Adelaide Minding the Person

of 61
Transcript of Adelaide Minding the Person
-
7/27/2019 Adelaide Minding the Person
1/61
Minding the person the clinicalapplication of mentalisationbased treatment in patients and
families
Prof Anthony W BatemanAAIMH Conference 2008
Adelaide, South Australia
-
7/27/2019 Adelaide Minding the Person
2/61
20062004
-
7/27/2019 Adelaide Minding the Person
3/61
Therapist stance
-
7/27/2019 Adelaide Minding the Person
4/61
Therapist Stance
Not-Knowing
Neither therapist nor patient experiences interactions other thanimpressionistically
Identify difference I can see how you get to that but when I thinkabout it it occurs to me that he may have been pre-occupied withsomething rather than ignoring you.
Acceptance of different perspectives Active questioning Eschew your need to understand do not feel under obligation to
understand the non-understandable.
Monitor you own mistakes Model honesty and courage via acknowledgement of your own mistakes
o Currento Future
Suggest that mistakes offer opportunities to re-visit to learn more aboutcontexts, experiences, and feelings
-
7/27/2019 Adelaide Minding the Person
5/61
-
7/27/2019 Adelaide Minding the Person
6/61
Essential to the Stance Keep it current what the patient feels right now
Start by empathising finding a way of stating
that you genuinely understand distress Explore in the relational realm not just the intra-
psychic
Lower arousal by bringing it to the person of thetherapist
What have I done?
Stick to mentalizing aim in somewhat doggedmanner
Quickly step back if patient seems to lose control
-
7/27/2019 Adelaide Minding the Person
7/61
Therapist Stance
Explicit Mentalization Not directly concerned with content but with helping the
patient to generate multiple perspectives on the fly
to free himself up from being stuck in the realityof one view
(primary representations and psychic equivalence) to experience an array of mental states (secondary
representations) and
to recognize them as such (meta-representation).
Explication draws attention back to implicitrepresentationsfeelings for example
use language to bolster engagement on the implicit level ofmentalization
highlight the experience of feeling felt (mentalized affectivity)
-
7/27/2019 Adelaide Minding the Person
8/61
MBT Family also knownas SMART
LONDON-AFC HOUSTON-BAYLOR
Pasco Fearon Laurel WilliamsMary Target J ackie McGregorPeter Fonagy J ohn Sargeant
Stephen Butler Efrain BleibergPeter Fuggle
-
7/27/2019 Adelaide Minding the Person
9/61
MBT-FT Assumptions Mentalizing is powerfully effected by family
influences
Mentalizing is impaired acutely anddevelopmentally under conditions of stress
Problems with mentalizing may reduce families
capacities to repair relationships and findsolutions to relational problems
MBT-FT aims to improve general family-wide
mentalizing skills and target specific mentalizingdifficulties implicated in an identified relationalproblem
-
7/27/2019 Adelaide Minding the Person
10/61
Basic Clinical Model
Key proposition: emotional and behaviouralproblems are essentially relational in nature
Consideration, interpretation and appraisal ofmental states (in self and other) essential forhealthy relationships
Families and individuals vary in their capacity to
mentalize for a multitude of reasons (e.g. earlyexperience, genetics, current stressors)
Problems with mentalizing create distressing and
stressful family interactions which furtherundermine mentalizationThese interactions give rise to relational problems
that undermine family coping, creativity andresilience
-
7/27/2019 Adelaide Minding the Person
11/61
Cycles of inhibition of mentalizing in a family
Powerful emotion
Poor mentalising
Inability to understandor even pay attention
to feelings of others
Others seem
incomprehensible
Try to control or
change others
Frightening, undermining,frustrating, distressing or
coercive interactions
Loss of certaintythat thoughts are
not real
-
7/27/2019 Adelaide Minding the Person
12/61
Vicious Cycles of Mentalizing Problems
Within the Family
Powerful emotion
Poor mentalising
Inability to understand
or even pay attention
to feelings of others
Others seem
incomprehensible
Frightening, undermining,frustrating, distressing orcoercive interactions
