adrenal medulla was distinguished from adrenal cortex
1886 pheochromocytomas were described by Frankel
1896 Manasse: chromaffin tumors 1901 J. Takamine: adrenalin T.B. Aldrich:
epinephrine 1926 successful surgery of pheochromocytoma
by C.H. Mayo and Roux

CATECHOLAMINES
Include: dopamine, nor-epinephrine, epinephrine Epinephrine is synthesized mainly in adrenal
medulla Nor-epinephrine is found in adrenal medulla,
central nervous system, peripheral sympathetic nerves
Dopamine: precursor of nor-epinephrine Catestatin inhibits catecholamine release

SYNTHESIS OF CATECHOLAMINES
TYROSINE L-dihydroxyphenylalanine (L-dopa)
Tyrosine hydroxylase
Dopamine
Dopamine-ß-hydroxylaseDopa decarboxylase
norepinephrine
Epinephrine PNMT
PNMT 4-phenylethanolamine-N-methyl transferase
In adrenal medulla: 80% epinephrine, 20% norepinephrine

Catecholamines are stored in granules Secretion is increased by exercise, angina
pectoris, myocardial infarction, hemorrhage, ether anesthesia, surgery, hypoglycemia, anoxia, and asphyxia
When released into circulation, catecholamines are bound to albumin
They are quickly metabolized into inactive compounds metanephrine, vanillylmandelic acid (VMA), and conjugated catecholamines

ADRENERGIC RESPONSES OF SELECTED TISSUES
Organ or tissue Receptor Effect
Heart (myocardium)Blood vessels
KidneyGutPancreas
LiverAdipose tissueMost tissuesSkin (apocrine glands)BronchiolesUterus
ß1Αß2ßΑ,ßΑßΑ,ßßßΑß2Αß2
Force and rate of contractionVasocontrctionVasodilation Renin released Motility and sphincter toneInsulin and glucagon releaseInsulin and glucagon release Glycogenolysis Lipolysis Calorigenesis SweatingDilationContractionRelaxation

ADRENAL MEDULLARY HYPOFUNCTION
Hypofunction of adrenal medulla alone: adrenocortical steroid replacement therapy following adrenalectomy.
Autonomic insufficiency (deficiency of adrenal medullary epinephrine secretion: minor defects in recovery from insulin-induced hypoglycemia

ADRENAL MEDULLARY HYPERFUNCTION
Catecholamines can increase blood pressure by increasing cardiac output, by increasing peripheral resistance, and by increasing renin release.
The adrenal medulla is not known to play a significant role in essential hypertension

PHEOCHROMOCYTOMA
Rare tumors, 2 patients per million people yearly or 0.1% of hypertensive population
Pheochromocytomas are usually derived from the adrenal medulla but may develop from chromaffin cells in or about sympathetic ganglia (extraadrenal or paragangliomas)
>1/3 of pheochromocytomas cause death prior to diagnosis. Cause of death: myocardial infarction, cerebrovascular accident, arrhythmias, irreversible shock, renal failure, dissecting aortic aneurysm
15% of pheochromocytoma are malignant

PATIENTS TO BE SCREENED FOR PHEOCHROMOCYTOMA
Young with hypertension Hypertensive patients with: symptoms of
pheochromocytoma, weight loss, seizures, orthostatic hypotension, unexplained shock, family history of pheochromocytoma or medullary carcinoma of thyroid, neurofibromatosis and other neurocutaneus syndromes, mucosal neuromas, hyperglycemia, cardiomyopathy
Marked lability of blood pressure Shock or severe pressor responses with: induction of
anesthesia, parturition, surgery, invasive procedures, antihypertensive drugs
Radiologic evidence of adrenal mass

COMMON SYMPTOMS IN PATIENTS WITH HYPERTENSION DUE TO PHEOCHROMOCYTOMA
Symptoms during or following paroxysms: headache (80%), sweating (70%), forceful heartbeat with or without tachycardia (60%), anxiety (50%) or fear of impending death, tremor (40%), fatigue or exhaustion, nausea and vomiting, abdominal or chest pain, visual disturbance
Symptoms between paroxysms: increased sweating, cold hands and feet, weight loss, constipation
Fatal paroxysms may be induced by opiates, histamine, glucagon

HYPERTENSION IN PHEOCHROMOCYTOMA
Hypertension (90%), paroxysms of severe hypertension (50%), orthostatic changes in blood pressure, it may drop even to hypotension levels after arising from supine position standing for 3 minutes (especially when accompanied by a rise in heart rate)
Epinephrine secretion may cause episodic hypotension and even syncope

DIAGNOSIS
Urinary test of metanephrine or catecholamine Analysis of a full 24-h urine sample is
preferable, (where possible) the collection should be made on rest no medication no recent exposure to radiographic contrast media, urine should be acidified
Normal upper limit of catecholamine 590-885 mmol (100-150 ug)/24 h
Normal upper limit of metanephrine 7 ummol (1.3 mg)/24 h

TREATMENT
Surgery Preoperative management: blockade of alpha
receptor by phenoxybenzamine. Initial dose 10 mg/12 h added by 10-20 mg every few days until blood pressure is controlled and paroxysms disappear. Patient should be monitored of supine and upright blood pressures

PROGNOSIS
After surgery: 5-year survival rate >95% with recurrence <10%
Malignant pheochromocytoma: 5-year survival rate <50%