Adaptive Treatment Strategies S.A. Murphy Workshop on Adaptive Treatment Strategies Convergence,...
24
Adaptive Treatment Strategies S.A. Murphy Workshop on Adaptive Treatment Strategies Convergence, 2008
-
date post
21-Dec-2015 -
Category
Documents
-
view
221 -
download
2
Transcript of Adaptive Treatment Strategies S.A. Murphy Workshop on Adaptive Treatment Strategies Convergence,...

Adaptive Treatment Strategies
S.A. Murphy
Workshop on Adaptive Treatment Strategies
Convergence, 2008

2
Outline
• What are Adaptive Treatment Strategies?• What are SMART trials?• SMART Designing Principles and
Analysis

3
Adaptive Treatment Strategies are individually tailored sequences of treatments, with treatment type and dosage adapted to the patient.
•Generalization from a one-time decision to a sequence of decisions concerning treatment
•Operationalize clinical practice.

4
Why use an Adaptive Treatment Strategy?
– High heterogeneity in response to any one treatment
• What works for one person may not work for another
• What works now for a person may not work later
– Improvement often marred by relapse• Remitted is not the same as cured.
– Co-occurring disorders/adherence problems are common

5
Example of an Adaptive Treatment Strategy
Treatment of depression. Goal is to achieve and maintain remission.
Provide Citalopram for up to 12 weeks gradually increasing dose as required. If the maximum dose has been provided for two weeks or if 12 weeks have occurred with no remission, but there has been a 50% improvement in symptoms, augment with Mirtazapine. Otherwise switch treatment to Bupropion. If remission is achieved, maintain on Citalopram and provide web-based disease management.
6
The Big Questions
•What is the best sequencing of treatments?
•What is the best timing of alterations in treatments?
•What information do we use to make these decisions?

7
What are Sequential Multiple Assignment Randomized Trials?
• Pinpoint a small number of critical decisions per patient to investigate.
• A randomization takes place at each critical decision (multiple randomizations for each patient).
•Goal is to inform the construction of an adaptive treatment strategy.
8
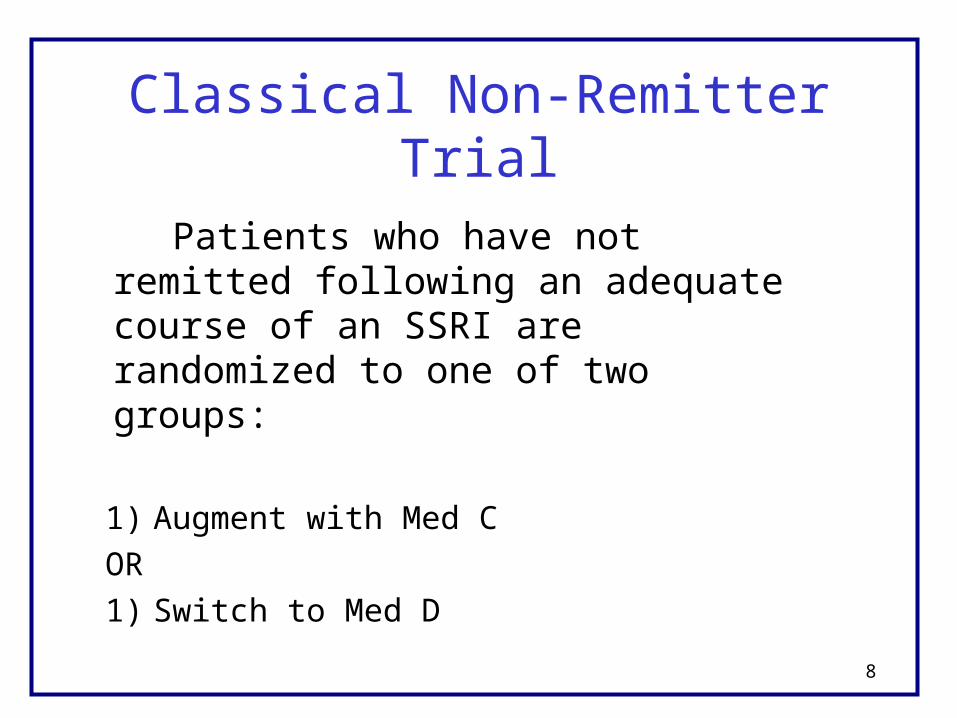
Classical Non-Remitter Trial
Patients who have not remitted following an adequate course of an SSRI are randomized to one of two groups:
1) Augment with Med C
OR
1) Switch to Med D