Try to control orchange others oroneself
Person 1
Powerful emotion
Poor mentalising
Inability to understandor even pay attention
to feelings of others
Others seem
incomprehensible
Try to control or
change others oroneself
Frightening, undermining,frustrating, distressing or
coercive interactions
Person 2
-
7/27/2019 Adelaide Minding the Person
13/61
Treatment to promote mentalizing: the MBT-
FT protocol Objectives:
To help families shift from coercive, non-mentalizingcycles (impasses) to mentalizing discussions that canpromote trust, security and attachment
To promote parents sense ofcompetence in generaland, in particular, help them to help their children developmentalizing skills and attitudes
To practice mentalizing in the specific areas in which
mentalizing has become inhibited
To initiate virtuous cycles within the family, with peers,and in school which reinforce mentalizing, communication
and mutually supportive solutions to problems
-
7/27/2019 Adelaide Minding the Person
14/61
Similarities with other therapies PsychodynamicDrawing attention to, encouraging recognition of,
unacknowledged feelings, inner experiences, conflictingfeelings and repetitive patterns of behaviour
No transference interpretation of unconscious conflict Here-and-now psychological content in relationship context
CBT
Thought processes are mediators between experience andbehaviourNo reference to cognitive errors, distortions, negative automatic
thoughts, attentional biases or schemas
Family therapy Focuses on how thoughts and feelings affect behaviour within
relationships Systemic in seeing problems as inherently relational and
encouraging curiosity about other peoples thoughts andfeelings (cf. circular questioning) Fully articulated to the family, directive and psychoeducational
-
7/27/2019 Adelaide Minding the Person
15/61
Core mentalizing interventions Overarching principal is to take and encourage the
familial inquisitive stanceby collaborating in thedevelopment of a mentalizing formulations
Identifying, highlighting and praising examples ofpositive mentalizing
Sharing curiosity about mental states Pause and search tracking mental state
changes as they occur during interactions
Identifying and labeling hidden feeling states
Identifying and working with typical non-
mentalizing impassesTherapists use of self
-
7/27/2019 Adelaide Minding the Person
16/61
Pilot Study of MBT-FT at Baylor
and Anna Freud Centre AFC sample
33 families recruited65% of index child gender is male
Average age was 11.7, SD=3.0, range: 6-17
39% male and 35% female caregiver blackand ethnic minority
38% of women married or cohabiting
60% of men and 62% of women haveuniversity education
Compared to UK Consortium of Child andAdolescent Mental Health Service outomes
-
7/27/2019 Adelaide Minding the Person
17/61
Parent rated pre-post strength and difficultiesscores (SDQ)
P
-
7/27/2019 Adelaide Minding the Person
18/61
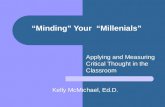
Value added pre-post SDQ scores
2.3
5.7
0.8
2.2
1.5
3.9
0.0
1.0
2.0
3.0
4.0
5.0
6.0
CORC comparison (n=225) SMART (n=33)
Using the youthinmind formula to calculate the added value of specialistintervention over 6 m. relative to change without treatment
Value added = 2.3 + 0.8*T1Total + 0.2*T1Impact 0.3*T1Emotion T2Total
Value added= 3.9 (95% CI: 2.3, 5.7) Effect size= .80
-
7/27/2019 Adelaide Minding the Person
19/61
Creating a peaceful schoollearning environment
Stuart W. Twemlow, Peter Fonagy,
Eric M. Vernberg, J ennifer A. Mize,Edward J . Dill, Todd D. Little,
J ohn A. Sargent
-
7/27/2019 Adelaide Minding the Person
20/61
Assumptions, Aims and Adjuncts
The whole school community contributesto bullying-related dysfunction
Peaceful collaboration with othersrequires prioritizing their subjectivestates, thus placing limits upon the urge
to violently control the behaviour of lesspowerful members of the group
-
7/27/2019 Adelaide Minding the Person
21/61
Assumptions, Aims and Adjuncts
CAPSLE aims constantly to focus on the mentalstates of all those involved in the power dynamicsof interpersonal violence (the bystander as well
as the bully and the victim) through:a positive climate campaign to draw attention to the
subjective experiences of bully, victim, and bystander
