ADHD Therapeutics to 2020 - MarketResearch.com: Market ... · ADHD Therapeutics to 2020 ... The...
27
ADHD Therapeutics to 2020 Broadened Diagnostic Criteria and Growing Adult Prevalence to Drive Market Growth despite Patent Expirations
Transcript of ADHD Therapeutics to 2020 - MarketResearch.com: Market ... · ADHD Therapeutics to 2020 ... The...

ADHD Therapeutics to 2020 Broadened Diagnostic Criteria and Growing Adult Prevalence to Drive Market Growth despite Patent Expirations

GBI Research Report Guidance
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 2
GBI Research Report Guidance
Chapter two provides an introduction to ADHD, detailing the symptoms, epidemiology, etiology, pathophysiology and diagnostic rating scales utilized in diagnosis. A detailed analysis of current treatment algorithms and options is also included, alongside safety and efficacy data for all treatments approved in the first, second and third lines
Chapter three offers detailed analysis of the products currently marketed for ADHD, detailing their key characteristics, including safety and efficacy, clinical trial outcomes, tolerability, dosing, administration, pricing, and overall competitive strength. These products are also compared in a comprehensive heat map.
Chapter four provides detailed analysis of the pipeline for ADHD by stage of development, molecule type, program type, mechanism of action and molecular target. It also analyses recent clinical trials in this indication by enrollment, duration and failure rate, and provides a primary endpoint analysis of ADHD clinical trials. Promising late‐stage pipeline molecules are also analyzed and assessed in terms of their potential competitive strength.
Chapter five contains market forecasts for the ADHD market, covering epidemiology, treatment usage patterns, pricing and market size for the 2013–2020 forecast period. Eight major markets – the US, Canada, Germany, the UK, France, Italy, Spain and Japan – are covered, and data are presented on a country‐by‐country level, with further analysis of key market drivers and barriers.
Chapter six describes the major deals that have taken place in the global ADHD market in recent years. This coverage analyzes licensing and co‐development agreements, segmented by stage of development, year, molecule type, mechanism of action, and value. Network graphs for these deals are also included, organized by the location of company headquarters.

© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014
Page 3
Executive Summary
Executive Summary
New Market Entrants and Rising Prevalence Help Maintain Moderate Growth
The Attention‐Deficit Hyperactivity Disorder (ADHD) therapeutics market in the eight major markets – the US, the UK, France, Germany, Spain, Italy, Japan and Canada – was worth $XX billion in 2013, and is expected to grow at a Compound Annual Growth Rate (CAGR) of XX% to $XX billion by 2020. The US constituted the largest market in 2013, valued at $XX billion, equivalent to a global share of XX%, followed by the UK with $XXm and Japan with $XXm. Despite having one of the smallest market sizes, second to only Italy, Spain is expected to witness rapid growth over the forecast period, with a CAGR of XX%. This will only be surpassed by Japan, which is expected to witness growth at a CAGR of XX%.
Broadening of Diagnostic Criteria to Drive ADHD Market
Despite the generic entry of previous blockbuster drugs, novel non‐stimulant therapies, notably Sofinicline, Edivoxetine and Metadoxine Extended Release (ER) will prevent significant reductions in the average annual cost of therapy and provide further non‐stimulant therapies in markets still reluctant to fully utilize stimulant therapeutics. Furthermore, the only prodrug marketed for the treatment of ADHD, Vyvanse, is expected to dominate the ADHD market.
The DSM‐V was published in 2013 and broadened the diagnostic criteria for ADHD. The changes included alterations in the symptom threshold for adolescents and adults, requiring only five symptoms in either the inattentive or hyperactive‐impulsive domain instead of six. The number of hyperactive‐impulsive symptoms required remains the same; however, the list includes more specific descriptions of behavior, some of which are more applicable to adults than to children. Autism spectrum disorder is no longer listed as an exclusion criterion and the age of onset has been broadened to include ‘noticeable inattentive or hyperactive‐impulsive symptoms by the age of 12 years’, however, clear evidence of impairment is no longer required.
These changes recognize that impairment from symptoms of ADHD may develop in later life and in some cases cannot be clearly identified until the early adolescent years. The broader diagnostic criteria and reduction in symptom threshold for adults, compared to children, recognizes the age‐dependent changes in the course of the disorder. This better reflects the characteristics and natural course of the disorder, as the lower threshold in adults is still clinically significant where there is clear evidence of impairment from the symptoms of ADHD. These changes herald the final acceptance of adult ADHD in a clinical setting and mean many people who met the ‘partial remission’ criteria will now meet full criteria for ADHD, leading to an increase in diagnosis.
The adult ADHD segment has the potential to be the largest and fastest‐growing segment within the ADHD indication, as XX% of US adults are believed to suffer with adult ADHD, of which XX% are classed as severe (NIMH, 2005). This will be a significant driver of ADHD over the forecast period, as those previously unable to obtain an ADHD diagnosis will now be eligible for treatment.
Impact of Patent Expiration Unlikely to be Diminished by New Market Entrants
Despite the anticipated approval of up to eight drugs during the forecast period, it is not expected to be significant enough to diminish the impact of generic erosion. Generic alternatives are already available for previous blockbuster drugs Concerta and Ritalin LA with further patent expiration expected for Strattera, Daytrana, Intuniv and Kapvay resulting in further generic completion over the forecast period. As new market entrants will be competing against cheaper generic products, they are not expected to demand a premium price. An example is SPN‐812 which is being developed by Supernus. It will face strong competition from generic alternatives to Strattera, Kapvay and Intuniv if approved.

© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014
Page 4
Table of Contents
1 Table of Contents
1 Table of Contents ........................................................................................................................................ 4 1.1 List of Tables .................................................................................................................................... 6 1.2 List of Figures ................................................................................................................................... 6
2 Introduction ................................................................................................................................................ 8 2.1 Disease Introduction ....................................................................................................................... 8 2.2 Symptoms ........................................................................................................................................ 9 2.3 Epidemiology ................................................................................................................................... 9 2.4 Etiology .......................................................................................................................................... 10 2.5 Pathophysiology ............................................................................................................................ 11
2.5.1 Diagnosis Rating Scales ......................................................................................................... 14 2.5.2 DSM‐5 Criteria for ADHD ....................................................................................................... 15 2.5.3 ICD‐10 Criteria for Hyperkinetic Disorder .............................................................................. 17
2.6 Treatment ...................................................................................................................................... 18 2.6.1 Treatment Algorithm ............................................................................................................. 19
3 Marketed Products ................................................................................................................................... 20 3.1 Stimulant Drugs ............................................................................................................................. 21
3.1.1 Adderall XR – Shire ................................................................................................................ 21 3.1.2 Concerta – Janssen Pharmaceuticals ..................................................................................... 22 3.1.3 Daytrana – Noven Pharmaceuticals ...................................................................................... 23 3.1.4 Focalin XR – Novartis ............................................................................................................. 25 3.1.5 Ritalin LA – Novartis .............................................................................................................. 26 3.1.6 Provigil – Teva Pharmaceutical ............................................................................................. 26 3.1.7 Quillivant XR– Pfizer Pharmaceuticals ................................................................................... 27 3.1.8 Vyvanse – Shire ..................................................................................................................... 28
3.2 Non‐stimulant Drugs ..................................................................................................................... 29 3.2.1 Strattera – Eli Lilly ................................................................................................................. 29 3.2.2 Intuniv – Shire ........................................................................................................................ 30 3.2.3 Kapvay – Concordia Pharmaceuticals ................................................................................... 31
3.3 Comparative Efficacy and Safety ................................................................................................... 32 4 ADHD Pipeline ........................................................................................................................................... 34
4.1 Overview ....................................................................................................................................... 34 4.2 Mechanisms of Action in the Pipeline ........................................................................................... 36 4.3 Clinical Trials .................................................................................................................................. 39
4.3.1 Attrition Rate ......................................................................................................................... 39 4.3.2 Clinical Trial Duration ............................................................................................................ 41 4.3.3 Clinical Trial Size .................................................................................................................... 43 4.3.4 Comparative Clinical Trial Metrics Analysis ........................................................................... 46 4.3.5 SHP465 – Shire ...................................................................................................................... 47 4.3.6 NT‐0202 – Neos Therapeutics ............................................................................................... 47 4.3.7 Edivoxetine – Eli Lilly ............................................................................................................. 48 4.3.8 NWP09 – Pfizer ...................................................................................................................... 49 4.3.9 NT‐0102 – Neos Therapeutics ............................................................................................... 50 4.3.10 Metadoxine ER – Alcobra ...................................................................................................... 50 4.3.11 SPN‐812 – Supernus Pharmaceuticals ................................................................................... 51 4.3.12 Dextroamphetamine Transdermal – Noven Pharmaceuticals ............................................... 52
4.4 Comparative Efficacy and Safety ................................................................................................... 53 5 Market Forecast to 2020 ........................................................................................................................... 56
5.1 Global Market ................................................................................................................................ 57 5.2 North America ............................................................................................................................... 60
5.2.1 Treatment Usage Patterns .................................................................................................... 60

© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014
Page 5
Table of Contents
5.2.2 Annual Cost of Treatment ..................................................................................................... 61 5.2.3 Market Size ............................................................................................................................ 62
5.3 Leading Five EU Countries (EU5) ................................................................................................... 63 5.3.1 Treatment Usage Patterns .................................................................................................... 63 5.3.2 Annual Cost of Treatment ..................................................................................................... 64 5.3.3 Market Size ............................................................................................................................ 65
5.4 Japan ............................................................................................................................................. 66 5.4.1 Treatment Usage Patterns .................................................................................................... 66 5.4.2 Annual Cost of Treatment ..................................................................................................... 66 5.4.3 Market Size ............................................................................................................................ 66
5.5 Drivers and Barriers ....................................................................................................................... 68 5.5.1 Drivers ................................................................................................................................... 68 5.5.2 Barriers .................................................................................................................................. 69
6 Deals and Strategic Consolidations ........................................................................................................... 70 6.1 Overview ....................................................................................................................................... 70 6.2 Co‐development Deals .................................................................................................................. 72
7 Appendix ................................................................................................................................................... 75 7.1 Market Definition .......................................................................................................................... 79 7.2 Abbreviations ................................................................................................................................ 79 7.3 References ..................................................................................................................................... 80 7.4 Research Methodology ................................................................................................................. 86
7.4.1 Secondary Research .............................................................................................................. 87 7.4.2 Marketed Product Profiles ..................................................................................................... 87 7.4.3 Late‐Stage Pipeline Candidates ............................................................................................. 87 7.4.4 Comparative Efficacy and Safety Heat Map for Marketed and Pipeline Products ................ 87 7.4.5 Product Competitiveness Framework .................................................................................... 88 7.4.6 Pipeline Analysis .................................................................................................................... 88 7.4.7 Forecasting Model ................................................................................................................. 89 7.4.8 Deals Data Analysis ............................................................................................................... 90
7.5 Contact Us ..................................................................................................................................... 90 7.6 Disclaimer ...................................................................................................................................... 90

© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014
Page 6
Table of Contents
1.1 List of Tables
Table 1: Common Assessment Scales Used to Aid ADHD Diagnosis .......................................................... 14 Table 2: DSM‐5 Criteria for Attention Deficit Hyperactivity Disorder ........................................................ 15 Table 3: ICD‐10 Criteria for Attention Deficit Hyperactivity Disorder ........................................................ 17 Table 4: ADHD Therapeutics Market, Global, Pipeline, Discovery, 2014 ................................................... 75 Table 5: ADHD Therapeutics Market, Global, Pipeline, Preclinical, 2014 ................................................... 75 Table 6: ADHD Therapeutics Market, Global, Pipeline, Phase I, 2014 ........................................................ 75 Table 7: ADHD Therapeutics Market, Global, Pipeline, Phase II, 2014 ....................................................... 76 Table 8: ADHD Therapeutics Market, Global, Pipeline, Phase III, 2014 ...................................................... 76 Table 9: ADHD Theapeutics Market, Global, Pipeline, Pre‐Registration, 2014 .......................................... 76 Table 10: ADHD Therapeutics Market, Global, Market Forecast, 2013‐2020 .............................................. 77 Table 11: ADHD Therapeutics Market, US, Market Forecast, 2013‐2020 .................................................... 77 Table 12: ADHD Therapeutics Market, Canada, Market Forecast, 2013‐2020 ............................................. 78 Table 13: ADHD Therapeutics Market, UK, Market Forecast, 2013‐2020 .................................................... 78 Table 14: ADHD Therapeutics Market, France, Market Forecast, 2013‐2020 .............................................. 78 Table 15: ADHD Therapeutics Market, Germany, Market Forecast, 2013‐2020 .......................................... 78 Table 16: ADHD Therapeutics Market, Italy, Market Forecast, 2013‐2020 .................................................. 79 Table 17: ADHD Therapeutics Market, Spain, Market Forecast, 2013‐2020 ................................................ 79 Table 18: ADHD Therapeutics Market, Japan, Market Forecast, 2013‐2020 ............................................... 79
1.2 List of Figures
Figure 1: ADHD Treatment Algorithm .......................................................................................................... 19 Figure 2: ADHD Therapeutics Market, Marketed Products, Heat Map, 2013 ............................................... 33 Figure 3: ADHD Therapeutics Market, Global, Pipeline (%), 2013 ................................................................ 35 Figure 4: ADHD Therapeutics Market, Global, Pipeline Distribution by Mechanism of Action and Program
Type, 2013 ..................................................................................................................................... 36 Figure 5: ADHD Therapeutics Market, Global, Pipeline Distribution by Mechanism of Action (Tier 1) and
Stage of Development, 2013 ......................................................................................................... 37 Figure 6: ADHD Therapeutics Market, Global, Pipeline Distribution by Mechanism of Action (Tier 2) and
Stage of Development, 2013 ......................................................................................................... 38 Figure 7: ADHD Therapeutics Market, Global, Pipeline, Attrition Rate (%), 2013 ........................................ 40 Figure 8: ADHD Therapeutics Market, Global, Attrition Rate by Mechanism of Action (%), 2013 ............... 41 Figure 9: ADHD Therapeutics Market, Global, Pipeline, Clinical Trial Duration (months), 2013 .................. 42 Figure 10: ADHD Therapeutics Market, Global, Pipeline, Clinical Trial Duration by Mechanism (months),
2013 ............................................................................................................................................... 43 Figure 11: ADHD Therapeutics Market, Global, Pipeline, Clinical Trial Size, 2013 .......................................... 44 Figure 12: ADHD Therapeutics Market, Global, Pipeline, Clinical Trial Size per Product by Mechanism of
Action, 2013 ................................................................................................................................... 45 Figure 13: ADHD Therapeutics Market, Global, Pipeline, Size by Clinical Trial by Mechanism of Action, 2013
....................................................................................................................................................... 46 Figure 14: ADHD Therapeutics Market, Global, Pipeline, Mechanism of Action Heat Map, 2013 ................. 47 Figure 15: ADHD Therapeutics Market, Global, Sales Forecast for Edivoxetine ($m), 2016–2020 ................. 49 Figure 16: ADHD Therapeutics Market, Global, Sales Forecast for Metadoxine ER ($m), 2017–2020 ........... 51 Figure 17: ADHD Therapeutics Market, Global, Sales Forecast for SPN‐812 ($m), 2019–2020 ...................... 52 Figure 18: ADHD Therapeutics Market, Promising Pipeline Molecules, Heat Map ........................................ 54 Figure 19: ADHD Therapeutics Market, Marketed Products, Heat Map, 2013 ............................................... 55 Figure 20: ADHD Therapeutics Market, Global, Treatment Patterns (million), 2013–2020 ........................... 57 Figure 21: ADHD Therapeutics Market, Global, Market Size ($bn), 2013–2020 ............................................. 58 Figure 22: ADHD Therapeutics Market, Global, 2013–2020 ........................................................................... 59 Figure 23: ADHD Therapeutics Market, North America, Treatment Patterns, 2013–2020 ............................ 60 Figure 24: ADHD Therapeutics Market, North America, Annual Cost of Treatment ($), 2013–2020 ............. 61 Figure 25: ADHD Therapeutics Market, North America, Market Size ($m), 2013–2020 ................................ 62 Figure 26: ADHD Therapeutics Market, Top Five EU Countries, Treatment Patterns, 2013–2020 ................. 63 Figure 27: ADHD Therapeutics Market, Top Five EU Countries, Annual Cost of Treatment ($), 2013–2020 .. 64 Figure 28: ADHD Therapeutics Market, Top Five EU Countries, Market Size ($m), 2013–2020 ..................... 65 Figure 29: ADHD Therapeutics Market, Japan, 2013–2020 ............................................................................ 67

© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014
Page 7
Table of Contents
Figure 30: ADHD Therapeutics Market, Global, Major Licensing Deals by Year and Value, 2006–2014 ........ 70 Figure 31: ADHD Therapeutics Market, Global, Major Licensing Deals, 2006–2014 ...................................... 71 Figure 32: ADHD Therapeutics Market, Global, Major Co‐developments Distribution, 2006–2014 .............. 72 Figure 33: ADHD Therapeutics Market, Global, Major Co‐developments by Year and Phase, 2006–2014 .... 73

© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014
Page 8
Introduction
2 Introduction
Attention Deficit/Hyperactivity Disorder (ADHD) is a psychiatric disorder of the neurodevelopment type and the most commonly diagnosed in children and adolescents, with an estimated global prevalence of XX% (Polanczyl et al., 2007). It is defined as a clinical syndrome exhibited by the presence of hyperactivity, impulsivity and inattention. Once thought to be solely a childhood disorder, it is now well documented that ADHD causes significant impairment for many adults. Its symptoms and broad impact mean that it affects children, adults and the wider society both economically and socially. Although the underlying cause is not known, both genetic and environmental factors contribute to the disorder and, as a result, there is no biological test for ADHD. However, the FDA approved the first brain‐wave test in 2013, to aid diagnosis when used as part of a complete medical and psychological examination (Lia et al., 2013). The lack of a definitive biomarker, along with comorbidities, makes diagnosis difficult and sporadic, leading to some patients being undiagnosed. The recent publication of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM‐5) aims to tackle these issues by allowing adolescents and adults to be diagnosed without a prior diagnosis in childhood. This is expected to significantly increase the number of diagnosed and medicated individuals over the forecast period (2013–2020), as XX% of US adults are believed to have ADHD, XX% of which are classified as severe cases (Kessler et al., 2005). Furthermore, recent advancements in neuroimaging have identified potential new pathways in the cause of ADHD, such as the neuronal nicotinic pathway, which is reflected by pipeline drugs targeting proteins in these pathways.
Since the first approval of methylphenidate in 1955, psychostimulant therapeutics have remained the cornerstone of ADHD therapy despite requiring multiple daily doses, having a poor safety profile and possessing significant potential for abuse. However, over the last decade, the ADHD market has shifted towards novel extended‐release delivery methods and non‐stimulant alternatives in an attempt to improve patient adherence and provide a therapeutic option for those who do not respond to stimulant medications. As a result, the ADHD market is now extremely competitive, with an abundance of generic immediate‐release stimulant drugs and branded extended‐release therapeutics, that offer effective symptom relief with moderate tolerability.
Despite the availability of effective once‐daily treatments, unmet need remains in the ADHD market. Although existing treatments are effective in suppressing symptoms, none has an attractive safety profile. Furthermore, most psychostimulants are Schedule II controlled substances and the current non‐stimulant alternatives are not as effective at alleviating symptoms.
It is promising that some of this unmet need is being addressed in the pipeline. The majority of the promising pipeline molecules are non‐stimulant drugs, three of which employ novel mechanisms of action in an attempt to improve efficacy. If their effectiveness can be established in future trials, they are expected to displace current non‐stimulants Intuniv and Kapvay as they both display the poorest efficacy profiles. Furthermore, given highly efficacious results, it is possible that they could compete with first‐line stimulants late in the forecast period. These pipeline drugs will further broaden the range of treatment options available, and when coupled with the rising prevalence and diagnosis of ADHD, will continue to drive the ADHD market.
2.1 Disease Introduction
ADHD is a highly prevalent, clinically heterogeneous disorder that represents an enormous burden on society in terms of financial cost, stress to families, and adverse academic and vocational outcomes (Biederman et al., 2004). It is a multifactorial disorder with complex etiology and strong genetic underpinnings (Faraone et al., 2005).
There are three sub‐types of ADHD as defined by the DSM‐5: predominantly inattentive (ADHD‐PI), hyperactive impulsive (ADHD‐H) and combined (ADHD‐C). ADHD‐C is the most common form and accounts for XX–XX% of cases, whereas ADHD‐H and ADHD‐PI account for XX–XX% and XX–XX% respectively.
The inattention component of ADHD is manifested as distractibility, daydreaming, and difficulty focusing on a single task for a prolonged period, whereas the hyperactivity component is expressed as excessive talking, fidgeting, and restlessness. The symptoms of ADHD predispose patients to accidents, create strain in interpersonal relationships, and disrupt the environment through interruptions and inappropriate behavior. It is notable that the more overt symptoms of hyperactivity/impulsivity tend to wane early in life, whereas the more covert symptom of inattention tends to persist over time (Biederman et al., 1996).

ADHD Pipeline
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 34
4 ADHD Pipeline
4.1 Overview
Although behavioral therapies are used as a frontline treatment, pharmacotherapy remains the cornerstone of ADHD management. Stimulants are the most widely used medications for the treatment of ADHD. These drugs have a paradoxical effect on patients, calming them and improving both the cognitive and non‐cognitive domains of the disorder (Swanson et al., 2011).
The understanding of the MoA of stimulant medications is undergoing constant revision, however the PFC is known to be of central relevance to the neuronal pathways implicated in ADHD, as the PFC has extensive connections to sensory and motor cortices, as well as to the cerebellum and basal ganglia. Catecholamines have an inverted U influence on PFC function, whereby either too little or too much DA or NE impairs PFC cognitive abilities. Since the PFC is essential for attention regulation, poor concentration and distractibility are common symptoms of weakened PFC function (Arnsten, 1998). Stimulants such as methylphenidate (which blocks the DAT) increase the levels of catecholamines in the PCF to alleviate symptoms. However, the increase of extraneuronal catecholamines leads to the possibility of substance abuse, and as a result, most stimulants are classified as Schedule II controlled substances.

