Addressing the Social Determinants of Health Challenges and...
36
Addressing the Social Determinants of Health Challenges and Pathways Thelma Narayan Centre for Public Health and Equity, SOCHARA Bangalore, India Member , People’s Health Movement (PHM) Nuffield Council on Bioethics Symposium , 22 nd June 2011, London, United Kingdom
-
Upload
phungquynh -
Category
Documents
-
view
221 -
download
1
Transcript of Addressing the Social Determinants of Health Challenges and...
Addressing the Social Determinants of HealthChallenges and Pathways
Thelma NarayanCentre for Public Health and Equity, SOCHARA
Bangalore, IndiaMember , People’s Health Movement (PHM)
Nuffield Council on Bioethics Symposium , 22nd June 2011, London, United Kingdom
Plan of Presentation• The first 10 slides offer brief reflections about the societal determinants of health and health inequalities
•The following 5 slides provide an overview of health indicators from India which are dependent on the SDH
•Together they highlight the nature of the challenges
• The last 15 slides are a snapshot of responses by the community, civil society, governments and academics over the past decade indicating critical pathways and partnerships to address health inequalities
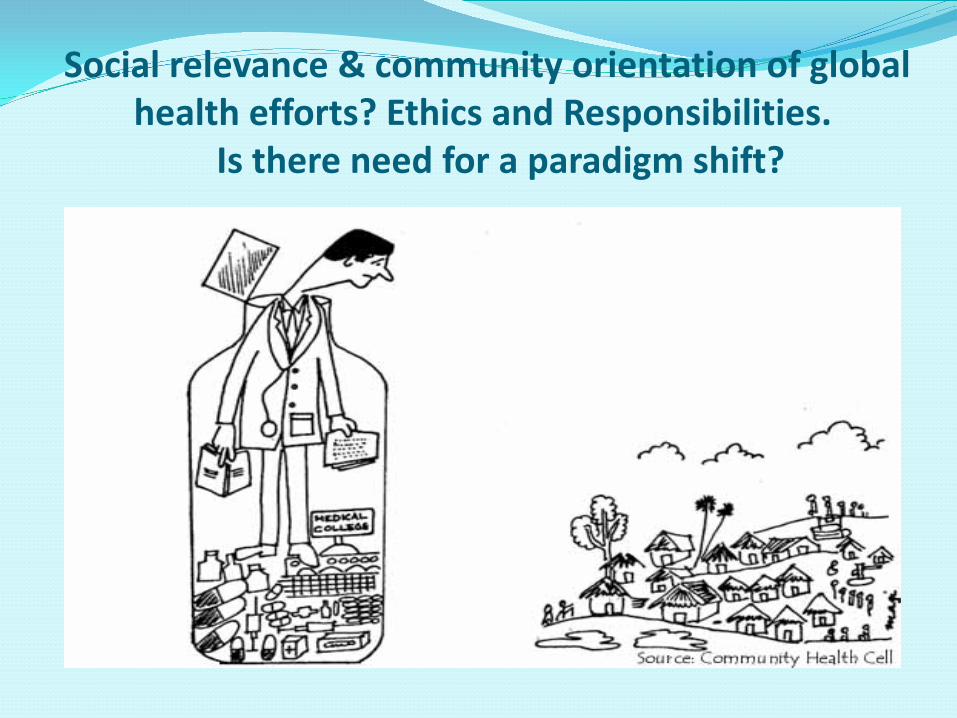
Social relevance & community orientation of global health efforts? Ethics and Responsibilities.
Is there need for a paradigm shift?
Tackling the Social Determinants of Health in an Era of Globalization
There is an urgent need to address the root cause of inequalities in disease, disability and health.
Social conditions in which people live and work or the social determinants of health.
Source: WHO Commission on Social Determinants of Health (WHO- CSDH), 2005 -2008