a classroom management plan that requires teachersto elaborate the thoughts and feelings associated withacts of aggression in the classroom
a defensive martial arts program based on mindfulness
peer or adult mentorship that create additionalopportunities for reflective interpersonal interaction
reflection time which offers opportunities for the classto consider shared immediate past experience together
-
7/27/2019 Adelaide Minding the Person
22/61
Increasing Mentalization Should Reduce
Violence: The Peaceful Schools Project9 schools randomly assigned to
CAPSLESchool Psychiatric Consultation
Treatment as usualoProgrammes as usual
Design3 year study
2 years of formal manualized intervention3rd year test of generalisation
-
7/27/2019 Adelaide Minding the Person
23/61
10 Schools, including 2,712Children, Stratified and Cluster
Randomized
19 Eligible Elementary Schools,Including 6,522 K-5th Grade Children
10 Elementary Schools Elected ToParticipate, Including 2,712 Children
1 School(178 Children)Withdrew FromTreatment as
Usual
Condition
675 Children
Treatment as Usual
In 3 Schools
824 Children
SPC
In 3 Schools
1,035 Children
CAPSLE
In 3 Schools
Only 3rd-5th Grade ChildrenCompleted Research Instruments
SPC Children
Participating296 in Year 1283 in Year 2323 in Year 3
CAPSLE Children
Participating391 in Year 1356 in Year 2395 in Year 3
Treatment as Usual
Children Participating271 in Year 1221 in Year 2217 in Year 3
-
7/27/2019 Adelaide Minding the Person
24/61
Key Results of The Peaceful Schools
Project: Peer Nomination SPC vs TAU
Increase in helpful bystanding (p
-
7/27/2019 Adelaide Minding the Person
25/61
Mean Proportions of Observed
Disruptive Behaviors Over Two Yearsof Active Intervention
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
Time 1 Time 2
ControlCAPSLE
SPC
Tests of simple effects between 1st and 2nd year of intervention
CAPSLE: t(106) = 5.21, p < .001, d=.94 (95% CI: -1.0, 2.9)SPC: t(106) = .50, p > .05TAU: t(106) = .13, p > .05
-
7/27/2019 Adelaide Minding the Person
26/61
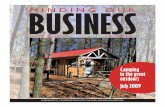
Mean Proportions of Observed Off-task
Behaviors Over Two Years of ActiveIntervention
0
0.02
0.04
0.06
0.08
0.1
0.12
0.14
Time 1 Time 2
Control
CAPSLE
SPC
Tests of simple effects between 1st and 2nd year of intervention
CAPSLE: t(106) = 8.26, p < .001, Cohens d=1.61 (95% CI: -.38, 3.6)SPC: t(106) = 1.19, p > .05TAU: t(106) = .14, p > .05
-
7/27/2019 Adelaide Minding the Person
27/61
Minding the baby
Arietta Slade, PhD,
Lois Sadler, PhD, APRN, PNPLinda Mayes, MD,
A Collaboration:
Yale Child Study Center Yale University School of Nursing Fair Haven Community Health Center
-
7/27/2019 Adelaide Minding the Person
28/61
Theory-based Intervention
Social cognition plays a crucial role in protectingagainst the effects of trauma
A Reflective Parenting Program Enhancing a mothers capacity to understand her own
as well as the babys mental states: feelings, thoughts,
desires, and intentions that underlie behavior Other theoretical emphases Human ecology/transition to parenthood
Build maternal self efficacyDevelopmentally (teen-friendly) and culturally
sensitive
-
7/27/2019 Adelaide Minding the Person
29/61
Sample of Families An urban at-risk population - with
emotional/physical trauma and muchpoverty
Minding the Baby Mothers
Women between 14 and 25First pregnancy
No active drug use at time of pregnancydiagnosis
No serious or terminal medical illness
-
7/27/2019 Adelaide Minding the Person
30/61
Characteristics of our Families
Enrolled 49 intervention, & 25 control Moms
(60 babies so far) 3 LBW, 4 preterm
Mothers average age 19.5 years (range=14-25)
Ethnicity: 66% Latina, 24% African-American,10% white & mixed heritage
Marital status: 12% married, 60% cohabiting,
28% single with no FOB involvement Multigenerational family violence patterns
-
7/27/2019 Adelaide Minding the Person
31/61
The Setting and Plan of Visits
Recruitment of mothers during pregnancyfrom prenatal care groups run by nurse
midwives- consent process Initial engagement and assessment phase
Weekly home visits through one yearTransition visit at one year
Bi weekly visits during second year Graduation at two years
h i fl i i h
-
7/27/2019 Adelaide Minding the Person
32/61
What is a Reflective Parenting Approach?