ADHD Pipeline
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 35
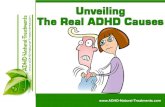
Figure 3: ADHD Therapeutics Market, Global, Pipeline (%), 2013
Dis
cove
ry
Pre
clin
ical
Pha
se I
Pha
se II
Pha
se II
I
Unk
now
n
Pre
-re
gist
ratio
n
Num
ber o
f pro
duct
s
D) Pipeline by Program Type and Stage of Development
Repositioned
Generic
Novel
Discovery
PreclinicalPhase I
Phase II
Phase III
Unknown
A) Pipeline by Stage of Development
Total: X X
Small molecule
Undisclosed
B) Pipeline by Molecule Type
Total: X X
Generic
Novel
Repositioned
C) Pipeline by Program Type
Total: X X
Source: GBI Research Proprietary Pipeline Product Database
As shown in Figure 3.A, the distribution by Phase is particularly unbalanced, with discovery, Preclinical and Phase I accounting for a combined XX% of the pipeline, which is small in comparison to most indications. A brimming Preclinical and Phase I pipeline is essential to sustain progressive growth and development for a market. Over the last decade, CNS has increasingly been regarded as a challenging and increasingly unattractive therapy area due to complex physiology, a lack of validated therapeutic targets and poor product performance. Given the poor understanding of ADHD pathophysiology, it is no surprise that R&D activity is unhealthily distributed.

ADHD Pipeline
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 38
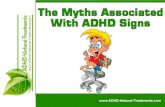
Studies of these signaling interactions have demonstrated that the NMDA receptor is crucial in activating dopamine neurons in the Ventral Tegmental Area (VTA) and Substantia Nigra (SN). Furthermore, dopamine D2 receptor stimulation is involved in the downstream inhibition of the NDMA receptor, which weakens the excitatory response to those neurons (Kotecha et al., 2002). Activation of dopamine D4 receptors also reduces AMPA receptor‐mediated synaptic transmission in the PFC, which in turn causes a decrease of AMPA receptors at the synapse (Warton et al., 2002). These findings have indicated that the dopamine and glutamate systems work in tandem to create a balance of neurotransmitters in these regions, and the targeting of this system may be of interest in ADHD (Yuen et al., 2010). The interest in this system is highlighted Figure 5 and Figure 6, particularly in the early Phases of development.
Figure 6: ADHD Therapeutics Market, Global, Pipeline Distribution by Mechanism of Action (Tier 2) and Stage of Development, 2013
DRI
nAChRNDMA agonist
NDRI
A) Pre-clinical by MoA
Total: X X
Adrenergic receptor agonist AMPA
receptor agonist
NDRI
NRI
Serotonin receptor agonist
SNDRI
B) Phase I by MoA
Total: X X
Adrenergic receptor agonist
Dopamine receptor agonist
DRI
NDMA agonist NDRI
NRI
Serotonin receptor agonist
SNDRISSRI
C) Phase II by MoA
Total: X X
DRI
NDRI
NRI
Serotonin receptor agonist
SNDRI
D) Phase III by MoA
Total: X X
Source: GBI Research Proprietary Database, Products, Pipeline Products
DRI: Dopamine Re‐uptake Inhibitor; NDRI: Norepinephrine, Dopamine Re‐uptake Inhibitor; nAChR: Nicotinic Acetylcholine Receptor; SNDRI: Serotonin, Norepinephrine, Dopamine Re‐uptake Inhibitor; SSRI: Selective Serotonin Re‐uptake Inhibitor
Recent evidence has also shown that cholinergic dysregulation, particularly involving neuronal Nicotinic Acetylcholine Receptors (nAChR), may play a role in the pathophysiology of ADHD. Nicotine has demonstrated pro‐cognitive effects in humans and has positive efficacy results in small proof‐of‐concept adult ADHD trials. The pharmacological enhancement of the cholinergic system in the PFC can improve a host of cognitive processes and recent studies have identified cognitive improvements associated with nicotine administration in human non‐ADHD subjects (Levin et al., 2006).

ADHD Pipeline
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 41
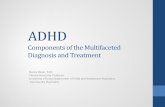
Interestingly, in Phase I novel ADHD targets (glutamatergic and cholinergic) show the lowest attrition rates, as shown in Figure 8.B. In contrast, monoaminergic agonists demonstrate the highest attrition rate at XX% compared to MRIs at XX%, even though these are well established. In Phase II and Phase III, the results are as expected, with innovative targets displaying the highest attrition rates. There is clearly a greater risk associated with such targets.
The overall attrition rates for MRIs and monoaminergic agonists were XX% and XX%, respectively. Due to a lack of precedence for compounds in Phase III, sample sizes were too small to be meaningful for glutamatergic and cholinergic targets, but it is currently XX% because no therapeutics with these MoAs have entered the ADHD market. The exceptionally low attrition rates for these mechanisms can also be accounted for by the low number of trials for these targets categories and are therefore not as robust. Additionally, many clinical trials were ongoing, and as such were not taken into account in the calculation of attrition rates.
Figure 8: ADHD Therapeutics Market, Global, Attrition Rate by Mechanism of Action (%), 2013
Undisclosed
Cholinergic
MRI
Monoaminergic agonist
Glutamatergic
Failure rate (%)
A) Attrition rate
Undisclosed
Cholinergic
MRI
Monoaminergic agonist
Glutamatergic
Failure rate (%)
B) Phase I
Undisclosed
Cholinergic
MRI
Monoaminergic agonist
Glutamatergic
Failure rate (%)
C) Phase II
Undisclosed
Cholinergic
MRI
Monoaminergic agonist
Glutamatergic
Failure rate (%)
D) Phase III
Source: GBI Research Proprietary Database, Products, Pipeline Products

ADHD Pipeline
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 43
Analysis by MoA revealed some substantial differences in trial duration between different target areas, as shown in Figure 10. Most notably, novel targets are on average markedly shorter than established targets across all Phases. Histaminergic, cholinergic and glutamatergic targets also have a significantly smaller distribution compared to monoaminergic targets. In Phase II, cholinergic and glutamatergic targets had an average duration of XX and XX respectively, notably shorter than the XX and XX for monoaminergic agonists and MRIs. This is interesting given the prevalence of established monoaminergic‐targeting ADHD therapeutics.
Figure 10: ADHD Therapeutics Market, Global, Pipeline, Clinical Trial Duration by Mechanism (months), 2013
Cholinergic Monoaminergic agonist Undisclosed
Ave
rage
clin
ical
tria
l dur
atio
n (m
onth
s)
A) Phase I
Cholinergic Glutamatergic M onoaminergic agonist
MRI Undisclosed
Ave
rage
clin
ical
tria
l dur
atio
n (m
onth
s)
B) Phase II
Glutamatergic M onoaminergic agonist
MRI Undisclosed
Ave
rage
clin
ical
tria
l dur
atio
n (m
onth
s) C) Phase III
Third quartileSecond quartileAverage
Source: GBI Research Proprietary Database, Products, Pipeline Products
MRI: Monoamine Re‐uptake Inhibitor