Need for policies and practice that tackle the underlying determinants of health inequalities, within a framework of cross-cutting rights.
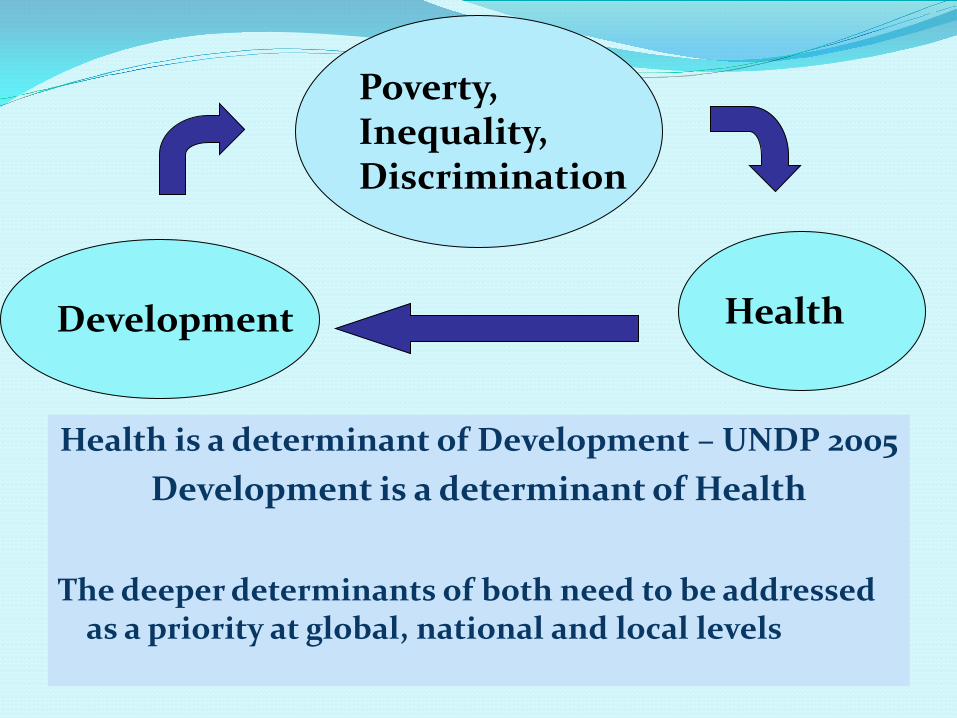
Health is a determinant of Development – UNDP 2005Development is a determinant of Health
The deeper determinants of both need to be addressed as a priority at global, national and local levels
Poverty, Inequality, Discrimination
Development Health
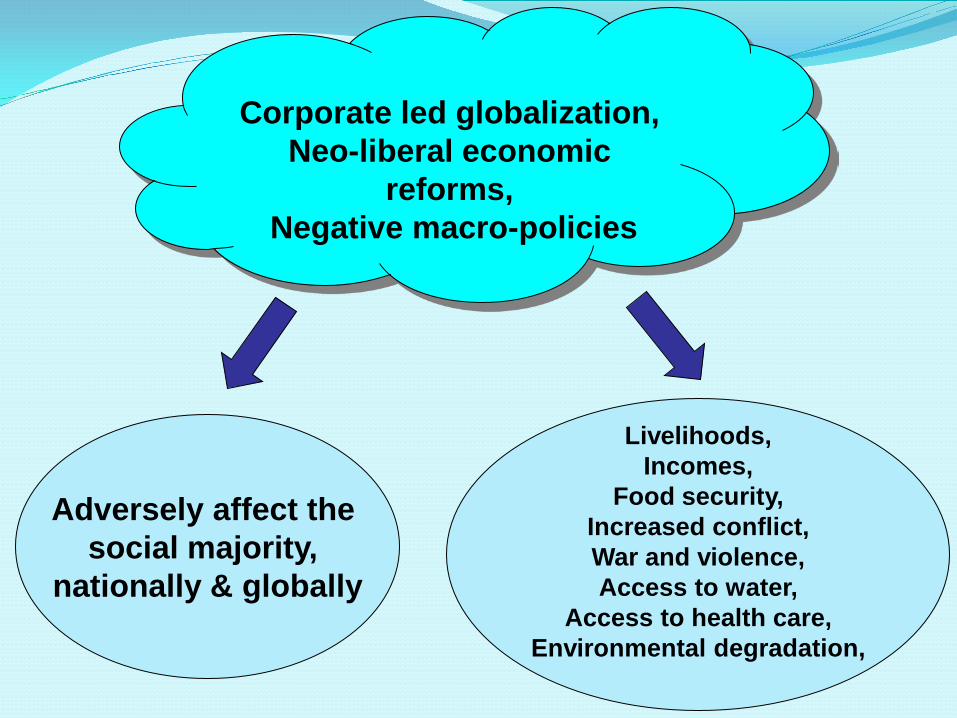
Corporate led globalization, Neo-liberal economic
reforms,Negative macro-policies
Adversely affect the social majority,
nationally & globally
Livelihoods,Incomes,
Food security,Increased conflict,War and violence,Access to water,
Access to health care,Environmental degradation,
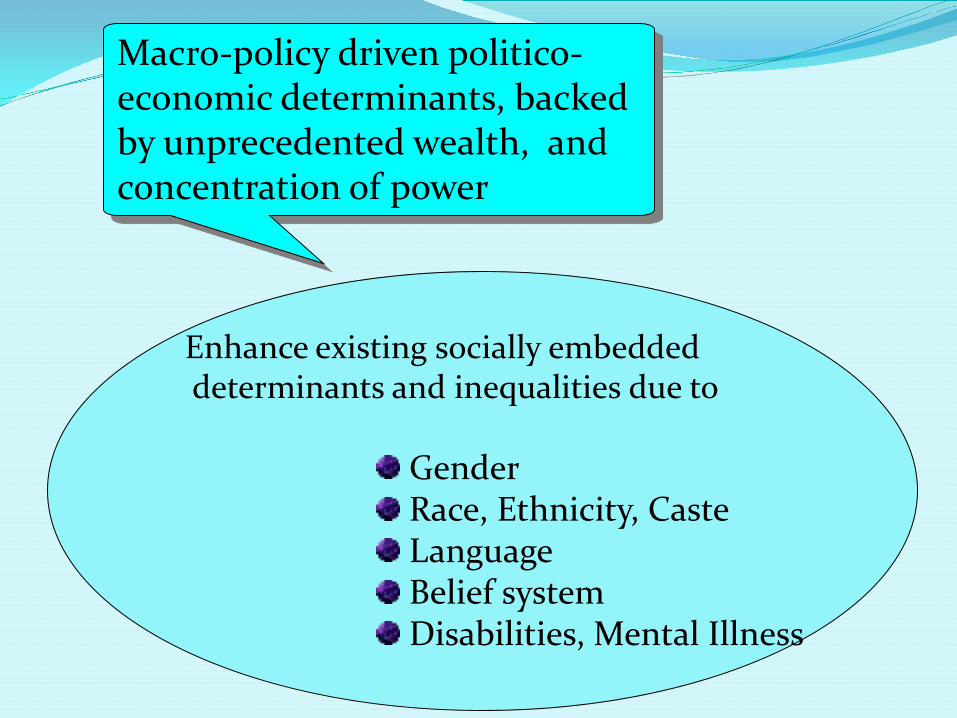
Macro-policy driven politico-economic determinants, backed by unprecedented wealth, and concentration of power
Enhance existing socially embeddeddeterminants and inequalities due to
GenderRace, Ethnicity, CasteLanguageBelief systemDisabilities, Mental Illness
“Disparities hampering progress are systematic, reflecting hierarchies of
advantage and disadvantage and
public policy choice”UNDP, 2005
Global Inequalities
High income countries represent 15 % of the world’s population
40% of the world’s population, ie 2.5 billion people living on less than $2 a day,
account for 5% of the global income
UNDP 2005

Trade, Development and Health
Over 2/3rd of the poor are small farmers and agricultural laborers
Unfair trade undermines their livelihood Led by the EU and USA developed country
agricultural subsidies are over $ 350 billion a year, ie, almost $ 1 billion a day, supporting large farmers and corporate agri-business
For a fraction of the cost, universal education, health and water for all can be achieved.