Strategies to give voice to the babys experience(both physical and emotional).
Strategies to give voice to the mothers
experience of herself as a parent. Strategies to bring alive mothers positive
feelings for the child.
Strategies to develop the mothers capacities toreflect and contemplate. Help mother to learn words and ideas to express ideas about own
lifebefore she can think about how the baby experiences her. A reality tohow she feels; then how the baby might feel. Using own experience of themother to demonstrateit seems to me that you are.then how does this fitinto the babys life/experience/feelings
Strategies to develop mothers sense ofcompetence
Wh i R fl i P i A h?
-
7/27/2019 Adelaide Minding the Person
33/61
What is a Reflective Parenting Approach?
Contact; looking babies in the eyes; speaking tobabies; listening to what they are telling the mother
Strategies such as speaking for the baby - useful for
issues of discipline, spoiling, cryingTalking about the babys behavior and intentions
underlying his behavior. Shes not hitting, grabbing,
biting, breaking the remote on purpose because shesbad and is trying to hurt you, but because of hercuriosity and need to explore and touch
Using teachable momentsto point outdevelopmental changes and refer those back to thebabies intentions, emotions etc. Oh look at how
interested she is in grabbing my earringsshe wantsto see and touch them
-
7/27/2019 Adelaide Minding the Person
34/61
What is a Reflective Parenting Approach?
Encouraging mothers expression of feelings (inparticular as they underlie her impulses) the feelingsshe is having when she turns away from or ignoresthe baby
Attend to mothers desire to be a good mother; giveself credit and look for strengths within own life andbehaviors
Have parent imitate what the child is doingto help toget into the childs experience, then link with fun and
games for parent and child (parent may not rememberhaving fun or playtime as child)
-
7/27/2019 Adelaide Minding the Person
35/61
-
7/27/2019 Adelaide Minding the Person
36/61
-
7/27/2019 Adelaide Minding the Person
37/61
Case Example
Amanda
17 years old, living with FOB and paternal family(dysfunctional family system)
Long history of parental substance abuse,neglect, DCF placement, violent parental death
Own health/social problems include malnutrition
during pregnancy, depression, conflict with FOBabout having and raising infant, chronic povertyand food insufficiency
-
7/27/2019 Adelaide Minding the Person
38/61
Amanda in Pregnancy
Overall RF Score: 3
While some awareness of own emotionalexperience, primary experience is ofblocking feelings, finding themoverwhelming, and being unable toregulate them when they do erupt.
I didnt want the baby. I felt like I was tooyoung. I just kinda blocked it out until Iended up in the hospital.
-
7/27/2019 Adelaide Minding the Person
39/61
Amanda 27 months later Overall RF Score: 6 (J ust short of Marked RF)
Less emphasis on confusion and helplessness thanin earlier interview. Negative affect, but regulated.