Market Forecast to 2020
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 60
5.2 North America
5.2.1 Treatment Usage Patterns
According to the Centers for Disease Control and Prevention (CDC), the percentage of children diagnosed with ADHD increased from XX% in 2003 to XX% in 2011. The current estimate of ADHD prevalence in the US is XX million, making the US the nation with the highest prevalence population of ADHD across the eight key developed markets analyzed here. As such, the US represents a major market for ADHD, with further potential growth as the prevalence is expected to rise to XX million by 2020.
The treatment population in the US is high when compared to the other seven major markets, as is the diagnosis population. The reason for this is that ADHD is much more recognized in the US than it is in other key markets. Diagnosis rates are expected to increase with prevalence across the forecast period due to an expansion of DMS‐V diagnostic criteria. However, they suggest underdiagnoses. This is due to the nature of ADHD diagnosis and the fact that there is no specific biological test that can definitively confirm the presence of ADHD; it therefore comes down to the perception of the clinician. Despite the high treatment population in the US compared to other markets, the data suggest there is still a sizable untreated patient population. This can be put down to poor patient compliance with ADHD medications and the reluctance of clinicians to prescribe stimulant therapeutics for young patients.
The current prevalence population in Canada is estimated at XX and is expected to rise to XX across the forecast period as shown in Figure 23.A. Despite utilizing the same diagnostic guidelines as the US, the data in Figure 23.A suggest broad‐scale underdiagnosis.
Figure 23: ADHD Therapeutics Market, North America, Treatment Patterns, 2013–2020
2013 2014 2015 2016 2017 2018 2019 2020
Pat
ient
s ('0
00)
A) US
2013 2014 2015 2016 2017 2018 2019 2020
Patie
nts
('000
)
B) Canada
Prevalence population Diagnosed population Treatment population
Source: GBI Research Proprietary Pipeline Products Database; GBI Research Proprietary Marketed Products Database

Market Forecast to 2020
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 64
5.3.2 Annual Cost of Treatment
The ACoT in the EU5 is set to decrease across all nations however at a lower rate in the UK and Germany, where Vyvanse is expected to have a a moderate impact after entering these markets. The ACoT in Italy and France on the other hand is expected to decrease due to a lack of Vyvanse penetration and increased generic competition.
The UKs ACoT was valued at $XX in 2013, and is expected to decrease to XX by 2020, at a negative CAGR of XX%. However in the peak scenario, in which Vyvanse is expected to have stronger market potential, the ACoT is expected to increase to $XX in 2020, at a CAGR of XX%. This is also the case for Germany which is expected to decrease from $XX in 2013 to $XX in 2020, at a negative CAGR of XX%, or rise to $XX in the peak case scenario at a CAGR of XX%.
Despite the approval of Vyvanse in Spain, the uptake is not expected to be a strong as the UK and Germany and therefore the ACoT is expected to decrease from £XX in 2013, to $XX in 2020, at a negative CAGR of XX%.
Vyvanse is yet to gain approval in Italy and France and these skeptical markets are expected to decrease at negative CAGRs of XX% and XX% respectively.
Figure 27: ADHD Therapeutics Market, Top Five EU Countries, Annual Cost of Treatment ($), 2013–2020
2013 2014 2015 2016 2017 2018 2019 2020
Ann
ual c
ost o
f the
rapy
($)
A) UKProjected CAGR: XX%Peak CAGR: XX%Low CAGR: XX%
2013 2014 2015 2016 2017 2018 2019 2020
Ann
ual c
ost o
f the
rapy
($)
B) France
Projected CAGR: XX%Peak CAGR: XX%Low CAGR: XX%
2013 2014 2015 2016 2017 2018 2019 2020
Ann
ual c
ost o
f the
rapy
($)
C) GermanyProjected CAGR: XX%Peak CAGR: XX%Low CAGR: XX%
2013 2014 2015 2016 2017 2018 2019 2020
Ann
ual c
ost o
f the
rapy
($)
D) Italy
Projected CAGR: XX%Peak CAGR: XX%Low CAGR: XX%
2013 2014 2015 2016 2017 2018 2019 2020
Ann
ual c
ost o
f the
rapy
($)
E) Spain
Low variance
Medium variance
High variance
Projected
Projected CAGR: XX%Peak CAGR: XX%Low CAGR: XX%
Source: GBI Research Proprietary Pipeline Products Database; GBI Research Proprietary Marketed Products Database

Appendix
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 75
7 Appendix
Table 4: ADHD Therapeutics Market, Global, Pipeline, Discovery, 2014
Product Name Company Stage of Development
Source: GBI Research Proprietary Pipeline Products Database
Table 5: ADHD Therapeutics Market, Global, Pipeline, Preclinical, 2014
Product Name Company Stage of Development
Source: GBI Research Proprietary Pipeline Products Database
Table 6: ADHD Therapeutics Market, Global, Pipeline, Phase I, 2014
Product Name Company Stage of Development
Source: GBI Research Proprietary Pipeline Products Database

Appendix
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 76
Table 7: ADHD Therapeutics Market, Global, Pipeline, Phase II, 2014
Product Name Company Stage of Development
Source: GBI Research Proprietary Pipeline Products Database
Table 8: ADHD Therapeutics Market, Global, Pipeline, Phase III, 2014
Product Name Company Stage of Development
Source: GBI Research Proprietary Pipeline Products Database
Table 9: ADHD Theapeutics Market, Global, Pipeline, Pre‐Registration, 2014
Product Name Company Stage of Development
Source: GBI Research Proprietary Pipeline Products Database

Appendix
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 77
Table 10: ADHD Therapeutics Market, Global, Market Forecast, 2013‐2020
2013 2014 2015 2016 2017 2018 2019 2020
Prevalence Population ('000)
Diagnosis Population ('000)
Treatment Population ('000)
Maximum Market Size ($m)
Projected Market Size ($m)
Minimum Market Size ($m)
Predicted Sales of Amphetamine mixed salts ($m)
Predicted Sales of Amphetamine mixed salts ER ($m)
Predicted Sales of Atomoxetine ($m)
Predicted Sales of Dexmethylphenidate ($m)
Predicted Sales of Dexmethylphenidate XR ($m)
Predicted Sales of Dextroamphetamine IR ($m)
Predicted Sales of Dextroamphetamine SR ($m)
Predicted Sales of Lisdexamphetamine ($m)
Predicted Sales of methylphenidate ER ($m)
Predicted Sales of Methylphenidate Transdermal patch ($m)
Predicted Sales of Methylphenidate ER oral suspension ($m)
Predicted Sales of Methylphenidate IR ($m)
Predicted Sales of Methylphenidate ER ($m)
Predicted Sales of Guanfacine hydrochloride ($m)
Predicted Sales of Clonidine hydrochloride ($m)
Predicted Sales of Edivoxetine ($m)
Source: GBI Research
Table 11: ADHD Therapeutics Market, US, Market Forecast, 2013‐2020
2013 2014 2015 2016 2017 2018 2019 2020
Prevalence population (‘000)
Treatment population (‘000)
ACoT ($)
Maximum Market Size ($m)
Projected Market Size ($m)
Minimum Market Size ($m)
Source: GBI Research