9
Non-Remitter Trial
Stage 1 Intermediate Stage 2 Final Decision Outcome Decision Outcome
Transfer Remission
SSRI
Augment w C No Remission R
Switch to D

10
Remitter/Non-Remitter Trial
Stage 1 Intermediate Stage 2 Final Decision Outcome Decision Outcome
WebDM Remission
R Monitor
SSRIAugment w C
No Remission RSwitch to D

11
From a Remitter/Non-Remitter Trial to a SMART
Stage 1 Intermediate Stage 2 Final Decision Outcome Decision Outcome
WebDM Remission R
Monitor SSRI
Augment w C No Remission R
Switch to D
RAugment w C
No Remission RSwitch to D
SSRI +WebCBT WebDM
RRemission Monitor

12
SMART Designing Principles
•KEEP IT SIMPLE: At each stage, restrict class of treatments only by ethical, feasibility or strong scientific considerations. Use a summary (responder status) instead of all intermediate outcomes (time until nonresponse, adherence, burden, stress level, etc.) to restrict class of next treatments.
•Collect intermediate outcomes that might be useful in ascertaining for whom each treatment works best; information that might enter into the adaptive treatment strategy.

13
SMART Designing Principles
•Choose primary hypotheses that are both scientifically important and aid in developing the adaptive treatment strategy.
•Power trial to address these hypotheses.

14
SMART Designing Principles:Primary Hypothesis
•EXAMPLE 1: (sample size is highly constrained): Hypothesize that the initial treatment SSRI + WebCBT leads to lower levels of symptoms over entire study than the initial treatment, SSRI alone (controlling for subsequent treatments via experimental design).
•EXAMPLE 2: (sample size is less constrained): Hypothesize that subjects who do not remit at the first stage of treatment will exhibit higher remission rates if provided a switch to med D as opposed to augmenting by med C. (embedded non-remitter trial).

15
Ex. 1: Two-Group ComparisonStage 1 Intermediate Stage 2 Final Decision Outcome Decision Outcome
WebDM Remission R
Monitor SSRI
Augment w C No Remission R
Switch to D
RAugment w C
No Remission RSwitch to D
SSRI +WebCBT WebDM
RRemission Monitor

16
Ex. 2: Two-Group ComparisonStage 1 Intermediate Stage 2 Final Decision Outcome Decision Outcome
WebDM Remission R
Monitor SSRI
Augment w C No Remission R
Switch to D
RAugment w C
No Remission RSwitch to D
SSRI +WebCBT WebDM
RRemission Monitor

17
SMART Designing Principles
•Choose secondary hypotheses that further develop the adaptive treatment strategy and use the randomization to eliminate confounding.
•EXAMPLE: Hypothesize that patients who have experienced less than a 50% improvement in response in the first stage will be more likely to remit if they receive a switch to Med D as opposed to augmentation by Med C.