UNDP, 2006

International organisations & institutions
Roles and responsibilities for Global Health

INDIA: ? shining global example Overall employment growth in 1990s was 2/3rd to
half of 1980 For agricultural labourers, bulk of poor in India,
rate of growth of real wages per annum almost halved in the 1990s, compared to 1980s. Worsening of working conditions of labourers
in the informal sector and agriculture in past decade Open unemployment serious
- Jeyarajan and Swaminathan, 2003
JOBLESS GROWTH
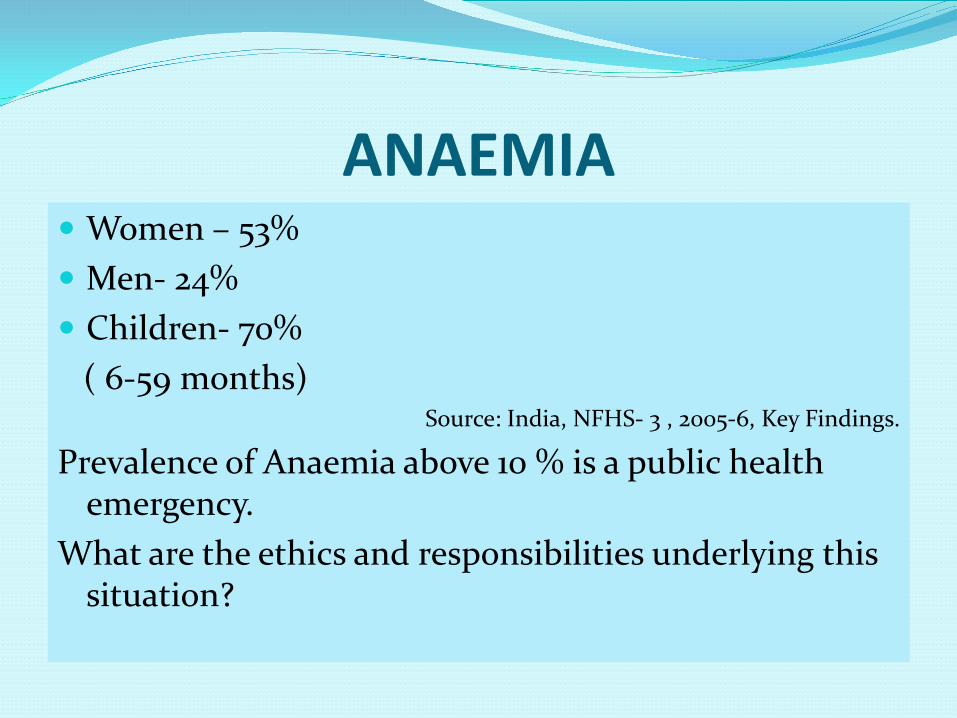
ANAEMIA Women – 53% Men- 24% Children- 70%
( 6-59 months) Source: India, NFHS- 3 , 2005-6, Key Findings.
Prevalence of Anaemia above 10 % is a public health emergency.
What are the ethics and responsibilities underlying this situation?
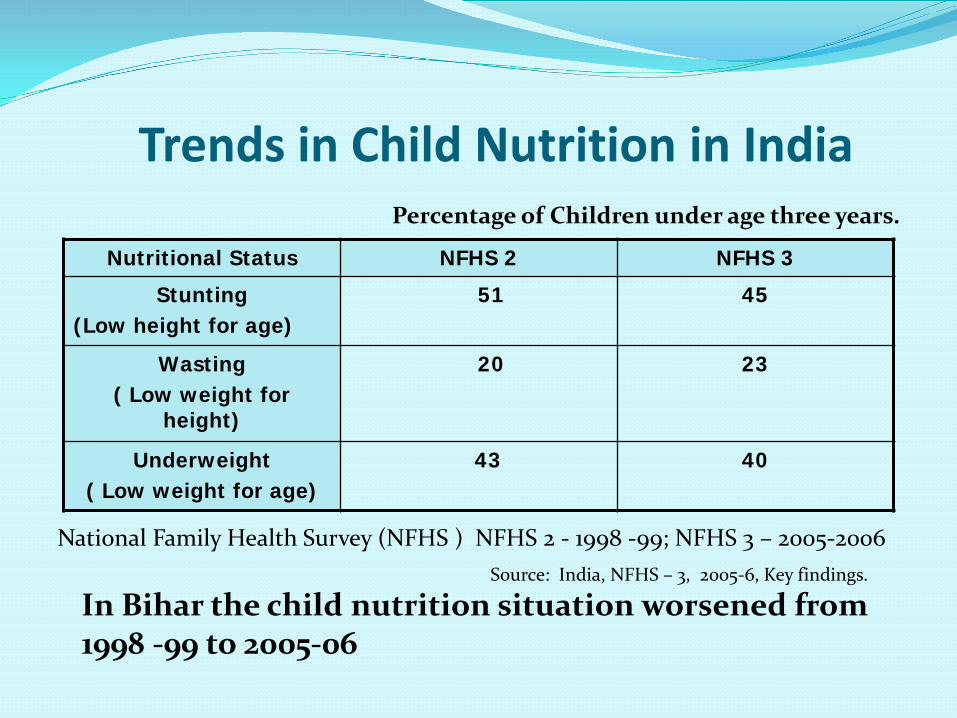
Trends in Child Nutrition in IndiaPercentage of Children under age three years.