Appendix
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 78
Table 12: ADHD Therapeutics Market, Canada, Market Forecast, 2013‐2020
2013 2014 2015 2016 2017 2018 2019 2020
Prevalence Population ('000)
Treatment Population ('000)
ACoT ($)
Maximum Market Size ($m)
Projected Market Size ($m)
Minimum Market Size ($m)
Source: GBI Research
Table 13: ADHD Therapeutics Market, UK, Market Forecast, 2013‐2020
2013 2014 2015 2016 2017 2018 2019 2020
Prevalence population (‘000)
Treatment population (‘000)
ACoT ($)
Maximum Market Size ($m)
Projected Market Size ($m)
Source: GBI Research
Table 14: ADHD Therapeutics Market, France, Market Forecast, 2013‐2020
2013 2014 2015 2016 2017 2018 2019 2020
Prevalence population (‘000)
Treatment population (‘000)
ACoT ($)
Maximum Market Size ($m)
Projected Market Size ($m)
Minimum Market Size ($m)
Source: GBI Research
Table 15: ADHD Therapeutics Market, Germany, Market Forecast, 2013‐2020
2013 2014 2015 2016 2017 2018 2019 2020
Prevalence population (‘000)
Treatment population (‘000)
ACoT ($)
Maximum Market Size ($m)
Projected Market Size ($m)
Minimum Market Size ($m)
Source: GBI Research

Appendix
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 79
Table 16: ADHD Therapeutics Market, Italy, Market Forecast, 2013‐2020
2013 2014 2015 2016 2017 2018 2019 2020
Prevalence population
Treatment population
ACoT ($)
Maximum Market Size ($m)
Projected Market Size ($m)
Minimum Market Size ($m)
Source: GBI Research
Table 17: ADHD Therapeutics Market, Spain, Market Forecast, 2013‐2020
2013 2014 2015 2016 2017 2018 2019 2020
Prevalence population (‘000)
Treatment population (‘000)
ACoT ($)
Maximum Market Size ($m)
Projected Market Size ($m)
Minimum Market Size ($m)
Source: GBI Research
Table 18: ADHD Therapeutics Market, Japan, Market Forecast, 2013‐2020
2013 2014 2015 2016 2017 2018 2019 2020
Prevalence population (‘000)
Treatment population (‘000)
ACoT ($)
Maximum Market Size ($m)
Projected Market Size ($m)
Minimum Market Size ($m)
Source: GBI Research
7.1 Market Definition
The global Attention Deficit Hyperactivity Disorder (ADHD) therapeutics market in the report refers to the top eight national ADHD therapeutics markets: the US, the UK, Germany, France, Spain, Italy, Japan and Canada.
The prevalence population is the estimated number of people at any given time who have ADHD.
7.2 Abbreviations
ADHD: Attention Deficit Hyperactivity Disorder
ADHD‐C: Attention Deficit Hyperactivity Disorder – Combined type
ADHD‐H: Attention Deficit Hyperactivity Disorder – Hyperactive type
ADHD‐PI: Attention Deficit Hyperactivity Disorder – Primarily Inattentive type

Appendix
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 80
ADHD‐RS: Attention Deficit Hyperactivity Disorder Rating Scale
AE: Adverse Event
ANDA: Abbreviated New Drug Application
bpm: beats per minute
CAARS: Conners’ Adult ADHD Rating Score
CAARS‐INV: Conners’ Adult ADHD Rating Score
CADS‐T: Conners’ ADHD Teachers‐total subscale
CBCL: Child Behavior Checklist
CBRS‐SR: Conners’ Self Report
CGI‐I: Clinical Global Impressions ‐ Improvement
CTRS‐R: Conners’ Teacher Rating Scale
D‐AMPH: Dextroamphetamine
DAT: Dopamine Active Transporter
DRS: Dermal Response Score
DT‐MRI: Diffusion‐Tensor Magnetic Resonance Imaging
HA: Histamine
HKD: Hyperkinetic Disorder
HSQ: Home Situations Questionnaire
IR: Immediate Release
LS: Least‐Squares
mmHg: millimeters of mercury
MPH: Methylphenidate
MTS: Methylphenidate Transdermal System
NAT: Norepinephrine Active Transporter
NET: Norepinephrine Transporter
NRI: Norepinephrine Reuptake Inhibitor
OROS: Oral Osmotic Release System
PCB: Polychlorinated Biphenyl
PET: Positron Emission Topography
SNAP‐IV: Swanson, Nolan and Pelham Questionnaire‐IV
SODAS: Spheroidal Oral Drug Absorption System
SPECT: Single Photon Emission Tomography
SSQ: School Situations Questionnaire
WRAADDS: Wender‐Reimherr Adult Attention Deficit Disorder Scale
7.3 References
Adams CP and Brantner VV (2010). Spending on new drug development. Health Econ; 19: 130–141.
Adler LD and Nierenberg AA (2010). Review of medication adherence in children and adults with ADHD. Postgraduate Medicine; 122: 184–191.

Appendix
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 81
Adler LA, et al. (2008). Double‐blind, placebo‐controlled study of the efficacy and safety of lisdexamfetamine dimesylate in adults with attention‐deficit/hyperactivity disorder. The Journal of Clinical Psychiatry; 69 (9): 1,364–1,373.
Adler LA, et al. (2009). Long‐term effectiveness and safety of dexmethylphenidate extended‐release capsules in adult ADHD. Journal of Attention Disorders; 12 (5): 449–459.
Anderson VR and Scott LJ (2006). Methylphenidate transdermal system: In attention‐deficit hyperactivity disorder in children. Drugs; 66 (8): 1,117–1,126.
Arnsten AF (1998). Catecholamine modulation of prefrontal cortical cognitive function: Circuits and pathways. Journal of Clinical Psychiatry; 67:410–422.
Arnsten AF (2006). Fundamentals of attention‐deficit/hyperactivity disorder: Circuits and pathways. Journal of Clinical Psychiatry; 67 (suppl. 8): 7–12.
Arnsten AF, et al. (1996): The contribution of alpha 2‐noradrenergic mechanisms of prefrontal cortical cognitive function: Potential significance for attention‐deficit hyperactivity disorder. Archive of General Psychiatry; 53: 448–455.
Arnsten AF, et al. (1998). The alpha‐2 adrenergic agonist guanfacine improves memory in aged monkeys without sedative or hypotensive side effects: evidence for alpha‐2 receptor subtypes. The Journal of Neuroscience; 8: 4,287–4,298.
Aron R and Poldrack RA (2005). The cognitive neuroscience of response inhibition: relevance for genetic research in attention‐deficit/hyperactivity disorder. Biological Psychiatry; 57: 1,285–1,292.
Ashtari M (2005). Attention‐deficit/hyperactivity disorder: a preliminary diffusion tensor imaging study. Biological Psychiatry; 57: 448–455.
Bain EE, et al. (2013). A Randomized, Double‐Blind, Placebo‐Controlled Phase 2 Study of α4β2 Agonist ABT‐894 in Adults with ADHD. Neuropsychopharmacology; 38: 3,405–3,413.
Ballon JS and Feifel D (2006). A systematic review of modafinil: potential clinical uses and mechanisms of action. Journal of Clinical Psychiatry; 67: 554–566.
Biederman J, et al. (1990). Family‐genetic and psychosocial risk factors in DSM‐III attention deficit disorder. Journal of the American Academy of Child and Adolescent Psychiatry; 29: 526–533.
Biederman J, et al. (1992). Further evidence for family‐genetic risk factors in attention deficit hyperactivity disorder. Patterns of comorbidity in probands and relatives psychiatrically and pediatrically referred samples. JAMA Psychiatry; 728–738.
Biederman J, et al. (1995). High risk for attention deficit hyperactivity disorder among children of parents with childhood onset of the disorder: A pilot study. The American Journal of Psychiatry; 152: 431–435.
Biederman J, et al. (1996). Predictors of persistence and remission of ADHD: Results from a four‐year prospective follow‐up study of ADHD children. J Am Acad Child Adolesc Psychiatry; 35: 343–351.
Biederman J, et al. (2003). Efficacy and safety of Ritalin LA, a new, once daily, extended‐release dosage form of methylphenidate, in children with attention deficit hyperactivity disorder. Paediatr Drugs; 5 (12): 833–841.
Biederman J, et al. (2004). Gender effects of attention deficit hyperactivity disorder in adults, revisited. Biol Psychiatry; 55: 692–700.
Biederman J, et al. (2005). Efficacy and safety of modafinil film‐coated tablets in children and adolescents with attention‐deficit/hyperactivity disorder: results of a randomized, double‐blind, placebo‐controlled, flexible‐dose study. Pediatrics; 116: e777–784.
Biederman J, et al. (2006). A randomized, placebo‐controlled trial of OROS methylphenidate in adults with attention‐deficit/hyperactivity disorder. Biol Psychiatry; 59: 829–35.
Biederman J and Pliszka SR (2008). Modafinil improves symptoms of attention‐deficit/hyperactivity disorder across subtypes in children and adolescents. J Pediatr; 152 (3): 394–399.