She is very aware of her babys thoughts andfeelings, and very interested in responding to these,even though she sometimes finds this taxing and
frustrating Highly attuned to the dynamic aspects of mental
states, especially in relation to her child
Particularly conscious of the intergenerationaleffects of her mothers way of regulating affects andrelationships upon her parenting
Still afraid to speak
Reflective Comments from Mothers about
-
7/27/2019 Adelaide Minding the Person
40/61
Reflective Comments from Mothers aboutMTB
When you are
aware about
yourself, its easier
to be aware of your
child
They changed my
framework ofthinking about my
daughter. They
helped me to think
things out and tothink about her
personality when I
talk to her.
They help you to help you,
-
7/27/2019 Adelaide Minding the Person
41/61
MBT-BPD
Anthony Bateman
Peter Fonagy
Rory Bolton
Karen OShaugnessy
-
7/27/2019 Adelaide Minding the Person
42/61
Interventions: Spectrum
Supportive/empathic
Mostinvo
lved
Clarification, elaboration, challenge
Basic mentalizing and affect focus
Leastin
volved
Interpretive mentalizing
Mentalizing the transference
Interventions:
-
7/27/2019 Adelaide Minding the Person
43/61
Interventions:
Supportive & empathic Identifying and exploring positive mentalizing
judicious praise you have really managed to understand what
went on between you Examine how it feels to others when such mentalizing occurs
how do you think they felt about it when you explained it to them
Explore how it feels to self when an emotional situation ismentalized how did working that out make you feel
Identifying non-mentalizing fil lers Fillers: typical non-mentalizing thinking or speaking, trite
explanations Highlight these and explore lack of practical success associated
with them
Interventions:
-
7/27/2019 Adelaide Minding the Person
44/61
Interventions:
Basic Mentalizing Stop, Re-wind, Explore
Lets go back and see what happened just then. At first you
seemed to understand what was going on but then Lets try to trace exactly how that came about Hang-on, before we move off lets just re-wind and see if we can
understand something in all this.
Labeling with qualification (I wonder ifstatements) Explore manifest feeling but identify consequential experience
Although you are obviously dismissive of them I wonder if thatleaves you feeling a bit left out?
I wonder if there are some resentments that make it hard for youto allow yourself to listen to rules. Lets think about why the rulesare there?
I wonder if you are not sure if its OK to show your feelings toother people?
Interventions:
-
7/27/2019 Adelaide Minding the Person
45/61
Interventions:
Interpretive Mentalizing Transference tracers always currentLinking statements and generalization
o That seems to be the same as before and it may be thato So often when something like this happens you begin to feel
desperate and that they dont like you
Identifying patternso It seems that whenever you feel hurt you hit out or shout at
people and that gets you into trouble. May be we need toconsider what happens otherwise.
Making transference hintso I can see that it might happen here if you feel that something I
say is hurtful
Indicating relevance to therapyoThat might interfere with us working together
Components of mentalizing the
-
7/27/2019 Adelaide Minding the Person
46/61
Components of mentalizing the
transference Validation of experience
Exploration in the current relationship Accepting and exploring enactment (therapist
contribution, therapists own distortions)
Collaboration in arriving at an understanding
Present an alternative perspective
Monitor the patients reaction
Explore the patients reaction to the new
understanding
-
7/27/2019 Adelaide Minding the Person
47/61
-
7/27/2019 Adelaide Minding the Person
48/61
Trial 2:
Cohort of MBT Partial HospitalTreatment (18 months)
(Bales and Verheul, Holland)
Attempted Suicide: NNT (18 months)=2.4
Self-Mutilating: NNT (18 months)=2.3
General dysfunction: ES(18m)=1.9
Depression: ES (18m)=2.8
-
7/27/2019 Adelaide Minding the Person
49/61
Trial 3:
8 year follow up of patientstreated with MBT compared withTAU
(Bateman & Fonagy submitted)
Design of MBT Partial Hospital follow-up study
-
7/27/2019 Adelaide Minding the Person
50/61
g p p y
41 (22 MBT v 19 TAU) patients followed up 8years after they started treatment
Contact was made by letter, via their generalpractitioner, and by telephone.
Medical and psychiatric records were obtained
for all 41 patients and relevant informationextracted.