Nutritional Status NFHS 2 NFHS 3
Stunting(Low height for age)
51 45
Wasting( Low weight for
height)
20 23
Underweight( Low weight for age)
43 40
Source: India, NFHS – 3, 2005-6, Key findings.
In Bihar the child nutrition situation worsened from 1998 -99 to 2005-06
National Family Health Survey (NFHS ) NFHS 2 - 1998 -99; NFHS 3 – 2005-2006
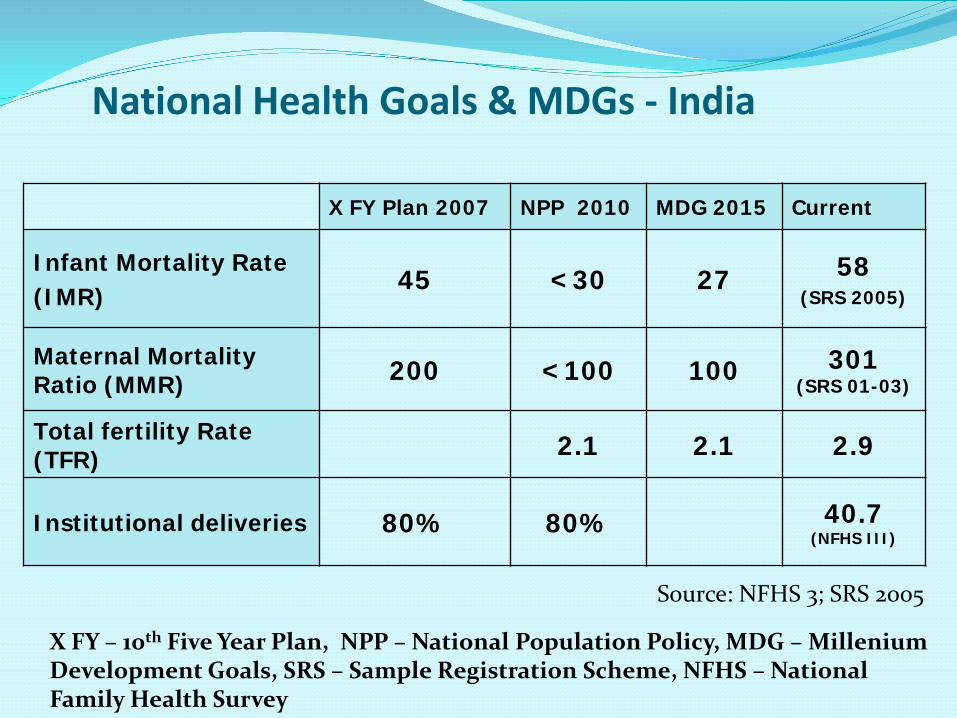
National Health Goals & MDGs - India
X FY Plan 2007 NPP 2010 MDG 2015 Current
Infant Mortality Rate(IMR)
45 <30 27 58(SRS 2005)
Maternal Mortality Ratio (MMR) 200 <100 100 301
(SRS 01-03)
Total fertility Rate (TFR) 2.1 2.1 2.9
Institutional deliveries 80% 80% 40.7 (NFHS III)
X FY – 10th Five Year Plan, NPP – National Population Policy, MDG – MilleniumDevelopment Goals, SRS – Sample Registration Scheme, NFHS – National Family Health Survey
Source: NFHS 3; SRS 2005
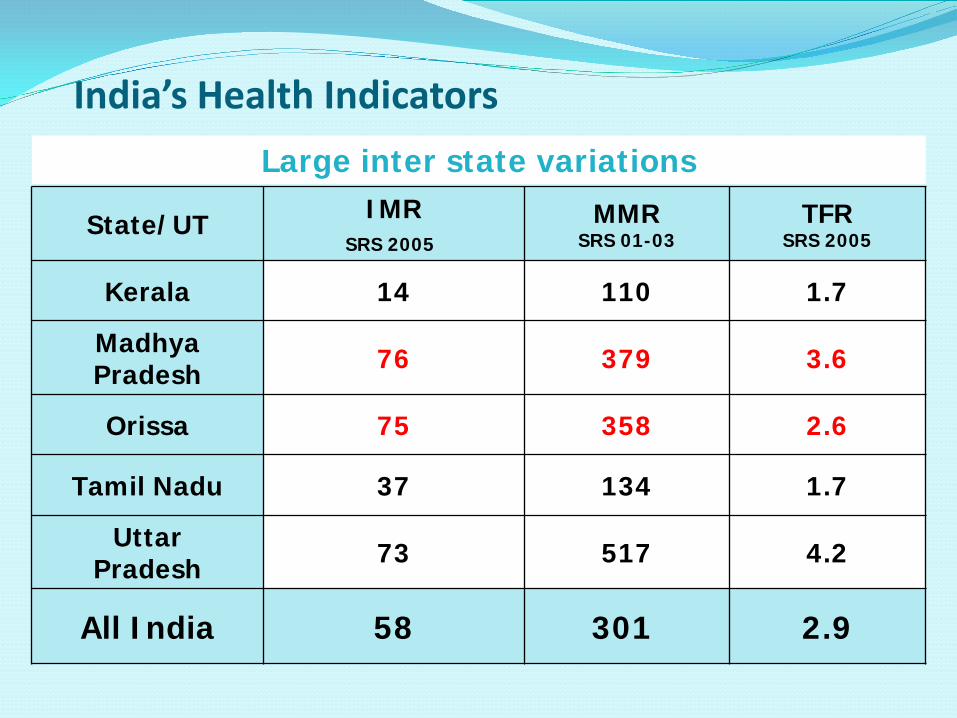
State/UT IMRSRS 2005
MMR SRS 01-03
TFR SRS 2005
Kerala 14 110 1.7
Madhya Pradesh 76 379 3.6