Appendix
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 86
Weisler RH, et al. (2006). Mixed amphetamine salts extended‐release in the treatment of adult ADHD: a randomized, controlled trial. CNS Spectr: 8 (11): 625–639.
Weiss M, et al. (2006). Medication satisfaction among adults with ADHD: long term results from the Quality of Life, Effectiveness, Safety, and Tolerability (Qu. S.T.) study. Program and abstracts of the 19th US Psychiatric and Mental Health Congress: New Orleans; Abstract 120.
Weiss M and Weiss JR (2004). A guide to the treatment of adults with ADHD. J Clin Psych; 65 (3): 27–37.
Wigal SB, et al. (2013). NWP06, an Extended‐Release Oral Suspension of Methylphenidate, Improved Attention‐Deficit/Hyperactivity Disorder Symptoms Compared with Placebo in a Laboratory Classroom Study. J Child Adolesc Psychopharmacol; 23 (1): 3–10.
Willcut EG (2012). The prevalence of DSM‐IV attention‐deficit/hyperactivity disorder: a meta‐analytic review. Neurotherapeutics; 9 (3): 490‐9.
Wilens TE, et al. (2006). An open‐label study of the tolerability of mixed amphetamine salts in adults with attention‐deficit/hyperactivity disorder and treated primary essential hypertension. J Clin Psychiatry; 67: 696–702.
Wilens TE (2006). Mechanism of action of agents used in attention‐deficit/hyperactivity disorder. J Clin Psychiatry; 67 (8); 32–7.
Williams JH and Ross L (2007). Consequences of prenatal toxin exposure for mental health in children and adolescents: a systematic review. Eur Child Adolesc Psychiatry; 16: 243–253.
Yuen EY, et al. (2010). Regulation of AMPA receptor channels and synaptic plasticity by cofilin phosphatase Slingshot in cortical neurons. J Physiol; 588 (Pt 13): 2,361–2,371.
Zametkin AJ and Liotta W (1998). The neurobiology of attention‐deficit/hyperactivity disorder. J Clin Psychiatry; 59 (7); S17–S23.
7.4 Research Methodology
GBI Research aims to help clients within the life sciences industries to better understand their business environment, compete successfully within it, and achieve growth.
Our goal is to be the business intelligence partner of choice for companies in the life sciences arena that are looking for meaningful, innovative and evidence‐based analysis to inform their key decision‐making.
Our coverage extends to the major indications across all therapy areas with a particular focus on oncology, CNS and immunology and a weighting towards indications demonstrating significant innovation in early‐stage development. Our complex proprietary data methodologies drive our specialisms in indications with clearly established therapeutic landscapes, significant pipeline activity and a high proportion of approved products with market exclusivity.
Everything we do at GBI Research is rooted in extensive data validation, interrogation and analysis. Our R&A teams are constantly looking for ways to evolve our products in order to provide ever more understanding and transparency around what is really happening in the market.
There are a number of key themes running through all of our product offerings that serve to define our proposition and position in a crowded market:
Data integrity:
GBI Research has full access to comprehensive, market‐leading proprietary databases covering marketed and pipeline products, clinical trials, and licensing and co‐development deals. In addition to the daily database updates made by that specific team, GBI Research validates all data used in research reports, ensuring an exceptionally high degree of data accuracy.
Data are refreshed immediately prior to publication to ensure the final report reflects any changes that took place during the authoring effort.
Innovative and meaningful analytical techniques and frameworks:
GBI Research recognizes the value of highly accurate raw data, but this is simply the platform.

Appendix
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 87
The entire proposition is built around understanding clients’ needs related to business intelligence, and the ambition to develop novel proprietary data interrogation methodologies to extract meaningful and innovative data sets and provide insightful analyses.
Evidence based analysis and insight:
Proprietary data interrogation methodologies are applied to provide visibility over such vital and tangible data parameters as clinical trial attrition rates versus industry averages, clinical trial endpoint design, product competitiveness benchmarking and multi‐scenario forecasting.
7.4.1 Secondary Research
The research process begins with extensive secondary research utilizing proprietary databases and external sources, including qualitative and quantitative information relating to each market.
The secondary research sources that are typically referred to include, but are not limited to:
Company websites, annual reports, financial reports, broker reports, investor presentations and US Securities and Exchanges Commission (SEC) filings
Industry trade journals, scientific journals and other technical literature
Internal and external databases
Relevant patent and regulatory databases
National government documents, statistical databases and market reports
Procedure registries
News articles, press releases and web‐casts specific to the companies operating in the market
7.4.2 Marketed Product Profiles
The marketed products section provides an overview of the market landscape and gives qualitative profiles of the leading marketed therapies. These profiles describe molecule type, mechanism of action, companies involved in development and marketing, overall clinical and commercial strength, and future prospects. Emphasis is placed on analyzing efficacy and safety data in order to comparatively determine the strongest products available for treatment and assess the clinical and commercial positioning in the current market. In addition, our marketed product profiles assess the clinical and commercial threats and opportunities in the context of late‐stage pipeline products in order to provide an evidence‐based outlook and perspective for product performance during the forecast period.
Where available, historical revenue data are also provided.
7.4.3 Late‐Stage Pipeline Candidates
This section consists of qualitative profiles of drugs in the late stages of the developmental pipeline. The focus here is predominantly on Phase III drugs and, depending on clinical and commercial potential, Phase II drugs.
The profiles cover areas including, but not limited to, a drug’s molecule type and mechanism of action, companies involved in its development, performance in clinical trials specifically relating to efficacy and safety endpoints, and overall clinical and commercial potential. Typically, a revenue forecast for the drug candidate in the covered indication is also provided. This includes peak, medium and low‐variance ranges throughout the forecast period, which take into consideration variable factors with a high degree of inherent unpredictability such as marketing approval of pipeline products, clinical uptake and potential competition, drug price inflation rates and many more.
7.4.4 Comparative Efficacy and Safety Heat Map for Marketed and Pipeline Products
The comparative efficacy and safety heat map provides a visual representation of the comparative clinical profile of each marketed product based on available clinical trial data. GBI Research aims to aggregate and integrate all available clinical trial efficacy and safety data, organized by the respective endpoints into heat maps to assist in direct performance benchmarking of each drug.