18
Regression using Response Level during Stage 1
Stage 1 Intermediate Stage 2 Final Decision Outcome Decision Outcome
WebDM Remission R
Monitor SSRI
Augment w C No Remission R
Switch to D
RAugment w C
No Remission RSwitch to D
SSRI +WebCBT WebDM
RRemission Monitor

19
Two-Group Comparison of Remitters
Stage 1 Intermediate Stage 2 Final Decision Outcome Decision Outcome
WebDM Remission R
Monitor SSRI
Augment w C No Remission R
Switch to D
RAugment w C
No Remission RSwitch to D
SSRI +WebCBT WebDM
RRemission Monitor

20
Discussion
• Secondary analyses can use patient characteristics/outcomes to provide evidence for a more sophisticated adaptive treatment strategy.
• SMART studies and analyses targeted at scientific goal of informing the construction of a high quality adaptive treatment strategy

21
Acknowledgements: This presentation is based on work with many individuals including Daniel Admirall, Linda Collins, Kevin Lynch, Jim McKay, David Oslin, and Tom Ten Have.
Email address: [email protected]
Slides with notes at:
http://www.stat.lsa.umich.edu/~samurphy/
Click on seminars > health science seminars
Extra slides follow

22
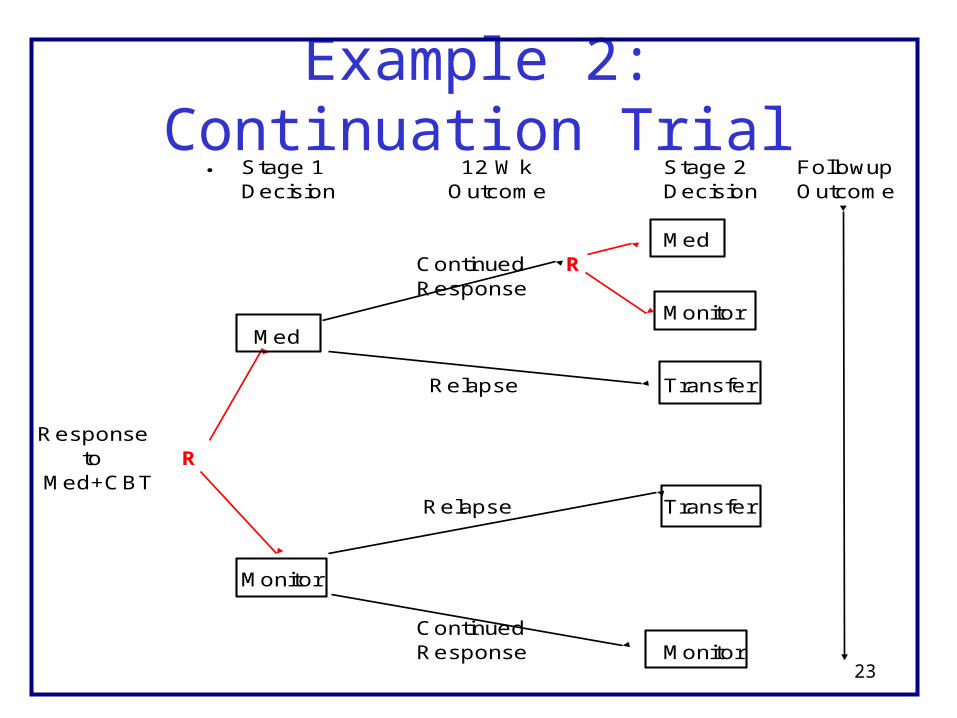
Example 2: Classical Continuation Trial
Subjects who have responded are randomized to one of three groups:
1) Continue on lower intensity version of treatment for 24 additional weeks as long as there is no relapse
2) Continue on lower intensity version of treatment for 12 additional weeks as long as there is no relapse
3) No treatment as long as there is no relapse
23
Example 2: Continuation TrialStage 1 12 Wk Stage 2 FollowupDecision Outcome Decision Outcome
Med Continued R Response Monitor
Med
Relapse Transfer
Response to R Med+CBT
Relapse Transfer
Monitor
Continued Response Monitor

24
Example 2: Continuation to SMART Initial 12 Wk Second Followup Decision Outcome Decision Outcome
Med Continued R Response Monitor
Med
Relapse Med +CBT
Response to R Med+CBT Med
Relapse RCBT
Monitor
Continued Response Monitor