Orissa 75 358 2.6
Tamil Nadu 37 134 1.7
Uttar Pradesh 73 517 4.2
All India 58 301 2.9
Large inter state variations
India’s Health Indicators
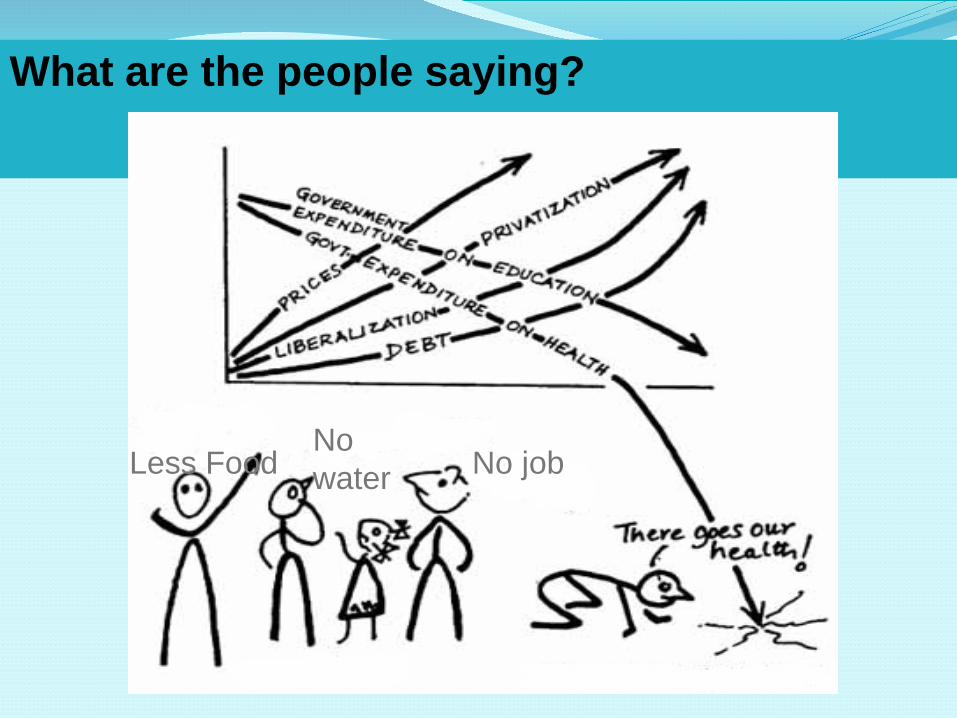
What are the people saying?
Less Food No jobNo water
Meeting Challenges in the New Millennium: with a People Centric Approach
With people back into the centre of primary health careThe public back into public health and
health systems and community voice and power back
into health policy discourse & decisions,As subjects & co-creators not objects
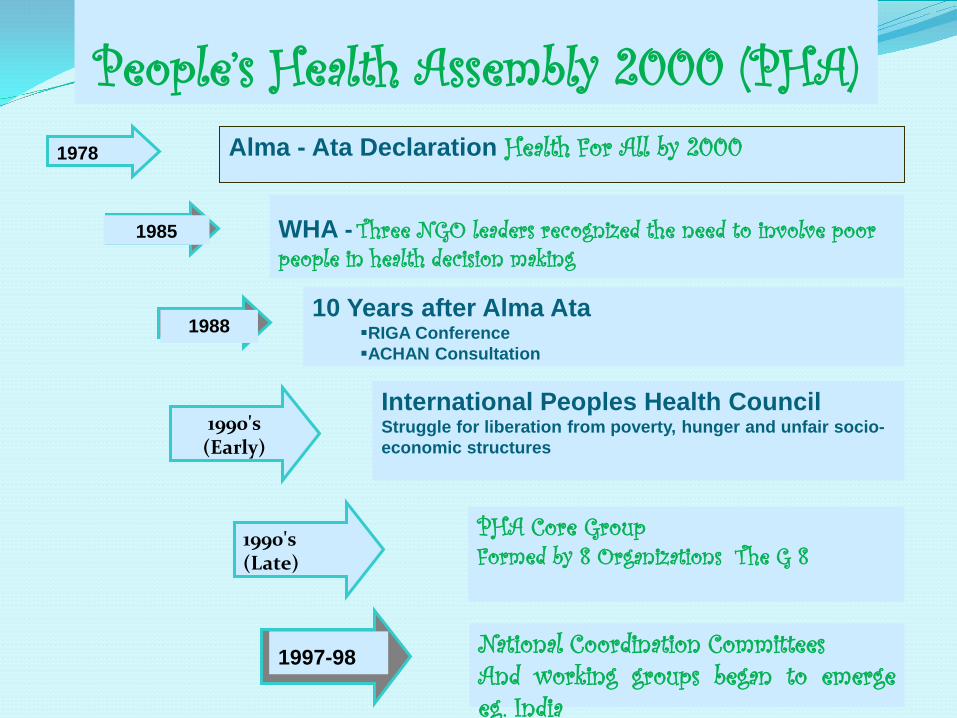
1978 Alma - Ata Declaration Health For All by 2000
1985 WHA - Three NGO leaders recognized the need to involve poor people in health decision making
10 Years after Alma AtaRIGA ConferenceACHAN Consultation
1988
1990's (Early)
International Peoples Health CouncilStruggle for liberation from poverty, hunger and unfair socio-economic structures
1990's (Late)
PHA Core Group Formed by 8 Organizations The G 8