Appendix
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 88
The heat map uses conditional formatting to color‐code the performance of each marketed drug from strongest to weakest. This is applied to each clinical trial endpoint, allowing us to determine the strongest performer in each endpoint category. A dark blue color indicates the strongest performers in that category, whereas light gray colors indicate weaker performers.
7.4.5 Product Competitiveness Framework
The product competitiveness frameworks translate the clinical trial data in heat maps into performance benchmarks that express the comparative efficacy and safety performance as a ratio. The safety and efficacy data by endpoint are aggregated and compared to the strongest marketed product in each parameter. The baseline, as defined by the strongest marketed product on each endpoint, is defined as 1. The performance of all other marketed and pipeline products is expressed as a comparative ratio in comparison to the strongest performing product on that endpoint. Dark blue values indicate strong performers in that category and lighter gray values indicate weaker performers. This includes qualitative assessment of product features that offer meaningful differentiation from competitor’s products, such as route of administration and dosage/administration frequency. Overall, this type of analysis helps to determine the potential impact of a specific new drug on the market, as well as the future competitive landscape.
7.4.6 Pipeline Analysis
7.4.6.1 Overall Pipeline
This section analyzes proprietary pipeline data and provides a thorough overview of the current pipeline landscape for the indication in question. Using proprietary data analysis techniques, the pipeline is broken down by stage of development, molecule type, mechanism of action and/or molecular target. Each of these categories is subject to further granulation depending on the level of data available and any observed trends or findings. It is broken down by program type to determine the degree of novelty within the pipeline. Each drug development program is defined as being novel, generic or repositioned using methodologies and processes and drawing upon multiple databases, including market and pipeline datasets. Repositioned drugs are defined as those that are already marketed for another indication and that are now in development for the indication being assessed. Novel products are defined as containing active pharmaceutical ingredients that are currently not approved in the market, whereas generic products include approved compounds that are no longer under patent. The accuracy of the data is validated using external sources such as company websites.
Like all sections within the report, the data analysis provides the basis for in‐depth written discussion, which determines the broader implications of the results obtained.
7.4.6.2 Clinical Trials
The clinical trial landscape for each indication is comprehensively profiled using proprietary clinical trial data. The factors assessed include, but are not limited to, clinical trial failure rate, size and duration and endpoint analysis. Each is analyzed by clinical stage of development.
7.4.6.2.1 Failure Rate
Failure rate analysis helps to determine the risk profile associated with drug development for the indication in question. The failure rate is defined as the percentage of products that fail to progress to the next stage of clinical development or reach marketing approval, as is the case for products in Phase III. Inactive development programs are defined as those for which no progress has been made and for which no further updates have been disclosed for over four years.
This analysis is typically subject to further granulation, such as failure rate by Phase, mechanism of action and molecule type, to provide further insight into the risks associated with the development of certain classes of drugs and product technology.
7.4.6.2.2 Clinical Trial Size
Clinical trial size assesses the mean and median subject recruitment size of clinical trials by Phase and compares the respective indications against the wider therapy area or industry benchmarks. This is commonly analyzed further by molecule type and mechanism of action.

Appendix
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 89
7.4.6.2.3 Clinical Trial Duration
Like clinical trial size, clinical trial duration analyzed and disclosed the mean and median duration (in months) of clinical trials by Phase and molecule type/mechanism of action.
7.4.6.2.4 Clinical trial Endpoint Analysis
A clinical trial endpoint is a measure from which a decision can be made to accept or reject the null hypothesis. The primary and secondary endpoints used in clinical trials can be used to provide insight into the patient outcomes driving drug development.
The analysis is designed to extract the primary and secondary outcome measures used across all clinical trials in the indication, whether different safety, efficacy or pharmacokinetic endpoints. These data are then graphically presented to display the most prominent primary and secondary endpoints.
Trends in primary and secondary endpoints are assessed by Phase of development and, when possible, over a specified timeframe to identify any changing patterns in clinical trial design.
7.4.7 Forecasting Model
This GBI Research report covers the following major developed markets: the US; Canada; the top five countries in Europe: the UK, Germany, France, Spain, Italy; and Japan. The total market size for each country is provided, which is the sum value of the market sizes of all the indications for that particular country.
Our forecasting model uses an epidemiology‐based approach, in which sales for each product are calculated based on the cost of the drug, and the number of patients using it.
Initially, based on peer‐reviewed literature, the disease prevalence is calculated and extrapolated with historic trends and any other relevant inputs gathered from the literature. In the same way, the fraction of prevalent patients that is diagnosed and the proportion of diagnosed patients that is ultimately treated are also calculated.
If relevant, the treatment population is then divided into segments using any available inputs from scientific literature. For example, in oncology indications it is common for us to divide the patient population based on the stage of disease. Each drug may appear in more than one segment within this model and, if used as part of a combination of products, revenues are calculated on single product levels across all segments and combinations.
The use of each drug within each segment (as a percentage) is estimated as accurately as possible, primarily using treatment guidelines, primary research and any other relevant peer‐reviewed data inputs for each indication. The market penetration of pipeline products in their first few years after approval is estimated based primarily on published clinical trial data, with the safety and efficacy profiles of each pipeline drug being compared against any other competitors in their patient segment(s).
Pipeline products that are expected to fulfill an unmet need and perform better than marketed products are typically given higher distributions than those that are not. While efficacy and safety data are usually the most important criteria for making these estimates, other characteristics such as the route of administration and dosing convenience are weighted more strongly in relevant indications.
The cost of each drug is estimated based on its cost per gram (cost of one unit divided by the size of each unit in grams) and the number of grams taken by each patient in a single year (or a course of therapy). For the purposes of this model, different formulations for a single drug with different dosages (for example, a pediatric and adult formulation) are treated as separate entities.
For pipeline drugs, the cost is estimated based on a benchmark of existing marketed products (typically within the indication). Based on their ability to fulfill unmet needs and compete effectively with marketed products, a percentage markup (or occasionally a markdown) versus its benchmark is assigned. This benchmark may be an individual product (such as a direct competitor) or an average of existing products.
The cost is adjusted to take into account inflation of pharmaceutical products and any estimated effects of patent expiries (with biologics having a slower and weaker price erosion than small molecules following patent expiry). Finally, based on percentage distributions, a weighted average cost of each drug is estimated for all patients treated for the disease. This can then be multiplied by the treatment population to arrive at a sales estimate for that drug, and the total sales of all drugs is then the overall market size.

Appendix
© GBI Research. This is a licensed product and is not to be photocopied GBIHC337MR / Published JUL 2014Page 90
From this primary forecast, peak and low market sizes and drug sales are estimated based on potential variations and uncertainties in price inflation, patent expiry, distribution shifts, pipeline product market penetration, and drug pricing for pipeline products. Inherently unpredictable events such as policy changes are not modeled directly in the scenarios, but are accounted for in the numeric inputs. These multiple scenarios aim to supplement the primary forecast with an accurate, transparent picture of the inherent uncertainty of the future market, and the likely range of outcomes.
7.4.8 Deals Data Analysis
This section includes analysis of GBI Research proprietary strategic deals data relevant to the indication being assessed. The two major deal types analyzed are co‐development deals and licensing deals.
When analyzing co‐development and licensing deals data, the parameters assessed are often consistent, although there can be some variation depending on data availability. Firstly, deals are analyzed by country, value and year.
Analysis by country includes the use of network charts, which visually represent links between different nations to visualize where companies involved in deals are headquartered and to identify deal hubs.
The deals data are analyzed further to display the number of deals by stage of development, molecule type and mechanism of action. Qualitative analysis of the major deals within the indication is also provided.
7.6 Disclaimer
All Rights Reserved.
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission of the publisher, GBI Research.