Patients interviewed by research psychologists
who remained blind to original group allocation. 5 patients (2 MBT/3TAU) refused interview
1 patient from TAU had died from suicide
Assessment at follow-up interview
-
7/27/2019 Adelaide Minding the Person
51/61
Assessment at follow up interview
Primary outcome
Zanarini Rating Scale for DSM-IV BPD (ZAN-
BPD)Global Assessment of Function (GAF)
Secondary outcomes
Number of self-harm and suicide attemptsNumber of emergency room visits
Length of hospitalization
Continuing out-patient psychiatric careUse of medication, psychological therapies, and
community support.
Vocational status
Zan-BPD (22 v 15) Means (SD)
-
7/27/2019 Adelaide Minding the Person
52/61
Zan BPD (22 v 15) Means (SD)
MBT-PH TAU Significance
Positive criteria
n (%)
3 (13.6) 13 (86.7) 2 = 16.5 p=.000004
Total mean (SD) 5.5 (5.2) 15.1 (5.3) F1,35 = 29.7 p=.000004
Affect mean (SD) 1.6 (2.0) 3.7 (2.0) F1,35 = 9.7p=.004
Cognitive mean(SD)
1.1 (1.4) 2.5 (2.0) F1,35 = 6.9 p=.02
Impulsivity mean(SD) 1.6 (1.8) 4.1 (2.3)
F1,35
= 13.9 p=.001
Interpersonalmean (SD)
1.5 (1.7) 4.7 (2.3) F1,35 = 23.2p=.00003
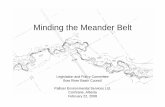
Partial Hospital RCT: GAF Scores
-
7/27/2019 Adelaide Minding the Person
53/61
p
30
35
40
45
50
55
60
65
Baseline End
treatment
4 yrs FU 6 yrs FU 8 yrs FU
MeanG
AFScore
MBT-PH
TAU
-
7/27/2019 Adelaide Minding the Person
54/61
Conclusions from long term follow-up
-
7/27/2019 Adelaide Minding the Person
55/61
MBT-PH group continued to do well 5 years after allMBT treatment had ceased A strong correlate of improvement in the MBT-PH
group is vocational status ?cause or consequence TAU did badly within services despite significant input. TAU is not necessarily ineffective in its components
but package or organization is not facilitating possible
natural recovery. BUTSmall sample, allegiance effects (despite attempts
being made to blind the data collection) limit theconclusions.
GAF scores continue to indicate deficits. Suggestsless focus during treatment on symptomatic
problems greater concentration on improvinggeneral social adaptation.
-
7/27/2019 Adelaide Minding the Person
56/61
Design of Intensive out-patient MBT randomisedcontrolled trial
-
7/27/2019 Adelaide Minding the Person
57/61
controlled trial.
Referrals (n=71 & n=63 for IOP-MBTand SCM groups respectively)
Random allocation (minimisation forage, gender, antisocial PD)
Individual (50 mins) + Group (1.5 hrs)weekly for 18 months
Assessments at admission, 6months, 12 months, 18 months
Medication followed protocol
Suicide attempts in 6 month period
-
7/27/2019 Adelaide Minding the Person
58/61
Suicide attempts in 6 month period
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
Baseline 6 months 12 months 18 months
Proportionsuicideattempt
ControlMBT
Limitations
-
7/27/2019 Adelaide Minding the Person
59/61
Limitations
Not all outcome data analysed
Outcome diagnostic data not yet available Small number of therapists
Conclusion
-
7/27/2019 Adelaide Minding the Person
60/61
In advocating mentalization-based treatment weclaim no innovation.
Mentalization-based treatment is the least novel
therapeutic approach imaginable: it addressesthe bedrock human capacity to apprehend mindas such.
Is all psychotherapy mentalization basedtreatment? No more than all therapy influencingbehaviour is behaviour therapy!
Nonetheless, fostering the capacity to mentalizemight be our most significant therapeuticendeavour: cultivating a fully functioning mind is ahigh aspiration indeed.
-
7/27/2019 Adelaide Minding the Person
61/61
Thank you formentalizing!