1997-98 National Coordination Committees And working groups began to emergeeg. India
People’s Health Assembly 2000 (PHA)
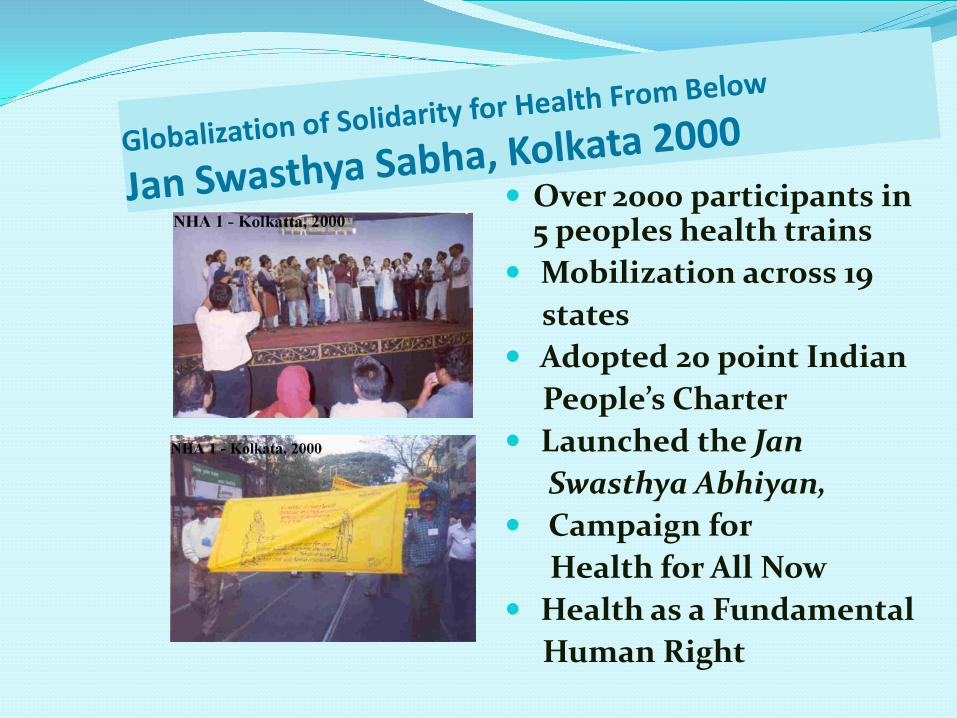
Over 2000 participants in 5 peoples health trains
Mobilization across 19 states
Adopted 20 point IndianPeople’s Charter
Launched the Jan Swasthya Abhiyan,
Campaign for Health for All Now
Health as a Fundamental Human Right
Globalization Of Health From Below The First Global People’s Health Assembly
In 2000 December , 1454 health activists from 75 countries met in Savar, Bangladesh to discuss the challenge of attaining Health for All, Now! Over 250 Indian delegates attended
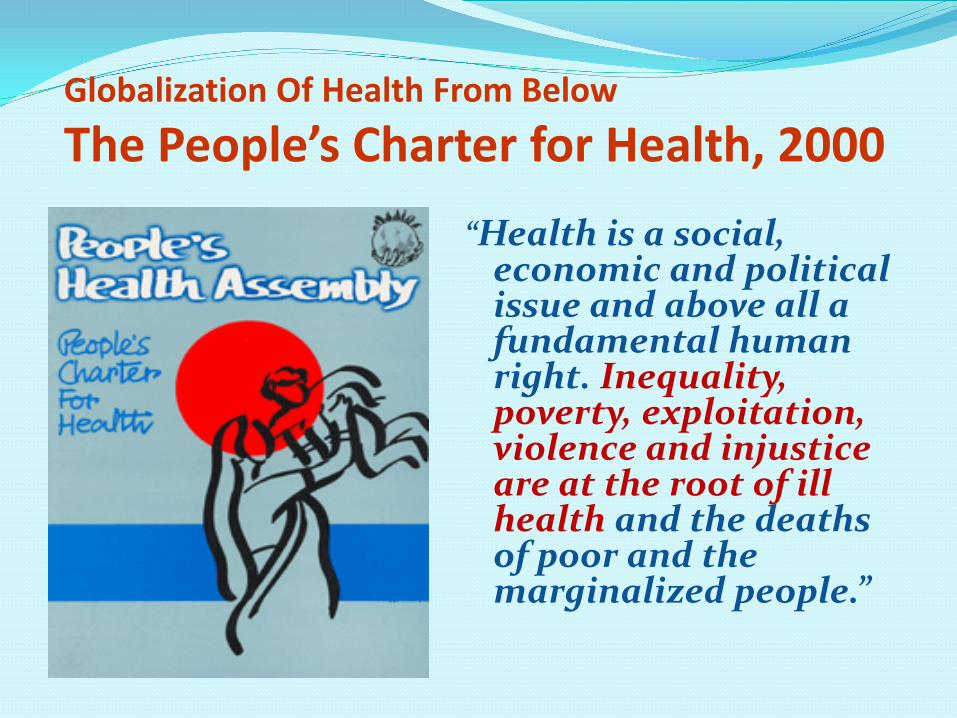
Globalization Of Health From Below
The People’s Charter for Health, 2000“Health is a social,
economic and political issue and above all a fundamental human right. Inequality, poverty, exploitation, violence and injustice are at the root of ill health and the deaths of poor and the marginalized people.”

Campaign on the Right to Health Care PHM - IndiaPublic Hearing
State and district action, from 2000 onwards
Indian Social Forum, November 2006
Second National Health Assembly – February 2007
Critical collaboration with National Rural Health Mission
Participation in the World Social Forum
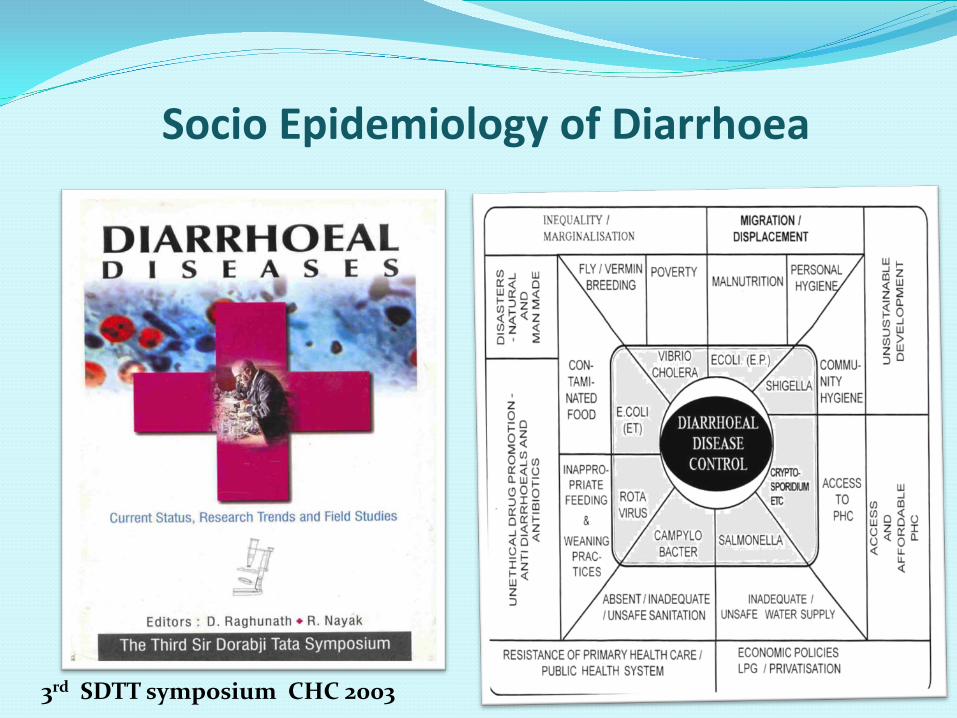
Socio Epidemiology of Diarrhoea
3rd SDTT symposium CHC 2003

Asian Social Forum, January 2003, Hyderabad
JSA members organized workshopson:1. The Right to Health Care2. Environment and Health3. Tobacco and Health4. The People’s Health Movement
Asian Social ForumJanuary 2003, Hyderabad - INDIA
World Social Forum, January 2004, MumbaiWorkshops on health rights & determinants by JSA and PHM

Campaigns on Gender Issues (an example from among several campaigns)
Campaign Against Sex Selective Abortion or Female Foeticide – 2001 onwards
Campaign on Violence against Women as a Public Health Challenge – 2000 onwards
Women’s Access to Primary Health Care - 2003 People’s Tribunal on Population Policies – 2004 10th International Women and Health Meeting –
2005 Gender and Power Issues in Medical Education Women’s Health Charter - 2007
Participants converge from many streams, groups,not only PHM/ JSA
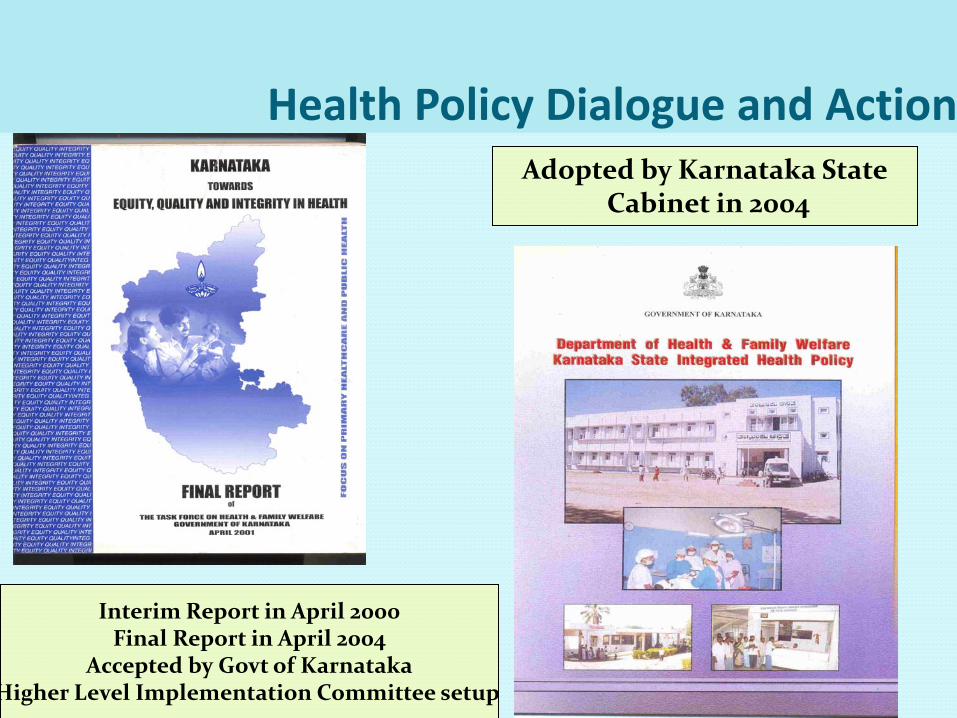
Health Policy Dialogue and ActionAdopted by Karnataka State
Cabinet in 2004
Interim Report in April 2000Final Report in April 2004
Accepted by Govt of KarnatakaHigher Level Implementation Committee setup

MAINSTREAM DEVELOPMENTS IN PUBLIC HEALTH WITH PARTNERSHIP OF ALTERNATIVE SECTOR – 1998-2008
National Health Policy Interaction - INDIAwith the National Rural Health Mission (NRHM)2005 0nwards
Members of Task Forces and Advisory Committees Shifted focus from Demography to Public Health
and community involvement Community Monitoring of the Health System. People’s Rural Health Watch Community Action for Health National ASHA Mentoring Group Universal Access to Health Care
Recently a National Mental Health Policy Group
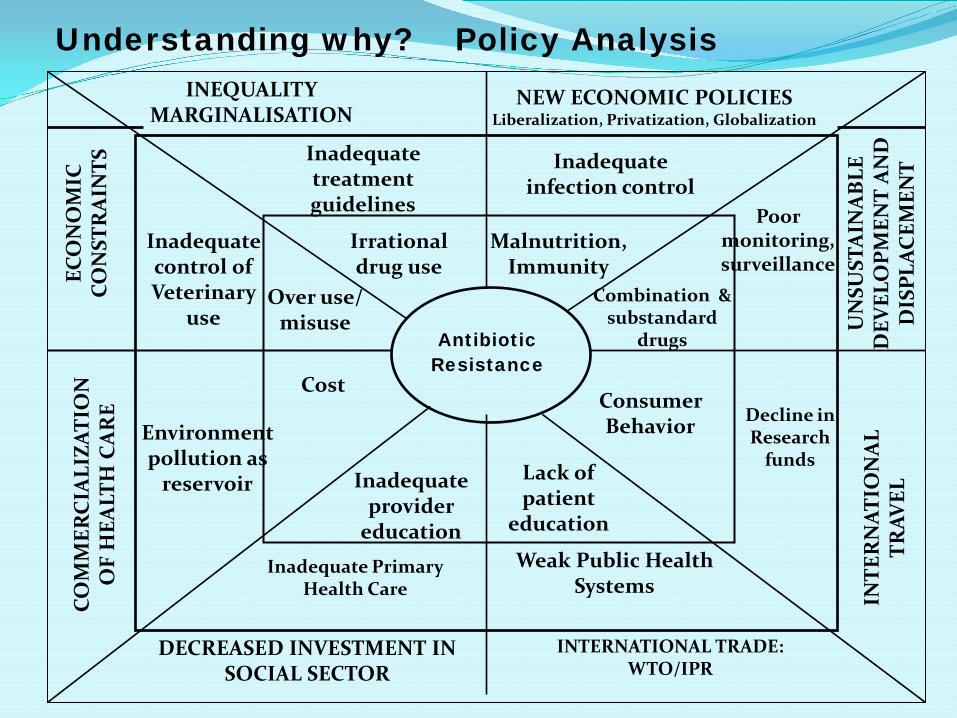
Antibiotic Resistance
Inadequate treatment guidelines
Inadequate infection control
Inadequate control of Veterinary
use
Poor monitoring, surveillance
Environment pollution as
reservoir
Inadequate Primary Health Care
Weak Public Health Systems
Decline in Research
funds
Consumer Behavior
Lack of patient
education
Inadequate provider
education
Cost
Over use/ misuse
Irrational drug use
Malnutrition, Immunity
Combination & substandard
drugs
Understanding why? Policy AnalysisINEQUALITY
MARGINALISATIONNEW ECONOMIC POLICIES
Liberalization, Privatization, Globalization
ECO
NO
MIC
CO
NST
RA
INTS
COM
MER
CIA
LIZA
TIO
N
OF
HEA
LTH
CA
RE
DECREASED INVESTMENT IN SOCIAL SECTOR
INTERNATIONAL TRADE: WTO/IPR
INTE
RN
ATIO
NA
L TR
AVEL
UN
SUST
AIN
AB
LE
DEV
ELO
PMEN
T A
ND
D
ISPL
ACEM
ENT

Antibiotic resistance
Antibiotic treatment guidelines/ schedules
Strengthening infection control in health care
institutions
Veterinary Use
Guidelines
Improving surveillance
Hospital waste
disposal.
Strengthening Primary Health Care
Strengthening Public Health Systems
Promoting more
research on the
problem
Promoting rational
consumer education
Multifaceted approaches for
Behavioral change
Provider / prescriber education
Cost control
Controlling OTC sales
Rational prescribing
Strengthening Nutrition
Controlling combination
drugs
What can be done…. Policy ActionLocal/national/regional
global actionPeople’s need oriented
economic/trade policies
Poli
tica
l Aw
aren
ess
and
supp
ort
Increased investment in health, nutrition, social welfare, education
sectors
Countering commercialization of health care
Equi
tabl
eto
uris
m
opti
ons
Tack
lin
g En
viro
n m
enta
l ch
alle
nge
s
Safe
dri
nki
ng
wat
er,
san
itat
ion

Globalization Of Health From Below Globalizing Solidarity
Folk from over 80 countries at the Second People’s Health Assembly, Cuenca, Ecuador, 2005

Second People’s Health Assembly (PHA2)July 2005, Cuenca - Ecuador
PHM Evaluation, 2004
ConclusionWorking together towards greater social justice in global health is imperative. The pathways are many. What will be our path?
Is there a role for community and civil society engagement?
What are the barriers in reaching the Health for All Goal?